")
Back to Journals » Journal of Inflammation Research » Volume 15
Nomogram Based on Inflammatory Biomarkers and Nutritional Indicators for Predicting Overall Survival in Locoregionally Advanced Nasopharyngeal Carcinoma
Authors Zhao R , Liang Z, Chen K, Zhu X
Received 13 March 2022
Accepted for publication 4 May 2022
Published 16 May 2022 Volume 2022:15 Pages 2971—2981
DOI https://doi.org/10.2147/JIR.S366299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Rong Zhao,1 Zhongguo Liang,1 Kaihua Chen,1 Xiaodong Zhu1– 3
1Department of Radiation Oncology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, People’s Republic of China; 2Affiliated Wu-Ming Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 3Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education/Guangxi Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Guangxi, People’s Republic of China
Correspondence: Xiaodong Zhu, Department of Radiation Oncology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, People’s Republic of China, Tel +86 13978873616, Email [email protected]
Purpose: To establish and validate a nomogram to predict overall survival in locoregionally advanced nasopharyngeal carcinoma (LA-NPC) based on inflammatory biomarkers and nutritional indicators.
Patients and Methods: A total of 1304 patients who underwent concurrent chemoradiotherapy (CCRT) with or without induction chemotherapy (IC) or adjuvant chemotherapy (AC) were included in the study. The prognosis factors of overall survival (OS) were selected by Cox regression analysis to establish the nomogram. Concordance index (C-index), calibration curves, decision curve analysis (DCA) and Kaplan–Meier curves were used to evaluate the nomogram.
Results: Using multivariate Cox analysis of clinically important variables, the following variables were incorporated in the prediction of OS: age, gender, T stage, N stage, pre-treatment plasma Epstein–Barr virus (EBV) DNA, neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), lactic dehydrogenase-to-albumin ratio (LAR) and prognostic nutritional index (PNI). The discriminative ability, clinical usefulness and calibration of the nomogram revealed good predictive ability as indicated by the C-index (0.717 in nomogram and 0.602 in the 8th AJCC staging system), decision curves, calibration curves and K-M curves.
Conclusion: Inflammatory biomarkers and nutritional indicators of survival for LA-NPC were selected to create a nomogram predicting OS. The proposed nomogram resulted in more accurate prognostic prediction than 8th AJCC staging system.
Keywords: locoregionally advanced nasopharyngeal carcinoma, inflammatory biomarker, nutritional indicator, nomogram, overall survival
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor in the head and neck, whose incidence has a distinct geographical distribution, mainly in east and Southeast Asia.1 There were about 133,354 new cases and 80,008 deaths of NPC worldwide in 2020.2 Due to the concealment of early symptoms of NPC, up to 80% of patients with locally advanced NPC (LA-NPC) were newly diagnosed in endemic areas, with a 5-year overall survival (OS) of 68.9–78.6%.3–5 Concurrent chemoradiotherapy (CCRT) is the core of the treatment for patients with LA-NPC, and the addition of induction chemotherapy (IC) or adjuvant chemotherapy (AC) to CCRT is controversial.6–8 Therefore, the identification of patients who might profit from IC or AC remains a challenge.
Currently, the prognosis and treatment plan options of NPC patients are mainly according to the tumor–node–metastasis (TNM) staging system of the Union of International Cancer Control and the American Joint Committee on Cancer (UICC/AJCC) 8th edition. However, patients with LA-NPC have significantly different survival outcomes at the same stage on account of the inherent heterogeneity of the organism. Therefore, an increasing number of approaches have been used to explore functional biomarkers that can improve the prognosis prediction of nasopharyngeal carcinoma. Recently, a great deal of emphasis has been dedicated to the role of nutrition and inflammatory status in the growth, biological aggressiveness and spread of different types of cancer.9–11 Several inflammatory biomarkers, such as platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR) and lymphocyte–monocyte ratio (LMR), have been demonstrated to be associated with the prognosis of various cancers.12–16 Nutritional indicators, such as prognostic nutritional index (PNI), lactate dehydrogenase-to-albumin ratio (LAR) were suggested as effective prognostic factors of NPC.17,18 The prognostic value of these biomarkers for NPC remains inconclusive. In the majority of studies concerning inflammatory predictors, only one of these biomarkers was analyzed without considering the others, and inflammatory factors were not analyzed in combination with nutritional indicators.
Epstein-Barr virus (EBV) DNA, an established biomarker, is associated with prognosis in patients with NPC, which can direct the choice of treatment options.19–22 It has been established that pre-treatment EBV DNA load can improve TNM staging.23,24 The aim of this study was to establish a nomogram based on inflammatory biomarkers, nutritional indicators and pre-treatment EBV DNA to predict individual prognosis of patients with LA-NPC and provide a framework for individualized treatment.
Materials and Methods
Participants and Data Collection
Patients were identified from a retrospective database between January 2010 and December 2017. The inclusion criteria of patients were as follows: (a) age at diagnosis ranged from 18 to 65 years; (b) histopathology confirmed NPC; (c) restaged to stage III or IVA according to the tumor–node–metastasis (TNM) staging system of the Union of International Cancer Control and the American Joint Committee on Cancer (UICC/AJCC) 8th edition; (d) received concurrent chemoradiotherapy (CCRT) with or without induction chemotherapy (IC) or adjuvant chemotherapy (AC). The exclusion criteria were as follows: (a) double or multiple cancers at diagnosis; (b) with missing values in relevant predictors or follow-up data. Ultimately, a total of 1304 patients were enrolled in the study. The research protocol was approved by the Medical Ethics Committee of the Affiliated Cancer Hospital of Guangxi Medical University (IRB approval number: LW2022052) and no additional patient informed consent that was specific to this study was required given its retrospective nature. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Demographic and clinical data were collected, including age, gender, T stage, N stage and treatment regimen. The hematology specimens were gathered within 1 week before treatment to acquire inflammatory biomarkers, nutritional indicators and pre-treatment Epstein–Barr Virus (EBV) DNA. EBV genomic BamHI-W fragment region was amplified using a real-time quantitative polymerase-chain reaction technique to determine EBV pre-processed DNA loading (pre-EBV DNA). The results were displayed as the number of copies of EBV genome per milliliter of plasma. The calculation formulas of inflammatory biomarkers and nutritional indicators were as follows:
PLR (platelet-to-lymphocyte ratio) = platelet count (109/L)/lymphocyte count (109/L);
NLR (neutrophil-to-lymphocyte ratio) = neutrophil count (109/L)/lymphocyte count (109/L);
LMR (lymphocyte-to-monocyte ratio) = lymphocyte count (109/L)/monocyte count (109/L);
LAR (lactate dehydrogenase-to-albumin ratio) = lactate dehydrogenase (U/L)/serum albumin (g/L);
PNI (prognostic nutritional index) = serum albumin (g/L) + 5 × 10−9 × lymphocyte count (109/L).
Treatment and Follow-Up
All the patients acquired radical intensity modulated radiation therapy with 6 megavoltage photons for 6–7 weeks. The cumulative radiation doses were 70 Gray or greater to the primary tumor and 60–70 Gray to the involved neck area. All potential sites of local infiltration and bilateral cervical lymphatics were irradiated to 54 Gray or greater. Chemotherapy was cisplatin-based and repeated every 3 weeks for 2–3 cycles depending on patient tolerance. The concurrent chemotherapy regimen was cisplatin delivered by either 40 mg/m2 per week or one administration of 100 mg/m2 every three weeks. The induction chemotherapy (IC) was TPF regimen (consisting of docetaxel [1 day of 60 mg/m2], cisplatin [1 day of 60 mg/m2] and 5-fluorouracil [600 mg/m2, by 120 hours of continuous intravenous infusion]) or GP regimen (consisting of gemcitabine [1000 mg/m2 on days 1 and 8], cisplatin [1 day of 60 mg/m2]). The adjuvant chemotherapy (AC) was PF regimen (cisplatin 80 mg/m2 and 5-fluorouracil 750 mg/m2 for 96 hours continuously).
Survival data were collected by follow-up. Patients were requested to reexamination every 3 months for the first year after treatment, every 6 months in next 4 years, and once a year after that. The primary outcomes of interest were overall survival (OS), defined as the period from the date of diagnosis to death in any case or last visit.
Statistical Analysis
The population was randomly divided into a training cohort and a validation cohort with a ratio of 3:2 (caret in R, version 6.0–90). Continuous variables were reported as medians with interquartile ranges (IQRs), and classification or grade variables were reported as whole numbers and proportions. Mann–Whitney U-tests were used for continuous variables, and pearson’s chi-square tests were applied to compare the classified variables and the constituent ratio of grade variables. Continuous variables were converted into binary variables according to cut-off values obtained through survival receiver operating characteristic (survivalROC) curve analysis. Predictors with P-values <0.1 in the univariate cox analysis and clinical importance variables were included in the multivariate Cox analysis. Multifactorial Cox proportional hazards model analysis was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs), and to identify factors, where P < 0.05.
Significant independent prognostic factors and clinically important variables were incorporated in the nomogram to predict the probability of 3-year and 5-year OS rates (rms in R, version 6.2–0). The model performance was assessed by the predictive accuracy of individual outcomes (discriminating ability), the accuracy of point estimates of the survival function (calibration) and by clinical usefulness. The discriminating ability of the nomogram was estimated using the Harrell’s C-index. The calibration curves quantified the prediction accuracy of nomogram measured by bootstrap verification with 1000 resamples. Decision curve analysis was used to evaluate the net benefit of the predictive model (ggDCA in R, version 1.2). The risk scores of patients were calculated via nomogram, and patients were divided into low-risk and high-risk groups based on the cut-off value acquired by survival ROC. The Kaplan–Meier method was used to analyze different groups, and the Log-rank test was devoted to examine the difference between survival curves.
All statistical analysis steps were performed in R, version 4.0.3 (http://www.r-project.org/). All P values were bilateral, and P < 0.05 was considered statistically significant in all analyses.
Results
Patient Characteristics
A total of 1304 patients were enrolled in the study and randomly assigned to a 3:2 ratio of 784 in the training cohort and 520 in the validation cohort (Table 1). In the total population, the median patient age was 46 years (IQR, 38–53 years), and 74.31% (969 of 1304) of the patients were male. According to the 8th AJCC/UICC staging system, there were 30 (2.30%) in T1, 401 (30.75%) in T2, 530 (40.64%) in T3 and 343 (26.30%) in T4. There were 27 (2.07%) in N0, 301 (23.08%) in N1, 675 (51.76%) in N2 and 301 (23.08%) in N3. Most patients received CCRT+IC/AC (57.67% [752 of 1304]). The median values of PLR, NLR, LAR, LMR and PNI were 144.91 (IQR, 112.10–189.04), 2.22 (IQR, 1.70–2.94), 4.17 (IQR, 3.62–4.91), 4.23 (IQR, 3.21–5.43), 51.90 (IQR, 48.20–55.50). The baseline data of the training cohort and validation cohort were balanced.
 |
Table 1 Patients’ Characteristics |
At a median follow-up of 67 months (range, 2–132 months), 30.5% (398 of 1304) of the patients had died. The 3-year, and 5-year OS percentages were 85.7% and 75.3%, respectively.
Factors Associated with OS in the Training Cohort
As per the survival ROC curves in the training cohort, the optimal cut-off values for age, PLR, NLR, LMR, LAR and PNI were identified to be 47 years, 157.14, 2.75, 9.83, 3.67 and 50.95, respectively (Supplementary Figure). Pre-treatment EBV DNA was classified into a high- and low-risk group based on a detectable/undetectable cut-off value of 5000 copies/mL defined by the laboratory. Established risk factors, as well as clinically important demographic and tumor characteristics, were selected as candidate variables for predictive models. Multivariable cox regression analysis identified the following variables independently associated with OS (Table 2): age (HR, 1.48; 95% CI, 1.13–1.94; P = 0.004), gender (HR, 1.47; 95% CI, 1.07–2.03; P = 0.019), EBV DNA (HR, 2.42; 95% CI, 1.83–3.21; P < 0.001), NLR (HR, 1.40; 95% CI, 1.03–1.90; P = 0.030), LMR (HR, 2.16; 95% CI, 1.10–4.24; P = 0.026), LAR (HR, 1.49; 95% CI, 1.06–2.09; P = 0.022) and PNI (HR, 0.71; 95% CI, 0.53–0.95; P = 0.021).
 |
Table 2 Univariable and Multivariable Cox Regression Analysis in the Training Cohort |
Nomogram and Model Performance
The nomogram to predict the OS of the patients with LA-NPC is shown in Figure 1. The nomogram to predict OS was created based on the following prognostic factors: age (≤47 or >47 years), gender (female or male), EBV DNA (<5000 or ≥5000 copies/mL), T stage (T1, T2, T3, or T4), N stage (N0, N1, N2 or N3), NLR (≤2.75 or >2.75), LMR (≤9.83 or >9.83), LAR (≤3.67 or >3.67) and PNI (≤50.95 or >50.95). Points were assigned to each variable based on its contribution to the outcome event. Higher total points according to the sum of the allocated points for each factor in the nomogram were associated with a worse prognosis.
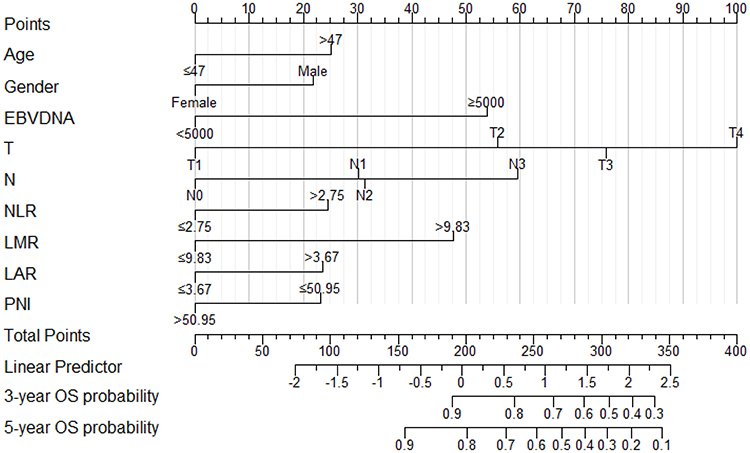 |
Figure 1 OS nomogram in the training cohort. Abbreviations: OS, overall survival; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; LAR, lactic dehydrogenase-to-albumin ratio; PNI, prognostic nutritional index. Notes: The line segment corresponding to each variable is marked with a scale, which represents the range of possible values of the variable and draws a vertical line upward to get the corresponding score. Add all the variables to get the total score and draw a vertical line downward to get the probability of survival of OS at 3 or 5 years. |
The discriminative ability of the nomogram for OS was assessed using the C-index (Table 3). The C-indexes for predicting OS in the nomogram were 0.717 in the training cohort and 0.688 in the validation cohort, which is higher than 8th TNM system (0.602 in the training cohort and 0.599 in the validation cohort). To further estimate the discriminative ability of the nomogram, the predicted probability of OS was then sketched as Kaplan–Meier curves (Figure 2). The risk stratification was established in the OS nomogram of the training and validation cohort, divided into low-risk and high-risk groups based on a cut-off value of 200 points (Supplementary Figure). Patients in the high-risk group had a substantially worse outcome compared with patients in the low-risk group (P < 0.0001).
 |
Table 3 Comparison of the C-Index of Nomogram and TNM Staging System |
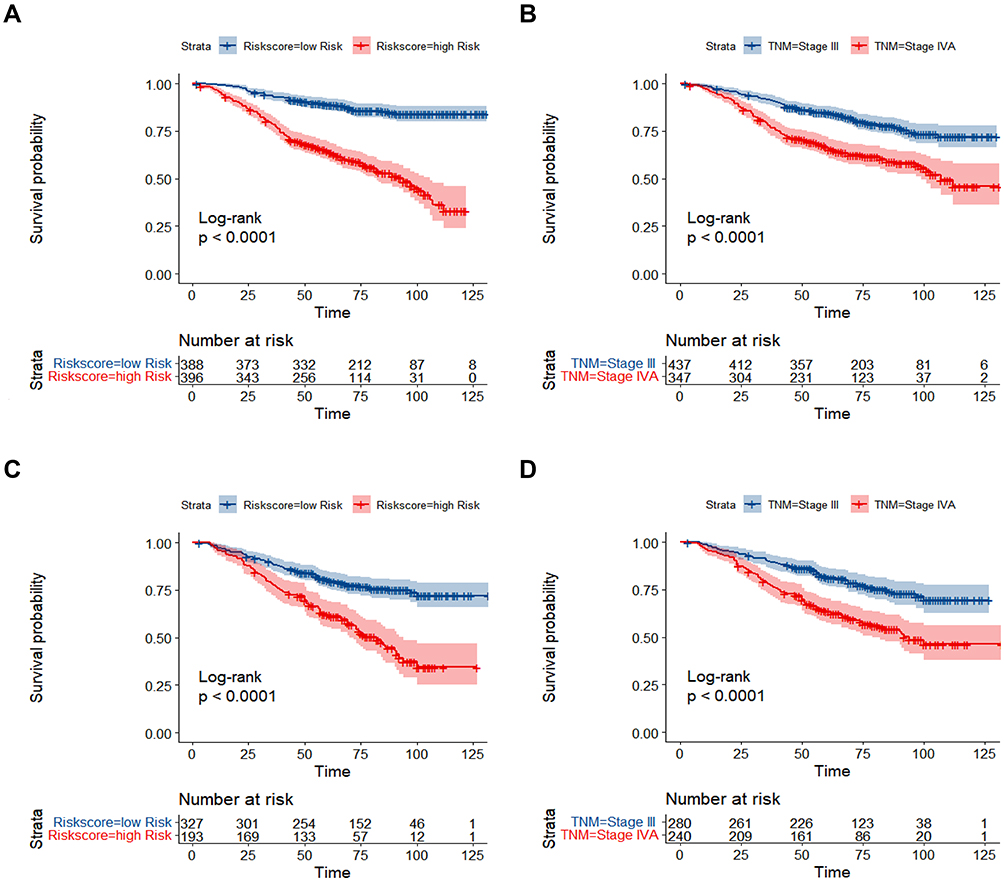 |
Figure 2 Kaplan–Meier curves demonstrating OS in patients of LA-NPC. Abbreviations: OS, overall survival; LA-NPC, locoregionally advanced nasopharyngeal carcinoma. Notes: Kaplan–Meier survival curves for OS of the training cohort (A and B) and validation cohort (C and D) in different models. The nomogram was divided into a high-risk group and a low-risk group comparison (A and C); AJCC/UICC 8th staging system was divided into stage III and stage IVA comparisons (B and D). |
Similarly, there were significant differences in the OS probability between stage III and stage IVA patients in the 8th TNM system (P < 0.0001).
The accuracy of the nomogram and potential overfit were evaluated by bootstrap validation with 1000 resamples. The calibration plots for the prediction of 3- and 5-year OS are displayed in Figure 3. The calibration curve diagrams demonstrated that the predicted probabilities were generally consistent with the actual probabilities.
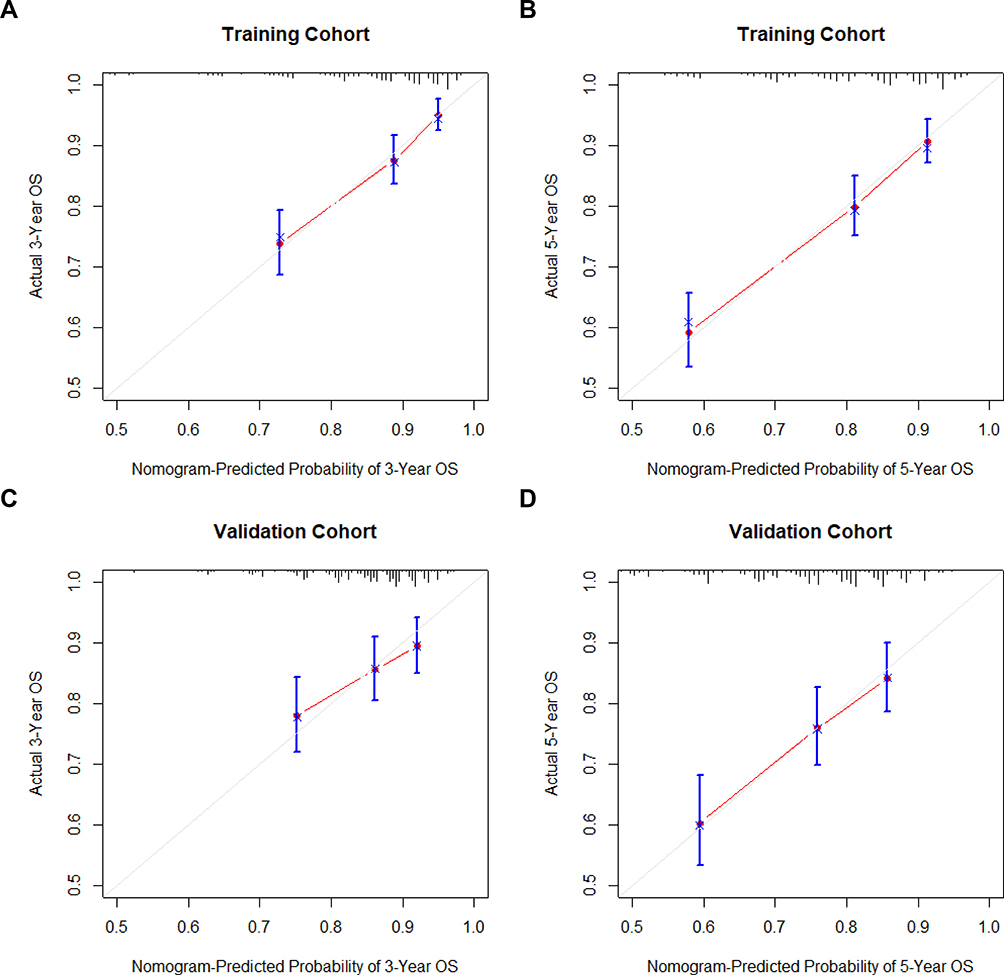 |
Figure 3 Calibration curve graphs for nomograms of OS. Abbreviation: OS, overall survival. Notes: Calibration curve graphs to predict the 3 and 5-year OS of the nomogram in the training cohort (A and B) and validation cohort (C and D). Nomogram-estimated OS were drawn on the abscissa; the observed OS were drawn on the ordinate. The diagonal representing the predicted probability was equal to the actual probability. The closer the nomogram curve is to the diagonal line, the more closely the predicted probability matches the actual probability. |
The decision curve analysis was applied to render the clinical validity of the nomogram, which revealed that the nomogram in predicting OS had a higher net benefit than the 8th TNM staging system (Figure 4).
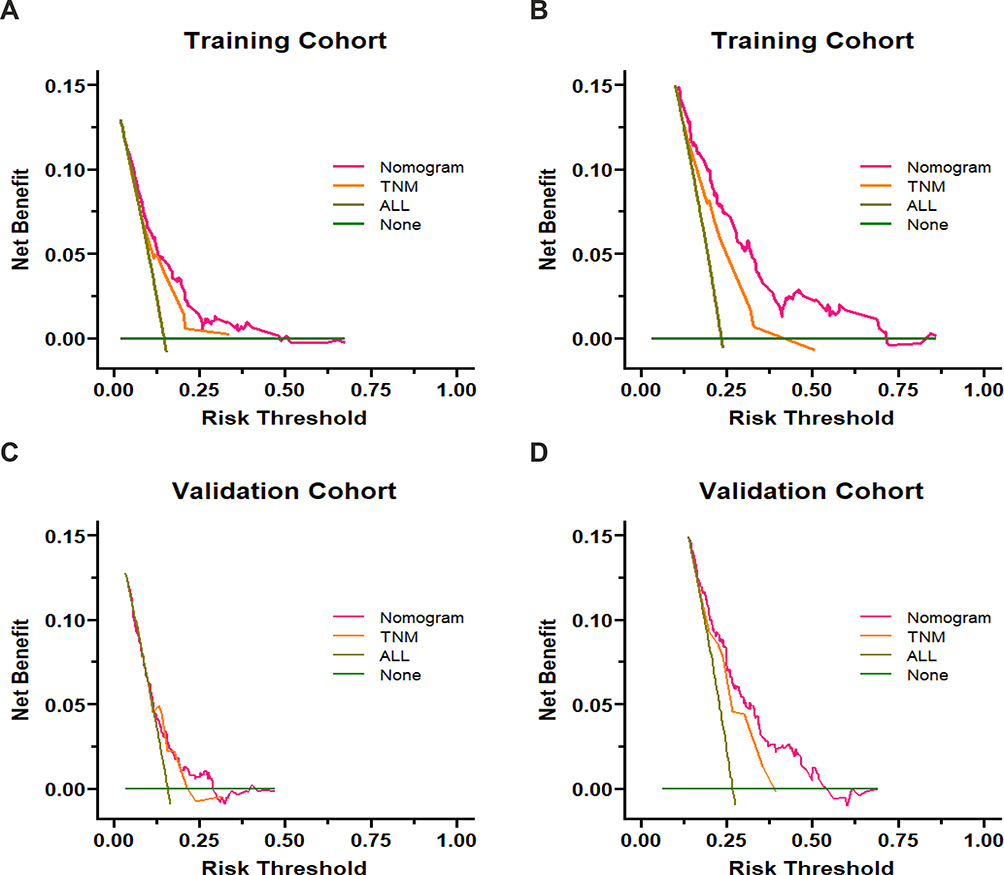 |
Figure 4 Decision curves of nomogram and 8th TNM staging system. Notes: Decision curves to predict the 3 and 5-year overall survival in the training cohort (A and B) and validation cohort (C and D). The x-axis was determined by the threshold probability, at which the harm of false-positive intervention exceeded the harm of a false-negative non-intervention, and thus an intervention was triggered. The y-axis was a net benefit, which was the relative benefit derived from the proportion of true-positive results subtracted from the proportion of false-positive results weighted by a ratio of threshold probabilities. Under the same probability, the clinical usefulness was better when the net benefit was higher. |
Discussion
In the current study, we constructed a nomogram for OS in patients with locally advanced nasopharyngeal carcinoma, combined clinical features and experimental factors, which was able to stratify high-risk and low-risk groups. It outperformed the overall staging of the eighth edition of the AJCC staging system on both the training and validation cohorts.
According to the 2020 National Comprehensive Cancer Network (NCCN) guidelines, the recommended treatment for LANPC is induction chemotherapy plus concurrent chemoradiotherapy (IC+CCRT) or concurrent chemoradiotherapy with adjuvant chemotherapy (CCRT+AC) as level 2A evidence, and CCRT as level 2B evidence.6 However, not all patients with LANPC who received CCRT would benefit from induction chemotherapy or adjuvant chemotherapy.7,25,26 Therefore, risk stratification of patients with LANPC and interventions in the high-risk group may improve prognosis.
The current staging of NPC patients is mainly the 8th edition of AJCC, and age, gender, and EBVDNA have also been confirmed to be associated with prognosis. It demonstrated that advanced age was a risk factor for prognosis, and male had a worse prognosis than female.27,28 Plasma EBV DNA has also been proved as a valuable biomarker for NPC.29 To personalize the prognosis of patients with NPC, inflammatory and nutritional indicators are gradually being explored, such as PLR, NLR, LMR, LAR, PNI.
It is known that inflammation is implicated with the development and progression of cancer, including promotion, cell transformation, survival, proliferation, angiogenesis, invasion and metastasis.30 Inflammation can be assessed by calculating changes in different clinical blood count parameters, such as white blood cells, platelets, neutrophils, lymphocytes, monocytes and so on.31 Jiang et al32 demonstrated that NLR is an independent prognostic indicator for OS, PFS, and DMFS in patients with NPC. Lu et al33 found that LMR was significantly associated with a relatively short OS in NPC. Our study shows that inflammatory biomarkers (such as NLR and LMR) have a strong survival predictive power in NPC patients.
Nutrition is an important aspect of cancer management, which determines the patient’s functional status, tolerance to therapeutic interventions and overall prognosis.34 PNI, an indicator of nutritional status, has been confirmed to have an important predictive value for metastasis and mortality in patients with NPC by Du et al17 Similarly, LAR, as an index that can respond to both nutritional status and tumor burden, was shown to be a valuable independent factor in NPC by Peng et al18 In our study, these inflammatory and nutritional indicators were also observed to be independently related to the overall survival of patients with NPC.
Nomograms, which generate individual probabilities of clinical events by integrating different prognostic and determinant variables, are more accurate than traditional staging. In addition, nomograms maximize the translation of complex regression equations into graphs, and the results of predictive models are more readable for patient assessment. Therefore, we established a nomogram in terms of pre-treatment clinical factors, EBV DNA, NLR, LMR, LAR and PNI, which enabled more accurate prognostic prediction for patients with LANPC and risk stratification to provide basis for individualized treatment plans.
There are several limitations of this study. First, this nomogram is only internally validated, and a large number of multicenter external validations are needed. Second, due to the nature of retrospective studies, selection bias may occur because patients are included only when they meet specific selection criteria. Third, there is no consensus on the expression of EBV DNA in plasma. Fourth, each biomarker will fluctuate with the state of the body and treatment, and this study only explored the relationship between inflammatory and nutritional indicators and prognosis before treatment. However, which of these markers before, after or during treatment were more valuable for prognosis is worthy of further discussion, which could be the direction of our future study. Furthermore, the chemokine and cytokine analyses were absent in the study because they were not routinely done in clinical practice. Besides, in order to explore the precision treatment regimen, we included stage III and IVA patients in the nomogram construction, which may be heterogeneity in the exploration process. Finally, this study focused on the first diagnosis and treatment of LA-NPC, and in no way explored the impact of its salvage treatment on overall survival.
Conclusion
Nomogram based on inflammatory and nutritional indicators can be applied as a clinically personalized tool to predict OS in patients with locally advanced nasopharyngeal carcinoma, offering reliable prognostic information and treatment strategies for patients in tiered management to obtain the maximum survival benefit.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Key Research and Development Program Project of Guangxi Zhuang Autonomous Region (Grant No. GuikeAB18221007), Guangxi Colleges and Universities Young and Middle-aged Teachers Research Basic Ability Improvement Project (2022KY0087), and the Independent Project of Key Laboratory of Early Prevention &Treatment for Regional High-Incidence-Tumor (GKE-ZZ202120).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Chen Y-P, Chan ATC, Le Q-T, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/s0140-6736(19)30956-0
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Mao YP, Xie FY, Liu LZ, et al. Re-evaluation of 6th edition of AJCC staging system for nasopharyngeal carcinoma and proposed improvement based on magnetic resonance imaging. Int J Radiat Oncol. 2009;73(5):1326–1334. doi:10.1016/j.ijrobp.2008.07.062
4. Wei KR, Zheng RS, Zhang SW, Liang ZH, Ou ZX, Chen WQ. Nasopharyngeal carcinoma incidence and mortality in China in 2010. Chin J Cancer. 2014;33(8):381–387. doi:10.5732/cjc.014.10086
5. Zhang MX, Li J, Shen GP, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy: a 10-year experience with a large cohort and long follow-up. Eur J Cancer. 2015;51(17):2587–2595. doi:10.1016/j.ejca.2015.08.006
6. Pfister DG, Spencer S, Adelstein D, et al. Head and neck cancers, version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;18(7):873–898. doi:10.6004/jnccn.2020.0031
7. Tan T, Lim WT, Fong KW, et al. Concurrent chemo-radiation with or without induction gemcitabine, carboplatin, and paclitaxel: a randomized, Phase 2/3 trial in locally advanced nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2015;91(5):952–960. doi:10.1016/j.ijrobp.2015.01.002
8. Chen L, Hu C-S, Chen X-Z, et al. Adjuvant chemotherapy in patients with locoregionally advanced nasopharyngeal carcinoma: long-term results of a Phase 3 multicentre randomised controlled trial. Eur J Cancer. 2017;75:150–158. doi:10.1016/j.ejca.2017.01.002
9. Bullock AF, Greenley SL, McKenzie GAG, Paton LW, Johnson MJ. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: systematic review, narrative synthesis and meta-analysis. Eur J Clin Nutr. 2020;74(11):1519–1535. doi:10.1038/s41430-020-0629-0
10. Philip M, Rowley DA, Schreiber H. Inflammation as a tumor promoter in cancer induction. Semin Cancer Biol. 2004;14(6):433–439. doi:10.1016/j.semcancer.2004.06.006
11. Yalcin S, Gumus M, Oksuzoglu B, et al. Nutritional aspect of cancer care in medical oncology patients. Clin Ther. 2019;41(11):2382–2396. doi:10.1016/j.clinthera.2019.09.006
12. Liu D, Czigany Z, Heij LR, et al. The value of platelet-to-lymphocyte ratio as a prognostic marker in cholangiocarcinoma: a systematic review and meta-analysis. Cancers. 2022;14(2):438.
13. Valero C, Lee M, Hoen D, et al. Pretreatment neutrophil-to-lymphocyte ratio and mutational burden as biomarkers of tumor response to immune checkpoint inhibitors. Nat Commun. 2021;12(1). doi:10.1038/s41467-021-20935-9
14. Zhang Q, Song MM, Zhang X, et al. Association of systemic inflammation with survival in patients with cancer cachexia: results from a multicentre cohort study. J Cachexia Sarcopeni. 2021;12(6):1466–1476. doi:10.1002/jcsm.12761
15. Nost TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
16. Kumarasamy C, Tiwary V, Sunil K, et al. Prognostic utility of platelet-lymphocyte ratio, neutrophil-lymphocyte ratio and monocyte-lymphocyte ratio in head and neck cancers: a detailed PRISMA compliant systematic review and meta-analysis. Cancers. 2021;13(16):4166. doi:10.3390/cancers13164166
17. Du XJ, Tang LL, Mao YP, et al. Value of the prognostic nutritional index and weight loss in predicting metastasis and long-term mortality in nasopharyngeal carcinoma. J Transl Med. 2015;13(1). doi:10.1186/s12967-015-0729-0
18. Peng RR, Liang ZG, Chen KH, Li L, Qu S, Zhu XD. Nomogram based on Lactate Dehydrogenase-to- Albumin Ratio (LAR) and Platelet-to-Lymphocyte Ratio (PLR) for predicting survival in nasopharyngeal carcinoma. J Inflamm Res. 2021;14:4019–4033. doi:10.2147/Jir.S322475
19. Tan LP, Tan GW, Sivanesan VM, et al. Systematic comparison of plasma EBV DNA, anti-EBV antibodies and miRNA levels for early detection and prognosis of nasopharyngeal carcinoma. Int J Cancer. 2020;146(8):2336–2347. doi:10.1002/ijc.32656
20. Liu L-T, Chen Q-Y, Tang L-Q, et al. Neoadjuvant or adjuvant chemotherapy plus concurrent CRT versus concurrent CRT alone in the treatment of nasopharyngeal carcinoma: a Study Based on EBV DNA. J Natl Compr Canc Netw. 2019;17(6):703–710. doi:10.6004/jnccn.2018.7270
21. Hui EP, Li WF, Ma BB, et al. Integrating postradiotherapy plasma Epstein-Barr virus DNA and TNM stage for risk stratification of nasopharyngeal carcinoma to adjuvant therapy. Ann Oncol. 2020;31(6):769–779. doi:10.1016/j.annonc.2020.03.289
22. Wang W-Y, Twu C-W, Chen -H-H, et al. Plasma EBV DNA clearance rate as a novel prognostic marker for metastatic/recurrent nasopharyngeal carcinoma. Clin Cancer Res. 2010;16(3):1016–1024. doi:10.1158/1078-0432.CCR-09-2796
23. Tang L-Q, Li C-F, Li J, et al. Establishment and validation of prognostic nomograms for endemic nasopharyngeal carcinoma. J Natl Cancer Inst. 2016;108(1):djv291. doi:10.1093/jnci/djv291
24. Guo R, Tang -L-L, Mao Y-P, et al. Proposed modifications and incorporation of plasma Epstein-Barr virus DNA improve the TNM staging system for Epstein-Barr virus-related nasopharyngeal carcinoma. Cancer. 2019;125(1):79–89. doi:10.1002/cncr.31741
25. Lan XW, Xiao Y, Zou XB, Zhang XM, OuYang PY, Xie FY. Outcomes of adding induction chemotherapy to concurrent chemoradiotherapy for stage T3N0-1 nasopharyngeal carcinoma: a propensity-matched study. Onco Targets Ther. 2017;10:3853–3860. doi:10.2147/OTT.S133917
26. Frikha M, Auperin A, Tao Y, et al. A randomized trial of induction docetaxel-cisplatin-5FU followed by concomitant cisplatin-RT versus concomitant cisplatin-RT in nasopharyngeal carcinoma (GORTEC 2006-02). Ann Oncol. 2018;29(3):731–736. doi:10.1093/annonc/mdx770
27. Huang WY, Lin CL, Lin CY, et al. Survival outcome of patients with nasopharyngeal carcinoma: a nationwide analysis of 13 407 patients in Taiwan. Clin Otolaryngol. 2015;40(4):327–334. doi:10.1111/coa.12371
28. Xu C, Chen YP, Liu X, et al. Establishing and applying nomograms based on the 8th edition of the UICC/AJCC staging system to select patients with nasopharyngeal carcinoma who benefit from induction chemotherapy plus concurrent chemoradiotherapy. Oral Oncol. 2017;69:99–107. doi:10.1016/j.oraloncology.2017.04.015
29. Chan ATC, Hui EP, Ngan RKC, et al. Analysis of plasma Epstein-Barr virus DNA in nasopharyngeal cancer after chemoradiation to identify high-risk patients for adjuvant chemotherapy: a randomized controlled trial. J Clin Oncol. 2018:JCO2018777847. doi:10.1200/JCO.2018.77.7847
30. Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and cancer. Ann Afr Med. 2019;18(3):121–126. doi:10.4103/aam.aam_56_18
31. Riesco A. Five-year cancer cure: relation to total amount of peripheral lymphocytes and neutrophils. Cancer. 1970;25(1):135–140. doi:10.1002/1097-0142(197001)25:1<135::aid-cncr2820250120>3.0.co;2-9
32. Jiang Y, Qu S, Pan X, Huang S, Zhu X. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in intensity modulated radiation therapy for nasopharyngeal carcinoma. Oncotarget. 2018;9(11):9992–10004. doi:10.18632/oncotarget.24173
33. Lu A, Li H, Zheng Y, et al. Prognostic significance of neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio, and platelet to lymphocyte ratio in patients with nasopharyngeal carcinoma. Biomed Res Int. 2017;2017:3047802. doi:10.1155/2017/3047802
34. Dewys WD, Begg C, Lavin PT, et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med. 1980;69(4):491–497. doi:10.1016/s0149-2918(05)80001-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.