")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Nomogram Based on Risk Factors for Type 2 Diabetes Mellitus Patients with Coronary Heart Disease
Authors Shi R, Wu B , Niu Z , Sun H, Hu F
Received 25 July 2020
Accepted for publication 21 November 2020
Published 18 December 2020 Volume 2020:13 Pages 5025—5036
DOI https://doi.org/10.2147/DMSO.S273880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Rong Shi, Birong Wu, Zheyun Niu, Hui Sun, Fan Hu
School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Fan Hu
School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Tel/Fax +862151322466
Email [email protected]
Introduction: This study aimed to study risk factors for coronary heart disease (CHD) in type 2 diabetes mellitus (T2DM) patients and establish a clinical prediction model.
Research Design and Methods: A total of 3402 T2DM patients were diagnosed by clinical doctors and recorded in the electronic medical record system (EMRS) of six Community Health Center Hospitals from 2015 to 2017, including the communities of Huamu, Jinyang, Yinhang, Siping, Sanlin and Daqiao. From September 2018 to September 2019, 3361 patients (41 patients were missing) were investigated using a questionnaire, physical examination, and biochemical index test. After excluding the uncompleted data, 3214 participants were included in the study and randomly divided into a training set (n = 2252) and a validation set (n = 962) at a ratio of 3:1. Through lead absolute shrinkage and selection operator (LASSO) regression analysis and logistic regression analysis of the training set, risk factors were determined and included in a nomogram. The C-index, receiver operating characteristic (ROC) curve, calibration plot and decision curve analysis (DCA) were used to validate the distinction, calibration and clinical practicality of the model.
Results: Age, T2DM duration, hypertension (HTN), hyperuricaemia (HUA), body mass index (BMI), glycosylated haemoglobin A1c (HbA1c), high-density lipoprotein (HDL-C) and low-density lipoprotein (LDL-C) were significant factors in this study. The C-index was 0.750 (0.724– 0.776) based on the training set and 0.767 (0.726– 0.808) based on the validation set. Through ROC analysis, the set area was 0.750 for the training set and 0.755 for the validation set. The calibration test indicated that the S:P of the prediction model was 0.982 in the training set and 0.499 in the validation set. The decision curve analysis showed that the threshold probability of the model was 16– 69% in the training set and 16– 73% in the validation set.
Conclusion: Based on community surveys and data analysis, a prediction model of CHD in T2DM patients was established.
Keywords: prediction model, coronary heart disease, type 2 diabetes mellitus
Introduction
As the most common form of diabetes mellitus (DM), type 2 diabetes mellitus (T2DM) has become the leading cause of morbidity and mortality worldwide. In 2019, approximately 4.2 million people (20–79 years old) worldwide died of diabetes or its complications, equivalent to 1 person dying of diabetes every eight seconds, accounting for approximately 11.3% of all deaths worldwide.1 In 2019, the number of patients with diabetes in the world reached 463 million.1 By 2040, the world’s prevalence will increase to 629 million, accounting for approximately 90% of all cases.2 In recent years, the global diabetes epidemic has rapidly spread to every country in Asia.3 The number of people with diabetes in Asia is expected to exceed 355 million. Among them, India and China will have the largest number of people with diabetes in the world with 110 million and 69.2 million cases, respectively.2 In recent years, the population of diabetes in China has increased significantly from 114.4 million in 2017 to 166.4 million in 2019.1
Among people with diabetes, 76.4% reported at least one complication.4 Compared with adults without diabetes, adults with DM have a 2- to 4-fold increased risk of cardiovascular complications, and this risk increases as blood glucose control deteriorates. Diabetes is associated with a 75% increase in adult mortality with cardiovascular complications accounting for a large part of all-cause mortality.5 The Epi-Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medication (EpiDREAM) study includes 25,063 people at high risk for diabetes with a death rate accounting for cardiovascular complications of 1.27 per 100 person-years for diabetic patients and 0.51 per 100 person-years for normal blood glucose.6 Cardiovascular complications related to diabetes include peripheral vascular disease cerebrovascular disease, cardiovascular autonomic neuropathy, coronary heart disease (CHD) and heart failure.5 According to the World Health Organization (WHO), CHD is the leading cause of death for both men and women with more than 7 million deaths per year.7 Related studies have also shown that CHD is one of the most common causes of the death of T2DM, and CHD accounts for approximately 65% of the deaths of diabetic patients.8 T2DM is one of the important risk factors for CHD, and the risk of CHD in diabetic patients is twice that in nondiabetic patients.9 The main reason is that chronic hyperglycaemia plays an important role in the occurrence and development of cardiovascular diseases, which will aggravate atherosclerosis.10 In addition, other risk factors, such as hypertension, smoking, obesity and sedentary lifestyle, can also lead to rapid deterioration of heart function.11
In this study, we used relevant studies on CHD in T2DM as evidence to filter correspondence variables, including age, sex, T2DM duration, hypertension (HTN), hyperuricaemia (HUA), diabetic retinopathy (DR), diabetic nephropathy (DN), smoking, alcohol, body mass index (BMI), diastolic blood pressure (DBP), systolic blood pressure (SBP), fasting blood glucose (FBG), postprandial blood glucose (PBG), glycosylated haemoglobin A1c (HbA1c), triglyceride (TG), total cholesterol (TC), high-density lipoprotein (HDL-C), low-density lipoprotein (LDL-C), serum creatinine (SCR), uric acid (UA), blood urea nitrogen (BUN), urine creatinine (UCR), microalbuminuria (UMA), glomerular filtration rate (eGFR) and the ratio of urinary microalbumin to uric creatinine (ACR). At present, most studies have mainly concentrated on the influencing factors of T2DM or CHD, whereas a prediction model suitable for patients with T2DM complicated with CHD is lacking. The aim of this study was to generate a valid model to predict the risk of CHD in Chinese T2DM patients. A nomogram plot was established to help predict the CHD risk in T2DM patients by analysing characteristic factors related to CHD risk in patients with T2DM.
Participants and Methods
Participants
Community Health Center Hospitals in Shanghai have established an electronic medical record system (EMRS) covering all community residents. In cooperation with the Community Center Hospitals Affiliated to Shanghai University of Traditional Chinese Medicine, including Huamu community, Jinyang community, Yinhang community, Siping community, Sanlin community and Daqiao community, our team reviewed the EMRS of 3402 patients with type 2 diabetes who had been diagnosed by clinical doctors from 2015 to 2017. The health status of the patients met the diagnostic criteria of WHO type 2 diabetes in 1999. From September 2018 to September 2019, these patients were followed up to collect data. Written informed consent from all participants was obtained before incorporating the data into the study. First, 3361 patients were investigated (41 patients were missing during follow-up), 147 were excluded due to incomplete data, and 3214 patients were finally included in the analysis. The effective questionnaire recovery rate was approximately 95.63% (Figure 1).
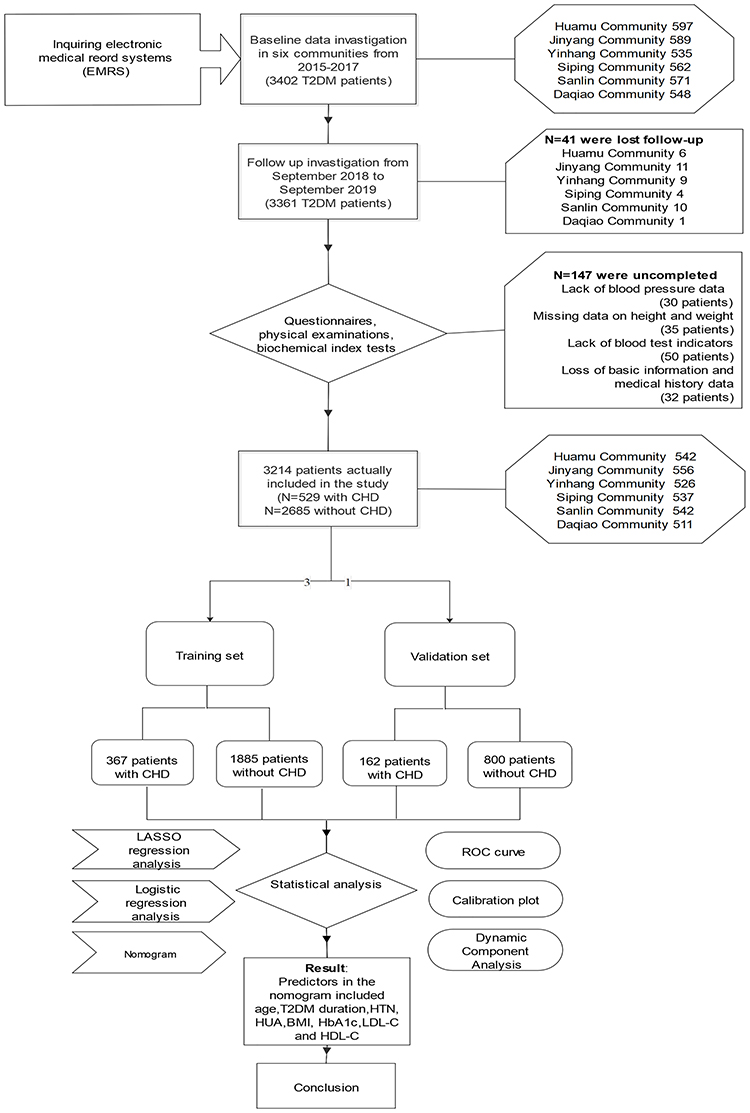 |
Figure 1 The flow chart presents the entire process of patient follow-up, data collection and statistical analysis in this study. |
Data Collection
Through the Community Health Center Hospitals Affiliated to Shanghai University of Traditional Chinese Medicine, we determined the population of T2DM patients in each community, sent an invitation for examination to the patient group, and informed them of the following precautions: (1) All participants were required to maintain a normal lifestyle of at least 5 days before examination. (2) All participants were required to fast for at least 10 hours the day before the examination. The methods of investigation included questionnaire investigation, physical examination and biochemical examination. Fasting blood samples were collected at 7 o’clock in the morning. The participants then ate breakfast and waited at the Community Center Hospitals for 2 hours to collect blood samples again and urine samples. During the waiting period, the professional staff assisted the patients in completing the questionnaire survey and physical examination. All blood samples were centrifuged in situ within 30 minutes after collection. Urine biochemical indexes were analysed using the urine test 500B (RIT, China). All samples were sent to Ruijin Hospital Affiliated with Shanghai Jiaotong University for testing on the same day to obtain the data.
Using the patient’s personal identity information to match the information in the EMRS of the community centre hospitals, the past medical history, including CHD, HTN, HUA, DR and DN, was assessed. The questionnaire included basic sociodemographic information (age, sex), T2DM duration and daily life habits (smoking, alcohol). Physical examination included height, weight, SBP and DBP. According to Chinese guidelines for type 2 diabetes published in 2017, BMI was calculated as the weight (kg) divided by the height (m) squared. Patients’ SBP and DBP were measured twice within 5 minutes, and the average value of the two results was recorded as the final SBP value and DBP value. The laboratory indexes included FBG, PBG, HbA1c, LDL-C, HDL-C, TG, TC, SCR, BUN, UA, UCR, and UMA. eGFR was calculated according to SCR, age and sex in light of the Modification of Diet in Renal Disease Trial (MDRD) formula. In addition, ACR was calculated as UMA divided by UCR.
Statistical Analysis
The statistical analysis of the data in this study was conducted using R software (version 3.6.2; https://www.r-project.org). First, the patients were divided into a training set and a validation set for external validation conforming to the ratio of 3:1 with R software.12 Then, the data of the training set were analysed using least absolute shrinkage and selection operator (LASSO) regression. LASSO regression analysis is a method to simplify high-dimensional data and can be used to analyse the optimal predicted risk factors for the disease.13 After features with nonzero coefficients in the LASSO regression model were selected, multivariable logistic regression analysis was performed to screen out all significant risk factors. Multivariable logistic regression analysis is typically used to develop a prediction model.14 The features were assessed by odds ratios (ORs) with 95% confidence intervals (CIs), and the corresponding P-values were then obtained. The statistical significance levels were all two-sided. Then, the features with P≤0.05 were selected to build the nomogram prediction model. To test the accuracy of the risk prediction model, the C-index, receiver operating characteristic (ROC) curve, calibration plot and dynamic component analysis (DCA) were calculated using the data of the training set and the validation set, respectively.
Results
Finally, 3214 valid data points were included in this study: 1605 males and 1609 females. The average age of the patients was 65.00 years (60.00, 69.00), and 529 (16.46%) of patients had CHD. For external verification, the total cases were divided into a training set (2252 patients) and a validation set (962 patients) at a ratio of approximately 3:1. There were 1125 males and 1127 females in the training set with an average age of 65.00 (60.00, 69.00) years old. There were 367 (16.30%) patients with CHD. The validation set included 480 males and 482 females with an average age of 65.00 (60.00, 68.00) years old, and 162 (16.84%) patients had CHD. Specific demographic and clinical characteristics are presented in Table 1.
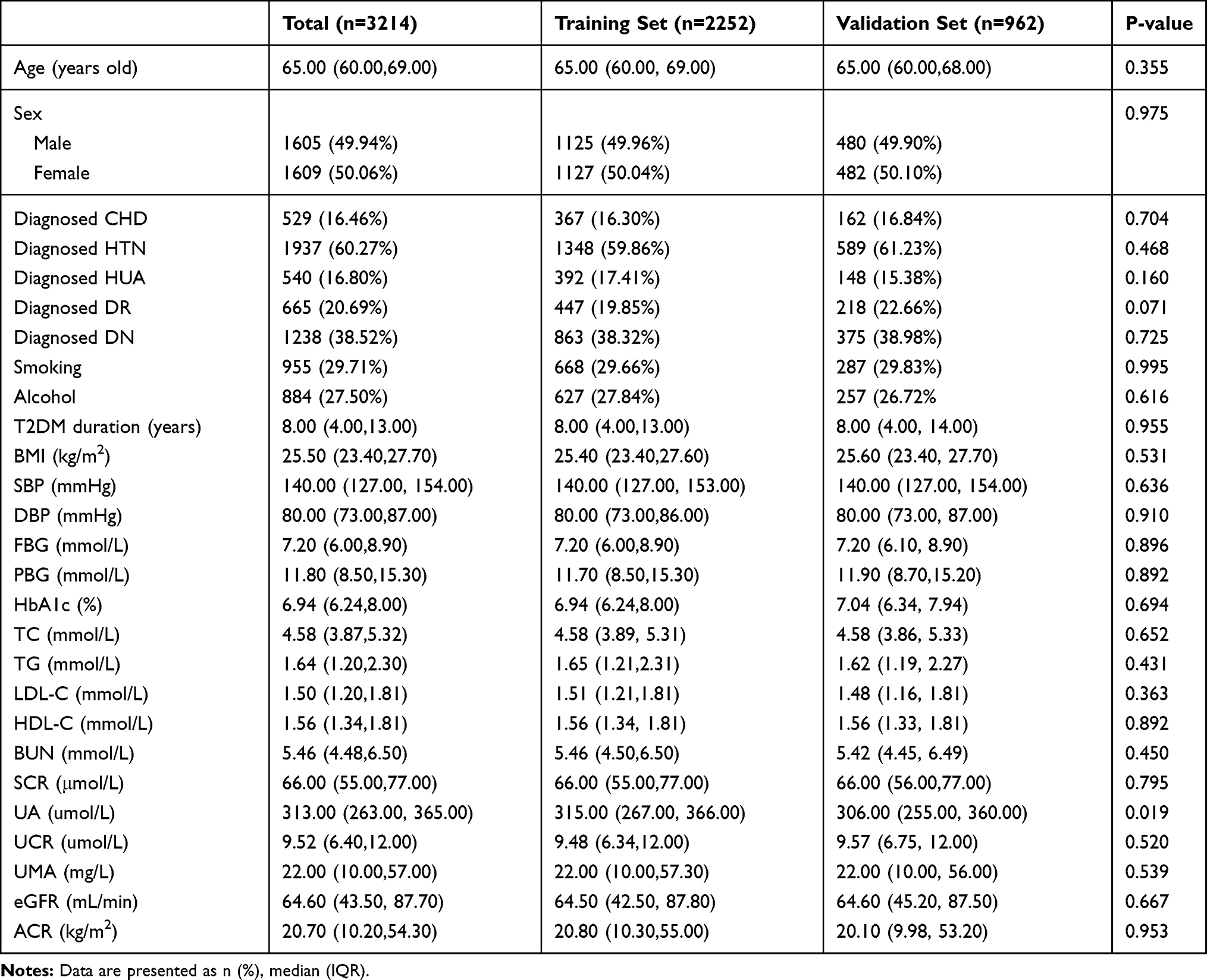 |
Table 1 Characteristics of the Participants in Different Groups |
LASSO regression analysis was performed for the training set data. By selecting nonzero features in the result of LASSO regression analysis, the number of potential predictors decreased from 26 to 8 (Figure 2A and B), including age, T2DM duration, HTN, HUA, BMI, HbA1c, LDL-C and HDL-C (Table 2). Then, using logistic regression analysis, the risk characteristic factors with P-values less than 0.05 were screened out from the above 8 factors, and all the factors were significant (Table 3). The above 8 independent risk characteristic factors were used to establish a prediction model to predict the risk of CHD in T2DM patients and displayed as a nomogram (Figure 3A).
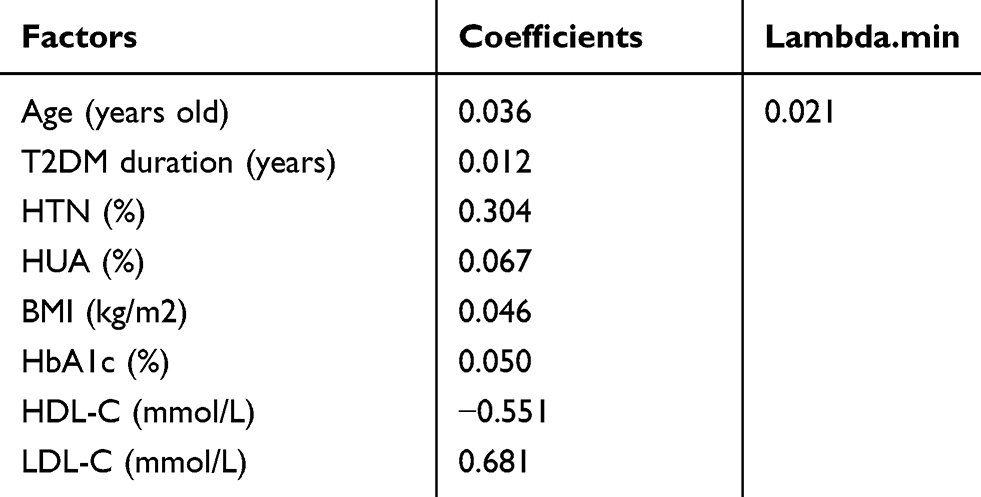 |
Table 2 Coefficients and Lambda.min Value of the LASSO Regression Based on the Training Set |
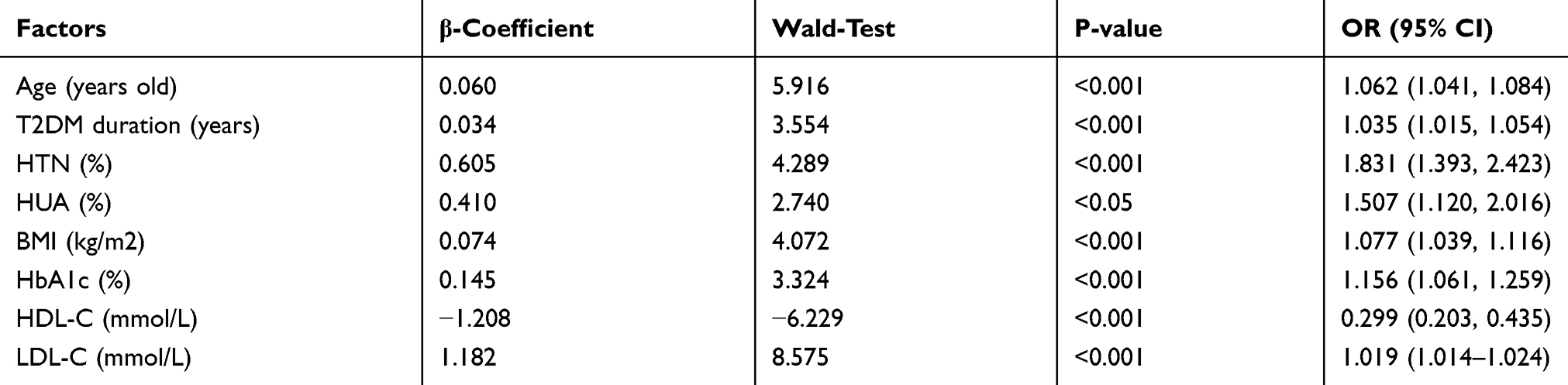 |
Table 3 Model Established by Logistic Regression Analysis Based on the Training Set |
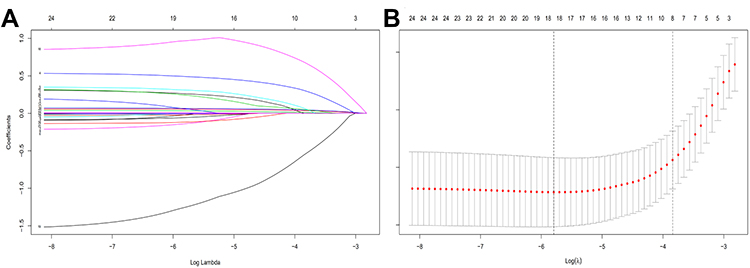 |
Figure 2 Demographic and clinical feature selection using the LASSO binary logistic regression model in T2DM patients with CHD based on the training set. Abbreviations: LASSO, least absolute shrinkage and selection operator; SE, standard error. Notes: (A) Optimal parameter (lambda) selection in the LASSO model used fivefold cross-validation based on minimum criteria. The partial likelihood deviance (binomial deviance) curve was plotted versus log(lambda). Dotted vertical lines were drawn at the optimal values by using the minimum criteria and the 1 SE of the minimum criteria (the 1-SE criteria). LASSO coefficient profiles of the 8 features. (B) A coefficient profile plot was produced against the log(lambda) sequence. A vertical line was drawn at the value selected using fivefold cross-validation, where optimal lambda resulted in 8 features with nonzero coefficients. |
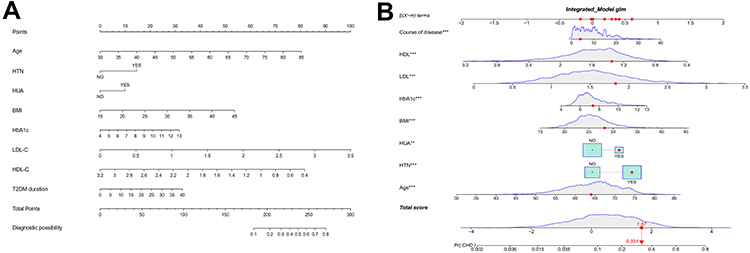 |
Figure 3 Developed nomogram for CHD. Notes: (A) The nomogram for CHD in T2DM patients was developed in the cohort by integrating age, T2DM duration, HTN, HUA, BMI, HbA1c, HDL-C and LDL-C. (B) An example of nomogram for CHD in T2DM patients. Logistic regression results showed that there were corresponding P values for each index, and the indicators with statistical significance level P ≤ 0.05 were included in the nomogram. “***” means P<0.001, “**” means P<0.05. |
To verify the reliability of the prediction model, the data of the training set and validation set were used to test the model. The C-index based on the training set was 0.750 (0.724–0.776), and the C-index based on the validation set was 0.767 (0.726–0.808) (Table 4). The set area under the ROC curve is 0.750 for the training set (Figure 4A) and 0.755 for the validation set (Figure 4B), demonstrating that the prediction model has good performance. The calibration test indicated that the S:P ratio of the prediction model was 0.982 in the training set (Figure 5A) and 0.499 in the validation set (Figure 5B). The DCA decision curve shows that the threshold probability of the model is 16–69% in the training set (Figure 6A) and 16–73% in the validation set (Figure 6B). In conclusion, it can be proven that the risk prediction model exhibits good prediction ability.
 |
Table 4 C-Index in the Array Based on Training Set and Validation Set |
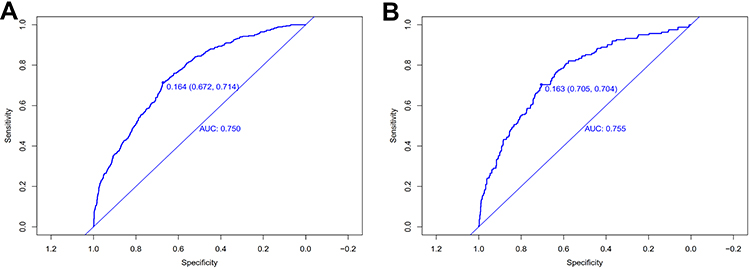 |
Figure 4 The pooled AUC of the ROC curve. Notes: (A) Training set and (B) Validation set: The pooled AUC of the ROC curve. The y-axis indicates the true positive rate of the risk prediction. The x-axis indicates the false positive rate of the risk prediction. The blue line represents the performance of the nomogram. |
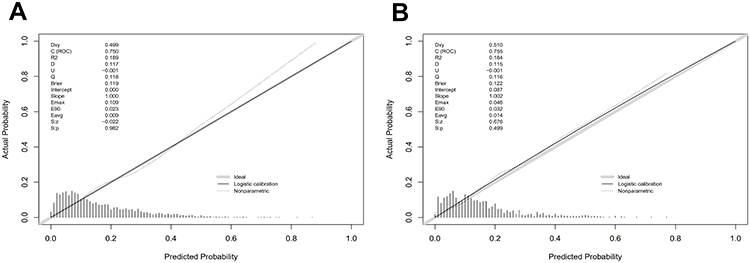 |
Figure 5 The calibration curves of the CHD incidence risk prediction in the array. Notes: (A) Training set and (B) Validation set: Calibration curves of the CHD incidence risk prediction in the array. The x-axis represents the predicted incidence risk. The y-axis represents the actual diagnosed CHD. The diagonal dotted line represents a perfect prediction by an ideal model. The solid line represents the performance of the nomogram; a closer fit to the diagonal dotted line represents a better prediction. |
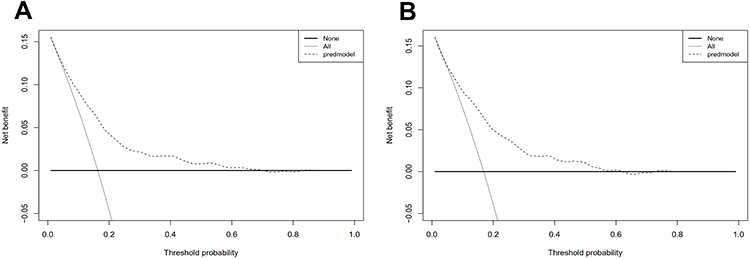 |
Figure 6 Decision curve analysis for the incidence risk nomogram of CHD. Notes: (A) Training set and (B) Validation set: The y-axis indicates the net benefit. The dotted line represents the incidence risk nomogram of CHD. The thin solid line represents the assumption that all patients are diagnosed with CHD. The thin thick solid line represents the assumption that no patients are diagnosed with CHD. |
Discussion
A nomogram is a type of two-dimensional graph that uses approximate graph calculations of mathematical functions.15 It has a user-friendly interface, better accuracy and easy-to-understand results and has been widely used in the field of medicine. In this study, we developed a new tool for predicting CHD risk in patients with T2DM. The app was developed using R language with the shiny package. The URL is https://doctorhu.shinyapps.io/DynNomapp_CHD/. The app is mainly used to help clinical prediction and promote individualized evaluation. The nomogram involves eight variables, and the external verification reveals fairly good recognition and verification ability.
In this study, the prevalence of CHD was 16.46% in all patients, 16.30% in the training set and 16.84% in the validation set, which is similar to the results in other relevant studies.
If the T2DM subject was 64 years old, had HUA and HTN, diabetes duration of 4 years, HbA1c of 7.34%, HDL of 1.35 mmol/l, LDL of 1.83 mmol/l, and BMI of 28.25 kg/m2, the probability of CHD was estimated to be 32.4% (Figure 3B).
A systematic literature review across the world from 2007–2017 analysed 4,549,481 patients with T2DM based on 57 articles. Globally, CHD accounts for 32.2% of all T2DM patients. The prevalence of T2DM with CHD was estimated at 21.2%.16
In China, Hu Xiao et al analysed the prevalence and risk characteristic factors of chronic complications in hospitalized patients with T2DM in Central China. After investigating 3469 T2DM subjects, 25.8% of participants were found to develop CHD.17
Through LASSO and logistic regression analyses, we concluded that the risk characteristic variables affecting CHD in patients with T2DM based on the training group in this study consisted of age, T2DM duration, HTN, HUA, BMI, HbA1c, LDL-C and HDL-C. Through the ROC curve analysis, C-index and calibration plots, the nomogram exhibited moderately good predictive power. Thus, the influence of each of the eight factors cannot be ignored, and they are all closely related to CHD risk in patients with T2DM.
Our study shows that age is one of the most influential factors in T2DM patients with CHD. The findings of this study have been reported in many previous studies. Similar to our results, Igley et al found that the prevalence of CHD increased with age.18 With increasing age, the prevalence of CHD in patients increased. The relative probability of atherosclerotic plaques increases in elderly patients.19 In addition, age increases the incidence of peripheral arterial disease, which subsequently increases the risk of CHD.20 Carotid atherosclerosis is common in T2DM patients and increases with age. Carotid atherosclerosis is positively correlated with the 10-year risk of coronary heart disease and stroke and is an independent risk factor for the 10-year risk of coronary heart disease.21 Ramachandran and his colleagues demonstrated a significant association between age and chronic heart disease.22 Aurora Baluja et al developed PG-HACKER (sex, age, peripheral arterial disease, left ventricle function, previous congestive heart failure, Killip class and optimal medical therapy), a risk scoring system for cardiovascular and cerebrovascular diseases in patients with DM. In this system, age is a major indicator, and the risk score is relatively high.23 According to the American Heart Association scoring system, atherosclerosis is more common in elderly T2DM patients compared with younger patients,24 and atherosclerosis is a significant cause of CHD.
This study reveals a great correlation between T2DM duration and the risk of CHD. In a study in China, multivariate logistic stepwise regression analysis was used to determine the risk factors for T2DM-related chronic complications. Diabetes duration > 5 years is a common risk factor for CHD.25
Many studies have indicated that high blood pressure is the main factor leading to increased cardiovascular event risk in patients with DM. Our study found HTN as an important factor in CHD in T2DM patients. A multivariate logistic regression analysis showed that systolic blood pressure > 125 mmHg was a common risk factor for CHD.25 A survey of postmenopausal women showed that hypertension, T2DM and renal involvement were associated with an increased frequency of multivessel disease.26 To prevent and reduce the occurrence of chronic complications of type 2 diabetes, efforts should be made to control blood glucose, hypertension and dyslipidaemia.25 Long-term hypertension can affect the elasticity of blood vessels, thus accelerating the process of atherosclerosis to induce CHD. According to related reports, reactive oxygen can affect the function of blood vessels to a certain extent, and this effect is related to hypertension. In the process of hypertension, reactive oxygen species participate in the oxidative stress of blood vessels, which may explain one of the mechanisms by which hypertension contributes to CHD. Therefore, it is very important to control blood pressure in a proper range to prevent CHD.
HUA refers to a condition in which the concentration of UA in human serum is greater than the upper limit of normal reference under the condition of a normal purine diet: greater than 420 mmol/L in men and 360 mmol/L in women. A systematic retrospective analysis indicated that UA increased the risk of CHD events in the general population, mainly in adult women, whereas the mortality rate of CHD in women was also affected by a high level of UA.27 In a meta-analysis SEO YOUNG KIM et al noted that for every 1 mg/dl increase in UA, the comprehensive multivariate RR of CHD mortality was 1.12.28 A cross-sectional study of 1213 patients demonstrated that HUA was associated with microangiopathy and macroangiopathy and was a predictor of CHD in T2DM patients.29 In a study of an elderly population in China, HUA was positively correlated with the 10-year risk of CHD and possibly an independent risk factor for CHD in the elderly population.30
Our study identified BMI as an essential element of CHD in T2DM patients. The higher BMI, the greater risk of CHD. Obese patients can experience excessive lipid deposition in the blood vessel wall, causing atherosclerosis, plaque formation, stenosis and even occlusion of the blood vessel, which can manifest in the cardiovascular system, coronary artery stenosis and blockage, resulting in coronary heart disease. Hala O. El Mesallamy et al showed that adipose tissue of obese patients with type 2 diabetes can release proinflammatory mediators and participate in vascular injury and insulin resistance, thus participating in the pathogenesis of coronary heart disease to a certain extent.31 R. Haider et al performed a 6-month randomized clinical trial of short message intervention in patients with CHD. A significant difference in BMI between the intervention group and the nonintervention group,32 which also revealed a correlation between BMI and CHD. Effective control of BMI would reduce the risk of CHD. BMI was also mentioned as an important influencing factor of CHD in patients with T2DM in a survey of 181,045 diabetic patients in Sweden.33 The Gensini score was also positively correlated with BMI, indicating that an increase in BMI would aggravate the degree of coronary atherosclerosis.34 Therefore, it is necessary to control weight in patients with or without T2DM.
The results of this study revealed a positive correlation between HbA1c level and CHD prevalence in T2DM patients. The level of glycosylated haemoglobin in patients with type 2 diabetes mellitus complicated with coronary heart disease is higher.35 Glycosylated haemoglobin (GHB) is a product of the combination of haemoglobin in red blood cells and sugar in serum. GHB is formed by slow, continuous and irreversible glycosylation, and its content depends on the concentration of blood glucose and the contact time between blood glucose and haemoglobin. HbA1c accounts for approximately 70% of GHB. In addition, its structure is stable, so it is most commonly used as a signal of long-term blood glucose control in patients with DM.36 A multivariate Cox proportional model confirmed that a high HbA1c value was a significant predictor of coronary heart disease.37 In addition, a large number of studies have analysed the correlation between HbA1c level and CHD severity. For example, Garg et al used grammar scores to assess the severity of CHD and concluded that HbA1c levels increased significantly in patients with increased CHD severity.38
In this study, LDL-C was a risk factor for CHD in T2DM patients and was positively correlated with the probability of CHD. When the level of LDL-C in the blood increases, LDL-C is deposited in the artery wall and gradually forms atherosclerotic plaques to block the corresponding blood vessels. This condition causes coronary heart disease, stroke, peripheral artery disease and other serious diseases. The results from a multiple-hospital study showed that 25.8% of 3469 patients with type 2 diabetes had CHD. Logistic regression showed that LDL-C > 3.12 mmol/l was a risk factor for CHD.25 A study of 5354 patients with T2DM in Taiwan identified LDL-C variability as a predictable factor of adverse cardiovascular events in T2DM. Patients with T2DM and high variability in LDL-C tend to exhibit an increased risk of cardiovascular events.39 After a 10-year follow-up of 6417 subjects, David M. Tehrani et al reported that LDL-C (P <0.05) was positively correlated with CHD in the DM group.40 During a 2-year follow-up, LDL-C levels in men were significantly different between participants with and without carotid IMT progression.41 A retrospective study of the prevalence of chronic complications of inpatients with T2DM in Hubei Province in central China demonstrated that HbA1c >7.0%, LDL-C levels >3.12 mmol/L and age >45 at the time of admission were risk factors for CHD.17
Our study found that HDL-C was negatively associated with the incidence of CHD in patients with T2DM. The lower the level of HDL-C, the greater the risk of CHD in the population. Numerous medical studies have shown that LDL cholesterol is closely related to CHD, which is consistent with the general direction of our research results. However, the object of this study is based on patients with T2DM. In a comparative study conducted by Jia Teng Sun et al, HDL-C levels were lower in the diabetic group compared with the healthy group.42 In fact, in T2DM patients, HDL-C levels are decreased, and its biochemical effect is also altered. At normal levels, HDL-C exhibits anti-inflammatory properties. However, its anti-atherosclerotic properties are very variable, and weakened anti-inflammatory properties have been reported. In addition, HDL-C can even promote inflammation in chronic inflammatory diseases.43 TNF-α is a critical factor in the occurrence and development of atherosclerosis. Low HDL-C levels in diabetic patients can activate monocytes and increase TNF-α secretion.44 In other words, in the presence of T2DM, HDL-C will transform into atherogenic granules.45 Renal diseases have complex effects on the function and structure of HDL. For example, serum amyloid A (SAA) can activate the NF-KB pathway and reverse the anti-inflammatory effect of HDL-C.45 Therefore, the development of renal dysfunction in DM patients may aggravate the metabolism of SAA-rich HDL and transform HDL-C into proinflammatory granules. In addition, a long duration of diabetes and poor blood glucose control interfere with HDL-C vascular function, which leads to the enhancement of systemic inflammation in diabetic patients.46 During a 2-year follow-up, a significant difference in HDL-C levels was noted between women with and without carotid IMT progression.41 Sex analysis revealed that higher TGs and lower HDL-C increased the risk of T2DM and T2DM + CHD.47 The results of the matched case-control study from Japan demonstrated that HDL-C was significantly related to CHD and that non-HDL-C was the most effective predictor of the development of CHD in T2DM patients.48
At present, the data of domestic research on the risk of CHD in patients with T2DM is mainly derived from inpatients. Few epidemiological investigations have been conducted on community patients. At the beginning of the study, a nomogram based on the different risk factors was established through external validation. The nomogram can be used to assess the risk of CHD in patients with T2DM. According to validation methods, the predictive nomogram employs moderately good prediction factors. After the application of the nomogram in the evaluation of patients with T2DM, it is necessary for doctors to provide health education from the perspective of medical and skill guidance to help patients develop a healthier lifestyle.
Objectively, there are some limitations in our study. First, we did not have a sufficient number of cases in the study. The object of this study was only T2DM patients in three communities in Shanghai, and some patients were too seriously ill to participate in our study. For the prediction of risk factors for T2DM patients complicated with CHD in other areas of China, more data support is needed to improve the prediction model. Second, the indicators included in our study are relatively small. We can also include more lifestyle and socioeconomic factors, such as exercise, level of education, income and medication condition, in this study. In addition, the indicators included in the study were not dynamically monitored, which may influence the accuracy of this prediction model to a certain extent.
Conclusions
By investigating the physical and biochemical indexes of patients with T2DM in six communities in Shanghai and analysing the relevant data, we established a prediction model of CHD risk of patients with T2DM, including age, T2DM duration, HTN, HUA, BMI, HbA1c, LDL-C and HDL-C. Using C-index, ROC, calibration curves and DCA, it was further verified that the characteristic variables of the nomogram could predict the risk of CHD in patients with T2DM with moderate accuracy.
Abbreviations
DM, diabetes mellitus; T2DM, type 2 diabetes mellitus; EpiDREAM, The Epi-Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medication study; CHD, coronary heart disease; WHO, World Health Organization; HTN, hypertension; HUA, hyperuricaemia; DR, diabetic retinopathy; DN, diabetic nephropathy; BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; FBG, fasting blood glucose; PBG, postprandial blood glucose; HbA1c, glycosylated haemoglobin A1c; TG, triglyceride; TC, total cholesterol; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein; SCR, serum creatinine; UA, uric acid; BUN, blood urea nitrogen; UCR, urine creatinine; UMA, microalbuminuria; GFR, glomerular filtration rate; ACR, The ratio of urinary microalbumin to uric creatinine; EMRS, electronic medical record systems; MDRD, Modification of Diet in Renal Disease Trial; LASSO, least absolute shrinkage and selection operator; ROC, receiver operating characteristic; DCA, decision curve analysis; SAA, serum amyloid A.
Data Sharing Statement
Because the data used in this study involve the privacy of patients and are related to the management of patient information in community hospitals, the data cannot be used publicly. If you are interested or have similar research directions, you can contact the corresponding author.
Ethics Approval and Informed Consent
The protocol for this research project was approved by a suitably constituted Ethics Committee of the institution, and it conforms to the provisions of the Declaration of Helsinki (Ethics Committee of Shanghai Oriental Hospital affiliated with Tongji University, Batch number: [2017] Research Review No. 20). All the subjects were carefully informed about the protocol and provided written informed consent before inclusion in the study. This study protected the subject’s anonymity, and there is no identifiable information in this manuscript. Researchers kept all the questionnaires and provided informed consent with signatures of all participants in the study. The cooperation of the medical and testing centre of the project with the social centre was consistent with the standards and medical ethics.
Acknowledgments
The communities of Huamu, Jinyang, Yinhang, Siping, Sanlin, and Daqiao and the street staff participated in questionnaire surveys; medical staff at community centre hospitals participated in blood and urine collection; and medical testing centre staff participated in blood and urine biochemical indicator testing and recorded corresponding data. We appreciate all the enrolled participants, the cooperative community health centre, and all the staff for their contributions to this study.
Author Contributions
All the authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; participated in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
The numbers next to the authors’ names are ordered according to the authors’ contributions to the manuscript: Rong Shi1, Birong Wu2, Zheyun Niu3, Hui Sun4, and Fan Hu1.
Funding
This research was financially supported by the fourth round of Shanghai Public Health Three-Year Action Plan Key Discipline Construction–Health Education and Health Promotion (Grant No. 15GWZK1002).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. IDF. Available from: https://diabetesatlas.org/en/. Accessed December 10, 2020.
2. International Diabetes Federation IDF Diabetes Atlas. Epidemiology and morbidity. Available from: https://diabetesatlas.org/en/.Accessed December 10, 2020.
3. Ramachandran A, Ma RCW, Snehalatha C. Diabetes in asia. Lancet. 2010;375(9712):408–418. doi:10.1016/S0140-6736(09)60937-5
4. Hu H, Sawhney M, Shi L. A systematic review of the direct economic burden of type 2 diabetes in China. Diabetes Ther. 2015;6(1):7–16. doi:10.1007/s13300-015-0096-0
5. Dal Canto E, Ceriello A, Ryden L, et al. Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol. 2019;26(2_SUPPL):25–32. doi:10.1177/2047487319878371
6. Anand SS, Dagenais GR, Mohan V, et al. Glucose levels are associated with cardiovascular disease and death in an international cohort of normal glycaemic and dysglycaemic men and women: the EpiDREAM cohort study. Eur J Prev Cardiol. 2012;19(4):755–764. doi:10.1177/1741826711409327
7. Ali A, Abu Zar M, Kamal A, et al. American heart association high blood pressure protocol 2017: a literature review. Cureus. 2018;10(8):e3230–e3230.
8. Gaman M-A, Cozma M-A, Dobrica E-C, Bacalbasa N, Bratu OG, Diaconu CC. Dyslipidemia: a trigger for coronary heart disease in Romanian patients with diabetes. Metabolites. 2020;10(5):195. doi:10.3390/metabo10050195
9. Kautzky-Willer A, Kamyar MR, Gerhat D, et al. Sex-specific differences in metabolic control, cardiovascular risk, and interventions in patients with type 2 diabetes mellitus. Gend Med. 2010;7(6):571–583. doi:10.1016/j.genm.2010.12.001
10. Cikim G, Canatan H, Gursu MF, Gulcu F, Baydas G, Kilicoglu AE. Levels of zinc and lipid peroxidation in acute coronary syndrome. Biol Trace Elem Res. 2003;96(1–3):61–69. doi:10.1385/BTER:96:1-3:61
11. Wu J, Xun P, Tang Q, Cai W, He K. Circulating magnesium levels and incidence of coronary heart diseases, hypertension, and type 2 diabetes mellitus: a meta-analysis of prospective cohort studies. Nutr J. 2017;16.
12. Li W, Xie B, Qiu SH, et al. Non-lab and semi-lab algorithms for screening undiagnosed diabetes: a cross-sectional study. EBioMedicine. 2018;35:307–316. doi:10.1016/j.ebiom.2018.08.009
13. Wang HJ, Zhang L, Liu Z, et al. Predicting medication nonadherence risk in a Chinese inflammatory rheumatic disease population: development and assessment of a new predictive nomogram. Patient Prefer Adherence. 2018;12:1757–1765. doi:10.2147/PPA.S159293
14. Huang. Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer (vol 34, pg 2157, 2016). J Clin Oncol. 2016;34(20):2435.
15. Chen L, Wei B, Xu L, Wu Y. The association of inflammatory markers and periodontal indexes with the risk of coronary heart disease in Chinese patients with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2018:S0168822717313372.
16. Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):19. doi:10.1186/s12933-018-0728-6
17. Xiao H, Du AM, Yun P, Zhang HF, Tian Y, Xiao FX. Prevalence and risk factors of chronic complications of type 2 diabetic inpatients in Hubei Province of central China: results from a multiple-hospital study. Int J Diabetes Dev Ctries. 2016;36(2):242–247. doi:10.1007/s13410-015-0452-7
18. Iglay K, Hannachi H, Howie PJ, et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016:1–44.
19. Dodos I, Georgopoulos S, Dodos K, et al. Correlation of glycosylated hemoglobin levels with histological and ultrasound characteristics of the carotid plaque in diabetic and nondiabetic patients. Ann Vasc Surg. 2019;61:218–226. doi:10.1016/j.avsg.2019.04.013
20. Pang X-H, Han J, Ye W-L, et al. Lower extremity peripheral arterial disease is an independent predictor of coronary heart disease and stroke risks in patients with type 2 diabetes mellitus in China. Int J Endocrinol. 2017;2017:9620513. doi:10.1155/2017/9620513
21. Wu Y, He J, Sun X, et al. Carotid atherosclerosis and its relationship to coronary heart disease and stroke risk in patients with type 2 diabetes mellitus. Medicine. 2017;96:39.
22. Ramachandran A, Snehalatha C, Satyavani K, Latha E, Sasikala R, Vijay V. Prevalence of vascular complications and their risk factors in type 2 diabetes. J Assoc Physicians India. 1999;47(12):1152.
23. Baluja A, Rodriguez-Manero M, Cordero A, et al. Prediction of major adverse cardiac, cerebrovascular events in patients with diabetes after acute coronary syndrome. Diabetes Vasc Dis Res. 2020;8.
24. Dodos I, Georgopoulos S, Dodos K, et al. Correlation of glycosylated hemoglobin (HbA1c) levels with histological and ultrasound characteristics of the carotid plaque in diabetic and non-diabetic patients. Ann Vasc Surg. 2019;61:218–26.
25. Xiao H, Du A-M, Yun P, Zhang H-F, Tian Y, Xiao F-X. Prevalence and risk factors of chronic complications of type 2 diabetic inpatients in Hubei Province of central China: results from a multiple-hospital study. Int J Diabetes Dev Ctries. 2016;36(2):242–247.
26. Gajardo-Navarrete J, Ibieta G, Concha M, et al. Coronary artery disease in pre and postmenopausal women. The influence of tune 2 diabetes mellitus. Rev Med Chil. 2020;148(2):145–150. doi:10.4067/s0034-98872020000200145
27. Braga F, Pasqualetti S, Ferraro S, Panteghini M. Hyperuricemia as risk factor for coronary heart disease incidence and mortality in the general population: a systematic review and meta-analysis. Clin Chem Lab Med. 2016;54(1):7–15. doi:10.1515/cclm-2015-0523
28. Kim SY, Guevara JP, Kim KM, Choi HK, Heitjan DF, Albert DA. Hyperuricemia and coronary heart disease: a systematic review and meta-analysis. Arthritis Care Res. 2010;62(2):170–180.
29. Ito H, Abe M, Mifune M, et al. Hyperuricemia is independently associated with coronary heart disease and renal dysfunction in patients with type 2 diabetes mellitus. PLoS One. 2011;6(11):11. doi:10.1371/journal.pone.0027817
30. Yang Y, Tian J, Zeng C, et al. Relationship between hyperuricemia and risk of coronary heart disease in a middle-aged and elderly Chinese population. J Int Med Res. 2017;45(1):254–260. doi:10.1177/0300060516673923
31. El-Mesallamy HO, Hamdy NM, Salman TM, Ibrahim SM. Adiponectin and sE-selectin concentrations in relation to inflammation in obese type 2 diabetic patients with coronary heart disease. Angiology. 2012;63(2):96–102. doi:10.1177/0003319711408587
32. Haider R, Hyun K, Cheung NW, Redfern J, Thiagalingam A, Chow CK. Effect of lifestyle focused text messaging on risk factor modification in patients with diabetes and coronary heart disease: a sub-analysis of the TEXT ME study. Diabetes Res Clin Pract. 2019;153:184–190. doi:10.1016/j.diabres.2019.04.030
33. Edqvist J, Rawshani A, Adiels M, et al. Contrasting associations of body mass index and hemoglobin a1c on the excess risk of acute myocardial infarction and heart failure in type 2 diabetes mellitus. J Am Heart Assoc. 2019;8(24):e013871. doi:10.1161/JAHA.119.013871
34. Guo L, Cheng Y, Wang X, et al. Association between microalbuminuria and cardiovascular disease in type 2 diabetes mellitus of the Beijing Han nationality. Acta Diabetol. 2012;49(S1):S65–S71. doi:10.1007/s00592-010-0205-5
35. Yang Y, Huang B, Tan S, et al. Risk factor differences between type 2 diabetes patients with ischemic cerebrovascular versus coronary heart diseases at admission. J Diabetes Complications. 2015;29(6):783–787. doi:10.1016/j.jdiacomp.2015.04.016
36. Malmberg K, Ryden L, Wedel H, et al. FASTTRACK intense metabolic control by means of insulin in patients with diabetes mellitus and acute myocardial infarction (DIGAMI 2): effects on mortality and morbidity. Eur Heart J. 2005;26(7):650–661. doi:10.1093/eurheartj/ehi199
37. Ehara H, Yamamoto-Honda R, Kitazato H, et al. ApoE isoforms, treatment of diabetes and the risk of coronary heart disease. World J Diabetes. 2012;3(3):54–59. doi:10.4239/wjd.v3.i3.54
38. Garg N, Moorthy N, Kapoor A, et al. Hemoglobin A(1c) in nondiabetic patients: an independent predictor of coronary artery disease and its severity. Mayo Clin Proc. 2014;89(7):908–916. doi:10.1016/j.mayocp.2014.03.017
39. Hsu WH, Lai CW, Chen SC, et al. Greater low-density lipoprotein cholesterol variability increases the risk of cardiovascular events in patients with type 2 diabetes mellitus. Endocr Pract. 2019;25(9):918–925. doi:10.4158/EP-2019-0002
40. Tehrani DM, Zhao YL, Blaha MJ, et al. Discordance of low-density lipoprotein and high-density lipoprotein cholesterol particle versus cholesterol concentration for the prediction of cardiovascular disease in patients with metabolic syndrome and diabetes mellitus (from the multi-ethnic study of atherosclerosis MESA). Am J Cardiol. 2016;117(12):1921–1927.
41. Chin SO, Hwang JK, Rhee SY, et al. Risk factors for the progression of intima-media thickness of carotid arteries: a 2-year follow-up study in patients with newly diagnosed type 2 diabetes. Diabetes Metab J. 2013;37(5):365–374. doi:10.4093/dmj.2013.37.5.365
42. Sun JT, Liu Y, Lu L, et al. Diabetes-invoked high-density lipoprotein and its association with coronary artery disease in patients with type 2 diabetes mellitus. Am J Cardiol. 2016;118(11):1674–1679. doi:10.1016/j.amjcard.2016.08.044
43. Tolle M, Huang T, Schuchardt M, et al. High-density lipoprotein loses its anti-inflammatory capacity by accumulation of pro-inflammatory-serum amyloid A. Cardiovasc Res. 2012;94(1):154–162. doi:10.1093/cvr/cvs089
44. Tousoulis D, Papageorgiou N, Androulakis E, et al. Diabetes mellitus-associated vascular impairment novel circulating biomarkers and therapeutic approaches. J Am Coll Cardiol. 2013;62(8):667–676. doi:10.1016/j.jacc.2013.03.089
45. Cai H, Song CJ, Endoh I, et al. Serum amyloid A induces monocyte tissue factor. J Immunol. 2007;178(3):1852–1860. doi:10.4049/jimmunol.178.3.1852
46. King DE, Mainous AG, Buchanan TA, Pearson WS. C-reactive protein and glycemic control in adults with diabetes. Diabetes Care. 2003;26(5):1535–1539. doi:10.2337/diacare.26.5.1535
47. Wu G, Li G-B, Dai B, Zhang D-Q. Novel KIF6 polymorphism increases susceptibility to type 2 diabetes mellitus and coronary heart disease in Han Chinese men. J Diabetes Res. 2014;2014:1–8. doi:10.1155/2014/871439
48. Fumisawa Y, Funase Y, Yamashita K, et al. Systematic analysis of risk factors for coronary heart disease in japanese patients with type 2 diabetes: a matched case-control study. J Atheroscler Thromb. 2012;19(10):918–923. doi:10.5551/jat.13334
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.