")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 12
Nocturnal hemodialysis: improved quality of life and patient outcomes
Authors Koh TJK
Received 1 November 2018
Accepted for publication 12 January 2019
Published 3 April 2019 Volume 2019:12 Pages 59—68
DOI https://doi.org/10.2147/IJNRD.S165919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Timothy Jee Kam Koh
Department of Renal Medicine, Tan Tock Seng Hospital, 308433, Singapore
Abstract: Conventional hemodialysis is associated with high morbidity and mortality rates, as well as a reduced quality of life. There is a growing interest in the provision of more intensive hemodialysis, due to associated benefits in terms of reduced cardiovascular morbidity, better regulation of mineral metabolism, as well as its impact on quality of life measures, fertility, and sleep. Nocturnal hemodialysis, both in center and at home, allows the delivery of more intensive hemodialysis. This review discusses the benefits of nocturnal hemodialysis and evaluates the evidence based on available literature.
Keywords: nocturnal hemodialysis, quality of life, benefits, outcomes, survival, cardiac
Introduction
The history of nocturnal hemodialysis (NHD) mirrors that of chronic hemodialysis itself. The first patient on chronic hemodialysis started on March 9, 1960, with the first dialysis session lasting for a total of 76 hours, including three nights on dialysis.1 However, NHD in its current form is widely recognized to be pioneered by Dr Stanley Shaldon in 1963, where his team was the first to report the successful use of unattended overnight hemodialysis.2 Dr Robert Uldall is recognized as having established the first successful regular nocturnal home hemodialysis program in Toronto in 1994.3
NHD is currently practiced in many parts of the world; however, its true prevalence is not known. The International Quotidian Dialysis Registry (IQDR) was established in June 2004, with the aim to study practices and outcomes associated with the use of hemodialysis regimens of increased frequency and/or duration. However, the IQDR only has established agreements with Australia, New Zealand, France, UK, USA, and Canada, hence data are only available from these countries. Based on the IQDR Annual Report 2010, there were 216, 1,030, 2,069, and 12 patients from Canada, USA, Australia/New Zealand, and France, respectively, undergoing NHD during that period.4
For this review, a search on PubMed for articles related to NHD in adults, that were published in English, was conducted up to August 2018, without a specific start date. As far as possible, full text articles were reviewed for completed studies, and references were also evaluated. The indications for NHD, benefits in terms of quality of life (QOL), and other patient outcomes were reviewed as well as possible complications.
NHD: how is it performed?
NHD can either be performed in the center or within the home setting. Home NHD affords the patient the ability and flexibility to increase the frequency of dialysis beyond the three times per week schedule, which is usually limited in-center for logistic or financial reason. Suitable patients for consideration should be physically and intellectually capable of performing such a therapy at home or have a suitable care partner. Most importantly, such patients should be motivated for this therapy. Patients will need to undergo a training program to assess competence. A physical space is also necessary to perform the therapy and provide storage for the supplies. However, it is recognized that not all patients may be suitable for a home-based dialysis program, due to physical inability, lack of home support or a suitable home, or an unwillingness to perform dialysis away from nursing care or medical support. In-center NHD provides an alternative to such patients who may want more intensive hemodialysis but are not suitable for a home program, while at the same time providing the associated benefits of more intensive dialysis.
The typical prescriptions for NHD are as indicated in Table 1. Of note, it may be necessary to alter the dialysate prescription due to the long duration of each dialysis session. A higher dialysate calcium (1.5–1.75 mmol/L), lower bicarbonate (30 mmol/L for 5–7 nights per week, 35 mmol/L for 3–4 nights per week), and phosphate additives may become necessary for some patients.
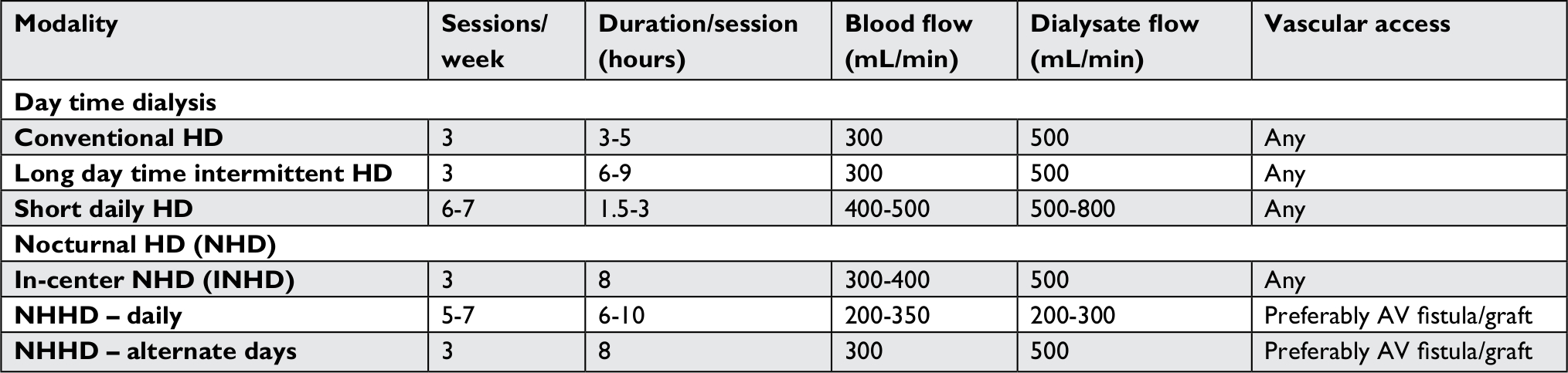 | Table 1 Classification and characteristics of the various hemodialysis modalities Notes: Reprinted with permission from Ranganathan D, John GT. Nocturnal hemodialysis. Indian J Nephrol. 2012;22(5):323–332.5 Copyright © 2012, Wolters Kluwer Medknow Publications. Available at: http://www.indianjnephrol.org/article.asp?issn=0971-4065;year=2012;volume=22;issue=5;spage=323;epage=332;aulast=Ranganathan#. The Creative Commons license does not apply to this content. Use of the material in any format is prohibited without written permission from the publisher, Wolters Kluwer Health, Inc. Please contact [email protected] for further information. Abbreviations: EQ-5D, EuroQoL EQ-5D; FHN, Frequent Hemodialysis Network; NHD, nocturnal hemodialysis; PHC, Physical Health Composite; KDQOL, Kidney Disease QOL; KDQOL-SF, Kidney Disease QOL-Short Form; QOL, quality of life; SF-36 RAND, RAND 36-item Short Form Survey. |
What is wrong with conventional hemodialysis (CHD)?
The current standard of care for patients on hemodialysis in many parts of the world is a three times per week regime, ranging from 3 to 5 hours depending on local practice. However, mortality remains high in this group.6 Cardiovascular disease remains the leading cause of death in end-stage renal disease (ESRD). Risk factors contributing to these include hypertension, uremia, anemia, left ventricular (LV) hypertrophy, hyperphosphatemia, and poor extracellular volume control. Conventional intermittent hemodialysis has not been shown to correct these factors adequately, possibly leading to the high mortality in this group of patients. CHD also results in wide fluctuations in biochemical parameters and intravascular fluid volumes. In hemodialysis patients, blood pressure (BP) steadily increases during the interdialytic interval, and the rate of BP increment is proportional to the interdialytic weight gain.7 In addition to the elevated interdialytic BP, excess volume accumulation over the long interdialytic interval also affects hemodynamic stability during dialysis.8 Bleyer et al demonstrated that patients who died during the last 12-hour period of the long interdialytic interval had higher average serum potassium levels as compared to survivors.9 This was recognized as early as 1974 by Kjellstrand et al,10 who described this as the “unphysiology” of dialysis.
As a result, there is a growing interest in the provision of intensive hemodialysis, as it is believed to provide superior dialysis due to an increased dose, duration, and frequency of dialysis. Increasing dialysis duration is increasingly being recognized as an important factor in the delivery of hemodialysis. In the National Cooperative Dialysis Study,11 in both the high and low time-averaged urea groups, those patients dialyzed for the shorter therapy duration (2.3–3.5 hours) experienced more hospitalizations than the patients undergoing longer therapy duration (4.5–5 hours, P=0.06). Observational studies have suggested that rapid ultrafiltration rates are associated with poorer cardiovascular outcomes, with rates of >13mL/kg/hour associated with a 59% increase in all-cause mortality, and a 71% increase in cardiovascular mortality (P<0.01) in a post hoc analysis of the Hemodialysis (HEMO) study.12 Besides contributing to an increased dialysis dose and clearance, an increase in dialysis duration also allows the need for rapid ultrafiltration rates to be mitigated due to lower hourly ultrafiltration rates. Home NHD with the capability of increasing the frequency of therapy also avoids the long interdialytic interval. Large registry-based cohort studies have consistently linked intermittent dialysis schedules with an elevated risk of death and cardiovascular complications, with such events occurring more commonly on the first dialysis day of the week.13 NHD, performed either in the center or at home, will allow an increase in either duration or frequency of dialysis, or both.
NHD: what are the clinical benefits?
Survival
NHD has been associated with improved long-term survival compared to CHD. Randomized controlled trials assessing survival in this cohort of patients are limited, and data demonstrating benefit have been based mainly on observational studies. The Frequent Hemodialysis Network (FHN) Nocturnal Trial published by Rocco et al14 in 2011 randomized 87 patients to three times per week CHD or NHD six times per week, with the two coprimary outcomes of 1) death or 12-month change of LV mass and 2) death or 12-month change in the RAND 36-item Short Form Survey Physical Health Composite (PHC). There was no significant effect for NHD on either of the two coprimary outcomes (death or LV mass HR of 0.68, or of death or RAND PHC HR of 0.91). Of note, there were several limitations of the trial, including the small sample size (original sample size calculation of 250) and lower adherence to the dialysis prescription in the nocturnal arm. Recruitment for the trial was challenging due to the initial forced assignment to either in-center or home.15 Patients included in the trial were also incident patients with better residual renal function and younger in age. The mortality in the control arm (1/42 or 2.38%) was also a lot lower than that of the general hemodialysis population in the USA. Lastly, the outcomes of the trial were driven predominantly by the nonmortality endpoints. In conclusion, the FHN Nocturnal Trial was a negative trial in terms of mortality benefit, limited by its lack of power.
Registry-based studies have reported an association with better survival for NHD. An analysis of 338 patients in the IQDR (which consisted mainly of NHD patients) reported an improved survival compared to 1,388 from the Dialysis Outcomes and Practice Patterns cohort, with an HR of 0.55 (95% CI of 0.34 and 0.87, respectively).16 An analysis of an US Renal Data System (USRDS) cohort comparing frequent hemodialysis vs CHD included 94 patients on NHD. Ten propensity score-matched control patients for each NHD patient were identified from the USRDS database. NHD was associated with a significant reduction in mortality risk with an HR of 0.36 (95% CI: 0.22–0.61, P=0.0001).17 Lastly, data from Fresenius Medical Care North America facilities compared patients who converted to in-center NHD to patients on CHD in a 1:3 propensity score-matched cohort. NHD was associated with a 25% reduction in the risk of death after adjustment for age, body mass index, and dialysis vintage, with an HR of 0.75 (95% CI: 0.61–0.91, P=0.004).18 It is important to remember, however, that registry data have its inherent biases, including the self-selection of patients for more intensive hemodialysis as well as the potential for other unknown exposures.
Renal transplantation is considered the gold standard renal replacement therapy for ESRD. However, not every patient may be suitable for renal transplant due to medical issues. Pauly et al19 performed a matched study of a Canadian cohort of home NHD patients with a matched cohort of patients from the USRDS who had undergone either a living (LTX) or a deceased donor (DTX) kidney transplant in a 1:3:3 ratio, matching for race, diabetic status, and duration of CHD prior to treatment with NHD, DTX, or LTX. There was no difference in adjusted survival between DTX and NHD (HR: 0.87, 95% CI: 0.50–1.51, P=0.61, NHD control group), whereas LTX survival was better (HR: 0.51, 95% CI: 0.28–0.91, P=0.02). Of note, the CI in the comparison between the DTX and NHD group is wide.
In summary, as a randomized trial of survival on NHD vs CHD is unlikely to be repeated due to the challenges mentioned previously, the currently available literature supports the association between improved survival and NHD.
Cardiac
Patients with ESRD have a high cardiovascular morbidity and mortality. Factors unique to patients on dialysis include anemia, chronic inflammation, pressure, and fluid overload.20 These lead to LV hypertrophy, which is a strong predictor of poor cardiac outcomes in chronic hemodialysis.21 NHD, both in-center and frequent home, has been shown to result in a reduction in LV hypertrophy and mass.
Chan et al22 first reported a significant reduction in LV mass index in 28 patients who were converted to NHD (from 147±42 to 114±40 g/m2, P=0.004), with 20 of the 28 patients achieving normal LV mass by Framingham criteria. Culleton et al23 conducted a randomized controlled trial to compare the effects of frequent NHD vs CHD on change in LV mass (as assessed by cardiac MRI) and health-related QOL (HRQOL) over 6 months. Fifty-two patients were assigned in a 1:1 ratio to receive NHD six times weekly or CHD three times weekly. Frequent NHD significantly improved the primary outcome (mean LV mass difference between groups 15.3 g, 95% CI: 1–29.6, P=0.04). As discussed previously, the FHN Nocturnal Trial14 included death or 12-month change of LV mass as one of its coprimary outcomes. Although the difference was not statistically significant, the mean difference in the change in LV mass between the two arms after adjustment for pre-specified covariates was −10.9 g (95% CI: −23.7 to +1.8 g). The authors commented that the results neither prove nor disprove the hypothesis that frequent NHD leads to clinically important reduction in LV mass, and that reduction of LV mass close to the center of the interval has been associated with differences in mortality in other studies.24 In addition, as the FHN Nocturnal Trial included a larger proportion of incident patients, it may have resulted in urine volume and renal solute clearance reducing the contribution of the dialysis regimens to total solute and fluid removal.
The effect of home NHD on cardiac remodeling has also been examined, however, the results are inconclusive. Eleven patients who underwent home NHD also underwent transthoracic echocardiography (TTE) and cardiac MRI at baseline, and after 1 year on NHD. LV mass index decreased significantly at 1 year by both TTE (152±7–129±8 g/m2, P<0.05) and cardiac MRI (162±4–124±4 g/m2, P<0.05). There was also a significant reduction in both left and right atrial volumes as well as in right ventricular (RV) mass index over 1 year of follow-up.25 Diastolic dysfunction also improved from a baseline grade of 3.4 to 1.2 at 1 year of follow-up. In contrast, an analysis of the FHN Nocturnal Trial26 revealed that there was no significant difference in LV or RV volume, or ejection fractions, with a good residual renal function for this cohort postulated to be one of the reasons contributing to this difference.
Conversion from in-center conventional to in-center nocturnal may also result in similar benefits to the cardiac structure and function. Wald et al27 conducted a retrospective cohort study on 37 CHD patients, who converted to in-center NHD, examining the effects on LV mass as assessed by cardiac MRI. LV mass declined by 32±58 g (P=0.002) at 6-month postconversion and by 40±56 g (P=0.0004) at 12-month postconversion. The rate of change of LV mass decreased significantly from 0.4 g/year before conversion to −11.7 g/year following conversion (P<0.0001). There was no significant change of left atrial volume or remodeling after conversion to NHD.28 These findings on LV mass reduction were replicated in another cohort of patients on in-center NHD by Ok et al,29 where 247 NHD patients were compared to 247 CHD patients in a prospective controlled study, with LV mass assessed by echocardiography. With similar LV mass indices at baseline (NHD 140±44 g/m2 vs CHD 142±52 g/m2), the NHD group had a final LV mass index of 116±34 g/m2 compared to the CHD group (139±45 g/m2), with a P-value <0.001. In contrast to the study by the Toronto group, left atrial diameter and left ventricular end-diastolic diameter were also significantly reduced in this NHD group. Possible causes of the difference in outcome include a difference in assessment tool (echocardiography readings limited by geometric assumptions) as well as other factors affecting chamber remodeling. In summary, conversion to in-center NHD was associated with improvements in LV mass reduction in the above two studies.
CHD has also been associated with myocardial stunning,30 with the induction of global and segmental myocardial ischemia. This has been associated with an increased mortality.31 Factors associated with myocardial stunning include ultrafiltration volume/rate and intradialytic hypotension.31 Home NHD, as a form of frequent dialysis, has been shown to reduce the extent and severity of dialysis-induced regional wall motion abnormalities compared to CHD.32
Benefits in terms of hospitalization related to cardiovascular events have also been demonstrated.33 In a prospective controlled study of patients converted to NHD compared to controls on CHD, conversion to NHD was associated with a decrease in the composite endpoint of dialysis or cardiovascular-related admission rate (0.5±0.15–0.17±0.06 admissions per patient year, P=0.04). In contrast, patients on CHD had a stable admission rate.
In summary, NHD (both home and in-center) has been shown to have beneficial effects on cardiac parameters in terms of LV mass reduction. In addition, home frequent NHD has been associated with a reduction of myocardial stunning compared to CHD. The effect on other parameters like left atrial remodeling and volume reduction remain inconclusive.
Blood pressure
BP reduction has been consistently demonstrated in NHD, both in-center and home frequent NHD. A reduction of the number of BP medications has also been demonstrated. There are several postulated mechanisms by which this is achieved. A reduction of peripheral resistance has been demonstrated in NHD, driven in part by a reduction in sympathetic activity, with a significant reduction of plasma norepinephrine levels.34 Amelioration of sleep apnea is another mechanism by which BP control is improved, as nocturnal hypoxemia is strongly linked to sympathetic nervous system activation. NHD reduces the number of episodes of hypopnea and apnea significantly and improves the balance between sympathetic and vagal pulse rate modulations. There may also be an improvement in endothelial function with more intensive hemodialysis.35 Last, better volume control has also been postulated to contribute to better BP control.
In the two randomized controlled trials involving patients on frequent NHD, better BP control was achieved. In the study by Culleton et al,23 6-month SBP decreased in patients randomized to NHD by 7 mmHg and increased in patients on CHD by 4 mmHg (mean difference of 11 mmHg, 95% CI: –2 to 24 mmHg). After adjustment for mean baseline BP, this mean difference between groups increased to 14 mmHg (95% CI: 3–26 mmHg, P=0.01). This was achieved despite a reduction of antihypertensive medication. In the FHN Nocturnal trial,14 hypertension was better controlled in the NHD arm, with a reduction in weekly SBP of −9.7 mmHg (95% CI: −16.9 to −2.5 mmHg, P=0.009). Again, this was achieved despite a significant reduction in the number of antihypertensive medications supplied.
With in-center NHD, despite the relative reduction in frequency of therapy as compared to frequent home NHD, a reduction in number of antihypertensive medications was noted, although the change in BP was not statically significant. The study by Ok et al29 discussed earlier did not demonstrate a change in BP levels over 12 months, however, the need for antihypertensive medication declined from 22% to 8% in NHD patients (P=0.02), while it did not change in the conventional arm. In the study by Wald et al,27 conversion to in-center NHD was associated with a nonsignificant reduction in both SBP and DBP. The mean number of antihypertensive medications declined, with a between group reduction of −0.7 (95% CI: −1.1 to −0.3, P=0.002). The difference in BP reduction between the frequent home and in-center NHD patients could perhaps be attributed to the increased frequency of treatment performed in the home setting.
Quality of life
CHD is an inadequate treatment for ESRD patients. Conventional targets for dialysis adequacy in terms of small solute clearance represent only about 15% of that achieved by a normal functioning kidney.36 Patients also experience symptoms of cramps or dizziness during CHD due to high ultrafiltration rates or accumulated fluid volumes, with patients feeling “washed out” and fatigued after each dialysis session.37 Due to the inadequacy of CHD, medications must be consumed to achieve better BP control and phosphate control. This also contributes to the pill burden of this group of patients, which is one of the highest in any chronic disease state.38 It is hence unsurprising that patients on CHD have poorer QOL scores.
The effect of NHD on QOL is more variable, depending on the cohort and assessment tool/scale used. There have been several randomized controlled trials assessing QOL as one of their primary/secondary outcomes. The FHN Nocturnal Trial14 included death or 12-month change in the SF-36 RAND PHC as one of its two coprimary outcomes. The mean PHC score increased for the entire cohort by 2.4 points (95% CI: 0.3–4.5 points, P=0.02). This increase in PHC score was similar between both the groups, with an estimated mean difference of only 0.6 points. One possible explanation of this result was that the improvement in PHC scores in both arms may have resulted from a change of venue rather than the therapy itself. The Culleton study23 also assessed HRQOL as one of its secondary outcome measures, using the EuroQoL EQ-5D (EQ-5D) index score (scale range 0.0 [dead] to 1.0 [full health]) as its primary HRQOL outcome, with a minimum increment of 0.03 being considered clinically important. This study also utilized the ED-5D visual analog scale score (0–100, with 100 representing perfect health) and the Kidney Disease QOL-Short Form (KDQOL-SF) questionnaire (the authors choosing four out of the 11 dimensions a priori, ie, kidney disease-related symptoms/problems, effects of kidney disease, burden of kidney disease, and sleep). In the primary analysis, NHD did not improve the change of EQ-5D scores from baseline to 6 months compared to CHD (between group difference: 0.05, 95% CI: −0.07 to 0.17, P=0.43). Similarly, NHD did not result in a statistically significant change of EQ-5D visual analog scale score from baseline. However, when the above scores were compared to the scores at time of randomization, the between group difference was larger for the EQ-5D score (between group difference: 0.12, 95% CI: −0.005 to 0.25, P=0.06) and was statistically significant for the EQ-5D visual analog scale score (P=0.03). In terms of the KDQOL-SF domains, NHD statistically improved the domains “effects of kidney disease” and “burden of kidney disease” compared to CHD, with the results not changing appreciably when adjusting for baseline HRQOL values and baseline dialysis modality. It is important to note that in this study, the baseline scores for the entire cohort was in the 0.7 range for the EQ-5D score, which is substantially higher than what is typically seen in hemodialysis patients, in fact, being like the scores in patients following successful renal transplantation. This may have limited the ability of NHD in improving overall QOL scores in this study.
Several observational studies have also assessed the impact of NHD on QOL. An Australian group assessed changes in QOL after conversion from conventional home hemodialysis to home NHD in 63 patients in an observational cohort study.39 Outcome measures included KDQOL, assessment of QOL instruments, and 6-minute walk test, which were assessed at baseline and 6 months. For KDQOL, significant improvements in general health (P=0.02), overall health ratings (P=0.008), physical function (P=0.003), physical role (P=0.018), and energy and fatigue (P=0.027) were documented. There was a trend toward improvement in burden of kidney disease (P=0.05) and emotional role (P=0.066). On assessment of QOL, there was a trend toward improvement in overall utility score from 0.65 (0.39–0.81) to 0.73 (0.46–0.86), P=0.096. A Toronto group conducted interviews with 24 home NHD patients and compared them to 19 in-center hemodialysis patients.40 Home NHD was associated with a higher utility score (as assessed by the standard gamble technique), with NHD scoring 0.77±0.23 and CHD scoring 0.53±0.35 (P=0.03). The London Ontario group also reviewed QOL among patients on more intensive dialysis, including 12 on NHD, compared to CHD, using the time trade-off method.41 Utility scores were significantly higher for the NHD group (0.781±0.171) vs CHD group (0.703±0.266), P<0.05.
Lastly, further analyses of the FHN Nocturnal Trial were conducted to assess the impact of frequent home NHD on other aspects like physical performance, health, and functioning42 and mental health.43 With regards to physical performance, health, and functioning, the main outcome measures were adjusted change in scores over 12 months on the short physical performance battery (SPPB), PHC, and physical functioning subscale (PF) based on an intention to treat principle. There was no significant difference in the SPPB (adjusted mean change of −0.92±0.44 to −0.41±0.43, P=0.41), PHC (2.7±1.4 vs 2.1±1.5, P=0.75), or PF (−3.1±3.5 vs 1.1±3.6, P=0.40). Depressive symptoms and self-reported mental health were assessed by the Beck Depression Inventory (BDI), and the mental health composite score and emotional subscale of the RAND 36-Item Health Survey were also assessed with the mental health composite score derived by summarizing the emotional, role emotional, energy/fatigue, and social functioning scales of the RAND 36-Item Health Survey. Mean BDI score showed a 1.6-unit greater decrease (95% CI: −4.9 to 1.7, P=0.3). There were no statistically significant changes between the groups for any of the other assessments of depressive symptoms or self-reported mental health at month 12. However, the signs for all comparisons were in the direction favoring the frequent NHD intervention, with trends generally showing magnitudes similar to those observed in the larger Daily Trial.
In summary, the effect of NHD on QOL is variable, depending on the population and assessment method used, with the associated limitations of each scale. Benefits in terms of QOL may be limited to certain kidney disease-specific QOL outcomes.
A summary of the studies is provided in Table 2.
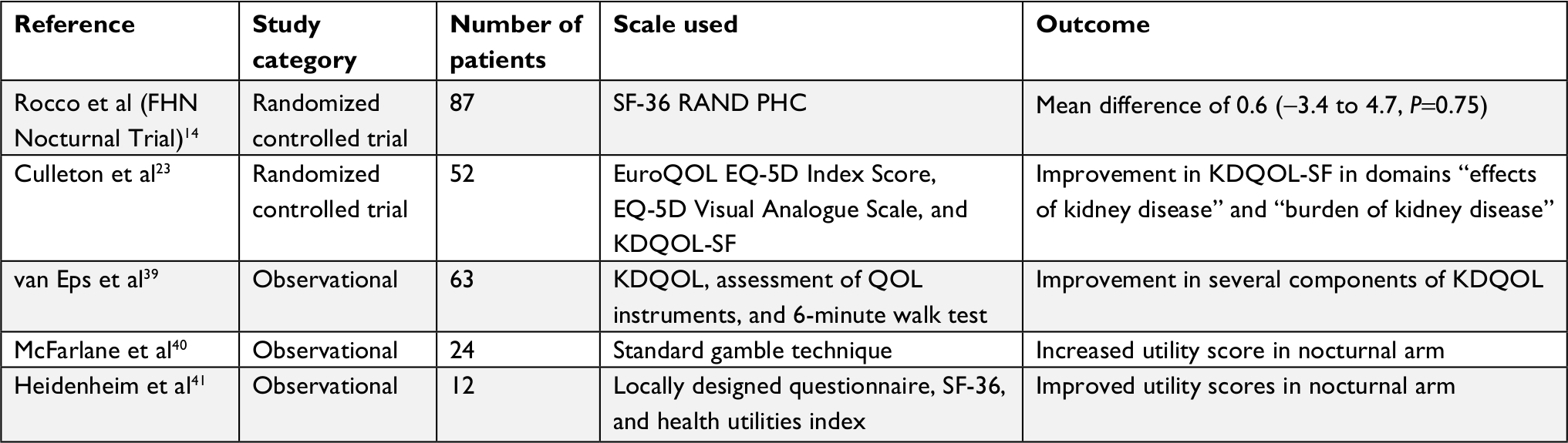 | Table 2 Summary of studies evaluating QOL outcomes in NHD Abbreviations: EQ-5D, EuroQoL EQ-5D; FHN, Frequent Hemodialysis Network; NHD, nocturnal hemodialysis; PHC, Physical Health Composite; KDQOL, Kidney Disease QOL; KDQOL-SF, Kidney Disease QOL-Short Form; QOL, quality of life; SF-36 RAND, RAND 36-item Short Form Survey. |
Phosphate and mineral metabolism
Disorders related to hyperphosphatemia, hypercalcemia, and hypo- or hyperparathyroidism are prevalent in CHD.44 Hyperphosphatemia and hypercalcemia are associated with increased vascular calcification, increased cardiovascular morbidity, and mortality.45 The beneficial effect of NHD on phosphate and mineral metabolism is a lot clearer and consistent.
In their study comparing the effect of NHD vs CHD on LV mass, the Alberta group also performed analysis on secondary outcomes relating to mineral metabolism.46 Serum phosphate, serum calcium, calcium–phosphate product, and intact parathyroid hormone (iPTH) levels were collected as part of the study protocol. Patients in the NHD group had a 1.1-mmol2/L2 decrease in the calcium–phosphate product compared to the CHD group (95% CI: 0.53–1.68 mmol2/L2, P<0.001). Serum phosphate decreased an average of 0.49 mmol/L (95% CI: 0.24–0.74, P<0.001) in the NHD group compared to the CHD group. These differences in serum phosphate developed within the first 2 months of the study and remained stable for the remainder of the study. In addition, the reduction in serum phosphate occurred despite a significant reduction in the use of phosphate binders. Twenty patients (77%) decreased or discontinued their calcium-based and/or sevelamer phosphate binder dose in the NHD group compared to only three (12%) in the CHD group (P<0.001). Of note, of the 23 patients that completed both baseline and exit dietary journals, phosphate intake was not different between the groups. With regard to iPTH levels, although the difference in median iPTH levels between the two groups was 99 mmol/L (P=0.05), analysis of iPTH levels using longitudinal models and adjusting for baseline values demonstrated no significant difference between the groups. The FHN Nocturnal Trial14 discussed earlier also demonstrated a reduction in serum phosphorus with NHD, with a treatment comparison of change between NHD and CHD of −1.4 (95% CI: −2.1 to −0.7, P<0.001).
NHD has also been shown to have benefits in improving both 25-hydroxy (25D) and 1,25D vitamin D levels. Nessim et al47 performed a longitudinal cohort study on 35 patients who were converted from CHD to frequent home NHD. Levels of 25D increased significantly from 26 (10.8–41.2) to 32 (6.4–57.6) ng/mL (P=0.009). 1,25D increased significantly from 7.32 (0.9–19.6) to 11.94 (0.02–23.9) pg/mL (P=0.004). Sun exposure did not differ significantly at baseline testing and subsequent testing. A significant correlation between dialysis dose and levels of both hydroxylated forms of vitamin D was found (r=−0.27, P=0.03 for 25D and r=0.28, P=0.02 for 1,25D). The authors concluded that improving uremia with NHD in the absence of exogenous supplementation was associated with increased 25D and 1,25D levels, with improved 1-alpha hydroxylation possibly by normalization of serum phosphorus levels.
In summary, the use of NHD may allow improved phosphate control, as well as a reduction in the need for use of phosphate binders in patients on hemodialysis. In fact, patients on frequent NHD may require phosphate supplementation in the dialysate to avoid hypophosphatemia. Improvements in vitamin D levels may also be achieved via more intensive NHD.
Sleep
Sleep is an essential function of the body and is crucial in the daily performance of a person. Sleep-disordered breathing, including sleep apnea, is common in patients with ESRD, with sleep apnea being ten times more common in hemodialysis than in the general population.48 Central and obstructive sleep apnea are believed to both occur in patients with ESRD on hemodialysis. Central sleep apnea is characterized by complete or partial cessation of airflow in the absence of upper airway obstruction, caused by cessation of the central respiratory drive. Obstructive sleep apnea is characterized by the repetitive collapse of the upper airway during sleep. These result in hypoxemia and disruption of sleep as well as increased sympathetic tone. Increased cardiovascular morbidity has been associated with sleep apnea, including an increased prevalence of atrial fibrillation and ventricular arrhythmias, LV hypertrophy, and congestive cardiac failure as well as an increase in mortality.49 In addition, sleep apnea may also result in daytime somnolence, affecting the QOL and function of the patient. Fluid overload and rostral fluid shifts (from the lower limbs) are believed to contribute to both forms of sleep apnea. The uremic milieu is also believed to contribute to altered chemo-responsiveness, affecting the respiratory drive.50
CHD has not been found to reduce the prevalence or severity of sleep apnea in patients with chronic kidney disease. NHD with its associated benefits in terms of fluid control and higher dialysis dose has been postulated to improve the severity of sleep apnea.
Hanly and Pierratos51 evaluated 14 patients on CHD, who switched to NHD for 8 hours during each six or seven nights a week. Polysomnography was compared from baseline on CHD to a repeat of 6–15 months later when they were on NHD (one night when they were undergoing NHD and on another night when they were not). The conversion from conventional to NHD was associated with a reduction in the frequency of apnea and hypopnea (95% CI: 25±25–8±8, P=0.03). This reduction occurred predominantly in seven patients with sleep apnea, in whom the frequency of episodes fell from 46±19–9±9 per hour (P=0.006). Of note, the apnea–hypopnea index (AHI) on nights when they were not undergoing NHD was greater than that of nights when they were undergoing NHD, but it remained lower than it had been when compared to the period they were on CHD (P=0.05). A systematic review and meta-analysis of the effects of conversion from CHD to NHD on sleep parameters were conducted by Li et al.52 The pooled results based on four studies (62 patients) showed that such a switch resulted in a significant reduction of the AHI (mean difference [MD] =−14.90, 95% CI: −20.12 to −9.68, I2=60.4%). In the subgroup analysis for the patients with sleep disorders, AHI decreased to a greater degree (MD =−20.01, 95% CI: −30.86 to −9.17, I2=71.1%). With regards to mean oxygen saturation (SaO2) during sleep, the two studies included in the meta-analysis showed a statistically significant increase after conversion to NHD (MD =1.38%, 95% CI: 0.35%–2.42%, I2=63.5%). In patients with sleep disorders, a larger improvement on SaO2 was observed, with an increase in off-dialysis SaO2 of 1.01% (95% CI: 0.11%–1.91%, I2=0.0%) and increase in the combined on–off dialysis SaO2 level of 1.68% (95% CI: 0.28%–3.09%, I2=62.9%).
In conclusion, conversion from conventional to NHD is associated with improvements in sleep apnea and AHI as well as improvements in SaO2 levels. This effect is more prominent in patients with sleep disorders, suggesting that this may be a therapeutic consideration in this group of patients.
Pregnancy
It is well recognized that fertility reduces in parallel with glomerular filtration rate.53 Among patients on hemodialysis, the incidence of pregnancy has been quoted to be between <1% and 7%.54 Menstrual irregularities, infertility, and sexual dysfunction are known to occur in ESRD. The lack of ovulation, lack of luteal hormone surge, and estradiol peak are absent in patients with kidney disease.55 In addition, the use of medication, anemia, fatigue, and depression may also contribute to a lack of libido. Even if conception should occur, maternal, and fetal mortality rates are elevated.56 Success in pregnancy in this group of patients seems to be dependent on an enhanced clearance of uremic solutes, and intensive hemodialysis has been shown to reduce the uremic milieu.
Barua et al57 retrospectively studied their cohort of five patients achieving a pregnancy and delivering a live infant while on NHD in Toronto, Canada from 2001 to 2006. All patients had previously been on CHD but failed to conceive during that time. While on NHD, these women became pregnant, with an intensification of dialysis dose after conception (from a weekly mean of 36±10–48±5, P<0.01). Mean pre-dialysis urea and mean arterial BP were kept within physiological limits. The mean gestational age of the cohort was 36.2±3 weeks, and the mean birth weight was 2,417.5±657 g. This cohort also had reduced maternal and fetal complications compared to historical controls.
The Toronto group subsequently compared pregnancy outcomes from 22 pregnancies in the Toronto Pregnancy and Kidney Disease Clinic and Registry (2000–2013) with outcomes from 70 pregnancies in the American Registry for Pregnancy in Dialysis Patients (1990–2011).58 The live birth rate in the Canadian cohort (86.4%) was significantly higher than the American cohort (61.4%, P=0.03). The median duration of pregnancy in the more intensely dialyzed Toronto cohort was 36 weeks (interquartile range 32–37) compared to 27 weeks (interquartile range 21–35) in the American cohort.
In summary, intensive hemodialysis is associated with an increased likelihood of conception, as well as improved maternal and fetal outcomes. NHD is a feasible means by which more intensive hemodialysis can be offered to this group of patients.
Anemia
NHD has also been associated with an improvement in anemia and improvement in erythropoietin (EPO) responsiveness, although this has not been consistently demonstrated. Using a prospective cohort design, Schwartz et al59 evaluated the effect of conversion from CHD to NHD in 63 patients. Postconversion, there was a significant improvement in hemoglobin (Hb) concentration from a baseline of 115±2 g/L to 122±2 g/L at 6 months and 124±2 g/L at 12 months (P=0.03). This occurred despite a reduction in EPO requirement from 10,400±1,400 to 8,500±1,300 U/week at 6 months and 7,600±1,100 U/week at 12 months (P=0.03). In contrast, the control group of patients on CHD demonstrated no change in either EPO requirement or Hb concentration. A higher proportion of patients on NHD also did not require the use of EPO (24% in NHD vs 9% in CHD, P=0.01). A similar observation was also noted in the Hong Kong group of 25 NHD patients when compared to 23 CHD patients.60 Hb concentration improved from a baseline of 9.37±1.39 g/dL to 11.34±2.41 g/dL at 24 months (P<0.001). EPO requirement decreased from 103.44±53.55 U/kg/week to 47.33±50.62 U/kg/week, P<0.001). At 24 months, Hb concentration increased by 1.98±2.74 g/dL in the NHD group, whereas it decreased by 0.20±2.32 g/dL in the CHD group (P=0.007). EPO requirement also decreased by 53.49±55.50 U/kg/week in the NHD group but increased by 16.22±50.01 U/kg/week in the CHD group (P<0.001). The London Daily/NHD Study group61 also noted an improvement in Hb concentration in the NHD cohort (n=12) at 18 months (11.94 g/dL vs 10.95 g/dL at baseline, P=0.047). In contrast however, there was no significant effect on either Hb concentration or EPO requirement in both the Culleton study23 and the FHN Nocturnal Trial.62 The London Daily/NHD Study noted an increased EPO dose requirement in the NHD group, although this was not statistically significant. These studies are limited by their small numbers, hence the effect of NHD on anemia is still inconclusive.
Risks
There have been certain risks associated with the performance of more intensive hemodialysis. The accelerated loss of residual renal function has been described in an analysis of the FHN Nocturnal Trial.63 In those assigned to frequent NHD, residual renal function as assessed by mean urine volume, mean urine creatinine clearance, and mean urine urea clearance were significantly lower at month 4 and mostly so at month 12 compared to controls. Possible mechanisms leading to this phenomenon include discontinuation of angiotensin-converting enzyme inhibitors as well as an increased inflammatory response due to an increased blood-to-circuit contact time.
An increase in access related events has also been described with more intensive hemodialysis. In the FHN Nocturnal Trial,14 there was a trend toward an increased rate of access complications in the nocturnal arm, mainly driven by a higher number of vascular access procedures. A total of 34 vascular events (17 failures and 17 access procedures) occurred in the frequent nocturnal arm, and 21 events (13 failures and 8 access procedures) in the conventional arm (P=0.01). A total of 51% of the patients in the frequent nocturnal arm and 36% of the patients in the conventional arm suffered a vascular access failure or underwent at least one vascular access procedure (time to first access event HR =1.88, 95% CI: 0.97–3.64, P=0.06).
Summary
NHD is an important means to increase the intensity of dialysis and is associated with many clinical benefits. Benefits in terms of reduction of LV mass, better BP control, phosphate and mineral metabolism, sleep apnea and sleep parameters, and pregnancy outcomes have been consistently demonstrated. NHD has also been associated with improvements in survival, anemia management, and QOL, although these benefits have not been as consistently demonstrated. There are certain drawbacks in terms of loss of residual renal function and access complications. This modality should be included as an option for patients who reach ESRD.
Disclosure
The author reports no conflicts of interest in this work.
References
Scribner BH, Buri R, Caner JE, Hegstrom R, Burnell JM. The treatment of chronic uremia by means of intermittent hemodialysis: a preliminary report. Trans Am Soc Artif Intern Organs. 1960;6:114–122. | ||
Editorial. New developments with artificial kidney. Br Med J. 1963;1(5347):1685–1686. | ||
Pierratos A, Ouwendyk M, Francoeur R, et al. Nocturnal hemodialysis: three-year experience. J Am Soc Nephrol. 1998;9(5):859–868. | ||
Lindsay RM, Suri RS, Moist LM, et al. International quotidian dialysis Registry: Annual Report 2010. Hemodial Int. 2011;15(1):15–22. | ||
Ranganathan D, John GT. Nocturnal hemodialysis. Indian J Nephrol. 2012;22(5):323–332. | ||
Saran R, Robinson B, Abbott KC, et al. US Renal Data System 2017 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2018;71(3S1):A7–S672. | ||
Argawal R, Light RP. Arterial stiffness and interdialytic weight gain influence ambulatory blood pressure patterns in hemodialysis patients. Am J Physiol Renal Physiol. 2008;294:F303–F308. | ||
Agarwal R. How can we prevent intradialytic hypotension? Curr Opin Nephrol Hypertens. 2012;21(6):593–599. | ||
Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G. Characteristics of sudden death in hemodialysis patients. Kidney Int. 2006;69(12):2268–2273. | ||
Kjellstrand CM, Evans RL, Petersen RJ, Shideman JR, von Hartitzsch B, Buselmeier TJ. The “unphysiology” of dialysis: a major cause of dialysis side effects? Hemodial Int. 2004;8(1):24–29. | ||
Lowrie EG, Laird NM, Parker TF, Sargent JA. Effect of the hemodialysis prescription of patient morbidity: report from the National Cooperative Dialysis study. N Engl J Med. 1981;305(20):1176–1181. | ||
Flythe JE, Kimmel SE, Brunelli SM. Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality. Kidney Int. 2011;79(2):250–257. | ||
Georgianos PI, Sarafidis PA, Sinha AD, Agarwal R. Adverse effects of conventional thrice-weekly hemodialysis: is it time to avoid 3-day interdialytic intervals? Am J Nephrol. 2015;41(4-5):400–408. | ||
Rocco MV, Lockridge RS, Beck GJ, et al. The effects of frequent nocturnal home hemodialysis: the frequent hemodialysis network nocturnal trial. Kidney Int. 2011;80(10):1080–1091. | ||
Pipkin M, Eggers PW, Larive B, et al. Recruitment and training for home hemodialysis: experience and lessons from the nocturnal dialysis trial. Clin J Am Soc Nephrol. 2010;5(9):1614–1620. | ||
Nesrallah GE, Lindsay RM, Cuerden MS, et al. Intensive hemodialysis associates with improved survival compared with conventional hemodialysis. J Am Soc Nephrol. 2012;23(4):696–705. | ||
Johansen KL, Zhang R, Huang Y, et al. Survival and hospitalization among patients using nocturnal and short daily compared to conventional hemodialysis: a USRDS study. Kidney Int. 2009;76(9):984–990. | ||
Lacson E, Xu J, Suri RS, et al. Survival with three-times Weekly in-center nocturnal versus conventional hemodialysis. J Am Soc Nephrol. 2012;23(4):687–695. | ||
Pauly RP, Gill JS, Rose CL, et al. Survival among nocturnal home haemodialysis patients compared to kidney transplant recipients. Nephrol Dial Transplant. 2009;24(9):2915–2919. | ||
Zumrutdal A. Determinants of cardiovascular risk in hemodialysis patients without significant comorbidities. In Carpi A, editor. Progress in Hemodialysis—From Emergent Biotechnology to Clinical Practice. London, UK: IntechOpen Limited. 2011:281–296. | ||
Harnett JD, Kent GM, Barre PE, Taylor R, Parfrey PS. Risk factors for the development of left ventricular hypertrophy in a prospectively followed cohort of dialysis patients. J Am Soc Nephrol. 1994;4(7):1486–1490. | ||
Chan CT, Floras JS, Miller JA, Richardson RM, Pierratos A. Regression of left ventricular hypertrophy after conversion to nocturnal hemodialysis. Kidney Int. 2002;61(6):2235–2239. | ||
Culleton BF, Walsh M, Klarenbach SW, et al. Effect of frequent nocturnal hemodialysis vs conventional hemodialysis on left ventricular mass and quality of life: a randomized controlled trial. JAMA. 2007;298(11):1291–1299. | ||
London GM, Pannier B, Guerin AP, et al. Alterations of left ventricular hypertrophy in and survival of patients receiving hemodialysis: follow-up of an interventional study. J Am Soc Nephrol. 2001;12(12):2759–2767. | ||
Friesen T, Jassal DS, Zhu M, et al. Cardiovascular remodeling during long-term nocturnal home hemodialysis. Clin Exp Nephrol. 2015;19(3):514–520. | ||
Chan CT, Greene T, Chertow GM, et al. Effects of frequent hemodialysis on ventricular volumes and left ventricular remodeling. Clin J Am Soc Nephrol. 2013;8(12):2106–2116. | ||
Wald R, Yan AT, Perl J, et al. Regression of left ventricular mass following conversion from conventional hemodialysis to thrice Weekly in-centre nocturnal hemodialysis. BMC Nephrol. 2012;13(1):3. | ||
Tk L, Wald R, Goldstein M. Left atrial remodeling assessed by cardiac MRI after conversion from conventional hemodialysis to In-center nocturnal hemodialysis. J Nephrol. 2018;24:1–9. | ||
Ok E, Duman S, Asci G, et al. Long Dialysis Study Group. Comparison of 4- and 8-h dialysis sessions in thrice-weekly in-centre haemodialysis: a prospective, case-controlled study. Nephrol Dial Transplant. 2011;26(4):1287–1296. | ||
Mcintyre CW, Burton JO, Selby NM, et al. Hemodialysis-induced cardiac dysfunction is associated with an acute reduction in global and segmental myocardial blood flow. Clin J Am Soc Nephrol. 2008;3(1):19–26. | ||
Burton JO, Jefferies HJ, Selby NM, Mcintyre CW. Hemodialysis-induced cardiac injury: determinants and associated outcomes. Clin J Am Soc Nephrol. 2009;4(5):914–920. | ||
Jefferies HJ, Virk B, Schiller B, Moran J, Mcintyre CW. Frequent hemodialysis schedules are associated with reduced levels of dialysis-induced cardiac injury (myocardial stunning). Clin J Am Soc Nephrol. 2011;6(6):1326–1332. | ||
Bergman A, Fenton SS, Richardson RM, Chan CT. Reduction in cardiovascular related hospitalization with nocturnal home hemodialysis. Clin Nephrol. 2008;69(1):33–39. | ||
Chan CT, Harvey PJ, Picton P, Pierratos A, Miller JA, Floras JS. Short-term blood pressure, noradrenergic, and vascular effects of nocturnal home hemodialysis. Hypertension. 2003;42(5):925–931. | ||
Chan CT, Shen XS, Picton P, Floras J. Nocturnal home hemodialysis improves baroreflex effectiveness index of end-stage renal disease patients. J Hypertens. 2008;26(9):1795–1800. | ||
Casino FG, Lopez T. The equivalent renal urea clearance: a new parameter to assess dialysis dose. Nephrol Dial Transplant. 1996;11(8):1574–1581. | ||
Jhamb M, Weisbord SD, Steel JL, Unruh M. Fatigue in patients receiving maintenance dialysis: a review of definitions, measures, and contributing factors. Am J Kidney Dis. 2008;52(2):353–365. | ||
Chiu YW, Teitelbaum I, Misra M, de Leon EM, Adzize T, Mehrotra R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin J Am Soc Nephrol. 2009;4(6):1089–1096. | ||
van Eps CL, Jeffries JK, Johnson DW, et al. Quality of life and alternate nightly nocturnal home hemodialysis. Hemodial Int. 2010;14(1):29–38. | ||
Mcfarlane PA, Bayoumi AM, Pierratos A, Redelmeier DA. The quality of life and cost utility of home nocturnal and conventional in-center hemodialysis. Kidney Int. 2003;64(3):1004–1011. | ||
Heidenheim AP, Muirhead N, Moist L, Lindsay RM. Patient quality of life on quotidian hemodialysis. Am J Kidney Dis. 2003;42(1 Suppl):36–41. | ||
Hall YN, Larive B, Painter P, et al. Effects of six versus three times per week hemodialysis on physical performance, health, and functioning: frequent hemodialysis network (FHN) randomized trials. Clin J Am Soc Nephrol. 2012;7(5):782–794. | ||
Unruh ML, Larive B, Chertow GM, et al. Effects of 6-times-weekly versus 3-times-weekly hemodialysis on depressive symptoms and self-reported mental health: frequent hemodialysis network (FHN) trials. Am J Kidney Dis. 2013;61(5):748–758. | ||
Block GA, Hulbert-Shearon TE, Levin NW, Port FK. Association of serum phosphorus and calcium X phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis. 1998;31(4):607–617. | ||
Ganesh SK, Stack AG, Levin NW, Hulbert-Shearon T, Port FK. Association of elevated serum PO4 product, and parathyroid hormone with cardiac mortality risk in chronic hemodialysis patients. J Am Soc Nephrol. 2001;12(10):2131–2138. | ||
Walsh M, Manns BJ, Klarenbach S, Tonelli M, Hemmelgarn B, Culleton B. The effects of nocturnal compared with conventional hemodialysis on mineral metabolism: a randomized-controlled trial. Hemodial Int. 2010;14(2):174–181. | ||
Nessim SJ, Jassal SV, Fung SV, Chan CT. Conversion from conventional to nocturnal hemodialysis improves vitamin D levels. Kidney Int. 2007;71(11):1172–1176. | ||
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–1235. | ||
Findley LJ, Zwillich CW, Ancoli-Israel S, Kripke D, Tisi G, Moser KM. Cheyne-Stokes breathing during sleep in patients with left ventricular heart failure. South Med J. 1985;78(1):11–15. | ||
Lyons OD, Bradley TD, Chan CT. Hypervolemia and sleep apnea in kidney disease. Semin Nephrol. 2015;35(4):373–382. | ||
Hanly PJ, Pierratos A. Improvement of sleep apnea in patients with chronic renal failure who undergo nocturnal hemodialysis. N Engl J Med. 2001;344(2):102–107. | ||
Li L, Tang X, Kim S, Zhang Y, Li Y, Fu P. Effect of nocturnal hemodialysis on sleep parameters in patients with end-stage renal disease: a systematic review and meta-analysis. PLoS One. 2018;13(9):e0203710. | ||
Holley JL, Schmidt RJ, Bender FH, Dumler F, Schiff M. Gynecologic and reproductive issues in women on dialysis. Am J Kidney Dis. 1997;29(5):685–690. | ||
Hladunewich M, Engel Hercz AA, Keunen J, et al. Pregnancy in end-stage kidney disease. Semin Dial. 2011;24(6):634–639. | ||
Tangren J, Nadel M, Hladunewich MA. Pregnancy and end-stage renal disease. Blood Purif. 2018;45(1-3):194–200. | ||
Nevis IF, Reitsma A, Dominic A, et al. Pregnancy outcomes in women with chronic kidney disease: a systematic review. Clin J Am Soc Nephrol. 2011;6(11):2587–2598. | ||
Barua M, Hladunewich M, Keunen J, et al. Successful pregnancies on nocturnal home hemodialysis. Clin J Am Soc Nephrol. 2008;3(2):392–396. | ||
Hladunewich MA, Hou S, Odutayo A, et al. Intensive hemodialysis associates with improved pregnancy outcomes: a Canadian and United States cohort comparison. J Am Soc Nephrol. 2014;25(5):1103–1109. | ||
Schwartz DI, Pierratos A, Richardson RMA, Fenton SSA, Chan CT. Impact of nocturnal home hemodialysis on anemia management in patients with end-stage renal disease. Clin Nephrol. 2005;63(03):202–208. | ||
Poon CK, Tang HL, Wong JH, et al. Effect of alternate night nocturnal home hemodialysis on anemia control in patients with end-stage renal disease. Hemodial Int. 2015;19(2):235–241. | ||
Rao M, Muirhead N, Klarenbach S, Moist L, Lindsay RM. Management of anemia with quotidian hemodialysis. Am J Kidney Dis. 2003;42(1 Suppl):18–23. | ||
Ornt DB, Larive B, Rastogi A, et al. Impact of frequent hemodialysis on anemia management: results from the frequent hemodialysis network (FHN) trials. Nephrol Dial Transplant. 2013;28(7):1888–1898. | ||
Daugirdas JT, Greene T, Rocco mV. Frequent nocturnal hemodialysis accelerates the decline of residual renal function. Kidney Int. 2013;83(5):949–958. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.