")
Back to Journals » International Journal of Women's Health » Volume 11
New Findings On Gender: The Effects Of Employment Status On Suicide
Authors Kposowa AJ , Aly Ezzat D, Breault K
Received 26 May 2019
Accepted for publication 9 October 2019
Published 4 November 2019 Volume 2019:11 Pages 569—575
DOI https://doi.org/10.2147/IJWH.S216504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Augustine J Kposowa,1 Dina Aly Ezzat,1 Kevin Breault2
1Department of Sociology, University of California, Riverside, CA, USA; 2Department of Sociology and Anthropology, Middle Tennessee State University, Murfreesboro, TN, USA
Correspondence: Augustine J Kposowa
Department of Sociology, University of California, 900 University Ave, Riverside, CA 92521, USA
Tel +1 951 456 5425
Fax +1 951 827 5444
Email [email protected]
Background and objectives: The purpose of the study was to evaluate the impact of gender and employment on suicide with the use of expanded unemployment statuses as covariates.
Methods: Data were obtained from release 5 of the National Longitudinal Mortality Study, a prospective study of deaths in the United States. Proportional hazards regression models were fitted to the data based on follow-up from 1990 to 2011.
Results: Unemployment was significantly associated with suicide (ARR=1.628, 95% CI=1.356, 1.954), and men had suicide deaths that were five times greater than women (ARR=5.104, 95% CI=4.565, 5.707), however when the sample was stratified by sex, the impact of unemployment on suicide was much higher among women (ARR=2.988, 95% CI=2.045, 4.366) than among men (ARR=1.393, 95% CI=1.131, 1.717).
Conclusion: Contrary to many findings and gender assumptions, unemployed women in the U.S. have higher deaths from suicide than unemployed men. Discussion focused on explanations for gender disparities in unemployment.
Keywords: suicide, unemployment, gender
Introduction
After a period of consistent decline in suicide in the United States between 1986 and 1999, suicide rates increased steadily from 1999 to 2014, from 10.5 to 13.0 per 100,000 population, an age-adjusted increase of 24 percent.1 As the 10th leading cause of death in the U.S., 45,000 Americans die from suicide every year.2 Moreover, more than a half-million people are seen in emergency rooms yearly for injuries due to self-harm, and it is estimated 1.3 million adults in the U.S. attempt suicide annually.1,2
Longitudinal individual-level studies of unemployment have with rare exception found that unemployment increases the risk for suicide. Also, the finding than men have higher suicide deaths than women is well understood. Thus, for the year 2016 in the U.S., the suicide rate for males was 13.9 per 100,000, while the rate for women was 4.0 per 100,000. Similarly, longitudinal studies outside of the U.S. generally find that unemployed men have higher suicide than unemployed women.3–6 One exception to this pattern is based on U.S. data where unemployed women had higher suicide deaths than unemployed men, but these data involved relatively few female suicides and limited unemployment statuses.7
Many studies on the relationship between unemployment and suicide do not include the employment status of the disabled (unable to work), and those not looking for work, or who have been discouraged from finding work. One important advantage of using additional categories of employment status is that it helps to reduce the “self-selection” problem. It has been suggested that the association between unemployment and suicide may be spurious because unemployed people are more likely to be mentally ill.8,9 The use of these other categories has the effect of moving more of the mentally ill out of the unemployed (looking for work) category, thus reducing the self-selection problem.10
Thus, the purpose of this study was to use longitudinal individual-level research to revisit U.S. data by stratifying the analysis by gender, including a much larger sample of suicides, and by using an expanded number of unemployment statuses as covariates. We studied the years 1990–2011 covering almost 1.5 million persons of whom 2,013 died of suicide, including 414 women, the largest U.S. sample available.
Methods
Data
Data were obtained from version 5 of the National Longitudinal Mortality Study (NLMS) released in October 2015.11 The NLMS is a prospective study of mortality in the United States, and is sponsored by the National Heart, Lung, and Blood Institute, the National Cancer Institute, the National Institute on Aging, the National Center for Health Statistics, and the U.S. Bureau of the Census. The full NLMS comprises a database developed for the purpose of studying the effects of demographic and socio-economic attributes on disparities in U.S. mortality. It is based on a multistage stratified sample of the non-institutionalized population and includes information from the Current Population Surveys. The full study, which is restricted, currently has approximately 3.8 million records with 550,000 identified mortality cases. The NLMS Public Use Microdata Sample used in the present study is an extract of the full NLMS designed to provide easy access to the main study while protecting the confidentiality of those who have responded to the original surveys. Data from deaths occurring from April 1, 1990 to April 30, 2011 were obtained from death certificates by linking individuals in the Current Population Surveys to a mortality database through the National Death Index (NDI). Created in 1979 and maintained by the National Center for Health Statistics, the NDI is a computerized and centralized index of deaths occurring in the United States. It was designed to provide researchers with a simplified method of obtaining mortality information in prospective studies. Detailed information about the NLMS and NDI, including data linkage and obtaining death records, is available at the U.S. Bureau of the Census12,13 and the National Center for Health Statistics.14 Mortality experiences of cohort members were studied until 2011, and individuals alive at the end of the study received the maximum follow-up period of 4,018 days or 11 years. Analyses in the present study were limited to persons 15 years old and above, 1,477,743 individuals at the beginning of the study. To estimate suicide mortality risk, all individuals surviving beyond the 4,018 days of follow-up, and persons dying from other causes were treated as right censored observations.
Variables And Measurement
The dependent variable was completed suicide (intentional self-harm), identified by codes X60-X84, Y87.0 from the International Statistical Classification of Diseases, 10th revision. All covariates in the analyses were measured at baseline, and their effects on suicide risk during follow-up were assessed. The key independent variable was employment status, comprising those who were employed; unemployed, but looking for work; disabled, unable to work; retired, housekeeping, student or others doing something else not classified in previous categories of employment status; and those for whom employment status was unknown/missing. For data analysis, each was measured as series of dummy variables with 1, and individuals employed at baseline were the reference group for the other employment categories. Other variables were similarly based on the longitudinal literature when available in the NLMS and measured as dummy variables: sex; marital status; race/ethnicity; place of residence; housing tenure; educational attainment; family income; age; and region of residence as identified by the U.S. Bureau of the Census. Women, the married, non-Hispanic African Americans, those living in urban areas, homeowners, those with some education, and income from US$40,000–59,999 were the comparison groups. Age at baseline was left in its interval format.
Statistical Estimation
Proportional hazards regression models were fitted to the NLMS data to compare the risk of suicides during follow-up while controlling for potential confounders.15 The model may be specified as:
(1)
where h(t) is the hazard or risk of suicide at time t, ßks are a set of unknown parameters to be estimated and Xks are k covariates. h0(t) is a baseline hazard function and is defined when all the covariates in the model are set to zero. The survival distribution function, defined as the probability of surviving from start of follow-up to at least time t, is given by
(2)
where S0(t) is the baseline survivor function representing the reference categories of the covariates. The proportionality of hazards, an assumption in the Cox model, is tested by inspecting the plots of ln[-ln{S(t)}] against survival time t for the various covariate categories. If the resulting plots are found to be approximately parallel, the proportionality assumption is assumed to be satisfied by the data.
Estimated relative risks (hazard ratios) were obtained by exponentiating the hazard coefficients (βk’s) in Equation 1. Thus, relative risk (RR) = exp(βk’s). The statistical significance of the effects of each covariate in the above model (Equation 1) was assessed via the t-statistic, obtained as a ratio of the parameter estimate to its corresponding asymptotic standard error. Parameters were estimated by the method of partial maximum likelihood using the PHREG procedure.16 Proportional hazards model was selected over the logistic model because the latter fails to account for differences in survival from start of follow-up until event occurrence.
Results
As may be seen in Table 1, the unemployed (looking for work) were 63 percent more likely to have higher suicide deaths than their employed counterparts (ARR=1.628, [95%] CI=1.356, 1.954). The disabled and those unable to work were nearly 2.4 times more likely to have higher suicide deaths than the employed (ARR=2.374, 95% CI=1.904, 2.296). Individuals who were retired, doing housekeeping, students, or others had a suicide risk that was 1.5 times more elevated than that of the employed (ARR=1.513, 95% CI=1.343, 1.704).
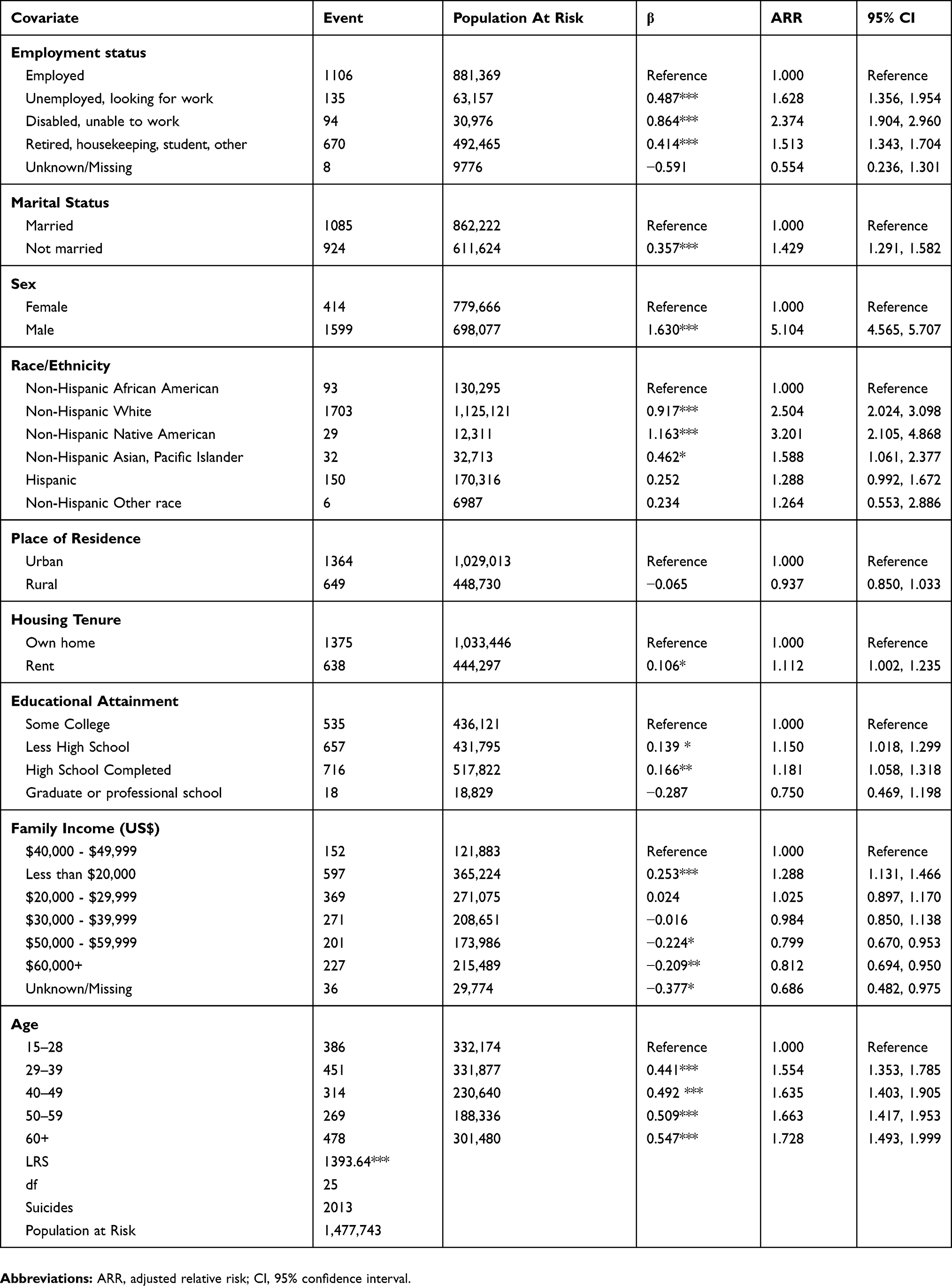 |
Table 1 Hazards Regression Results Of The Effects Of Employment Status On Suicide: The National Longitudinal Mortality Study, 1990–2011 |
Men were over 5 times more likely to have higher suicide deaths than women. The unmarried were 42% more likely have higher suicide than the married. Non-Hispanic whites had a suicide risk that was 2.5 times that of non-Hispanic African Americans. Likewise, non-Hispanic Native Americans experienced suicide mortality risks that were 3.2 times those of non-Hispanic African Americans.
Due to the reduced number of suicides because of stratification by sex some variables were collapsed to reduce the risk of deriving unstable estimates (see Table 2).
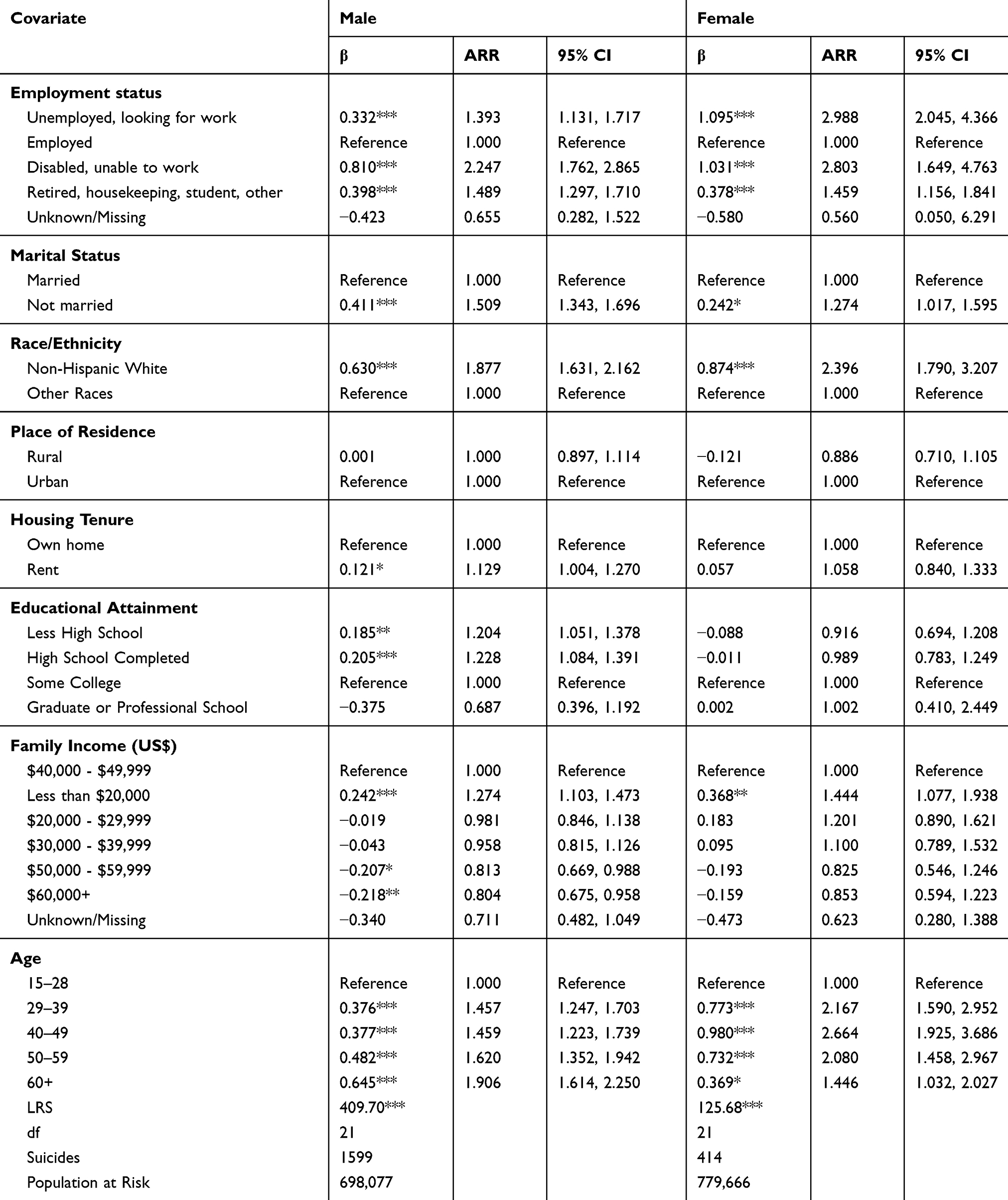 |
Table 2 Employment Status On Suicide By Sex, 1990–2011 |
As seen, unemployed men had nearly 1.4 times more suicide deaths than employed men (ARR=1.393, 95% CI=1.131, 1.717). However, unemployed women had nearly 3 times more suicide than employed women (ARR=2.988, 95% CI=2.045, 4.366), the strongest covariate in the sample. The strongest covariate for men was disabled (ARR=2.247, 95% CI=1.762, 2.865).
Among other findings, being unmarried was significant in explaining suicide risk for both sexes, but the effect was stronger in men (ARR=1.509, 95% CI=1.343, 1.696) than in women (ARR=1.274, 95% CI=1.017, 1.595), and non-Hispanic white men had nearly 1.9 times more suicide deaths than other racial/ethnic groups (ARR=1.877, 95% CI=1.632, 2.162), but non-Hispanic white women experienced risk of death that was over 2.4 times that of other racial/ethnic groups (ARR=2.396, 95% CI=1.790, 3.207). While the educational attainment variables were significant for men, importantly that was not the case for women. In addition, having a family income of less than $20,000 was stronger for women than men (APR=1.444 versus 1.274), but women did not significantly benefit from higher family income as men did. Finally, in every age category women’s risk for suicide was significantly greater than that for men with the exception of those 60 years or older.
Discussion
We expanded the category of employment status to move more of the mentally ill out of the unemployed status. This is important because of the self-selection problem that suggests unemployed people have higher risks for suicide because they are mentally ill. The main limitation of the study is that the NLMS does not include psychiatric morbidity as a covariate, and the effects of unemployment may be modified as a result. Unfortunately, this is true for all U.S. data. Another limitation is that, ideally, more work is needed to separate out the category of retired, homemakers, students and others. The problem here as in much suicide research is that sample size is a limiting factor. Finally, two other variables not available in the NLMS, job demoralization and demotion, might alter the effects of employment on suicide as they may potentially lead to suicide.
The strong relationship between female unemployment and suicide shown in this study is generally contrary to long standing notions about gender and suicide. Because men are at higher risk for suicide, the general understanding was that unemployed men would be at higher risk than unemployed women. Traditionally seen as holding the primary role in the family, socialized to be the major breadwinners, and viewed as expecting gainful employment, it was assumed that unemployment would affect men more strongly than women.17–19
Four factors may help to explain the greater risk for suicide among unemployed women. One explanation is unemployed women are more likely to have higher rates of depression. While we expanded the category of unemployment status in an attempt to reduce the number of mentally ill among the unemployed, it is likely some depressed individuals remained in the unemployed category. Depression is a major risk factor for suicide, and women are more likely to be diagnosed, 4.0% compared to 2.7% for men (a 48% difference).20,21 In addition, a survey of 235,067 people in the U.S. found 6.4% of employed persons had depression compared to 39.1% who were unable to work, 21.3% of the unemployed, 9.2% of homemakers and students, and 6.3% of the retired.20 Even though gender disparities in depression require more investigation, these studies may suggest part of the suicide risk affecting unemployed women may be the result of depression. There is also evidence that for some of the unemployed the pathway from mental illness to suicide begins with unemployment,22–24 thus a better understanding of the causal directions concerning unemployment and depression is needed.
Another factor is gender discrimination. In an environment where women’s occupational chances are blocked for reasons of discrimination, it is reasonable to think unemployed women will have higher suicide than men. Despite evidence that discrimination in employment on the basis of sex has not gone away, rates of female labor force participation show it is considerably less common today in the U.S. than in the past.25 However, this does not mean women have benefited equally. Members of the LGBT community are of special concern because they experience high levels of employment discrimination26 and suicide.27
Another approach to the linkage between unemployed women and suicide is a Durkheimian one.28 Both men and women lack for income and status during unemployment, but they also lose social integration, the connectiveness between themselves and the workplace, and others in the workplace. But many women today maybe more bonded to and see themselves as more connected with the workplace than men. They may also be more strongly connected to the shared values of the workplace, and perhaps more likely to react negatively when those bonds are severed. In a recent study covering nearly 500 men and women, the negative impact on life satisfaction during unemployment was higher in women than men for those who had stronger work identity.29 This study also showed women with egalitarian gender attitudes experienced higher loss of life satisfaction during unemployment.
On the other hand, while some women may see the workplace as a source of social integration, others have found it to be an environment rife with the risk of harassment. In a recent study of 64,000 employees across 279 companies, 35% of women had been sexually harassed, including 55% of women in senior management.30 Job loss is a common effect of sexual harassment in the workplace.31 The link between the harassment of women physicians, and suicide has been discussed in several reports.32,33 In a study of 290 women firefighters sexual harassment was significantly related to suicide ideation.34 A study of sexual harassment in the U.S. military found in a sample of 12,567 soldiers, those who experienced harassment were five times more likely to commit suicide.35
Conclusion
Contrary to many findings and gender assumptions, this paper shows that while men have higher suicide deaths than women, in the U.S. unemployed women have higher suicide risks than unemployed men. Understanding the pathways in women’s lives from unemployment to suicide is an important next step, perhaps one with greater urgency now.
Acknowledgments
We thank the U.S. Bureau of the Census and the National Center for Health Statistics for providing the data for this research. The views and opinions of the paper are those of the authors and they do not necessarily reflect those of these institutions. We also thank the anonymous reviewers of the paper for their constructive comments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Suicide Mortality in the United States, 1999 to 2017. NCHS Data Brief, No. 330. November 2018. Available from: https://www.cdc.gov/nchs/products/databriefs/db330.htm.
2. Suicide Statistics [homepage on the Internet]. Washington: American Foundation of Suicide Prevention; 2019. Available from: https://afsp.org/about-suicide.
3. Johansson SE, Sundquist J. Unemployment is an important risk factor for suicide in contemporary Sweden: an 11-year follow up study of a cross-sectional sample of 37,789 people. Pub Health. 1997;111:41–45. doi:10.1038/sj.ph.1900317
4. Lundin A, Lundberg I, Alebeck P, Hemmingsson T. Unemployment and suicide in the Stockholm population: a register-based study of 771,068 men and women. Pub Health. 2009;126:371–377. doi:10.1016/j.puhe.2012.01.020
5. Qin P, Agerbo E, Westergard-Nielsen N, Eriksson T, PB M. Gender differences in risk factors for suicide. Br J Psychiatry. 2000;177:546–550. doi:10.1192/bjp.177.6.546
6. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a National Register based study of all suicides in Denmark, 1981–1997. Am J Psychiatry. 2003;160:765–772. doi:10.1176/appi.ajp.160.4.765
7. Kposowa AJ. Unemployment and suicide: a cohort analysis of social factors predicting suicide in the US National Longitudinal Mortality Study. Psych Med. 2001;31:127–138. doi:10.1017/S0033291799002925
8. Agerbo E. Effect of psychiatric illness and labour market status on suicide: a healthy worker effect? J Epidemiol Community Health. 2005;59:598–602. doi:10.1136/jech.2004.025288
9. Yip PF, Caine ED. Employment status and suicide: the complex relationship between changing unemployment rates and death rates. J Epidemiol Community Health. 2010;65:733–736. doi:10.1136/jech.2010.110726
10. Blakely TA, Collings SCD, Atkinson J. Unemployment and suicide: evidence for a causal association. J Epidemiol Community Health. 2003;57:594–600. doi:10.1136/jech.57.8.594
11. U.S. Bureau of the Census. Public Use Microdata Sample (PUMS) File Release 5 Documentation. Washington: Department of Commerce; 2015.
12. Current Population Survey TP66. [homepage on the Internet]. Washington: U.S. Bureau of the Census; 2006. Available from: https://www.census.gov/prod/2006pubs/tp-66.pdf.
13. Resign of the Sample for the Current Population Survey. [homepage on the Internet]. Washington: U.S. Bureau of the Census; 2014. Available from: https://www.bls.gov/cps/sample_redesign_2014.pdf.
14. National Death Index Data Users’ Guide [homepage on the Internet]. Washington: National Center for Health Statistics; 2017. Available from: https://www.cdc.gov/nchs/ndi/index.htm.
15. Cox DR. Regression models and life-tables (with discussion). J R Stat Soc. 1972;1972(34):187–220.
16. SAS Institute. SAS/STAT Software: The PHREG Procedure. Cary: SAS Institute; 2018.
17. Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. 1998;28:1–23.
18. Ensminger ME, Celentano DD. Gender differences in the effect of unemployment on psychological distress. Soc Sci Med. 1990;30:469–477. doi:10.1016/0277-9536(90)90349-w
19. Jones L. Effects of unemployment on women. Affilia. 1989;4:54–67. doi:10.1177/088610998900400404
20. Current Depression Among Adults [homepage on the Internet]. Washington: Centers for Disease Control and Prevention; 2010. Available from: https://www.cdc.gov/mmwr/preview/nmwrhtm//mm5938a2.htm?s_htm?s_cid=mm5938a2_x.
21. Gender and Women’s Mental Health [homepage on the Internet]. Geneva: World Health Organization; 2018. Available from: www.who.int/mental_health/prevention/genderwomen/en/.
22. Mucci N, Giorgi G, Roncaioli M, Perez J, Arcangeli G. The correlation between stress and economic crisis: a systematic review. Neuropsychiatr Dis Treat. 2016;12:983–993. doi:10.2147/NDT.S98525
23. Paul K, Moser K. Unemployment impairs mental health: meta-analyses. J Vocat Behav. 2009;74:264–282. doi:10.1016/j.jvb.2009.01.001
24. Phillips JA, Nugent CN. Suicide and the great recession of 2007-2009: the role of economics factors in the 50 U.S. states. Soc Sci Med. 2014;116:22–31. doi:10.1016/j.socscimed.2014.06.015
25. Local Area Unemployment Statistics [homepage on the Internet]. Washington: U.S. Bureau of Labor Statistics; 2018. Available from: https://www.bls.gov/lav/lastrk17.htm.
26. Documented evidence of employment discrimination & its effects on LGBT people [homepage on the Internet]. Los Angeles: Williams Institute; 2011. Available from: https://williamsinstitute.law.ucla.edu/research/discrimination/document-evidence-of-employment-discrimination_its_effects_on_lgbt_people.
27. King M, Semlyen J, Tai SS, et al. A systematic review of mental disorders, suicide, and deliberate self-harm in lesbian, gay and bisexual people. BMC Psychiatry. 2008;8:1–17. doi:10.1186/1471-244X-8-1
28. Durkheim E. Suicide: A Study in Sociology. New York: The Free Press; 1979.
29. Longhi S, Nandi A, Bryan M, Connolly S, Gedikli C. Gender and Unemployment: Analysis of Understanding Society: The UK Household Longitudinal Survey. Available from: https://uhra.herts.ac.uk/bitstream/handle/2299/19331/technical_report_FINAL.pdf?sequence=2&isallowed=y.
30. Women in the Workplace [homepage on the Internet]. New York: Leanin.org and McKinsey & Company; 2018. Available from: https://womenintheworkplace.com.
31. McLaughlin H, Uggen C, Blackstone A. The economic and career effects of sexual harassment on working women. Gend Soc. 2017;31:333–358. doi:10.1177/0891243217704631
32. Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. Am J Psychiatry. 1999;156:1882–1894.
33. Schernhammer E. Taking their own lives: the high rate of physician suicide. N Engl J Med. 2005;352:2473–2476. doi:10.1056/NEJMp058014
34. Horn MA, Stanley IH, Spencer-Thomas S, Joiner T. Women firefighters and workplace harassment: associated suicidality and mental health sequelae. J Nerv and Ment Dis. 2017;205:910–917. doi:10.1097/NMD.0000000000000759
35. Griffith J. The sexual harassment-suicide connection in the U.S. military: contextual effects of hostile work environment and trusted unit leaders. Suicide Life Threat Behav. 2017;47:910–917.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.