")
Back to Journals » Patient Preference and Adherence » Volume 16
Non-Adherence to Antiepileptic Drugs and Associated Factors among Epileptic Patients at Ambulatory Clinic of Southwestern Ethiopian Hospital: A Cross-Sectional Study
Authors Bekele F
Received 9 June 2022
Accepted for publication 15 July 2022
Published 2 August 2022 Volume 2022:16 Pages 1865—1873
DOI https://doi.org/10.2147/PPA.S377910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Firomsa Bekele
Department of Pharmacy, College of Health Science, Mattu University, Mattu, Ethiopia
Correspondence: Firomsa Bekele, Department of Pharmacy, College of Health Science, Mattu University, Mattu, Ethiopia, Email [email protected]
Background: Non-adherence to anti-epileptic drugs (AEDs) was the most common drug therapy issue that hampered epileptic patients’ treatment success. As a result, the barriers to patients adhering to their treatment should be investigated in depth in order to prevent poor treatment outcomes.
Methods: A hospital-based cross-sectional study was conducted on epileptic patients who had followed up at Mettu Karl Comprehensive Specialized Hospital (MKCSH). Data collection was done through patient interview and medical charts review. Hill-Bone Compliance to High Blood Pressure Therapy Scale was used to measure medication adherence. The data were analyzed using SPSS version 23 after data were entered by Epi Info7.2.1. The multivariable logistic regressions were utilized and P < 0.05 was used to declare association.
Results: Over the study period, more than half of the participants 172 (57.7%) were males, and the median age of participants was 29 years. The magnitude of non-adherence to ant-epileptic drugs (AEDs) was 120 (40.27%). The results of multivariable analysis revealed that patients who had experienced the medication side effects, adjusted odds ratio (AOR) = 2.199; 95% CI: 1.21, 4.00, P = 0.010, a poly-pharmacy, adjusted odds ratio (AOR) = 5.166; 95% CI: 2.63, 10.14, P = < 0.001 and the presence of a co-morbidity, adjusted odds ratio (AOR) =3.70; 95% CI: 2.058, 6.65, P = < 0.001 were the predictors of medication non-adherence.
Conclusion: The magnitude of non-adherences to AEDs was found to be high. Phenobarbitone was the most prescribed AEDs. The number of medications taken by the patients, the presence of co-morbidity and the occurrence of medication side effects had a significant association with non-adherence to AEDs. Therefore, the pharmaceutical care in general and drug information services in particular should be established to enhance medication adherence in our study area.
Keywords: non-adherence, epilepsy, associated factors, Ethiopia
Background
Epilepsy is a neurologic illness characterized by frequent seizures that affects around 50 million individuals worldwide, with more than three-quarters of them living in poor nations.1–3 Epilepsy affects 64 people out of every 100,000 people in Ethiopia.2
The degree to which a patient’s conduct matches to a health professional’s advice is referred to as medication adherence. Medication adherence is usually better when the patient is more involved in the treatment decision, as well as when the health professional and the patient work together and agree.4
Regardless, epilepsy drug therapy should be tailored to the patient’s specific needs in order to avoid drug-related complications.1
In low-resource areas, the vast majority of them lacked access to appropriate therapy. Antiepileptic medications (AEDs) efficiently control seizures in the vast majority of individuals. Even with the finest available treatment, more than 30% of persons with epilepsy do not achieve complete seizure control.5 Poor adherence to AEDs is one possible cause of epileptic treatment failure.5,6
Although various interventions have been undertaken to enhance anti-epileptic drug adherence in patients with epilepsy, most interventions appear to fall short of their objectives, and anti-epileptic medication non-adherence remains an issue.7
Non-adherence to AEDs was the most common drug therapy issue that hampered epileptic patients’ treatment success. As a result, the barriers to patients adhering to their treatment should be investigated in depth in order to prevent poor treatment outcomes.3
Noncompliance may result in seizure control failure, hospitalization, increased health-care costs, and a lower quality of life.3,8,9 Aside from that, the death rate is higher as a result of pharmaceutical therapy issues.9,10 As a result, AED non-adherence is one of the most common causes of epilepsy treatment gaps, and maintaining anti-epileptic medication adherence is critical for achieving the best therapeutic health results.7
The studies of different settings reported that about half of the epileptic patients were non-adherent to the AEDs.6,11 Non-adherence to AEDs has been linked to a number of conditions, including polytherapy, duration of the disease, lower education level, substance use, comorbidity, female sex, and a history of hospitalization.6,8,11,12 Despite this, there were a scanty of findings in Ethiopia, and no research has been done on the magnitude and predictors of anti-epileptic drug non-adherence among ambulatory clinic epileptic patients in our study area. Therefore, the study aimed to assess the magnitudes and determinants of non-adherence among ambulatory epileptic patients.
Patients and Methods
Study Area, Design and Period
A cross-sectional study was conducted at Mettu Karl Comprensive Specialized Hospital (MKCSH) from February 12, 2020 to August 11, 2020. MKCSH is found in Mattu town, South West Oromia, Ethiopia, which is found 600 km from Finfinne.
Study Participants and Eligibility Criteria
Adult patients (age ≥18 years) with the diagnosis of the epilepsy who have been on regular follow-up for at least two years with complete registration charts who were on drug therapy were included, whereas patients who had a follow-up period of less than two years, seriously ill to complete the interview, refused to give consent, and those with incomplete medical records were excluded.
Study Variables and Outcome Endpoints
The medication non-adherence was the primary outcome. Hill-Bone Compliance to Therapy Scale was used to measure medication adherence.13 For the purpose of this study, we used a 9-item medication-taking sub-scale. Each item is a 4-point Likert type scale (none of the time, some of the time, most of the time, and all the time). The median split was used and dichotomies into adherent and non-adherent to the treatment. The work has been reported in line with the strengthening of the reporting of cohort studies in surgery (STROCSS) criteria.14
Sample Size and Sampling Technique
A total of 311 epileptic patients were refilling their treatment at MKCSH from February 12, 2020 to August 11, 2020. However, 298 epileptic patients fulfilling the inclusion criteria were included in the final analysis. Hence, the study participants were selected using a convenience sampling technique.
Data Collection Process and Management
The standardized data collection tool was adapted to collect the data.13 For the purpose of this study, we selected the 9-item medication-taking subscale. The total scores on this subscale range from 9 to 36 with higher scores reflecting poorer adherence to antiepileptic drug. This 9-item adherence scale includes questions like asking how often patients forgot to take their medication, how often do you decide not to take your AEDs, how often do you forget to get prescriptions filled, how often do you run out of AEDs pills, how often do you skip your AEDs medicine before you go to the doctor, how often do you miss taking your AEDs pills when you feel better, how often do you miss taking your AEDs pills when you feel sick, how often do you take someone else’s AEDs pills, and how often do you miss taking your AEDs pills when you are careless. The median split was used and dichotomized into two groups 1 = Adherent to the treatment and 0 = Non-adherent to the medication. The current medications, co-morbidities, relevant previous medical and medication histories were collected using data abstraction format from medical chart review. Three medical doctors and two clinical pharmacists were recruited for data collection; one clinical pharmacist was assigned to supervise the data collection process. To ensure the consistency of the data collection tool, it was pretested at a nearby hospital called Bedele General Hospital prior to the data collection.
Data Processing and Analysis
The data were entered into a computer using EpiData version 3.1 developed by JM Lauritsen M Bruus.15 Principal investigators had daily checked and cleaned the data. The data were then exported to Statistical Software for Social Sciences (SPSS) 24.0 for analysis. Multivariable logistic regression was used to analyze the variable by using crude odds ratio (COR) and adjusted odds ratio (AOR) with 95% CI. All variables associated with the drug-related problems at a P-value ≤0.25 on the bivariate analysis were entered into a multivariable logistic regression analysis to control for confounders. Finally, the predictors of non-adherence to AEDs were declared if a P value of ≤0.05
Ethics Approval and Consent-to-Participate
Ethical approval was obtained from the Research Ethics Review Committee (RERC) of Mattu University with no CHS/RERC/89/2020. The study protocol was performed in accordance with the Declaration of Helsinki. Permission was given by the administrators and medical directors of MKCSH to conduct the study. The pros and cons of the study were explained to the patients participating in the study, and written informed consent was obtained from patients. The names of patients and prescribers were not written on the tool to ensure confidentiality.
Operational Definitions
Non-adherence: Below median split of medication adherence scale.13
Adherence: Above median split of medication adherence scale.13
Poly-pharmacy: The daily consumption of 5 or more medications.16
Co-morbidity: Patients diagnosed with two or more diseases.16
Result
Socio-Demographic Characteristics of Participants
Over the study period, more than half of the participants 172 (57.7%) were males. The median age of the participants was 29 years and was majorly distributed to age of 18–30-year class. Majority, 235 (78.9%) of participants were single and 139 (46.6%) of were attended high school (Table 1).
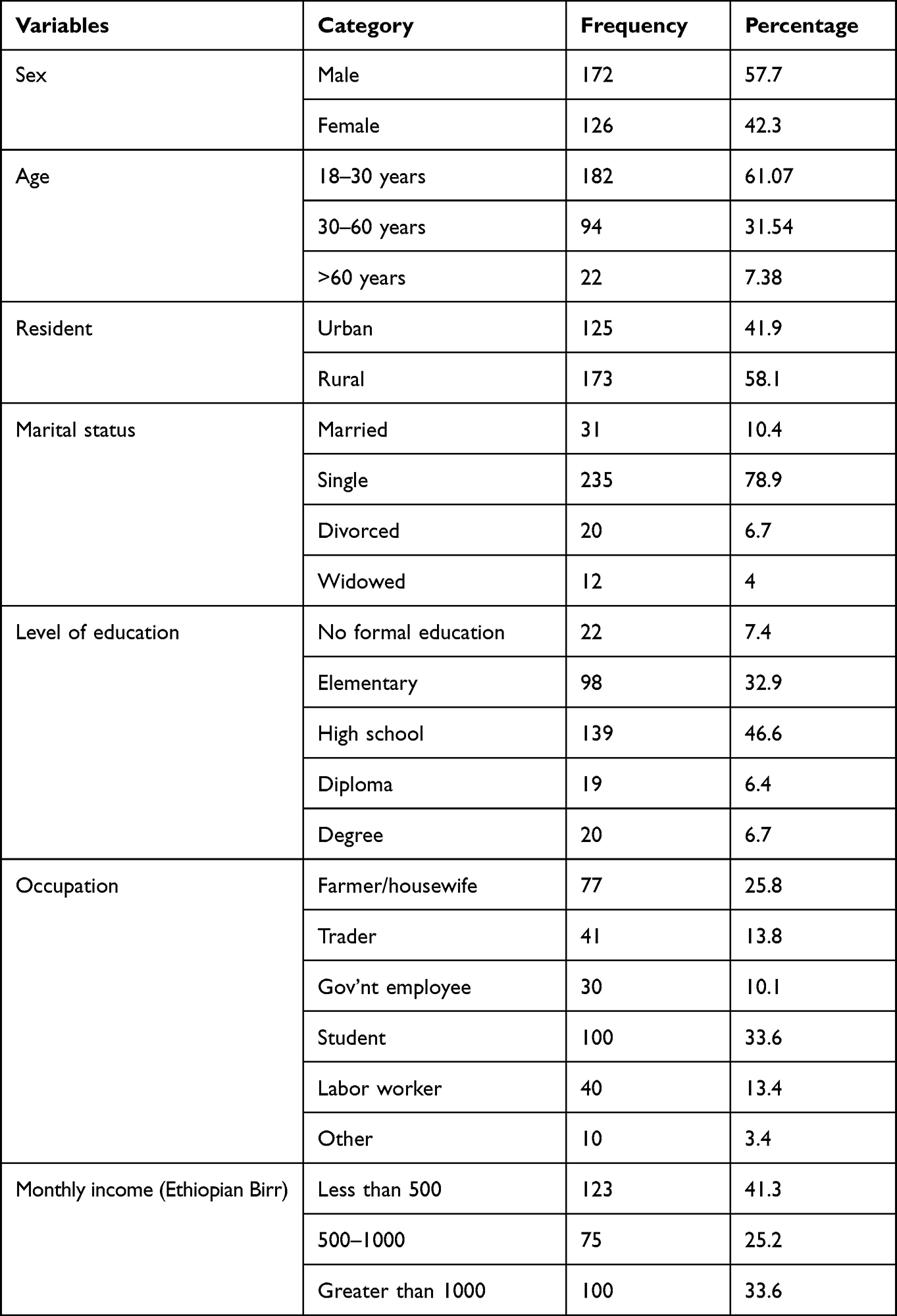 |
Table 1 Socio-Demographic Characteristics of Epileptic Patients at Ambulatory Clinic of Southwestern Ethiopian Hospital |
Clinical Characteristics of the Epileptic Patients
Among majority 249 (83.6%) of participants, the onset of seizure was in less than 30 years of age. More than one fourth of the patients were suffering from absent seizure 85 (28.5%) and general tonic clonic 83 (27.9%). More than half, 169 (56.7%) of the participants had a history of head injury; nearly two third of the patients have no family history of epilepsy and 92 (30.9%) had comorbidity (Table 2).
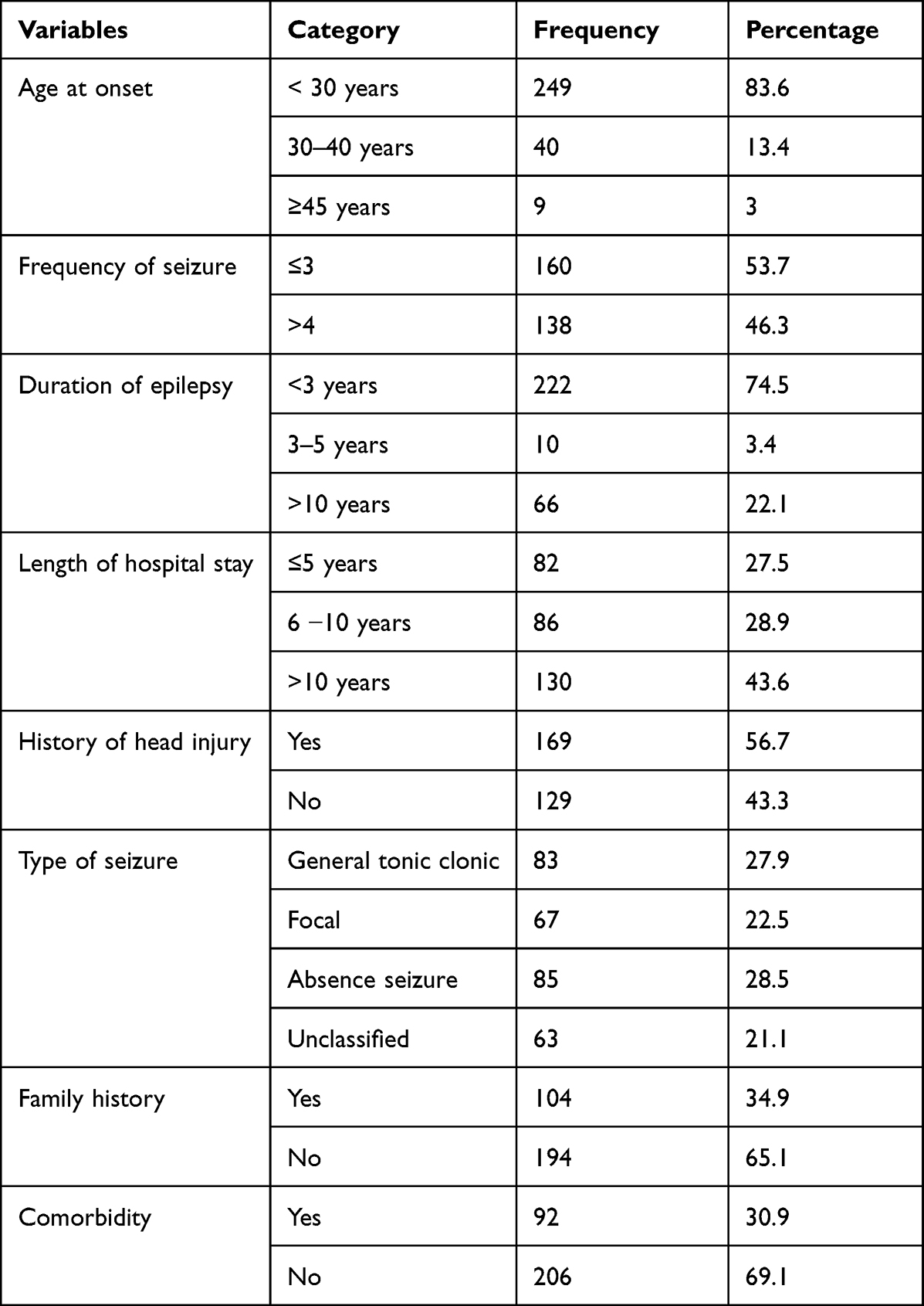 |
Table 2 Clinical Characteristics of Epileptic Patients at Ambulatory Clinic of Southwestern Ethiopian Hospital |
Medication Characteristics of Epileptic Patients
The most commonly prescribed medication was Phenobarbitone that accounts 34 (11.41%), whereas Valproic acid 8 (2.68%) was the least prescribed. Poly pharmacy was reported among 70 (23.5%) of the epileptic patients (Table 3).
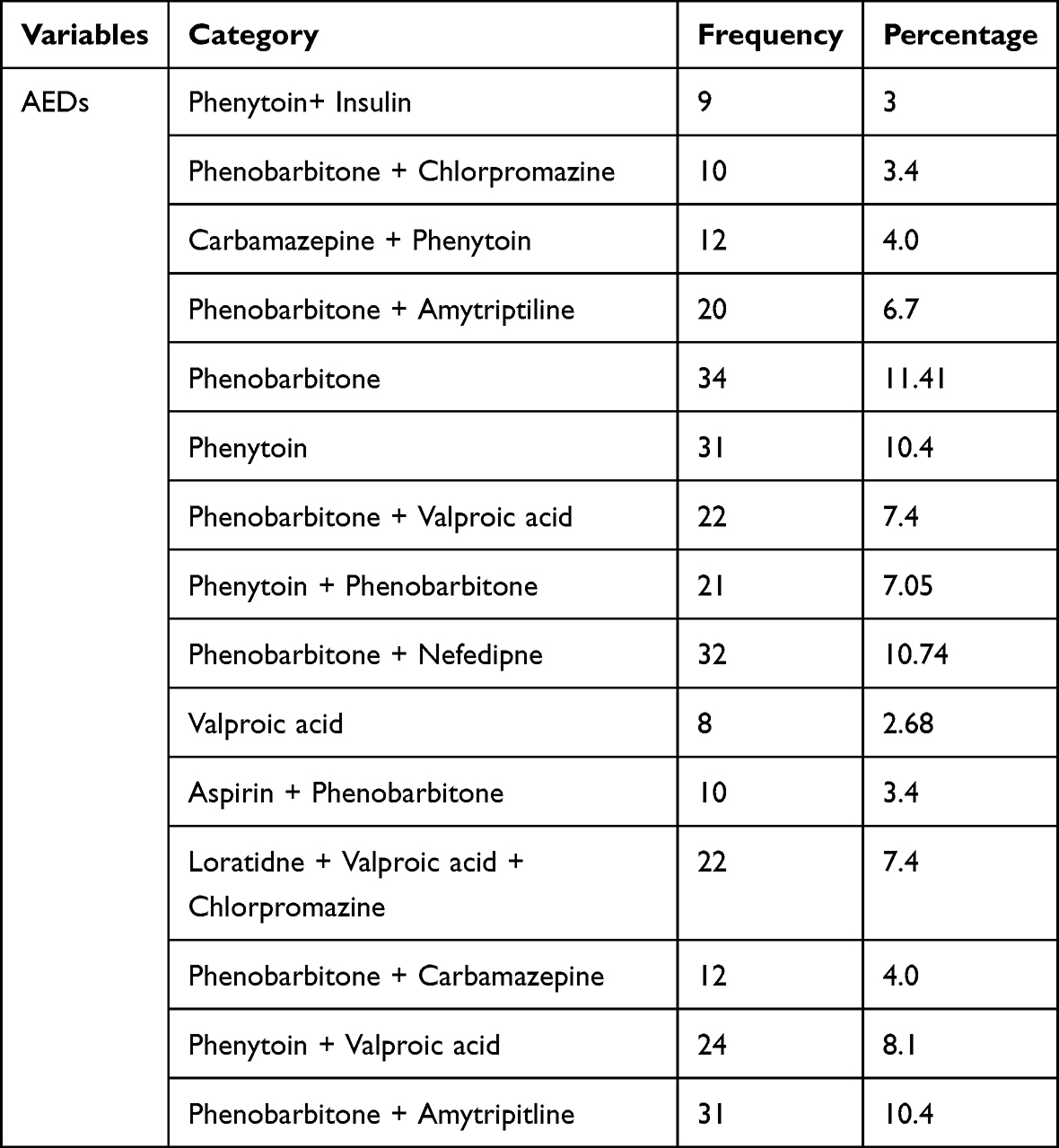 |
Table 3 Commonly Prescribed Antiepileptic Drugs at Ambulatory Clinic of Southwestern Ethiopian Hospital |
Factors Associated with Non-Adherence to AEDs
The 9 items adherence rate was added up to get sum index with a distribution ranging from 9 to 31 with mean 17.42 ±1.81. The median split was used (16.7) to dichotomize into two groups: 1 = adherent to the treatment, 0 = non-adherent to the treatment to the prescribed medication, which was 9–16 and 17–36, respectively. Our study showed that the magnitude of non-adherence to AEDs was 120 (40.27%). The results of multivariate analysis revealed that patients who had experienced the medication side effects were 2 times more likely to be non-adherent to the AEDS when compared to patients who did not experienced the side effects (AOR = 2.199; 95% CI: 1.21, 4.00, P = 0.010). The epileptic patients that were prescribed a poly-pharmacy were 5 times more likely to be non-adherent to the AEDS when compared to their counterparts (AOR = 5.166; 95% CI: 2.63, 10.14, P=<0.001). Similarly, patients with two or more diseases were 3.7 times more likely to be non-adherent to the AEDS when compared to patients who did not have a co-morbidity (AOR = 3.70; 95% CI: 2.058,6.65, P=<0.001,) (Table 4).
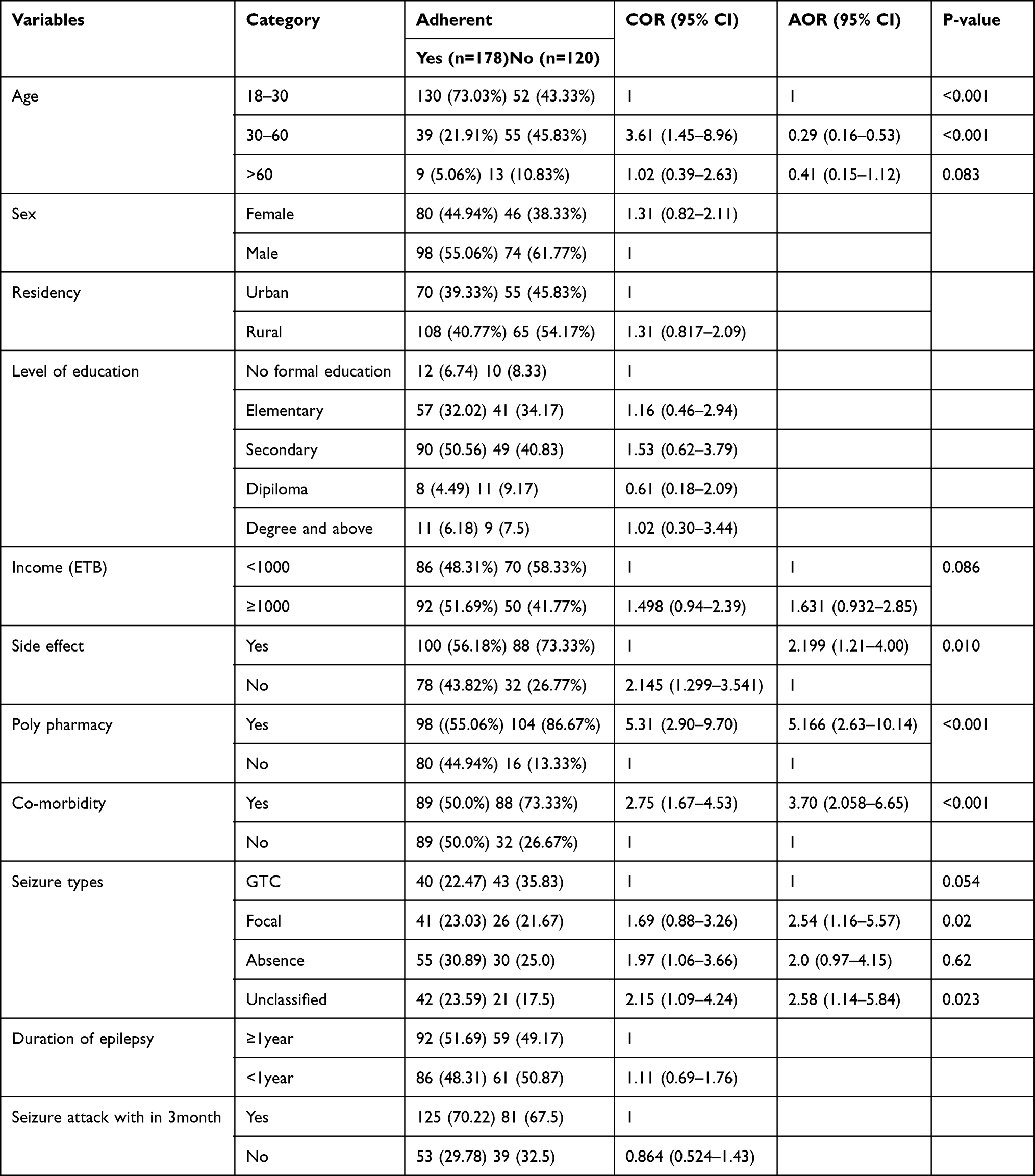 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with Non-adherence to AEDs among Epileptic Patients at Chronic Care Follow-Up of MKCSH |
Discussion
The magnitude of non-adherence to AEDs was 120 in our sample (40.27%). This matched the results of a systematic and meta-analysis undertaken by Belayneh Z et al, 2020 (39.77%)7 and a Saudi Arabian study (38.3%).17 On the contrary, it was greater than the Southern Ethiopian study (35%),18 the Dessie Referral Hospital (34.1%),5 and the Sudanese study (35%).19 The large disparities in adherence rates between trials are related to the diverse methodologies employed to assess adherence. Even when using the same assessment instruments, such as self-reported adherence, the lack of validated questionnaires causes adherence rates to vary between research.
Non-adherence to AEDs among epileptic patients may be influenced by a variety of factors, including the number of medicines taken,12 the types of medical conditions, polypharmacy, female sex, and previous hospitalization.8 As a result, identifying characteristics that contribute to non-adherence is critical for improving epileptic patient outcomes.20
When compared to patients who had not encountered the side effects, those who had experienced the side effects were 2 times more likely to be non-adherent to the AEDS (AOR = 2.199; 95% CI: 1.21, 4.00, P = 0.010). This was supported by the Sudan,19 Dessie Referral Hospital,5 and Belayneh Z et al, 2020 comprehensive and meta-analysis.7 This could be related to the patient’s lack of faith in the medication’s efficacy as well as their fear of side effects.
When compared to their peers, epileptic patients who were prescribed a polypharmacy were 5 times more likely to be non-adherent to AEDs (AOR = 5.166; 95% CI: 2.63, 10.14, P = 0.001). Sudan, University of Gondar Referral Hospital, Tikur Anbessa Specialized Hospital, and Jimma University Medical Center all reported comparable findings.1,19,21,22 Patients who have been prescribed a polypharmacy may forget to take it, or they may be unwilling or unable to take it as directed by their prescribers, resulting in non-adherence.
When compared to patients without a co-morbidity, individuals with two or more diseases were 3.7 times more likely to be non-adherent to AEDs (AOR = 3.70; 95% CI: 2.058,6.65, P = 0.001). This was in line with the Belayneh Z et al, 2020 study.7 This could be due to the disease’s severity and a concern of drug–disease interactions.
The study revealed that about three fourth (74.5%) of the patients had duration of epilepsy of <3 years. This is consistent with the study of Uganda that is 77%.0123 and inconsistent with the study of Kalpana Chawla Government Medical College (KCGMC), Karnal, in which about half of them had a duration of >10 years.6 However, the duration of epilepsy was not the predictors of patient’s non-adherence to AEDs. This is in line with the finding of Saudi Arabia.17
Phenobarbitone was the most commonly administered AED 34 (11.41%). The University of Gondar Teaching Hospital, Jimma University Specialized Hospital, and Tikur Anbessa Specialized Hospital also reported similar findings.2,24,25 On the contrary, Valproic acid was commonly prescribed in Saudi Arabia.17
This was attributable to drug availability and physicians’ predilection for prescribing phenobarbitone rather than phenytoin due to concerns about phenytoin’s unpredicted pharmacokinetic characteristics in our research area.
In our study, the most common type of seizure was absence seizure and GTC seizure that accounts 85(28.5%) and 83(27.9%), respectively. This was consistent with the study of Saudi Arabia17 and Mizan-Tepi University Teaching Hospital, Southwest Ethiopia.26 The reason for high prevalence of GTC was due to the patients with GTCS may be present with violent body movements and often prominent autonomic changes. As a result, the health care seeking in those populations is higher than other types of seizures and other types of seizures often underdiagnosed in our setting.
Limitations
As a limitation, the result of the study may not be generalizable to all hospitals because it was a single centred study and the causal effect relationship was not assessed due to the retrospective nature of the study.
Conclusion
In conclusion, findings of this study showed that the magnitude of non-adherences to AEDs was found to be high. Phenobarbitone was the most prescribed AEDs. The number of medications taken by patients, the presence of co-morbidity and the occurrence of medication side effects had a significant association with non-adherence to AEDs. Therefore, the pharmaceutical care in general and drug information services in particular should be established to enhance medication adherence in our study area. In addition to this, the prescriber should check for any possibility of side effects of AEDs, and they should avoid unwanted effects of medication before reaching the patients.
Abbreviations
AED, Antiepileptic drug; AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Crude Odds Ratio; GTC: Generalized Tonic Clonic Seizure; MKSCH, Mettu Karl Comprehensive Specialized Hospital.
Data Sharing Statement
The materials used while conducting this study are obtained from the corresponding author on reasonable request.
Acknowledgment
I thank Mettu University for providing the chance to conduct this study. Lastly, I acknowledge hospital administrators, data collectors, and study participants for extending their helping hands towards my study.
Author Contributions
The author made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Nasir BB, Berha AB, Gebrewold MA, Yifru YM, Engidawork E, Woldu MA. Drug therapy problems and treatment satisfaction among ambulatory patients with epilepsy in a specialized hospital in Ethiopia. PLoS One. 2020;15(1):e0227359. doi:10.1371/journal.pone.0227359
2. Birru EM, Shafi M, Geta M. Drug therapy of epileptic seizures among adult epileptic outpatients of University of Gondar Referral and Teaching Hospital, Gondar, North West Ethiopia. Neuropsychiatr Dis Treat. 2016;12:3213. doi:10.2147/NDT.S119030
3. Ejeliogu EU, Courage A. Prevalence and factors associated with non-adherence to antiepileptic drugs among children with epilepsy in Jos, Nigeria. Niger J Paediatr. 2020;47(3):240–245. doi:10.4314/njp.v47i3.8
4. Gurumurthy R, Chanda K, Sarma GR. An evaluation of factors affecting adherence to antiepileptic drugs in patients with epilepsy: a cross-sectional study. Singapore Med J. 2017;58(2):98. doi:10.11622/smedj.2016022
5. Kassahun G, Moges G, Demessie Y. Assessment of patients’ adherence to antiepileptic medications at Dessie referral hospital, chronic follow-up, south wollo, Amhara region, north east Ethiopia. Neurol Res Int. 2018;2018:1–6. doi:10.1155/2018/5109615
6. Govil N, Chahal S, Gupta N, Kaloti AS, Nadda A, Singh P. Factors associated with poor antiepileptic drugs adherence in below poverty line persons with epilepsy: a cross-sectional study. J Neurosci Rural Pract. 2021;12(01):095–101. doi:10.1055/s-0040-1721200
7. Belayneh Z, Mekuriaw B. A systematic review and meta-analysis of anti-epileptic medication non-adherence among people with epilepsy in Ethiopia. Arch Public Health. 2020;78(1):1–4. doi:10.1186/s13690-020-00405-2
8. Adem F, Abdela J, Edessa D, Hagos B, Nigussie A, Mohammed MA. Drug-related problems and associated factors in Ethiopia: a systematic review and meta-analysis. J Pharm Policy Pract. 2021;14(1):1–24. doi:10.1186/s40545-021-00312-z
9. Ahmed I, Tesema AA, Demeke T. Medication adherence and associated factors among patients with epilepsy at follow up clinics of Jimma Town Public Hospitals, Jimma, South West, Ethiopia, 2019. J of Pharmacol Clin Res. 2020;8(1):555735. JPCR.MS.ID.555735.
10. Ayalew MB, Megersa TN, Mengistu YT. Drug-related problems in medical wards of Tikur Anbessa specialized hospital, Ethiopia. J Res Pharm Pract. 2015;4(4):216. doi:10.4103/2279-042X.167048
11. Alsous M, Hamdan I, Saleh M, McElnay J, Horne R, Masri A. Predictors of nonadherence in children and adolescents with epilepsy: a multimethod assessment approach. Epilepsy Behav. 2018;85:205–211. PMID: 30032809. doi:10.1016/j.yebeh.2018.06.022
12. Ayele Y, Tesfaye ZT. Drug-related problems in Ethiopian public healthcare settings: systematic review and meta-analysis. SAGE Open Med. 2021;9:20503121211009728. doi:10.1177/20503121211009728
13. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the hill‐bone compliance to high blood pressure therapy scale. Prog Cardiovasc Nurs. 2000;15(3):90–96. doi:10.1111/j.1751-7117.2000.tb00211.x
14. Agha R, Abdall-Razak A, Crossley E, Dowlut N, Iosifidis C, Mathew G; The STROCSS Group. The STROCSS 2019 guideline: strengthening the reporting of cohort studies in surgery. Int J Surg. 2019;72:156–165. doi:10.1016/j.ijsu.2019.11.002
15. Lauritsen JM, Bruus M. EpiDataEntry Version 3.1. A comprehensive Tool for Validated Entry and Documentation Ofdata. Odense Denmark: The EpiData Association; 2008.
16. Bekele F, Tsegaye T, Negash E, Fekadu G. Magnitude and determinants of drug-related problems among patients admitted to medical wards of southwestern Ethiopian hospitals: a multicenter prospective observational study. PLoS One. 2021;16(3):e0248575. doi:10.1371/journal.pone.0248575
17. Gabr WM, Shams ME. Adherence to medication among outpatient adolescents with epilepsy. Saudi Pharm J. 2015;23(1):33–40. doi:10.1016/j.jsps.2014.05.003
18. Karthik L, Kumar G, Keswani T, Bhattacharyya A, Chandar SS, Bhaskara Rao KV. Protease inhibitors from marine actinobacteria as a potential source for antimalarial compound. PLoS One. 2014;9(3):e90972. doi:10.1371/journal.pone.0090972
19. Elsayed MA, El-Sayed NM, Badi S, Ahmed MH. Factors affecting adherence to antiepileptic medications among Sudanese individuals with epilepsy: a cross-sectional survey. Fam Med Prim Care Rev. 2019;8(7):2312. doi:10.4103/jfmpc.jfmpc_405_19
20. Bekele F, Fekadu G, Bekele K, Dugassa D, Sori J. Drug-related problems among patients with infectious disease admitted to medical wards of Wollega University Referral Hospital: prospective observational study. SAGE Open Med. 2021;9:2050312121989625. doi:10.1177/2050312121989625
21. Ayalew MB, Muche EA. Patient reported adverse events among epileptic patients taking antiepileptic drugs. SAGE Open Med. 2018;6:2050312118772471. doi:10.1177/2050312118772471
22. Garedow AW, Mulisa Bobasa E, Desalegn Wolide A, et al. Drug-related problems and associated factors among patients admitted with chronic kidney disease at Jimma University Medical Center, Jimma zone, Jimma, Southwest Ethiopia: a hospital-based prospective observational study. Int J Nephrol. 2019;2019:1–9. doi:10.1155/2019/1504371
23. Nazziwa R, Mwesige AK, Obua C, et al. Adherence to antiepileptic drugs among children attending a tertiary health unit in a low resource setting. Pan Afr Med J. 2014;17:44. doi:10.11604/pamj.2014.17.44.3399
24. Gurshaw M, Agalu A, Chanie T. Anti-epileptic drug utilization and treatment outcome among epileptic patients on follow-up in a resource poor setting. J Young Pharm. 2014;6(3):47. doi:10.5530/jyp.2014.3.8
25. Nasir BB, Yifru YM, Engidawork E, Gebrewold MA, Woldu MA, Berha AB. Antiepileptic drug treatment outcomes and seizure-related injuries among adult patients with epilepsy in a tertiary care hospital in Ethiopia. Patient Relat Outcome Meas. 2020;11:119. doi:10.2147/PROM.S243867
26. Zewudie A, Mamo Y, Feyissa D, Yimam M, Mekonen G, Abdela A. Epilepsy treatment outcome and its predictors among ambulatory patients with epilepsy at Mizan-Tepi University Teaching Hospital, southwest Ethiopia. Neurol Res Int. 2020;2020:1–8. doi:10.1155/2020/8109858
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.