")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Non-Selective Alpha-Blockers Provide More Stable Intraoperative Hemodynamic Control Compared with Selective Alpha1-Blockers in Patients with Pheochromocytoma and Paraganglioma: A Single-Center Retrospective Cohort Study with a Propensity Score-Matched Analysis from China
Authors Yang Y, Zhang J, Fang L, Jia X, Zhang W
Received 16 June 2022
Accepted for publication 28 September 2022
Published 17 October 2022 Volume 2022:16 Pages 3599—3608
DOI https://doi.org/10.2147/DDDT.S378796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Yang Yang,1,2 Jie Zhang,3 Liqun Fang,2 Xue Jia,1,2 Wensheng Zhang1,2
1Laboratory of Anaesthesia & Critical Care Medicine, Translational Neuroscience Center, The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 2Department of Anaesthesiology, West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3Department of Anaesthesiology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China
Correspondence: Wensheng Zhang, Laboratory of Anaesthesia & Critical Care Medicine, Translational Neuroscience Center, The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, West China Hospital of Sichuan University, Chengdu, People’s Republic of China, Tel/Fax +81-28-85164144, Email [email protected]
Purpose: Alpha-adrenergic blockers are used in the preoperative preparation of patients with pheochromocytomas and paragangliomas (PPGLs) despite the controversial on perioperative hemodynamics. We aimed to determine whether selective or non-selective α-adrenergic blockers can provide better efficacy on patients’ intraoperative hemodynamics.
Patients and Methods: This single-center retrospective study was conducted in 2507 adult patients undergoing PPGL resections, patients received alpha-adrenergic receptor blockers as a binary variable (selective or non-selective). Propensity score matching was performed and 201 patients were matched successfully.
Results: A total of 201 patients with PPGL were included in this study. The HI score scores were higher in the selective group than in the non-selective group (60.5 [44.5– 84.0] vs 49.0 [37.0– 67.25], P=0.027), as well as in the hemodynamic variables section [14.0 [8.0– 20.0] vs 10 [6.0– 16.0], P=0.009). In terms of specific indicators for each component, the lowest MAP in the selective group (55± 10 mmHg vs 59± 8 mmHg, P=0.038), the time to MAP below 60 mmHg (0.011% vs 0.022%, P=0.033) and the use of other vasoconstrictors (56.5% vs 35.5%, P=0.019) were significantly lower than in the non-selective group. Among the secondary outcome indicators, the incidence of intraoperative maximum SBP was significantly higher in the selective group than in the non-selective group (32.3% vs 11.3%, P=0.005). There were no significant differences in postoperative outcome indicators between the two groups.
Conclusion: In patients with PPGL, patients prepared preoperatively with non-selective alpha-blockers presented more stable hemodynamics intraoperatively compared to selective alpha1-blockers.
Keywords: α-adrenergic blockers, PPGLs, hemodynamic instability, perioperative management
Introduction
Pheochromocytomas (PCC) and paragangliomas (PGL) are two types of relatively rare neuroendocrine tumors that are referred to as PPGLs.1,2 PPGLs cause severe hypertension, as well as a variety of cardiovascular, cerebral, renal vascular problems, and metabolic alterations. The severity of complications depends on the type and amount of catecholamines produced, while there is no direct association between severe hypertension and elevated plasma concentrations of catecholamines.
Complete surgical resection is the curative treatment for PPGLs.3,4 Severe hemodynamic fluctuations and shock can occur during PPGL surgery, due to acute withdrawal of catecholamines by tumor resection.5 Due to the varied effects on catecholamine release and the acting time, some researchers have suggested that α-adrenergic receptor blockers could cause intraoperative or postoperative hypotension.6,7 However, the preoperative use of α-adrenergic receptor blockers has still been recommended by several guidelines.8,9
To improve efficiency and reduce adverse effects, researchers have tried to find a more suitable subtype of alpha-adrenergic blockers. Some studies have compared the effects of non-selective alpha- with selective alpha1-adrenergic blockers on intraoperative hemodynamics and clinical outcomes, however, the results varied.4,10–13
Therefore, we conducted this study to determine whether selective α1-adrenergic or non-selective alpha-adrenergic blockers are more effective for the perioperative management of patients with PPGL, and propensity score matching was used to control for confounding factors.
Materials and Methods
Study Design and Participants
We conducted a retrospective cohort study of 2077 patients who underwent PPGL resection at the West China Hospital of Sichuan University from 1 January 2016 to 31 December 2020. This study complied with the Declaration of Helsinki and was approved by review of the Clinical Research Ethics Committee of the West China Hospital of Sichuan University [Ethics approval number: 2022 Review (136)] and was registered in the Chinese Clinical Trial Registry (ChiCTR2200057291), and the patients provided their written informed consent to participate in this study.
Study Inclusion and Exclusion Criteria
In this study, adult patients who underwent surgery for PPGLs and had postoperative pathological diagnosis of confirmed PPGLs were allocated. Exclusion criteria include not using alpha-blockers for preoperative preparation, bilateral PPGLs, receiving complex surgery or multiple surgeries, and incomplete information.
Preoperative Preparation
Patients received selective alpha-1 or non-selective alpha-blockers for 2–4 weeks before surgery, respectively, titrated according to blood pressure. If normotension could not be achieved, calcium channel blockers were added to maintain blood pressure control. If a patient developed symptomatic tachycardia after an alpha-blocker, a beta-blocker was added to continue treatment. In addition, patients were instructed to consume high-sodium foods and more fluids to increase blood volume.
Data Collection
All data were extracted from the electronic patient data monitoring system starting with induction of anesthesia and ending with discharge from the post-anesthesia care unit or the intensive care unit. We mainly collected preoperative data that included demographic data (sex, age, body mass index (BMI), comorbidities, American Society of Anesthesiologists (ASA) classification), typical symptoms, maximum tumor diameter, pathological diagnosis, plasma catecholamine level, preoperative preparation medication, other antihypertensive drugs, β-blockers, preoperative infusion volume status, blood pressure one day before surgery, and heart rate one day before surgery.14
Surgical data included intraoperative hemodynamic status [Systolic arterial pressure (SAP), mean arterial pressure (MAP), and heart rate (HR)], the mode and time of surgery, the mode and time of maintenance of anesthesia, the amount of intraoperative vasoactive drugs and the level of intraoperative fluid infusion.
Postoperative data including 24-hour postoperative SBP, 24-hour postoperative HR, 24-hour postoperative fluid volume, postoperative use of vasoactive drugs, postoperative complications (Clavien-Dindo) classification,15 and postoperative hospital stay were recorded in our study.
Outcomes
The primary outcome was the intraoperative hemodynamic instability score (HI-score); it consists of three components: hemodynamic variables (ie, blood pressure and heart rate), vasoactive drug dosage, and fluid input level.16
Secondary outcomes included the incidence of severe hemodynamic fluctuations (including intraoperative SBP > 200 mmHg, MAP below 40 mmHg, HR > 120 beats/min and HR below 40 beats/min), 24-hour postoperative hemodynamic indices (including SBP and HR), 24-hour postoperative total fluid input, postoperative vasoactive drug use, postoperative complications (Clavien-Dindo) grading, and postoperative hospital stay.
Statistical Analyses
All data were evaluated by SPSS (SPSS Inc., Chicago, USA). The Shapiro–Wilk test was used to assess data normality. Normally distributed continuous variables were expressed as means ±SD and are analyzed using Student’s t-test. Abnormality distributed continuous variables are expressed as median (IQR) and were analyzed by Independent-Samples Mann–Whitney U-test. Qualitative variables are expressed as frequencies and percentages and were analyzed using the χ2-test or Fisher’s exact tests. P < 0.05 was considered statistically significant for the two groups of data tested.
A propensity score matching (PSM) model was established to balance differences in baseline characteristics between the two groups (Table 1). We identified 84 patients who were treated with non-selective α-adrenergic blockers and 117 patients with selective-1 α-adrenergic blockers. Finally, we successfully matched 62 pairs who had propensity scores of 0.04 (20% of the standard deviation of the overall propensity score)17 based on the following patient characteristics: age, sex, BMI, comorbidities, typical symptoms, plasma catecholamine levels, maximum tumor diameter, pathological diagnosis, use of other antihypertensive drugs, use of β-blockers, preoperative volume expansion, systolic blood pressure one day before surgery, heart rate one day before surgery, ASA classification, duration of anesthesia, mode of anesthesia maintenance, surgical time, and surgical approach. After matching was completed, the absolute standardized differences of the matched variables were further calculated for assessment.
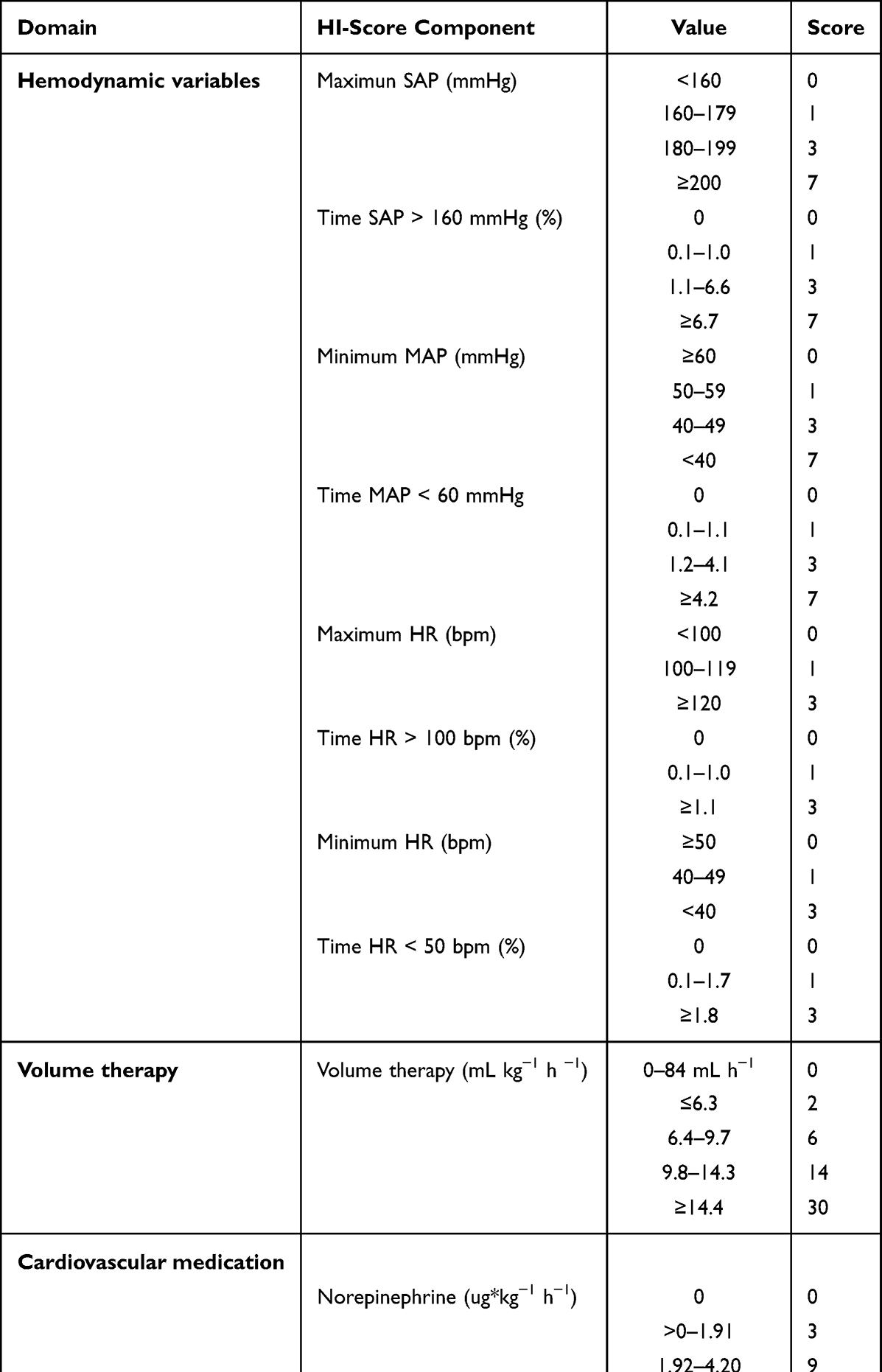 |
Table 1 Weighted Scores for Each Item for HI Score |
Results
A total of 2507 adult patients underwent surgery for PPGLs from 1 January 2016 to 31 December 2020. Of these, 351 patients were confirmed with PPGLs after postoperative pathology. A total of 150 patients met the exclusion criteria and were not included in the analysis, of which, 117 patients did not use or used both alpha-blockers for preoperative preparation, 9 patients had bilateral PPGLs, 14 patients underwent complex surgery or multiple surgeries, and 10 patients had incomplete data. A total of 201 patients were finally included in the analysis and were divided into a non-selective group (n=83) and a selective group (n=118) according to the type of α-blocker used preoperatively. To control the cofounders and risk factors, a propensity score at a 1:1 ratio was performed, and 62 pairs matched successfully (Figure 1).
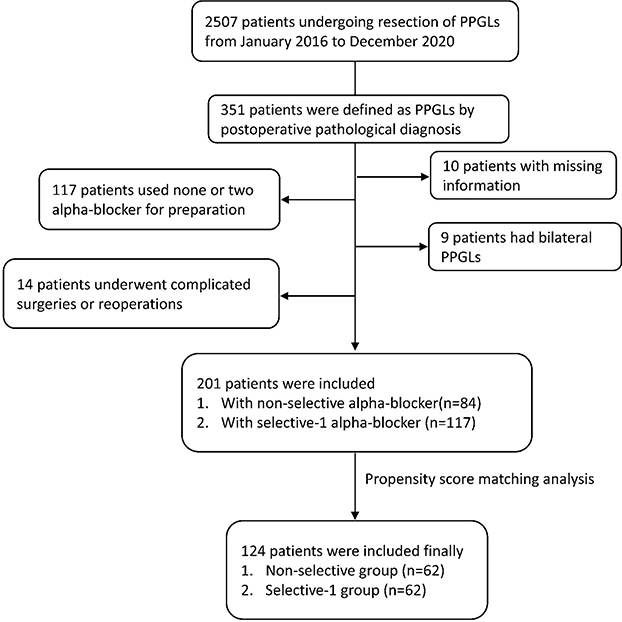 |
Figure 1 Study flowchart. Abbreviation: PPGLs, pheochromocytoma and paraganglioma. |
Baseline Characteristics
The surgeon decided the type of alpha-blocker to be used preoperatively according to the clinical condition of the patients.83 patients (41.3%) were given non-selective alpha-blocker phenazopydidine, while 118 patients were given selective alpha1-blockers, including 56 (27.9%) of terazosin, 49 (24.3%) of prazosin and 13 (6.5%) of doxazosin.
As shown in Table 2, there were no significant differences in preoperative baseline information between patients in the non-selective and selective-1 groups after propensity score matching was performed, including sex, age, BMI, ASA, comorbidities, clinical symptoms, pathological diagnosis, pretreatment drugs, daily expansion of plasma volume, preoperative 24-hour SAP and HR. We also analyzed factors related to surgery and anesthesia and found no statistically significant differences between the two groups after propensity matching (Table 3).
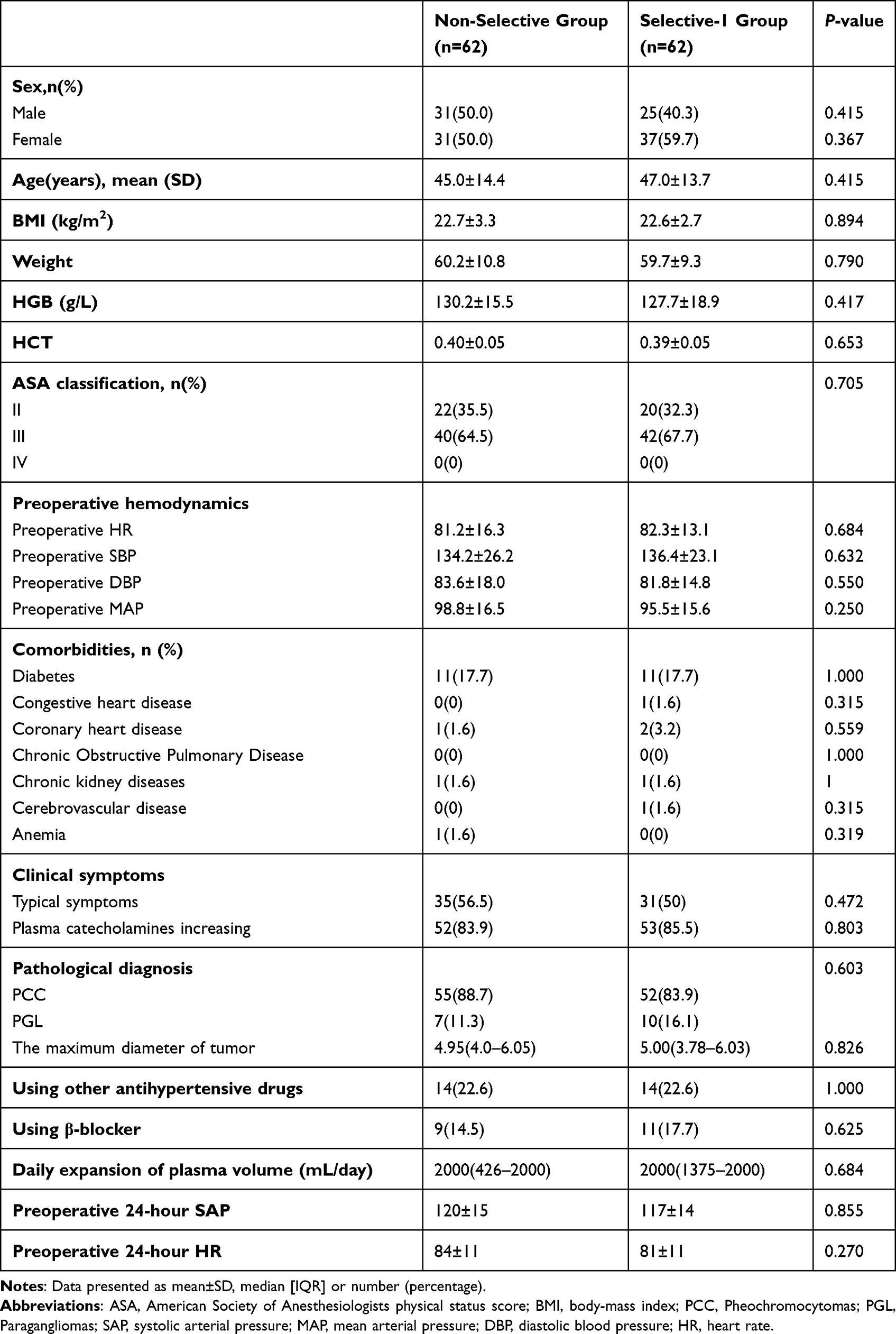 |
Table 2 Baseline Characteristics of PPGLs Patients with Non-Selective or Selective-1 Alpha-Blocker Treatment |
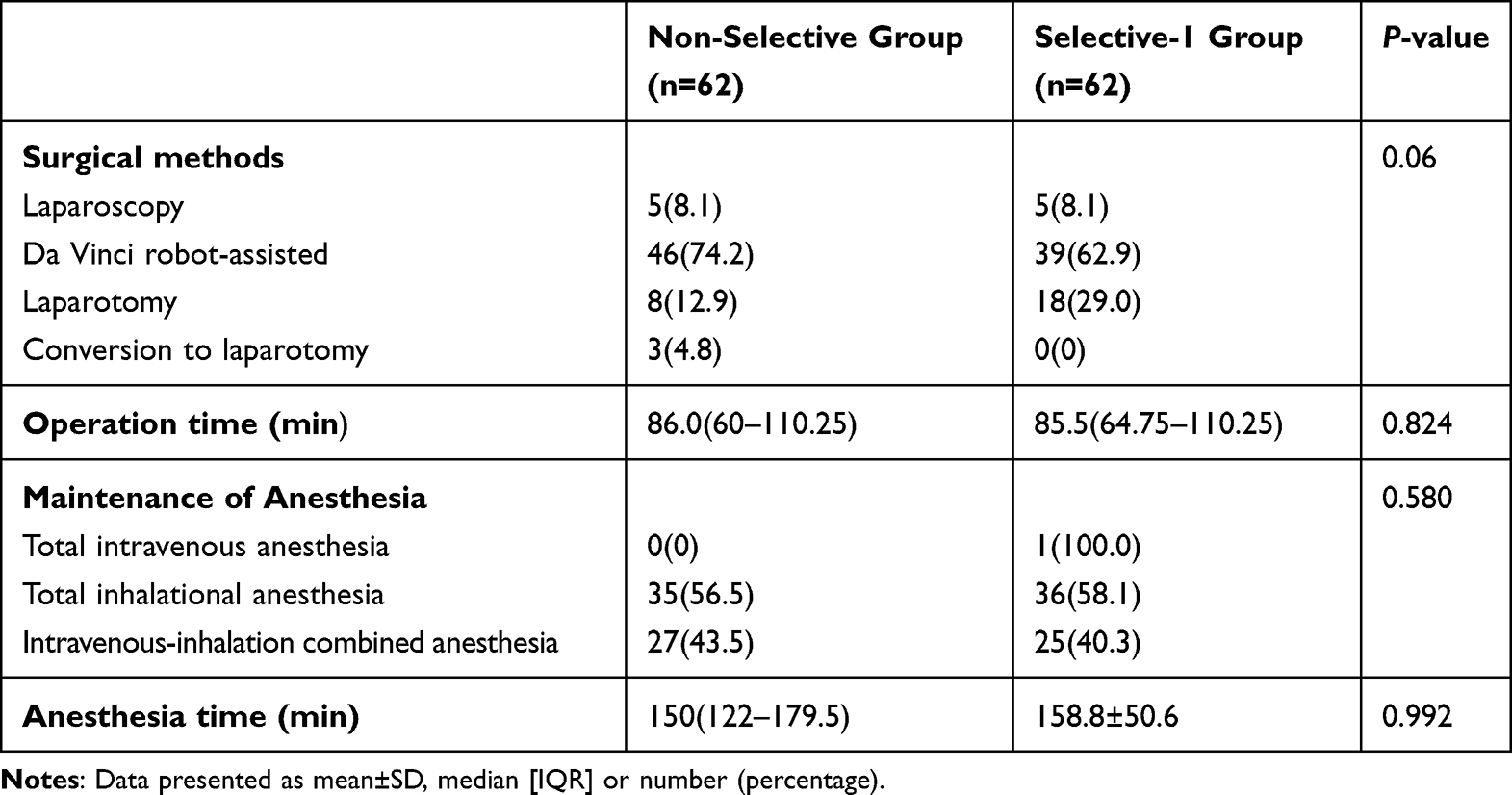 |
Table 3 Surgery- and Anesthesia-Related Information of PPGLs Patients with Non-Selective or Selective-1 Alpha-Blocker Treatment |
Outcomes
As shown in Table 4, the total HI-score scores were higher in the selective-1 group than in the non-selective group (60.5 [44.5–84.0] vs 49.0 [37.0–67.25], P=0.027), and showed the same trend in the hemodynamic variables section (14.0 [8.0–20.0] vs 10 [6.0–16.0], P=0.009). However, there were no significant differences in the volume therapy and cardiovascular drug scores between the two groups. In terms of specific outcomes in each section, the minimum MAP (55±10 mmHg vs 59±8 mmHg, P=0.038), time MAP <60 mmHg (0.011% vs 0.022%, P=0.033), and the use of other vasoconstrictors (56.5% vs 35.5%, P=0.019) in the selective-1 group was significantly lower than the non-selective group, and the remaining outcomes showed no statistically significant differences.
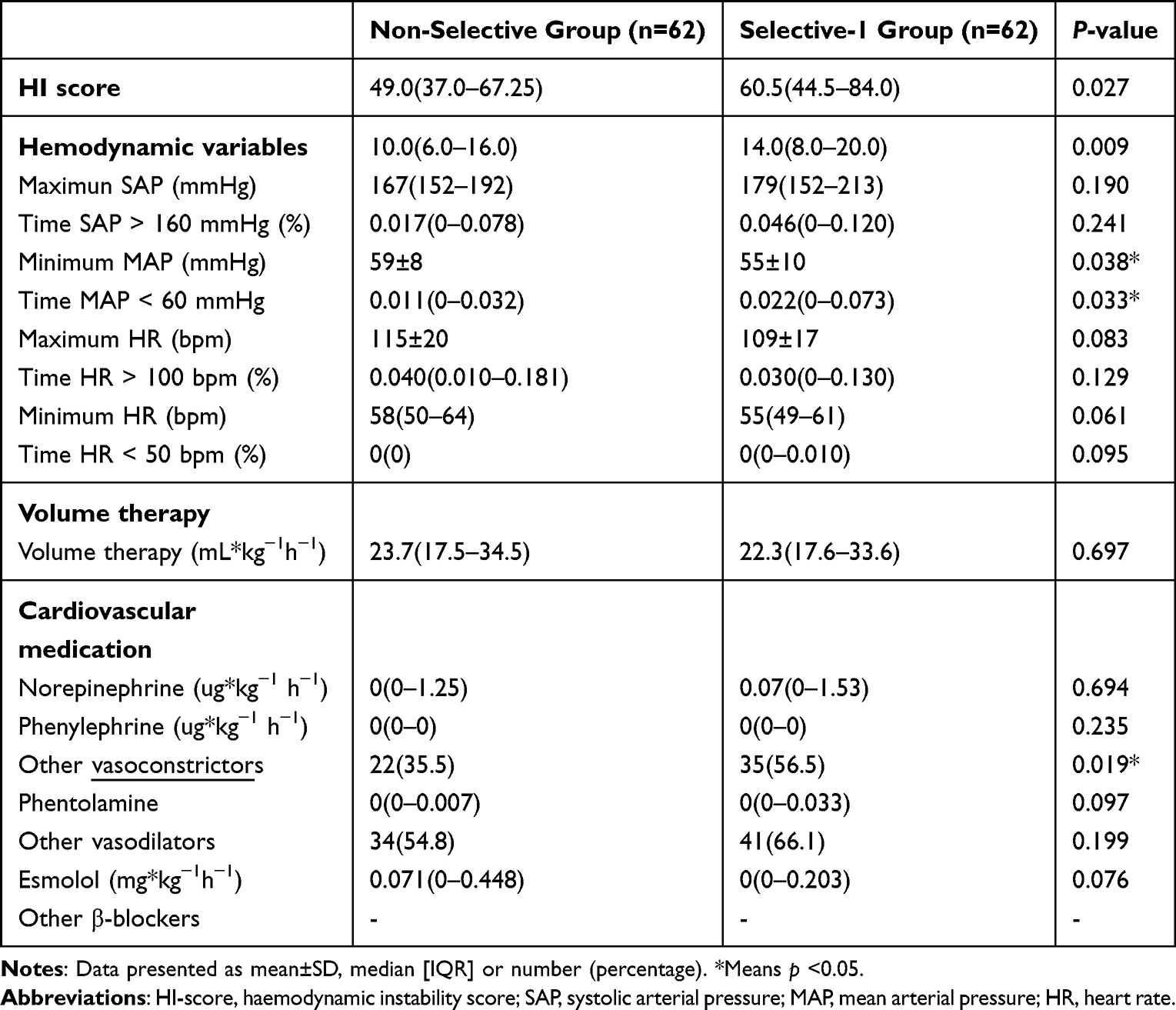 |
Table 4 Primary Outcomes of PPGLs Patients with Non-Selective or Selective-1 Alpha-Blocker Treatment |
As shown in Table 5, the incidence of SBP> 200 mmHg was significantly higher in the selective-1 group than in the non-selective group (32.3% vs 11.3%, P=0.005). There were no significant differences between the two groups in terms of perioperative and postoperative 24-hour MAP and HR, total volume of infusion, postoperative vasoactive agents, postoperative Clavien-Dindo classification and postoperative hospital stay.
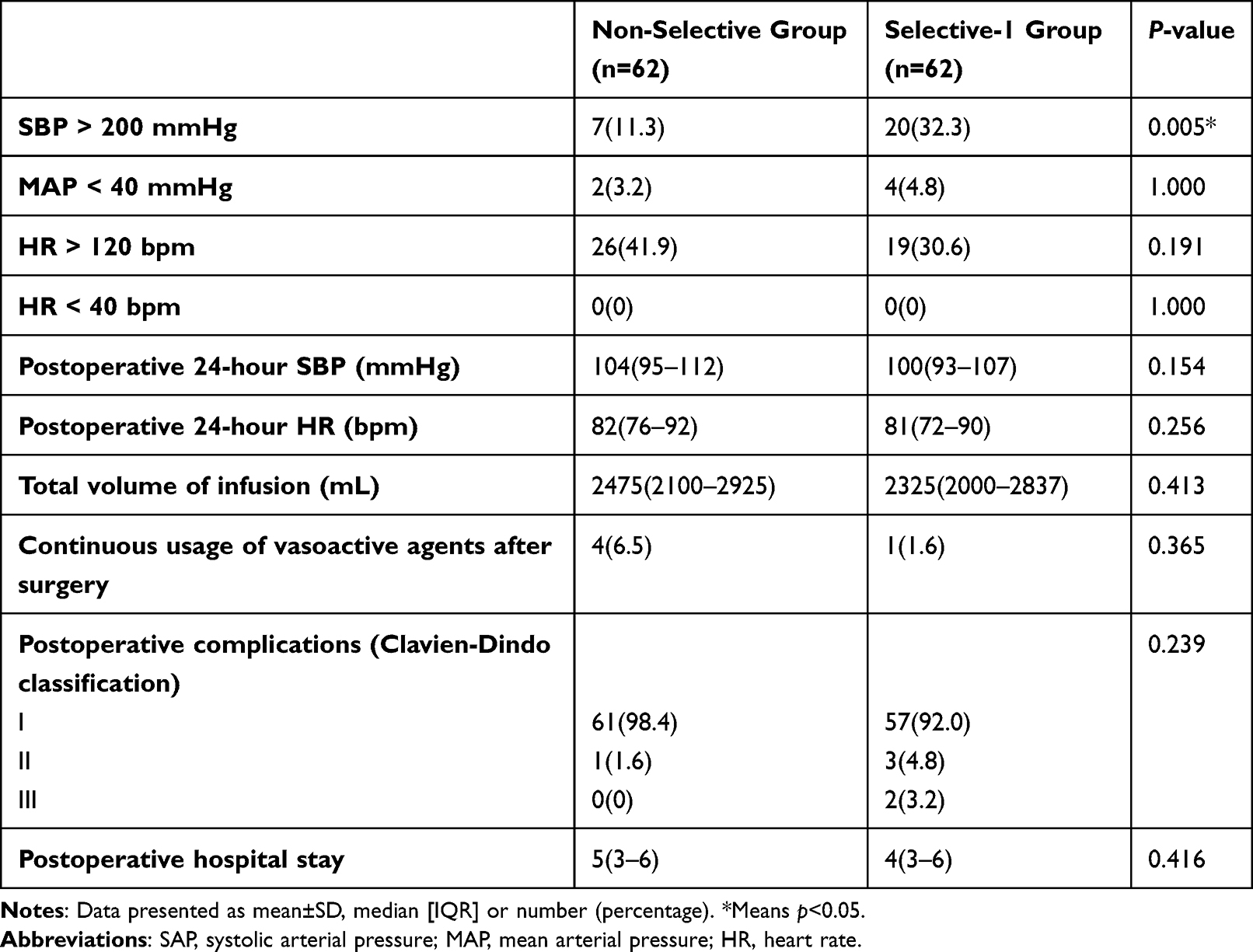 |
Table 5 Secondary Outcomes of PPGLs Patients with Non-Selective or Selective-1 Alpha-Blocker Treatment |
Discussion
In this retrospective cohort study with propensity score matching, we demonstrated that the use of non-selective alpha-adrenergic blockers were associated with more stable hemodynamics intraoperatively compared to selective alpha1-adrenergic blockers in patients with PPGL.
A number of previous studies have produced conflicting results regarding the effects of two types of α-blockers on perioperative hemodynamics in patients with PPGLs. Some studies have shown that non-selective α-blockers are superior to selective α1-blockers, but others have found opposite results or no difference. Weingarten et al compared two preoperative management protocols at the Mayo Center and the Cleveland Center and found that phenibutin resulted in better control of intraoperative blood pressure and reduced intraoperative fluid input levels reducing intraoperative fluid rehydration, but the incidence of hypotension was significantly higher.18 Agrawal et al compared the hemodynamic effects of preoperative phenazopyridine and prazosin and found that phenazopyridine was superior to prazosin in maintaining intraoperative hemodynamic stability and that patients in the prazosin group experienced more frequent blood pressure elevations than the phenazopyridine group.19 However, studies by Conzo and Zhu et al showed higher intraoperative systolic blood pressure fluctuations in patients using non-selective α-blockers.20,21 On the other hand, the study by Malec and Kocak et al showed no significant differences in intraoperative and postoperative hemodynamic status of patients regardless of the preoperative choice of alpha-blocker.22 The reasons for controversial results may be a small sample size, uncontrolled confounding factors, and insufficiently clear outcome measures.
Previous investigators evaluated whether patients were hemodynamically stable by blood pressure thresholds (SBP greater than 160 mmHg and MAP less than 60 mmHg), but it should be noted that intraoperative blood pressure levels can be affected by certain doses of general anesthetics, vasoactive drugs and intravenous fluids used by anesthesiologists, and these interventions have been recognized as essential markers of hemodynamic stability.11 To reduce the influence of confounding factors and to provide a relatively intuitive analysis of results with a large sample size, we used propensity score matching to control factors, then HI score was chosen for semi-quantitative outcome analysis. The reason we used HI score as our primary outcome is because the most visual manifestation of hemodynamic instability is the change in blood pressure and heart rate, and this change is mainly affected by vasoactive drugs and fluids in addition to intraoperative stimulation and bleeding. And in an article which used HI as a secondary outcome, they found their primary endpoint (the median cumulative time outside the blood pressure target range during surgery) had no significant difference between groups, while the HI score has a significant statistical difference.22 Thus, we think HI score can be a primary outcome instead the cumulative time.
In our study, we found that for patients with PPGLs, preoperative use of a non-selective α-blocker compared to selective α1-blockers had more stable intraoperative hemodynamics with an incidence of intraoperative maximum blood pressure greater than 200 mmHg. This result may be due to the competitive nature of selective α1-blockers, so that they are ineffective against excessive intraoperative catecholamine release and may theoretically be less effective in controlling blood pressure intraoperatively. This is consistent with the results conducted by Edward et al who showed that there was no difference in the duration of blood pressure outside the target range during resection of PPGLs, regardless of preoperative phenibut or doxazosin, but that phenibut was more effective in preventing intraoperative hemodynamic instability.23 The results of a recent Meta-analysis also showed that the highest intraoperative systolic blood pressure value was lower in the non-selective α-blocker group than in the selective group (P< 0.0001), and there were fewer cases of systolic blood pressure above 200 mmHg than in the selective α1-blocker group (P=0.04), while there was no significant difference in the lowest intraoperative systolic blood pressure value and range of fluctuations, suggesting that the selection of non-selective α-blockers was more effective than Selective α1-blockers are more effective in lowering blood pressure and can reduce complications caused by rapid perioperative blood pressure rise, including cardiovascular, cerebrovascular and renal events, and have more stable blood pressure control, so intraoperative safety is higher.24
Furthermore, compared to the non-selective group, patients in the selective-1 group had a lower minimum MAP, a longer time < 60 mmHg, and a higher incidence of SBP over 200 mmHg. Selective α1-adrenergic blockers, containing doxazosin, prazosin, and terazosin, are more hemodynamically unstable because they are short-A cting and have a limited effect on blood pressure fluctuations caused by excessive intraoperative catecholamine release.4,5 In contrast, non-selective adrenergic blockers are long-acting and remain effective in the presence of excessive intraoperative catecholamine release. Although there were differences in hemodynamic variables, the incidence of short-term complications and other postoperative indicators did not differ significantly between the two groups, which was also confirmed in previous studies,12,13,22,25 suggesting that the lower mean arterial pressure in the selective-1 group did not result in serious consequences in the short term.
Strengths of this study include a relatively large sample size of rare tumors, data obtained from an electronic medical record system and therefore less subject to observer bias, and the use of propensity score matching to further reduce bias.
There were, however, some limitations to this study. First, the cases collected in this study span 5 years, and clinical practice has changed accordingly during this period. Despite the propensity score matching, we could not exclude residual imbalances or biases arising from unidentified factors when comparing the results of the two patient populations. Second, as a retrospective study, we did not collect data on the incidence of adverse reactions, which may have differed between patients using selective α1- or non-selective α-adrenergic blockers. Further large prospective RCTs are needed to validate preferences for preoperative α-blockade in patients with PPGL.
Conclusion
In patients with PPGLs, patients receiving preoperative treatment with non-selective alpha-blockers presented more stable hemodynamics intraoperatively compared to selective alpha1-blockers, although it is uncertain whether their use is associated with better clinical outcomes.
Data Sharing Statement
Individual participant data underlying published results reported in this study can be accessed with approval from the corresponding author after 6 months of publication of the main results. The study protocol, statistical analysis plan, and clinical study report will also be available.
Funding
This research was supported by the West China Hospital Postdoctoral Sustentation Fund (2020HXBH096, Y.Y.).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kim JH, Moon H, Noh J, Lee J, Kim SG. Epidemiology and prognosis of pheochromocytoma/paraganglioma in Korea: a nationwide study based on the national health insurance service. Endocrinol Metab. 2020;35(1):157–164. doi:10.3803/EnM.2020.35.1.157
2. Turkova H, Prodanov T, Maly M, et al. Characteristics and outcomes of metastatic sdhb and sporadic pheochromocytoma/paraganglioma: an national institutes of health study. Endocr Pract. 2016;22(3):302–314. doi:10.4158/EP15725.OR
3. Neumann HPH, Young WF
4. García M, Palasí R, Gómez RC, Marco JLP, Merino-Torres JF. Surgical and Pharmacological Management of Functioning Pheochromocytoma and Paraganglioma. In: Mariani-Costantini R, editor. Paraganglioma: A Multidisciplinary Approach. Brisbane (AU): Codon Publications. Copyright: The Authors; 2019.
5. Lenders JW, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(6):1915–1942. doi:10.1210/jc.2014-1498
6. Groeben H, Nottebaum BJ, Alesina PF, Traut A, Neumann HP, Walz MK. Perioperative α-receptor blockade in phaeochromocytoma surgery: an observational case series. Br J Anaesth. 2017;118(2):182–189. doi:10.1093/bja/aew392
7. Groeben H, Walz MK, Nottebaum BJ, et al. International multicentre review of perioperative management and outcome for catecholamine-producing tumours. Br J Surg. 2020;107(2):e170–e178. doi:10.1002/bjs.11378
8. Lenders JWM, Kerstens MN, Amar L, et al. Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: a position statement and consensus of the working group on endocrine hypertension of the European society of hypertension. J Hypertens. 2020;38(8):1443–1456. doi:10.1097/HJH.0000000000002438
9. Pacak K. Preoperative management of the pheochromocytoma patient. J Clin Endocrinol Metab. 2007;92(11):4069–4079. doi:10.1210/jc.2007-1720
10. Weingarten TN, Cata JP, O’Hara JF, et al. Comparison of two preoperative medical management strategies for laparoscopic resection of pheochromocytoma. Urology. 2010;76(2):508.e506–511. doi:10.1016/j.urology.2010.03.032
11. Malec K, Miśkiewicz P, Witkowska A, et al. Comparison of phenoxybenzamine and doxazosin in perioperative management of patients with pheochromocytoma. Kardiol Pol. 2017;75(11):1192–1198. doi:10.5603/KP.a2017.0147
12. Randle RW, Balentine CJ, Pitt SC, Schneider DF, Sippel RS. Selective versus non-selective α-blockade prior to laparoscopic adrenalectomy for pheochromocytoma. Ann Surg Oncol. 2017;24(1):244–250. doi:10.1245/s10434-016-5514-7
13. Liu C, Lv Q, Chen X, et al. Preoperative selective vs non-selective α-blockade in PPGL patients undergoing adrenalectomy. Endocr Connect. 2017;6(8):830–838. doi:10.1530/EC-17-0232
14. Buisset C, Guerin C, Cungi PJ, et al. Pheochromocytoma surgery without systematic preoperative pharmacological preparation: insights from a referral tertiary center experience. Surg Endosc. 2021;35(2):728–735. doi:10.1007/s00464-020-07439-1
15. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
16. Buitenwerf E, Boekel MF, van der Velde MI, et al. The haemodynamic instability score: development and internal validation of a new rating method of intra-operative haemodynamic instability. Eur J Anaesthesiol. 2019;36(4):290–296. doi:10.1097/EJA.0000000000000941
17. Kong H, Li N, Yang XC, Nie XL, Tian J, Wang DX. Nonselective compared with selective α-blockade is associated with less intraoperative hypertension in patients with pheochromocytomas and paragangliomas: a retrospective cohort study with propensity score matching. Anesth Analg. 2021;132(1):140–149. doi:10.1213/ANE.0000000000005070
18. Livingstone M, Duttchen K, Thompson J, et al. Hemodynamic stability during pheochromocytoma resection: lessons learned over the last two decades. Ann Surg Oncol. 2015;22(13):4175–4180. doi:10.1245/s10434-015-4519-y
19. Ma L, Shen L, Zhang X, Huang Y. Predictors of hemodynamic instability in patients with pheochromocytoma and paraganglioma. J Surg Oncol. 2020;122(4):803–808. doi:10.1002/jso.26079
20. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
21. Song G, Joe BN, Yeh BM, Meng MV, Westphalen AC, Coakley FV. Risk of catecholamine crisis in patients undergoing resection of unsuspected pheochromocytoma. Int Braz J Urol. 2011;37(1):35–40;discussion 40–31. doi:10.1590/S1677-55382011000100005
22. Buitenwerf E, Osinga TE, Timmers H, et al. Efficacy of α-blockers on hemodynamic control during pheochromocytoma resection: a randomized controlled trial. J Clin Endocrinol Metab. 2020;105(7):2381–2391. doi:10.1210/clinem/dgz188
23. Jiang M, Ding H, Liang Y, et al. Preoperative risk factors for haemodynamic instability during pheochromocytoma surgery in Chinese patients. Clin Endocrinol. 2018;88(3):498–505. doi:10.1111/cen.13544
24. Agrawal R, Mishra SK, Bhatia E, et al. Prospective study to compare peri-operative hemodynamic alterations following preparation for pheochromocytoma surgery by phenoxybenzamine or prazosin. World J Surg. 2014;38(3):716–723. doi:10.1007/s00268-013-2325-x
25. Kiernan CM, Du L, Chen X, et al. Predictors of hemodynamic instability during surgery for pheochromocytoma. Ann Surg Oncol. 2014;21(12):3865–3871. doi:10.1245/s10434-014-3847-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.