")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
New alternative in the treatment of rheumatoid arthritis: clinical utility of baricitinib
Authors Kawalec P, Śladowska K , Malinowska-Lipień I , Brzostek T , Kózka M
Received 27 October 2018
Accepted for publication 22 December 2018
Published 13 February 2019 Volume 2019:15 Pages 275—284
DOI https://doi.org/10.2147/TCRM.S192440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Paweł Kawalec,1 Katarzyna Śladowska,2 Iwona Malinowska-Lipień,3 Tomasz Brzostek,3 Maria Kózka4
1Drug Management Department, Institute of Public Health, Faculty of Health Sciences, Jagiellonian University Medical College, Kraków, Poland; 2Department of Experimental Hematology, Institute of Zoology and Biomedical Research, Faculty of Biology and Earth Sciences, Jagiellonian University, Kraków, Poland; 3Department of Internal and Community Nursing, Institute of Nursing and Midwifery, Faculty of Health Sciences, Jagiellonian University Medical College, Kraków, Poland; 4Department of Clinical Nursing, Institute of Nursing and Midwifery, Faculty of Health Sciences, Jagiellonian University Medical College, Kraków, Poland
Abstract: Baricitinib is an innovative small-molecule drug that reversibly inhibits continuous activation of JAK/STAT pathway, thus reducing joint inflammation. The drug was approved for use as monotherapy or in combination with methotrexate (MTX) in the treatment of adults with moderately to severely active rheumatoid arthritis (RA). The aim of this paper was to review the studies on pharmacology, mode of action, pharmacokinetics, efficacy, and safety of baricitinib in patients with RA. Baricitinib provides an innovative approach to modulating the immune and inflammatory response in patients with RA, which is especially important in individuals who do not respond to disease-modifying antirheumatic drugs or standard biologic drugs (tumor necrosis factor inhibitors) or who lose response over time. Baricitinib therapy reduces symptoms of RA and improves the quality of life. Moreover, it has shown high efficacy and an acceptable safety profile in Phase III randomized controlled trials (RCTs) and become another JAK inhibitor approved for RA treatment, providing a useful alternative option. RCTs have revealed a significant benefit of baricitinib over placebo, MTX, and adalimumab in terms of standard efficacy outcomes, especially the American College of Rheumatology ACR20, ACR50, and ACR70 response rates. Additionally, a clinically meaningful improvement in patient-reported outcomes, including the quality of life, compared with placebo has been reported. The safety profile seems acceptable, although some rare but potentially severe adverse events have been observed, such as serious infections, opportunistic infections (eg, herpes zoster), malignancies, and cardiac or hepatic disorders. Baricitinib administered at an approved dose of 2 or 4 mg once daily offers a novel and promising alternative to parenterally administered biologic drugs used in RA treatment.
Keywords: JAK inhibitor, baricitinib, efficacy, rheumatoid arthritis, safety
Introduction
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease characterized by persistent joint inflammation leading to loss of joint function as well as cartilage and bone damage. Chronic, progressive course of the disease results in disability, reduced quality of life, as well as higher comorbidity and mortality rates.1,2 With an estimated prevalence of 0.3%–1%, RA is the most common inflammatory joint disease in adults.3,4
The aim of RA treatment is to achieve remission or reduction of disease activity by preventing inflammation, progression of joint damage, and disability.3,5 RA treatment has been significantly improved over the past several decades, with numerous effective targeted drugs currently available.5 The treatment options include NSAIDs, glucocorticoids, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs; such as methotrexate [MTX], sulfasalazine, and leflunomide), biologic DMARDs (bDMARDs; including tumor necrosis factor [TNF] inhibitors such as adalimumab, infliximab, certolizumab pegol, golimumab, and etanercept, as well as non-TNF drugs such as abatacept, rituximab, and tocilizumab), biosimilar DMARDs, and targeted synthetic DMARDs (tofacitinib, baricitinib).3–5
Therapy with DMARDs should be started immediately after the diagnosis of RA and should be adjusted to disease activity and individual prognostic factors.3,5 According to the latest clinical guidelines,3–5 MTX monotherapy is recommended as a first-line treatment, with concomitant short-term low-dose glucocorticoid therapy where indicated. In patients who fail this treatment due to an inadequate response to or intolerance of MTX, another synthetic DMARD (sulfasalazine or leflunomide), or a combination of a synthetic DMARD (MTX) with a bDMARD or targeted synthetic DMARD (tofacitinib, baricitinib) should be considered depending on the patient’s condition. Patients with poor response to the first bDMARD or targeted synthetic DMARD should be offered another bDMARD or targeted DMARD. Patients who fail treatment with the first TNF inhibitor can be given either a second TNF inhibitor or a bDMARD with a different mode of action.3–5
The standard end point to measure the efficacy of treatment in clinical trials on RA is the American College of Rheumatology (ACR) response rate. The ACR20, ACR50, and ACR70 response is defined as a reduction of ≥20%, ≥50%, and ≥70%, respectively, in the number of tender and swollen joints and in at least three of the following ACR core measures: patient’s assessment of pain, physician’s global assessment of disease, patient’s global assessment of disease, physical function as assessed by the Health Assessment Questionnaire-Disability Index (HAQ-DI), and the level of acute-phase reactants: erythrocyte sedimentation rate or C-reactive protein.6
The aim of this paper was to review the mode of action, pharmacology, pharmacokinetics, as well as the efficacy and safety of a targeted synthetic DMARD, baricitinib, as monotherapy or in combination with csDMARDs, in patients with RA. A literature search was conducted by two reviewers in the main electronic databases: Medline via PubMed, EMBASE, and Cochrane Central Register of Controlled Trials (last search September 2018). The keywords “baricitinib” and “rheumatoid arthritis” were used for the search. The appropriate randomized controlled trials (RCTs) and their long-term extensions (LTEs) published in English were selected based on the titles and abstracts. An additional analysis of the safety profile, especially regarding adverse events (AEs) of special interest, was performed according to pooled data from the main clinical trials and Summary of Product Characteristics. Moreover, the ClinicalTrials.gov website was searched to find ongoing clinical trials assessing the efficacy of baricitinib in conditions other than RA.
Baricitinib: mechanism of action and pharmacology
Baricitinib is a synthetic small-molecule drug, which modulates cytokine signaling by targeting the JAK/STAT pathway involved in inflammatory response.7 This oral drug is a preferential and highly selective JAK1 and JAK2 inhibitor that has shown efficacy in Phase II studies in patients with RA who had an inadequate response to csDMARDs.8,9 The JAK family, consisting of JAK1, JAK2, and tyrosine kinase 2, is involved in the signaling pathways of various cytokines and growth factors that have been implicated in the pathogenesis of RA.10 Activation of proinflammatory cytokine pathways is essential in the disease pathogenesis, especially of IL-6, IL-2, and interferons, which use JAK-dependent pathways.11
Baricitinib preferentially targets signaling receptors associated with JAK1 and JAK2 pathways believed to be important in the pathogenesis of RA. This results in the inhibition of transmigration of STAT molecules to the nucleus. JAK1 and JAK2 are widely expressed and mediate signaling of multiple cytokines implicated in the pathogenesis of RA, such as interferons, IL-6, and granulocyte macrophage colony-stimulating factor.12 Baricitinib has a short half-life. The pharmacokinetic profile of the molecule is characterized by rapid absorption and elimination in humans, with a time to peak concentration of approximately 1.5 hours following oral administration and a half-life of approximately 3 hours. In humans, approximately 75% of the administered dose is cleared in the urine, while about 20%, in the feces; the drug metabolism is mediated by CYP3A4, with <10% of the dose identified as undergoing biotransformation.13
The European Commission granted a marketing authorization valid throughout the European Union for Olumiant® (Eli Lilly) on 13 February 2017. It was approved for use at a dose of 2 or 4 mg administered orally, in combination with MTX, for the treatment of moderately to severely active RA in adult patients. In case of intolerance or contraindications to MTX, it can be given as monotherapy.13 In May 2018, the US Food and Drug Administration approved the 2 mg once-daily dose of Olumiant® for the treatment of adults with moderately to severely active RA who have had an inadequate response to one or more therapies with a TNF inhibitor.14
Clinical efficacy of baricitinib
Four large Phase III trials assessing the efficacy and safety of baricitinib at a registered dose of 2 or 4 mg once daily in patients with RA were identified: RA-BEACON,15–17 RA-BUILD,18,19 RA-BEAM,20,21 and RA-BEGIN22,23 (Table 1). In the randomized double-blind RA-BEACON trial,15–17 527 patients with moderate-to-severe RA were assigned in a 1:1:1 ratio to baricitinib at a dose of 2 mg, baricitinib at a dose of 4 mg, or placebo. Before the study, patients showed an inadequate response or intolerance to at least one therapy with TNF inhibitors. Patients who received baricitinib had significantly higher ACR20 and ACR50 response rates than patients given placebo. At 12 weeks, the percentage of patients who achieved the ACR20 response was significantly higher in the group treated with baricitinib (2 and 4 mg) than in the placebo group (49% and 55% vs 27%). Similarly, more patients in the 2 and 4 mg baricitinib groups achieved the ACR50 response at 12 weeks than in the placebo group (20%, 28%, and 8%, respectively). A significant benefit of baricitinib over placebo in terms of ACR20 and ACR50 response rates was also maintained at 24 weeks of therapy.
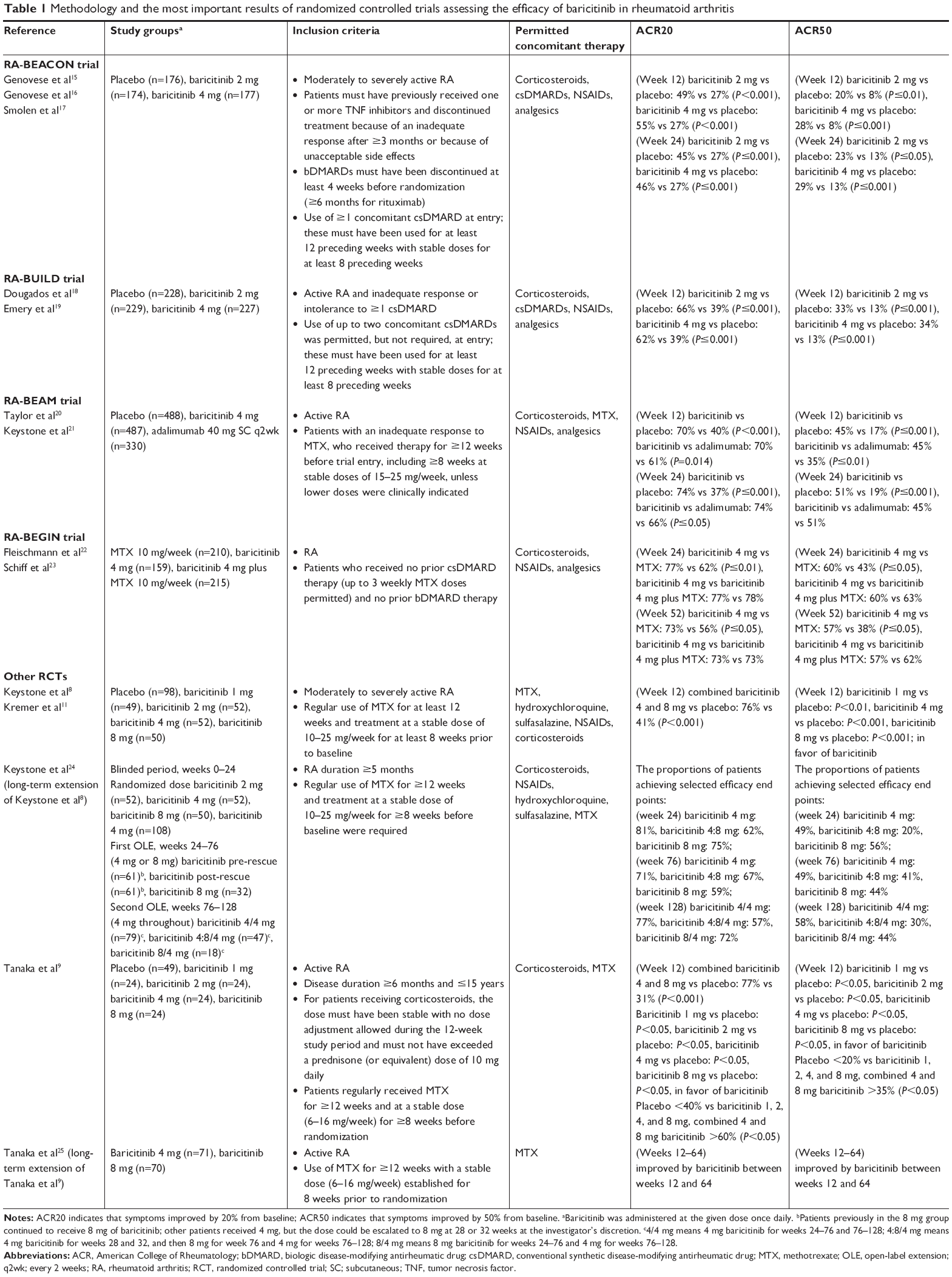 | Table 1 Methodology and the most important results of randomized controlled trials assessing the efficacy of baricitinib in rheumatoid arthritis |
In the RA-BUILD trial,18,19 684 patients with active RA and an inadequate response to one or more csDMARDs were randomized into three groups: placebo, baricitinib at a dose of 2 mg, or baricitinib at a dose of 4 mg once daily over 12 weeks. The ACR20 response was achieved by a higher percentage of patients in baricitinib groups than in the placebo group (66% in the 2 mg dose group, 62% in the 4 mg dose group, and 39% in the placebo group; P≤0.001).
The efficacy of baricitinib was confirmed in the RA-BEAM20,21 trial, which included 1,305 patients with active RA and an inadequate response to MTX. The trial compared baricitinib at a dose of 4 mg with adalimumab and placebo. Baricitinib was shown to decrease the activity of the disease at 12 and 24 weeks. At 12 weeks, the ACR20 response was achieved by 70% of patients receiving baricitinib and 40% of those receiving placebo (P<0.001). A significant improvement was also observed in the case of baricitinib administration compared with adalimumab: the ACR20 response was achieved by 70% in baricitinib group and 61% in adalimumab group (P=0.014). The effect was maintained at 24 weeks of therapy. As for the other secondary and exploratory end points, the comparison showed a benefit of baricitinib over placebo in the ACR50 response rate at 12 weeks (45% vs 17%; P≤0.001) and at 24 weeks (51% vs 19%; P≤0.001), as well as of baricitinib over adalimumab at 12 weeks (45% vs 35%; P≤0.01).
The RA-BEGIN trial22,23 was a randomized double-blind trial with an active comparator. Patients were randomized in a 4:3:4 ratio to receive MTX monotherapy (given orally once a week), baricitinib (4 mg once daily), or a combination of baricitinib 4 mg and MTX (baricitinib plus MTX). Baricitinib decreased the activity of RA in patients without prior DMARD therapy or with prior limited MTX therapy. Monotherapy with baricitinib was shown to outweigh monotherapy with MTX at 24 weeks, with the ACR20 response rate being 77% and 62%, respectively (P≤0.01).
The efficacy and safety of baricitinib administered at a dose from 1 to 8 mg once daily were assessed in randomized multicenter Phase IIb double-blind trials in patients with moderately to severely active RA.8,9,11,24,25 In the studies by Keystone et al8 and Tanaka et al,9 conducted in patients with inadequate response to MTX therapy, significantly more number of patients who received baricitinib at a dose of 4 mg once daily achieved the ACR20 and ACR50 response after 12 weeks than patients receiving placebo (Table 1). Moreover, the trial by Keystone et al8 showed that the 2 mg dose of baricitinib was less effective in terms of the ACR20, ACR50, and ACR70 response rates as well as low disease activity or remission at 12 and 24 weeks than the 4 mg dose. According to the results, the 4 mg dose of baricitinib was considered optimal for assessment in Phase III trials, while the 2 mg dose proved less effective.8
In the trial by Tanaka et al,9 baricitinib (4 mg) therapy resulted in a significant improvement of each ACR component, as compared with placebo (Table 1). In the group receiving baricitinib at a dose of 2 mg, the percentage of patients with the ACR20 response was significantly higher than in the group receiving placebo. However, the response to treatment did not occur as quickly as with the higher doses. The benefits of treatment with the 4 mg dose were observed immediately after 2 weeks, while the most notable effects were reported at 8 weeks.9 The percentage of patients who achieved the ACR20 response was higher at 12 weeks in all groups treated with baricitinib as compared with the placebo group. The percentage of patients who achieved ACR50 or ACR70 response also increased during the 12 weeks of therapy.9 Extended-phase studies24,25 revealed that the percentage of patients with ACR20 and ACR50 response was maintained or increased in the long-term follow-up.
Effect of baricitinib on patient-related outcomes (PROs)
Refractory patients with a previously inadequate response to bDMARDs who were treated with baricitinib (2 and 4 mg) showed a significant improvement over placebo in most PROs evaluated in the RA-BEACON trial.17 Improvements were generally faster and more notable in patients receiving baricitinib at a dose of 4 mg than those receiving 2 mg dose and were maintained until week 24. Compared with placebo-treated patients, a higher number of those receiving baricitinib reported improvements in the patient’s global assessment of disease activity (PtGA; P≤0.001) and pain (P≤0.001), a reduction in the duration of morning joint stiffness (P<0.01) and fatigue (Functional Assessment of Chronic Illness Therapy-Fatigue [FACIT-F] score ≥3.56; P≤0.05), and normal physical functioning (HAQ-DI score <0.5; P≤0.001). No significant differences were observed between patients treated with baricitinib and placebo in the 36-item Short Form Health Survey (SF-36) mental component score (MCS) and physical component score (PCS), which is consistent with observations from previous clinical trials.17
Compared with placebo, baricitinib at a dose of 2 or 4 mg resulted in a significant improvement in PROs across different domains of RA, including physical function, fatigue, pain, and quality of life. The 4 mg dose was associated with a more rapid improvement compared with the 2 mg dose. Significant improvements were observed for both baricitinib groups (2 and 4 mg) vs placebo in health-related quality of life (HRQoL), as measured by the EuroQoL-5D (EQ-5D) and SF-36 PCS at week 12. Patients in the baricitinib groups reported a significantly greater improvement in the FACIT-F score and EQ visual analog scale, PtGA, daily diary measures, and HAQ-DI at week 24, as compared with the placebo group.19
The above findings were confirmed by other studies.19,23 Baricitinib treatment resulted in a significantly greater improvement compared with placebo or adalimumab treatment in most of the prespecified PROs, including physical function, pain, fatigue, duration and severity of morning joint stiffness, as well as HRQoL (SF-36 PCS, EQ-5D index scores, and Activity Impairment Questionnaire: Rheumatoid Arthritis [WPAI-RA] daily activity) at 12 weeks. A significant improvement in the worst tiredness and worst joint pain was observed for baricitinib vs placebo and adalimumab at 12 weeks (P≤0.05). Furthermore, compared with placebo and adalimumab, baricitinib resulted in a rapid improvement in the diary PROs, including morning joint stiffness duration and severity, with significant differences vs placebo observed within a few days from treatment initiation. Compared with adalimumab, improvements in physical function, pain, fatigue, and HRQoL (eg, SF-36 PCS and EQ-5D) were maintained until week 52.21
In the RA-BEGIN23 study, patients in both baricitinib groups (baricitinib monotherapy and baricitinib plus MTX), compared with MTX-treated patients, reported a greater improvement (P≤0.01) in HAQ-DI, PtGA, pain, fatigue, worst join pain, SF-36 PCS, and EQ-5D at 24 and 52 weeks. They also reported a significant improvement (P≤0.01) in the SF-36 MCS at 52 weeks. In addition, they showed an improvement (P≤0.05) in the WPAI-RA score at 24 weeks. At week 52, significant improvement in WPAI-RA daily activity and work productivity scores was maintained only in the baricitinib-plus-MTX group compared with the MTX group.23
Summarizing, patients with active RA treated with baricitinib reported sustained, clinically meaningful, and significant improvements in most PROs compared to those treated with placebo, MTX, and adalimumab.17,19,21,23
Safety and tolerability of baricitinib
The safety and tolerability of baricitinib in patients with a moderate-to-severe RA were studied in several RCTs8,9,15,18,20,22 as well as an integrated analysis of nine trials, which evaluated baricitinib at doses ranging from 1 to 15 mg daily, with a maximum drug exposure period of up to 5.5 years.26,27 The general safety profile of baricitinib administered at an approved dose of 2 or 4 mg once daily was found to be acceptable irrespective of the concomitant use of csDMARDs.
In the studies by Tanaka et al9 and Keystone et al,8 with a relatively small population of patients (<60 in groups receiving baricitinib) and a short initial follow-up of 12 weeks, the incidence of treatment-emergent AEs did not differ between patients receiving 2 mg baricitinib (46%–50%), those receiving 4 mg baricitinib (42%–54%), and the placebo group (46%–53%). A similar tendency was observed in the large RA-BUILD study (with >200 patients in each group),18 with a comparable rate of AEs after 24 weeks of exposure between 2 mg baricitinib, 4 mg baricitinib, and placebo groups (67%, 71%, and 71%, respectively). In the other studies with a follow-up of 24 weeks, RA-BEACON15 and RA-BEAM,20 the percentage of patients who experienced any AEs was higher in the 2 and 4 mg baricitinib groups (71% and 71%–77%, respectively) than in the placebo group (60%–64%). As compared with an active comparator, the incidence of AEs at 52 weeks was similar with 4 mg baricitinib and adalimumab (79% vs 77%)20 as well as with 4 mg baricitinib and MTX (71% vs 72%);22 coadministration of MTX with 4 mg baricitinib increased the risk of AEs to 78%.22
The studies by Tanaka et al9 and Keystone et al8 revealed a similar, generally low incidence of serious AEs (SAEs) in a short-term follow-up of 12 weeks: 2%–3% in placebo group, 4%–6% in 2 mg baricitinib group, and interestingly, 0% in 4 mg baricitinib group. A similar incidence rate was observed in the RA-BUILD trial after 24 weeks of treatment: 5%, 3%, and 5% in the placebo, 2 mg baricitinib, and 4 mg baricitinib groups, respectively.18 A slightly higher rate of SAEs at 24 weeks was reported in the RA-BEACON study: 7%, 4%, and 10% in the placebo, 2 mg baricitinib, and 4 mg baricitinib groups, respectively.15 As compared with adalimumab (2%), the overall incidence of SAEs was higher after administration of baricitinib at a dose of 4 mg (5%) or placebo (5%); however, no particular type of event was noted at a lower rate in the adalimumab group at 24 weeks in the RA-BEAM study.20 The rates of SAEs were similar for MTX monotherapy (10%), monotherapy with 4 mg baricitinib (8%), and combined treatment with 4 mg baricitinib and MTX (8%) at 52 weeks in the RA-BEGIN study.22
The rates of treatment discontinuation due to AEs were generally low in baricitinib groups,8,9,15,18,20,22 irrespective of the concomitant use of MTX or other conventional DMARDs, and did not exceed 11%.22 In the study by Tanaka et al,9 during the 12-week follow-up, none of the patients in the 2 and 4 mg baricitinib groups stopped treatment due to AEs, as compared with 2% in the placebo group. In the 24-week follow-up, discontinuation due to AEs was reported for 3%20 to 4%15,18 in placebo, 2%8 to 4%15,18 in 2 mg baricitinib, 4%8 to 6%15 in 4 mg baricitinib, and 2%20 in adalimumab groups. In the RA-BEGIN trial,22 treatment discontinuation due to AEs at 52 weeks was reported for 11% of patients who received baricitinib with MTX, compared with 5% of those receiving MTX monotherapy and 6% of those on baricitinib alone. The integrated analysis of eight RCTs and one LTE study, including 3,492 patients treated with baricitinib for a total of 6,637 patient-years (PYs) and with a maximum drug exposure period of 5.5 years, revealed a similar risk of treatment discontinuation due to AEs in 4 mg baricitinib and placebo groups.26,27 The incidence rate (IR) of death during baricitinib treatment at a dose of 4 mg was estimated at 0.7 (95% CI: 0.1; 2.1) for 100 PYs and was higher as compared with that calculated for baricitinib groups, regardless of the dose (IR =0.33 [95% CI: 0.2; 0.5]), but similar to that for placebo (IR =0.5 [95% CI: 0.1; 1.8]).26,27
The safety profile of baricitinib may slightly differ depending on the patients’ age. A post hoc analysis of two Phase III studies evaluating the use of 4 mg baricitinib in patients with inadequate response to a csDMARD revealed that the risk of AEs increased with the patients’ age.28 A numerically higher percentage of patients in the older age group (≥65 years) reported AEs (99.3%), SAEs (8.8%), and serious infections (2.9%) than in the younger age groups (<50 years: AEs – 88.4%, SAEs – 3.1%, serious infections – 1.2%; ≥50 to <65 years: AEs – 92.8%, SAEs – 4.7%, serious infections – 0.6%). It should be noted that the incidence of AEs, SAEs, or withdrawals due to AEs in baricitinib-treated patients was generally similar to that observed for age-matched placebo-treated patients (for placebo group <50 years: AEs – 83.5%, SAEs – 3.9%; ≥50 to <65 years: AEs – 93.4%, SAEs – 3.2%; ≥65 years: AEs – 98.2%, SAEs – 10.6%). This may result from a higher incidence of comorbidities and changes in pharmacodynamics in older patients, so elderly people with RA should be followed very carefully during baricitinib therapy.28
AEs of special interest
Patients with RA have a higher incidence of comorbidities such as infections, cardiovascular events, or some types of cancer, as compared with the healthy population.29,30 Considering the disease background as well as the type and spectrum of applied treatment, it may be difficult to establish whether the comorbidities are the result only of RA or administered therapies.29 However, close monitoring of patients and screening for the above events is necessary irrespective of their origin.
As expected, the most common AEs reported during baricitinib therapy were infections, including bronchitis,15,20 upper respiratory tract infections,15,18,20,22 nasopharyngitis,9,15,20 pharyngitis,9,15,20 sinusitis,15 and urinary tract infections.15.20.22 The rates of serious infections were comparable between groups treated with 2 mg baricitinib, 4 mg baricitinib, and placebo (<1%–2%,15,18 2%–4%,15,18,20,22 and 2%–3%,15,18 respectively) and similar to those for active comparators: MTX – 4%,22 baricitinib plus MTX – 2%,22 and adalimumab – 2%.20 The IR of serious infections was estimated at 2.9 for 100 PYs (95% CI: 2.5; 3.4) for all baricitinib-treated patients and 3.8 (95% CI: 2.2; 6.2) for individuals receiving 4 mg baricitinib, with no difference from placebo (IR =4.2 [95% CI: 2.5; 6.8]), in the integrated analysis conducted by Genovese et al26 and Smolen et al.27
Opportunistic infections, such as herpes zoster, were not common, but their frequency was slightly higher in the 4 mg baricitinib group (2%–4%15,18,20,22) than in the 2 mg baricitinib group (1%–2%15,18). In most of the reported cases, patients previously received bDMARDs15 or were of Asian descent.20,22 The integrated analysis of the safety profile revealed that the IR of herpes zoster was significantly higher after administration of baricitinib at a dose of 4 mg (IR =4.3 per 100 PYs) than placebo (IR =1.0 per 100 PYs).26
Major adverse cardiovascular events (MACEs) were rare. In the RA-BEACON study, <1.5% (two cases) of adjudicated MACEs were reported in the 4 mg baricitinib group.15 A similar ratio was reported in the RA-BEGIN trial:22 <1% of patients treated with baricitinib at a dose of 4 mg and MTX experienced MACEs. No cases of MACEs were reported in the RA-BUILD study18 in both the 2 and 4 mg baricitinib groups. The IR calculated for MACEs was comparable between patients receiving 4 mg baricitinib (IR =0.8 [95% CI: 0.2; 2.2] for 100 PYs) and placebo (IR =0.5 [95% CI: 0.1; 2.0] for 100 PYs).26
Two cases (<1.5%) of cancer (non-melanoma) were reported during the administration of baricitinib at a dose of 4 mg in the RA-BEACON study,15 three cases (<1%) in the RA-BEAM study,20 and one case (<1%) in the RA-BUILD18 and RA-BEGIN study.22 The concomitant use of MTX and 4 mg baricitinib increased the rate of cancer up to 2%.22 However, concerning rare AEs, such as malignancies, the studies with a relatively short-term follow-up (up to 52 weeks) may be insufficient to fully analyze this effect. In the integrated analysis of RCTs and LTE studies, the IR of malignancies (excluding non-melanoma skin cancer) for all baricitinib groups (IR =0.8 per 100 PYs) as well as for 4 mg baricitinib group (IR =0.5 per 100 PYs) was low and similar to that for placebo (IR =0.5 per 100 PYs).26,27
The impact of baricitinib on the reproductive system is very poorly understood. Studies in animals have shown teratogenic effect of baricitinib and decreased female fertility with no effect on male spermatogenesis. There are no adequate data for the use of baricitinib in pregnant or breast-feeding women as well as its influence on fertility, so it is contraindicated during pregnancy.13 Only a single case of erectile dysfunction18 and serious metrorrhagia20 was reported in main clinical trials.
Changes in laboratory parameters
The common effects of baricitinib administration were changes in clinical laboratory parameters: neutrophil, lymphocyte, and platelet counts as well as hemoglobin, alanine aminotransferase, cholesterol, creatinine, and creatine kinase levels.15,18,20,22
Inhibition of the JAK/STAT pathway has been associated with modifications of hematopoiesis, resulting in changes in hematological parameters induced by baricitinib.31 The drug was observed to reduce neutrophil count and cause a moderate increase in platelet count.15,18,20,22 There were no differences between the number of patients experiencing thrombocytosis defined as ≥600,000 platelets/mm3 in groups treated with baricitinib compared with placebo, adalimumab, and MTX.15,18,20,22 A transient elevation of the lymphocyte count was noted during early administration of baricitinib at a dose of 4 mg, but the values returned to baseline during weeks 24–52 of treatment.20 A small decrease in the hemoglobin level was observed in 2 mg and 4 mg baricitinib groups, as compared with placebo;18 however, the risk of anemia was similar between placebo and baricitinib groups.15,18
Baricitinib at a dose of 2 and 4 mg was shown to affect liver function seen by a small increase of the alanine aminotransferase level;15,18,20,22 however, in most cases, the abnormalities were transient and generally without concomitant bilirubin level elevation.15,18,20
As compared with placebo, the levels of high-density lipoprotein (HDL) and low-density lipoprotein (LDL) were increased during baricitinib therapy with the 2 mg15,18 and the 4 mg dose.15,18,20 At 24–52 weeks of 4 mg baricitinib therapy, the LDL level stabilized while the HDL level remained elevated with a tendency to slowly decrease.20 A higher increase of LDL and HDL levels was seen in the baricitinib groups than in the MTX monotherapy group.22 However, the mechanism of baricitinib’s action on lipoprotein levels was not fully understood. It was found that the increase in HDL levels was associated with improved clinical outcomes such as the Simplified Disease Activity Index and Disease Activity Score 28-joint assessment in Phase II trials. Interestingly, no similar correlations were observed for the changes in total cholesterol, LDL, and triglyceride levels.11
The mean serum creatinine level increased slightly during baricitinib treatment15,18,20,22 but did not exceed grade 1–2,15,20,22 which means mild-to-moderate severity according to Common Terminology Criteria for Adverse Events (CTCAE), and was transient in most cases, irrespective of the length of treatment period.15,18,20,22 The observed effect may reflect the small changes in renal function.18
The serum level of creatine kinase increased in the 4 mg1518,20,22 and the 2 mg baricitinib groups.15,18 The elevation of creatine kinase levels classified as grade 3 (severe) or 4 (life-threatening, according to CTCAE) was rare, and in most cases, it resulted from physical activity or abnormalities at baseline.15,18,20,22
Baricitinib in the therapy of diseases other than RA
The immunosuppressive properties of baricitinib could be useful in the treatment of different immune diseases, including systemic lupus erythematosus, psoriasis, or atopic dermatitis.31–33 The hypothesis that baricitinib might have a therapeutic benefit in patients with systemic lupus erythematosus was confirmed in a double-blind, placebo-controlled RCT32 conducted in patients with active disease involving the skin or joints. The results indicated that baricitinib administered only as a 4 mg dose significantly improved the signs and symptoms of systemic lupus erythematosus in patients with inadequate disease control despite standard-of-care therapy, with an acceptable safety profile.32 A promising effect of baricitinib on psoriasis was found in an RCT by Papp et al.31 Patients with moderate-to-severe psoriasis treated with baricitinib achieved significant improvements in the Psoriasis Area and Severity Index (PASI)-50 (only at doses of 4, 8, or 10 mg) and PASI-75 (only at doses of 8 or 10 mg) over placebo. The majority of safety findings were consistent with the known safety profile of baricitinib and observed with a higher frequency in the groups treated with the 8 and 10 mg dose, while the rates of AEs in the 2 and 4 mg dose groups were comparable to placebo.31 Another placebo-controlled RCT33 revealed that baricitinib at a dose of 4 mg used with topical corticosteroids reduced inflammation and pruritus, and improved sleep in patients with moderate-to-severe atopic dermatitis.
Currently, there are many ongoing Phase II and III studies assessing the efficacy and safety of baricitinib in populations of patients with lupus erythematosus, atopic dermatitis, giant cell arteritis, alopecia areata, and chronic graft-vs-host disease (Table 2). The positive results of these trials may lead to the extension of registered indications for baricitinib in the future.
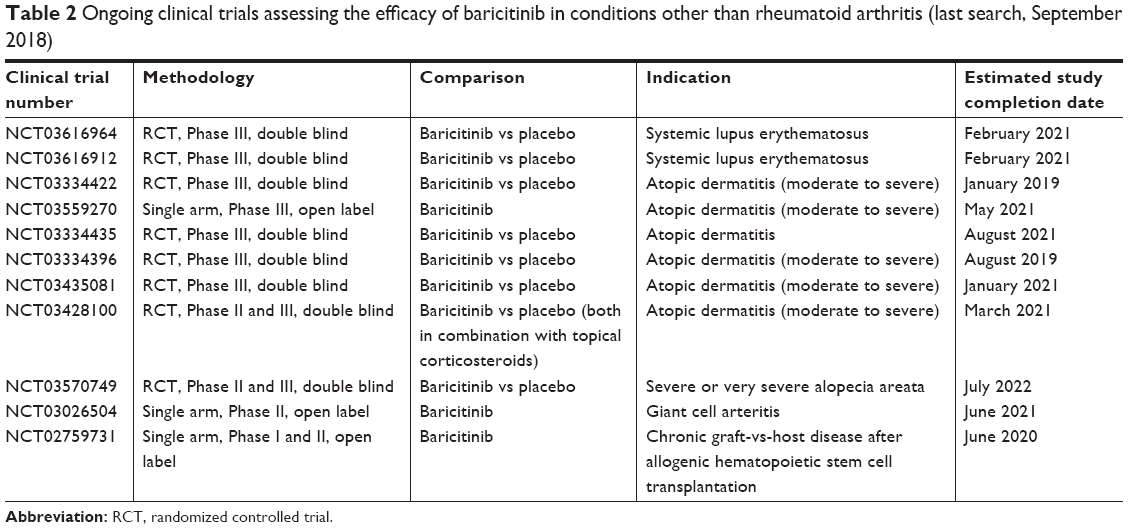 | Table 2 Ongoing clinical trials assessing the efficacy of baricitinib in conditions other than rheumatoid arthritis (last search, September 2018) |
Conclusion
Baricitinib is a drug with a mechanism of action similar to that of tofacitinib but different than that of other products approved for the treatment of RA. It may be considered as a therapeutic option in some patients with no response to the standard therapy. An oral route of administration seems to be a quite new and promising alternative, as compared with subcutaneous or intravenous biologic drugs. Some RCTs revealed a significant benefit of baricitinib over placebo in terms of the efficacy outcomes (ACR20, ACR50, and ACR70 response rates). Clinical trials on baricitinib provided data of a good safety profile, with increased incidence of infections and abnormal laboratory parameters reported as the most common AEs. The majority of AEs proved to be nonserious and did not lead to treatment discontinuation. Further research is needed to provide more information on the clinical effectiveness and safety profile of baricitinib.
Disclosure
The authors report no conflicts of interest in this work.
References
Calabresi E, Petrelli F, Bonifacio AF, Puxeddu I, Alunno A. One year in review 2018: pathogenesis of rheumatoid arthritis. Clin Exp Rheumatol. 2018;36(2):175–184. | ||
Myasoedova E, Davis JM, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379–385. | ||
Gaujoux-Viala C, Gossec L, Cantagrel A, et al. Recommendations of the French Society for Rheumatology for managing rheumatoid arthritis. Joint Bone Spine. 2014;81(4):287–297. | ||
Singh JA, Saag KG, Bridges SL, et al. 2015 American College of rheumatology guideline for the treatment of rheumetoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. | ||
Smolen JS, Landewé R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76(6):960–977. | ||
Felson DT, Anderson JJ, Boers M, et al. American College of rheumatology preliminary definition of improvement in rheumatoid arthritis. Arthritis & Rheumatism. 1995;38(6):727–735. | ||
Shi JG, Chen X, Lee F, et al. The pharmacokinetics, pharmacodynamics, and safety of baricitinib, an oral JAK 1/2 inhibitor, in healthy volunteers. J Clin Pharmacol. 2014;54(12):1354–1361. | ||
Keystone EC, Taylor PC, Drescher E, et al. Safety and efficacy of baricitinib at 24 weeks in patients with rheumatoid arthritis who have had an inadequate response to methotrexate. Ann Rheum Dis. 2015;74(2):333–340. | ||
Tanaka Y, Emoto K, Cai Z, et al. Efficacy and safety of baricitinib in Japanese patients with active rheumatoid arthritis receiving background methotrexate therapy: a 12-week, double-blind, randomized placebo-controlled study. J Rheumatol. 2016;43(3):504–511. | ||
Fridman JS, Scherle PA, Collins R, et al. Selective inhibition of JAK1 and Jak2 is efficacious in rodent models of arthritis: preclinical characterization of INCB028050. J Immunol. 2010;184(9):5298–5307. | ||
Kremer JM, Genovese MC, Keystone E. Effects of baricitinib on lipid, apolipoprotein, and lipoprotein particle profiles in a phase IIb study of patients with active rheumatoid arthritis. Arthritis & Rheumatology. 2017;69(5):943–952. | ||
O’Shea JJ, Kontzias A, Yamaoka K, Tanaka Y, Laurence A. Janus kinase inhibitors in autoimmune diseases. Ann Rheum Dis. 2013;72(suppl 2):ii111–ii115. | ||
European Medicines Agency. Olumiant® – Summary of Product Characteristics. EMA; 2017. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/004085/WC500223723.pdf. Accessed September 30, 2018. | ||
U.S. Food and Drug Administration Drug Approval Package: Olumiant® (baricitinib). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/207924Orig1s000TOC.cfm. Accessed September 30, 2018. | ||
Genovese MC, Kremer J, Zamani O, et al. Baricitinib in patients with refractory rheumatoid arthritis. N Engl J Med. 2016;374(13):1243–1252. | ||
Genovese MC, Kremer JM, Kartman CE, et al. Response to baricitinib based on prior biologic use in patients with refractory rheumatoid arthritis. Rheumatology. 2018;57(5):900–908. | ||
Smolen JS, Kremer JM, Gaich CL, et al. Patient-reported Outcomes from a randomised phase III study of baricitinib in patients with rheumatoid arthritis and an inadequate response to biological agents (RA-BEACON). Ann Rheum Dis. 2017;76(4):694–700. | ||
Dougados M, van der Heijde D, Chen Y-C, et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: results from the RA-BUILD study. Ann Rheum Dis. 2017;76(1):88–95. | ||
Emery P, Blanco R, Maldonado Cocco J, et al. Patient-reported Outcomes from a phase III study of baricitinib in patients with conventional synthetic DMARD-refractory rheumatoid arthritis. RMD Open. 2017;3(1):e000410. | ||
Taylor PC, Keystone EC, van der Heijde D, et al. Baricitinib versus placebo or adalimumab in rheumatoid arthritis. N Engl J Med. 2017;376(7):652–662. | ||
Keystone EC, Taylor PC, Tanaka Y, et al. Patient-reported Outcomes from a phase 3 study of baricitinib versus placebo or adalimumab in rheumatoid arthritis: secondary analyses from the RA-BEAM study. Ann Rheum Dis. 2017;76(11):1853–1861. | ||
Fleischmann R, Schiff M, van der Heijde D, et al. Baricitinib, methotrexate, or combination in patients with rheumatoid arthritis and no or limited prior disease-modifying antirheumatic drug treatment. Arthritis & Rheumatology. 2017;69(3):506–517. | ||
Schiff M, Takeuchi T, Fleischmann R, et al. Patient-reported outcomes of baricitinib in patients with rheumatoid arthritis and no or limited prior disease-modifying antirheumatic drug treatment. Arthritis Res Ther. 2017;19(1):208. | ||
Keystone EC, Genovese MC, Schlichting DE, et al. Safety and efficacy of baricitinib through 128 weeks in an open-label, longterm extension study in patients with rheumatoid arthritis. J Rheumatol. 2018;45(1):14–21. | ||
Tanaka Y, Ishii T, Cai Z, Schlichting D, Rooney T, Macias W. Efficacy and safety of baricitinib in Japanese patients with active rheumatoid arthritis: a 52-week, randomized, single-blind, extension study. Modern Rheumatology. 2018;28(1):20–29. | ||
Genovese MC, Smolen JS, Takeuchi T, et al. Safety profile of baricitinib for the treatment of rheumatoid arthritis up to 5.5 years: an updated integrated safety analysis. Arthritis Rheumatol. 2017;69(suppl 10):Abstract 511. | ||
Smolen JS, Genovese MC, Takeuchi T, et al. Safety profile of baricitinib in patients with active rheumatoid arthritis with over 2 years median time in treatment. J Rheumatol. 2019;46(1):7–18. | ||
Fleischmann R, Alam J, Arora V, et al. Safety and efficacy of baricitinib in elderly patients with rheumatoid arthritis. RMD Open. 2017;3(2):e000546. | ||
Dougados M. Comorbidities in rheumatoid arthritis. Curr Opin Rheumatol. 2016;28(3):282–288. | ||
Dougados M, Soubrier M, Antunez A, et al. Prevalence of comorbidities in rheumatoid arthritis and evaluation of their monitoring: results of an international, cross-sectional study (COMORA). Ann Rheum Dis. 2014;73(1):62–68. | ||
Papp KA, Menter MA, Raman M, et al. A randomized phase 2B trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br J Dermatol. 2016;174(6):1266–1276. | ||
Wallace DJ, Furie RA, Tanaka Y, et al. Baricitinib for systemic lupus erythematosus: a double-blind, randomised, placebo-controlled, phase 2 trial. The Lancet. 2018;392(10143):222–231. | ||
Guttman-Yassky E, Silverberg JI, Nemoto O, et al. Baricitinib in adult patients with moderate-to-severe atopic dermatitis: a phase 2 parallel, double-blinded, randomized placebo-controlled multiple-dose study. J Am Acad Dermatol. Epub 2018 Feb 1. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.