")
Back to Journals » Research and Reports in Urology » Volume 12
No Relationship Between the International Prostate Symptom Score and Post-Void Residual Volume in Primary Care
Authors Lammers HA , Teunissen TAM , Bor H, Smid IS , Lagro-Janssen ALM
Received 19 December 2019
Accepted for publication 17 February 2020
Published 5 May 2020 Volume 2020:12 Pages 167—174
DOI https://doi.org/10.2147/RRU.S241961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
HA Lammers, TAM Teunissen, H Bor, IS Smid, ALM Lagro-Janssen
Radboudumc, Department of Primary and Community Care/Gender & Women’s Health, Nijmegen, the Netherlands
Correspondence: HA Lammers
Radboudumc, Huispost 117, Postbus 9101, Nijmegen 6500 HB, the Netherlands
Tel +316 52378946
Email [email protected]
Background: Lower urinary tract symptom (LUTS) is a common condition in older men. In accordance with the Dutch College of General Practitioners Guideline “Micturition symptoms in men”, the diagnosis can be made based on a patient’s medical history and a physical examination. GPs lack additional tools in primary care to assess the residual urine volume. A residual volume usually requires a referral to a urologist. We hypothesized that the IPSS screening questionnaire score (measuring the severity of symptoms) might be related to patients’ residual urine volume. The research objective was to examine the relation between the IPSS score and the residual urine volume.
Methods: In a cross-sectional study, we analysed patients’ IPSS and residual urine volume. Men aged over 50 with LUTS who consulted Dutch primary-care physicians were included. The interventions comprised an IPSS screening and a bladder scan. Data regarding the patients’ residual volume, total IPSS score, single IPSS score, IPSS storage score, and IPSS voiding score were recorded and analysed. We used odds ratios to describe the relation between the IPSS categories associated with the presence of a normal or abnormal (above 100 cc and above 200 cc) residual urine volume.
Results: A total of 126 patients were included in this study. Patients with higher scores on the overall IPSS, separate IPSS, IPSS storage and IPSS voiding showed no higher odds ratios of having an abnormal residual volume, neither above 100 mL or 200 mL.
Conclusion: We did not find a relation between the IPSS core to an abnormal residual urine volume in men aged over 50 with LUTS consulting primary-care physicians.
Trial Registration: This study has been approved by the Central Committee on Research Involving Human Subjects for the Arnhem-Nijmegen Region and is registered with ToetsingOnline under ID number 29822.091.10.
Keywords: lower urinary tract symptoms, primary care, international prostate symptom score, post-void residual volume
Background
Lower urinary tract symptom (LUTS) is the collective term for a large number of urinary problems.1 Previously, these symptoms were referred to as prostatism, but the current opinion is that the relationship between prostate enlargement, obstruction and voiding symptoms is not unambiguous. Prostate enlargement does not necessarily lead to obstruction and/or discomfort. The micturition problems are not specific to prostate enlargement and the symptoms may also be caused by other conditions, such as pelvic floor changes, a restriction elsewhere in the urethra or bladder overactivity.2 In recent decades, urinary symptoms have been considered multifactorial.3
LUTS is categorised into two groups: storage (or irritative) symptoms and voiding (or obstructive) symptoms.4 The symptoms of frequency, urgency, urge incontinence and nocturia belong to storage symptoms. Straining, a poor and/or intermittent stream, prolonged micturition, a feeling of incomplete bladder emptying and dribbling belong to voiding symptoms.4 Lower urinary tract symptoms are a common health issue in ageing men, due to a changing urological system. Several studies show that between 20% and 30% of men over the age of 50 have moderate to severe symptoms.1,6,7 About one third of men with LUTS experience spontaneous improvement, one third notice no changes and one third experience an increase of symptoms.5 Age-specific changes include increased or decreased bladder elasticity and prostate size, or changes in the pelvic floor muscles.
The percentage visiting a general practitioner (GP) varies from 17% of men with mild symptoms to 70% of men with severe symptoms.6–8 Voiding symptoms are usually accepted as part of the ageing process. Many seek professional help only when their inconvenience has risen to an unacceptable level.9,10 Additional symptoms, such as pain during micturition, or the fear of prostate and other cancers, can reinforce the burden of inconvenience caused by the voiding symptoms. LUTS can considerably reduce a man’s quality of life.1,12,13
According to the Dutch guideline for GPs entitled “Micturition symptoms in men”, diagnostics by a GP should be limited to history-taking and performing a physical examination including a rectal examination.5 The diagnostic process in patients with LUTS is aimed at excluding causes of specific pathology. If an abnormal post-void residual volume is suspected, further investigation by a urologist is required. An abnormal residue may indicate chronic infections, hydronephrosis and urinary retention by bladder contraction disorders.2 For several indications, about 30% of the patients with LUTS in the Netherlands are referred to the urologist.13
Investigation into validity and reliability shows that the International Prostate Symptom Score (IPSS) is useful for estimating the severity of symptoms.14 The IPSS is designed to be self-administered by patients, with speed and ease in mind, and can be used in both secondary care and primary care.
In the last few decades, the treatment of LUTS underwent major transformations. Surgery can now often be replaced by medication, which places the treatment of LUTS into the domain of primary care.12 In addition, it is preferable that patients are managed by their GPs, who provide continuity of care.15 For this reason, it is important to have tools in primary care that can properly assess the post-void residual volume, so as not to miss the presence of a residue in patients, which is reason to refer to secondary care.
Several studies in secondary care show a statistically significant relation between the IPSS score and residual volume. Unfortunately, the correlation is too weak to be useful in practice.1,16,17 Because it is mainly patients with severe symptoms who consult a urologist, this relation does not automatically apply the population in primary care. The relation between the IPSS score and residual volume has not previously been studied in primary care. In addition, it is especially important to establish whether an IPSS score can differentiate between a normal and an abnormal residue. To this end, our research questions are: What is the relation between the IPSS score for the presence of an abnormal residue in men over 50 years with LUTS in primary care? And does this value differ per age category?
Methods
Study Design
This study is a cross-sectional study and part of the “LUTS/BPH in primary care, a new approach” randomised controlled trial (RCT). Inclusion of participants took place between 1 October 2010 and 1 October 2017. All participants gave written informed consent. This study has been approved by the Central Committee on Research Involving Human Subjects for the Arnhem-Nijmegen Region and is registered with ToetsingOnline under ID number 29822.091.10.
Study Design
The original research population comprised all 24,000 patients listed in five healthcare centres in a city located in the middle of the Netherlands. All men aged over 50 who consulted their GP for the first time because of LUTS were asked to participate. LUTS is defined as described by the NHG guideline “Micturition symptoms in men”.4 Exclusion criteria were the use of an α-blocker or 5α-reductase inhibitor, transurethral resection of the prostate (TURP) in patients’ history, prostate cancer or suspected prostate cancer by abnormal digital rectal examination or other urological diseases, haematuria and urinary tract infection.
In the original study, 486 patients were included for participation in the RCT. Of all patients, 133 were excluded (Figure 1). Patients (n=353) were randomised at GP level to an intervention group or a control group.
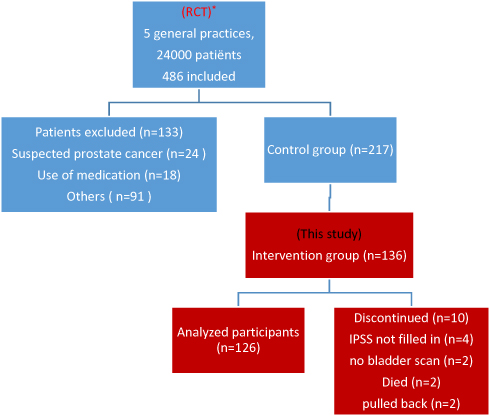 |
Figure 1 Study participants flow chart. *The study population of this study is part of a RCT. |
Study Participants
The present study population comprised 136 patients focussing only on the intervention group, given that we were interested in the relation between the IPSS-score and the bladders scan, as they were part of the intervention (Figure 1). Interventions were the IPSS questionnaire, including a quality-of-life question, and the bladder scan. The IPSS was filled in directly after the first visit. The bladder scan was performed within a week after the first visit by a trained GP (HL). Test results were interpreted by the same trained GP researcher (HL).
Measurements
Bladder Scan
The bladder scan used for this study is the BVI9400 bladder scan. This scan is a portable 3D ultrasound device that quickly, accurately and noninvasively measures urinary bladder volume and post-void residual volume. Based on these data, the bladder scan calculates and displays the bladder volume. Results are displayed as a number (in mL).
The investigation of all patients took place under similar circumstances. Patients had to wait until they had the urge to urinate. After urination, they were asked about representativeness of the micturition. Only in case of representativeness, a bladder scan was carried out representative a bladder scan was carried out.
We defined residue as the volume of urine remaining in the bladder after the completion of micturition. In the literature, two cut-off points are used to distinguish abnormal residue from normal residue: 100 mL18–20 and 200 mL.15,21 According to the EAU guideline,11 no residue threshold for treatment has yet been established, so this study will use both cut-off points (100 and 200 mL).
International Prostate Symptom Score (IPSS)
The IPSS measures the severity of LUTS. This questionnaire is based on the American Urological Association (AUA) symptom index.14 The AUA concluded that the test is clinically sensible, reliable, valid and responsive. As a result, the NHG guideline recommends using this test in primary care. The questionnaire consists of seven questions, covering incomplete emptying, increased frequency, intermittency, urgency, weak stream, straining and nocturia. Every individual question can be answered on a ranking scale from 0 (never) to 5 (almost always). The total IPSS score can be classified, according to the classification of the AUA, into three categories: mild (1–7 points), moderate (8–19 points) and severe (20–35 points).
Separate IPSS questions can be classified into two categories: IPSS storage and IPSS voiding. IPSS storage comprises the combination of the symptoms of increased frequency, urgency and nocturia (questions 2, 4 and 7).1 Symptoms of incomplete emptying, intermittency, weak stream and straining form the combination for IPSS voiding (questions 1, 3, 5 and 6).1
Statistical Analyses
We used the IPSS questionnaire as an independent variable and the bladder scan as a dependent variable. Participants with one or more missing answers on the IPSS were left out of the analysis of the total IPSS score. Patients’ age was divided into three categories: 50–59 years, 60–69 years and 70 years and over. Data were collected in SPSS24.0. We used descriptive statistics to describe the study population. One-way ANOVA tests and Pearson’s chi-squared tests were used to investigate differences in symptoms between age categories.
The relationships between the IPSS scores and the post-void residual volume were evaluated using binary logistic regression, with the IPSS in categories and the normal/abnormal residue as a dependent variable. No patients with a mild IPSS score had a residue >200 mL. As a result, no odds ratios could be calculated for the total IPSS score. Instead of the binary logistic regression, we analysed the total IPSS score using the exact chi-squared test.
For the separate IPSS questions, we used the categories rarely (score 0–1), sometimes (score 2–3) and often (score 4–5). For the IPSS storage, we used the categories mild (score 0–5), moderate (score 6–10) and severe (score 11–15) and for the IPSS voiding mild (score 0–6), moderate (score 7–13) and severe (score 14–20). In order to investigate whether the relationship differed per age category, we added the interaction for age categories. We analysed both the 100 mL cut-off point and the 200 mL cut-off point. The level of statistical significance was set at p=0.05 (two-tailed).
Results
Background
After randomisation, 136 patients were included in the intervention group and the population of this study. Ten patients dropped out, two patients died during the study period, four because the IPSS was not filled in, two because no bladder scan was made and two patients pulled back.
The mean age of the patients was 64.8 (±SD 7.2) years, ranging between 50 and 85 years (Table 1). Total IPSS scores ranged between 3 and 33, with a mean score of 16.5 (±6.8). The majority of patients experienced moderate symptoms. A weak stream was the question on which most participants mentioned “almost always occur”. An abnormal residue (residue >100 mL) was measured in 27% of the cases (N=34), of which 44% were above 200 mL (N=15). Differences in the frequency of symptoms were not significant between the age categories. No significant differences were present in the IPSS scores between the three age categories of 50–59 years, 60–69 years and 70 years and older. In addition, the post-void residual volume also did not differ significantly between these age categories.
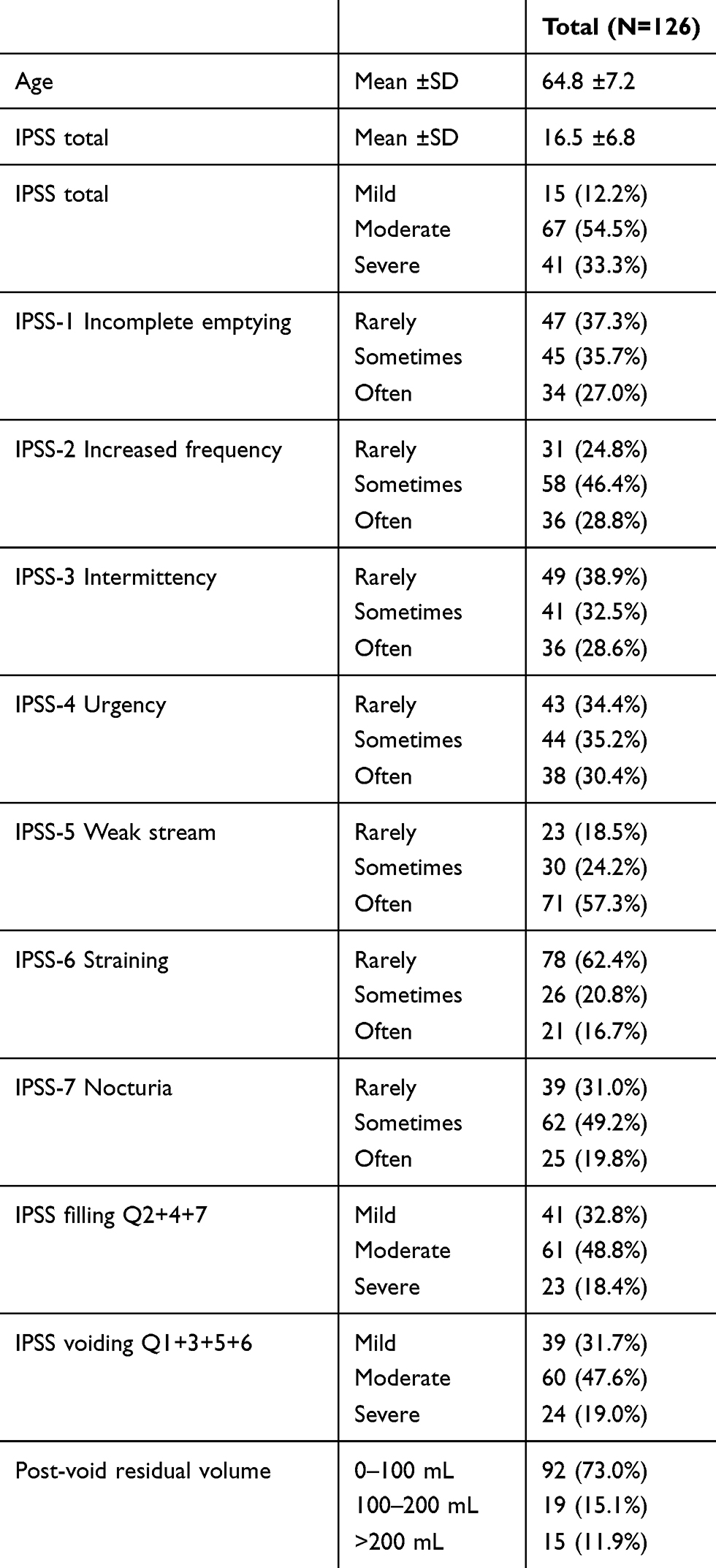 |
Table 1 Characteristics of Study Population |
Relation of IPSS Score and Post-Void Residual Volume
100 ML Cut-off Point
There was no significant difference between the amount of patients with a residue >100 mL and a mild total IPSS score compared to the amount of patients with a residue >100 mL and a moderate total IPSS score (Table 2). This was neither the case between the number of patients with a residue >100 mL in and a mild total IPSS score compared to the number of patients with a residue >100 mL and a severe total IPSS score.
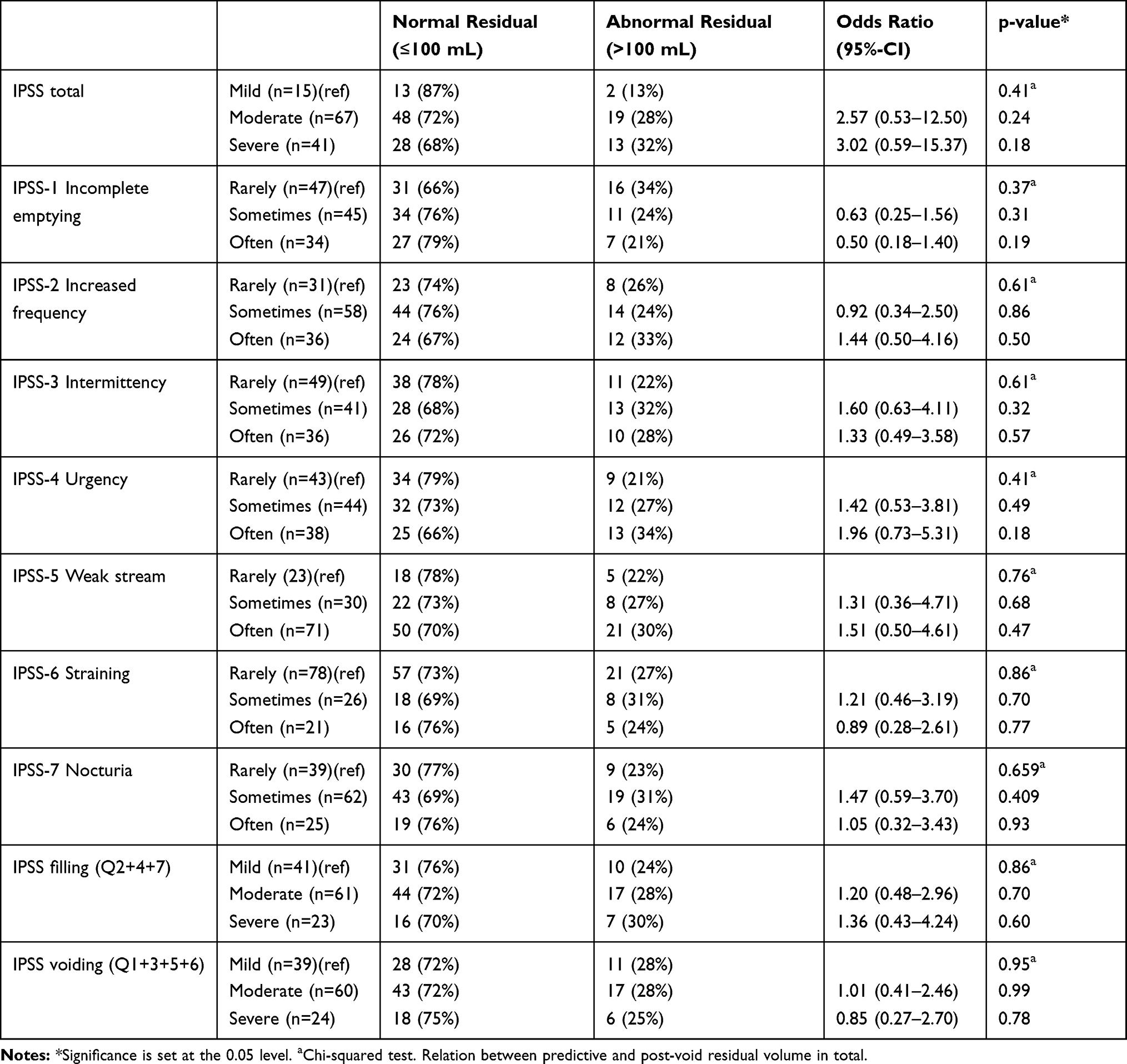 |
Table 2 Relation IPSS with Post-Void Residual Volume, Cut-off Point 100 Ml |
In addition, for all seven separate IPSS questions we did not find a significant difference between the number of patients with a residue >100 mL and a mild IPSS score on a question compared to the number of patients with a residue >100 mL and a moderate score. Nor did we find a significant difference between having a residue >100 mL and a moderate score on a question compared to a severe score.
Lastly, for the subgroups IPSS filling and IPSS voiding, we also did not find a significant difference between the number of patients with a residue >100 mL and a mild score, and the subgroup and patients with a residue >100 mL and a moderate score on the subgroup. Nor did we find a significant difference between a mild subgroup score compared with severe. All these findings also did not differ between the different age groups.
200 ML Cut-off Point
For a residue >200 mL, we also did not find a significant difference between a mild vs moderate total IPSS score and moderate vs severe total IPSS score and the number of patients with a residue (Table 3). Neither did we find this for the seven separate IPSS questions and the categories storage and voiding. For a residue >200 mL these findings also did not differ between the different age groups.
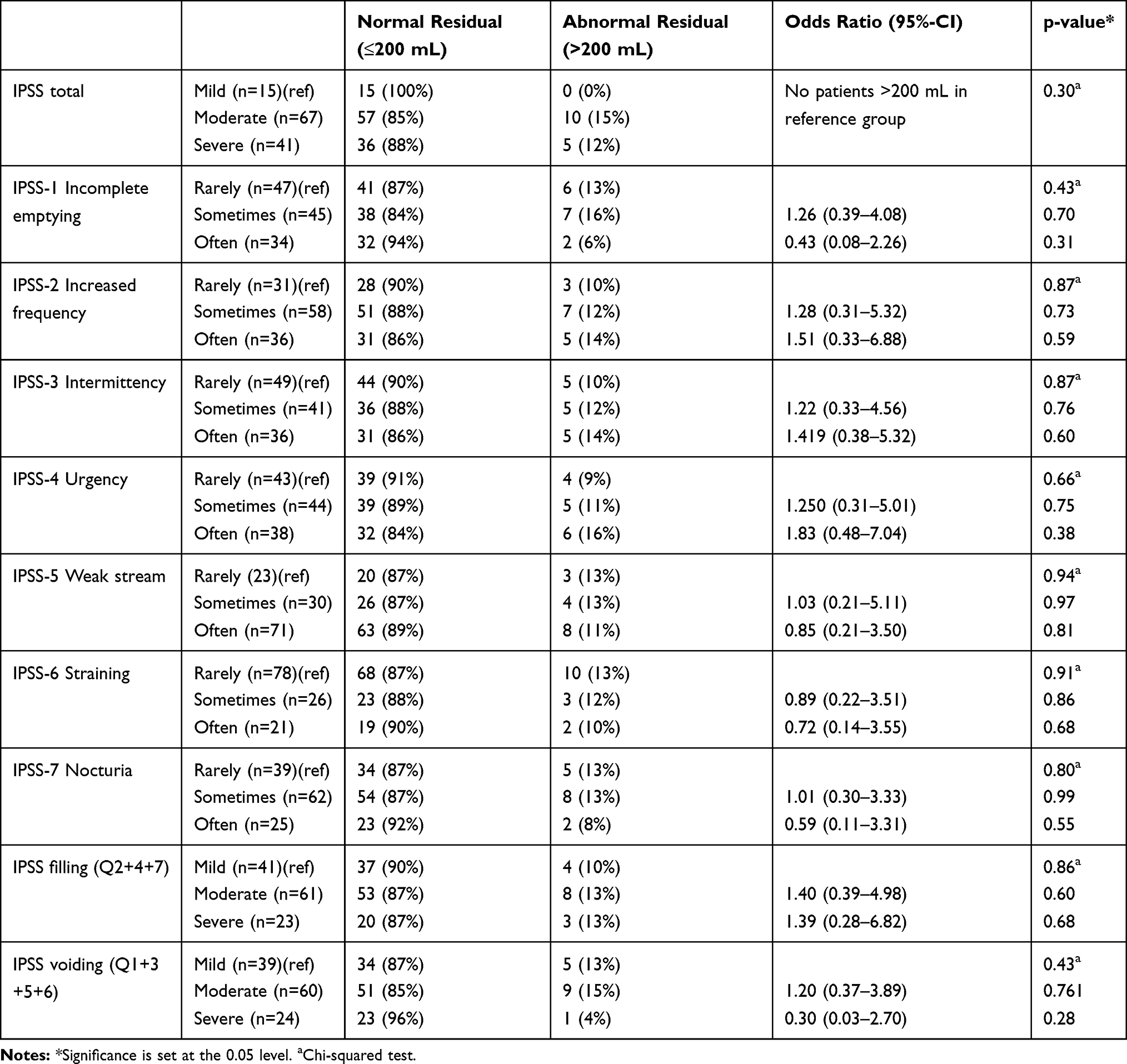 |
Table 3 Relation IPSS with Post-Void Residual Volume, Cut-off Point 200 Ml |
Discussion
We did not find a relation between a high total IPSS score and the presence of an abnormal residue for either the 100 mL cut-off point or the 200 mL cut-off point. We also did not find this between a high score on one of the seven separate IPSS question or a high score on the categories IPSS storage or IPSS voiding and the presence of a residue of 100 or 200 mL. The same applied within the different age groups.
Previous studies evaluating the relationship between the IPSS and the residue demonstrated inconsistent results. A few studies showed a correlation between the IPSS (or IPSS categories) and the residue.1,16,17,22 However, there were also some studies that did not find a correlation.23 In our study, we were unable to show a significant correlation between these variables. A possible reason for this discrepancy is that most studies involved community-based or hospital-based research, while we investigated patients in primary care. However, even though a correlation was found in some studies conducted in secondary care, the correlation was too weak to be useful in practice.
Our findings suggest that the IPPS is not a sensitive instrument for determining whether a residue is abnormal and does not have a predictive value for the residue measured by a bladder scan. Therefore, making a proper diagnosis of an abnormal residue by symptomatic assessment involving only the IPSS is not possible. As the symptom score is an easy and reliable method to assess the severity of symptoms, we recommend using the IPSS scale only to achieve insight into the severity of LUTS symptoms in primary care.
A strength of our study is that to our knowledge this is the first study that investigates the relationship between the IPSS scale and post-void residual volume in men with LUTS in primary care. There was limited selection bias because patients participating in the study came from different GPs and all men with LUTS were included, regardless of cofactors such as the severity of symptoms or comorbidity. Nevertheless, we must be cautious with any generalisations. We performed a single measurement using a bladder scan, which limited the validity. We recommend a second measurement considering the substantial within-patient variability. Since this study is a part of a RCT we did not perform a separate power or sample size calculation. This might have an effect on the statistical analysis.
Conclusion
A higher score on the total IPSS, separate IPSS scores, IPSS storage and IPSS voiding seems not to be related to an abnormal residue. More research have to be done in primary care on factors that are related to a residual volume.
Data Sharing Statement
The data that support the findings of the study are available from the corresponding author upon reasonable request.
Ethics and Consent Statement
This study has been approved by the Central Committee on Research Involving Human Subjects for the Arnhem-Nijmegen Region and is registered with ToetsingOnline under ID number 29822.091.10. This study is conducted in accordance with the Declaration of Helsinki.
Author Contributions
HA Lammers and ALM Lagro-Janssen designed the protocol. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
We received a contribution by Agis Health Insurance (now Zilveren Kruis Achmea).
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Institute for Health and Care Excellence. Clinical guideline(CG97). Lower Urinary Tract Symptoms in Men: Management. June 2015.
2. NVU: Richtlijn diagnostiek en behandeling van LUTS-BPH (Dutch Association of Urology: guideline for diagnostics and treatment of LUTS-BPH). 2006.
3. Chapple CR, Wein AJ, Abrams P, et al. Lower urinary tract symptoms revisited: a broader clinical perspective. Eur Urol. 2008;54(3):563–569. doi:10.1016/j.eururo.2008.03.109
4. Lepor H. Pathophysiology of lower urinary tract symptoms in the aging male population. J Urol. 2005;7:S3–S11.
5. Blanker MH, Breed SA, van der Heide WK, et al. NHG-standaard Mictieklachten bij mannen (Dutch College of general practitioners-guideline: micturition symptoms in men). Huisarts Wet. 2013;56:114–122.
6. Bosch JL, Hop WC, Kirkels WJ, Schroder FH. The international prostate symptom score in a community-based sample of men between 55 and 74 years of age: prevalence and correlation of symptoms with age, prostate volume, flow rate and residual urine volume. Br J Urol. 1995;75(5):622–630. doi:10.1111/bju.1995.75.issue-5
7. Wolfs GG, Knottnerus JA, Janknegt RA. Prevalence and detection of micturition problems among 2734 elderly men. J Urol. 1994;152:1467–1470. doi:10.1016/S0022-5347(17)32447-3
8. Wolters R, Wensing M, van Weel C, van der Wilt GJ, Grol RP. Lower urinary tract symptoms: social influence is more important than symptoms in seeking medical care. BJU Int. 2002;90(7):655–661. doi:10.1046/j.1464-410X.2002.02996.x
9. Shim SR, Kim JH, Kim KH, et al. Association between the self-perception period of lower urinary tract symptoms and the international prostate symptom score. Urol Int. 2012;88(4):431–437. doi:10.1159/000334913
10. Ward J, Sladden M. Urinary symptoms in older men, their investigation and management: is there an epidemic of undetected morbidity in the waiting room? Fam Pract. 1994;11(3):251–259. doi:10.1093/fampra/11.3.251
11. Gratzke C, Bachmann A, Descazeaud A, et al. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67(6):1099–1109. doi:10.1016/j.eururo.2014.12.038
12. Rosenberg MT, Staskin DR, Kaplan SA, MacDiarmid SA, Newman DK, Ohl DA. A practical guide to the evaluation and treatment of male lower urinary tract symptoms in the primary care setting. Int J Clin Pract. 2007;61(9):1535–1546. doi:10.1111/ijcp.2007.61.issue-9
13. Dijsterbloem DALA, Schouten MA, Lagro-Janssen ALM. Benigne prostaathypertrofie in 4 huisartsenpraktijken. Voorkomen, beleid en beloop. (Benign prostatic hyperplasia in four general practices. Prevalence, policy and course). Huisarts Wet. 2003;46(3):133–137.
14. Barry MJ, Fowler FJ
15. Szeto PS. Application of the Chinese version of the international prostate symptom score for the management of lower urinary tract symptoms in a primary health care setting. Hong Kong Med J. 2008;14(6):458–464.
16. Ezz el Din K, Kiemeney LA, de Wildt MJ, Debruyne FM, de la Rosette JJ. Correlation between uroflowmetry, prostate volume, postvoid residue, and lower urinary tract symptoms as measured by the international prostate symptom score. J Urol. 1996;48(3):393–397. doi:10.1016/S0090-4295(96)00206-3
17. Singla S, Garg R, Singla A, Sharma S, Singh J, Sethi P. Experience with uroflowmetry in evaluation of lower urinary tract symptoms in patients with benign prostatic hyperplasia. J Clin Diagn Res. 2014;8(4):Nc01–Nc03. doi:10.7860/JCDR/2014/7909.4271
18. Kelly CE. Evaluation of voiding dysfunction and measurement of bladder volume. Rev Urol. 2004;6(Suppl 1):S32–S37.
19. Chapple CR, Tubaro A. Male LUTS/BPH Made Easy. London: Springer-Verlag; 2014.
20. Ouslander JG, Wood AJJ. Management of overactive bladder. N Engl J Med. 2004;350(8):786–799. doi:10.1056/NEJMra032662
21. Park HJ, Won JEJ, Sorsaburu S, Rivera PD, Lee SW. Urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) and LUTS/BPH with erectile dysfunction in Asian men: a systematic review. World J Men's Health. 2013;31(3):193–207. doi:10.5534/wjmh.2013.31.3.193
22. Wang JY, Liu M, Zhang YG, et al. Relationship between lower urinary tract symptoms and objective measures of benign prostatic hyperplasia: a Chinese survey. Chin Med J (Engl). 2008;121(20):2042–2045. doi:10.1097/00029330-200810020-00018
23. Tubaro A, Vecchia C. The relation of lower urinary tract symptoms with life-style factors and objective measures of benign prostatic enlargement and obstruction: an Italian survey. Eur Urol. 2004;45:767–772. doi:10.1016/j.eururo.2004.01.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.