")
Back to Journals » Drug Design, Development and Therapy » Volume 16
New Oral Anticoagulants Open New Horizons for Cancer Patients with Venous Thromboembolism
Authors Wumaier K, Li W, Cui J
Received 11 May 2022
Accepted for publication 16 July 2022
Published 3 August 2022 Volume 2022:16 Pages 2497—2507
DOI https://doi.org/10.2147/DDDT.S373726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Kaidireyahan Wumaier,1 Wenqian Li,1 Jiuwei Cui2
1The First Hospital of Jilin University, Jilin University, Changchun, People’s Republic of China; 2Department of Cancer Center, the First Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Jiuwei Cui, Department of Cancer Center, the First Hospital of Jilin University, Changchun, Jilin, 130021, People’s Republic of China, Tel/Fax +86-0431-88782178, Email [email protected]
Abstract: Venous thromboembolism (VTE) is associated with increased morbidity and mortality, decreased quality of life, and higher economic burden in patients with cancer. Currently, the treatment of VTE in patients with cancer is particularly challenging. For many years, low molecular weight heparin (LMWHs) has been the standard for the treatment of cancer-associated VTE. Recently, the introduction of new oral anticoagulants (NOACs) may offer an oral anticoagulant option for some patients with cancer-associated thrombosis (CAT) as a growing body of literature supports the use of NOACs in the setting of CAT. With the use of NOAC as a new option in the management of CAT, clinicians now face several choices for the individual cancer patient with VTE. We need a more in-depth understanding of the drug properties, efficacy and safety, economic analysis that allows us to choose the most appropriate treatment for each patient. In the review, we will present an overview of CAT management, discuss the available evidence, economic costs for NOACs in the treatment of CAT, and seek to provide the best range of treatments for cancer patients.
Keywords: new oral anticoagulants, low molecular weight heparin, venous thromboembolism, cancer-associated thrombosis, anticoagulants
Introduction
Venous thromboembolic (VTE) disease is a continuing global health burden, particularly in cancer patients.1–4 The incidence of cancer-associated thrombosis (CAT) continues to rise over the years.5 It is also recognised that anticoagulant treatment is important in this growing population. Vitamin K antagonists (VKAs) have been for a long time the only option for oral anticoagulation. Low molecular weight heparins (LMWHs) have been shown to be superior to VKAs6–11 and recommended by guidelines as the standard of treatment for CAT in the last few years.12–14 However, the treatment with LMWHs still has limitations like an inconvenience for patients and costly for health care systems.15 The introduction of new oral anticoagulants (NOACs) has remodeled the antithrombotic therapy of choice, with a tendency of widening the range of indications. Taking into account the positive results of the studies so far, NOACs have been included in current guidelines as important alternatives to LMWHs for the treatment of VTE in suitable patients with cancer, but further studies are expected. Herein, in the present review, we have discussed recent evidence and their potential clinical and economic impact to will further our understanding of the optimal antithrombotic approach to the management of VTE in this patient population.
Burden of Venous Thromboembolism in Patients with Cancer
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common complication in patients with cancer and is termed as cancer-associated thrombosis (CAT). Patients with cancer have a four to sevenfold increased risk of VTE compared with patients without cancer.16 The factors that are responsible for the increase of risk basically include cancer type and anticancer-associated treatment.17–21 The highest incidence rate of 42% (OR 2.55; 95% CI 2.10–3.09) (p<0.001) was observed in patients with pancreatic cancer.22 Chemotherapy in anticancer-associated treatment is an independent risk factor for CAT. The annual incidence of chemotherapy-related VTE is about 11%, and this rate may rise to 20% with the use of different chemotherapy medicines.23 Data from a recent study indicated that the risk of VTE in cancer patients is increasing steadily and is ninefold higher than in the general population.24 The incidence of CAT may have changed in the past decade,6 which is associated with 4–20% among different cancers.25 However, of all cancer patients, only 15% develop symptomatic VTE, while up to 50% have evidence of asymptomatic DVT/PE and as many as 50% have VTE at autopsy, with VTE being the second-leading cause of death after cancer progression.2,26
VTE has a significant negative impact on the quality of life in patients with cancer, which is associated with a variety of poor consequences including an increased risk of VTE recurrence, major bleeding, and early mortality.5,26–31 It has long been observed that thromboembolism represents a major cause of death among patients with cancer after the malignancy itself.5,31,32 The occurrence of VTE has been reported to increase the likelihood of death for cancer patients by 2- to 6-fold.4,5,28,33 A large-scale survey revealed that in-hospital mortality was observed in 5.5% of cancer patients without a VTE diagnosis, whereas in 15.0% of those with VTE, including 19.4% with a pulmonary embolism, in the United States.34 Moreover, when cancer patients develop VTE, they have a significantly increased risk of VTE recurrence and bleeding with a threefold higher risk of recurrent VTE, and a twofold higher risk of anticoagulation-associated bleeding compared to patients without cancer.35 Furthermore, recurrent VTE is associated with a higher risk for a range of VTE-related complications, including venous ulcers, pulmonary hypertension, and venous insufficiency, which has a broader impact on the patient’s quality of life.36 For these reasons, VTE may lead to otherwise unnecessary hospitalizations and increased annual health care costs.3,37 Several qualitative studies have explored patients’ experiences of cancer-associated thrombosis, with consistent reports of VTE causing considerable distress to patients with cancer and their families.38–40
VTE events place a substantial economic burden on the healthcare system that is further amplified among patients with cancer. Compared to cancer patients without VTE, cancer patients with VTE have been shown to have three times as many all-cause hospitalizations, more days spent in the hospital, and a significantly higher number of outpatient visits.3 Mean total hospitalization costs were 2.5-times ($17,089) higher among cancer patients with VTE compared to patients without VTE and accounted for 62% of the VTE-related total healthcare costs.41 Total (all-cause) health care costs were about 80% higher in cancer patients with VTE (mean unadjusted cost of $74,959 per patient) in comparison with matched cancer patients without VTE ($41,691)42 and remain significantly higher for years after the index VTE event.43 Using claims data, Khorana et al found that cancer patients with VTE incurred significantly higher total healthcare costs compared to cancer patients without VTE ($74,959 vs $41,691 per patient over the 12-month follow-up period; p<0.0001).3 Furthermore, in a real-world study, cancer patients with recurrent VTE incurred nearly twice the total healthcare costs relative to cancer patients without recurrent VTE, of which nearly 75% of the increased cost was associated with VTE recurrence.44
Evolution from Traditional Anticoagulants to NOACs for CAT
Tailoring anticoagulation with the optimal agents in patients with cancer is of utmost importance due to dismal prognosis and higher healthcare costs. Historically, vitamin K antagonists (VKAs) were the mainstay of therapy for VTE in patients with cancer.45 However, published studies showed that the use of VKAs for CAT is associated with a higher risk for both recurrence and bleeding compared with the general population. Patients with cancer had a threefold to fourfold higher risk for VTE recurrence with VKAs treatment and a sixfold higher risk for anticoagulant-associated bleeding compared with non-cancer patients.46,47 Furthermore, the management of VKAs is further complicated by frequent blood test monitoring and numerous drug-drug and drug-food interactions.48
Low molecular weight heparins (LMWHs) were the first available alternatives to VKAs in the past few years, which represent a more effective and stable pharmacological approach to CAT treatment. The anticoagulant effect of LMWHs is due to the inhibition of the final common pathway of the coagulation cascade by activation of antithrombin III, which promotes the inactivation factors Xa and IIa.49 Compared with VKAs, the major advantages of LMWHs are their independence from gut absorption, fewer drug-drug interactions, and similar or lower rates of VTE recurrence bleeding in cancer patients.6,10,50
The two largest studies, CLOT (Comparison of Low Molecular Weight Heparin versus Oral Anticoagulant Therapy) and CATCH (Comparison of Acute Treatments in Cancer Haemostasis) studies, investigated the safety and efficacy of LMWHs compared with VKAs in patients with cancer-associated VTE. In 2003, the CLOT trial (Randomised Comparison of Low Molecular Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer), which was a large randomized clinical trial comparing VKAs to an LMWHs in 672 cancer patients, demonstrated that LMWHs dalteparin was associated with significantly lower rates of recurrent VTE with no increased risk of major bleeding when compared to warfarin.6 In the CLOT study, 336 patients received dalteparin 200 international units (IU) per kilogram of body weight once daily (maximum 18,000 IU per day) for 1 month followed by 150 IU per kilogram once daily for 5 months. 336 patients received VKAs for six months after initial anticoagulation with dalteparin 200 IU/kg for 5 to 7 days.6 The results of the multinational CLOT trial showed that the rates of recurrent VTE were 8% (27/336) and 16% (53/336) in the dalteparin and VKAs groups, corresponding to a hazard ratio (HR) of 0.48 (95% confidence interval (CI): 0.30–0.77, p ¼ 0.002). Furthermore, there was no significant difference in major bleeding with rates of 6% in the dalteparin group and 4% in the VKAs arm (p=0.27). Thus, this led to LMWHs being the first-line treatment for CAT and is still widely used. Subsequently, this recommendation was supported by the more contemporary CATCH trial published in 2015, which was the largest trial to compare LMWHs with VKAs.10 In 900 cancer patients with cancer-associated VTE, 6-month treatment with LMWHs tinzaparin nonsignificantly reduced the primary efficacy outcome of recurrent VTE and did not affect major bleeding compared with the VKAs warfarin. The rates for recurrent VTE were not statistically significant with 31/449 (7%) patients receiving tinzaparin and 45/451 (10%) patients on warfarin (p=0.07), corresponding to a nonsignificant risk reduction with an HR of 0.65 (95% CI: 0.41–1.03). Rates of major bleeding were found at 2.7% in the tinzaparin arm and 2.4% in the warfarin arm (p=0.77), while clinically relevant nonmajor bleeding (CRNMB) was statistically significant with 49 (10.9%) patients in the tinzaparin group compared to 69 (15.3%) in the warfarin group (p=0.004). As for LMWHs vs VKAs, meta-analyses and retrospective studies confirmed the superiority of LMWHs over conventional treatment in reducing recurrences, reinforcing the use of LMWHs over VKAs for the treatment of CAT. A meta-analysis including six randomized controlled trials comparing LMWHs with VKAs reported an overall reduction in risk of recurrent VTE with LMWHs (odds ratio (OR): 0.55; 95% CI: 0.40–0.75) with no increased risk in bleeding (relative risk(RR): 1.10; 95% CI: 0.71–1.69).51 And one retrospective study52 found that LMWHs were more efficacious in the treatment of cancer-associated VTE with similar bleeding risk compared with VKAs.
Although effective and safe, LMWHs treatment has practical limitations, including the daily subcutaneous injections and associated costs, which may limit long-term adherence in some patients. Daily subcutaneous injections that can lead to pain, bruising, and hematomas, may have an impact on the patient’s quality of life.53,54 An additional limitation is the high cost of LMWHs therapy relative to VKAs.55 Thus, the compliance of treatment with LMWHs is low in patients with cancer-associated VTE. However, real-world data suggest that patient compliance with LMWHs is only 37% still on therapy at 6 months (vs 61% of patients prescribed oral agents).56 As a result, safer and more convenient new agents have been sought for patients with cancer who have VTE.
New oral anticoagulants (NOACs) represent a convenient and effective treatment option, which have certainly changed the landscape of anticoagulation in specific patient populations affected by cancer. Three of these molecules (namely, apixaban, edoxaban, and rivaroxaban) target activated factor X, and one molecule (ie, dabigatran) is directed against activated factor II, thrombin. In this study, the wording NOACs refer to apixaban, rivaroxaban, and edoxaban—except for dabigatran, which has not been specifically studied in a randomized trial in patients with cancer-associated VTE. They offer many advantages over VKAs, including predictable pharmacokinetics and pharmacodynamics, rapid onset and offset of action, short half-life, wide therapeutic window, few drug-drug and drug-food interactions, and no need for laboratory monitoring.57 In addition, unlike LMWHs, NOACs are administered orally, are cheaper than LMWHs,58 and therefore an attractive potential alternative to traditional anticoagulants for the treatment of CAT.
Evidence for the Use of NOACs in Cancer Patients
Evidence from Randomized Clinical Trials
Initial evidence from analysis of cancer patient subgroups included in the landmark NOACs trials, which focused on the general patient population,59–64 showed that the efficacy and safety of NOACs were similar to those found in the general population.64–69 Subsequently, randomized clinical trials (RCTs) specifically focusing on VTE cancer patients have confirmed previous observations related to the efficacy of NOACs in the treatment of CAT, and have further provided safety of NOACs in the cancer setting. Four head-to-head randomized clinical trials have been conducted, including HOKUSAI VTE Cancer (edoxaban),70 SELECT-D (rivaroxaban),53 and ADAM VTE71 and Caravaggio (apixaban).72 NOACs, in particular the Factor Xa direct inhibitors apixaban (10 mg twice daily for 7 days followed by 5 mg twice daily), rivaroxaban (15 mg twice daily for 3 weeks followed by 20 mg once daily), and edoxaban (60 mg daily after at least 5 days of LMWHs therapy), have been compared with LMWHs as suggested by the CLOT study (dalteparin 200 IU/kg for 1 month, followed by dalteparin 150 IU/kg) for CAT in four RCTs. In each study, patients were followed for at least 6 months. The primary endpoint in the SELECT-D and CARAVAGGIO studies was recurrent VTE, in the ADAM VTE was major bleeding, while the Hokusai-VTE Cancer study chose a combined endpoint of recurrent VTE and major bleeding. In all three studies, major bleeding was defined according to the International Society of Thrombosis and Haemostasis (ISTH) criteria in three studies. The European Medicines Agency definition was used in the Caravaggio study73 and includes all the ISTH criteria for major bleeding and bleeding requiring surgical intervention. Specifics of study and the conclusions of outcome are in Table 1.
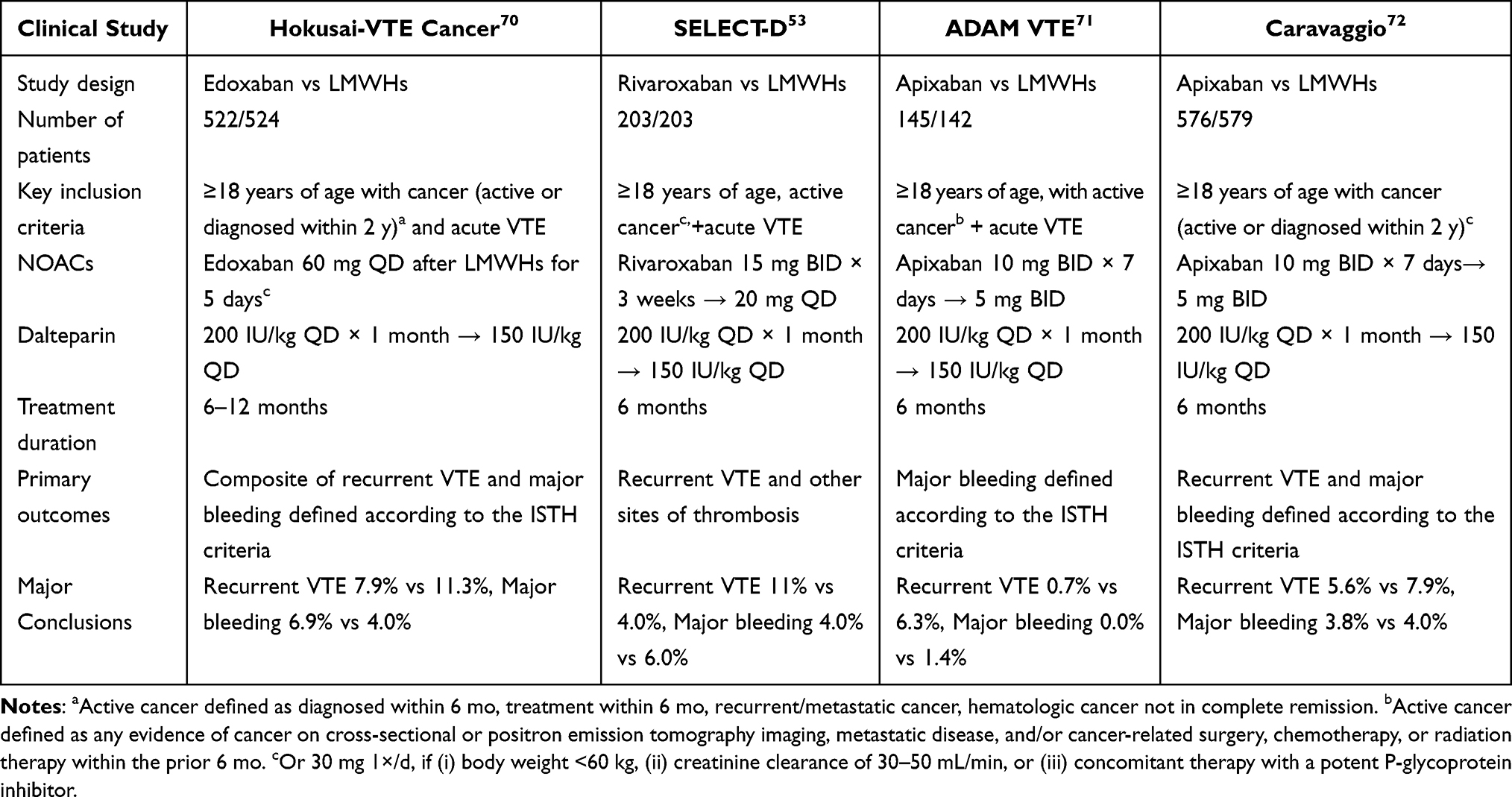 |
Table 1 Clinical Study to Evaluate the Efficacy and Safety of NOACs in CAT Treatment |
The Hokusai-VTE Cancer study showed an incidence of the primary composite outcome (recurrent VTE or major bleeding) of 12.8% in the edoxaban arm and 13.5% in the dalteparin arm (HR: 0.97, 95% CI: 0.70–1.36, p=0.006 for non-inferiority).70 Recurrent VTE was lower in the edoxaban group compared to the dalteparin group (7.9% vs 11.3%; HR: 0.71, 95% CI: 0.48–1.06, P=0.09), but major bleeding was significantly increased with edoxaban compared to dalteparin (6.9% vs 4.0%; HR: 1.77; 95% CI: 1.03–3.04, P=0.04) driven by higher bleeding rates in patients with gastrointestinal cancers (13.2% vs 2.4%).70 The second published trial was the SELECT-D study.53 The primary outcome of VTE recurrence rate was 4% with rivaroxaban and 11% with dalteparin (HR, 0.43; 95% CI: 0.19–0.99) with a rate of major bleeding of 6% for rivaroxaban and 4% for dalteparin (HR: 1.83, 95% CI: 0.68 to 4.96) and rates of CRNMB of 13% and 4%, respectively (HR: 3.76, 95% CI: 1.63 to 8.69).53 As in the Hokusai-VTE Cancer study, it was observed that the risk of major bleeding with rivaroxaban was higher in patients with malignancies of the gastrointestinal tract. The results of the ADAM VTE Trial found that NOACs treatment for cancer patients reduced the incidence of major bleeding and recurrent VTE compared with LMWHs. No patients on apixaban suffered a major bleeding complication compared to 1.4% of patients receiving LMWHs.71 The secondary outcome of the VTE recurrence rate was 0.7% in the apixaban group and 6.3% in the dalteparin group (HR: 0.099, 95% CI: 0.013–0.780, P=0.0281).71 The recently published CARAVAGGIO study confirmed recurrent VTE was 5.6% in the apixaban group and 7.9% in the dalteparin group (HR: 0.63, 95% CI: 0.37 to 1.07, P<0.001 for non-inferiority).72 Major bleeding rates were 3.8% in apixaban group and 4.0% in dalteparin group (HR: 0.82, 95% CI: 0.40 to 1.69, P=0.60). CRNMB rates were 9.0% with apixaban and 6.0% with dalteparin (HR: 1.42, 95% CI: 0.88 to 2.30).72
The above four trials suggest that NOACs had a significantly lower risk of recurrent VTE, without a significantly higher likelihood of major bleeding than when treated with dalteparin. However, the overall heterogeneity contribution for major bleeding was mainly related to the apixaban studies. Hokusai VTE Cancer and SELECT-D reported an increased risk of major bleeding with NOACs compared with dalteparin in patients with gastrointestinal cancer. In contrast, bleeding rates were very low with both apixaban and dalteparin in the ADAM VTE trial, and in the Caravaggio trial, bleeding rates were similar in the apixaban and dalteparin arms. Given the absence of a direct head-to-head comparison of the different NOACs, the differences in safety profiles should be regarded with caution.
Evidence from Meta-Analyses and Observational Studies
The validity and generalizability of the efficacy of NOACs compared with dalteparin in the treatment of VTE in cancer patients are strengthened by meta-analysis. Within the previous evidence-based analysis, Vedovati et al74 conducted a meta-analysis of randomized studies with NOACs assessing the safety and efficacy of NOACs in patients with thrombosis and cancer. In recent years, a meta-analysis of four randomized controlled studies (2894 patients) comparing apixaban, edoxaban, or rivaroxaban with dalteparin shows that cancer-associated VTE who were treated with NOACs had a significantly lower risk of recurrent VTE, without a significantly higher likelihood of major bleeding than when treated with dalteparin.75 Another meta-analysis found that NOACs significantly reduced VTE recurrence (RR: 0.59, 95% CI: 0.48–0.73) compared with conventional therapy. Results were similar in the LMWHs and VKAs subgroups.76 NOACs had a higher, though the nonsignificant, risk of major bleeding compared with LMWHs (RR: 1.33, 95% CI: 0.94–1.89) lower risk of major bleeding compared with VKAs (RR: 0.60, 95% CI: 0.39–0.93).76
Although RCTs provide the highest level of clinical evidence, applying the results of RCTs to assessments of clinical effectiveness in real-world practice may be challenging. Emerging real-world studies have recently been published, describing initial experiences in the cancer population. A real-world study evaluating NOACs (including rivaroxaban, apixaban, edoxaban, or dabigatran) vs LMWHs enoxaparin for cancer-associated VTE showed that the groups had a similar risk of VTE recurrence (HR: 0.62, 95% CI: 0.39–1.01, P=0.05) and major bleeding (HR: 0.80, 95% CI: 0.52–1.24, P=0.32) at 12 months of follow-up. However, taking NOACs was associated with a significantly lower risk of gastrointestinal bleeding compared with receiving enoxaparin (10 patients (1.9%) vs 41 patients (7.1%), HR: 0.29, 95% CI: 0.15–0.59, P<0.001).77 Findings for both primary outcomes were consistent with competing risk analyses (recurrent VTE: HR: 0.68, 95% CI: 0.45–1.01, P=0.05; major bleeding: HR: 0.77, 95% CI: 0.51–1.16, P=0.21).77 This cohort study found that in real-world practice, among Asian patients with cancer-associated VTE, the use of NOACs was associated with a similar risk for recurrent VTE or major bleeding compared with the use of the LMWHs enoxaparin. Nonetheless, the use of NOACs was associated with a significantly lower rate of gastrointestinal bleeding.77 In a large retrospective study comparing outcomes in patients with cancer treated with rivaroxaban or standard treatment, the overall VTE recurrence was significantly lower by 28% in patients treated with rivaroxaban versus LMWHs. Major bleeding rates were similar in patients taking rivaroxaban in comparison with patients receiving LMWHs.78 Smaller retrospective studies reported similar results with NOACs in comparison with LMWHs in patients with cancer.79–82
Ongoing Studies
Several ongoing studies are evaluating NOACs versus LMWHs for the treatment of cancer-associated VTE. The Comparing Oral and Injectable Blood Thinners to Prevent and Treat Blood Clots in Patients with Cancer (CANVAS; NCT02744092) trial is a 940-patient study with the primary objective of evaluating comparing NOACs therapy (rivaroxaban, apixaban, edoxaban, or dabigatran, by investigator’s choice) with LMWHs with or without a transition to warfarin.83 The primary outcome in CANVAS is VTE recurrence; secondary outcomes include major bleeding, health-related quality of life, and the burden of anticoagulant therapy. The CASTA-DIVA (NCT02746185)84 study (rivaroxaban vs dalteparin) for the treatment of CAT has primary outcomes of recurrent VTE, major bleeding, and clinically relevant nonmajor bleeding and mortality. The API-CAT trial (NCT03692065) is comparing the efficacy and safety of two doses of apixaban for the extended treatment of VTE in cancer patients (breast, prostate, and colon-rectum);85 the EVEExtended study compares the safety of two doses of apixaban for the extended treatment of cancer patients with VTE; and other studies such as COSIMO37 (NCT027426239), a prospective cohort study (patient-reported outcomes with rivaroxaban: a noninterventional study), and Conko-011 (NCT02583191) evaluating rivaroxaban versus LMWHs with patient-reported treatment satisfaction as the primary outcome.85 These clinical trials will provide further evidence for the use of these agents in patients with cancer and will help to clarify remaining the questions.
Current Clinical Guidelines
Treatment of VTE in cancer patients represents a continuing clinical challenge. Evidence-based guidelines from professional organizations have provided treatment recommendations for the management of CAT. Major guidelines include the American College of CHEST Physicians (CHEST), National Comprehensive Cancer Network (NCCN), European Society for Medical Oncology (ESMO), American Society of Clinical Oncology (ASCO), and European Society of Cardiology (ESC).14,15,86–88 Nearly a decade of several international guidelines has given preference to NOACs over LMWHs in selected patients with cancer-associated VTE.89 Most recently, the National Comprehensive Cancer Network (NCCN) guidelines indicate that are preferred or acceptable for particular cancer patients without gastric or gastroesophageal lesions.90 The use of NOACs was also entered as an alternative treatment for CAT in the recent the American Society of Clinical Oncology (ASCO) guidelines.91 However, guidelines caution about their use in patients with Gastrointestinal (GI) and genitourinary (GU) malignancies due to the higher risk of bleeding until more experience is accrued to inform clinical practice. In the future, NOACs may become even more prominent in further CAT guidelines. Unfortunately, during the last decade, half of the patients with CAT fail to receive guideline-concordant therapy.92 As treatment options for CAT expand, further efforts are needed to understand the factors associated with anticoagulant use in a non-trial setting to close the gap between ideal and actual care.
Cost-Effectiveness
Economic evaluation has gained widespread application in many areas of clinical research as health care costs consume an increasing proportion of the gross domestic product (GDP). In particular, health economics help address the clinical decision-making process. Although we were not trained in economics, and as physicians, we care about patients’ well-being and not about costs, economic issues impinge on our clinical practice on daily, and should help patients explore resources that may facilitate receiving the best anticoagulant for their particular situation.
The cost-effectiveness studies comparing NOACs with LMWHs in patients with cancer will provide perspective regarding the selection of NOACs for the treatment of CAT. The cost-effectiveness and budget impact of rivaroxaban compared with dalteparin in patients with cancer at risk of recurrent VTE in the Netherlands found that the use of rivaroxaban instead of dalteparin can save over €10 million per year, primarily driven by the difference in drug costs.93 An economic comparison of edoxaban and LMWHs in the Brazilian population showed Edoxaban represents a cost-saving alternative to LMWHs for the management of CAT.94 Furthermore, Li et al found that rivaroxaban or edoxaban as compared to dalteparin is cost saving from a payer’s perspective for the treatment of CAT.95 Other studies showed that edoxaban, when compared to LMWHs, was a cost-effective treatment for six months in cancer patients in the United States.96 The study from the perspective of the Chinese healthcare system, which compared the cost-effectiveness of using NOACs and LMWHs for treating CAT, showed that NOACs can be a cost-saving anticoagulant choice.97 The 6-month cost of NOACs was $ 654.65 with 0.40 quality adjusted life-years (QALYs) while the 6-month cost of LMWHs was $USD 1,719.31 with 0.37 QALYs. Similarly, treatment with NOACs had a lower cost ($USD 657.85 vs $USD 1,716.56) and more health benefits (0.40 QALYs vs 0.37 QALYs) than treatment with LMWHs in a subgroup of patients with gastrointestinal malignancy. The study found treatment with NOACs would result in a large reduction in cost ($USD 1,447.22 vs $USD 3,374.70) but a small reduction in QALYs (3.07 QALYs vs 3.09 QALYs) compared with LMWHs over a 5-year time frame, resulting in an ICER of $USD 112,895.50/QALYs. The results of the cost-effectiveness analysis in different countries are summarized in Table 2.
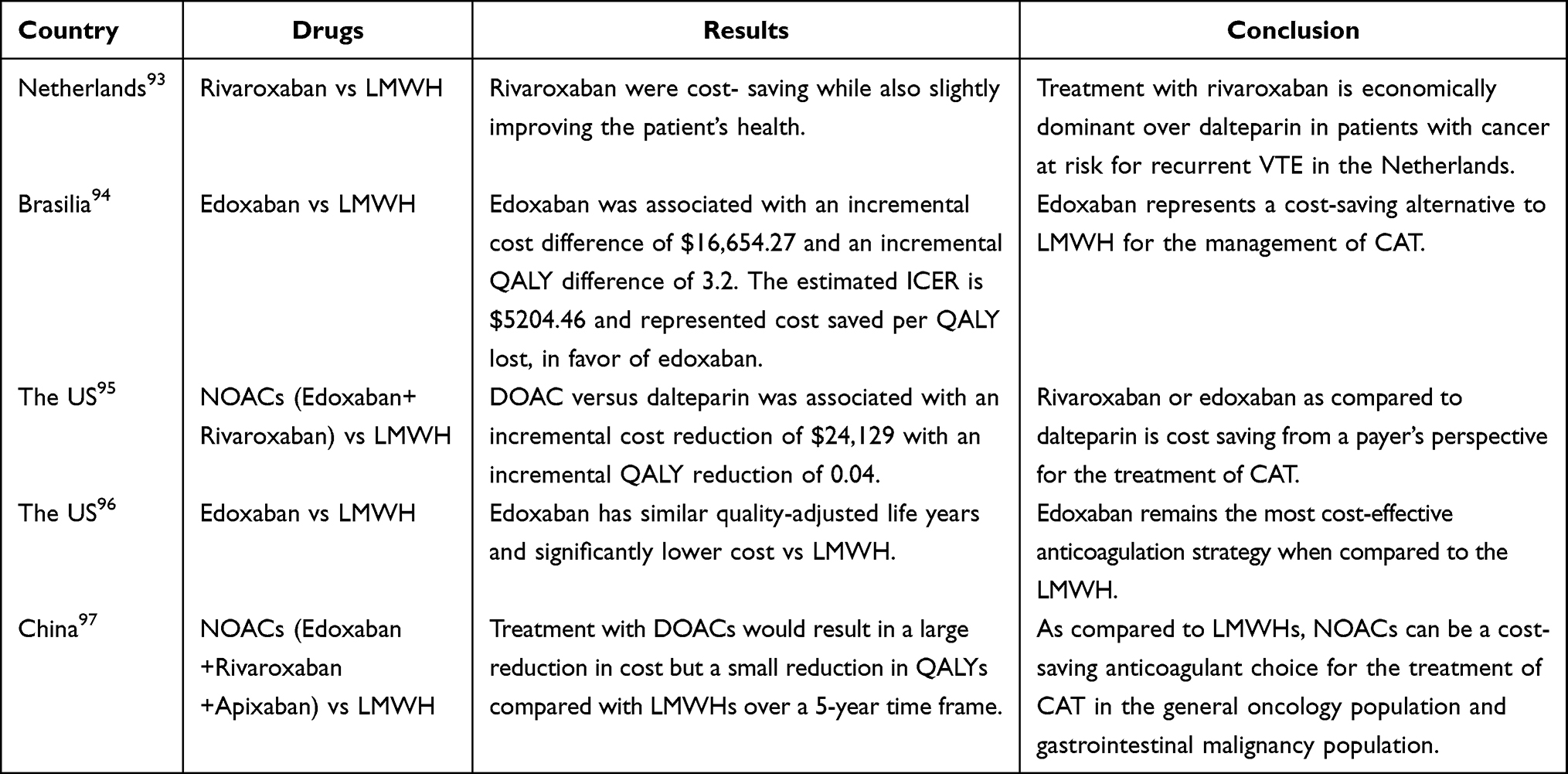 |
Table 2 Cost-Effectiveness Analyses |
These findings may provide a better understanding of VTE treatment-related utilization of healthcare resources and corresponding costs in patients with cancer. Nevertheless, in the existing literature, there is limited information on the healthcare resource use and costs associated with anticoagulants in patients with cancer. However, cost-effectiveness may depend heavily on country-specific health system organizations and economics. We should encourage other countries to conduct a similar reflection and to think about the respect of the good practice recommendations to optimize the public healthcare expenditure in this group of population.
Conclusion
VTE is a common and serious complication among patients with cancer, resulting in a substantial clinical and economic burden in the oncology setting. Cancer patients are at greater risk for VTE compared with patients without cancer. VTE is associated with higher morbidity, mortality, and rates of recurrent VTE as well as bleeding rates, all leading to increased healthcare costs and decreased quality of life. Consequently, anticoagulant therapy is essential and should take into consideration the potential of clinical benefit and economic costs for the management of VTE in patients with cancer.
Adding further complexity to the management of CAT, the emergence of NOACs challenges the concept of traditional anticoagulants as the standard of care. These products are considered appealing alternatives as they have practical advantages providing great opportunities to improve the quality of life. Gegard studies of NOACs in recent years illustrated that NOACs are at least as safe and effective as initial LMWHs followed by vitamin K antagonists for the treatment of cancer-associated VTE. Given the potentially favorable features of NOACs in the setting of active cancer treatment and the suggestion of better efficacy of NOACs with similar safety in studies for the treatment of VTE, NOACs have recently been added to clinical practice guidelines as alternative treatment in particular patients with cancer. While the majority of clinical recommendations discuss LMWHs as the standard of treatment for several years in cancer patients with VTE, more recent guidelines also increasingly consider NOACs as an alternative option in selected patients with cancer. The guidelines also advise caution with using NOACs in patients with GI and GU malignancies, and further research of their safety profile is still needed.
In modern healthcare, the economic sustainability of any treatment has gained paramount importance and we cannot just turn away when we are faced with cost-effectiveness issues. The knowledge of the economic impact of VTE in cancer patients would allow us to choose the most appropriate treatment in this group of the population. In the future, NOACs may become the best treatment approach in this specific population.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Lloyd AJ, Dewilde S, Noble S, Reimer E, Lee AY. What impact does venous thromboembolism and bleeding have on cancer patients’ quality of life? Value Health. 2018;21(4):449–455. doi:10.1016/j.jval.2017.09.015
2. Khorana AA, Francis CW, Culakova E, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632–634. doi:10.1111/j.1538-7836.2007.02374.x
3. Khorana AA, Dalal MR, Lin J, Connolly GC. Health care costs associated with venous thromboembolism in selected high-risk ambulatory patients with solid tumors undergoing chemotherapy in the United States. Clinicoecon Outcomes Res. 2013;5:101–108. doi:10.2147/CEOR.S39964
4. Sørensen HT, Mellemkjær L, Olsen JH, Baron JA. Prognosis of cancers associated with venous thromboembolism. N Engl J Med. 2000;343(25):1846–1850. doi:10.1056/NEJM200012213432504
5. Chew HK, Wun T, Harvey D, et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–464. doi:10.1001/archinte.166.4.458
6. Lee AY, Levine MN, Baker RI, Bowden C. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146–153. doi:10.1056/NEJMoa025313
7. Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729–1735. doi:10.1001/archinte.162.15.1729
8. Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006;119(12):1062–1072. doi:10.1016/j.amjmed.2006.02.022
9. Deitcher SR, Kessler CM, Merli G, et al. Secondary prevention of venous thromboembolic events in patients with active cancer: enoxaparin alone versus initial enoxaparin followed by warfarin for a 180-day period. Clin Appl Thromb Hemost. 2006;12(4):389–396. doi:10.1177/1076029606293692
10. Lee AYY, Kamphuisen PW, Meyer G, et al. Tinzaparin vs warfarin for treatment of acute venous thromboembolism in patients with active cancer: a randomized clinical trial. JAMA. 2015;314(7):677–686. doi:10.1001/jama.2015.9243
11. Romera A, Cairols MA, Vila-Coll R, et al. A randomised open-label trial comparing long-term sub-cutaneous low-molecular-weight heparin compared with oral-anticoagulant therapy in the treatment of deep venous thrombosis. Eur J Vasc Endovasc Surg. 2009;37(3):349–356. doi:10.1016/j.ejvs.2008.11.030
12. Lyman GH, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American society of clinical oncology clinical practice guideline update. J Clin Oncol. 2013;31(17):2189–2204. doi:10.1200/JCO.2013.49.1118
13. Farge D, Debourdeau P, Beckers M, et al. International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. J Thromb Haemost. 2013;11(1):56–70. doi:10.1111/jth.12070
14. Mandalà M, Falanga A, Roila F. Management of venous thromboembolism (VTE) in cancer patients: ESMO clinical practice guidelines. Ann Oncol. 2011;22(Suppl 6):vi85–92. doi:10.1093/annonc/mdr392
15. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315–352. doi:10.1016/j.chest.2015.11.026
16. Fuentes HE, Tafur AJ, Caprini JA. Cancer-associated thrombosis. Dis Mon. 2016;62(5):121–158. doi:10.1016/j.disamonth.2016.03.003
17. Lyman G. Venous thromboembolism in the patient with cancer: focus on burden of disease and benefits of thromboprophylaxis. Cancer. 2011;117(7):1334–1349. doi:10.1002/cncr.25714
18. Khorana A, Dalal M, Lin J, et al. Incidence and predictors of venous thromboembolism (VTE) among ambulatory high-risk cancer patients undergoing chemotherapy in the United States. Cancer. 2013;119(3):648–655. doi:10.1002/cncr.27772
19. Kourlaba G, Relakis J, Mylonas C, et al. The humanistic and economic burden of venous thromboembolism in cancer patients: a systematic review. Blood Coagul Fibrinolysis. 2015;26(1):13–31. doi:10.1097/MBC.0000000000000193
20. Ay C, Dunkler D, Marosi C, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010;116(24):5377–5382. doi:10.1182/blood-2010-02-270116
21. Khorana A, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10):2339–2346. doi:10.1002/cncr.23062
22. Ogren M, Bergqvist D, Wåhlander K, Eriksson H, Sternby NH. Trousseau’s syndrome - what is the evidence? A population-based autopsy study. Thromb Haemost. 2006;95(3):541–545. doi:10.1160/TH05-10-0694
23. Otten H-M-MB, Mathijssen J, ten Cate H, et al. Symptomatic venous thromboembolism in cancer patients treated with chemotherapy: an underestimated phenomenon. Arch Intern Med. 2004;164(2):190–194. doi:10.1001/archinte.164.2.190
24. Mulder F, Horváth-Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959–1969. doi:10.1182/blood.2020007338
25. Wang H, Xu X, Pu C, et al. Clinical characteristics and prognosis of cancer patients with venous thromboembolism. J Cancer Res Ther. 2019;15(2):344–349. doi:10.4103/jcrt.JCRT_121_18
26. Kuderer NM, Ortel TL, Francis CW. Impact of venous thromboembolism and anticoagulation on cancer and cancer survival. J Clin Oncol. 2009;27(29):4902–4911. doi:10.1200/JCO.2009.22.4584
27. Alcalay A, Wun T, Khatri V, et al. Venous thromboembolism in patients with colorectal cancer: incidence and effect on survival. J Clin Oncol. 2006;24(7):1112–1118. doi:10.1200/JCO.2005.04.2150
28. Chew HK, Wun T, Harvey DJ, et al. Incidence of venous thromboembolism and the impact on survival in breast cancer patients. J Clin Oncol. 2007;25(1):70–76. doi:10.1200/JCO.2006.07.4393
29. Lyman GH. Venous thromboembolism in the patient with cancer: focus on burden of disease and benefits of thromboprophylaxis. Cancer. 2011;117(7):1334–1349.
30. Lyman GH. Impact of venous thromboembolism on survival in patients with advanced cancer: an unmet clinical need. Intern Emerg Med. 2014;9(5):497–499. doi:10.1007/s11739-014-1087-2
31. Connolly GC, Khorana AA, Kuderer NM, et al. Leukocytosis, thrombosis and early mortality in cancer patients initiating chemotherapy. Thromb Res. 2010;126(2):113–118. doi:10.1016/j.thromres.2010.05.012
32. Ambrus JL, Ambrus CM, Mink IB, et al. Causes of death in cancer patients. J Med. 1975;6(1):61–64.
33. Martino MA, Williamson E, Siegfried S, et al. Diagnosing pulmonary embolism: experience with spiral CT pulmonary angiography in gynecologic oncology. Gynecol Oncol. 2005;98(2):289–293. doi:10.1016/j.ygyno.2005.04.020
34. Lyman GH, Culakova E, Poniewierski MS, et al. Morbidity, mortality and costs associated with venous thromboembolism in hospitalized patients with cancer. Thromb Res. 2018;164(Suppl 1):S112–s118. doi:10.1016/j.thromres.2018.01.028
35. Streiff MB. Thrombosis in the setting of cancer. Hematology Am Soc Hematol Educ Program. 2016;2016(1):196–205. doi:10.1182/asheducation-2016.1.196
36. Lefebvre P, Laliberté F, Nutescu EA, et al. All-cause and disease-related health care costs associated with recurrent venous thromboembolism. Thromb Haemost. 2013;110(6):1288–1297. doi:10.1160/TH13-05-0425
37. Lyman GH, Eckert L, Wang Y, et al. Venous thromboembolism risk in patients with cancer receiving chemotherapy: a real-world analysis. Oncologist. 2013;18(12):1321–1329. doi:10.1634/theoncologist.2013-0226
38. Seaman S, Nelson A, Noble S. Cancer-associated thrombosis, low-molecular-weight heparin, and the patient experience: a qualitative study. Patient Prefer Adherence. 2014;8:453–461. doi:10.2147/PPA.S58595
39. Noble S, Prout H, Nelson A. Patients’ Experiences of LIving with CANcer-associated thrombosis: the PELICAN study. Patient Prefer Adherence. 2015;9:337–345. doi:10.2147/PPA.S79373
40. Font C, Nelson A, Garcia-Fernandez T, et al. Patients’ Experience of Living with Cancer-associated thrombosis in Spain (PELICANOS). Support Care Cancer. 2018;26(9):3233–3239. doi:10.1007/s00520-018-4174-5
41. Connolly GC, Dalal M, Lin J, et al. Incidence and predictors of venous thromboembolism (VTE) among ambulatory patients with lung cancer. Lung Cancer. 2012;78(3):253–258. doi:10.1016/j.lungcan.2012.09.007
42. Khorana A, Dalal MR, Lin J, Connolly GC. Health care costs associated with venous thromboembolism in selected high-risk ambulatory patients with solid tumors undergoing chemotherapy in the United States. Clinicoecon Outcomes Res. 2013;5:101–108.
43. Cohoon KP, Ransom JE, Leibson CL, et al. Direct medical costs attributable to cancer-associated venous thromboembolism: a population-based longitudinal study. Am J Med. 2016;129(9):
44. Khorana A, McCrae KR, Milentijevic D, et al. Healthcare resource utilization and costs associated with venous thromboembolism recurrence in patients with cancer. J Med Econ. 2020;23(4):323–329. doi:10.1080/13696998.2019.1703190
45. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
46. Prandoni P, Lensing AWA, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–3488. doi:10.1182/blood-2002-01-0108
47. Hutten BA, Prins MH, Gent M, et al. Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio: a retrospective analysis. J Clin Oncol. 2000;18(17):3078–3083. doi:10.1200/JCO.2000.18.17.3078
48. Hull RD, Garcia DA, Vazquez SR. Warfarin and other VKAs: dosing and adverse effects; 2019. Available from: https://www.uptodate.com/contents/warfarin-and-other-vkas-dosing-and-adverse-effects.
49. Mulloy B, Hogwood J, Gray E, et al. Pharmacology of heparin and related drugs. Pharmacol Rev. 2016;68(1):76–141. doi:10.1124/pr.115.011247
50. Farge D, Bounameaux H, Brenner B, et al. International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2016;17(10):e452–e466. doi:10.1016/S1470-2045(16)30369-2
51. Sanfilippo KM, Wang TF. Prevention and treatment of cancer-associated venous thromboembolism: a review. Curr Treat Options Cardiovasc Med. 2019;21(11):70. doi:10.1007/s11936-019-0764-x
52. Woodruff S, Feugère G, Abreu P, et al. A post hoc analysis of dalteparin versus oral anticoagulant (VKA) therapy for the prevention of recurrent venous thromboembolism (rVTE) in patients with cancer and renal impairment. J Thromb Thrombolysis. 2016;42(4):494–504. doi:10.1007/s11239-016-1386-8
53. Young AM, Marshall A, Thirlwall J, et al. Comparison of an oral factor xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol. 2018;36(20):2017–2023. doi:10.1200/JCO.2018.78.8034
54. Terrace L. Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project. Qual Saf Health Care. 2003;12(1):18–23. doi:10.1136/qhc.12.1.18
55. Smrke A, Gross PL. Cancer-associated venous thromboembolism: a practical review beyond low-molecular-weight heparins. Front Med. 2017;4:142. doi:10.3389/fmed.2017.00142
56. Khorana AA, McCrae KR, Milentijevic D, et al. Current practice patterns and patient persistence with anticoagulant treatments for cancer-associated thrombosis. Res Pract Thromb Haemost. 2017;1(1):14–22. doi:10.1002/rth2.12002
57. Mekaj YH, Mekaj Y, Duci S, et al. New oral anticoagulants: their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events. Ther Clin Risk Manag. 2015;11:967–977. doi:10.2147/TCRM.S84210
58. Wittkowsky AK. Barriers to the long-term use of low-molecular weight heparins for treatment of cancer-associated thrombosis. J Thromb Haemost. 2006;4(9):2090–2091. doi:10.1111/j.1538-7836.2006.02073.x
59. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. doi:10.1056/NEJMoa0906598
60. Schulman S, Kakkar AK, Goldhaber SZ, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–772. doi:10.1161/CIRCULATIONAHA.113.004450
61. Einstein–PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287–1297.
62. Einstein Investigators. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–2510.
63. Hokusai-VTE Investigators. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–1415.
64. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799–808. doi:10.1056/NEJMoa1302507
65. Raskob GE, van Es N, Segers A, et al. Edoxaban for venous thromboembolism in patients with cancer: results from a non-inferiority subgroup analysis of the Hokusai-VTE randomised, double-blind, double-dummy trial. Lancet Haematol. 2016;3(8):e379–87. doi:10.1016/S2352-3026(16)30057-6
66. Schulman S, Goldhaber SZ, Kearon C, et al. Treatment with dabigatran or warfarin in patients with venous thromboembolism and cancer. Thromb Haemost. 2015;114(1):150–157. doi:10.1160/TH14-11-0977
67. Prins MH, Lensing AW, Brighton TA, et al. Oral rivaroxaban versus enoxaparin with vitamin K antagonist for the treatment of symptomatic venous thromboembolism in patients with cancer (EINSTEIN-DVT and EINSTEIN-PE): a pooled subgroup analysis of two randomised controlled trials. Lancet Haematol. 2014;1(1):e37–46. doi:10.1016/S2352-3026(14)70018-3
68. Carrier M, Cameron C, Delluc A, et al. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer-associated thrombosis: a systematic review and meta-analysis. Thromb Res. 2014;134(6):1214–1219. doi:10.1016/j.thromres.2014.09.039
69. van der Hulle T, den Exter PL, Kooiman J, et al. Meta-analysis of the efficacy and safety of new oral anticoagulants in patients with cancer-associated acute venous thromboembolism. J Thromb Haemost. 2014;12(7):1116–1120. doi:10.1111/jth.12605
70. Raskob GE, van Es N, Verhamme P, et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N Engl J Med. 2018;378(7):615–624. doi:10.1056/NEJMoa1711948
71. McBane RD, Wysokinski WE, Le-Rademacher JG, et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: the ADAM VTE trial. J Thromb Haemost. 2020;18(2):411–421. doi:10.1111/jth.14662
72. Agnelli G, Becattini C, Meyer G, et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N Engl J Med. 2020;382(17):1599–1607. doi:10.1056/NEJMoa1915103
73. Guideline on clinical investigation of medicinal products for the treatment of venous thromboembolic disease; 2021. Available from: https://www.ema.europa.eu/en/documents/regulatory-procedural-guide-line/guideline-clinical-investigation-medicinal-products-treatment-venous-thromboembolic-disease_en.pdf.
74. Vedovati MC, Germini F, Agnelli G, et al. Direct oral anticoagulants in patients with VTE and cancer: a systematic review and meta-analysis. Chest. 2015;147(2):475–483. doi:10.1378/chest.14-0402
75. Giustozzi M, Agnelli G, del Toro-Cervera J, et al. Direct oral anticoagulants for the treatment of acute venous thromboembolism associated with cancer: a systematic review and meta-analysis. Thromb Haemost. 2020;120(7):1128–1136. doi:10.1055/s-0040-1712098
76. Dong S, Zhang Y, Li Y, et al. Direct oral anticoagulant for the treatment of VTE in cancer patients: a systematic review and meta-analysis. Ann Pharmacother. 2021;55(4):430–439. doi:10.1177/1060028020960037
77. Chen D, Tseng C-N, Hsieh M-J, et al. Comparison between non-vitamin K antagonist oral anticoagulants and low-molecular-weight heparin in asian individuals with cancer-associated venous thromboembolism. JAMA Netw Open. 2021;4(2):e2036304. doi:10.1001/jamanetworkopen.2020.36304
78. Streiff MB, Milentijevic D, McCrae K, et al. Effectiveness and safety of anticoagulants for the treatment of venous thromboembolism in patients with cancer. Am J Hematol. 2018;93(5):664–671. doi:10.1002/ajh.25059
79. Alzghari SK, Seago SE, Garza JE, et al. Retrospective comparison of low molecular weight heparin vs. warfarin vs. oral Xa inhibitors for the prevention of recurrent venous thromboembolism in oncology patients: the Re-CLOT study. J Oncol Pharm Pract. 2018;24(7):494–500. doi:10.1177/1078155217718382
80. Nicklaus MD, Ludwig SL, Kettle JK. Recurrence of malignancy-associated venous thromboembolism among patients treated with rivaroxaban compared to enoxaparin. J Oncol Pharm Pract. 2018;24(3):185–189. doi:10.1177/1078155217690922
81. Ross JA, Miller MM, Rojas Hernandez CM. Comparative effectiveness and safety of direct oral anticoagulants (DOACs) versus conventional anticoagulation for the treatment of cancer-related venous thromboembolism: a retrospective analysis. Thromb Res. 2017;150:86–89. doi:10.1016/j.thromres.2016.12.016
82. Uppuluri EM, Burke KR, Haaf CM, et al. Assessment of venous thromboembolism treatment in patients with cancer on low molecular weight heparin, warfarin, and the direct oral anticoagulants. J Oncol Pharm Pract. 2019;25(2):261–268. doi:10.1177/1078155217730129
83. Bavalia R, Middeldorp S, Weisser G, et al. Treatment of venous thromboembolism in special populations with direct oral anticoagulants. Thromb Haemost. 2020;120(6):899–911. doi:10.1055/s-0040-1710314
84. Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–992. doi:10.1056/NEJMoa1107039
85. Riess H, Prandoni P, Harder S, et al. Direct oral anticoagulants for the treatment of venous thromboembolism in cancer patients: potential for drug-drug interactions. Crit Rev Oncol Hematol. 2018;132:169–179. doi:10.1016/j.critrevonc.2018.09.015
86. Streiff MB, Holmstrom B, Angelini D, et al. NCCN guidelines insights: cancer-associated venous thromboembolic disease, version 2.2018. J Natl Compr Canc Netw. 2018;16(11):1289–1303. doi:10.6004/jnccn.2018.0084
87. Lyman GH, Bohlke K, Khorana AA, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American society of clinical oncology clinical practice guideline update 2014. J Clin Oncol. 2015;33(6):654–656. doi:10.1200/JCO.2014.59.7351
88. Mazzolai L, Aboyans V, Ageno W, et al. Diagnosis and management of acute deep vein thrombosis: a joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function. Eur Heart J. 2018;39(47):4208–4218. doi:10.1093/eurheartj/ehx003
89. Khorana AA, Noble S, Lee AYY, et al. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: guidance from the SSC of the ISTH. J Thromb Haemost. 2018;16(9):1891–1894. doi:10.1111/jth.14219
90. NCCN guideline on cancer-associated venous thromboembolic disease; 2021. Available from: https://www.nccn.org/professionals/physician_gls/pdf/vte.pdf.
91. Stockler MR. ASCO updated recommendations for preventing and treating VTE in adults with cancer. Ann Intern Med. 2020;172(2):Jc2. doi:10.7326/ACPJ202001210-002
92. Mahé I, Chidiac J, Helfer H, et al. Factors influencing adherence to clinical guidelines in the management of cancer-associated thrombosis. J Thromb Haemost. 2016;14(11):2107–2113. doi:10.1111/jth.13483
93. de Jong L, van der Velden AWG, Hulst MV, et al. Cost-effectiveness analysis and budget impact of rivaroxaban compared with dalteparin in patients with cancer at risk of recurrent venous thromboembolism. BMJ open. 2020;10(11):e039057. doi:10.1136/bmjopen-2020-039057
94. Lopes DG, Tamayo A, Schipp B, et al. Cost-effectiveness of edoxaban vs low-molecular-weight heparin and warfarin for cancer-associated thrombosis in Brazil. Thromb Res. 2020;196:4–10. doi:10.1016/j.thromres.2020.08.014
95. Li A, Manohar PM, Garcia DA, et al. Cost effectiveness analysis of direct oral anticoagulant (DOAC) versus dalteparin for the treatment of cancer associated thrombosis (CAT) in the United States. Thromb Res. 2019;180:37–42. doi:10.1016/j.thromres.2019.05.012
96. Connell NT, Connors JM. Cost-effectiveness of edoxaban versus dalteparin for the treatment of cancer-associated thrombosis. J Thromb Thrombolysis. 2019;48(3):382–386. doi:10.1007/s11239-019-01903-z
97. Wumaier K, Li W, Chen N, et al. Direct oral anticoagulants versus low molecular weight heparins for the treatment of cancer-associated thrombosis: a cost-effectiveness analysis. Thromb J. 2021;19(1):68. doi:10.1186/s12959-021-00319-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.