")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Newborn Birth Weight and Associated Factors Among Mother-Neonate Pairs in Public Hospitals, North Wollo, Ethiopia
Authors Wubetu AD , Amare YE , Haile AB , Degu MW
Received 25 December 2020
Accepted for publication 1 March 2021
Published 9 March 2021 Volume 2021:12 Pages 111—118
DOI https://doi.org/10.2147/PHMT.S299202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Abate Dargie Wubetu,1 Yosef Eshetie Amare,2 Assalif Beyene Haile,3 Melkam Wagaye Degu4
1Debre Berhan University, College of Health Science, Department of Psychiatry, Debre Berhan, Ethiopia; 2Debre Berhan University, College of Health Science, Department of Medical Physiology, Debre Berhan, Ethiopia; 3Debre Berhan University, College of Health Science, Department of Midwifery, Debre Berhan, Ethiopia; 4North Wollo Zone, Raya Kobo Municipality, Robbit, Ethiopia
Correspondence: Abate Dargie Wubetu Email [email protected]
Background: Birth weight or size at birth is an important indicator of the child’s vulnerability to the risk of childhood illnesses and diseases. Low birth weight is closely associated with fetal and neonatal morbidity, inhibited growth and cognitive development, and chronic diseases in life. The study was aimed to assess the birth weight of neonates and associated factors among mothers who gave birth at a public hospital in North Wollo, 2020.
Methods: A hospital-based cross-sectional study was conducted among 337 mothers who gave birth in public hospitals of North Wollo, Ethiopia from January 1st to June 30, 2020. A systematic sampling technique was used to reach the study participants. Data were entered using Epi data 3.1 software and analysis will be done using SPSS 20. Adjusted beta coefficient with 95% confidence interval and p-value ≤ 0.05 was used to declare statistical significance.
Results: A total of 337 mothers were included with a response rate of 100%. The mean ± SD weight of the child was 2.94 ± 0.65 kilograms. The prevalence of low birth weight was 24% (95% CI= 19.6, 28.8). Maternal nutritional factors correlate with newborn weight. Age of the mother, family average monthly income, being single, alcohol use, education, female sex, had no abortion history and multigravida became statistically significant predictors of birth weight.
Conclusion: Almost one-fourth of the newborn child had low birth weight. It will be better to give special attention to mothers with associated factors.
Keywords: newborn, birth weight, prevalence, Ethiopia
Background
Birth weight or size at birth is an important indicator of the child’s vulnerability to the risk of childhood illnesses and diseases. Birth weight also predicts the child’s future health, growth, psychosocial development, and chances of survival. Low birth- weight (LBW) is defined by the World health organization as the weight of a neonate below 2.5 kilograms at birth, often corresponding to the 10th percentile for its gestational age.1
This practical cut-off for international comparison is based on epidemiological observations that infants weighing less than 2.5 kilograms are approximately 20 times more likely to die than heavier babies.2 Those who survived from low birth weight have impaired immune function and increased risk of disease; they are likely to remain undernourished, with reduced muscle strength, throughout their lives, and to suffer a higher incidence of diabetes and heart disease.3
Globally, it is estimated that 15% to 20% of all births worldwide are low birth weight, representing more than 20 million births a year.4 The incidence has not declined in the last decade in Sub-Saharan Africa (SSA) and Asia.5
The goal of the 2012 World Health Assembly was a 30% reduction in the number of infants born with a weight lower than 2.5 kilograms by the year 2025. This would translate into a 3% relative reduction per year between 2012 and 2025 and a reduction from approximately 20 million to about 14 million infants with low weight at birth.3
Africa is a home for 22% of low birth weight and in Sub-Saharan Africa, LBW level is around 13–15% with a little variation across the regions.6
In Ethiopia prevalence of LBW is high. In 2012 the United Nations Children’s Fund (UNICEF) estimated the national prevalence of LBW was 20%.7 According to EDHS 2016, the proportion of births weighing less than 2.5 kg in Ethiopia at birth in the past three DHS surveys was 14% in 2005, 11% in 2011, and 13% in 2016.8 Similarly, in different studies, Ethiopia showed that 10.5% of live births in the northern region,9 11.2% of deliveries in Gondar were LBW.10 According to EDHS 2016 reports in Addis Ababa the prevalence of LBW is 11.4%,11 11.5%,8 in 2011, and 2016 respectively.8
The etiology of LBW is yet to be completely understood even though several studies have attempted to unravel the underlying causes. Sociodemographic factors such as sex,1 maternal height,12 and weight13 have been identified as risk factors for LBW. Similarly, maternal health, demographic and nutritional factors which include maternal age, parity,14 birth interval,1 multiple gestations, maternal comorbidity,11 and skilled antenatal care14 have been linked with LBW. Also, maternal socioeconomic and psychological factors which comprise education,1 alcohol intake,15 occupation,16 wealth status,1 and domestic violence17 were also found to be associated with LBW.
The Ethiopian government takes policy based commitment to mitigate the low birth problem. Despite the effort, there is current research done to determine the prevalence and factors which affect birth weight. Therefore this study aimed to determine the birth weight status and its associated factors. Findings from this study will add to the current knowledge about birth weight and identify risk factors of birth weight. The result of this study will serve as a baseline for other studies as well as for planning health interventions to improve the wellbeing of children and women.
Methods
Study Design, and Period
An Institutional based cross-sectional study was done from January 1st to June 30, 2020.
Study Setting
The study was carried out at a public hospital in North Wollo Zone, Amhara national regional state that is located 521 km away from Addis Ababa and 360 km from Bahir-Dar.
There are five public hospitals in North Wollo Zone. Namely: Woldia general, Kobo primary hospital; Lalibela primary hospital, Mekiet primary hospital, and Wadila primary hospital. On average, there were expected 530 delivery visits by taking the past 6 months low, medium and, high picks visits of delivery service.
Population
Source Population
All mothers who gave birth at public hospitals of North Wollo Zone were the source population.
Study Population
All mothers who gave birth at public Hospitals of North Wollo Zone during the data collection period were considered as the study population.
Eligibility
Inclusion Criteria
All selected mothers who delivered at the public Hospital of North Wollo Zone during the data collection period were included in the study.
Exclusion Criteria
Mothers who were sick seriously and unable to respond during the data collection period, and delivered before 28 weeks were excluded from the study. Stillbirth, IUFD, and multiple pregnancies were excluded from the study.
Sample Size Determination
The sample size was determined by using a single population proportion formula by considering Zα/2=critical value = 1.96 (Z value at 95% CL), P (estimated proportion of low birth weight) =11.2% is taken from a previous study conducted in Gondar referral Hospital,4 d (Margin of error) = 0.05, and 10% none- response rate. The sampling technique used in this stud was simple one-stage sampling. The researcher multiplied the sample size by 2 to manage the external validity of the study (153*2=306). By considering a 10% non-response rate (n=31) the final sample size becomes (N=337) mothers who gave birth.
Sampling Technique and Procedure
Two public hospitals were selected among five hospitals in North Wollo Zone using a simple random sampling method (lottery). The sample size assigned to the study hospitals is proportionally based on reviewing the average three-month delivery service report of the two study hospitals. Systematic random sampling technique was used to select the study populations until the required sample was reached. Skip fraction (k) of two was used to meet and interview the study participants (k=530/337 ≈ 2)
Study Variables
Dependent Variable
Birth weight.
Independent Variables
Socio-demographic factors: Maternal age, marital status, religion, ethnicity, drinking alcohol during pregnancy, the height of the mother, weight of the mother, education, occupation status of the mother, monthly average income of the family.
Obstetric factors: Gestational age, parity, ANC visit, hemoglobin, comorbid illness during pregnancy, history of abortion, PROM, APH, STI, gravidity, history of prenatal iron supplementation.
Nutritional factors: Maternal MUAC, exposure to nutrition counseling during the pregnancy, maternal BMI, frequency of additional meal intake during the current pregnancy.
Neonatal factors: Infant’s sex, GA, and birth-to-birth interval.
Data Collection Tools and Procedures
The data were collected by interviewing the mothers, reviewing medical records, and measuring the anthropometry of the mothers and the newborns using structured and pretested questionnaire. The interview and anthropometric measurements were conducted by trained midwives and nurses working in the delivery wards of the study public hospitals. The questionnaire was prepared in English language and translated to Amharic language and back to English to check for language consistency.
The questionnaire was adopted from the Ethiopian demographic health survey (EDHS) and other peer-reviewed articles.18–20
The socio-demographic and obstetric factors part of the questionnaire filled by interviewing the mother and from the ANC records. Questions in the third section were related to nutritional factors, maternal MUAC, exposure to nutrition counseling during the pregnancy, and neonatal factors. The weight of the newborns measured within 1 hour after birth using a valid balanced Seca weight scale which was used by clinical midwifery professionals and rounded to the nearest 100 grams. The scale was checked and zeroed after weighing each newborn child. Eligible mothers were interviewed face to face within 24 h after delivery.
Maternal height was measured against a wall height scale to the nearest centimeter. Maternal body mass index was subsequently be calculated. Maternal MUAC was measured by MUAC tape and rounded to the nearest 0.1 cm. All information was recorded on a data collection sheet designed for the study.
Data Quality Management
On each data collection day, the collected data were reviewed and checked for mistakes, legibility of handwriting, completeness, and consistency, and any mistake or principal investigator and supervisor cleared ambiguities. Any problems faced at the time of data collection were discussed and an immediate solution was taken. A pre-test was done out of the study health facilities out of 5% of sample size two weeks before the actual data collection to see the accuracy of responses, language clarity, and appropriateness of the tools. The necessary amendments were done based on the findings of the pretest. The amended tools were used for actual data collection at the selected health facilities.
Data Processing and Analysis
The collected data were coded, entered into Epi-data version 3.1, and analyzed by using SPSS version 20. Descriptive statistics (frequency, percent, mean and standard deviation) were used to summarize data and evaluate the distribution of responses. Simple and multiple linear regression analysis was used to identify associated factors of birth weight. Linear regression was used over ordinal logistic regression due to the overweight children count was very low (n=7) and this affects the model fitness. Ordinal logistic regression model fitness was failed (Hosmer Lemeshow p-value=0.01) and we changed the model to a linear regression model. The four most important assumption tests of the multiple linear regression model (linearity, normality, homoscedasticity, and multicollinearity) were checked and fitted. For analysis, dummy variables (for k categories, k-1 dummy variable) were created for categorical variables such as educational status, marital status, occupational status. In simple linear regression, variables with p-value <0.20 were entered into multiple linear regression to overcome confounding variables. The multiple coefficients of determination (R2) were used for the model fitness and its value was 0.74. The result was expressed as an unstandardized “ß” coefficient with a 95% confidence level and a p-value <0.05 was considered as statistically significant.
Results
Birth Weight
Three hundred thirty-seven mothers who delivered at the study area were included with a response rate of 100%. The mean ± SD weight of the newborn child was 2.94 ± 0.65 kilograms. The prevalence of low birth weight was 24% (95% CI= 19.6, 28.8).
Socio-Demographic Characteristics
A total of 337 laboring women were involved in this study. A total of 222 (65.9%) of the women were from Woldia General Hospital, and 115 (34.1%) were from Kobo primary hospital. About 53.1% of women came from urban, and the rest from rural areas. The mean age of the pregnant women was 32.7 with an SD of 5.4 years within the age range of 18–38 years. The majority of the mother was Orthodox Christian followed by Muslims in religion. Based on the educational status about 45.7% and 29.4% of mothers were primary and secondary education respectively. The remaining 29.4% did not attend modern education. The majority, 79.8% of women were married. More than half of the women (52.5%) of study participants were housewives, 27.0% were a merchant. The median household incomes of the laboring mothers were 5000 ETB (138.9USD) per month.
Obstetrical Characteristics of Mothers
In this study, about 90.2% of respondents were multigravida and the rest (9.8%) were prim gravida. Regarding the period of ANC initiation, 74.8% of laboring mothers were less than four months, and the rest was greater or equal to four months. A majority, 93.5% of respondents were delivered above 38 weeks, and in this study, normal vaginal delivery was the commonest mode of delivery (90.8%). Concerning the number of ANC visits, 54.8% of women had greater than or equal to four, and about 45.2% of respondents had got less than or equal to three ANC visits. The majority, 61.3%, of women had less than four ANC visits. Regarding birth spacing, more than fifty-five percent of the study subjects were waited less than 24 months after delivery, and about 44.4% of delivering mothers waited greater than or equal to 24 months. About sixty-seven and thirty-two percent of the study participants were had taken iron folate during ANC visits respectively.
Associated Factors of Birth Weight of Newborns
Simple and multiple linear regression was conducted to examine the association between birth weight and the predictor variables. Firstly, on simple linear regression analysis, those variables which have a significant association with the dependent variables with p-values of less than or equal to 0.2 were included in multiple linear regression.
Among all studied associated factors, 21 variables were independently associated with birth weight in simple linear regression analysis. Among them, 11 variables were statistically significant at a p-value of less than 0.05. A collinear variable with Variance Inflation Factor (VIF) was excluded and the counterpart is considered for simple linear regression. Variance Inflation Factor (VIF) range 1–4 considered tolerable variance. Maternal BMI was excluded due to higher Variance Inflation Factor (VIF) with maternal mid-upper arm circumference. Instrumental mode of delivery (dummy variable) was also excluded since it had higher multicollinearity with the primary educational level of the women.
Among socio-demographic characteristics of the women, age of the mother, family average monthly income, single, alcohol use, and education were statistically significant factors of the birth weight. As the age of the mother increases in a year, the child’s weight decrease by 27.4 grams (β = - 27.4, 95% CI=−52.6, −2.2). As the family average monthly income increase in a Birr, the weight of the child increased by 0.17 gram (β =0.17, 955CI=0.1, 0.2). Children’s weight reduces by nearly 231, and 270 grams among women not attended modern education and primary education as compared with a child from women with another educational level. A child weight born from single women in marital status increased by nearly 382 gram as compared with another marital status (β =391.8, 95% CI=204.7, 578.9). A child weight born from a woman who drinks alcohol at least once during the current pregnancy increase by 552 grams (β =251.7, 95% CI=397.1, 706.2)
Among neonatal factors, female sex becomes a statistically significant factor associated with birth weight There is almost 160-grams female child weight reduction as compared with the male child (β = −159.4, 95% CI=−244.9, 73.9).
Obstetrical factors also contribute to the birth weight of the child. Among them, had no abortion history, and multigravidas become statistically significant factors. A child from a woman who had no abortion history weight improved by 325 grams as compared with a child from a woman with an abortion history (β= 325.3, 95% CI=177.6, 473.0). Multigravida mothers have a child with improved weight. A child from multigravida women has an increased weight by almost 107 grams as compared with primipara women (β=107.2, 95% CI=10.4, 204.0).
Nutritional and health promotion factors also contribute to the newborn weight change. As a woman, MUAC increased in centimeters the child weight increased by almost 20 grams (β =20.3, 95% CI=3.4, 37.3). As the duration of iron folate treatment increased in a day the child’s weight decreased by nearly 7 grams (β =−6.8, 95%= −10.5, −3.1), (Table 1).
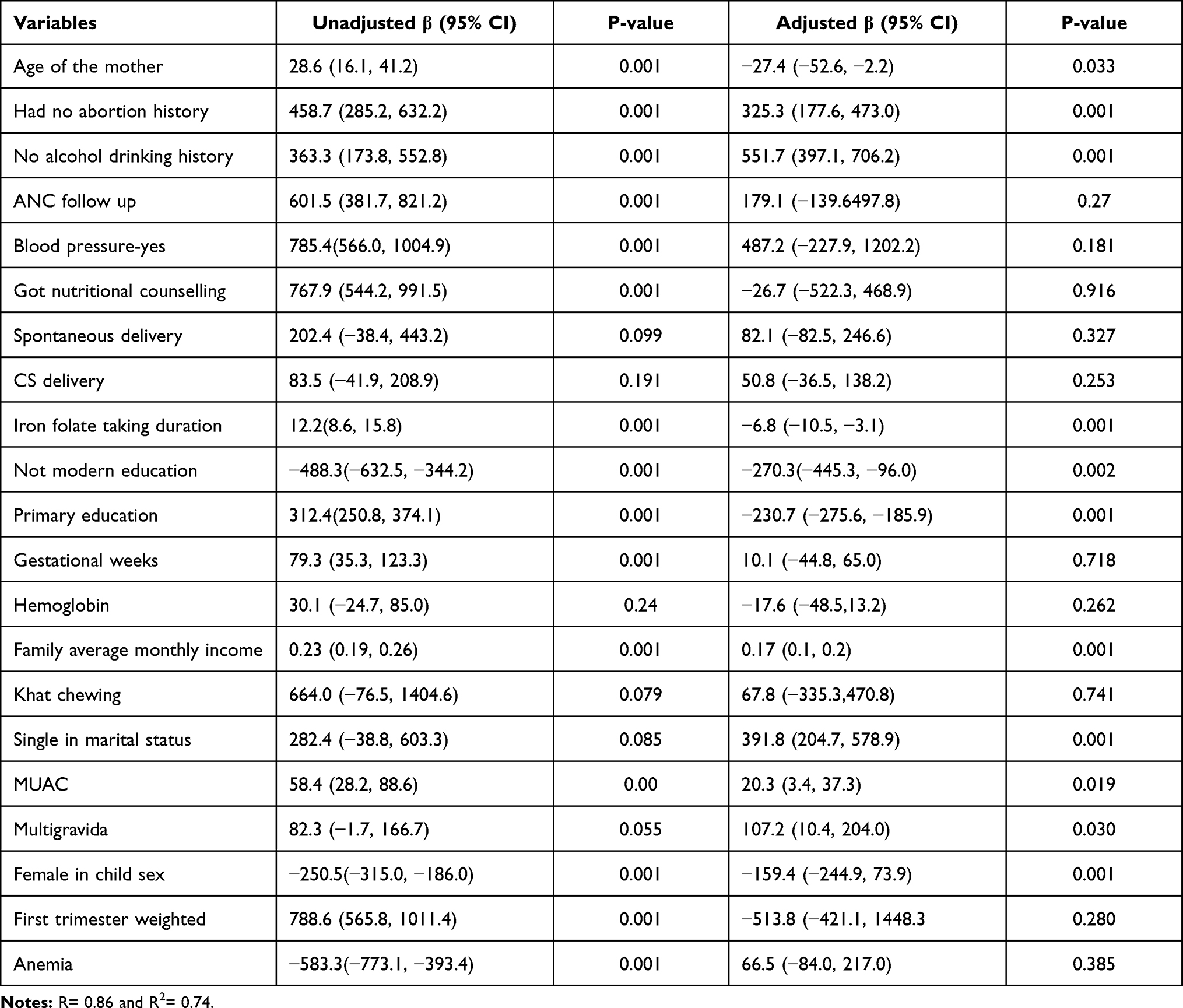 |
Table 1 Simple and Multiple Linear Regression Analysis to Identify Associated Factors of Newborn Birth Weight, Ethiopia, 2020 |
Discussion
The prevalence of low birth weight was 24% (95% CI= 19.6, 28.8). Maternal nutritional factors correlate with newborn weight. Maternal Mid-Upper Arm Circumference (MUAC) had a statistically significant association with newborn birth weight as one sample t-test revealed (t=183.6 at 2 tailed p-values ≤ 0.001)
The prevalence of low birth weight is in line with the study done Ethiopia Kersa district 28%,21 and EDHS 2016 report in the Amhara region 21.8%.8
Most studies done across the world shows the prevalence of low birth weight in this study is higher. The studies from Gondar teaching hospital, 17%,22 Iran 11%,23 Zimbabwe 16.7%,15 Kenya 12.3%,24 and Wolayta Sodo 8.1%25 showed a lower prevalence than the current study. The possible reason might be due to the current study area is one of the places where wasting and stating is prevalent in the Amara regional state.
However, the studies from India 32.8%,26,27 Nigeria 40%,28 EDHS 2016 report in Ethiopia, Afar region, 39.1%8 revealed a higher prevalence than the current study. The possible reason might be the Afar region is one of the Ethiopian regions, which had a higher prevalence of low birth weight.
Among sociodemographic factors, age of the mother, being single, family average monthly income, no modern education, primary education, and no alcohol use history showed statistical association with birth weight. The age of the mother and family average monthly income showed a positive association with neonate’s birth weight. This association is supported by the studies from developing countries,14 Nepal,29 Cameron,30 and Ethiopia- Adwa.31 In fact, a family with a higher monthly income can accommodate family expenses and the pregnant mother can get a balanced diet. Money had the power to fulfill the family’s basic needs like nutrition. Moreover, mothers who did not attend modern education, primary education, and being single showed a negative association with neonate’s birth weight. A mother with a lower educational level had a neonate with lower birth weight. This association is supported by the studies from the EDHS-2016 report,8 Ethiopia-bale Zone,17 and Ethiopia-Wolaita Sodo.32 Lower educational level may not allow mothers to read, ask, and understand the nutritional needs of the fetus and lack health promotion information. As an internal comparison, this might be due to higher education may indicate employment and get a better monthly salary. Therefore, a mother can buy her nutritional needs. Additionally, a neonate from unmarried mothers had a higher risk to have low birth weight as compared with their counterparts. A mother who did not use alcohol in the current pregnancy had a neonate with good birth weight. The possible justification might be due to that alcohol use during pregnancy decrease nutrient absorption and affect child outcome including birth weight.
Among neonatal factors, female sex neonates had lower birth weight than male neonates. Studies from Kenya,24 Amhara regional hospitals,33 Gondar,34 and Debre Berhan35 supported this outcome. The author is not sure about this association. However, due to some cultural issues mothers may have preferences for the male sex and allow them to nourish the fetus better than the unwanted gender.
Among obstetrical factors, mothers who had two or more pregnancies (multigravida) had a good birth weight child than prim gravida. This outcome is supported by the studies done in Iran,36 and Debre Markos.37 The association can be explained by as mothers had more pregnancies, they have a chance to get health information from others, health professionals, and from their own experience.
Maternal nutritional factors also contribute to neonate’s birth weight outcome. Mothers with higher mid-upper arm circumference (MUAC) had a better outcome for neonate birth weight. The studies were done in Amhara region hospitals,33 and Zimbabwe15 identified lower maternal MUAC puts the child at greater risk for low birth weight. The author is deadly sure that anthropometric measurements like MUAC are used as an indicator of the maternal nutritional status, and neonates’ birth outcome (birth weight).
Limitations and Strength
The cross-sectional nature of the study cannot determine the cause and effect relationship of the predictor variables with low birth weight. Since the data collected through face-to-face interviews, the mothers may underreport some factors due to social desirability bias; ie substance use, and abortion history.
Conclusion
Almost one-fourth of the children had low birth weight. Age of the mother, family average monthly income, being single, alcohol use, education, female sex, had no abortion history and multigravida became statistically significant predictors of birth weight.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Helsinki declaration for medical research involving human subjects was followed. Ethical clearance was obtained from the Institutional Health Research Review Committee (Ref. No. IHRERCB-0654/2020) of the college of health and medicine, Wollo University. Ethical clearance was obtained from the Institutional Health Research Review Committee of Wollo University, college of health science. A permission letter was written for each study health institution and a permission letter was taken from the study institution administrator. Written informed consent was taken from each study participant.
Consent for Publication
The manuscript did not contain individuals person detailed data in any form.
Acknowledgment
We would like to thank Wollo University, college of health science for giving ethical clearance. We would like to acknowledge the study hospitals and the study participants.
Author Contributions
MW select the title, develops the proposal, collect the data, and analyzed the outcome. AD, AB, and YE assist in the phase of proposal development, data collection, analysis, and manuscript preparation. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The budget needed for this research was covered by the study authors.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Sebayang SK, Dibley MJ, Kelly PJ, Shankar AV, Shankar AH, Group SS. Determinants of low birthweight, small‐for‐gestational‐age and preterm birth in Lombok, Indonesia: analyses of the birthweight cohort of the SUMMIT trial. Trop Med Int Health. 2012;17(8):938–950. doi:10.1111/j.1365-3156.2012.03039.x
2. Atitwa EB. Socio-economic determinants of low birth weight in Kenya: an application of logistic regression model. Am J Theor Appl Stat. 2015;4(6):438–445. doi:10.11648/j.ajtas.20150406.14
3. UNICEF. The State of the World’s Children 2008: Child Survival. Unicef; 2007.
4. Targets WWGN. 2025: Low Birth Weight Policy Brief. Geneva: WHO; 2014.
5. UNICEF D. Monitoring the Situation of Children and Women. 2005.
6. Lawn JE, Gravett MG, Nunes TM, Rubens CE, Stanton C, Group GR. Global report on preterm birth and stillbirth (1 of 7): definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth. 2010;10(S1):S1. doi:10.1186/1471-2393-10-S1-S1
7. Wardlaw T, Blanc A, Zupan J, Ahman E. Low Birthweight: Country. Regional and Global Estimates. 2004.
8. Ethiopia. Ethiopia Demographic and Health Survey, 2016. ICF International, Central Statistical Agency; 2017:2012.
9. Mengesha HG, Wuneh AD, Weldearegawi B, Selvakumar DL. Low birth weight and macrosomia in Tigray, Northern Ethiopia: who are the mothers at risk? BMC Pediatr. 2017;17(1):144. doi:10.1186/s12887-017-0901-1
10. Adane AA, Ayele TA, Ararsa LG, Bitew BD, Zeleke BM. Adverse birth outcomes among deliveries at Gondar University hospital, Northwest Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):90. doi:10.1186/1471-2393-14-90
11. Noureddine E, Abdellatif B. Prevalence and determinants of low birth weight: a case-control study in marrakesh (morocco). Iran J Public Health. 2015;44(3):422.
12. Heaman M, Kingston D, Chalmers B, Sauve R, Lee L, Young D. Risk factors for preterm birth and small‐for‐gestational‐age births among Canadian women. Paediatr Perinat Epidemiol. 2013;27(1):54–61. doi:10.1111/ppe.12016
13. Agarwal K, Agarwal A, Agrawal V, Agrawal P, Chaudhary V. Prevalence and determinants of” low birth weight” among institutional deliveries. Ann Niger Med. 2011;5(2):48. doi:10.4103/0331-3131.92950
14. Mahumud RA, Sultana M, Sarker AR. Distribution and determinants of low birth weight in developing countries. J Prev Med Public Health. 2017;50(1):18. doi:10.3961/jpmph.16.087
15. Feresu SA, Harlow SD, Woelk GB, Thorne C. Risk factors for low birthweight in Zimbabwean women: a secondary data analysis. PLoS One. 2015;10(6):e0129705. doi:10.1371/journal.pone.0129705
16. Deshpande Jayant D, Phalke D, Bangal V, Peeyuusha D. Maternal risk factors for low birth weight neonates: a hospital based case-control study in rural area of western maharashtra, India. Natl J Community Med. 2011;2(3):394–398.
17. Demelash H, Nigatu D, Gashaw K. A case-control study on intimate partner violence during pregnancy and low birth weight, Southeast Ethiopia. Obstet Gynecol Int. 2015;2015:2015. doi:10.1155/2015/394875
18. Demographic E. Health Survey: Addis Ababa. Ethiopia and Calverton, Maryland, USA: central statistics agency and ORC macro; 2011.
19. Wardlaw TM. Low Birthweight: Country, Regional and Global Estimates. Unicef; 2004.
20. Macro O. Central Statistical Agency. Addis Ababa, Ethiopia; 2006.
21. Assefa N, Berhane Y, Worku A, Sarkar IN. Wealth status, mid upper arm circumference (MUAC) and antenatal care (ANC) are determinants for low birth weight in Kersa, Ethiopia. PLoS One. 2012;7(6):e39957. doi:10.1371/journal.pone.0039957
22. Zeleke BM, Zelalem M, Mohammed N. Incidence and correlates of low birth weight at a referral hospital in Northwest Ethiopia. Pan Afr Med J. 2012;12(1).
23. Tabrizi FM, Saraswathi G. Maternal anthropometric measurements and other factors: relation with birth weight of neonates. Nutr Res Pract. 2012;6(2):132. doi:10.4162/nrp.2012.6.2.132
24. Muchemi OM, Echoka E, Makokha A. Factors associated with low birth weight among neonates born at Olkalou District Hospital, Central Region, Kenya. Pan Afr Med J. 2015;20(1). doi:10.11604/pamj.2015.20.108.4831
25. Zenebe K, Awoke T, Birhan N. Low birth weight & associated factors among newborns in Gondar town, North West Ethiopia: institutional based cross-sectional study. Indo Glob J Pharm Sci. 2014;4(2):74–80.
26. Kumari S, Garg N, Kumar A, et al. Maternal and severe anaemia in delivering women is associated with risk of preterm and low birth weight: a cross sectional study from Jharkhand, India. One Health. 2019;8:100098. doi:10.1016/j.onehlt.2019.100098
27. Jacob PS, Nath S. Periodontitis among poor rural Indian mothers increases the risk of low birth weight babies: a hospital-based case control study. J Periodontal Implant Sci. 2014;44(2):85–93. doi:10.5051/jpis.2014.44.2.85
28. Asundep NN, Carson AP, Turpin CA, et al. Determinants of access to antenatal care and birth outcomes in Kumasi, Ghana. J Epidemiol Glob Health. 2013;3(4):279–288. doi:10.1016/j.jegh.2013.09.004
29. Bhaskar RK, Deo KK, Neupane U, et al. A case control study on risk factors associated with low birth weight babies in Eastern Nepal. Int J Pediatr. 2015;2015:2015. doi:10.1155/2015/807373
30. Njim T, Atashili J, Mbu R, Choukem S-P. Low birth weight in a sub-urban area of Cameroon: an analysis of the clinical cut-off, incidence, predictors and complications. BMC Pregnancy Childbirth. 2015;15(1):1–8. doi:10.1186/s12884-015-0723-9
31. Gebregzabiherher Y, Haftu A, Weldemariam S, Gebrehiwet H. The prevalence and risk factors for low birth weight among term newborns in Adwa General Hospital, Northern Ethiopia. Obstet Gynecol Int. 2017;2017:2017. doi:10.1155/2017/2149156
32. Kastro S, Demissie T, Yohannes B. Low birth weight among term newborns in Wolaita Sodo town, South Ethiopia: a facility based cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):1–7. doi:10.1186/s12884-018-1789-y
33. Asmare G, Berhan N, Berhanu M, Alebel A. Determinants of low birth weight among neonates born in Amhara Regional State Referral Hospitals of Ethiopia: unmatched case control study. BMC Res Notes. 2018;11(1):1–7. doi:10.1186/s13104-018-3568-2
34. Adane AA, Ayele TA, Ararsa LG, Bitew BD, Zeleke BM. Adverse birth outcomes among deliveries at Gondar University hospital, Northwest Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):1–8.
35. Gizaw B, Gebremedhin S. Factors associated with low birthweight in North Shewa zone, Central Ethiopia: case-control study. Ital J Pediatr. 2018;44(1):1–9. doi:10.1186/s13052-018-0516-7
36. Momeni M, Danaei M, Kermani AJN, et al. Prevalence and risk factors of low birth weight in the southeast of Iran. Int J Prev Med. 2017;8:8. doi:10.4103/ijpvm.IJPVM_112_16
37. Gebrehawerya T, Gebreslasie K, Admasu E, Gebremedhin M. Determinants of low birth weight among mothers who gave birth in Debremarkos referral hospital, Debremarkos town, east Gojam, Amhara region, Ethiopia. Neonat Pediatr Med. 2018;4(1):145. doi:10.4172/2572-4983.1000145
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.