")
Back to Journals » Orthopedic Research and Reviews » Volume 8
New developments in prosthetic arm systems
Authors Vujaklija I, Farina D, Aszmann O
Received 7 March 2016
Accepted for publication 12 May 2016
Published 7 July 2016 Volume 2016:8 Pages 31—39
DOI https://doi.org/10.2147/ORR.S71468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung

Ivan Vujaklija,1 Dario Farina,1 Oskar C Aszmann2
1Institute of Neurorehabilitation Systems, Bernstein Focus Neurotechnology Göttingen, University Medical Center Göttingen, Georg-August University, Göttingen, Germany; 2Christian Doppler Laboratory for Restoration of Extremity Function, Division of Plastic and Reconstructive Surgery, Department of Surgery, Medical University of Vienna, Vienna, Austria
Abstract: Absence of an upper limb leads to severe impairments in everyday life, which can further influence the social and mental state. For these reasons, early developments in cosmetic and body-driven prostheses date some centuries ago, and they have been evolving ever since. Following the end of the Second World War, rapid developments in technology resulted in powered myoelectric hand prosthetics. In the years to come, these devices were common on the market, though they still suffered high user abandonment rates. The reasons for rejection were trifold – insufficient functionality of the hardware, fragile design, and cumbersome control. In the last decade, both academia and industry have reached major improvements concerning technical features of upper limb prosthetics and methods for their interfacing and control. Advanced robotic hands are offered by several vendors and research groups, with a variety of active and passive wrist options that can be articulated across several degrees of freedom. Nowadays, elbow joint designs include active solutions with different weight and power options. Control features are getting progressively more sophisticated, offering options for multiple sensor integration and multi-joint articulation. Latest developments in socket designs are capable of facilitating implantable and multiple surface electromyography sensors in both traditional and osseointegration-based systems. Novel surgical techniques in combination with modern, sophisticated hardware are enabling restoration of dexterous upper limb functionality. This article is aimed at reviewing the latest state of the upper limb prosthetic market, offering insights on the accompanying technologies and techniques. We also examine the capabilities and features of some of academia’s flagship solutions and methods.
Keywords: prosthetic, amputations, rehabilitation, hand, arm
Introduction
A significant portion of the injuries treated in the emergency rooms around the globe involve upper extremities.1–3 The majority of them occur at home,2 during work,4,5 or when performing sports.6 Considering that almost all our everyday activities depend on manipulation by the hands, severe hand injuries can truly be devastating. Consequences of such incidents can lead to long-term disabilities, also affecting the mental and social state, with difficult reintegration in the society.7,8
The severe consequences of upper limb loss have been recognized centuries ago,9 and the ideas of artificial substitution have been since then very appealing. Transition from simple cosmetic prostheses to a more functional solution was inevitable and in high demand, resulting in the development of early body-powered and cable-driven systems. These simple devices proved themselves to be very useful and, with modern materials, are still currently in use. Approximately half of the current market of upper limb prosthetics is indeed based on cable-driven systems.10
The first pneumatic hand was developed at the beginning of the 20th century, soon followed by the first electric-powered hand. At the end of the Second World War, early concepts of myoelectric prostheses were introduced.11 These devices, which linearly translated the electrical activity of the residual muscles of the stump into the velocity of closing and opening of gripers, started to be used in research laboratories and to be sold on the market in the late 1950s. The concept of direct proportional control is still present in current commercially available systems, due to its simplicity and robustness.
By the late 1960s, pneumatic prostheses were able to drive and control several joints and grip types. However, the control was inefficient and not robust enough, requiring specific anatomical features, dexterity, and cognitive effort of the patient.12 Myoelectric systems have tried to face these issues with state-based control. Accordingly, the patient would control the prosthesis using two control sites, as in the single degree of freedom (DoF) case. When there was the need to control a different joint or grip type, a co-contraction of the muscles under the two recording sites changed the control state of the prosthesis. This quite cognitively demanding system is still dominant on the market of dexterous prosthetics, mostly due to its robustness.
Numerous studies have been conducted in the past two decades, still indicating high rejection rates of all types of upper limb prosthetic devices across a variety of users.13–18 Depending on the study population, rejection rates vary from 25% to >50% for myolelectric and up to 35% for body-powered devices. However, these figures have leveled off with respect to previous periods,19,20 mainly due to modern technology. However, it is possible that the trend will eventually reverse.
Hand transplantation is an alternative to the prosthetic devices, offering functionality, superior visual appeal, and integrated sensory function.21 However, it is associated with the lifelong immunosuppressant therapy, lengthy rehabilitation, loss of grip force, and high risk of complications, leading to the possible rejection.22 These issues are then combined with very high costs.
Advances in micromachining and material design have enabled construction of versatile lightweight prosthetic hands and wrists. These market products, in combination with precise, small-sized, low-consumption electromotors, corresponded to highly actuated systems. Development of high-speed processing units with the top-end battery management and large memories in small housing propelled the research into more advanced and intuitive control systems. Greater understanding of the human neuromuscular system yielded new surgical and reconstructive techniques, which now provide access to high-quality and intuitive electromyography (EMG) sources even in high-level amputations. Socket design has also benefited from this rapid development of technology and now can offer solutions that are able to host multiple surface sensors, facilitate the use of implanted electrodes, and, in combination with surgical advancements, provide direct link with the skeletal system in the form of osseointegration. Finally, three-dimensional printing is quickly becoming a viable alternative for production of highly customizable products that are lightweight and inexpensive. Several open-source hand prosthetic projects are available for personal printing, and an ever growing number of companies are already using this method for building certain components of their own products.
Considering the latest rate of innovation in the field of prosthetics, significant increase in funding, and the number of new competitors on the market, this review aims to present the latest state of functional, myoelectrically controlled upper limb prosthetic solutions. The goal is to make a literature overview of the new developments of representative hardware, control algorithms, and interfaces from both the medical and technical perspective. Even though highly significant for prosthetic applications, solutions and research in the area of sensory feedback are beyond the scope of this review.
Hardware
The current market of actuated myoelectrically controlled upper limb prosthetic devices can roughly be divided into systems that address transradial/transcarpal, transhumeral, and shoulder disabilities. Each group features specific requirements, and, in general, the options for replacement are more advanced the more distal the level of impairment is.
Transradial/transcarpal solutions
Due to the complex anatomical nature of hands and yet crucial role in object handling and manipulation, their prosthetic counterparts have undergone an important evolution and functional advances in recent years. Although simple grippers are still dominant in the market, multi-actuated hands that provide several grip types or even fully controllable individual digits and finger joints are now common (Figure 1).
 | Figure 1 Examples of Ottobock prosthetic hands and cosmetics (from left to right): small System Inner Hand, small MyoHand VariPlus Speed, and medium Michelangelo hand. |
Some of the current common characteristics of the most promising commercial hand products – i-limb Quantum by Touch Bionics, RSL Steeper’s BeBionic v3, and Ottobock’s Michelangelo – are presented in Table 1. For the sake of putting these products into perspective, the same table lists three different, already established, products aiming at children with hand disabilities, adult long stump cases, and usual transradial users – Centri Child Myoelectric Hand, Transcarpal-Hand by Ottobock Healthcare, and Select Electric Hand by Liberating Technologies, respectively.
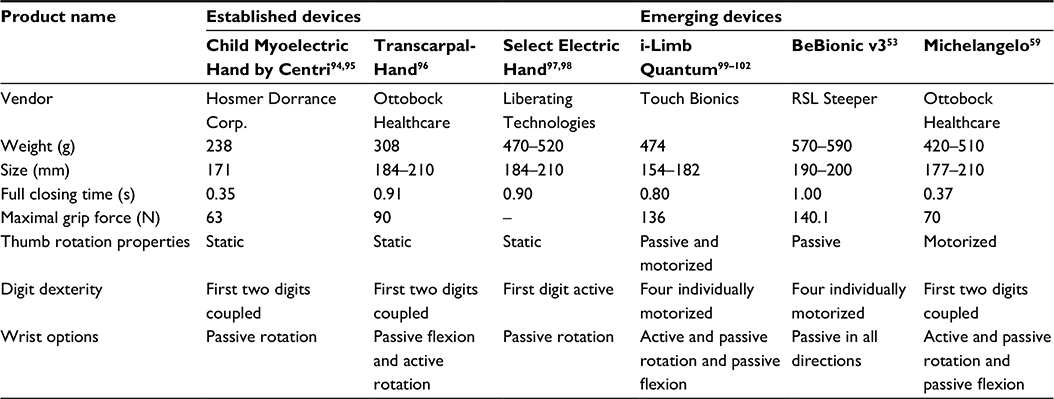 | Table 1 Features of three already established devices aiming at children population, transcarpal and transradial cases, and three commercially available flagship prosthetic hands |
From Table 1, it is evident that the increase in functionality did not significantly influence the size, the weight, and the power grasp force of prosthetic hands. Moreover, the listed products all offer certain wrist solutions, indicating an overall tendency of the market for further development of this joint. Besides the features listed, each of the hands in Table 1 is also equipped with a variety of product-specific features, mostly focusing on the different grasp types and safety measures (this is further discussed in the “Control strategies” section).
Prosthetic hand devices developed by smaller companies or research laboratories include the world’s first touch sensing hand prosthesis from Vincent Systems, Evolution 2, and DARPA founded DEKA Arm RC. Evolution 2 combines the sensory feedback information with the individually motorized digits and fully actuated thumb in a compact and light package (∼400 g).23 The DEKA Arm RC is the heaviest of the products so far listed (1,270 g)24 and, in its third generation, offers highly actuated digits and thumb with an included compound wrist that can be actuated in three DoFs.25
In order to provide a more natural object manipulation and therefore increase functional benefits to the users,26 modern prosthetic hand devices are frequently accompanied by an actively or passively controllable wrist joint. Passive versions of prosthetic wrists can be manually adjusted by the user in order to be in either compliant mode or to lock in one of the predefined positions in flexion/extension direction (Ottobock AxonWrist, Touch Bionics Flexion Wrist, BeBionic FlexionWrist) or along the rotation axis (Ottobock AxonRotation, Touch Bionics QWD, BeBionic Short Wrist). Additionally, certain vendors offer wrists that allow prosthetic hands to be positioned in any direction (MyolinoWrist 2000, BeBionic Multi-Flex). Commercial active units are almost exclusively focused on the wrist rotation (MC Wrist Rotator, Ottobock Electric Wrist Rotator).
Transhumeral and shoulder disarticulation solutions
The more proximal the upper limb impairment is, the greater the disability. In transhumeral amputations, the absence of an elbow requires an additional prosthetic joint to substitute the missing two DoFs. Even though the rotation of the forearm can be compensated using the wrist rotation unit, the major setback at this level of disability is the reduced number of sources and methods for controlling all the necessary prosthetic components. As for the wrist, prosthetic elbows can be passive or active with several locking positions. Passive or body-powered elbows are dominant on the market, though several major vendors also provide electrically powered, myoelectrically controllable devices. Some representative products and their characteristics are listed in Table 2. The DEKA Arm HC offers a motorized elbow solution with a limited range of motion to prevent reaching the face for safety reasons.25 This characteristics and the absence of the free swing mode have not been well received by the users.25
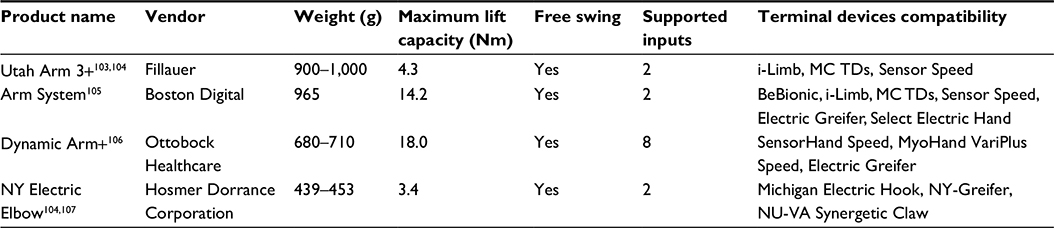 | Table 2 Features of commercially available myoelectric elbows |
Even though improvements in academia have indicated possible solutions in designing elbow joints with anthromorphic characteristics,27 one of the current main challenges is the design of a device fully compliant with all the standards and yet light enough to be suited for children and frail adults.
Powered shoulder joints are more complex and currently not present on the market. Nonetheless, promising solutions have been presented in research laboratories.25,28 The DEKA arm HC has recently received Food and Drug Administration approval,29 and it offers four movement directions in the shoulder joint.25 Moreover, for exploring the full possibilities of the targeted muscle reinnervation (TMR) approach, a modification of the LTI-Collier shoulder joint has been developed with an added electronic lock/unlock feature.28
Socket technology
The amount of time a user wears a prosthesis mainly depends on the socket fit and its design.30 Inadequate prosthetic fit might lead to limited range of motion, discomfort, and general poor performance,31 usually resulting in the abandonment of the device.32
After the development of the Otto Bock Muenster style socket in the 1960s33 and the Northwestern University socket in 1972,34 the transradial powered prosthesis socket design has not significantly changed. The introduction of flexible thermoplastics has indeed been the only major improvement.35 At the end of 1990s, silicon liners have been introduced, and the transparent, moldable plastics allowed better analysis of the inside socket dynamics, resulting in a tighter contouring around the fitted stump30 (Figure 2). Nowadays, new textile materials allow better, more hygienic, and less obstructing harnesses to be developed and custom fit to higher level upper limb amputees. The general tendency over the past few years, which was enabled through these novel materials, is the design of anatomically contoured sockets for all levels of amputation.36
 | Figure 2 Example socket design with custom pattern, silicon liner, and Ottobock Energy Pack housing. |
Based on the osseointegration technique introduced ∼60 years ago,37 an advanced mounting concept of the upper limb prosthesis has been developed and applied.38 The main idea behind this technique is to exploit the direct structural and functional connection between the skeletal bone and the surface of the titanium implant,39 which would further be connected to an additional implant penetrating the skin.40 In this way, a point for a direct, rigid connection of the prosthesis and the skeletal system is created.41 Osseointegration offers numerous advantages over the traditional sockets by providing a more intimate fit, increased range of motion, and osseoperception.42,43 However, it also requires additional surgery and poses potential risks of infection, implant fracture, or incomplete integration requiring revision surgeries.44,45
The introduction of implantable sensing technologies for EMG detection and control of prosthetic devices such as implantable myoelectric sensor46 requires certain revisions of the standard sockets. Namely, implantable myoelectric sensor compatible shafts are equipped with transmitter/receiver coil capable of enclosing the stump and receiving the signal transmitted by the implanted EMG electrodes.47
Other, more research-oriented, invasive solutions, such as implantable electrode arrays,48 fine wire-based systems,49 and epimysial electrodes,50 are at a prototype stage. Nerve interfacing solutions51 for efferent decoding remain currently highly complex without sufficient benefits.
Control strategies
Myoelectric prosthetic upper limbs have been known for over half a century.11 As previously elaborated, advances have been made in many aspects of these devices. Yet, the commercially available control systems up until recently have practically remained unchanged. The initial two-channel control allowing direct proportional steering of a single DoF has been extended to sequentially drivable multiple DoFs using a state machine approach.52 With this approach, the user can decide which DoF of the device to control by cycling through states using co-contractions or by quickly repeating a specific muscle activation pattern.53,54 For example, Michelangelo hand users may switch between DoFs by modulating the contraction speed.54 Regardless, all these approaches, even though quite robust, are unintuitive and cumbersome especially in the high-level amputation cases, which require articulation of numerous DoFs.55
Some prosthetic hand vendors proposed a decrease in the direct control by the user, with the introduction of supportive technologies. For example, BeBionic v3 has a plain switch for alternating between groups of preset grip types.56 Touch Bionics offers i-mo™ technology (Touch Bionics Inc., Livingston, UK) that utilizes gyroscopes in order to detect sudden, user-elicited direction changes of the device that is used to select preset gestures.57 Moreover, users of modern prosthetics are now given access to applications that can run on external devices capable of fine tuning and setting up gestures or gesture patterns.56,58,59 This allows high-level customization. Touch Bionics even proposed the exchange of control settings through QR codes.60 Finally, the same company introduced the so-called “grip chips” that can automatically preshape the hand once the prosthetic finds itself in the close proximity of one of these devices. Chips can then be placed in the characteristic spots within the user’s everyday environment.61 Even though promising, all these novel features are yet to be clinically tested and their impact on the improvement of the quality of life remains to be demonstrated.
Academia has been extensively working on numerous prosthetic control solutions in the form of machine-learning approaches that are mostly based on the assumption that distinguishable and repeatable signal patterns exist among different motor tasks.62,63 There are several classification schemes proposed in the past several decades. However, the transition from the laboratory tests to the clinical and everyday practice has been very challenging. Only recently, a first pattern recognition-based system, COAPT,64 has become commercially available, but it is yet to be seen how well this system will be accepted in the market.
The main issue of EMG pattern recognition-based systems is that they rely on repeatable matching of the produced EMG patterns during prosthetic manipulation to those used for system training. On the other hand, these patterns tend to significantly change due to environmental factors such as sweat or electrode shift, as well as fatigue, load, limb position, or simply due to the user’s change of focus.65–69 Another drawback of these solutions is their limited ability to successfully cope with simultaneous motions, which makes them still not fully intuitive and somewhat cognitively demanding.70
In order to overcome some of these issues, a new direction in myoelectric control research has been taken and biologically inspired algorithms have been designed. They combine techniques of mathematical regression with physiologically based models that allow intuitive control.71,72 These systems may enable the users to intuitively control multiple DoFs in a simultaneous and proportional way.73,74 These techniques have shown promising potential, though they are limited in the number of DoFs that can be controlled, at least without relying on nonintuitive motions and high-density EMG recordings.75
Recently, a system that combines signal classification and regression for the control of the hand and wrist, respectively, has been proposed,76 although full clinical testing is still lacking.77
Surgical techniques for improved prosthetic experience
The importance of a proper stump management has been recognized long time ago, and its influence on prosthetic fitting, control, and acceptance can be significant.78 Various surgical techniques have been used for salvation or restoration of the affected hand and arm function, thus enabling simpler and more efficient prosthetic solutions. Among others, these surgical methods include surgical tendon transfers,79,80 a variety of flaps,81–84 digit and toe transfers,85–87 and skin grafting.88,89
Mastering of the aforementioned techniques and broadening of the knowledge about nerve transfers in the past decade led to the development of TMR that transfers residual nerves that have lost their original targeted muscles to alternative muscle sites.90 By treating muscles as biological amplifiers of the signals transmitted through nerves,91 TMR allows reformation of several well-separated sources of intuitive EMG signals, which can be of high value for prosthetic control.92 The Ottobock DynamicArm Plus in combination with the MyoHand Vari PlusSpeed terminal device accompanied by Wrist Rotator and a custom TMR socket enables the control of up to six DoFs following successful TMR procedure. To our knowledge, this is currently the only strictly TMR dedicated commercially available prosthetic solution on the market.
Recently, the concept of bionic reconstruction has been proposed for various scenarios after hand/arm trauma, extending the reconstructive options beyond the biological scope. In patients suffering from severe brachial plexus injuries presenting permanent hand dysfunction, which is beyond restoration using usual biological means alone, bionic reconstruction can offer a valid solution for restoring hand use where even the simplest of the aforementioned terminal devices are now allowing them to have better quality of life.93 The success of this technique depends on numerous factors. One of the crucial aspects is the neurorehabilitation program that is delivered to the patients throughout the procedure.
Conclusion
By observing the current state of the upper limb prosthetic market, the most rapid development occurred during the last decade as the result of advances in technology, surgical techniques, and increased knowledge of human anatomy and physiology.
We have presented some of the latest prosthetic solutions on the market and have given insights in what academia is able to offer in the upcoming period. These systems offer numerous features when equipped with the state-of-the-art technology. Nowadays, prosthetic hands closely resemble the anatomical dimensions of their biological counterparts, while the solutions for higher level impairments are yet to match these specifications. Prosthetic solutions replacing certain DoFs, such as shoulder movements, are still missing.
The introduction of modern materials has allowed better and more intimate socket design that enables improved prosthetic experience for the users. This facilitated development of new socket fitting techniques allow orthopedic technicians to custom-match the residual limb anatomy of each user. Advances in implant design have come to a point where prosthetic fitting through osseointegration is a viable option. This kind of interface, directly coupled to the user’s skeletal system, provides increased range of motion and osseoperception. Following the advances of implantable sensor technologies, the new socket designs include features harvesting the significant potential of such solutions through embedded transmitter/receiver coils.
In order to improve the functional potential of upper limb-impaired patients, new surgical techniques have been recently proposed. TMR and bionic reconstruction, for example, provide important functional benefits to the user, in particular for high-level amputees and patients with brachial plexus injuries.
The current bottleneck of the upper limb prosthetic development seems to be the control of the robotic limbs. The majority of commercially available devices are still relying on the cumbersome mode-switching approaches dating some decades ago, while novel techniques seem to continuously fail in making a stable transition into the market. There are new solutions that have recently emerged but that have not yet been tested clinically on a large scale.
High prosthetic abandonment rates are still present, though they have been stagnating compared to the trends from about two decades ago. This can be attributed to the significant improvement in robustness and hardware design. Nevertheless, in order for these figures to start dropping, advances are still needed in prosthetic control, general system simplification, and custom, user-oriented solutions.
Acknowledgments
This work was supported by the Christian Doppler Research Foundation of the Austrian Federal Ministry of Science, Research and Economy and by the European Research Council Advanced Grant DEMOVE (contract #267888).
Disclosure
The authors report no conflicts of interest in this work.
References
Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010;(26):1–31. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20726217. Accessed June 1, 2016. | ||
Ootes D, Lambers KT, Ring DC. The epidemiology of upper extremity injuries presenting to the emergency department in the United States. Hand (N Y). 2012;7(1):18–22. | ||
Larsen CF, Mulder S, Johansen AM, Stam C. The epidemiology of hand injuries in the Netherlands and Denmark. Eur J Epidemiol. 2004;19(4):323–327. | ||
U.S Department of Labor, Bureau of Labor Statistics. Work Related Hand Injuries and Upper Extremity Amputation0073. Washington, DC: U.S. Department of Labor; 1982. [Bulletin 2]. | ||
Kahn AP. The Encyclopedia of Work-Related Hand Injuries and Upper Extremity Amputations. New York, NY: Facts on File; 2004. | ||
Rettig AC. Athletic injuries of the wrist and hand. Am J Sports Med. 2004;32(1):262–273. | ||
Grunert BK, Smithr JS, Devine CA, et al. Early psychological aspects of severe hand injury. J Hand Surg Am. 1988;13-B(2):177–180. | ||
Grob M, Papadopulos NA, Zimmermann A, Biemer E, Kovacs L. The psychological impact of severe hand injury. J Hand Surg Eur Vol. 2008;33(3):358–362. | ||
Putti V. Historical Prostheses. J Hand Surg . 2005;30:310–325. | ||
Merrill DR, Lockhart J, Troyk PR, Weir RF, Hankin DL. Development of an implantable myoelectric sensor for advanced prosthesis control. Artif Organs. 2011;35(3):249–252. | ||
Childress D. Historical aspects of powered limb prostheses. Clin Prosthet Orthot. 1985;9(1):2–13. | ||
Marquardt E. The Heidelberg pneumatic arm prosthesis. J Bone Jt. 1965;47(3):425. | ||
Biddiss E, Chau T. Upper-limb prosthetics: critical factors in device abandonment. Am J Phys Med Rehabil. 2007;86(12):977–987. | ||
Pylatiuk C, Schulz S, Döderlein L. Results of an Internet survey of myoelectric prosthetic hand users. Prosthet Orthot Int. 2007;31(4):362–370. | ||
Egermann M, Kasten P, Thomsen M. Myoelectric hand prostheses in very young children. Int Orthop. 2009;33(4):1101–1105. | ||
McFarland LV, Hubbard Winkler SL, Heinemann AW, Jones M, Esquenazi A. Unilateral upper-limb loss: satisfaction and prosthetic-device use in veterans and servicemembers from Vietnam and OIF/OEF conflicts. J Rehabil Res Dev. 2010;47(4):299–316. | ||
Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294–303. | ||
Silcox H, Rooks M, Vogel RR, Fleming LL. Myoelectric prostheses. A long-term follow-up and a study of the use of alternate prostheses. J Bone Joint Surg Am. 1993;75(12):1781–1789. | ||
Burrough SF, Brook JA. Patterns of acceptance and rejection of upper limb prostheses. Orthot Prosthet. 1985;39(2):40–47. | ||
Glynn M, Galway H, Hunter G, Sauter W. Management of the upper-limb-deficient child with a powered prosthetic device. Curr Orthop Pract. 1986;(209):202–205. | ||
Jones JW, Gruber SA, Barker JH, Breidenbach WC. Successful hand transplantation one-year follow-up. N Engl J Med. 2000;343(7):468–473. | ||
Salminger S, Sturma A, Roche A, et al. [Hand function after hand transplant and prosthetic reconstruction] Handfunktion nach Handtransplantation und prothetischer Rekonstruktion. In: 38. Seminar – Surgery meets Biomedical Engineering. Austrian Society for Surgical Research, Wagrain, Austria. 2014. | ||
Vincent Systems [webpage on the Internet]. Vincent Evolution 2; 2016. Available from: www.vincentsystems.de/en/prosthetics/vincent-evolution-2/. Accessed June 21, 2016 | ||
Resnik L, Klinger SL, Etter K. The DEKA arm: its features, functionality, and evolution during the veterans affairs study to optimize the DEKA arm. Prosthet Orthot Int. 2014;38(6):492–504. | ||
Resnik L, Klinger SL, Etter K. User and clinician perspectives on DEKA arm: results of VA study to optimize DEKA arm. J Rehabil Res Dev. 2014;51(1):27–38. | ||
Sears HH, Iversen E, Archer S, Jacobs T. Wrist innovations to improve function of electric terminal devices. In: Proc 2008 MyoElectric Control Prosthetics Symp. 2008:13–16. | ||
Bennett DA, Mitchell J, Goldfarb M. Design and characterization of a powered elbow prosthesis. In: 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE; 2015:2458–2461. | ||
Lipschutz RD, Kuiken TA, Miller LA, Dumanian GA, Stubblefield KA, Otr L. Shoulder disarticulation externally powered prosthetic fitting following targeted muscle reinnervation for improved myoelectric control. Prosthet Orthot Int. 2006;18(2):245–253. | ||
FDA [webpage on the Internet]. FDA allows marketing of first prosthetic arm that translates signals from person’s muscles to perform complex tasks. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm396688.htm. Accessed February 24, 2016. | ||
Lake C. The evolution of upper limb prosthetic socket design. JPO J Prosthet Orthot. 2008;20(3):85. | ||
Daly W, Voo L, Rosenbaum-Chou T, Arabian A, Boone D. Socket pressure and discomfort in upper-limb prostheses: a preliminary study. JPO J Prosthet Orthot. 2014;26(2):99–106. | ||
Biddiss EA, Chau TT. Upper limb prosthesis use and abandonment: a survey of the last 25 years. Prosthet Orthot Int. 2007;31(3):236–257. | ||
Hepp O, Kuhn GG. Upper extremity prostheses. In: Prosthetics International, Proceedings of the Second International Prosthetics Course. Committee on Prosthetics, Braces, and Technical Aids, International Society for the Welfare of Cripples, Copenhagen, Denmark: 1960:133–181. | ||
Billock JN. The Northwestern University supracondylar suspension technique for below-elbow amputations. Orthot Prosthet. 1972;26(4):16–23. | ||
Uellendahl JE, Ramdial S. Custom silicone sockets for myoelectric prostheses. In: MEC ’05 Intergrating Prosthetics and Medicine Proceedings of the 2005 MyoElectric Controls/Powered Prosthetics Symposium. Fredericton, NB: 2005:21–24. | ||
Alley RD. Advancement of upper extremity prosthetic interface and frame. In: MEC ’02 The Next Generation Proceedings of the 2002 MyoElectric Controls/Powered Prosthetics Symposium. Fredericton, NB: 2002. | ||
Branemark PI. Osseointegration and its experimental background. J Prosthet Dent. 1983;50(3):399–410. | ||
Brånemark R, Brånemark P-I, Rydevik B, Myers RR. Osseointegration in skeletal reconstruction and rehabilitation: a review. J Rehabil Res Dev. 2001;38(2):175–181. | ||
Tjellstrom A, Lindstrom J, Hallen O, Albrektsson T, Brånemark P-I. Osseointegrated titanium implants in the temporal bone. A clinical study on bone-anchored hearing aids. Am J Otol. 1981;2(4):304–310. | ||
Brånemark P-I, Chien S, editors. The Osseointegration Book: From Calvarium to Calcaneus. Hanover Park, IL: Quintessence Publishing Company; 2005. | ||
Jönsson S, Caine-Winterberger K, Brånemark R. Osseointegration amputation prostheses on the upper limbs: methods, prosthetics and rehabilitation. Prosthet Orthot Int. 2011;35(2):190–200. | ||
Gallagher P, Desmond D, MacLachlan M, editors. Psychoprosthetics. Berlin: Springer-Verlag; 2007. | ||
Klineberg I, Murray G. Osseoperception: sensory function and proprioception. Adv Dent Res. 1999;13:120–129. | ||
Zuo KJ, Olson JL. The evolution of functional hand replacement: from iron prostheses to hand transplantation. Can J Plast Surg. 2014;22(1):44–51. | ||
Shelton TJ, Beck PJ, Bloebaum RD, Bachus KN. Percutaneous Osseointegrated prostheses for amputees: limb compensation in a 12-month ovine model. J Biomech. 2011;44(15):2601–2606. | ||
Weir RFF, Troyk PRR, DeMichele G, Kuiken T, Ku T. Implantable myoelectric sensors (IMES) for upper-extremity prosthesis control- preliminary work. In: Proc 25th Annu Int Conf IEEE Eng Med Biol Soc. IEEE, Cancun, Mexico. 2003;(2):1562–1565. | ||
Weir R, Troyk P, Demichele G, Kerns D. Technical details of the implantable myoelectric sensor (IMES) system for multifunction prosthesis control. Conf Proc IEEE Eng Med Biol Soc. 2005;7:7337–7340. | ||
Muceli S, Poppendieck W, Negro F, et al. Accurate and representative decoding of the neural drive to muscles in humans with multi-channel intramuscular thin-film electrodes. J Physiol. 2015;593(17):3789–3804. | ||
Cipriani C, Segil JL, Birdwell JA, Weir RF. Dexterous control of a prosthetic hand using fine-wire intramuscular electrodes in targeted extrinsic muscles. IEEE Trans Neural Syst Rehabil Eng. 2014;22(4):828–836. | ||
Farnsworth BD, Talyor DM, Triolo RJ, Young DJ. Wireless in vivo EMG sensor for intelligent prosthetic control. In: TRANSDUCERS 2009 – 15th Int Conf Solid-State Sensors, Actuators Microsystems. IEEE, Denver, CO, USA. 2009:358–361. | ||
Micera S, Navarro X, Carpaneto J, et al. On the use of longitudinal intrafascicular peripheral interfaces for the control of cybernetic hand prostheses in amputees. IEEE Trans Neural Syst Rehabil Eng. 2008;16(5):453–472. | ||
Scott RN, Parker PA. Myoelectric prostheses: state of the art. J Med Eng Technol. 1988;12(4):143–151. | ||
RSL Steeper. BeBionic v3 Product Brochure. Leeds: RSL Steeper;2013. | ||
Otto Bock Healthcare GmbH. FDA 510(k) Premarket Notification: Summary Axon-Bus Prosthetic System. Silver Spring, MD: Otto Bock Healthcare GmbH; 2014. [20993-0002]. | ||
Williams TW 3rd. Practical methods for controlling powered upper-extremity prostheses. Assist Technol. 1990;2(1):3–18. | ||
RSL Steeper. Upper Limb Prosthetic Components – Technical Product Brochure. Leeds: RSL Steeper; 2014. | ||
Touch Bionics [webpage on the Internet]. How the i-limb works. Available from: http://www.touchbionics.com/products/how-i-limb-works. Accessed April 29, 2016. | ||
Touch Bionics. Biosim-i My i-limb Datasheet. Mansfield, MA: Touch Bionics; 2014. | ||
Otto Bock Healthcare GmbH. Michelangelo Technican Product Brochure. Duderstadt: Otto Bock Healthcare GmbH; 2013. | ||
Touch Bionics [webpage on the Internet]. i-limb QR codes. Available from: http://www.touchbionics.com/resources/qr-codes. Accessed April 29, 2016. | ||
Touch Bionics. Grip Chips – Product Overview. Mansfield, MA: Touch Bionics; 2015. | ||
Hudgins B, Parker P, Scott RN. A new strategy for multifunction myoelectric control. IEEE Trans Biomed Eng. 1993;40(1):82–94. | ||
Graupe D, Salahi J, Kohn KH. Multifunctional prosthesis and orthosis control via microcomputer identification of temporal pattern differences in single-site myoelectric signals. J Biomed Eng. 1982;4(1):17–22. | ||
Coapt LLC [homepage on the Internet]. Coapt Engineering; 2016. Available from: http://www.coaptengineering.com/. Accessed April 29, 2016. | ||
Young AJ, Hargrove LJ, Kuiken TA. The effects of electrode size and orientation on the sensitivity of myoelectric pattern recognition systems to electrode shift. IEEE Trans Biomed Eng. 2011;58(9):2537–2544. | ||
Hargrove L, Englehart K, Hudgins B. A training strategy to reduce classification degradation due to electrode displacements in pattern recognition based myoelectric control. Biomed Signal Process Control. 2008;3(2):175–180. | ||
Stango A, Negro F, Farina D. Spatial correlation of high density EMG signals provides features robust to electrode number and shift in pattern recognition for myocontrol. IEEE Trans Neural Syst Rehabil Eng. 2015;23(2):189–198. | ||
Ortiz-Catalan M, Brånemark R, Håkansson B, Delbeke J. On the viability of implantable electrodes for the natural control of artificial limbs: review and discussion. Biomed Eng Online. 2012;11(1):33. | ||
Roche AD, Rehbaum H, Farina D, Aszmann OC. Prosthetic myoelectric control strategies: a clinical perspective. Curr Surg Rep. 2014;2(3):44. | ||
Jiang N, Dosen S, Farina D [webpage on the Internet]. Myoelectric control of artificial limbs: is there the need for a change of focus? IEEE Signal Process Mag. 2012; 12–15. Available from: http://www.lifesciences.ieee.org/articles/174-myoelectric-control-of-artificial-limbs-is-there-a-need-to-change-focus. Accessed June 27, 2013. | ||
Jiang N, Englehart KB, Parker PA. Extracting simultaneous and proportional neural control information for multiple-DOF prostheses from the surface electromyographic signal. IEEE Trans Biomed Eng. 2009;56(4):1070–1080. | ||
Jiang N, Rehbaum H, Vujaklija I, Graimann B, Farina D. Intuitive, online, simultaneous, and proportional myoelectric control over two degrees-of-freedom in upper limb amputees. IEEE Trans Neural Syst Rehabil Eng. 2014;22(3):501–510. | ||
Jiang N, Vujaklija I, Rehbaum H, Graimann B, Farina D. Is accurate mapping of EMG signals on kinematics needed for precise online myoelectric control? IEEE Trans Neural Syst Rehabil Eng. 2014;22(3):549–558. | ||
Hofmann D, Jiang N, Vujaklija I, Farina D. Bayesian filtering of surface EMG for accurate simultaneous and proportional prosthetic control. IEEE Trans Neural Syst Rehabil Eng. Epub 2015 Nov 20:1. | ||
Ison M, Vujaklija I, Whitsell B, Farina D, Artemiadis P. High-density electromyography and motor skill learning for robust long-term control of a 7-DoF robot arm. IEEE Trans Neural Syst Rehabil Eng. 2016;24(4):424–433. | ||
Amsuess S, Vujaklija I, Gobel P, et al. Context-dependent upper limb prosthesis control for natural and robust use. IEEE Trans Neural Syst Rehabil Eng. Epub 2015 Jul 9:1. | ||
Roche AD, Vujaklija I, Amsuess S, et al. Structured rehabilitation training for improved multifunctional prosthetic control : a case study. J Vis Exp. 2015;(105):e52968. | ||
Dederich R. Plastic treatment of the muscles and bone in amputation surgery a method designed to produce physiological conditions in the stump. J Bone Joint Surg Am. 1963;45(B):60–66. | ||
Lieber RL. Skeletal muscel architecture implications for muscle function and surgical tendon transfer. J Hand Ther. 1993;6(2):105–113. | ||
Cooney WP, Linscheid RL, An KN. Opposition of the thumb: an anatomic and biomechanical study of tendon transfers. J Hand Surg Am. 1984;9(6):777–786. | ||
May JW, Gordon L. Palm of hand free flap for forearm length preservation in nonreplantable forearm amputation: a case report. J Hand Surg Am. 1980;5(4):377–380. | ||
Ulusal BG, Lin Y-T, Ulusal AE, Lin C-H. Free lateral arm flap for 1-stage reconstruction of soft tissue and composite defects of the hand: a retrospective analysis of 118 cases. Ann Plast Surg. 2007;58(2):173–178. | ||
Brandt K, Khouri RK, Upton J. Free flaps as flow-through vascular conduits for simultaneous coverage and revascularization of the hand or digit. Plast Reconstr Surg. 1996;98(2):321–327. | ||
Neumeister M, Hegge T, Amalfi A, Sauerbier M. The reconstruction of the mutilated hand. Semin Plast Surg. 2010;24(1):77–102. | ||
Blair VP, Byars LT. Toe to finger transplant. Ann Surg. 1940;112:287–290. | ||
Morrison WA, O’Brien B, MacLeod AM. Ring finger transfer in reconstruction of transmetacarpal amputations. J Hand Surg Am. 1984;9A(1):4–11. | ||
Foucher G, Moss ALH. Microvascular second toe to finger transfer: a statistical analysis of 55 transfers. Br J Plast Surg. 1991;44(2):87–90. | ||
Canty TJ, Bleck EE. Split-thickness skin grafting of amputation stumps. Plast Reconstr Surg. 1952;10(2):99–115. | ||
Wood MR, Hunter GA, Millstein SG. The value of stump split skin grafting following amputation for trauma in adult upper and lower limb amputees. Prosthet Orthot Int. 1987;11(2):71–74. | ||
Kuiken TA, Dumanian GA, Lipschutz RD, Miller LA, Stubblefield KA. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthet Orthot Int. 2004;28(3):245–253. | ||
Hoffer J, Loeb G. Implantable electrical and mechanical interfaces with nerve and muscle. Ann Biomed Eng. 1980;8(4):351–360. | ||
Kuiken TA, Li G, Lock BA, et al. Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms. JAMA. 2009;301(6):619–628. | ||
Aszmann OC, Roche AD, Salminger S, et al. Bionic reconstruction to restore hand function after brachial plexus injury : a case series of three patients. Lancet. 2015;385(9983):2183–2189. | ||
Hosmer Dorrance Corporation. Hosmer Upper Extremity Product Catalog; 2012. Available from: http://hosmer.com/products/PDFs/Fillauer Product Catalog.pdf. Accessed June 1, 2016. | ||
Hosmer Dorrance Corporation. Hooks, Hands, and Wrists – Product Brochure; 2003:1–58. Available from: http://hosmer.com/products/book3/pdfs/2-HooksHandsWrists.pdf. Accessed June 1, 2016. | ||
Otto Bock Healthcare GmbH. Upper Limb Prosthetics Catalog. Vol. 4. Duderstadt: Otto Bock Healthcare GmbH; 2014:177–184. | ||
Liberating Technologies Inc. Select Electric Hands for Adults Product Catalog. Holliston, MA: Liberating Technologies Inc. 2013. | ||
Liberating Technologies Inc [homepage on the Internet]. Select Electric Hands & Gloves Data Sheet; 2010. Available from: http://www.liberatingtech.com/products/documents/LTI_Data_Sheet_-_Electric_Hands_&_Wrists.pdf. Accessed June 21, 2016. | ||
Touch Bionics. i-Limb Quantum Clinician Manual. Mansfield, MA: Touch Bionics; 2015. [MA 01333 Issue No 1.]. | ||
Touch Bionics. i-Limb Quantum User Manual. 2015; 1(1):1–21. Available from: http://www.touchbionics.com/sites/default/files/files/i-limb quantum user manual July 2015.pdf. Accessed June 1, 2016. | ||
Touch Bionics. i-Limb Quantum Product Sheet. Mansfield, MA: Touch Bionics; 2015:1–2. | ||
Touch Bionics. Flexion Wrist Product Sheet. Mansfield, MA: Touch Bionics; 2015:1–2. | ||
Fillauer. Utah Arm 3 Plus Sales Sheet. Chattanooga, TN: Fillauer; 2012. | ||
Hussain I, Masood A, Iqbal J, Khan US. Design of high torque elbow joint for above elbow prosthesis. Int J Mech Aerosp Ind Mechatron Eng. 2011;5(11):318–321. | ||
Boston Digital. Boston Digital Arm System Catalog. Auckland: Boston Digital. 2013. | ||
Otto Bock Healthcare GmbH. Elbow Components – At a Glance. Duderstadt: Otto Bock Healthcare GmbH. 2014. | ||
Hosmer Dorrance Corporation Externally Powered Systems Product Catalog. Campbell, CA, 2015(18). Available at: http://hosmer.com/products/book3/pdfs/4-ExternallyPoweredSystems.pdf. Accessed June 21, 2016. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.