")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Neutrophil-to-Lymphocyte Ratio Better Than High-Sensitivity C-Reactive Protein in Predicting Stroke-Associated Pneumonia in Afebrile Patients
Authors Wu T, Zhang H, Tian X, Cao Y, Wei D, Wu X
Received 19 September 2021
Accepted for publication 30 November 2021
Published 9 December 2021 Volume 2021:17 Pages 3589—3595
DOI https://doi.org/10.2147/NDT.S340189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Ti Wu,1,* Haipeng Zhang,2,* Xiaolin Tian,3 Yang Cao,2 Dianjun Wei,4 Xiangkun Wu4
1Department of Neurology, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Department of Clinical Laboratory, The Second Hospital of Tianjin Medical University, Tianjin, People’s Republic of China; 3Department of Neurology, The Second Hospital of Tianjin Medical University, Tianjin, People’s Republic of China; 4Department of Clinical Laboratory, Hebei Yanda Hospital, Langfang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangkun Wu Tel +8615613682051
Email [email protected]
Purpose: To evaluate the association between neutrophil-to-lymphocyte ratio (NLR) and stroke-associated pneumonia (SAP) in patients with acute ischemic stroke (AIS) without fever and to clarify whether NLR has an advantage over high-sensitivity C-reactive protein (hs-CRP) in predicting SAP.
Patients and Methods: A total of 434 patients with AIS without fever were assessed in this study. Multivariable analysis was used to evaluate the relationship between NLR and SAP, and the receiver operating characteristic (ROC) curve was used to compare the predictive value of NLR and hs-CRP.
Results: Among the total patients, 18 (4.1%) developed SAP. After adjusting for confounders, NLR (adjusted odds ratio [aOR] = 1.60; 95% confidence interval [CI], 1.30– 1.96; p < 0.001) remained independently associated with an increased risk of SAP. In addition, the area under the curve (AUC) of NLR (0.862 [0.826– 0.893]) was higher than that of hs-CRP (0.738 [0.694– 0.779]).
Conclusion: We found that compared with hs-CRP, NLR was significantly associated with the occurrence of SAP in patients with AIS without fever and showed a more effective predictive value for SAP.
Keywords: stroke, pneumonia, neutrophil, lymphocyte, high-sensitivity C-reactive protein, inflammation
A Letter to the Editor has been published for this article.
Introduction
Stroke-associated pneumonia (SAP), defined as new onset pneumonia within 7 days after stroke, is a common complication in patients with acute ischemic stroke (AIS).1 It has been reported that 7–38% of patients with stroke experience SAP.2–6 For these patients, not only do the length of hospital stay and cost of hospitalization increase significantly, but the risks of disability and death also greatly increase.7,8 It is well known that pyrexia is key in the diagnosis of pneumonia; however, studies have shown that 25–66% of patients with SAP may not have pyrexia.9,10 This may make clinicians ignore the infection. Therefore, a simple and effective biomarker is needed to quickly identify SAP in afebrile patients.
Neutrophil-to-lymphocyte ratio (NLR), calculated by dividing the absolute neutrophil count by the absolute lymphocyte count, is a novel marker of systemic inflammation and infection.11,12 C-reactive protein (CRP), one of the most accessible and widely used biomarkers, also plays a key role in the identification and evaluation of infections.13,14 High-sensitivity C-reactive protein (hs-CRP) is a sensitive marker of inflammation, it detects low concentrations of CRP using a high-sensitivity assay technique.15 Several studies have demonstrated that high NLR and CRP levels could predict SAP in patients with AIS.16,17 At the same time, elevated CRP has also been shown to improve the diagnostic accuracy of the current SAP algorithms, independent of pyrexia.18 However, the predictive value of hs-CRP and NLR in patients with AIS without fever remains unknown. In this study, we aimed to evaluate the association between NLR and SAP in AIS patients without fever and to clarify whether NLR has an advantage over hs-CRP in predicting SAP.
Patients and Methods
Study Population
This study was approved by the Ethics Committee of The Second Hospital of Tianjin Medical University. We retrospectively studied all patients with AIS who were admitted to the neurology ward of The Second Hospital of Tianjin Medical University from November 2018 to October 2020. Computed tomography (CT) or magnetic resonance imaging (MRI) was used to confirm the diagnosis of AIS. Patients were eligible for inclusion if they were ≥ 18 years of age and had onset of symptoms ≤ 72 h at recruitment. The exclusion criteria were (1) patients with severe hepatic or renal diseases; (2) having recently undergone major trauma or surgery; (3) a history of a malignant tumor, hematologic disease, or immunosuppressive treatment; (4) temperature ≥ 38°C at any one time within 7 days of stroke onset; (5) active infection at admission or incomplete medical records.
Data Collection
The demographic and clinical characteristics, such as age, sex, previous history of diabetes, hypertension, atrial fibrillation, stroke, smoking, stroke severity at admission, occurrence of SAP, and relevant laboratory data (blood cell counts and hs-CRP), were recorded within 24 h of admission. Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS). The diagnostic criteria for SAP were based on the Chinese expert consensus on the diagnosis and treatment of SAP (Supplementary Table 1).
Statistical Analyses
For continuous variables with non-normal distributions, the data are presented as median + interquartile range (IQR), while normal distributions are expressed as mean ± standard deviation (SD). Univariate analyses were conducted using the Mann–Whitney U-test and the independent-samples t-test. For categorical variables, frequency and percentage were used to express the data and were evaluated using the chi-squared test. To assess the basic characteristics of the subjects in the high NLR group, we also conducted another comparison between the high and low NLR groups by dichotomizing the cohort with the median NLR (2.56). The predictive values of NLR and hs-CRP were compared using the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. All statistical analyses were performed using SPSS 19.0 and MedCalc 15.2.2, and statistical significance was set at P < 0.05.
Results
A total of 434 patients with AIS (mean age, 68 years; men, 66%) were included in our study, and the majority (60%) were admitted within 24 h of symptom onset. The median initial NIHSS and NLR were 2 (1–5) and 2.56 (1.95–3.60), respectively. Of the patients, 18 (4.1%) developed SAP, and none of them had a fever of > 38°C at any one time within 7 days of stroke onset.
Compared with the patients in the non-SAP group, patients in the SAP group were older and nonsmokers, had a higher proportion of females, atrial fibrillation, and had higher levels of initial NIHSS, hs-CRP, and white blood cell (WBC) counts. In addition, the level of NLR in the SAP group was also significantly higher than that in the non-SAP group (6.43 [4.39–8.00] vs 2.51 [1.91–3.45], P < 0.001) (Table 1). After adjusting for confounders, NLR (1.60 [1.30–1.96], P < 0.001) and initial NIHSS (1.16 [1.04–1.28], P = 0.006) remained independent predictors of SAP (Table 2).
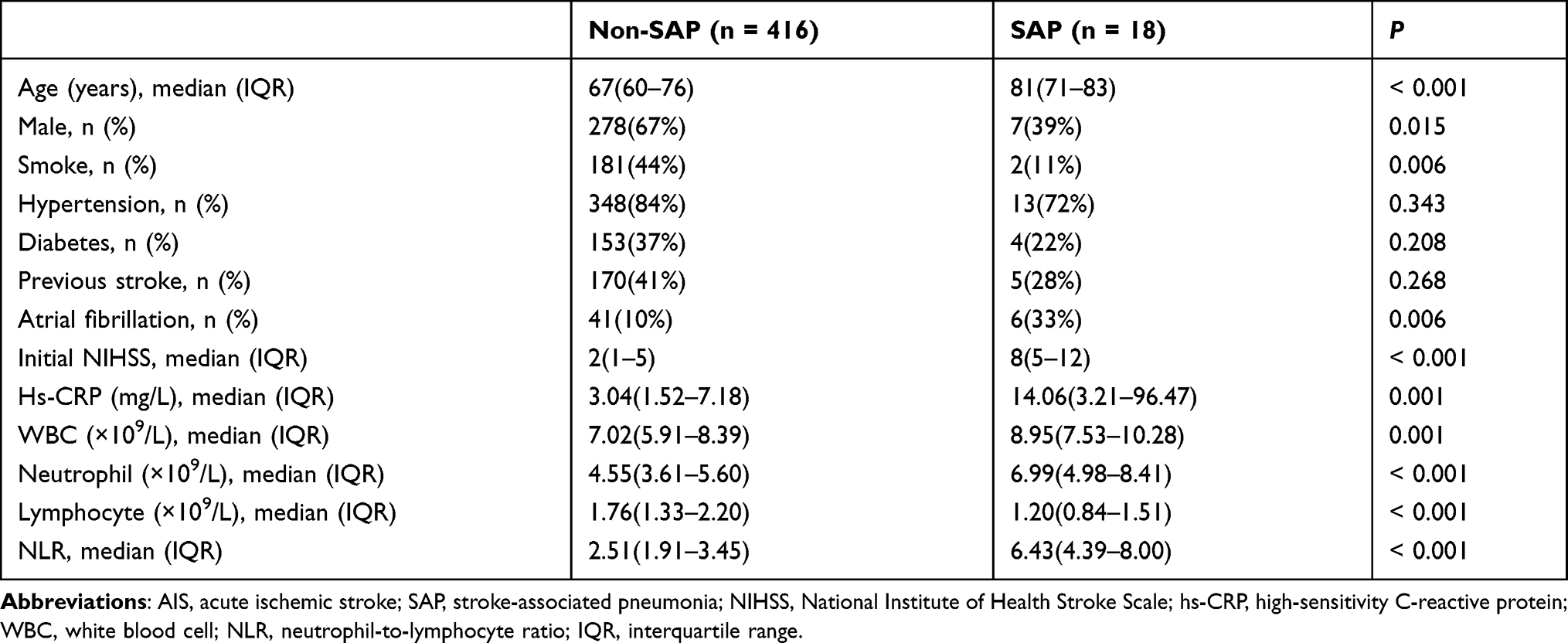 |
Table 1 Baseline Characteristics of Afebrile Patients with SAP and Non-SAP with AIS |
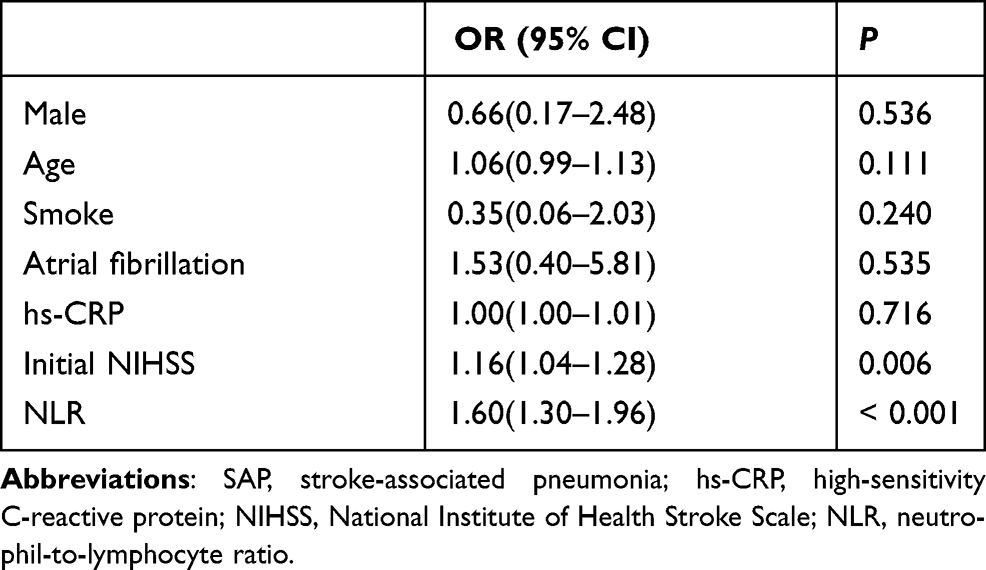 |
Table 2 Multivariable Analysis of Possible Predictors of SAP |
We also conducted another comparison between the high and low NLR groups. The incidence of SAP was significantly higher in the high NLR group than in the low NLR group (8.3% vs 0, P < 0.001). In addition, patients in the high NLR group were older and presented a higher proportion of hypertension and atrial fibrillation, and they had higher levels of initial NIHSS, hs-CRP and WBC counts than those in the low NLR group (Table 3).
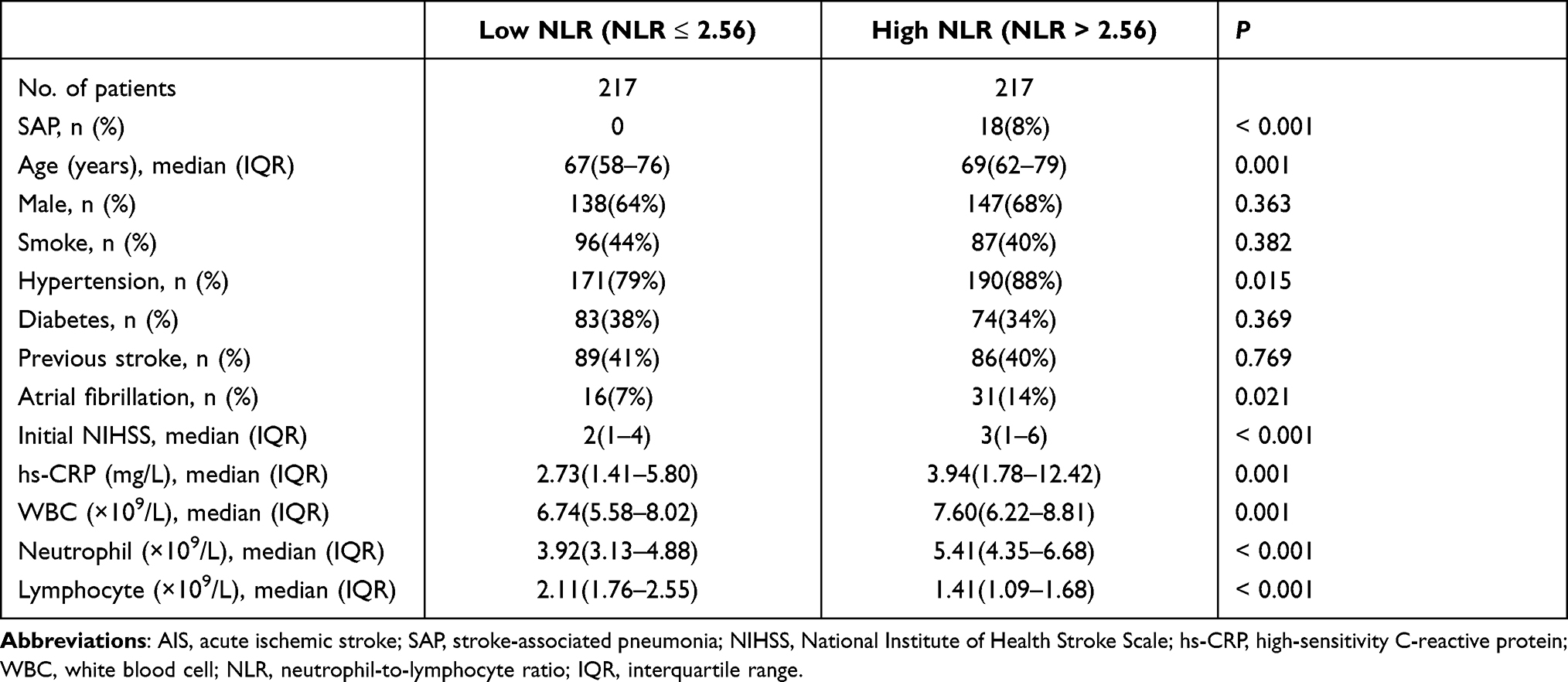 |
Table 3 Baseline Characteristics of Afebrile Patients with Low and High NLRs with AIS |
ROC analysis revealed that the optimal value for NLR to predict SAP was 4.64, with a sensitivity and specificity of 77.8% and 88.5%, respectively. NLR (0.862 [0.826–0.893]) showed a higher AUC value than that of WBC (0.729 [0.685–0.771]), neutrophils (0.800 [0.759–0.837]), lymphocytes (0.773 [0.731–0.812]), and hs-CRP (0.738 [0.694–0.779]) (Table 4).
 |
Table 4 Predictive Values of Different Indicators in the Prediction of Stroke-Associated Pneumonia in Afebrile Patients |
Discussion
To the best of our knowledge, our study was the first to investigate the relationship between NLR, hs-CRP, and SAP in afebrile patients. We found that compared with hs-CRP, NLR was significantly associated with the occurrence of SAP in AIS patients without fever and showed a more effective predictive value for SAP.
At present, the diagnosis of SAP is difficult. This is not only because the diagnostic criteria for SAP are inconsistent, but also because there is a lack of prospective studies for validation.19 It is also due to the fact that the clinical presentation of patients is often atypical and vague, and the sensitivity of laboratory and radiological tests, such as chest radiography and sputum cultures, is low.8,10,19,20 CRP, an acute-phase inflammatory protein, promotes the aggregation or deposition of damaged cells or exogenous microorganisms, leading to the activation of the classical complement pathway that promotes phagocytosis by macrophages.21 Currently, CRP is widely used as a biomarker for patients with cancer, stroke, infections and cardiovascular diseases.22–25 It has also been proven to be highly sensitive for the diagnosis of bacterial infections, even in patients without fever.26 In AIS, elevated CRP has been shown to be strongly associated with the occurrence of stroke-associated infection (SAI) and SAP.16,17,27
NLR is an economical, simple and timely blood biomarker that is well known as a predictor of infection and inflammation. It has shown a higher predictive value than the traditional inflammatory markers in various diseases, such as stroke, cancer, and multiple sclerosis.28–30 In patients with AIS, damage-associated molecular patterns (DAMPs) released from injured neurons exacerbate focal inflammation, causing the infiltration of neutrophils and other peripheral inflammatory cells, secretion of large amounts of inflammatory mediators, and a disseminated inflammatory response throughout the brain, leading to further damage to the brain tissue and neurons.31 After that, there is immunosuppression, as the injured brain initiates an adaptive response that reduces the inflammatory response as well as the autoimmune response to neuronal antigens.32 Meanwhile, the sympathetic and hypothalamic-pituitary-adrenal (HPA) axis is activated and secretes catecholamines and cortisol, leading to increased apoptosis and dysfunction of lymphocytes, as well as decreased secretion of immunoglobulins.33–37 The activation of the sympathetic nervous system after stroke also mobilizes neutrophils in peripheral reservoirs, leading to an increase in the number of circulating neutrophils.38 In addition, as shown in Table 3, patients in the high NLR group had more risk factors for developing SAP, such as advanced age, higher rates of hypertension and atrial fibrillation, and higher stroke severity. This may also be the reason that a high NLR could predict the occurrence of SAP in patients with AIS without fever.
In this study, we found that patients with a high initial NIHSS were more likely to develop SAP, which is consistent with the findings of the previous studies.16,17 Moreover, compared to hs-CRP, NLR may be a more valuable marker to help distinguish the SAP group from the non-SAP group. There are several possible explanations for this phenomenon. First, SAP, unlike simple bacterial infections, is a respiratory syndrome caused by a complex interaction between bacterial, chemical, and immunocompromising factors.35 This is the reason why prophylactic antibiotics neither reduce the incidence of SAP nor improve its prognosis.39,40 Immunosuppression is one of the main mechanisms leading to the development of SAP, and immunosuppression is highly correlated with NLR, which makes NLR a more effective predictor of the development of SAP. Second, the exact role of CRP in the diagnosis of SAP remains unclear. For example, in the studies of STROKE-INF and MAPS, elevated CRP was found in 44% and 91% of patients with AIS, while only 12% and 73% of these patients developed SAP, respectively.10,40 In the present study, hs-CRP levels were not independently associated with the occurrence of SAP. This was consistent with the study by Emsley et al, where it was found that an elevated CRP level is common in acute stroke patients due to inflammation caused by infarction or hemorrhage, even in the absence of infection.41 Therefore, as shown in Figure 1, the area under the curve (AUC) of NLR (0.862 [0.826–0.893]) was higher than that of hs-CRP (0.738 [0.694–0.779]).
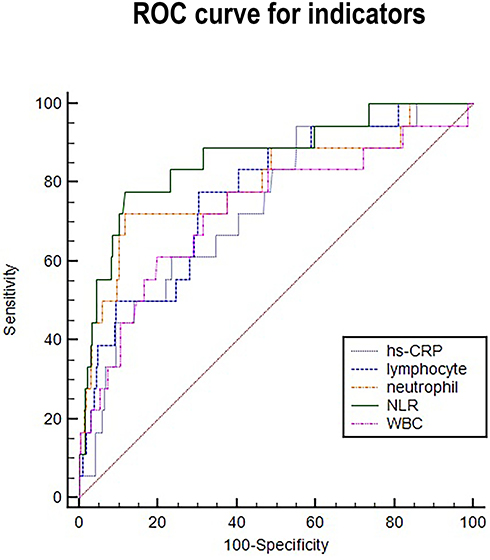 |
Figure 1 Comparison of predictive value between NLR and other indicators in the prediction of stroke-associated pneumonia in afebrile patients. |
Our study had several limitations. First, this study was a single-center retrospective design and was thus subject to selection bias. Second, the time of admission may have resulted in bias. SAP events have been reported to occur mainly during the first 2 to 3 days. Therefore, although 60% of our patients were admitted within 24 h of symptom onset, it was still possible to miss some of them. Third, due to incomplete data, we could not evaluate the relationship between the NLR and SAP dynamically. Fourth, there are still many other unknown factors influencing our results, despite our best efforts to control the bias with multivariate models. Fifth, although we reviewed 2 years of data, the sample size was small, especially for the patients in the SAP group. Therefore, a multicenter prospective study with more sample data is needed to confirm our findings.
Conclusion
Compared with hs-CRP, NLR was significantly associated with the occurrence of SAP in AIS patients without fever, and showed a more effective predictive value in predicting SAP. Moreover, NLR > 4.64 could be applied to screen for SAP, even in AIS patients without fever.
Ethics Statement
This study adheres to the principles of the Declaration of Helsinki. The study involving human participants were reviewed and approved by the Ethics Committee of The Second Hospital of Tianjin Medical University (No. KL2021K003). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Acknowledgments
We thank all the study participants and clinical staffs for their support and contribution to this project. Ti Wu and Haipeng Zhang are co-first authors for this study.
Funding
This work was supported by grant from Hebei Medical Research Foundation (20191061, 20191066).
Disclosure
Dr Xiangkun Wu reports personal fees from Hebei Yanda Hospital, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Smith CJ, Kishore AK, Vail A, et al. Diagnosis of stroke-associated pneumonia: recommendations from the Pneumonia in Stroke Consensus Group. Stroke. 2015;46(8):2335–2340. doi:10.1161/STROKEAHA.115.009617
2. Ji R, Wang D, Shen H, et al. Interrelationship among common medical complications after acute stroke: pneumonia plays an important role. Stroke. 2013;44(12):3436–3444. doi:10.1161/STROKEAHA.113.001931
3. Smith CJ, Bray BD, Hoffman A, et al. Can a novel clinical risk score improve pneumonia prediction in acute stroke care? A UK multicenter cohort study. J Am Heart Assoc. 2015;4(1):e001307. doi:10.1161/JAHA.114.001307
4. Teh WH, Smith CJ, Barlas RS, et al. Impact of stroke-associated pneumonia on mortality, length of hospitalization, and functional outcome. Acta Neurol Scand. 2018;138(4):293–300. doi:10.1111/ane.12956
5. Yu YJ, Weng WC, Su FC, et al. Association between pneumonia in acute stroke stage and 3-year mortality in patients with acute first-ever ischemic stroke. J clin neurosci. 2016;33:124–128.
6. Badve MS, Zhou Z, van de Beek D, Anderson CS, Hackett ML. Frequency of post-stroke pneumonia: systematic review and meta-analysis of observational studies. Int J Stroke. 2019;14(2):125–136. doi:10.1177/1747493018806196
7. Finlayson O, Kapral M, Hall R, et al. Risk factors, inpatient care, and outcomes of pneumonia after ischemic stroke. Neurology. 2011;77(14):1338–1345. doi:10.1212/WNL.0b013e31823152b1
8. Li L, Zhang LH, Xu WP, Hu JM. Risk assessment of ischemic stroke associated pneumonia. World J Emerg Med. 2014;5(3):209–213. doi:10.5847/wjem.j.issn.1920-8642.2014.03.009
9. Kalra L, Hodsoll J, Irshad S, Smithard D, Manawadu D, Investigators S-I. Comparison of the diagnostic utility of physician-diagnosed with algorithm-defined stroke-associated pneumonia. J Neurol Neurosurg Psychiatry. 2016;87(11):1163–1168.
10. Warusevitane A, Karunatilake D, Sim J, Smith C, Roffe C. Early diagnosis of pneumonia in severe stroke: clinical features and the diagnostic role of C-Reactive protein. PLoS One. 2016;11(3):e0150269. doi:10.1371/journal.pone.0150269
11. Cataudella E, Giraffa CM, Di Marca S, et al. Neutrophil-to-Lymphocyte ratio: an emerging marker predicting prognosis in elderly adults with community-acquired Pneumonia. J Am Geriatr Soc. 2017;65(8):1796–1801. doi:10.1111/jgs.14894
12. Mei Z, Shi L, Wang B, et al. Prognostic role of pretreatment blood neutrophil-to-lymphocyte ratio in advanced cancer survivors: a systematic review and meta-analysis of 66 cohort studies. Cancer Treat Rev. 2017;58:1–13. doi:10.1016/j.ctrv.2017.05.005
13. Worthmann H, Tryc AB, Dirks M, et al. Lipopolysaccharide binding protein, interleukin-10, interleukin-6 and C-reactive protein blood levels in acute ischemic stroke patients with post-stroke infection. J Neuroinflammation. 2015;12:13. doi:10.1186/s12974-014-0231-2
14. Bustamante A, Vilar-Bergua A, Guettier S, et al. C-reactive protein in the detection of post-stroke infections: systematic review and individual participant data analysis. J Neurochem. 2017;141(2):305–314. doi:10.1111/jnc.13973
15. Liu X, Guo X, Zhang Z. Preoperative serum hypersensitive-c-reactive-protein (Hs-CRP) to albumin ratio predicts survival in patients with Luminal B subtype breast cancer. Onco Targets Ther. 2021;14:4137–4148. doi:10.2147/OTT.S320111
16. Nam KW, Kim TJ, Lee JS, et al. High Neutrophil-to-Lymphocyte ratio predicts stroke-associated Pneumonia. Stroke. 2018;49(8):1886–1892. doi:10.1161/STROKEAHA.118.021228
17. Gens R, Ourtani A, De Vos A, De Keyser J, De Raedt S. Usefulness of the Neutrophil-to-Lymphocyte ratio as a predictor of pneumonia and urinary tract infection within the first week after acute ischemic stroke. Front Neurol. 2021;12:671739. doi:10.3389/fneur.2021.671739
18. Kalra L, Smith CJ, Hodsoll J, Vail A, Irshad S, Manawadu D. Elevated C-reactive protein increases diagnostic accuracy of algorithm-defined stroke-associated pneumonia in afebrile patients. Int J Stroke. 2019;14(2):167–173. doi:10.1177/1747493018798527
19. Kishore AK, Vail A, Chamorro A, et al. How is pneumonia diagnosed in clinical stroke research? A systematic review and meta-analysis. Stroke. 2015;46(5):1202–1209. doi:10.1161/STROKEAHA.114.007843
20. Hassan A, Khealani BA, Shafqat S, et al. Stroke-associated pneumonia: microbiological data and outcome. Singapore Med J. 2006;47(3):204–207.
21. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805–1812. doi:10.1172/JCI200318921
22. Ji M, Du L, Ma Z, et al. Circulating C-reactive protein increases lung cancer risk: results from a prospective cohort of UK Biobank. Int j Cancer. 2021;150:47–55. doi:10.1002/ijc.33780
23. Yu J, Shi X, Ma J, et al. C-Reactive protein is an independent predictor of 30-day bacterial infection post-liver transplantation. Biomolecules. 2021;11(8):1195. doi:10.3390/biom11081195
24. Da Venezia C, Hussein N, Hernandez M, et al. Assessment of cardiovascular risk in women with periodontal diseases according to C-reactive protein levels. Biomolecules. 2021;11(8):1238. doi:10.3390/biom11081238
25. Hurth H, Birkenhauer U, Steiner J, Schlak D, Hennersdorf F, Ebner FH. Delayed cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage - Serum D-dimer and C-reactive protein as early markers. J Stroke Cerebrovasc Dis. 2020;29(3):104558. doi:10.1016/j.jstrokecerebrovasdis.2019.104558
26. Liu A, Bui T, Van Nguyen H, Ong B, Shen Q, Kamalasena D. Serum C-reactive protein as a biomarker for early detection of bacterial infection in the older patient. Age Ageing. 2010;39(5):559–565. doi:10.1093/ageing/afq067
27. Cheng W, Chen L, Yu H, Lu D, Yu R, Chen J. Value of combining of the NLR and the fibrinogen level for predicting stroke-associated Pneumonia. Neuropsychiatr Dis Treat. 2021;17:1697–1705. doi:10.2147/NDT.S311036
28. Hu Y, Huang K, Ji Z, et al. High neutrophil-to-lymphocyte ratio is associated with poor clinical outcome in patients with critically ill stroke. Minerva Anestesiol. 2020;86(9):939–947. doi:10.23736/S0375-9393.20.14310-4
29. Iwai N, Okuda T, Sakagami J, et al. Neutrophil to lymphocyte ratio predicts prognosis in unresectable pancreatic cancer. Sci Rep. 2020;10(1):18758. doi:10.1038/s41598-020-75745-8
30. Olsson A, Gustavsen S, Gisselo Lauridsen K, et al. Neutrophil-to-lymphocyte ratio and CRP as biomarkers in multiple sclerosis: a systematic review. Acta Neurol Scand. 2021;143(6):577–586. doi:10.1111/ane.13401
31. Shi K, Tian DC, Li ZG, Ducruet AF, Lawton MT, Shi FD. Global brain inflammation in stroke. Lancet Neurol. 2019;18(11):1058–1066. doi:10.1016/S1474-4422(19)30078-X
32. Shi K, Wood K, Shi FD, Wang X, Liu Q. Stroke-induced immunosuppression and poststroke infection. Stroke Vasc Neurol. 2018;3(1):34–41. doi:10.1136/svn-2017-000123
33. Liu Q, Jin WN, Liu Y, et al. Brain ischemia suppresses immunity in the periphery and brain via different neurogenic innervations. Immunity. 2017;46(3):474–487. doi:10.1016/j.immuni.2017.02.015
34. McCulloch L, Smith CJ, McColl BW. Adrenergic-mediated loss of splenic marginal zone B cells contributes to infection susceptibility after stroke. Nat Commun. 2017;8:15051. doi:10.1038/ncomms15051
35. Cui P, McCullough LD, Hao J. Brain to periphery in acute ischemic stroke: mechanisms and clinical significance. Front Neuroendocrinol. 2021;63:100932. doi:10.1016/j.yfrne.2021.100932
36. Prass K, Meisel C, Hoflich C, et al. Stroke-induced immunodeficiency promotes spontaneous bacterial infections and is mediated by sympathetic activation reversal by poststroke T helper cell type 1-like immunostimulation. J Exp Med. 2003;198(5):725–736. doi:10.1084/jem.20021098
37. Vogelgesang A, Grunwald U, Langner S, et al. Analysis of lymphocyte subsets in patients with stroke and their influence on infection after stroke. Stroke. 2008;39(1):237–241. doi:10.1161/STROKEAHA.107.493635
38. Zhang J, Shi K, Li Z, et al. Organ- and cell-specific immune responses are associated with the outcomes of intracerebral hemorrhage. FASEB j. 2018;32(1):220–229. doi:10.1096/fj.201700324r
39. Westendorp WF, Vermeij JD, Zock E, et al. The Preventive Antibiotics in Stroke Study (PASS): a pragmatic randomised open-label masked endpoint clinical trial. Lancet. 2015;385(9977):1519–1526. doi:10.1016/S0140-6736(14)62456-9
40. Kalra L, Irshad S, Hodsoll J, et al. Prophylactic antibiotics after acute stroke for reducing pneumonia in patients with dysphagia (STROKE-INF): a prospective, cluster-randomised, open-label, masked endpoint, controlled clinical trial. Lancet. 2015;386(10006):1835–1844. doi:10.1016/S0140-6736(15)00126-9
41. Emsley HC, Smith CJ, Gavin CM, et al. An early and sustained peripheral inflammatory response in acute ischaemic stroke: relationships with infection and atherosclerosis. J Neuroimmunol. 2003;139(1–2):93–101. doi:10.1016/S0165-5728(03)00134-6
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.