")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
New Insights into Activities of Daily Living Performance in Chronic Obstructive Pulmonary Disease
Authors Kaptain RJ , Helle T, Patomella AH , Weinreich UM , Kottorp A
Received 5 June 2020
Accepted for publication 11 December 2020
Published 7 January 2021 Volume 2021:16 Pages 1—12
DOI https://doi.org/10.2147/COPD.S264365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Russell
Rina Juel Kaptain,1,2 Tina Helle,1,2 Ann-Helen Patomella,2 Ulla Møller Weinreich,3,4 Anders Kottorp2,5
1Department of Occupational Therapy, University College of Northern Denmark, Aalborg, Denmark; 2Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Stockholm, Sweden; 3Department of Respiratory Diseases, Aalborg University Hospital, Aalborg, Denmark; 4The Clinical Institute, Aalborg University, Aalborg, Denmark; 5Faculty of Health and Society, Malmö University, Malmö, Sweden
Correspondence: Rina Juel Kaptain Selma Lagerloefs Vej 2, Aalborg 9220, Denmark
Tel +4572690928
Email [email protected]
Purpose: There have been calls for more knowledge of activities of daily living (ADL) performance in order to address interventions in pulmonary rehabilitation effectively. Everyday technology (ET) has become an integrated dimension of ADL, impacting the ways in which ADL is performed. To improve everyday functioning and quality of life, the use of ADL and ET use needs to be evaluated and addressed effectively in interventions. Therefore, the aim of this study was twofold: 1) to explore the quality of ADL performance, and 2) to investigate the relationship between observation and self-reported ADL performance and ability to use everyday technologies in people living with COPD.
Methods: This cross-sectional study involved 84 participants aged 46– 87 years. Participants were recruited through healthcare centres in the Northern Region of Denmark using a convenience sampling procedure. Data were collected using standardized assessments that investigated different ADL perspectives: self-reported ADL tasks and ET use, observed motor and process ability, and need for assistance. Data were analysed and presented using descriptive statistics and Pearson’s correlation coefficient.
Results: The most affected ADL tasks were mobility within or outside the home, lower dressing, bathing, pedicuring, cooking, shopping, cleaning and washing clothes. New insights into the quality of ADL performance in people living with COPD were presented in terms of detailed ADL motor skills and ADL process skills, as well as the predicted need for support to function in the community. Moreover, new insights into the relationship between observation and self-reported ADL performance (r=0.546, p< 0.01; r=0.297, p< 0.01) and between ADL performance and self-perceived ability to use ET (r=0.524, p< 0.01; r=0.273, p< 0.05; r=0.044, p=0.692) were presented.
Conclusion: Overall, the knowledge from the present study is valuable for focusing interventions that address challenging ADL performance and ET use through relevant and realistic activities. The ability to use ET is important to evaluate and target pulmonary rehabilitation.
Keywords: ADL skills, AMPS, everyday technology, occupational therapy, pulmonary rehabilitation
Introduction
The ability to perform activities of daily living (ADL) often diminishes in individuals living with chronic obstructive pulmonary disease (COPD) due to ongoing symptoms such as breathlessness and fatigue.1–3 ADL is specified as tasks relevant for independent living and covers basic needs such as eating, showering and dressing, as well as more complex tasks such as transportation, shopping, cleaning and cooking.4,5 Everyday technology (ET) has an increasing impact on our everyday lives.6,7 ET refers here to mechanical, electronic and digital artifacts and services, often used on a daily basis and integrated in ADL, such as a microwave, GPS, ticket machines or mobile phones,8,9 and has been studied with growing interest in recent years.10–15 Also, literature of ET supporting health management among patients with COPD has expanded;15–19 however, the ability to use ET may be influenced by lacking confidence, lacking skills or little motivation or interest in using the technology.15,17 The use of ET is still not an integrated part of rehabilitation, and this can generate gaps between those who can use ET and those who cannot.7 ET is complex to integrate and integration of ET in rehabilitation requires health professionals staying updated and daring to take new challenges; however, focusing on ET makes it possible to support the benefits of digitalization.7 Since the ability to perform ADL and use ET are associated with health-related quality of life in people living with COPD,20 it is of critical importance to investigate ADL performance including ET use in order to support the development of interventions that could be integrated in pulmonary rehabilitation.
National and international COPD guidelines and policy statements acknowledge the importance of ADL, and include increased participation in everyday activities within the goals of pulmonary rehabilitation.1,21 However, evidence is sparse regarding how to target pulmonary rehabilitation to ADL.21 The Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances In Pulmonary Rehabilitation1 emphasizes the need for specific knowledge about individualized measures of daily activity limitations, and observation of ADL tasks receives particular mention.1
For healthcare professionals to be able to address ADL and ET use in interventions, evaluations are necessary. The COPD literature reveals that when applying ADL assessments, the concept measured differs. In a review by Paes et al,22 ADL assessments focusing on observation-based ADL were investigated. However, in this review, the constructs measured were primarily time spent during simulated tasks and the number of laps when performing either simulated tasks or functional exercises.22 This type of assessment measures the physical capacity that influences ADL, but does not measure ADL performance. As a supplement to the physical capacity measures, there is a need for assessments that focus on the activities performed, are self-nominated and take place in the home environment23 that can support understanding of the individual ADL challenges that people living with COPD encounter. This is necessary in order to plan specific individual interventions that focus directly on ADL performance and not on the underlying physical components. The assessments of ADL performance and ability to use ET applied in this study focus on the actual performance of specific activities and still demonstrate evidence of validity and reliability when used by individuals with COPD.
A review found that ADL assessments used in people with COPD employed several modes and variations of which most are self-reported, and only a few are observation based.23 Self-reported questionnaires are often preferred as they are simpler and less time-consuming to use. However, self-reporting may be affected by memory or the adaptation strategies developed over time in people living with COPD resulting in inaccurate reporting of performance.24,25 To achieve a thorough evaluation of ADL performance, a combination of self-reporting and observation is therefore recommended.5,26 The relationship between self-reporting and observation in ADL performance and ET use has been investigated among client groups with chronic diseases, and relationships from non-existent to moderate were found.27–30 However, to our knowledge, similar studies of concurrent ADL assessments have not been performed among people with COPD, and it is relevant to recommend to both clinicians and researchers which is appropriate.
In summary, more knowledge of ADL performance is needed, and there have been calls for observations of people with COPD performing ADL.1,23 Details of ADL performance are essential in order to be able to address interventions effectively in people living with COPD so as to improve everyday functioning and independence, and thus influence quality of life.20 Therefore, this study has a twofold aim: 1) to explore observed and self-reported ADL performance, and 2) to investigate the relationship between observation and self-reporting when evaluating ADL performance and between observed/self-reported ADL performance and the ability to use ET in people living with COPD.
Materials and Methods
Design and Sample
This cross-sectional study involves participants (N=84) aged 46–87 years who were recruited through healthcare centres in the Northern Region of Denmark using a convenience sampling procedure.31 To be eligible for inclusion, participants had to be registered with COPD as their primary diagnosis within primary healthcare. The diagnosis was determined by the general practitioner or at hospital, with spirometry as an important indicator and according to GOLD 1–4.32 Participants were excluded from participation if they were (i) unable to understand Danish sufficiently to answer the questions, (ii) if they were living in nursing homes and (iii) if they had a diagnosed cognitive impairment or visual or hearing impairment that could not be compensated for by technical aids. Nurses at the healthcare centres were informed about the inclusion and exclusion criteria; they asked potential participants if they would receive a telephone call from the head of the project (TH) or project coordinator (RJK). The inclusion and exclusion criteria were verified when the participants were contacted.
Instrumentation
Self-Reported ADL Performance
For data gathering, the standardized ADL-Interview (ADL-I)33 was used as it is found to be reliable and valid,34 also in persons with COPD.3 ADL-I is an occupational therapy assessment instrument that measures the quality of ADL performance based on self-reporting during interviews.34 The participants were asked to rate their performance on 47 ADL tasks that related to both personal ADL (PADL) and instrumental ADL (IADL). When rating the performance of each task, the answer was based on a seven-category (a-g) rating scale reflecting efficiency, effort/fatigue, safety and independence. If the person found the task irrelevant to his or her daily life, the task was marked “not relevant”34
Observed ADL Performance
The Assessment of Motor and Process Skills (AMPS)5 is a standardized assessment tool for measuring the observed quality of a person´s ADL performance. The AMPS is internationally recognized, valid and reliable, and has been used in persons with and without a diagnosis, including a diagnosis of COPD, and across ages and genders.5 The AMPS can be used by occupational therapists or occupational therapy students who have completed a training course and are calibrated as reliable raters.5 The calibration process in the AMPS training provides evidence that each rater demonstrates stability in his/her scorings (intra-rater reliability) as well as information to adjust for each unique rater’s severity when estimating the ADL performance measures in the AMPS software.5
When performing an AMPS evaluation, the client selects from a list of standardized tasks at least two standardised ADL tasks with which he/she is well acquainted and which are relevant to his/her everyday life and appropriate in terms of severity. The occupational therapist then observes the tasks performed and evaluates the quality of the ADL performance by scoring 16 ADL motor skills and 20 ADL process skills according to physical effort, efficiency, safety and independence on a four-point criterion-referenced scale, ranging from (4) Competent to (1) Unacceptable.35 Through the generated measures of ADL motor and ADL process ability, the need for assistance to live in the community can be predicted based on established cut-off values.36
Ability to Use Everyday Technology
The Everyday Technology Use Questionnaire (ETUQ) is an evaluation of the individual’s perceived ability to use various types of ETs at home and in public places.37 The ETUQ has previously demonstrated psychometric evidence of validity and precision/reliability.38–40 The ETUQ utilized in this study has been translated into Danish and has demonstrated validity and excellent test-retest and inter-rater reliability in older adults with and without chronic diseases, including COPD.41
The administration of the ETUQ was completed through a structured face-to-face interview that first involved assessing whether each of the 93 ETs was relevant for the person’s current life situation. If so, the extent of the person’s possibly perceived difficulties in using the ET in question was explored and their ability to use ET was indicated. Ratings were marked according to an ordinal five-category rating scale.37
Procedures
To prepare for data collection, five occupational therapists were trained in using the ADL-I and the ETUQ by the developers of the instruments. Furthermore, they were taught by an expert from Aalborg University how to use the Vitalograph COPD-6 (Vitalograph Ltd, Buckingham, United Kingdom) according to the standardization of spirometry of the American Thoracic Society and the European Respiratory Society.32,42 As the spirometry was intended for evaluating current disease severity only, no reversibility test was done.42,43 Data collection was conducted at two home visits at an interval of one to three weeks during a total period of ten months. The first home visit was completed by one of the occupational therapists, first orally informing the participants about the study aim and providing them with an information letter, after which written consent was obtained. Then, a simple measurement of lung function (forced expiratory volume (FEV) 1% predicted) using the Vitalograph COPD-6 was obtained, and information regarding sample characteristics was collected before the ADL-I and ETUQ were performed. Based on the gathered information and in collaboration with the participant, it was decided which two AMPS tasks the participant should perform at the second home visit. The second home visit was completed by one of ten occupational therapy students who had been trained and calibrated in performing the AMPS and thoroughly introduced to data collection procedures.
Data Analysis
Preparatory Analysis
To explore ADL performance and ability to use ET data were prepared for analysis. We used a procedure in line with previous studies when analysing and presenting data from ADL-I.30,34 Data on the observed ADL performance were initially used for descriptive analysis using the ordinal scores of the 16 ADL motor skills and 20 ADL process skills. Furthermore, Rasch rating scale models44 was used to convert the raw scores from the ADL-I, AMPS and ETUQ into individual interval measures of self-reported ADL performance, ADL motor ability, ADL process ability and ability to use ET using the WINSTEPS computer software program version 3.69.145 and AMPS computer-scoring software.5 These procedures are described in detail elsewhere.5,29,34,39,46
Categorical variables were presented as frequencies and percentages (%), while continuous variables (self-reported ADL performance, ADL motor ability, ADL process ability and ET use) were tested and met criteria for normality. These variables were presented as mean, standard deviations (SD) and minimum/maximum scores. All statistics were performed using the Statistical Package for the Social Sciences (SPSS) Statistics Version 26 (IBM Corp., New York, United States).
Primary Analysis
The self-reported ADL performance was presented by the frequencies of each of the 47 ADL tasks according to the ordinal scale. The ADL motor and ADL process skills were arranged by the calculated mean and SD of each skill indicating the level of challenge within this sample.
To further explore ADL performance, ADL motor ability and ADL process ability measures were matched according to the evidence-based cut-off measures by Fisher5 and Merrit36 of 1.5 logit (motor) and 1.0 logit (process). These cut-off measures were used to predict the potential need for assistance to live in the community. Persons with both measures above the cut-offs are likely to be independent in the community, and persons with both measures below the cut-offs are likely to need assistance to live in the community.5 When ADL motor and ADL process measures do not match in relation to the cut-off criteria, the ADL process ability cut-off is suggested as applicable when determining the potential need for assistance.5
Finally, to investigate the relationship between self-reported and observed ADL performance and ET use, the Pearson correlation coefficient (r)47 was calculated. The following measures were included: self-reported ADL performance (ADL-I), ADL motor ability (AMPS), ADL process ability (AMPS) and ability to use ET (ETUQ). The strength of the correlation coefficient was judged according to Munro, cited by Domholt48 (0.00–0.25 = little, if any correlation, 0.26–0.49 = low correlation, 0.50–0.69 = moderate correlation, 0.70–0.89 = high correlation, 0.90–1.00 = very high correlation). For interpretation, the shared variance (R2) was calculated by squaring r and to express as a percentage (%), multiplied by 100.40 P-values < 0.05 were considered statistically significant.
Results
For this study, 100 participants were initially recruited and 84 were included in the final analyses because of internal dropouts due to absent AMPS evaluations (Figure 1). The characteristics of the study participants are shown in Table 1.
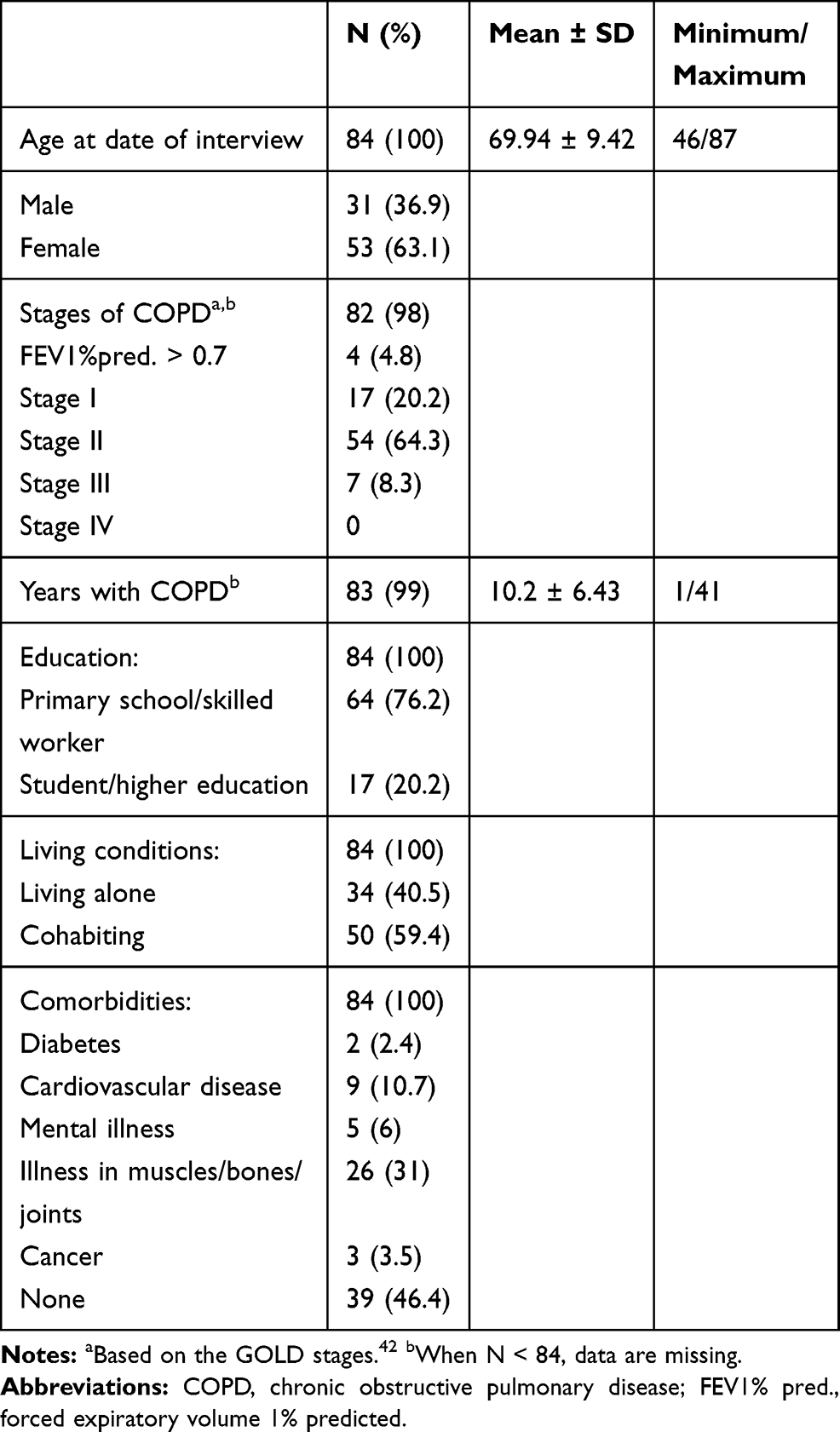 |
Table 1 Characteristics of the Study Participants (N=84) |
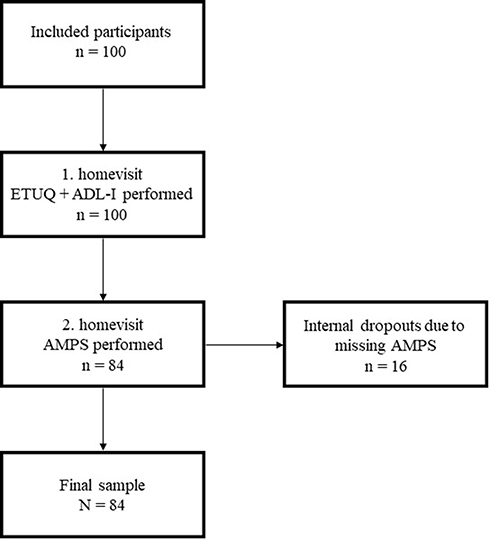 |
Figure 1 Flow chart of the data collection process. Abbreviations: ADL-I, activities of daily living – interview; AMPS, Assessment of Motor and Process Skills; ETUQ, Everyday Technology Use Questionnaire. |
Measures of self-reported ADL performance, ADL motor ability and ADL process ability based on observation, and self-perceived ability to use ET are presented in Table 2.
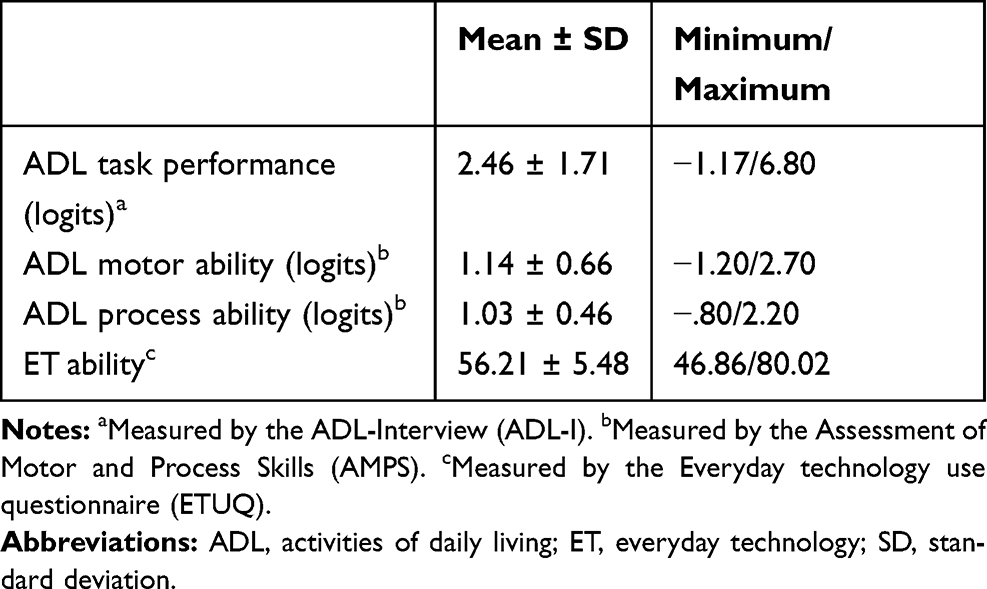 |
Table 2 Measures of ADL Task Performance, ADL Motor Ability, ADL Process Ability and Ability to Use ET (N=84) |
Self-Reported ADL Performance
The PADL tasks that were reported as being most affected related to moving around within or outside the home (eg, walking on stairs or walking outside), lower dressing, bathing and pedicuring (Figure 2). The IADL tasks most participants reported as affected were transportation outside home (eg, by train or driving a car), cooking, shopping, cleaning and washing clothes (Figure 3).
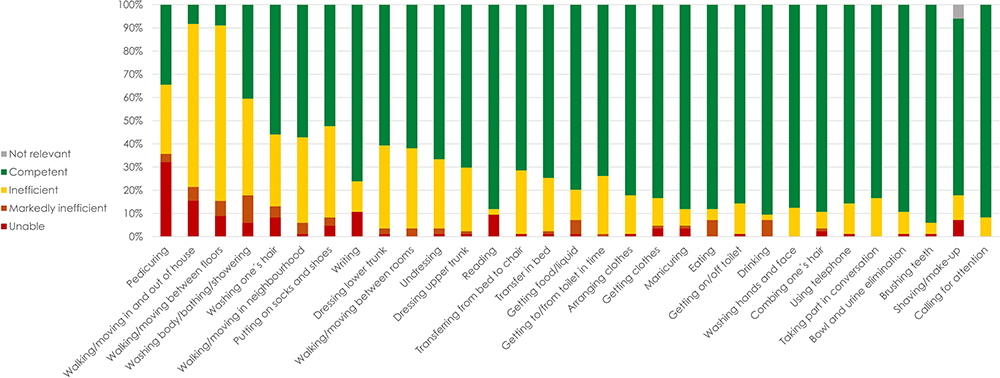 |
Figure 2 PADL tasks most affected to least affected in performance among participants with COPD when measured using the ADL-I. |
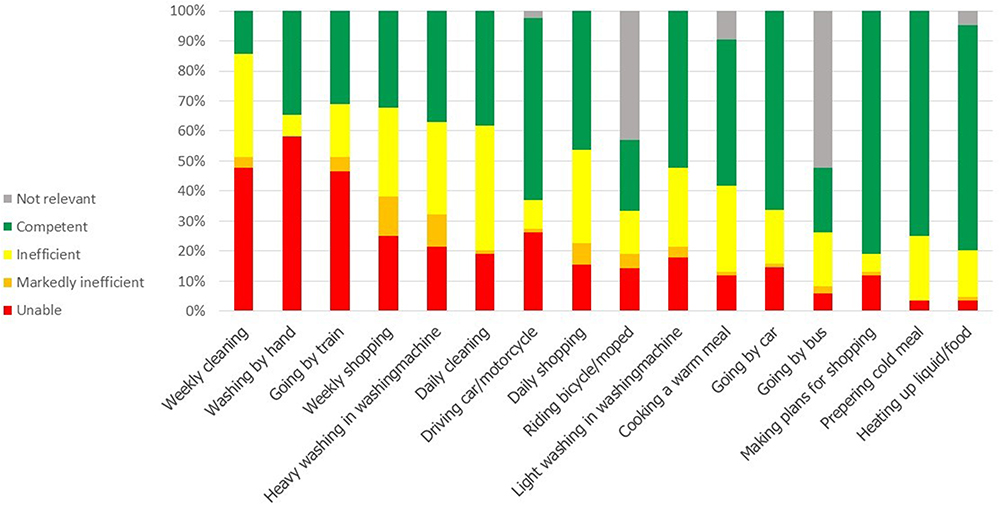 |
Figure 3 IADL tasks most affected to least affected in performance among participants with COPD when measured using the ADL-I. |
Observed ADL Performance
The ADL motor skills and ADL process skills with the highest means indicate the ADL skills that participants perform with greater ease (primarily related to ADL motor skills), and more efficiently, safely and independently (primarily related to ADL process skills) (Table 3). The lower scores indicate the ADL skills observed as being more challenging, using increased effort, as being more inefficient or unsafe, or requiring assistance.5,35 The most challenging ADL motor skills involved positioning their body effectively when interacting with task objects (Positions 2.07). Participants also demonstrated problems in stabilizing themselves effectively while walking or interacting with objects, also indicated by the need to walk with assistive devices (Stabilizes 2.32). They also demonstrated the need to pause to rest or demonstrated shortness of breath during task performance (Endures 2.48). Furthermore, increased effort was demonstrated when bending (Bends 2.55) or reaching for task objects (Reaches 2.49), also resulting in extra use of time. The most challenging ADL process skills were observed in an overall slow task performance or a performance that became slower during task progression (Paces 2.71). Participants also demonstrated problems in navigating their arms or body in the environment, resulting in bumping into furniture with their body or bumping their arm/hand into a jar on the table (Navigates 2.60). Problems also occurred in working effectively in a crowded workspace (Organizes 2.27). Finally, participants demonstrated consistent problems that could not be overcome by changing their methods or performance strategy (Accommodates 1.82). Several of the observed problems also remained throughout the task performance and included not changing methods that were ineffective (Benefits 1.99).35 Examples of AMPS ADL tasks often selected by the participants in the present study were Vacuuming – moving no or lightweight furniture, Putting away clean dishes from a dishwasher or Making a pot of coffee or tea.
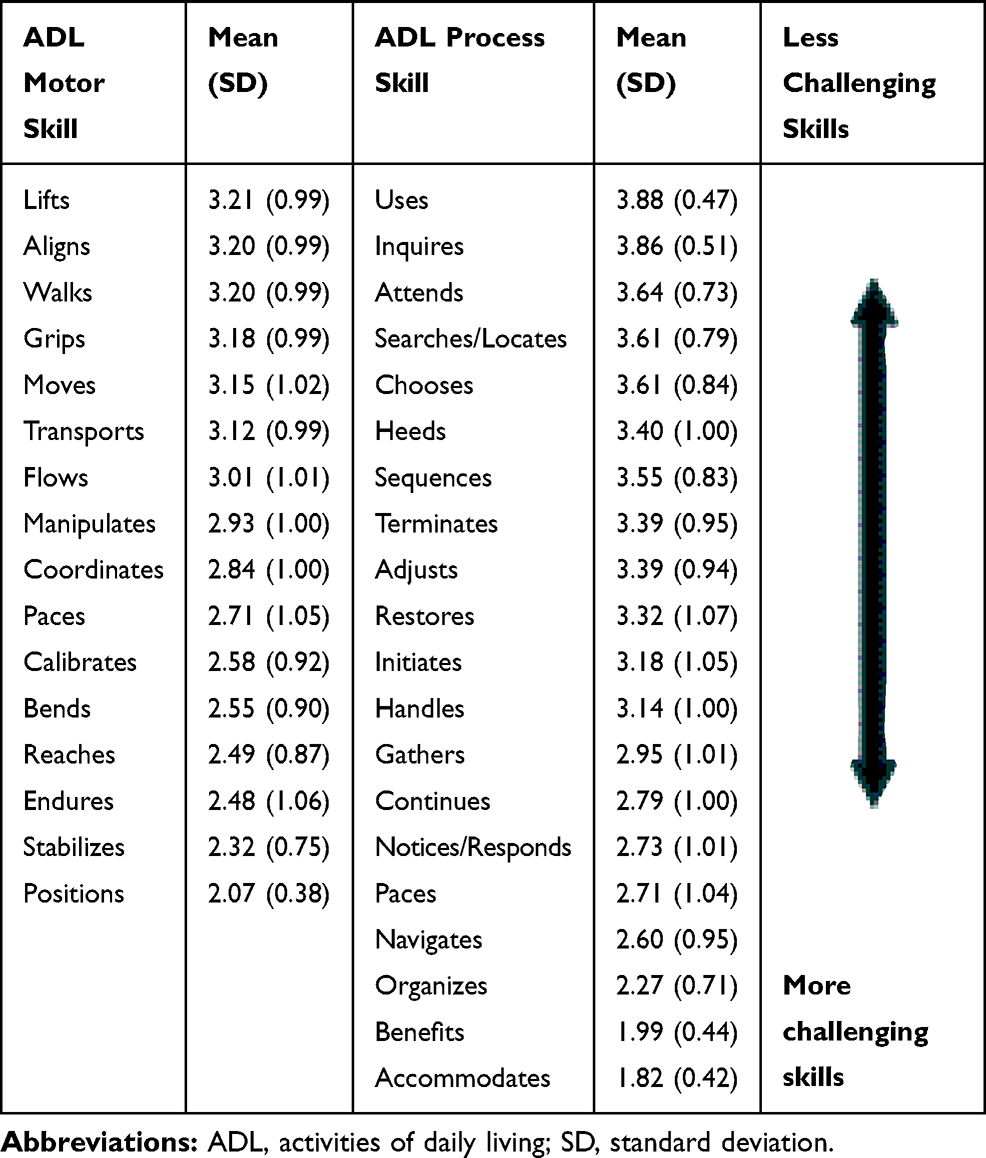 |
Table 3 Distribution of ADL Motor Skills and ADL Process Skills According to Mean Measures Based on Raw Scores. Each Participant Completed Two ADL Tasks, Meaning That Each Measure is Based on n=168 Scorings |
Predicted Need for Support to Function in the Community
Based on the ADL motor ability and ADL process ability measures the results presented in Table 4 indicate that n=23 (27.4%) of the participants in this study are potentially capable of functioning independently in the community; n=31 (36.9%) may need assistance to live in the community. Finally, 33.3% (n=28) are likely to be independent in the community; however, it is important to gather additional evidence as the ADL motor ability is below the cut-off measure.5
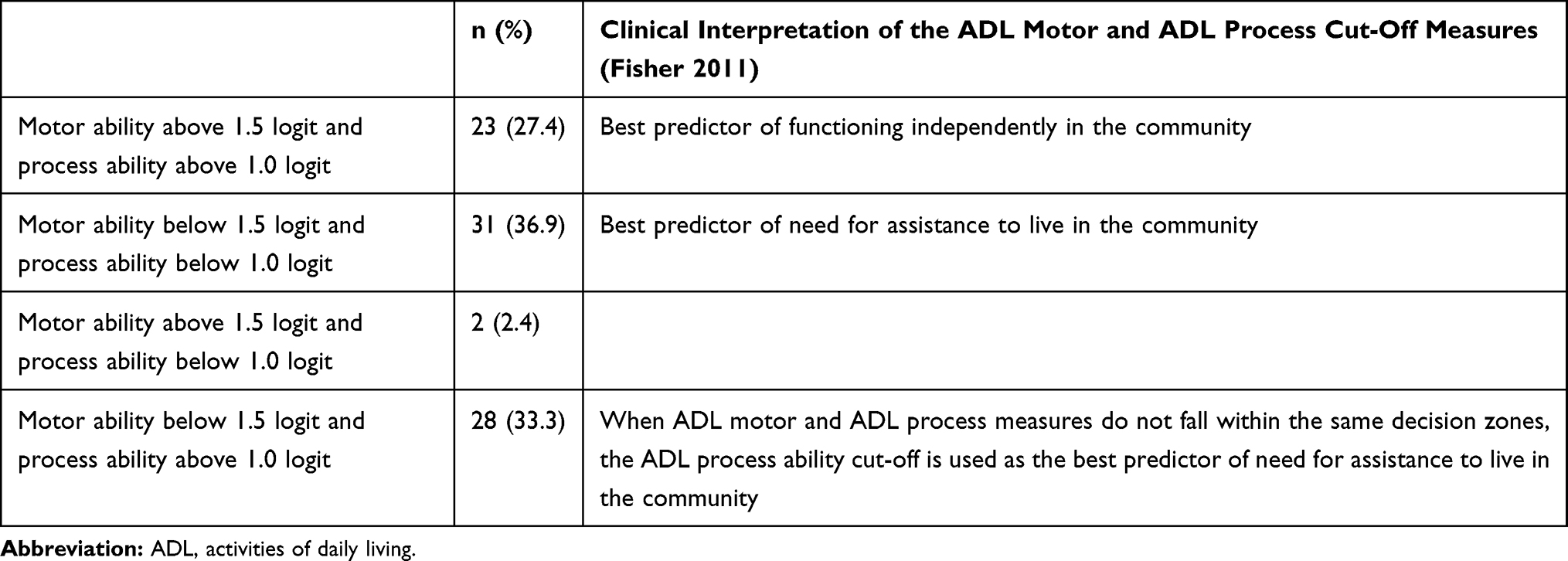 |
Table 4 Distribution of Matched Measures of ADL Motor Ability and ADL Process Ability According to Suggested Cut-Offs on the ADL Motor Ability Continuum (1.5 Logit) and the ADL Process Ability Continuum (1.0 Logit) (N=84) |
Self-Perceived Ability to Use Everyday Technology
For the self-perceived ability to use ET, the sample mean measure was 56.0 (Table 2). This exceeded the item mean difficulty (by default set at 50.0 logits) which indicates that the perceived ability to use ET in the sample was overall higher than the overall challenges encountered when using the ETs included in ETUQ. However, considering a standard deviation at 5.5 logits, approximately 20% of the sample have scores below 50.0 logits, indicating a diminished ability to use ET, as evaluated with the ETUQ.
The Relationship Between Observed and Self-Reported ADL Performance and Ability to Use Everyday Technology
The Pearson correlation coefficients revealed statistically significant moderate correlations in three pairs: (i) self-reported ADL performance and ADL motor ability with a shared variance of 29.8% (r=0.546, p < 0.001); (ii) self-reported ADL performance and ability to use ET with a shared variance of 27.5% (r=0.524, p < 0.001); and (iii) ADL motor ability and ADL process ability with a shared variance of 41.7% (r=0.646, p ≤ 0.001).
The Pearson correlation coefficients revealed statistically significant low correlations in two cases: 1) ADL motor ability and ability to use ET with a shared variance of 7.5% (r= 0.273, p=0.012); and 2) self-reported ADL performance and ADL process ability with a shared variance of 8.8% (r= 0.297, p=0.006).
The correlation coefficients between the last case of variables indicated “little, if any” relationship and were not statistically significant: ADL process ability and ability to use ET (Table 5).
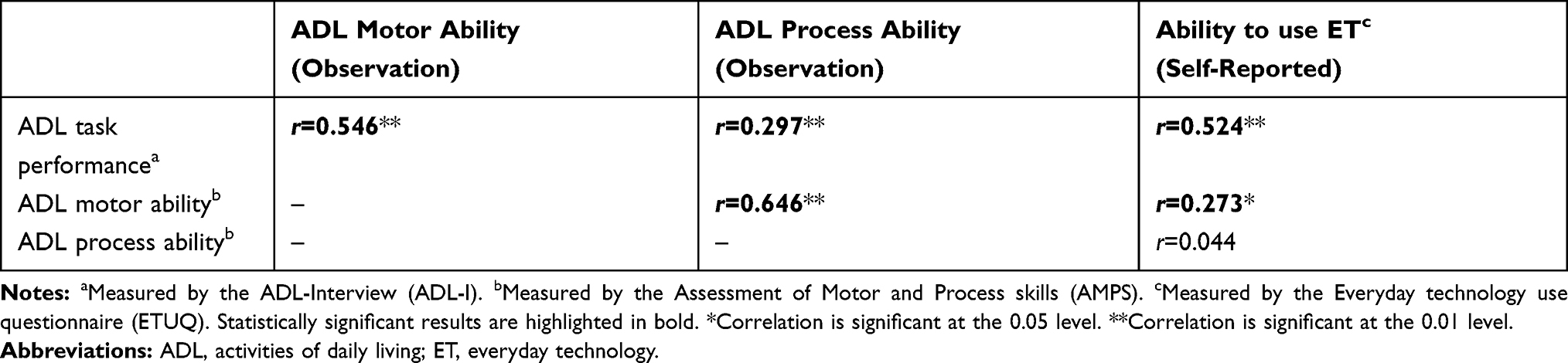 |
Table 5 Pearson Correlation of ADL Task Performance, ADL Motor Ability, ADL Process Ability and Ability to Use Everyday Technology (N=84) |
Ethical Considerations
This study was reported according to the Danish Data Protection Agency49 (GDPR reference number FOU-UU-2018-003) at the University College of Northern Denmark. According to Danish law, an ethical approval is only required if the project involves human biological material and not when conducting questionnaire surveys and interview research.50 The study complied in all aspects with the formal requirements for research on humans in Denmark50 and with the Declaration of Helsinki.51 Participants gave verbal and written consent immediately before data collection, where they were also informed that they could withdraw from the study at any time without any consequences. Participants were informed that the data would be anonymised and treated confidentially.
Discussion
When having explored ADL performance, this study presents new insights into both observed and self-reported ADL performance by presenting ADL performance skills and the following predicted need for support to function in the community when living with COPD. We have evaluated ADL performance with a specific focus on the ADL tasks and the ADL motor and process skills used when performing the tasks, not the underlying body functions. This has created a nuanced description of ADL performance by supplementing the exact observable ADL skills (motor and process) that are most challenging for COPD patients. Findings of the most affected ADL tasks based on self-report are overall in line with findings reported in earlier studies2,3 as mobility within or outside the home, lower dressing, bathing, pedicuring, cooking, shopping, cleaning and washing clothes. Moreover, new insights into the relationship between observation and self-reported ADL performance and self-perceived ability to use ET have been presented. The findings of the present study demonstrated low to moderate correlations indicating that the constructs evaluated are related, but still measure different aspects of functioning. This is in line with previous studies among people with chronic diseases.27–30
Given the overall physical fatigue and breathlessness affecting COPD patients,1 it is expected that ADL skills such as Paces and Endures are affected, even if the overall ADL performance is less affected. These symptoms generally slow down task progression, resulting in pauses, and they indirectly affect other ADL motor and ADL process skills.5 The skill items Reaches and Bends are also expected to be diminished, since arm and body movements are demanding for patients with COPD, and affect lung volume.52,53 The skill items Accommodates and Benefits are among the most challenging ADL process skills among the participants in this study. Accommodates and Benefits differ from the other ADL skills as they reflect the person’s ability to overcome the observed problems in ADL performance by changing or adapting his/her ADL performance. Accommodates and Benefits may be affected by both the physical fatigue and reduced cognitive function as seen among some patients with COPD.54,55 It is particularly problematic if these skills are challenged because this may prevent individuals from modifying actions effectively during the task to overcome the problems in performing the ADL task.
When addressing ADL performance in interventions, focus can be on a) compensation through adaptation in ADL tasks, b) developing ADL skills through performance of ADL, c) developing personal factors or body functions through performance of ADL, or through d) educational programs.5 A concrete (and simplified) example of integrating compensation through adaptive strategies through the knowledge gained about the challenged ADL motor and ADL process skills could be a re-organization in the kitchen, where the tools/utensils and materials used most often are placed on shelves and surfaces near the workspace and are easy to reach without having to bend the body. This intervention may then affect the quality and efficiency of certain ADL motor skills such as Reaches and Bends, which were generally more challenging skills for these participants. Such interventions may also impact on ADL process skills such as Organizes and Navigates. All ADL motor and ADL process skills are defined based on the quality of interaction between a person and his/her environment,5 and not his/her underlying capacities to reach and bend and plan/organize. The AMPS is a sensitive tool that targets quality when interacting with the environment in ADL tasks and could therefore also be used to detect changes in ADL performance, as a variety of interventions target the quality of performance and are not restricted only to addressing changes in the person’s capacities.
The integration of the AMPS skill items into research is undertaken with awareness as they are based on raw scores and are therefore not adjusted according to the difficulty of the ADL task performed, the skill item difficulty and rater severity as is the ADL ability measure.5 However, it is still relevant to investigate the challenged ADL motor and ADL process skills in research studies and use this concrete knowledge to focus targeted interventions. Based on the observed ADL ability measures, the results show that more than a third of the participants are likely to need assistance to live and function in the community. These particular participants demonstrate both ADL motor ability and ADL process ability below the expected cut-offs, which indicates that some COPD patients may need interventions even more focused on compensatory strategies and/or environmental adaptations and to less extend interventions focusing directly on restoration of body functions.3 Special attention is needed within pulmonary rehabilitation to reach patients with COPD that have several basic ADL limitations that include difficulty in getting around inside and outside their home. In contrast, one-third of the participants with affected ADL motor ability but higher ADL process ability are likely to be able to improve their overall ADL performance by changing their current strategies. The higher ADL process ability indicates greater potential to use and integrate adaptive strategies or benefit from environmental interventions integrated into their daily lives.5 A quarter of the participants are having both ADL motor and ADL process ability above the cut-offs and are likely to function independently in the community but may still need a focus on activities to prevent deterioration.
The statistically significant moderate correlation between self-reported ADL performance and observed ADL motor ability, indicate that constructs are related, but not similar, modes for data collection, when targeting increased effort in ADL performance. There are pros and cons in using self-reported evaluations. Self-report is important for getting the clients’ perspectives and experiences of strengths and problems in their everyday life.54,56 At the same time, these participants had their diagnosis for a mean of 10 years and had made continuing and often unconscious adaptations of performance according to their current ability.57 If they do not realise the decreased performance level and the engaging activities they let go of through the years, they may answer that they are managing their ADL independently and without increased effort.58 When their ADL performance is then observed, it may appear that their ADL performance is inefficient. Both self-reporting and observation are therefore suggested for an adequate evaluation. Self-reported evaluation indicates the clients’ perspectives on their own situation, whereas a standardized performance analysis such as the AMPS evaluates the effectiveness of ADL skills and can generate objective measures of the quality of ADL performance that are sensitive to change. Both evaluations are important when planning client-centred interventions, as they also take into consideration which ADL tasks that are relevant and important for the client to manage in his/her everyday life.34,35
The statistically significant moderate relationship between self-reported ADL performance and ET use indicates that the ability to perform ADL is related to individuals’ ability to use ET; however, as expected, the relationship is not complete as they are different constructs. Accordingly, the tasks reported in the ADL-I are related to both PADL and IADL tasks at home and in society, including tasks where ETs may be involved (eg, read/write on the computer, talk on the phone, transportation using an electronic travel card, cooking on the stove or by using the oven, washing in the washing machine, vacuuming, shopping on the internet or using a self-scanner). In the same manner, the ETs are evaluated in relation to individuals’ ability to use ETs in activities at home as well as in out-of-home activities. ETs are integrated in different types of everyday life activities12,59 and especially for patients with COPD activities also include e-health.17,21,60 Therefore, it is important to evaluate the ability to use relevant ETs in order to know where support is needed in interventions targeting problems in managing activities at home or in society. For COPD patients compensatory strategies, such as managing grocery shopping or participating in social relations online, may be particularly relevant as alternative ways of performing activities. The ability to use ET can be improved through targeted interventions such as adapting the environment for the current activity, integrating relevant strategies to compensate for motor limitations and identifying a match between the environment and the user’s capabilities.60 ET use is found to be related with ADL performance and significantly impact on health-related quality of life for people with COPD,20 hence it should be considered a target for interventions, also included in pulmonary rehabilitation.
As to the methodological strengths and limitations of the present study, a strength is the earlier well-established psychometric properties of the assessments used. The ADL-I, AMPS and ETUQ have been used in Danish contexts and among various samples including, and not limited to, people with COPD.3,41,61 The distribution of the sample across several stages of COPD is another strength of this study. With one-fifth of the participants at stage I, two-thirds at stage II, one-tenth stage III and none at stage IV, the stage-distribution only varies slightly from the Danish COPD population.62 The age diversity in the sample, from 46 to 87 years, also reflects the variety within the population. Although no adjustment for age was implemented in this explorative study in relation to ADL ability, future studies using the AMPS could make more systematic hypothesis-testing statistical comparisons between people with and without COPD adjusted for age. The sixteen internal dropouts due to missing AMPS evaluations were caused by a variety of reasons. A few participants were hospitalized, one participant passed away, but for several of the participants there was no clear and systematic reason indicated for not participating in the second visit. Thirteen of these participants were in stage I, indicating mild COPD which is somewhat surprising, as one could expect participants with moderate COPD to be those who were not able to cope with another visit, including performing ADL tasks. Indeed, it appears that there is no relationship between the level of COPD and ADL performance, as also indicated in other studies.3,63 To summarize the dropouts, no systematic reason was detected to explain the dropouts, which is why we assume the reasons must have been individual.
Given the relatively small sample size used in this study, the results are still only indications of ADL performance and ET use among people with COPD in Denmark, and caution is therefore suggested regarding the generalizability of findings. However, as standardized ADL assessments that focus on the performance of relevant and meaningful ADL activities performed in their natural context were employed in this study, the results can still be used to direct interventions that strive to adapt to the effort, efficiency, safety or need for assistance demonstrated in people with COPD. Due to the nature of this explorative study, no power calculations were performed before initiation. The findings could however be used for more hypothesis-testing studies in the future, and also support sample size and power calculations.
Future research should explore how interventions that focus on relevant ADL performance and ET use can be designed and implemented in order to contribute to current pulmonary rehabilitation, which may affect the quality of life for people living with COPD.
Conclusion
New insights into observed ADL performance in people living with COPD have been presented in terms of affected ADL motor skills and ADL process skills, and predicted need for support to function in the community. The self-reported ADL tasks that were most affected were mobility within or outside the home, lower dressing, bathing, pedicuring, cooking, shopping, cleaning and washing clothes. Moreover, ET use seem not to be a major issue for a majority of the sample, but only for a smaller part. The relationships between ADL performance and ET use also indicate that they are related concepts but it can not be assumed that problems in ADL also indicate problems in ET use for people with COPD, and vice versa. Overall, this knowledge is valuable for focusing targeted interventions that address challenging ADL performance and ET use through relevant and realistic activities. The ability to use ET is important to evaluate and target pulmonary rehabilitation.
Acknowledgment
The research within this manuscript is undertaken as a part of a doctoral research study. Link to thesis: https://openarchive.ki.se/xmlui/handle/10616/47301.
Disclosure
Dr Rina Juel Kaptain reports grants from The Danish Foundation of Occupational Therapy, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013.
2. Annegarn J, Meijer K, Passos VL, et al. Problematic activities of daily life are weakly associated with clinical characteristics in COPD. J Am Med Dir Assoc. 2012;13(3):284–290.
3. Bendixen HJ, Wæhrens EE, Wilcke JT, Sørensen LV. Self-reported quality of ADL task performance among patients with COPD exacerbations. Scand J Occup Ther. 2014;21(4):313–320.
4. American Occupational Therapy Association. Occupational therapy practice framework: domain and process (3rd ed.). FRAMEWORK: domain & process. Am J Occup Ther. 2014;68(Suppl 1):S1–S51.
5. Fisher AG, Jones KB. Assessment of Motor and Process Skills. Volume 1: Development, Standardization, and Administration Manual.
6. Emiliani PL. Assistive technology (AT) versus mainstream technology (MST): the research perspective. Technol Disabil. 2006;18(1):19.
7. Larsson-Lund M, Nyman A. Occupational challenges in a digital society: a discussion inspiring occupational therapy to cross thresholds and embrace possibilities. Scand J Occup Ther. 2018;1–4.
8. Nygård L, Starkhammar S. The use of everyday technology by people with dementia living alone: mapping out the difficulties. Aging Ment Health. 2007;11(2):144–155.
9. Ryd C, Nygård L, Malinowsky C, Öhman A, Kottorp A. Can the everyday technology use questionnaire predict overall functional level among older adults with mild cognitive impairment or mild-stage alzheimer’s disease? – a pilot study. Scand J Caring Sci. 2017;1–9.
10. Ballmer T, Helle T, Kaptain RJ, Malonowsky C, Kottorp A. Test-retest and inter-rater reliability of the Danish version of the management of everyday technology assessment for use with older adults with and without COPD. Scand J Occup Ther. 2019;26(6):463–474.
11. Hedman A, Kottorp A, Nygård L. Patterns of everyday technology use and activity involvement in mild cognitive impairment: a five-year follow-up study. Aging Ment Health. 2018;22(5):603–610.
12. Emiliani PL, Stephanidis C, Vanderheiden G. Technology and inclusion – past, present and foreseeable future. Am J Occup Ther. 2011;23:101–114.
13. Walsh R, Drasga R, Lee J, Leggett C, Shapnick H, Kottorp A. Activity engagement and everyday technology use among older adults in an urban area. Am J Occup Ther. 2018;72(4):195040p1–p7.
14. Zonneveld M, Patomella AH, Asaba E, Guidetti S. The use of information and communication technology in healthcare to improve participation in everyday life: a scoping review. Disabil Rehabil. 2019;1–8.
15. Early F, Young JS, Robinshaw E. A case series of an off-the-shelf online health resource with integrated nurse coaching to support self-management in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2955–2967.
16. Simonÿ C, Riber C, Bodtger U, Birkelund R. Striving for confidence and satisfaction in everyday life with chronic obstructive pulmonary disease: rationale and content of the tele-rehabilitation programme >COPD-Life> >. Int J Environ Res Public Health. 2019;16(3320):1–16.
17. Disler RT, Inglis SC, Newton P, Currow DC, Macdonald PS, Glanville AR. Older patients’ perspectives of online health approaches in chronic obstructive pulmonary disease. Telemed J E Health. 2019;25(9):840–846.
18. Morrison D, Mair F, Yardlyey L, Kirby S, Thomas M. Living with asthma and chronic obstructive airways disease: using technology to support self-management - an overview. Chron Respir Dis. 2017;14(4):407–419.
19. Nyberg A, Wadell K, Lindgren H, Tistad M. Internet-based support for self-management strategies for people with COPD-protocol for a controlled pragmatic pilot trial of effectiveness and a process evaluation in primary healthcare. BMJ Open. 2017;7:1–11.
20. Kaptain RJ, Helle T, Patomella AH, Weinreich UM, Kottorp A. Association between everyday technology use, activities of daily living and health-related quality of life in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:89–98.
21. Danish health authority [homepage on the Internet]. Copenhagen: Telemedicinsk understøttelse af behandlingstilbud til mennesker med KOL - anbefalinger for målgruppe, sundhedsfagligt indhold samt ansvar og samarbejde [Telemedicin support of treatment options for people with COPD - recommendations for target group, health professional content and responsibility and collaboration]; 2017. Available from: https://www.sst.dk/da/udgivelser/2017/telemedicinsk-understoettelse-af-behandlingstilbud-til-mennesker-med-kol.
22. Paes T, Machado FVC, Cavalheri V, Pitta F, Hernandes NA. Multitask protocols to evaluate activities of daily living performance in people with COPD: a systematic review. Expert Rev Respir Med. 2017;11(7):581–590.
23. Janaudis-Ferreira T, Beauchamp MK, Robles PG, Goldstein RS, Brooks D. Measurement of activities of daily living in patients with COPD. Chest. 2014;145(2):253–271.
24. Barusso-Grünninger MS, Gianjoppe-Santos J, Sentanin AC, Lorenzo VAP. Do London chest activity of daily living scale and St George´s respiratory questionnaire reflect limitations during activities of daily living in patients with COPD? J Cardiopulm Rehabil Prev. 2019;39:274–280.
25. Halding AG, Aarsheim EI, Dolmen NM, Jensen AJ, Stavøstrand S, Grov EK. COPD transitions in health and self-management: service users’ experiences from everyday life. Int J Chron Obstruct Pulmon Dis. 2018;13:2075–2088.
26. Taylor RR. Kielhofner’s Model of Human Occupation: Theory and Application.
27. Bartels SL, Assander S, Patomella AH, Jamnadas-Khoda J, Malinowsky C. Do you observe what I perceive? The relationship between two perspectives on the ability of people with cognitive impairments to use everyday technology. Aging Ment Health. 2019;1–11.
28. Ryd C, Nygård L, Malonowsky C, Öhman A, Kottorp A. Associations between performance of activities of daily living and everyday technology use among older adults with mild stage Alzheimer’s disease or mild cognitive impairment. Scand J Occup Ther. 2015;22(1):33–42.
29. Wæhrens EE, Bliddal H, Danneskiold-Samsøe B, Lund H, Fisher AG. Differences between questionnaire- and interview-based measures of activities of daily living (ADL) ability and their association with observed ADL ability in women with rheumatoid arthritis, knee osteoarthritis, and fibromyalgia. Scand J Rheumatol. 2012;41(2):95–102.
30. Nielsen KT, Wæhrens EE. Occupational therapy evaluation: use of self-report and/or observation? Scand J Occup Ther. 2015;22(1):13–23.
31. DePoy E, Gitlin LN. Introduction to Research: Understanding and Applying Multiple Strategies.
32. Global initiative for chronic obstructive lung disease (GOLD) [homepage on the Internet]. Fontana: Global Stragegy for the Diagnosis, Management and Prevention of COPD; 2019. Avaiable from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf.
33. Wæhrens E. ADL-Interview (ADL-I) Manual. 2011.
34. Wæhrens EE. Measuring Quality of Occupational Performance Based on Self-report and Observation: development and Validation of Instruments to Evaluate ADL Task Performance [dissertation]. Umeå: Umeå University; 2010.
35. Fisher AG, Jones KB. Assessment of Motor and Process Skills.
36. Merrit BK. Validity of using the assessment of motor and process skills to determine the need for assistance. Am J Occup Ther. 2011;65:643–650.
37. Nygård L, Rosenberg L, Kottorp A. User Manual: Everyday Technology Use Questionnaire (ETUQ) Everyday Technology in Activities at Home and in Society. Stockholm, Sweden: Karolinska Institutet, Division of Occupational Therapy; 2016.
38. Rosenberg L, Nygård L, Kottorp A. Everyday technology use questionnaire: psychometric evaluation of a new assessment of competence in technology use. OTJR. 2008;29(2):52–62.
39. Rosenberg L, Kottorp A, Winblad B, Nygård L. Perceived difficulty in everyday technology use among older adults with or without cognitive deficits. Scand J Occup Ther. 2009;16(4):216–226.
40. Nygård L, Pantzar M, Uppgard B, Kottorp A. Detection of activity limitations in older adults with MCI or Alzheimer´s disease through evaluation of perceived difficulty in use of everyday technology: a replication study. Aging Ment Health. 2012;16(3):361–371.
41. Kaptain RJ, Kottorp A, Patomella AH, Helle T. Inter-rater and test-retest reliability of the Danish version of the everyday technology use questionnaire. Scand J Occup Ther. 2019;26(3):226–234.
42. Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS task force. Standardisation of spirometry. Eur Respir J. 2005;26:319–338.
43. Neder JA. Lung function testing in chronic obstructive pulmonary disease. Clin Chest Med. 2020;41:347–366.
44. Bond TG, Fox CM. Applying the Rasch model: fundamental measurement in the human sciences. 2nd ed. J Educ Meas. 2007;360.
45. Linacre JM. WINSTEPS Rasch Measurement Computer Program. Chicago; 2009.
46. Hedman A, Nygård L, Almkvist O, Kottorp A. Patterns of functioning in older adults with mild cognitive impairment: a two-year study focusing on everyday technology use. Aging Ment Health. 2013;17(6):679–688.
47. Field A. Discovering Statistics Using IBM SPSS Statistics.
48. Domholdt E. Rehabilitation Research: Principles and Applications.
49. General Data Protection Regulation. Regulation (EU) 2016/679 of the European parliament and of the council of 27 april 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing directive 95/46/EC (general data protection regulation). OJ. 2019.
50. National Committee on Health Research Ethics. Act on research ethics review of health research projects. Available from: https://en.nvk.dk/rules-and-guidelines/act-on-research-ethics-review-of-health-research-projects.
51. World Medical Association. Declaration of Helsinki – ethical principles for medical research involving human subjects [Internet]; [
52. Costi S, Bari MD, Pillastrini P, et al. Short-term efficacy of upper-extremity exercise training in patients with chronic airway obstruction: a systematic review. Phys Ther. 2009;89(5):443–455.
53. Meijer K, Annegarn J, Passos VL, et al. Characteristics of daily arm activities in patients with COPD. Eur Respir J. 2014;43:1631–1641.
54. Schmitter-Edgecombe M, Parsey C, Cook DJ. Cognitive correlates of functional performance in older adults: comparison of self-report, direct observation, and performance-based measures. J Int Neuropsychol Soc. 2011;17(5):853–864.
55. Schou L, Østergaard B, Rasmussen LS, Rydahl-Hansen S, Phanareth K. Cognitive dysfunction in patients with chronic obstructive pulmonary disease - a systematic review. Respir Med. 2012;106(8):1071–1081.
56. Fisher AG, Marterella A. Powerful Practice – A Model for Authentic Occupational Therapy. Center for Innovative OT Solutions. Fort Collins, Colorado, USA; 2019.
57. Halding A-G, Aarsheim EI, Dolmen NM, Jensen AJ, Stavøstrand S, Grov EK. COPD transitions in health and self-management: service users’ experiences from everyday life. Int J Chron Obstruct Pulmon Dis. 2018;13:2075–2088.
58. Katz PP, Gregorich S, Eisner M, et al. Disability in valued life activities among individuals with COPD and other respiratory conditions. J Cardiopulm Rehabil Prev. 2010;30(2):126–136.
59. Malinowsky C, Kottorp A, Patomella AH, Rosenberg L, Nygård L. Changes in the technological landscape over time: relevance and difficulty levels of everyday technologies as perceived by older adults with and without cognitive impairment. Disabil Technol. 2015;27:91–101.
60. Kassberg A-C, Prellwitz M, Malonowsky C, Larsson-Lund M. Interventions aimed at improving the ability to use everyday technology in work after brain injury. Scand J Occup Ther. 2016;23(2):147–157.
61. Von Bülow C, Amris K, La Cour K, Danneskiold-Samsøe B, Wæhrens EE. Ineffective ADL skills in women with fibromyalgia: a cross-sectional study. Scand J Occup Ther. 2016;23(5):391–397.
62. Moll L, Lange P, Dahl BH. KOL Sygdom, Behandling Og Organisation. COPD Illness, Treatment and Organization. Copenhagen: Munksgaard, Danmark; 2011.
63. Ozsoy I, Kahraman BO, Acar S, Ozalevli S, Akkoclu A, Savci S. Factors influencing activities of daily living in subjects with COPD. Respir Care. 2019;64(2):189–195.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.