")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 13
New developments in optimizing bronchodilator treatment of COPD: a focus on glycopyrrolate/formoterol combination formulated by co-suspension delivery technology
Authors D'Urzo AD, Cazzola M , Hanania NA, Buhl R, Maleki-Yazdi MR
Received 26 February 2018
Accepted for publication 28 June 2018
Published 7 September 2018 Volume 2018:13 Pages 2805—2819
DOI https://doi.org/10.2147/COPD.S113306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Anthony D D’Urzo,1 Mario Cazzola,2 Nicola A Hanania,3 Roland Buhl,4 M Reza Maleki-Yazdi5
1Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, Toronto, ON, Canada; 2Department of Experimental Medicine and Surgery, Tor Vergata University of Rome, Rome, Italy; 3Section of Pulmonary and Critical Care Medicine, Baylor College of Medicine, Houston, TX, USA; 4Pulmonary Department, Mainz University Hospital, Mainz, Germany; 5Division of Respiratory Medicine, Women’s College Hospital, University of Toronto, Toronto, ON, Canada
Abstract: COPD causes considerable health and economic burden worldwide, with incidence of the disease expected to continue to rise. Inhaled bronchodilators, such as long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABAs), are central to the maintenance treatment of patients with COPD. Clinical studies have demonstrated that combined LAMA + LABA therapies improve efficacy while retaining a safety profile similar to LAMA or LABA alone. This has led to the development of several LAMA/LABA fixed-dose combination (FDC) therapies, which provide patients with the convenience of two active compounds in a single inhaler. GFF MDI (Bevespi Aerosphere®) is an FDC of glycopyrrolate/formoterol fumarate 18/9.6 µg formulated using innovative co-suspension delivery technology for administration via metered dose inhaler (MDI). GFF MDI was developed to make a treatment option available for patients who have a requirement or preference to use an MDI, rather than a dry powder or soft mist inhaler. Now that several LAMA/LABA FDCs have been approved for use in COPD, we review the impact of dual-bronchodilator treatment on COPD therapy and discuss recent clinical studies that are helping to develop a more comprehensive understanding of how LAMA/LABA FDCs can improve patient outcomes.
Keywords: long-acting bronchodilator, LAMA, LABA, chronic obstructive pulmonary disease, fixed-dose combination, GFF MDI
Abbreviations
ACL, aclidinium bromide; AUC0–12, area under the curve from 0 to 12 hours; BID, twice daily; BUD-FF, budesonide–formoterol fumarate; CAT, COPD Assessment Test; CID, clinically important deterioration; DPI, dry powder inhaler; FDC, fixed-dose combination; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GFF, glycopyrrolate/formoterol fumarate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GP, glycopyrrolate; IC, inspiratory capacity; ICS, inhaled corticosteroid; IND, indacaterol; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LSM, least squares mean; MDI, metered dose inhaler; mMRC, modified Medical Research Council (scale); MSCT, multislice computed tomography; OLO, olodaterol; PRO, patient-reported outcome; QD, once daily; SAL, salmeterol; SD, standard deviation; SGRQ, St George’s Respiratory Questionnaire; SMI, soft mist inhaler; TDI, Transition Dyspnea Index; TIO, tiotropium; UMEC, umeclidinium; VIL, vilanterol.
Introduction
COPD is an umbrella term that encompasses different pathophysiological processes in the lung (eg, emphysema and chronic bronchitis) that result in decline in pulmonary function.1 The condition, which is associated with smoking or exposure to biomass-fuel smoke/air pollution,1 can also occur in people not exposed to these risk factors, highlighting that there are many underlying mechanisms driving the development of the disease and its progression.1 Due to increasing exposure to risk factors and aging populations, COPD rates are projected to continue to rise.1,2 Here, we review the impact of dual-bronchodilator therapies on COPD therapy and how current clinical studies may further our understanding of how to optimize bronchodilator use in reducing the burden of COPD for patients, since improvements in lung function are linked with greater benefits in patient-reported outcomes (PROs).3
Burden of disease
In the Continuing to Confront COPD International Patient Survey across North and South America, Asia, and Europe in 2012–2013, approximately 7%–9% of people ≥40 years of age in all the countries included, except Brazil (12%), fulfilled the case definition of COPD.4 For the countries that participated in the corresponding study in 1999–2001, this represented an absolute increase of 1%–4%.4,5 Case-finding studies have demonstrated that the majority of individuals with COPD have not previously received a diagnosis, so the reported rates of COPD are likely to be an underestimation of actual prevalence.6–9
An international survey conducted in 14 countries in 2010 demonstrated that ≥78% of patients with COPD, chronic bronchitis, and/or emphysema experienced symptoms of breathlessness on exertion, with the majority of patients reporting fatigue, mucus/sputum/phlegm production, or chronic/troublesome cough.10 The same study found that 77% of patients were worried about their long-term health, and many (38% with a Medical Research Council [MRC] dyspnea-scale score ≤2 and 59% with an MRC score ≥3) feared premature death due to COPD.10 COPD symptoms are associated with reduced physical activity levels and sleep disturbance.11,12 The BREATHE study conducted in eleven countries across the Middle East, north Africa, and Pakistan also found that psychological distress was reported by a substantial proportion of patients with COPD (42.3%–53.2%).13 The combination of the negative physical and mental impact of COPD results in reduced quality of life for patients suffering with the disease.14,15 Despite treatments available for COPD, a survey conducted in 2013 reported that the symptom burden remained high for >80% of patients,16 and few patients in a 2010 survey considered their COPD to be “very well” controlled.10
Evolution of bronchodilators in the management of COPD
Long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABAs) have for many years been a cornerstone of pharmacotherapeutic maintenance treatment options for patients with COPD1 (Table 117–31).The delivery method for the different LAMAs and LABAs varies, but includes pressurized metered dose inhalers (MDIs), dry powder inhalers (DPIs), soft mist inhalers (SMIs), and nebulizers.32
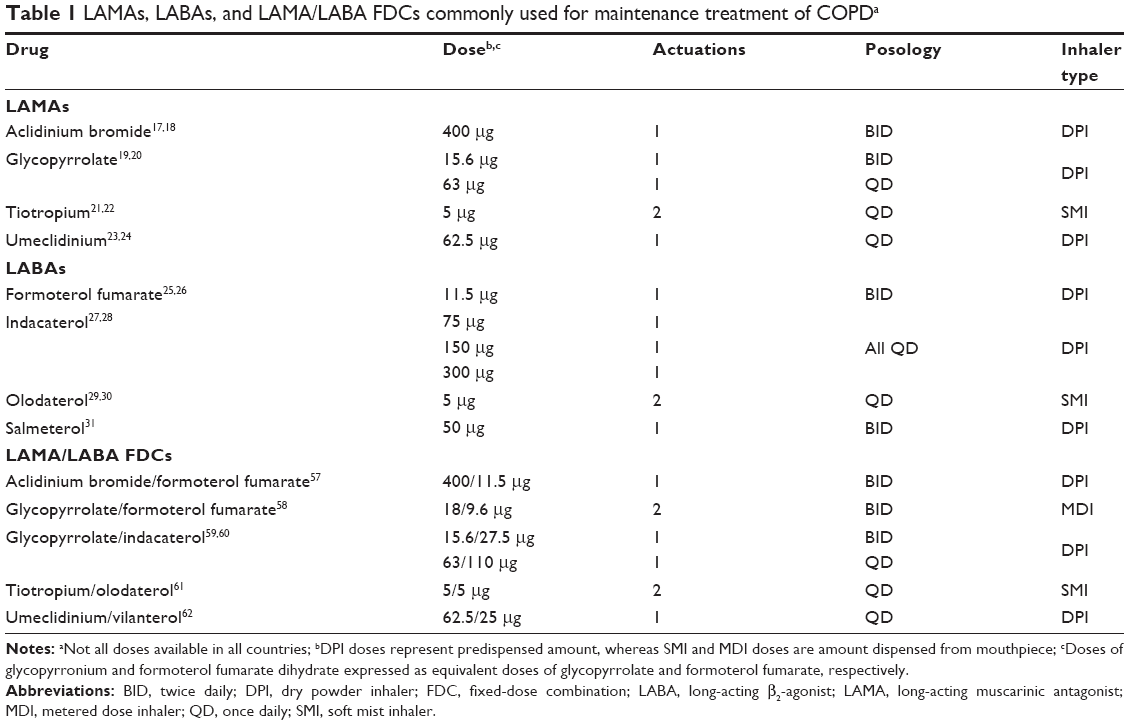 | Table 1 LAMAs, LABAs, and LAMA/LABA FDCs commonly used for maintenance treatment of COPDa |
The LABA formoterol fumarate (FF)25,26 has been a maintenance treatment for COPD since the early 1990s. Other LABAs now commonly used as monotherapies1 include salmeterol (SAL),31 indacaterol (IND),27,28 and olodaterol (OLO).29,30 In the mid-2000s, the LAMA tiotropium (TIO)21,22 became the first of its class to be available as an inhaled therapy for treatment of COPD, with long-term benefits on lung function, quality of life, and exacerbations demonstrated by the 4-year UPLIFT trial.33 Since then, three other LAMAs that have been developed as inhaled monotherapies for the management of COPD are aclidinium bromide (ACL),17,18 umeclidinium (UMEC),23,24 and glycopyrrolate (GP).19,20 A previous literature review34 and a recent network meta-analysis35 found that these newer LAMAs had comparable effectiveness to TIO and one another. Another large network meta-analysis demonstrated that overall, LAMAs and LABAs had similar effects on lung function (trough forced expiratory volume in 1 second [FEV1]) compared with placebo at 6 and 12 months, with little difference in effect between the treatments within each drug class.36 The meta-analysis ranked the LAMA drug class above LABAs for improvements in quality of life (St George’s Respiratory Questionnaire [SGRQ] score) vs placebo at 6 months, but there was no notable class difference at 12 months.36 Few studies have examined the efficacy of LAMAs and LABAs head to head. In a 52-week, randomized, parallel-group study in patients with severe COPD and history of one or more moderate-to-severe exacerbation in the previous year, the LABA IND demonstrated noninferiority to the LAMA TIO for improvements in trough FEV1 at week 12.37 However, in terms of annualized exacerbation rates over 52 weeks, IND (0.79) did not show noninferiority to TIO (0.61; ratio 1:29).37 There were no treatment-related differences in the number of patients who reported adverse events or serious adverse events.37
Due to the distinct mechanisms of action of LAMAs and LABAs, the potential additive/synergistic effects of using these drug classes together have been studied extensively.38,39 LAMAs and LABAs are thought to elicit their bronchodilator effects via interactions with muscarinic acetylcholine receptors and β2-adrenoceptors, respectively, with both receptor types located on airway smooth muscle cells and presynaptic parasympathetic nerves.40 The presynaptic action of both LAMAs and LABAs may modulate the release of acetylcholine into the synaptic space.40 On airway smooth muscle cells, LAMAs block the interaction between acetylcholine and muscarinic receptors to prevent cell contraction, while LABAs bind to β2-adrenoceptors to stimulate relaxation of airway smooth muscle.40
Cross talk between β2-adrenoceptors and muscarinic receptors on smooth muscle cells further potentiates the collective relaxation effect of LAMAs and LABAs.40 The differential expression of muscarinic acetylcholine-receptor and β-adrenoceptor subtypes throughout the lungs41 may also contribute to the benefits observed when LAMAs and LABAs are combined. Therefore, when used together, LAMAs and LABAs improve lung function compared with a LAMA or LABA alone, while both monotherapies and dual therapies are generally well tolerated.38,39 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) reports provide an excellent narrative for how bronchodilator treatment recommendations have evolved over time. From the inception of GOLD, when treatment choices were based mainly on lung-function impairment, bronchodilators have been central to an overall approach for managing stable COPD.42 Since the introduction in the 2011 GOLD report of the ABCD assessment tool that stratified COPD severity based on COPD symptoms and risk, recommendations for bronchodilator use have remained largely unchanged for 5 years.43,44 However, as a result of accumulating clinical evidence, from 2017 the GOLD report has placed additional emphasis on LAMA + LABA dual therapy in the treatment paradigm.1,45
In contrast to the treatment recommendations in the 2016 GOLD report, which suggested the combined use of LAMAs + LABAs for GOLD group B (high symptoms/low risk) patients if symptoms do not improve with single agents, GOLD now recommends that initial therapy with two long-acting bronchodilators can be considered for group B patients with severe breathlessness.1,45 Dual LAMA + LABA therapy is also now the preferred second-line treatment option for patients in GOLD group C (low symptoms/high risk), whereas no preference was stated for the alternative treatments listed in GOLD 2016.1,45
A recent study that demonstrated LAMA + LABA dual therapy was superior to inhaled corticosteroid (ICS) + LABA dual therapy at preventing exacerbations in patients with a history of one or more COPD exacerbations during the previous year and a blood eosinophil count ≤600 cells/μL supports the recommendation that patients in GOLD group D (high symptoms/high risk) are started on a LAMA + LABA combination, rather than an ICS + LABA.1,45,46 However, whether LAMA + LABA dual therapy improves exacerbation risk compared with ICS + LABA in patients with two or more COPD exacerbations in the previous year or with a blood-eosinophil count ≥150 cells/μL or ≥3% requires further investigation, as the results in these subgroups did not demonstrate a clear treatment difference.46,47 Prospective clinical trials examining the role of eosinophil levels and exacerbation risk are required, as most current analyses in this area have been based on retrospective data.47–49 Triple therapy with LAMA + LABA + ICS is recommended for patients in GOLD group D who continue to experience exacerbations despite receiving dual therapy (LAMA + LABA or LABA + ICS) or have persistent symptoms while receiving LABA + ICS.1 Studies that will determine the relative benefits of these LAMA + LABA + ICS, LAMA + LABA, and LABA + ICS on exacerbation prevention are ongoing or have recently been completed.50–53
From 2017, GOLD suggested ICS withdrawal may be considered for patients in GOLD group D treated with LAMA + LABA + ICS who still have exacerbations or an elevated risk of adverse events (eg, pneumonia).1,45 Evidence that ICS withdrawal may not increase exacerbation risk supports the notion that some patients could be treated with LAMA + LABA dual therapy after careful withdrawal of ICSs,54,55 though further studies in this regard are required. With the adoption of LAMA + LABA dual therapy, LAMA/LABA fixed-dose combinations (FDCs) have become available for patient convenience and ease of use, which may also help to improve treatment adherence compared with LAMA + LABA treatment with two separate inhalers.56
Pivotal studies for dual LAMA/LABA FDCs versus monotherapy
Currently there are five LAMA/LABA FDCs licensed for maintenance treatment of COPD (Table 1).57–62 Results of the pivotal studies of these LAMA/LABA FDCs are shown in Table 2.63–72 These studies ranged from 12 to 52 weeks in length, and each included trough FEV1 as a primary or coprimary end point, with the exception of the FLIGHT-1 and FLIGHT-2 studies, which both had FEV1 area under the curve from 0 to 12 hours (AUC0–12) at week 12 as the primary end point.63–72 Although the results of these separate studies cannot be compared directly with each other, in general the magnitude of improvements in lung function, rescue medication use and quality of life scores was greatest in patients treated with the LAMA/LABA FDCs compared with the corresponding monotherapies or placebo. When interpreting the rescue medication use and SGRQ score data reported in these different studies, it is important to consider whether the study entry criteria set a minimum baseline-symptom burden, such as modified MRC (mMRC) score ≥2,68,70–72 since the magnitude of improvement in these end points may increase as a function of baseline symptom burden.73 Both onset of action and exacerbation end points have not been included here, as these end points were not reported consistently or at all in many of these pivotal studies,63–72 which highlights a gap that could be addressed in future studies.
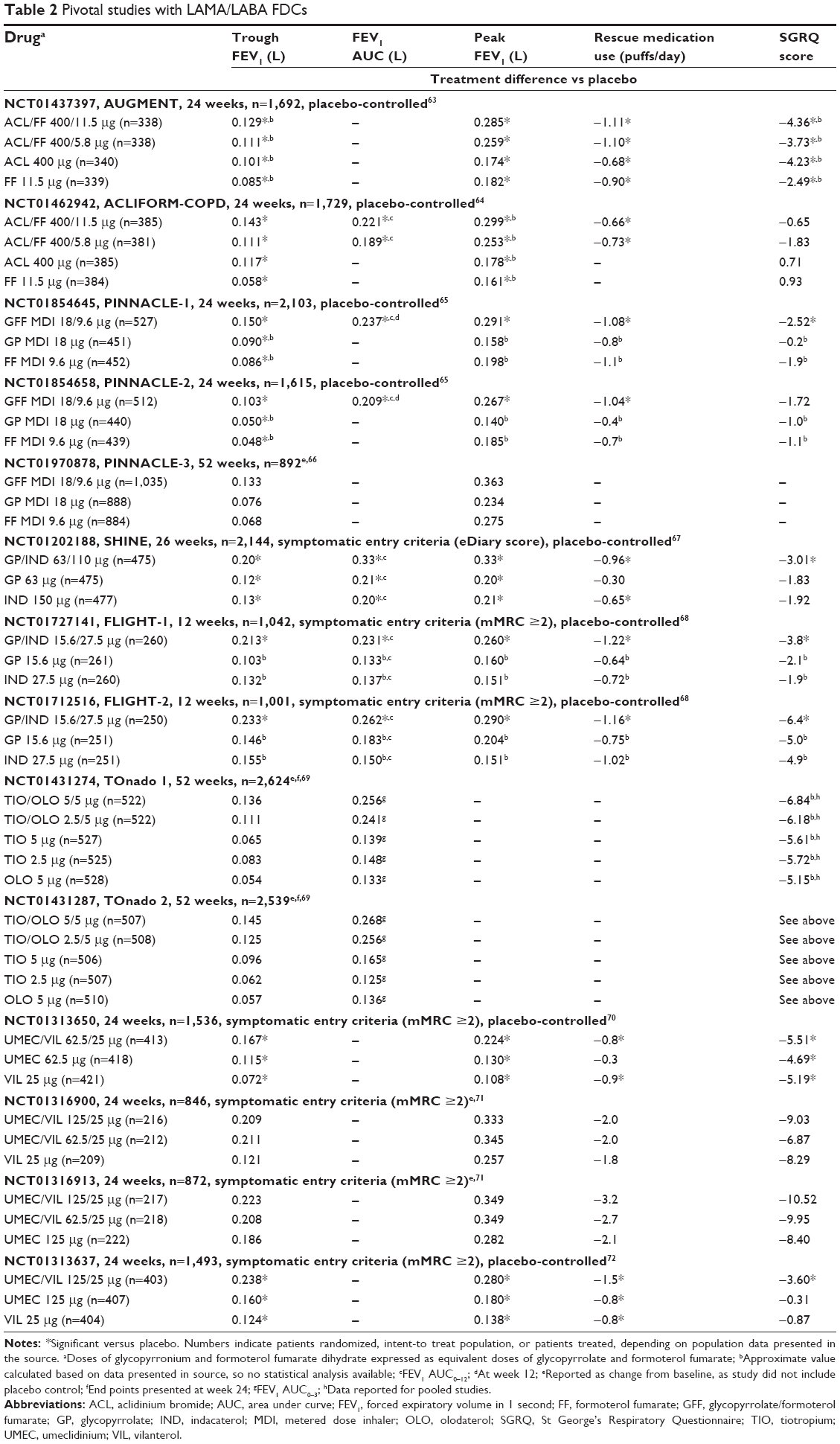 | Table 2 Pivotal studies with LAMA/LABA FDCs |
Meta-analyses of LAMA/LABA FDC studies have confirmed that overall LAMA/LABA FDC therapy improves lung function (trough FEV1), symptoms (transition dyspnea index [TDI] score), and quality of life (SGRQ score) compared with the constituent monocomponents.74,75 The safety profiles of LAMA/LABA FDCs are largely similar to their monocomponents, with little difference in the rate of adverse events, treatment-related adverse events, serious adverse events, and patient discontinuation observed between treatment groups in pivotal studies.63–72
LAMA/LABA FDC head-to-head studies
Recently, three studies reported direct head-to-head efficacy and safety assessments of LAMA/LABA FDCs.76,77 UMEC/vilanterol (VIL) was compared to TIO/OLO (both once daily [QD]) in an 8-week, randomized, crossover, open-label study in patients with symptomatic COPD (mMRC ≥2) and postbronchodilator FEV1 50%–70% predicted normal, the majority of whom (95%) were classified as GOLD group B at baseline.76 UMEC/VIL demonstrated statistically significant increases vs TIO/OLO across lung-function end points examined at weeks 4 and 8 (trough FEV1, forced vital capacity, and inspiratory capacity [IC]).76 However, PROs showed similar improvements with both UMEC/VIL and TIO/OLO, except for change from baseline in rescue medication use (weeks 1–8) and change from baseline in COPD Assessment Test (CAT) score at week 4.76 Safety profiles of the two treatments were similar.76
Two replicate, 12-week, randomized, double-blind, double-dummy, crossover trials compared GP/IND (twice daily [BID]) to UMEC/VIL (QD) in patients with moderate-to-severe COPD and an mMRC score ≥2.77 The primary efficacy objective of noninferiority of GP/IND to UMEC/VIL for change from baseline in FEV1 AUC0–24 at week 12 was not met in either study (least squares mean [LSM] treatment differences [95% CI] −11.5 mL [−26.9 to 3.8 mL] and −18.2 mL [−34.2 to −2.3 mL]).77 No clinically meaningful differences between treatments were reported for rescue medication use or diary-recorded total symptom scores.77 The overall incidence of adverse events was similar between treatment groups.77 A randomized, double-blind, double-dummy, parallel-group study is ongoing to compare glycopyrrolate/formoterol fumarate metered dose inhaler (GFF MDI) BID with UMEC/VIL QD over 24 weeks in patients with moderate-to-very severe COPD.78
If LAMA/LABA FDCs demonstrate similar efficacy and safety in the clinical trial setting, it will be important to consider optimizing their use in real-world situations by considering factors that can influence effective dose administration, such as patient preferences for a particular device and their ability to handle the device correctly.79,80
Highlighting the clinical benefits of dual bronchodilation: insights from GFF MDI
Development of GFF MDI
GFF MDI (Bevespi Aerosphere®, AstraZeneca, Wilmington, DE, USA) is an FDC of glycopyrrolate/formoterol fumarate 18/9.6 μg (equivalent to glycopyrronium/formoterol fumarate dihydrate 10–14.4 μg) delivered by MDI using innovative co-suspension delivery technology. For a comprehensive review of the clinical development program, see Rabe.81 GFF MDI provides a further treatment option for patients with a requirement or preference to use an MDI, rather than a DPI or an SMI, eg, patients who may struggle to achieve the inspiratory flow rate necessary to use a DPI.82,83
Combining respiratory drugs in a suspension-based MDI has been associated with formulation challenges, leading to poor colloidal stability and dosing variability.84 Co-suspension delivery technology overcame these challenges by including spray-dried phospholipid porous particles with drug crystals and propellant.85 As a result, MDIs formulated with co-suspension delivery technology have consistent aerosol performance with single drugs, dual, or triple FDCs,86,87 and overcome the dosing variability associated with simulated patient-handling errors.88 An extensive clinical development program, including nine double-blind studies, was undertaken to establish the dose response for GP and FF alone and in FDC as GFF MDI, in order to identify doses that achieve optimal bronchodilation with this innovative formulation, which could then be taken forward into the pivotal Phase III trials described.89–98
Looking beyond FEV1
To date, Phase III studies of the available LAMA/LABA FDCs have characterized traditional lung-function benefits for the FDCs over LAMA or LABA monotherapies in patients with COPD. In this section, we describe recent studies that have sought to define what could be meant by optimal bronchodilation, in order to gain a more comprehensive understanding of how LAMA/LABA FDCs can improve patient outcomes. We first look at lung deposition and examine aspects of lung function beyond FEV1. Then, we look at patient stratification as a step toward personalizing therapies, with the aim of maximizing the bronchodilation effect for each patient, and lastly whether LAMA/LABA FDCs may potentially slow disease progression.
Lung deposition
Both the large proximal and small distal airways in the lung display pathophysiological changes associated with COPD,99,100 so it is important to characterize the distribution of active compound delivered by a particular inhalation platform to ensure that it reaches the central and peripheral regions. γ-scintigraphy is an established technique for quantifying total lung deposition of inhaled drugs and also regional lung deposition, ie, outer lung versus inner lung.101–104 Taylor et al used γ-scintigraphy to assess the lung deposition of GFF MDI and placebo MDI (porous particles only) in ten healthy male volunteers.105 Both GFF MDI and placebo MDI delivered a similar proportion of the emitted dose to the lungs (mean [SD] 38.4% [10.0] and 32.8% [10.2], respectively), with a very low amount of the dose subsequently exhaled (mean [SD] 0.25% [0.26] and 0.24% [0.13], respectively).105 The proportion of GFF MDI and placebo MDI delivered to the lungs was similar to the result in healthy volunteers who received an ICS/LABA FDC delivered by MDI (mean [SD] 34.1 [9.3]).106 In relation to the regional distribution of GFF MDI and placebo MDI, doses emitted were deposited in both central and peripheral lung regions, with similar mean regional airway-deposition ratios (standardized central/peripheral [SD]) observed for GFF MDI and placebo MDI (1.85 [0.72] and 1.94 [1.15], respectively).105 de Backer et al reported a numerically greater central:peripheral ratio in patients with COPD vs healthy subjects,106 which is consistent with the disease causing deterioration of function in the distal airways of the lung.
Lung volumes
COPD is characterized by airflow limitation and defined by postbronchodilator FEV1:forced vital capacity ratio <0.7.1 However, FEV1 deterioration represents only part of the pathophysiology of COPD. Reduced expiratory airflow in patients with COPD, insufficient expiration during cycles of breathing, and decreased lung elasticity due to emphysema can lead to air becoming trapped, which contributes to lung hyperinflation.107,108 Lung hyperinflation can worsen at times when expiratory flow is suddenly reduced, such as during an exacerbation or bronchospasm, or when the rate of breathing is accelerated, such as during exercise.107,109
Lung hyperinflation is linked with reduced exercise capacity,110 both of which are independent predictors of increased mortality in COPD.111,112 Reducing lung hyperinflation has also been proposed to be one of the mechanisms by which bronchodilators reduce exacerbations.113 IC is an indirect measure of lung hyperinflation, since it decreases as more air becomes trapped in the lungs.107 Therefore, therapies that increase IC may help improve exercise tolerance, lower exacerbation risk, and ultimately result in a better prognosis for patients with COPD.
It has been established that long-acting bronchodilators can improve IC in patients with COPD,109 but relatively little is known about the magnitude of effect of LAMA/LABA FDCs on IC. In two 4-week, 24-hour lung-function studies in patients with COPD, GFF MDI significantly improved the peak change from baseline in IC compared with placebo MDI following both the evening and morning doses on day 29 (LSM difference 248–381 mL, all P<0.0001.)114 GFF MDI administered BID also significantly increased IC in both the evening and the morning relative to open-label TIO SMI QD (LSM differences 124 mL [P=0.0035] and 80 mL [P=0.0287], respectively).114
A post hoc IC-responder analysis of pooled data from the two 24-hour lung-function studies demonstrated that at both morning and evening assessments, treatment with GFF MDI had resulted in higher proportions of patients achieving a response in peak IC across all thresholds (>10%, >15%, >20%, >200 mL, >300 mL, and >400 mL increase from baseline) compared with patients treated with placebo MDI or open-label TIO SMI.114 For example, in the evening on day 29, 46.5% of patients treated with GFF MDI had achieved a >400 mL peak increase from baseline in IC vs 10.3% of patients treated with placebo MDI and 20.9% of patients treated with open-label TIO SMI.114 The results of these studies demonstrated that GFF MDI treatment led to improvements in IC that were sustained over 24 hours.114
Several other studies have examined the effect of LAMA/LABA FDCs on IC in patients with moderate-to-severe COPD.115–118 GP/IND significantly improved IC preexercise (75±15 minutes postdose) compared with placebo or TIO following 3 weeks of treatment (LSM treatment difference 0.34 L vs placebo and 0.15 L vs TIO [both P<0.001]).115 After 6 weeks of treatment, TIO/OLO significantly improved IC preexercise (2 hours postdose) by 0.25, 0.10, and 0.10 L compared with placebo, OLO, and TIO, respectively (all P<0.0001).117 A post hoc analysis of pooled data from two 12-week studies showed that UMEC/VIL significantly improved the percentage change from baseline of trough IC and 3-hour postdose IC vs monocomponents or placebo (all P<0.001).118 A recent meta-analysis has also shown that the combination of a LAMA + LABA is superior at increasing IC at exercise isotime compared with LAMA or LABA alone.119 Furthermore, in a 12-week study UMEC/VIL significantly improved trough IC on day 84 compared with the ICS/LABA fluticasone propionate/SAL (treatment difference 0.10 L [P<0.001]).116 Therefore, LAMA/LABA FDCs may relieve lung hyperinflation more effectively than an ICS/LABA FDC.
Functional respiratory imaging
Although measures of lung function (FEV1 and IC) provide an overall indication of the extent of bronchodilation, they provide no information about the specific regions of the lungs in which bronchodilation occurs following administration of LAMAs and/or LABAs. Using multislice computed tomography (MSCT) in combination with airway segmentation and computational fluid dynamics enables researchers to generate functional data about airflow throughout the lobes of the lungs in terms of airway volume and airway resistance.120,121 In a study that examined the effect of an inhaled FDC of budesonide/FF (BUD/FF) vs placebo 4 hours postdose in patients with COPD, MSCT revealed changes in airway geometry that were not evident in the spirometry data.121 The results of this study demonstrated that MSCT is a sensitive tool to measure bronchodilator effects in the lungs.121
In a 2-week dosing, double-blind study in patients with moderate-to-severe COPD (NCT02643082), GFF MDI increased specific image-based airway volume at the end of the treatment period by 75% relative to placebo MDI (P<0.0001), whereas specific image-based airway resistance was reduced by 71% with GFF MDI compared with placebo MDI (P<0.0001).122 Significant improvements in FEV1, IC, residual volume, and functional residual capacity were also observed for GFF MDI relative to placebo MDI (all P≤0.0006).122 These results indicate that in addition to spirometry and body plethysmography end points, GFF MDI provides significant benefits on functional respiratory imaging-based airway volume and resistance throughout the whole lung in patients with COPD.
As muscarinic acetylcholine-receptor and β-adrenoceptor subtypes are differentially expressed throughout the airways,41 it would be of interest to examine whether (through their distinct mechanisms of action) LAMAs and LABAs provide similar structural and airflow changes across lung regions. In this regard, a study using functional respiratory imaging to investigate the effect of monocomponent cosuspension-delivery technology MDIs, GP MDI, and FF MDI on bronchodilation throughout the airways is ongoing.123
Patient stratification
Stratifying patients by the characteristics of their disease is a method by which physicians can ensure that patients receive the most appropriate treatments based on the clinical evidence available, resulting in the greatest potential benefit to the patient. GOLD currently recommends patients in group A (low symptoms, low risk) and group B (high symptoms, low risk) receive a single bronchodilator, unless their symptoms persist following treatment.1 However, little is known about the efficacy of LAMA/LABA FDCs in these specific patient subpopulations.
Post hoc analyses of pooled data from two pivotal Phase III studies (PINNACLE-1 and PINNACLE-2) examined lung-function response in GOLD group A and group B patients (based on the GOLD 2015 ABCD assessment, which included airflow limitation and exacerbation history to classify risk) who received GFF MDI, GP MDI, FF MDI, or placebo MDI for 24 weeks.124,125 GFF MDI increased the change from baseline in morning predose trough FEV1 and peak change in FEV1 within 2 hours postdose compared with monocomponent and placebo MDIs in both the A and B groups, with the treatment effect at least as large in group A patients as in group B.124,125 These results suggest that prospective analyses of LAMA/LABA FDCs in these patient populations are merited, to elucidate whether earlier intervention with dual-bronchodilator therapy may result in additional clinical benefit compared with the current recommendations.
The current GOLD ABCD assessment tool uses a baseline symptom threshold of a CAT score ≥10 or an mMRC grade ≥2 to classify a patient as having high symptom burden,1 although few studies of bronchodilator therapy have stratified measures of efficacy by baseline symptom burden, in order to determine which patient subgroups may benefit the most from a particular therapy.73 This may in part be due to randomized clinical trials in patients with COPD often setting a minimum baseline symptom burden as part of the entry criteria, eg, mMRC score ≥2.68,70–72 In contrast, the recruitment criteria for the GFF MDI PINNACLE studies did not specify a minimum symptom score, so the studies included patients with a broad-range COPD symptom burden, as assessed by CAT score.65,73 In the resultant patient population, 87.2% of patients had a baseline CAT score ≥10% and 57.1% had an mMRC grade ≥2.65 This provided the opportunity to examine the relationship between patient symptom scores at baseline and response to GFF MDI.73
In a post hoc analysis of pooled data from PINNACLE-1 and PINNACLE-2, Martinez et al stratified the patient population based on baseline CAT scores (CAT ≥10, CAT ≥15, and CAT ≥20) and examined lung function and PROs across these subgroups.73 The magnitude of lung-function benefits with GFF MDI at week 24 (morning predose trough FEV1 and peak FEV1) was independent of baseline symptom burden.73 However, for SGRQ total score, rescue medication use, and moderate or severe exacerbations, most treatment comparisons of GFF MDI vs placebo or monocomponent MDIs exhibited a trend of greater improvement as symptom scores increased, which was most noticeable in patients with baseline CAT scores ≥20.73
The relationship between COPD symptom burden and PROs was also investigated in a post hoc analysis of daily, daytime, and nighttime symptom-score data that were pooled from PINNACLE-1 and PINNACLE-2.126 Patients recorded daytime and nighttime symptoms (cough, shortness of breath, sputum volume, and rescue medication use) in an “eDiary” and responses for each of these clinical manifestations were allocated numeric scores, the sum of which provided the total symptom score.126 Improvements in total symptom scores for GFF MDI compared with FF MDI or placebo MDI increased numerically as baseline CAT score increased, with the largest improvements in the baseline CAT ≥20 subgroup.126 Therefore, although several limitations apply to these findings, due to the analyses being conducted post hoc, the results may indicate that symptomatic patients gain more clinical benefit from dual bronchodilators than those with lower symptom burden.73,126
Clinically important deterioration
It will be of great interest to determine whether bronchodilator therapies may provide benefits to patients in terms of the deterioration of their disease over time. Clinically important deterioration (CID) is a composite end point that provides an indication of the progression of COPD. The different criteria that have been used to define CID are shown in Table 3.127–131
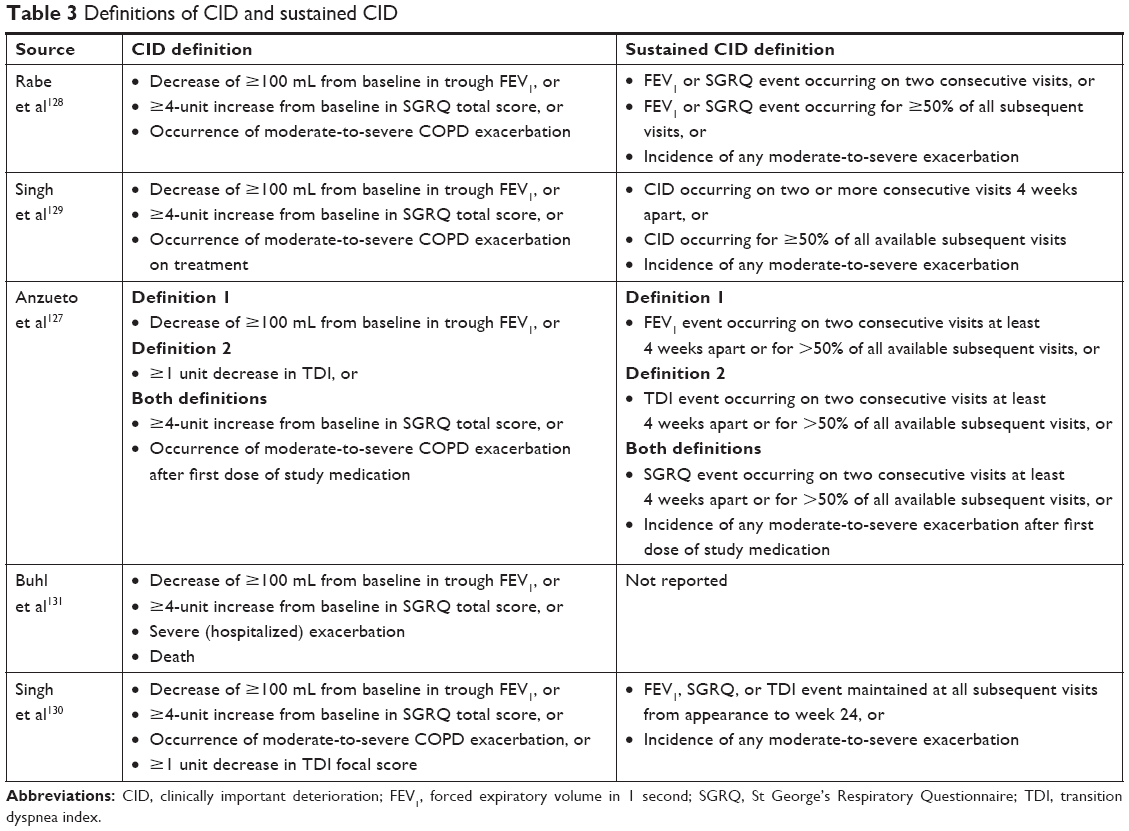 | Table 3 Definitions of CID and sustained CID |
In a post hoc analysis of pooled data from PINNACLE-1 and PINNACLE-2, GFF MDI significantly decreased the risk of patients experiencing a CID over 24 weeks compared with GP MDI, FF MDI, or placebo MDI (time-to-event HR [95% CI] 0.76 [0.68–0.85], 0.83 [0.74–0.93], and 0.56 [0.49–0.64], respectively; all P≤0.0011).128 This reduction in CID risk was in the same range reported by Singh et al for UMEC/VIL vs monocomponents (UMEC HR [95% CI] 0.80 [0.65–0.97], P<0.05; and VIL HR 0.67 [0.55–0.81], P<0.001) over 24 weeks.129 Based on a CID definition very similar to the definitions used by Rabe and Singh in these studies (Table 3), GP/IND also significantly reduced the risk of a CID over 26 weeks compared with the LAMA TIO (HR [95% CI] 0.72 [0.61–0.86]; P=0.0003).127 In GOLD group B (symptomatic COPD and low risk of exacerbations) patients with COPD, time to CID was significantly longer with TIO/OLO 5/5 μg than TIO monotherapy (HR [95% CI] 0.65 [0.52–0.81]; P<0.0001), although the definition of CID used in this study did not include moderate-exacerbation occurrences in their assessment of exacerbation risk.131
Using another slightly different approach to assessing CID, two studies included a change in TDI score (≥1 unit) in the definition of CID, as well as/instead of a ≥100 mL decrease in trough FEV1.127,130 In the first of these analyses, ACL/FF significantly reduced the risk of a CID over 24 weeks compared with Acl, FF, or placebo (HR 0.85, 0.82, and 0.55 respectively; all P<0.05).130 When Anzueto et al replaced the ≥100 mL decrease in trough FEV1 in the CID definition with the ≥1 unit change in TDI score (definition 2),127 a significant decrease in the risk of a CID was maintained for GP/IND vs TIO (HR [95% CI] 0.80 [0.64–0.99]; P=0.0359).127
In addition to assessing the risk of a CID occurring during the treatment period, these post hoc analyses of COPD progression also determined the risk that the CID experienced by a patient was “sustained”, eg, an FEV1 or SGRQ event observed on two consecutive visits or on ≥50% of subsequent visits or any occurrence of a moderate or severe COPD exacerbation128 (for other definitions of sustained CID, see Table 3). For almost all of these treatment comparisons, if sustained CID data were also reported, the pattern of risk reductions in patients experiencing a CID were maintained in the assessments of the risk of a sustained CID, ie, a significantly lower HR for LAMA/LABA FDC therapy versus comparator.127–130 Exceptions in which there was no significant difference in the risk of sustained CID were ACL/FF vs ACL,130 UMEC/VIL vs UMEC,129 and GP/IND vs TIO using CID definition 2.127
Overall, these post hoc analyses suggest that LAMA/LABA FDC therapies may slow the progression of COPD in terms of declining lung function and quality of life and reduce the risk of clinically significant events, such as exacerbations, in these patient populations over the time scales examined here. It will be important to determine if this effect of LAMA/LABA FDC therapies on disease progression is maintained over a longer time frame and in a real-world setting. For example, a recent meta-analysis by Calzetta et al suggested that the benefits of LAMA/LABA FDCs compared with monocomponent therapies in terms of lung function, dyspnea, and quality of life were retained at 3, 6, and 12 months of treatment.74 However, the relative magnitude of treatment difference between LAMA/LABA FDCs and monocomponents appeared to be greatest at 3 months and reduced by 6 and 12 months.74 It will also be interesting to establish whether early intervention with LAMA/LABA FDCs may improve disease progression, as a recent 24-month study in patients with mild or moderate COPD demonstrated that TIO monotherapy improved annual decline in FEV1 compared with placebo.132
Clinical decision-making
Many patients with COPD have not received a formal diagnosis,6–9 so it is necessary to raise awareness of the disease among physicians and devise methods that encourage people with COPD symptoms or a history of exposure to risk factors to seek medical advice. Encouraging early intervention is particularly important, since it has been hypothesized that individuals with typical COPD symptoms, but who do not yet fulfill the spirometric definition of COPD, may still benefit from treatment with bronchodilators.133,134 Given the new focus of ensuring appropriate use of ICSs and initiating LAMA/LABA FDCs in COPD, correct diagnosis is also important to ensure that cases of adult-onset asthma are distinguished from COPD in patients presenting with airflow limitation. Overall, timely diagnosis of patients with COPD will enable the early initiation of bronchodilator therapy, which has been shown to improve patients’ long-term health and quality of life.135
Combining bronchodilator therapy with pulmonary rehabilitation programs may provide another approach by which optimal bronchodilation can lead to improved PROs. For example, the addition of TIO to pulmonary rehabilitation leads to improvements in dyspnea and quality of life for patients with COPD compared with those who receive pulmonary rehabilitation plus placebo.136,137 Additional research is required to determine whether LAMA/LABA FDC therapies in combination with pulmonary rehabilitation can provide additional benefits vs a single bronchodilator plus pulmonary rehabilitation.
Recent studies have suggested that a LAMA/LABA FDC may provide further clinical benefits compared to ICS/LABA FDCs.46,138 However, although LAMA + LABA dual therapy consistently improved the change from baseline in trough FEV1 compared with LABA + ICS, results obtained for exacerbation and health-related quality of life end points were not consistent between the different studies of LAMA + LABA and ICS + LABA combinations.138,139 Therefore, more prospective studies are required to determine the particular patient subgroups that may benefit from ICS-containing therapies, eg, patients who report frequent exacerbations or those with asthma–COPD overlap syndrome, and to identify patient subgroups in which ICS withdrawal may be recommended.54 The role of eosinophils in COPD and whether patients with eosinophil counts above specific cutoffs may benefit from ICS therapy is also yet to be extensively investigated.
Conclusion
It is important that clinical trials are designed so that they can inform clinical decisions. Clinical trials in which patients are stratified by disease phenotype or endotype will help to delineate optimal treatment for patients in particular pathophysiological subgroups, although it must be highlighted that clinical phenotypes do not necessarily describe the underlying pathophysiology, and consequently may not predict response to potential, ideally curative, therapies.
COPD is a therapy area in which the incidence of disease is expected to continue to rise, and so it is crucial that treatments are optimized to meet the growing health and economic burden. While lung-function response to bronchodilators continues to be characterized, other studies are examining how bronchodilation ultimately translates into benefits in different patient subpopulations to ensure that optimal personalized therapeutic management of COPD can be realized. In particular, we must consolidate the emerging evidence and clarify which characteristics of patients with COPD can assist in selecting the most appropriate therapy.
Acknowledgments
The PINNACLE studies were supported by Pearl, a member of the AstraZeneca Group. Medical writing support, under the direction of the authors, was provided by Thomas Owens, PhD of CMC CONNECT, a division of Complete Medical Communications, Manchester, UK, funded by AstraZeneca, Cambridge, UK in accordance with Good Publication Practice (GPP3) guidelines. Bevespi Aerosphere is a trademark of the AstraZeneca group of companies. This review was supported by AstraZeneca. The sponsor did not place any restriction on authors about the statements made in the final article.
Author contributions
All authors contributed toward interpreting, critically revising, and providing final approval of the manuscript, and agree to be accountable for all aspects of the work.
Disclosure
ADD has received research, consulting, and lecturing fees from Almirall, Altana, AstraZeneca, Boehringer Ingelheim (Canada), Forest Laboratories, GlaxoSmithKline, KOS Pharmaceuticals, Merck Canada, Methapharm, Novartis Canada/USA, Ono Pharmaceutical, Pfizer Canada, Schering-Plow, Sepracor, and Skyepharma. MC has participated as a speaker and/or advisor in scientific meetings and courses under the sponsorship of Almirall, AstraZeneca, Biofutura, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Lallemand, Menarini Group, Mundipharma, Novartis, Pfizer, Verona Pharma, and Zambon, and is or has been a consultant to ABC Farmaceutici, Chiesi Farmaceutici, Lallemand, Novartis, Recipharm, Teva, Verona Pharma, and Zambon. His institution has received grants on his behalf from Almirall, Boehringer Ingelheim, Novartis, Verona Pharma, and Zambon. NAH has participated in scientific advisory boards and consulted for AstraZeneca, Genentech, GlaxoSmithKline, Mylan, Novartis, Roche, Sunovion, and Sanofi. His institution has received grants on his behalf from AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, GlaxoSmithKline, Mylan, and Sunovion. RB reports personal fees from AstraZeneca, Chiesi, GlaxoSmithKline, and Takeda, and grants and personal fees from Boehringer Ingelheim, Novartis, and Roche. MRMY has received research funding, consulting fees, and speaker honoraria from Almirall, AstraZeneca, Boehringer Ingelheim, Forest Laboratories, GlaxoSmithKline, Novartis, Merck, Ono Pharmaceuticals, and Pfizer. The authors report no other conflicts of interest in this work.
References
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD. COPD [updated 2018]. Available from: http://www.goldcopd.org. Accessed February 18, 2018. | ||
World Health Organization. Chronic obstructive pulmonary disease (COPD). Updated 2017. Available from: http://www.who.int/mediacentre/factsheets/fs315/en. Accessed February 18, 2018. | ||
Jones PW, Donohue JF, Nedelman J, Pascoe S, Pinault G, Lassen C. Correlating changes in lung function with patient outcomes in chronic obstructive pulmonary disease: a pooled analysis. Respir Res. 2011;12:161. | ||
Landis SH, Muellerova H, Mannino DM, et al. Continuing to Confront COPD International Patient Survey: methods, COPD prevalence, and disease burden in 2012–2013. Int J Chron Obstruct Pulmon Dis. 2014;9:597–611. | ||
Rennard S, Decramer M, Calverley PM, et al. Impact of COPD in North America and Europe in 2000: subjects’ perspective of Confronting COPD International Survey. Eur Respir J. 2002;20(4):799–805. | ||
Fukuchi Y, Nishimura M, Ichinose M, et al. COPD in Japan: the Nippon COPD Epidemiology study. Respirology. 2004;9(4):458–465. | ||
Miravitlles M, Soriano JB, García-Río F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–868. | ||
Nascimento OA, Camelier A, Rosa FW, et al. Chronic obstructive pulmonary disease is underdiagnosed and undertreated in São Paulo (Brazil): results of the PLATINO study. Braz J Med Biol Res. 2007;40(7):887–895. | ||
Shahab L, Jarvis MJ, Britton J, West R. Prevalence, diagnosis and relation to tobacco dependence of chronic obstructive pulmonary disease in a nationally representative population sample. Thorax. 2006;61(12):1043–1047. | ||
Barnes N, Calverley PM, Kaplan A, Rabe KF. Chronic obstructive pulmonary disease and exacerbations: patient insights from the global Hidden Depths of COPD survey. BMC Pulm Med. 2013;13:54. | ||
Miravitlles M, Worth H, Cataluña JJ, et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study. Respir Res. 2014;15:122. | ||
Price D, Small M, Milligan G, Higgins V, Gil EG, Estruch J. Impact of night-time symptoms in COPD: a real-world study in five European countries. Int J Chron Obstruct Pulmon Dis. 2013;8:595–603. | ||
Uzaslan E, Mahboub B, Beji M, et al. The burden of chronic obstructive pulmonary disease in the Middle East and North Africa: results of the BREATHE study. Respir Med. 2012;106 Suppl 2:S45–S59. | ||
Jones PW, Brusselle G, dal Negro RW, et al. Patient-centred assessment of COPD in primary care: experience from a cross-sectional study of health-related quality of life in Europe. Prim Care Respir J. 2012;21(3):329–336. | ||
Tsiligianni I, Kocks J, Tzanakis N, Siafakas N, van der Molen T. Factors that influence disease-specific quality of life or health status in patients with COPD: a systematic review and meta-analysis of Pearson correlations. Prim Care Respir J. 2011;20(3):257–268. | ||
Ding B, Small M, Holmgren U. A cross-sectional survey of current treatment and symptom burden of patients with COPD consulting for routine care according to GOLD 2014 classifications. Int J Chron Obstruct Pulmon Dis. 2017;12:1527–1537. | ||
AstraZeneca. Tudorza Pressair [prescribing information]. 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/202450s006lbl.pdf. Accessed February 18, 2018. | ||
AstraZeneca. Eklira Genuair [summary of product characteristics] 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002211/WC500132661.pdf. Accessed December 11, 2017. | ||
Novartis. Seebri Neohaler [prescribing information]. 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/207923s002lbl.pdf. Accessed February 18, 2018. | ||
Novartis Europharm. Seebri Breezhaler [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002430/WC500133769.pdf. Accessed December 11, 2017. | ||
Boehringer Ingelheim International GmbH. Spiriva Respimat [summary of product characteristics]. 2017. Available from: https://www.spiriva.com/global/sites/default/files/Spiriva%20Respimat%20SmPC%2013%20Jan%202017.pdf. Accessed February 18, 2018. | ||
Boehringer Ingelheim. Spiriva Respimat [prescribing information]. 2017. Available from: http://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Spiriva%20Respimat/spirivarespimat.pdf. Accessed February 18, 2018. | ||
GlaxoSmithKline. Incruse Ellipta [prescribing information]. 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/205382s008lbl.pdf. Accessed February 18, 2018. | ||
Glaxo Group. Incruse Ellipta [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002809/WC500167430.pdf. Accessed December 11, 2017. | ||
Schering. Foradil Aerolizer [prescribing information]. 2012. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020831s028lbl.pdf. Accessed February 18, 2018. | ||
Novartis Pharmaceuticals. Foradil [summary of product characteristics]. 2016. Available from: https://www.medicines.org.uk/emc/medicine/1286. Accessed February 5, 2018. | ||
Sunovion Pharmaceuticals. Arcapta Neohaler [prescribing information]. 2017. Available from: https://www.arcapta.com/Arcapta-Prescribing-Information.pdf. Accessed January 19, 2018. | ||
Novartis Europharm. Onbrez Breezhaler [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001114/WC500053732.pdf. Accessed December 11, 2017. | ||
Boehringer Ingelheim. Striverdi Respimat [summary of product characteristics]. 2016. Available from: https://www.medicines.org.uk/emc/medicine/28992. Accessed February 18, 2018. | ||
Boehringer Ingelheim. Striverdi Respimat [prescribing information]. 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/203108s003lbl.pdf. Accessed February 18, 2018. | ||
Glaxo Wellcome. Serevent Accuhaler [summary of product characteristics]. 2014. Available from: https://www.medicines.org.uk/emc/medicine/91. Accessed February 18, 2018. | ||
Laube BL, Janssens HM, de Jongh FH, et al. What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37(6):1308–1417. | ||
Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. | ||
D’Urzo A, Kardos P, Wiseman R. Practical considerations when prescribing a long-acting muscarinic antagonist for patients with COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:1089–1104. | ||
Ismaila AS, Huisman E, Punekar Y, Karabis A. Comparative efficacy of long-acting muscarinic antagonist monotherapies in COPD: a systematic review and network meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:2495–2517. | ||
Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. Cochrane Database Syst Rev. 2014;3:CD010844. | ||
Decramer ML, Chapman KR, Dahl R, et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med. 2013;1(7):524–533. | ||
Cazzola M, Molimard M. The scientific rationale for combining long-acting β2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–267. | ||
Cazzola M, Page CP, Calzetta L, Matera MG. Pharmacology and therapeutics of bronchodilators. Pharmacol Rev. 2012;64(3):450–504. | ||
Calzetta L, Matera MG, Cazzola M. Pharmacological interaction between LABAs and LAMAs in the airways: optimizing synergy. Eur J Pharmacol. 2015;761:168–173. | ||
Ikeda T, Anisuzzaman AS, Yoshiki H, et al. Regional quantification of muscarinic acetylcholine receptors and β-adrenoceptors in human airways. Br J Pharmacol. 2012;166(6):1804–1814. | ||
Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. | ||
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD. [updated 2011]. Available from: http://www.goldcopd.org. | ||
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD. [updated 2016]. Available from: http://www.goldcopd.org. Accessed October 30, 2016. | ||
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD. [updated 2017]. Available from: http://www.goldcopd.org. Accessed November 1, 2017. | ||
Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol–glycopyrronium versus salmeterol–fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. | ||
Roche N, Chapman KR, Vogelmeier CF, et al. Blood eosinophils and response to maintenance chronic obstructive pulmonary disease treatment: data from the FLAME trial. Am J Respir Crit Care Med. 2017;195(9):1189–1197. | ||
Watz H, Tetzlaff K, Wouters EF, et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: a post-hoc analysis of the WISDOM trial. Lancet Respir Med. 2016;4(5):390–398. | ||
Calverley PM, Tetzlaff K, Vogelmeier C, et al. Eosinophilia, frequent exacerbations, and steroid response in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(9):1219–1221. | ||
Pearl Therapeutics. Study to assess the efficacy and safety of PT010 relative to PT003 and PT009 in subjects with moderate to very severe COPD (ETHOS). Available from: https://clinicaltrials.gov/ct2/show/NCT02465567. NLM identifier: NCT02465567. Accessed February 18, 2018. | ||
Pascoe SJ, Lipson DA, Locantore N, et al. A phase III randomised controlled trial of single-dose triple therapy in COPD: the IMPACT protocol. Eur Respir J. 2016;48(2):320–330. | ||
Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. | ||
Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. | ||
Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. | ||
Frith P, Ashmawi S, Krishnamurthy S, et al. Assessing direct switch to indacaterol/glycopyrronium from salmeterol/fluticasone in moderate to severe symptomatic COPD patients: the FLASH study. Respirology. 2017;22 Suppl 3:AOL011. | ||
Yu AP, Guérin A, Ponce de Leon D, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14(4):486–496. | ||
AstraZeneca. Duaklir Genuair [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003745/WC500178413.pdf. Accessed December 11, 2017. | ||
AstraZeneca Pharmaceuticals. Bevespi Aerosphere [prescribing information]. 2017. Available from: http://www.azpicentral.com/bevespi/bevespi_pi.pdf. Accessed February 5, 2018. | ||
Novartis Europharm. Ultibro Breezhaler [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002679/WC500151255.pdf. Accessed December 11, 2017. | ||
Novartis Pharmaceuticals. Utibron Neohaler [prescribing information]. 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/207930s002lbl.pdf. Accessed February 18, 2018. | ||
Boehringer Ingelheim. Spiolto Respimat [summary of product characteristics]. 2017. Available from: https://www.medicines.org.uk/emc/medicine/30495. Accessed February 18, 2018. | ||
Glaxo Group. Anoro Ellipta [summary of product characteristics]. 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002751/WC500168424.pdf. Accessed December 11, 2017. | ||
D’Urzo AD, Rennard SI, Kerwin EM, et al. Efficacy and safety of fixed-dose combinations of aclidinium bromide/formoterol fumarate: the 24-week, randomized, placebo-controlled AUGMENT COPD study. Respir Res. 2014;15:123. | ||
Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14:178. | ||
Martinez FJ, Rabe KF, Ferguson GT, et al. Efficacy and safety of glycopyrrolate/formoterol metered dose inhaler formulated using co-suspension delivery technology in patients with COPD. Chest. 2017;151(2):340–357. | ||
Hanania NA, Tashkin DP, Kerwin EM, et al. Long-term safety and efficacy of glycopyrrolate/formoterol metered dose inhaler using novel co-suspension delivery technology in patients with chronic obstructive pulmonary disease. Respir Med. 2017;126:105–115. | ||
Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. | ||
Mahler DA, Kerwin E, Ayers T, et al. FLIGHT1 and FLIGHT2: efficacy and safety of QVA149 (indacaterol/glycopyrrolate) versus its monocomponents and placebo in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(9):1068–1079. | ||
Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. | ||
Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respir Med. 2013;107(10):1538–1546. | ||
Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2(6):472–486. | ||
Celli B, Crater G, Kilbride S, et al. Once-daily umeclidinium/vilanterol 125/25 μg therapy in COPD: a randomized, controlled study. Chest. 2014;145(5):981–991. | ||
Martinez FJ, Fabbri LM, Ferguson GT, et al. Baseline symptom score impact on benefits of glycopyrrolate/formoterol metered dose inhaler in COPD. Chest. 2017;152(6):1169–1178. | ||
Calzetta L, Rogliani P, Ora J, Puxeddu E, Cazzola M, Matera MG. LABA/LAMA combination in COPD: a meta-analysis on the duration of treatment. Eur Respir Rev. 2017;26(143):160043. | ||
Oba Y, Sarva ST, Dias S. Efficacy and safety of long-acting β-agonist/long-acting muscarinic antagonist combinations in COPD: a network meta-analysis. Thorax. 2016;71(1):15–25. | ||
Feldman GJ, Sousa AR, Lipson DA, et al. Comparative efficacy of once-daily umeclidinium/vilanterol and tiotropium/olodaterol therapy in symptomatic chronic obstructive pulmonary disease: a randomized study. Adv Ther. 2017;34(11):2518–2533. | ||
Kerwin E, Ferguson GT, Sanjar S, et al. Dual bronchodilation with indacaterol maleate/glycopyrronium bromide compared with umeclidinium bromide/vilanterol in patients with moderate-to-severe COPD: results from two randomized, controlled, cross-over studies. Lung. 2017;195(6):739–747. | ||
AstraZeneca. Efficacy and safety of glycopyrronium/formoterol fumarate fixed-dose combination relative to umeclidinium/vilanterol fixed-dose combination over 24 weeks in patients with moderate to very severe chronic obstructive pulmonary disease (AERISTO). Available from: https://clinicaltrials.gov/ct2/show/NCT03162055. NLM identifier: NCT03162055. Accessed January 16, 2018. | ||
Bonini M, Usmani OS. The importance of inhaler devices in the treatment of COPD. COPD Res Pract. 2015;1:9. | ||
Braido F, Chrystyn H, Baiardini I, et al. “Trying, but failing”: the role of inhaler technique and mode of delivery in respiratory medication adherence. J Allergy Clin Immunol. 2016;4(5):823–832. | ||
Rabe KF. GFF MDI for the improvement of lung function in COPD: a look at the PINNACLE-1 and PINNACLE-2 data and beyond. Expert Rev Clin Pharmacol. 2017;10(7):685–698. | ||
Mahler DA, Waterman LA, Gifford AH. Prevalence and COPD phenotype for a suboptimal peak inspiratory flow rate against the simulated resistance of the Diskus dry powder inhaler. J Aerosol Med Pulm Drug Deliv. 2013;26(3):174–179. | ||
Prime D, de Backer W, Hamilton M, et al. Effect of disease severity in asthma and chronic obstructive pulmonary disease on inhaler-specific inhalation profiles through the Ellipta dry powder inhaler. J Aerosol Med Pulm Drug Deliv. 2015;28(6):486–497. | ||
Ferguson GT, Hickey AJ, Dwivedi S. Co-suspension delivery technology in pressurized metered-dose inhalers for multi-drug dosing in the treatment of respiratory diseases. Respir Med. 2018;134:16–23. | ||
Vehring R, Lechuga-Ballesteros D, Joshi V, Noga B, Dwivedi SK. Cosuspensions of microcrystals and engineered microparticles for uniform and efficient delivery of respiratory therapeutics from pressurized metered dose inhalers. Langmuir. 2012;28(42):15015–15023. | ||
Joshi V, Lechuga-Ballesteros D, Flynn B, et al. Development of mono, dual, and triple combination pMDIs without co-formulation effect. Resp Drug Deliv Eur. 2011;2:383–386. | ||
Lechuga-Ballesteros D, Noga B, Vehring R, Cummings RH, Dwivedi SK. Novel cosuspension metered-dose inhalers for the combination therapy of chronic obstructive pulmonary disease and asthma. Future Med Chem. 2011;3(13):1703–1718. | ||
Doty A, Schroeder J, Vang K, et al. Drug delivery from an innovative LAMA/LABA co-suspension delivery technology fixed-dose combination MDI: evidence of consistency, robustness, and reliability. AAPS PharmSciTech. 2018;19(2):837–844. | ||
Fabbri LM, Kerwin EM, Spangenthal S, et al. Dose-response to inhaled glycopyrrolate delivered with a novel co-suspension delivery technology metered dose inhaler (MDI) in patients with moderate-to-severe COPD. Respir Res. 2016;17:109. | ||
Quinn D, Seale JP, Reisner C, et al. A randomized study of formoterol fumarate in a porous particle metered-dose inhaler in patients with moderate-to-severe COPD. Respir Med. 2014;108(9):1327–1335. | ||
Reisner C, Orevillo C, Fernandez C, et al. Pooled analyses of five phase 2B studies support dose selection of glycopyrrolate-formoterol (GFF) MDI (PT003) 18/9.6 μg for phase III development. Eur Respir J. 2013;42 Suppl 57:P4153. | ||
Reisner C, Fernandez C, St Rose E, et al. Characterization of the dose response of Pearl Therapeutics’ LAMA MDI (GP MDI, PT001) from 36 micrograms to 600 nanograms BID: results from an integrated analysis of phase IIB studies in patients with COPD. Am J Respir Crit Care Med. 2013;187:A4274. | ||
Rennard S, Fogarty C, Reisner C, et al. Randomized study of the safety, pharmacokinetics, and bronchodilatory efficacy of a proprietary glycopyrronium metered-dose inhaler in study patients with chronic obstructive pulmonary disease. BMC Pulm Med. 2014;14:118. | ||
Sethi S, Fogarty C, Hanania NA, et al. Efficacy of formoterol fumarate delivered by metered dose inhaler using co-suspension delivery technology versus Foradil Aerolizer in moderate-to-severe COPD: a randomized, dose-ranging study. Chronic Obstr Pulm Dis. 2017;4(1):21–33. | ||
St Rose E, Strom S, Fischer T, et al. Pharmacokinetic (PK) bioequivalence and comparable efficacy/safety were demonstrated with Pearl Therapeutics’ formoterol fumarate MDI (FF MDI, PT005) compared to Foradil Aerolizer in a randomized, double-blind, placebo-controlled phase 2B study in patients with moderate to very severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185:A2927. | ||
Tashkin DP, Martinez FJ, Rodriguez-Roisin R, et al. A multicenter, randomized, double-blind dose-ranging study of glycopyrrolate/formoterol fumarate fixed-dose combination metered dose inhaler compared to the monocomponents and open-label tiotropium dry powder inhaler in patients with moderate-to-severe COPD. Respir Med. 2016;120:16–24. | ||
Reisner C, Fabbri LM, Kerwin EM, et al. A randomized, seven-day study to assess the efficacy and safety of a glycopyrrolate/formoterol fumarate fixed-dose combination metered dose inhaler using novel co-suspension delivery technology in patients with moderate-to-very severe chronic obstructive pulmonary disease. Respir Res. 2017;18(1):8. | ||
Pearl Therapeutics. Study to evaluate single inhaled doses of PT001, PT003, PT005 and PT001 plus PT005 in healthy subjects. Available from: https://clinicaltrials.gov/ct2/show/NCT00893971. NLM identifier: NCT00893971. Accessed January 5, 2018. | ||
Baraldo S, Turato G, Saetta M. Pathophysiology of the small airways in chronic obstructive pulmonary disease. Respiration. 2012;84(2):89–97. | ||
Usmani OS, Barnes PJ. Assessing and treating small airways disease in asthma and chronic obstructive pulmonary disease. Ann Med. 2012;44(2):146–156. | ||
Biddiscombe MF, Meah SN, Underwood SR, Usmani OS. Comparing lung regions of interest in gamma scintigraphy for assessing inhaled therapeutic aerosol deposition. J Aerosol Med Pulm Drug Deliv. 2011;24(3):165–173. | ||
Chrystyn H. Methods to determine lung distribution of inhaled drugs: could gamma scintigraphy be the gold standard? Br J Clin Pharmacol. 2000;49(6):525–528. | ||
Darquenne C, Fleming JS, Katz I, et al. Bridging the gap between science and clinical efficacy: physiology, imaging, and modeling of aerosols in the lung. J Aerosol Med Pulm Drug Deliv. 2016;29(2):107–126. | ||
Newman S, Bennett WD, Biddiscombe M, et al. Standardization of techniques for using planar (2D) imaging for aerosol deposition assessment of orally inhaled products. J Aerosol Med Pulm Drug Deliv. 2012;25 Suppl 1:S10–S28. | ||
Taylor G, Warren S, Dwivedi S, et al. Gamma scintigraphic pulmonary deposition study of glycopyrronium/formoterol metered dose inhaler formulated using co-suspension delivery technology. Eur J Pharm Sci. 2018;111:450–457. | ||
de Backer W, Devolder A, Poli G, et al. Lung deposition of BDP/formoterol HFA pMDI in healthy volunteers, asthmatic, and COPD patients. J Aerosol Med Pulm Drug Deliv. 2010;23(3):137–148. | ||
O’Donnell DE. Impacting patient-centred outcomes in COPD: breathlessness and exercise tolerance. Eur Respir Rev. 2006;15(99):37–41. | ||
Ferguson GT. Why does the lung hyperinflate? Proc Am Thorac Soc. 2006;3(2):176–179. | ||
Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22(1):101–111. | ||
Diaz O, Villafranca C, Ghezzo H, et al. Role of inspiratory capacity on exercise tolerance in COPD patients with and without tidal expiratory flow limitation at rest. Eur Respir J. 2000;16(2):269–275. | ||
Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-Total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591–597. | ||
Celli BR. Predictors of mortality in COPD. Respir Med. 2010;104(6):773–779. | ||
Beeh KM, Burgel PR, Franssen FM, et al. How do dual long-acting bronchodilators prevent exacerbations of chronic obstructive pulmonary disease? Am J Respir Crit Care Med. 2017;196(2):139–149. | ||
Reisner C, Gottschlich G, Fakih F, et al. 24-h bronchodilation and inspiratory capacity improvements with glycopyrrolate/formoterol fumarate via co-suspension delivery technology in COPD. Respir Res. 2017;18(1):157. | ||
Beeh KM, Korn S, Beier J, et al. Effect of QVA149 on lung volumes and exercise tolerance in COPD patients: the BRIGHT study. Respir Med. 2014;108(4):584–592. | ||
Donohue JF, Worsley S, Zhu CQ, Hardaker L, Church A. Improvements in lung function with umeclidinium/vilanterol versus fluticasone propionate/salmeterol in patients with moderate-to-severe COPD and infrequent exacerbations. Respir Med. 2015;109(7):870–881. | ||
O’Donnell DE, Casaburi R, Frith P, et al. Effects of combined tiotropium/olodaterol on inspiratory capacity and exercise endurance in COPD. Eur Respir J. 2017;49(4):1601348. | ||
Singh S, Maltais F, Tombs L, Church A, Iqbal A, Riley JH. Effect of umeclidinium/vilanterol (UMEC/VI) on inspiratory capacity/total lung capacity ratio in hyperinflated COPD patients. Poster PA1493 presented at: European Respiratory Society International Congress; September 26–30, 2015; Amsterdam. | ||
Calzetta L, Ora J, Cavalli F, Rogliani P, O’Donnell DE, Cazzola M. Impact of LABA/LAMA combination on exercise endurance and lung hyperinflation in COPD: a pair-wise and network meta-analysis. Respir Med. 2017;129:189–198. | ||
de Backer JW, Vos WG, Devolder A, et al. Computational fluid dynamics can detect changes in airway resistance in asthmatics after acute bronchodilation. J Biomech. 2008;41(1):106–113. | ||
de Backer LA, Vos W, de Backer J, van Holsbeke C, Vinchurkar S, de Backer W. The acute effect of budesonide/formoterol in COPD: a multi-slice computed tomography and lung function study. Eur Respir J. 2012;40(2):298–305. | ||
de Backer W, de Backer J, Vos W, et al. Functional respiratory imaging (FRI) and lung function assessment of glycopyrronium/formoterol fumarate dihydrate fixed-dose combination delivered using novel co-suspension delivery technology (GFF MDI) in COPD. Eur Respir J. 2017;50 Suppl 61:OA4404. | ||
Pearl Therapeutics. A study to assess the effects of PT001 and PT005 MDI on specific image based parameters in subjects with moderate to severe COPD. Available from: https://clinicaltrials.gov/ct2/show/NCT02937584. NLM identifier: NCT02937584. Accessed February 23, 2018. | ||
Martinez FJ, Rabe KF, Rodriguez-Roisin R, et al. Beneficial effect of the novel LAMA/LABA co-suspension technology of glycopyrrolate/formoterol fixed-dose combination delivered by MDI in GOLD A and B COPD patients: pooled analyses from PINNACLE-1 and -2. Am J Respir Crit Care Med. 2016;193:A6785. | ||
Fabbri LM, Martinez F, Rabe KF, et al. Beneficial effect of the LAMA/LABA glycopyrronium (GP)/formoterol (FF) fixed-dose combination, delivered using a novel MDI co-suspension technology (GFF MDI), in COPD GOLD group A and B patients. Eur Respir J. 2016;48 Suppl 60:PA310. | ||
Martinez FJ, Fabbri LM, Ferguson GT, et al. Effect of glycopyrrolate/formoterol fumarate fixed-dose combination metered dose inhaler (GFF MDI) delivered by novel co-suspension delivery technology on daily symptoms in patients with COPD. Am J Respir Crit Care Med. 2017;195:A5469. | ||
Anzueto A, Vogelmeier C, Kostikas K, et al. The effect of indacaterol/glycopyrronium versus tiotropium or salmeterol/fluticasone on the prevention of clinically important deterioration in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1325–1337. | ||
Rabe KF, Martinez FJ, Rodriguez-Roisin R, et al. LAMA/LABA glycopyrrolate/formoterol fixed-dose combination, delivered using a novel MDI co-suspension delivery technology reduces risk of clinically important deteriorations in COPD versus placebo and monocomponent MDIs. Am J Respir Crit Care Med. 2017;195:A3594. | ||
Singh D, Maleki-Yazdi MR, Tombs L, Iqbal A, Fahy WA, Naya I. Prevention of clinically important deteriorations in COPD with umeclidinium/vilanterol. Int J Chron Obstruct Pulmon Dis. 2016;11:1413–1424. | ||
Singh D, D’Urzo AD, Chuecos F, Muñoz A, Garcia Gil E. Reduction in clinically important deterioration in chronic obstructive pulmonary disease with aclidinium/formoterol. Respir Res. 2017;18(1):106. | ||
Buhl R, Mcgarvey L, Korn S, et al. Benefits of tiotropium + olodaterol over tiotropium at delaying clinically significant events in patients with COPD classified as GOLD B. Am J Respir Crit Care Med. 2016;193:A6779. | ||
Zhou Y, Zhong NS, Li X, et al. Tiotropium in early-stage chronic obstructive pulmonary disease. N Engl J Med. 2017;377(10):923–935. | ||
Regan EA, Lynch DA, Curran-Everett D, et al. Clinical and radiologic disease in smokers with normal spirometry. JAMA Intern Med. 2015;175(9):1539–1549. | ||
Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med. 2016;374(19):1811–1821. | ||
Jones R, Østrem A. Optimising pharmacological maintenance treatment for COPD in primary care. Prim Care Respir J. 2011;20(1):33–45. | ||
Ambrosino N, Foglio K, Balzano G, et al. Tiotropium and exercise training in COPD patients: effects on dyspnea and exercise tolerance. Int J Chron Obstruct Pulmon Dis. 2008;3(4):771–780. | ||
Casaburi R, Kukafka D, Cooper CB, Witek TJ, Kesten S. Improvement in exercise tolerance with the combination of tiotropium and pulmonary rehabilitation in patients with COPD. Chest. 2005;127(3):809–817. | ||
Horita N, Goto A, Shibata Y, et al. Long-acting muscarinic antagonist (LAMA) plus long-acting beta-agonist (LABA) versus LABA plus inhaled corticosteroid (ICS) for stable chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2017;2:CD012066. | ||
Cazzola M, Rogliani P. In stable COPD, long-acting muscarinic antagonist plus long-acting beta-agonists resulted in less exacerbations, pneumonia and larger improvement in FEV1 than long-acting beta-agonists plus inhaled corticosteroids. Evid Based Med. 2017;22(5):183–184. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.