")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Neuromodulation in eating disorders and obesity: a promising way of treatment?
Authors Jáuregui-Lobera I , Martínez-Quiñones JV
Received 14 July 2018
Accepted for publication 31 August 2018
Published 26 October 2018 Volume 2018:14 Pages 2817—2835
DOI https://doi.org/10.2147/NDT.S180231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Ignacio Jáuregui-Lobera,1 José V Martínez-Quiñones2
1Department of Molecular Biology and Biochemical Engineering, University of Pablo de Olavide of Seville, Seville, Spain; 2Department of Neurosurgery, Mutua de Accidentes de Zaragoza (Servicio de Neurocirugía), Zaragoza, Spain
Abstract: Neuromodulation can affect the functioning of the central nervous system (CNS), and emotional/eating behavior is an exciting facet of that functioning. Therefore, it would be possible to offer an alternative (or complement) treatment to psychotropic medications and different psychological and nutritional approaches to both eating disorders (EDs) and obesity. Although there are a number of publications in these areas, a systematic review has not been conducted to date. Abstracts, letters, conference reports, dissertations, and reviews were excluded. Clinical trials and controlled human clinical trials were filtered and included in this study. Articles included were based on the population suffering from anorexia nervosa, bulimia nervosa, binge ED, overweight, and obesity. No restrictions were placed on the sample size. Only trials investigating the effect of neuromodulation by means of deep brain stimulation (DBS), transcranial direct current stimulation (tDCS), and transcranial magnetic stimulation (TMS) were included. The following databases were used to conduct the search: MEDLINE/PubMed, PsycINFO, PsycArticles, and Cochrane (Search Trials, CENTRAL). Study selection was performed following the PRISMA process (PRISMA 2009 Checklist). The total number of participants in all the trials was 562 (DBS, 25; tDCS, 138; TMS, 399; range, 3–90; median, 23.5). As a result, 50% of the studies had samples of between 14 and 38 participants. Neuromodulation in ED seems to have certain clinical potential, and therefore, this is a promising area for further research. Developments in ED neuromodulation will be linked to neuroimaging to identify potential stimulation targets and possible biomarkers of treatment response. To date, TMS and/or direct current stimulation (DCS) is not the first-line treatment yet, but it could become a preferred option of treatment in the future. Further studies should avoid small sample sizes and the use of different methodologies. Currently, neuromodulation techniques are in the experimental phase, and they are not an evidence-based treatment for ED.
Keywords: deep brain stimulation, transcranial direct current stimulation, transcranial magnetic stimulation, anorexia nervosa, bulimia nervosa, obesity
Introduction
Neuromodulation involves the modification of specific neural circuit activity without causing damage to the nervous tissue, which implies the recovery of the prior functional state after suspending the stimulus. This technique aims to activate or deactivate neural networks by applying an electric current, controllable with respect to frequency, amplitude, and pulse width.1
Neuromodulation has been proposed as an alternative to surgical procedures that were being applied in different pathologies. Experimental models have shown that the high-frequency electrical stimulation affects the whole neural system, altering its metabolism and modifying the production of neurotransmitters and even the protein synthesis. The side effects of surgical electrical stimulation are those inherent to the risk of surgery.1
The modern era of neuromodulation was started with the study of Benabid et al2 (1987) by means of deep brain stimulation (DBS) for the suppression of tremor in Parkinson’s disease. Progress in neuroimaging techniques, with the appearance of magnetic resonance and functional imaging, along with the improvement of surgical techniques has contributed to a greater development of these techniques and a greater precision in their applications.
Neuromodulation, by means of both invasive and noninvasive interventions, aims to alter the neural activity or excitability.3 It induces neuroplastic changes, and therefore, it could be used to attempt the reversibility of maladaptive neuroplastic changes in the brain, to prevent the development of maladaptive neuroplastic changes, or to improve adaptive neuroplastic changes occurring in the brain. Neuroplasticity is the ability of the neural tissue to reorganize, assimilate, and modify the biological, biochemical, and physiological mechanisms involved in intercellular communication and to adapt to receive stimuli.4,5 This implies modifications of the corresponding neural tissue, which includes, among many others, axonal regeneration, collateralization, neurogenesis, synaptogenesis, and functional reorganization.
These processes are based on signals facilitated or inhibited by the nervous system in the presence of different neurotransmitters that promote synaptic potentiation or depression in both the short and long term.6 These neurochemical mediators produce an increase or a decrease in the amplitude of the postsynaptic potential due to a repeated and usually rapid action known as tetanization (which can cause the mentioned potentiation or depression). This process may last for hours or days, partially sustained by molecules called “retrograde messengers.” This potentiation or inhibition (which may be homosynaptic or heterosynaptic) will affect the expression of second messengers such as cyclic AMP, either transitorily or permanently.7,8
DBS consists of the implantation of one or more electrodes (connected to a pulse generator) within the cerebral parenchyma. Different deep brain structures have been used as targets depending on the pathology to be treated. The therapeutic effect of DBS is due to a variety of mechanisms, modulating the monosynaptic or polysynaptic activity of the pathological network. In addition to neuronal changes, it causes synaptic and neurotransmitter changes, as well as changes in the cerebral blood flow and neuroplasticity stimulating neurogenesis. DBS was approved by the Food and Drug Administration as a treatment for essential tremor in 1997, for Parkinson’s disease in 2002, for primary dystonia in 2003, and for obsessive-compulsive disorder in 2009.9,10
Transcranial magnetic stimulation (TMS) is a focal, painless, and noninvasive brain stimulation technique that follows the fundamental principles of electromagnetic induction, where an electric current in the stimulation coil generates a magnetic field. The rate of change in this magnetic field induces an electric current flow in the near conductors. Thus, when the electric current passes through the stimulation coil and when it is placed tangentially on the skull, the generated magnetic field induces a parallel intracranial electric current of inverse direction that stimulates the cerebral cortex. The purpose of this technique is to modulate the excitability of the cerebral cortex through the application of brief magnetic pulses on the scalp. The adverse effects of TMS are mild and usually well tolerated.6,11
Finally, transcranial direct current stimulation (tDCS) is another noninvasive way of modulating cortical excitability by applying low-amplitude direct electrical stimulation currents through electrodes arranged on the scalp. This results in the neuromodulation of the motor cortex.12
From the psychopathological point of view, the use of electric current in the management of diseases is widely known, since electroconvulsive therapy (ECT) was first used in the 30s of last century. The pathologies that have accumulated more evidence are major depression, drug addiction, aggressiveness, and obsessive-compulsive disorder. In these cases, neuromodulation has been tried using DBS directed to brain structures that are active during the symptomatic phase of these pathologies. The aim is to inactivate these structures. The most used targets are the anterior arm of internal capsule, ventral striatum, subthalamus, inferior thalamic peduncle, external pallid globe, amygdala, and posteromedial hypothalamus. Currently, other brain stimulation techniques being studied in the treatment of psychiatric diseases are TMS and tDCS. Magnetic stimulation has shown a clear efficacy in the treatment of depression, and its use is approved by different public health agencies.13
With respect to eating disorders (EDs) and overweight/obesity, neuromodulation might be a useful therapeutic tool for several reasons. Traditionally, different psychotherapies, several medications, and family support have been used as key elements for treating these pathologies. Nevertheless, treatment outcomes remain modest, especially for anorexia nervosa (AN).14
Neuroimaging techniques have shown that psychotherapeutic and pharmacological treatments produce brain changes related to neuroplasticity. These changes have been reported to occur in a wide range of brain areas after therapy. A relevant problem is that no psychotherapeutic or pharmacological treatments target specific brain areas or have specific and localized effects.14
In this regard, the idea is that neuromodulation can affect the functioning of the central nervous system (CNS) and emotional/eating behavior is an exciting facet of that functioning. Consequently, it would be possible to offer an alternative (or complement) intervention to psychotropic medications and different psychological and nutritional approaches.14
Neuroimaging has contributed to the understanding of the neural correlates of AN, including comorbidities. Thus, the importance of affective brain processing in the symptomatology of AN has been reported, suggesting that affective regulation and alterations might play key roles in the maintenance of symptoms.15 With respect to bulimia nervosa (BN), imaging techniques, such as single-photon emission computed tomography (SPECT) and positron emission tomography (PET), usually indicate left frontal cerebral hypometabolism in both depressive and bulimic patients. These changes of activity in the frontal area might be critical for eating behavior.16 Along with BN, binge ED and some forms of obesity are characterized by compulsive overeating that is often precipitated by food craving. Neuromodulation could be relevant to suppress food craving since a growing number of studies have sought to directly manipulate dorsolateral prefrontal cortex (DLPFC) activation as a means of reducing cravings.17 Although overweight/obesity is not ED, it is a fact that food craving/overeating is usually a cause for obesity. In addition, it has been suggested that extreme weight conditions (eg, AN and obesity) have a similar dysfunctional executive profile that might play a role in the development and maintenance of such disorders.18
Although there are a number of publications in these areas, a systematic review has not been conducted to date. At least two questions remain: 1) How thoroughly has neuromodulation been tested in controlled human trials? 2) Do the results of these trials support the application of neuromodulation to get better psychological outcomes and mental health in EDs?
Bearing in mind the efficacy of neuromodulation in different psychopathological disorders, the aim of this work was to review the state of knowledge on the use of neuromodulation in ED and overweight/obesity. The objective of this review was to ascertain whether there is evidence, from controlled trials, of an effect of neuromodulation on either psychological outcomes or nutritional status in humans. To address this question, clinical trials were reviewed systematically in accordance with PRISMA guidelines.
Materials and methods
Overall, this study observed the methodological steps followed by Romijn and Rucklidge in their recent systematic review.19
Selection criteria
Selection criteria were defined before searches were completed. Only articles written or available in English and/or Spanish and published in full in peer-reviewed journals were included, and abstracts, letters, conference reports, dissertations, and reviews were excluded.
Types of studies
Clinical trials and controlled clinical trials were filtered and included in this study.
Types of participants
Only human trials were included. Articles included were based on the population suffering from AN, BN, binge ED, overweight, and obesity. No restrictions were placed on the sample size.
Types of interventions
Only trials investigating the effect of neuromodulation by means of DBS, tDCS, and TMS were included.
Outcome measures
Only studies with specific and adequate psychological measurements (eg, symptoms of EDs preintervention and postintervention) were included.
Searching process
Online databases were searched electronically. In addition, relevant studies were searched manually to identify studies published up to December 11, 2017.
Databases
Studies published up to December 11, 2017, were searched in the following databases: MEDLINE/PubMed, PsycINFO, PsycArticles, and Cochrane (Search Trials, CENTRAL).
The following search terms were used: neuromodulation, transcranial magnetic stimulation, deep brain stimulation, transcranial direct current stimulation, eating disorders, anorexia nervosa, bulimia nervosa, binge eating disorder, and obesity, as well as the corresponding abbreviations for the techniques (TMS, DBS, and tDCS). The Medical Subjects Headings and the Boolean operators AND/OR were used for the searching process. The final shared MeSH terms were as follows: 1) neuromodulation AND eating disorders; neuromodulation AND anorexia nervosa; neuromodulation AND bulimia nervosa; neuromodulation AND binge eating disorder; neuromodulation AND obesity; 2) transcranial magnetic stimulation AND eating disorders; transcranial magnetic stimulation AND anorexia nervosa; transcranial magnetic stimulation AND bulimia nervosa; transcranial magnetic stimulation AND binge eating disorder; transcranial magnetic stimulation AND obesity; 3) deep brain stimulation AND eating disorders; deep brain stimulation AND anorexia nervosa; deep brain stimulation AND bulimia nervosa; deep brain stimulation AND binge eating disorder; deep brain stimulation AND obesity; 4) transcranial direct current stimulation AND eating disorders; transcranial direct current stimulation AND anorexia nervosa; transcranial direct current stimulation AND bulimia nervosa; transcranial direct current stimulation AND binge eating disorder; transcranial direct current stimulation AND obesity. Terms covering the most common specific eating disorders were used.
Other sources
As mentioned earlier, relevant studies were searched manually to identify studies published up to December 11, 2017.
Selection of studies
Study selection was performed following the PRISMA process (PRISMA 2009 Checklist).20 First, titles, abstracts, and keywords were examined to exclude those citations that were clearly irrelevant. After this first screening, the remaining articles were examined by the authors independently. In case of doubt, a decision about inclusion/exclusion of a particular study was made after discussion.
Data extraction
The following data were extracted from the included studies: authors, date of publication, population (including any information on types of ED), gender and age of participants, sample size, number of participants in each group, comorbidity, types of interventions (TMS, DBS, and tDCS), length of the intervention period, measures, main outcomes, and others if necessary.
Assessment of methodological quality of included studies
Studies were evaluated by the authors following the Jadad scale.21 In this case, apart from the items related to bias control (randomization, quality of blinding, and reasons for withdrawal/dropouts) some others were considered: objectives, outcome measurements, well-defined inclusion/exclusion criteria, clear description of intervention, description of adverse effects, and statistical analyses. A score of 2 or above was accepted.
Data description
Table 1 shows the summary of main studies, and a narrative style was followed to better describe the results.
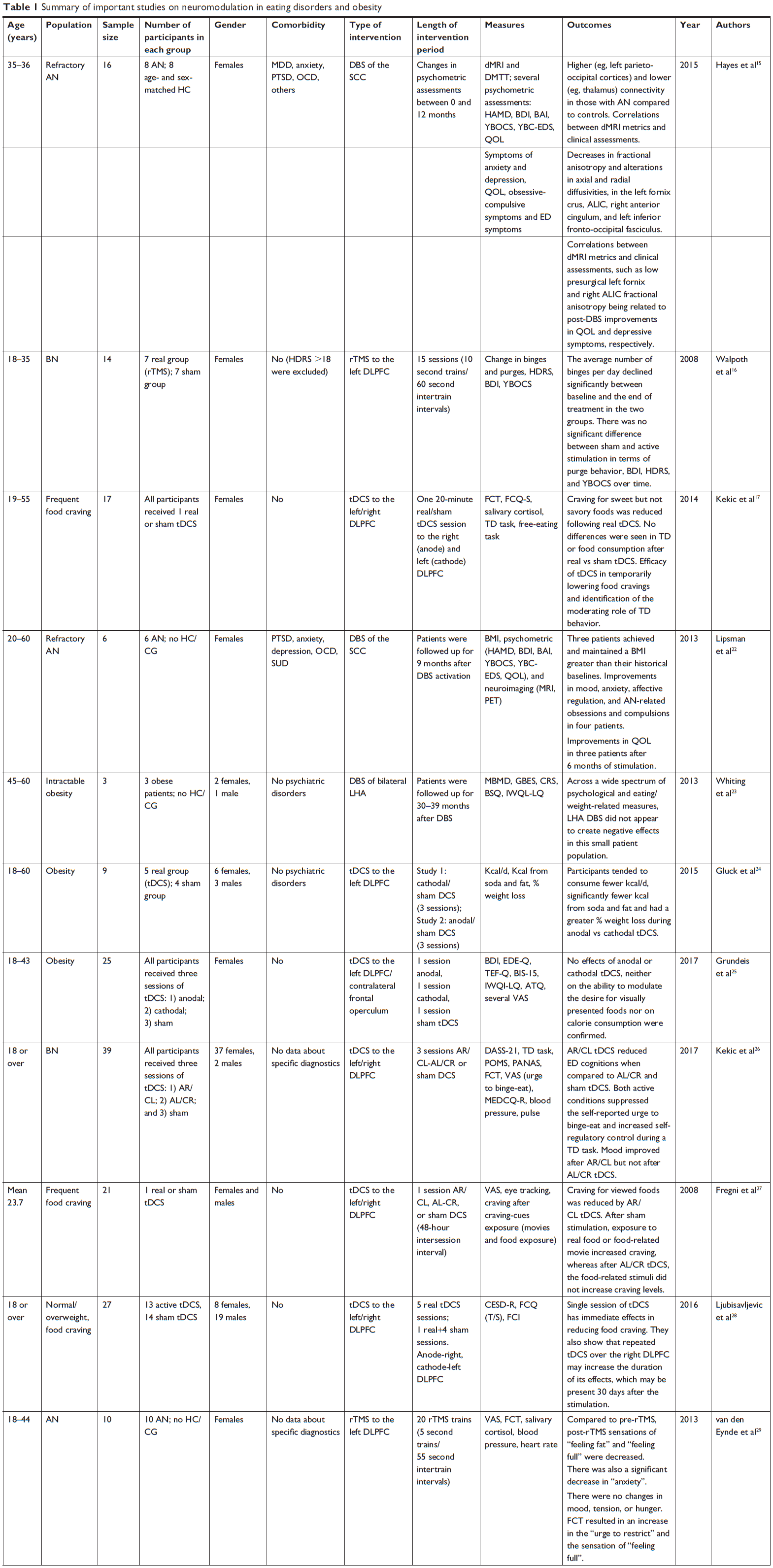  | Table 1 Summary of important studies on neuromodulation in eating disorders and obesity |
Results
Participants
The total number of participants in all trials was 562 (DBS: 25; tDCS: 138; TMS: 399; range, 3–90; median, 23.5). As a result, 50% of the studies had samples of between 14 and 38 participants. Participants were healthy controls and patients suffering from AN, BN, binge ED, and EDs not otherwise specified. In addition, patients with overweight, obesity, and frequent food craving were included.
Interventions
In this study, interventions based on DBS, tDCS, and TMS were analyzed.
DBS
The study by Hayes et al analyzed possible differences between AN patients and healthy controls with respect to subcallosal cingulate cortex (SCC) connectivity.15 After undergoing DBS, AN patients (n=8) were studied by means of diffusion magnetic resonance imaging (dMRI) and deterministic multitensor tractography. AN patients also completed affect-related clinical assessments presurgically and 12 months postsurgery. As a result, they found higher (eg, left parieto-occipital cortices) and lower (eg, thalamus) connectivity in those with AN compared to controls; decrease in fractional anisotropy; and alterations in axial and radial diffusivities, the left fornix crus, anterior limb of the internal capsule (ALIC), right anterior cingulum, and left inferior fronto-occipital fasciculus. In addition, they observed correlations between dMRI metrics and clinical assessments, such as low presurgical left fornix and right ALIC fractional anisotropy being related to post-DBS improvements in quality of life and depressive symptoms, respectively. The study revealed differences between SCC connectivity in AN compared to healthy controls. The authors suggested that differences in dMRI metrics along affect-related tracts may point to widespread structural abnormalities in AN.
Lipsman et al22 developed a prospective trial of SCC DBS in six patients with chronic, severe, and treatment-refractory AN. Patients were followed up for 9 months after DBS activation. After 9 months, three of the six patients had achieved and maintained a body mass index (BMI) greater than their historical baselines. In four patients, DBS was associated with improvements in mood, anxiety, affective regulation, and AN-related obsessions and compulsions. Three patients showed improvements in quality of life after 6 months of DBS. In addition, clinical benefits were associated with changes in cerebral glucose metabolism (PET scans at baseline and 6 months) that were consistent with a reversal of the abnormalities seen in the anterior cingulate, insula, and parietal lobe. The authors observed several adverse events such as pain, nausea, QT prolongation, air embolus, seizure, panic attack during surgery, and worsening mood. They also concluded that DBS might be able to change the natural history of AN, with the potential to improve clinical outcomes in some patients.
With respect to obesity, in the study by Whiting et al,23 DBS of the lateral hypothalamic area (LHA) was used (2.5 years of stimulation), considering DBS as a potential treatment for intractable obesity. This study included three patients with intractable obesity (including failed bariatric surgery). These patients underwent bilateral implantation of LHA-DBS electrodes. In this case, no severe adverse effects were detected, and promising weight loss trends were observed when monopolar DBS stimulation applied via specific contacts found to increase the resting metabolic rate measured in a respiratory chamber. Across a wide spectrum of psychological and eating/weight-related measures, LHA DBS did not appear to create negative effects (anxiety/tension, depression, cognitive dysfunction, emotional lability, and guardedness; binge eating episodes; cognitive restraint; hunger; body shape concerns; and quality of life).
tDCS
A total of six studies were considered, including patients with obesity, overweight, BN, and frequent food craving (n=138). No cases of AN were found in tDCS trials. All studies applied tDCS to DLPFC. The prefrontal cortex (PFC) and the dorsolateral sectors, in particular, play an important role in the organization and planning of behavior. It is possible that dysregulation of the left DLPFC in obesity and other eating disturbances might impair goal-oriented regulation of eating behavior and food choice, implicating that this region as a potential target for interventions.
Considering obesity, Gluck et al24 compared anodal/sham vs cathodal/sham tDCS (a total of six sessions: 2 mA, 40 minutes) aimed to the left DLPFC (LDLPFC). As a result, participants tended to consume fewer kcal/d, significantly fewer kcal from soda and fat, and had a greater % weight loss during anodal vs cathodal tDCS. With respect to side effects, the following were reported: scalp burn, tingling, skin redness, sleepiness, trouble concentrating, and mood change. The active group had a higher incidence of skin redness compared to the sham group. This study supported that tDCS as a useful tool for potentially modifying the activity of the PFC and decreasing food intake.
Another study based on tDCS in obesity was developed by Grundeis et al,25 with a sample of 25 females. In this case, anodal, cathodal, and sham tDCS to the LDLPFC and contralateral frontal operculum were applied by means of single session. The authors hypothesized that tDCS would improve the ability to regulate the desire for visually presented foods and thereby reducing their consumption. All participants tolerated tDCS well. Reported side effects such as headache, dizziness, or burning sensations were only temporary and did not lead to premature discontinuation of the sessions. The findings of this study did not confirm an effect of tDCS, either on regulating/admitting the desire for foods or on calorie consumption.
Other studies based on tDCS have been focused on BN and frequent food craving. Kekic et al26 studied 39 bulimic patients by means of tDCS to the left/right DLPFC. In a randomized and counterbalanced procedure, participants received anode right/cathode left (AR/CL), anode left/cathode right (AL/CR), and sham. With respect to AR/CL tDCS, reduced ED cognitions were observed when compared to AL/CR and sham tDCS. Both active conditions suppressed the self-reported urge to binge-eat and increased self-regulatory control during a temporal discounting (TD) task. Compared to sham stimulation, mood improved after AR/CL but not after AL/CR tDCS. Finally, the three tDCS sessions had comparable effects on the wanting/liking of food and on bulimic behaviors during the 24 hours after stimulation. All sessions were associated with low levels of discomfort.
Three main studies have focused their experiments on frequent food craving. Fregni et al27 analyzed, in a randomized sham-controlled cross-over study, the effect of sham and active tDCS (AL/CR and AR/CL) of the DLPFC. Participants were exposed to food and also watched a movie of food associated with strong craving. Desire for food consumption was evaluated by VAS and by measuring food consumption before and after treatment. In addition, visual attention to food was explored using an eye tracking system. After sham stimulation, exposure to real food or food-related movie increased craving, whereas after AL/CR tDCS, the food-related stimuli did not increase craving levels. Compared with sham stimulation, participants fixated food-related pictures less frequently after AR/CL tDCS and consumed less food after both active stimulation conditions. These changes were not related to mood changes after any type of tDCS treatment. The authors concluded that anodal tDCS of the DLPFC can suppress food craving. In another study, Kekic et al17 studied 17 females who reported frequent food cravings (≥1 per day, assessed by self-report questionnaire). The frequency of food craving and choice impulsivity (TD) were assessed. As a result, participants were exposed to food and a film of people eating, and food cravings and TD were assessed before and after active and sham stimulations. Craving for sweet but not savory foods was reduced following real tDCS. Participants who exhibited more reflective choice behavior were more susceptible to the anticraving effects of tDCS than those who displayed more impulsive choice behavior. No differences were seen in TD or food consumption after real vs sham tDCS. These findings supported the efficacy of tDCS in temporarily lowering food cravings and identification of the moderating role of TD behavior. The study by Ljubisavljevic et al28 aimed to evaluate the utility of repeated tDCS of the right DLPFC cortex in changing food craving in young, healthy adults, and these changes may differ between normal and overweight participants. Participants were randomized into an “active” (5 days of real tDCS; 20 minutes, AR/CL montage, 2 mA with current density kept at 0.06 mA/cm2, 1 minute ramp-up/ramp-down) and a “sham” group (1 day of real tDCS, on the first day – same parameters – followed by 4 days of sham tDCS). Food craving was assessed by the means of state/trait food craving questionnaires. The authors confirmed earlier findings showing that single session of tDCS had immediate effects in reducing food craving. Results also showed that repeated tDCS over the right DLPFC might increase the duration of its effects, which might be present 30 days after the stimulation.
TMS
A total of 11 studies published between 2008 and 2017 were included. In these studies, 399 participants suffering from AN, BN, binge eating disorder (BED), eating disorders not otherwise specified (EDNOS), and obesity were studies. In nine of these studies, repetitive TMS (rTMS) was applied to the left DLPFC, whereas in one study, the authors used rTMS targeting the dorsomedial prefrontal cortex (DMPFC).
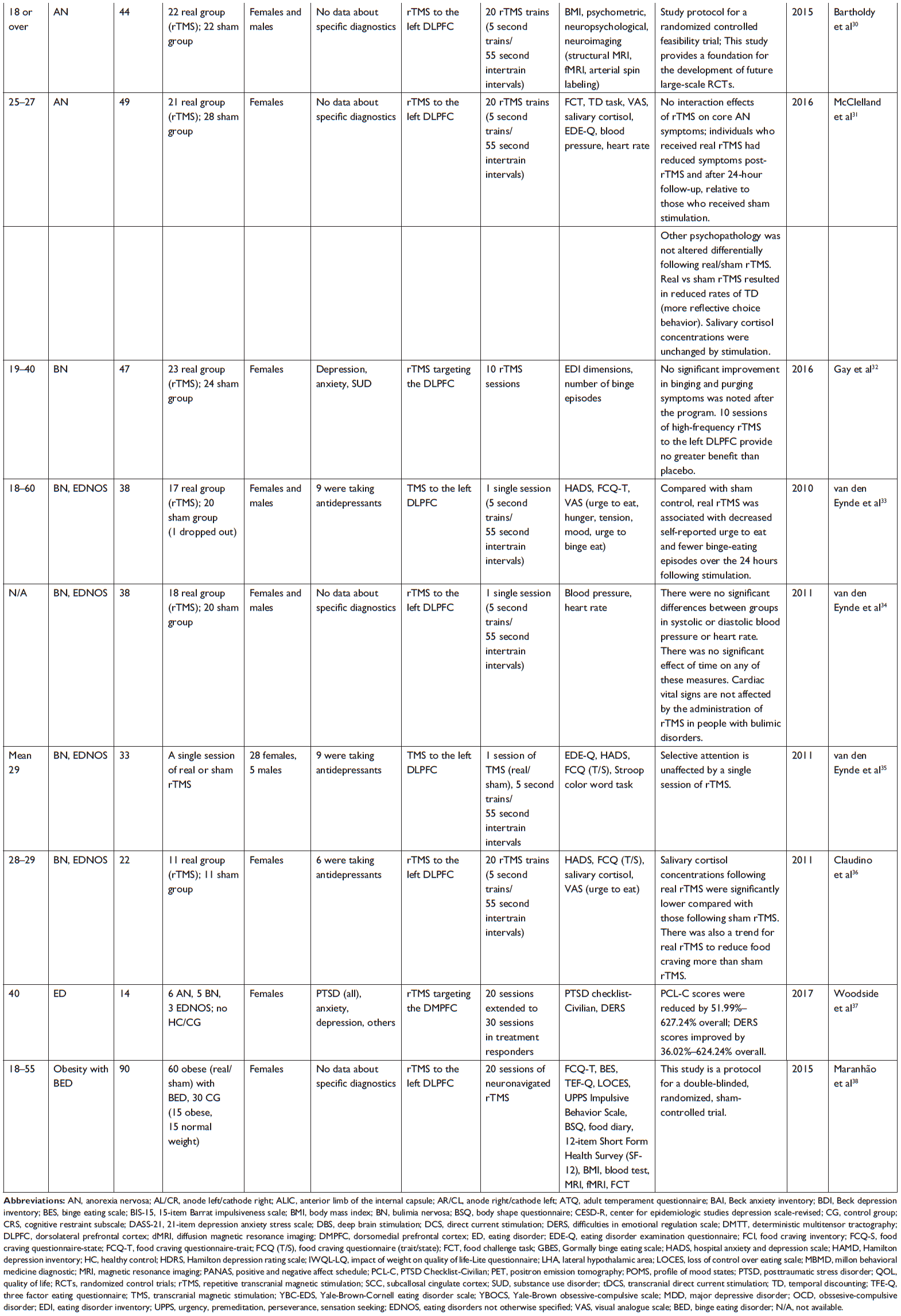
Considering AN, we found three studies based on the rTMS to the left DLPFC.29–31 In the first study, after applying 20 rTMS trains, when compared to pre-rTMS, post-rTMS sensations of feeling fat and feeling full were decreased. There was also a significant decrease in anxiety.29 There were no changes in mood, tension, or hunger. A food challenge task resulted in an increase in the urge to restrict and the sensation of feeling full. The authors concluded that rTMS appeared to be a safe and well-accepted brain modulation technique that might have an effect on core symptoms of AN such as feelings of fullness and fatness and anxiety. In the second study, a “study protocol” for a randomized controlled feasibility trial provided a foundation for the development of future large-scale RCTs.30 The study also proposed to include patients with an illness duration >3 years and a previous course of unsuccessful treatment who would receive 20 sessions of either real or sham rTMS. Due to its rigorous methodology, it is worth to include in this revision. In the third study,31 rTMS to the left DLPFC was applied in 49 patients. A food exposure task was administered before and after the procedure to elicit AN-related symptoms. Individuals who received real rTMS had reduced symptoms post-rTMS and at 24-hour follow-up, relative to those who received sham stimulation. In addition, real vs sham rTMS resulted in reduced rates of TD (more reflective choice behavior). Other psychopathology was not altered differentially following real/sham rTMS, and salivary cortisol concentrations were unchanged by stimulation. With respect to possible adverse effects, rTMS was safe, well tolerated, and considered an acceptable intervention.
With respect to BN, the study by Walpoth et al16 (2008) aimed to assess changes in binges and purges as well as in depressive and obsessive symptoms. Stimulation (to left DLPFC) was delivered for 3 weeks (3× for 5 days) with an intensity of 120% motor threshold using 20 Hz, in one session a day. Ten trains of 10 seconds, with a train interval of 60 seconds, were performed per session. To exclude patients highly responsive to placebo, all patients were first underwent a 1-week sham treatment. The authors reported that the average number of binges per day declined significantly between baseline and end of treatment in the two groups. There was no significant difference between sham and active stimulation in terms of purge behavior, depressive, and obsessive symptoms over time. Gay et al32 obtained similar results and they reported that 10 sessions of high-frequency rTMS to the left DLPFC provided no greater benefit than placebo. In this study, a total of 47 patients were included, and no significant results were reported considering binge and vomiting episodes, specific variables of ED-related problems, and other psychopathological variables.
Along with BN, other studies have included patients with EDNOS, including three studies by van den Eynde et al.33–35 The first by van den Eynde et al33 included a total of 37 patients (20 BN and 17 EDNOS) who received one session of real (n=17) or sham rTMS (n=20) to the left DLPFC. In this case, the authors reported that compared with sham control, real rTMS was associated with decreased self-reported urge to eat and fewer binge-eating episodes over the 24 hours following stimulation. In the second study, 38 patients were included to investigate cardiac safety of rTMS (to left DLPFC) in people with BN or EDNOS.34 Cardiac vital signs were not affected by the administration of rTMS. In addition, there was no significant change in blood pressure or heart rate over time in either the real or sham rTMS condition. Finally, the third study included 33 patients with BN (n=16) and EDNOS (n=17).35 They received a single session of high-frequency (10 Hz) rTMS (real or sham) to the left DLPFC. In this study, a cognitive measure (Stroop color word task) was used to evaluate the effect of rTMS. The authors did not detect a difference between a single session of real and sham rTMS on the “interference score”, so rTMS had no immediate negative effect on selective attention, and no beneficial effect on performance of the Stroop task was observed. To explain these findings, the authors state that in contrast with the other outcome measures (food cravings and salivary cortisol concentrations) that showed significant effects of rTMS, the Stroop task was performed prior to the exposure to high-calorie foods. In this regard, it is possible that administering the Stroop task after the stressful event of exposure to food would have affected the results. The study Claudino et al36 included patients with BN (n=14) and EDNOS (n=8). They aimed to explore the effect of one session of real high-frequency rTMS applied to the left DLPFC on food craving. Salivary cortisol concentrations following real rTMS were significantly lower compared with those following sham rTMS. In this study, there was also a trend for real rTMS to reduce food craving more than sham rTMS. The authors concluded that rTMS applied to the left DLPFC might alter hypothalamic–pituitary–adrenal axis activity in people with a bulimic disorder.
In other study, patients with AN (restrictive and binge-purge subtypes), BN, and EDNOS were included.37 In this study, 20–30 sessions of rTMS were applied to the bilateral DMPFC, and all patients suffered from posttraumatic stress disorder (PTSD). Improvements in emotional regulation (emotional dysregulation is a central symptom in PTSD) accompanied improvements in PTSD symptoms. The authors highlighted that DMPFC is involved in aspects of emotion regulation and the inhibition of prepotent responses. In addition, the DMPFC is abnormally activated in PTSD patients during emotion regulation and appraisal, and PTSD-related emotion regulation deficits are related to altered connectivity of the medial PFC to the amygdala. The therapeutic effects of rTMS on the DMPFC elicit changes through that circuitry.
Finally, Maranhão et al38 published a protocol to explore the effects of rTMS to the left DLPFC in patients with obesity and BED. As noted above, with respect to a protocol by Bartholdy et al,30 due to the rigorous methodology, this study is worth to be included in this revision.
Some relevant characteristics of these studies
Participants included in the abovementioned studies considered an age range from 18 to 60 years. Only 45.83% of females were included. With respect to comorbidity, 16.66% of these studies included patients suffering from different mental disorders apart from specific EDs. In other cases, no specific psychopathology was detailed, but some of participants took antidepressants (12.5%). Some of these studies did not include a control group (16.66%). Generally, the authors compared the effect of real vs sham applications of neuromodulation techniques. The total number of sessions ranged between 1 and 30.
As it was mentioned, patients with all types of ED and overweight and obesity have been included to treat them using different techniques of neuromodulation. In some cases, patients suffered from refractory AN15 or intractable obesity (failed bariatric surgery),23 suffered from PTSD,36 were considered chronic or with treatment resistance,22 (eg, without improvement under SSRI treatment),32 and showed a wide range of BMI.31 Healthy obese participants24,25 or healthy individuals who reported frequent food cravings17,27,28 took part in the studies, and sometimes the illness duration showed a very wide range (eg, 4–528 months).26
In most of the included studies, the authors obtained some positive results, despite three studies reporting no significant improvement in binging and purging symptoms,32 no effects either on the ability to modulate the desire for visually presented foods or on calorie consumption,25 and no effects on selective attention after applying TMS.35
With respect to security of neuromodulation, the specific study by van den Eynde et al showed that there were no significant differences between groups in systolic or diastolic blood pressure or heart rate. In addition, there was no significant effect of time on any of these measures, and cardiac vital signs were not affected by the administration of TMS.34
Discussion
AN has been associated with brain changes such as reduced gray matter in fronto-limbic-striatal areas.39,40 Functional neuroimaging studies have suggested an overrepresentation of limbic drives (eg, from the insula and amygdala), together with the altered prefrontal activity.41 Alterations in dopamine, serotonin, and brain-derived neurotrophic factor (BDNF) have also been found in systems that have been implicated in reward processing, mood, and symptom plasticity among others.42,43 In this regard, a disease model for AN has suggested altered interactions between “bottom-up” limbic drives (eg, reward and emotional processing) and “top-down” frontal lobe-mediated cognitive control.44–51 Specifically, hypoactivity of PFC regions during response inhibition and set-shifting tasks has been reported in AN.52–54 Reduced activity in the PFC might contribute to symptoms related to both impaired inhibitory control (ie, binge eating and purging) and poor cognitive flexibility (eg, compulsions such as body checking, exercising, and the obsessive concerns with eating, weight, and shape). The DLPFC has a key role in such self-regulatory control mechanisms and is a common target for neuromodulatory interventions in disorders of frontolimbic dysregulation.31
Functional imaging techniques, such as SPECT and PET, indicate left frontal cerebral hypometabolism in both depressive and bulimic patients. These changes of activity in the frontal area might be critical for eating control.55,56 There are also evidences that food craving is associated with DLPFC activity, and previous studies have found that the capacity for self-control depends on DLPFC activity levels. DLPFC is a part of the dorsal cognitive frontostriatal circuitry (representing the major neural structure involved in executive functions, including self-regulatory control) and is also implicated in reward processing due to its anatomical/functional connections with ventral limbic circuitry. Given the etiological relevance of these neurocognitive capacities in BN, manipulating the DLPFC might alleviate symptoms of the disorder.33,57
Apart from the role of DLPFC in both AN and BN, DMPFC seems to be more closely associated with emotional and behavioral self-control. In addition, the use of TMS on DMPFC has reported beneficial effects in major depression, binge eating and purging, and obsessive-compulsive disorder.58,59
Overall, there appear to be abnormalities in the use of cognitive reappraisal strategies, and brain systems that implement them contribute to disorders of eating behavior, including AN, BN, BED, obesity, and addiction. Across these disorders, there is often dysfunction in two major brain systems that also have key roles in cognitive reappraisal: one involving hypersensitivity to rewarding cues (eg, ventral striatum, amygdala, anterior insula, ventromedial prefrontal cortex [VMPFC], including orbitofrontal cortex) and the other involving deficient cognitive control over food or other substance use (eg, anterior cingulate, lateral prefrontal cortex [LPFC], including DLPFC).60–62
Considering structural imaging, ED patients show reductions in gray matter volume in regions involved in reward, impulse control, and emotion regulation: the caudate nucleus, ventral striatum, anterior cingulate, and orbitofrontal cortex. Functional imaging reveals abnormal patterns of resting-state connectivity in the default-mode network and other intrinsic brain networks incorporating the anterior cingulate and insula. ED patients also show abnormal ventral striatum activation in response to rewarding and aversive stimuli. Patients with BN usually show hyperactivity in medial frontal lobe regions during inhibition of prepotent actions and hypoactivity in response to food cues.63
Efficacy of neuromodulation in the treatment of different psychiatric disorders suggests that such techniques might be consider as another treatment tool in ED, especially in the context of modest success associated with current interventions.14 As stated by Van den Eynde et al,14 it is more appropriate to use the term neuromodulation than brain stimulation (thus referring not only to stimulation but also to inhibition or slow-downing brain functioning).
We have focused this review on an invasive technique (DBS) and two noninvasive procedures (tDCS and TMS). DBS aims to modulate the activity of dysfunctional brain circuits, and it has been used in different pathologies. DBS is an invasive but nonlesional procedure that exerts its effect both locally and remotely, across monosynaptically and polysynaptically linked networks.64,65 Generally, noninvasive techniques are feasible and acceptable as a treatment. These noninvasive procedures (eg, TMS and tDCS) avoid surgical interventions and base their action on magnetic fields that, after penetrating the skull, act on the brain. In 10 of 11 studies analyzed, which applied TMS, the technique was rTMS. In this case, magnetic fields are repeatedly applied, and this results in stimulation (high frequency, >1 Hz) or inhibition (low frequency, ≤1 Hz) of the underlying cortex. Most of the studies included in this review compared sham vs real rTMS. In the most common method for sham stimulation, the magnetic field is directed away from the brain.14,66 Generally, the period covered for this treatment ranged 1–30 sessions (the most common general period was 2–6 consecutive weeks; five sessions per week), and each session usually took 30–90 minutes.
In the studies by Hayes et al15 and Lipsman et al,22 based on DBS, SCC white matter was the chosen target given its role in affective regulation, its anatomic and physiologic links to relevant emotion and reward processing, and its relationship with abnormal serotonin receptor binding in ED patients. In addition, SCC is a widely connected hub containing appetitive- and aversive-responsive cells projecting to AN-affected regions, such as areas of the prefrontal, parietal and temporal cortices, insula, striatum, and amygdala. In the study by Whiting et al,23 the technique was applied to three patients with intractable obesity, and bilateral electrodes were implanted in the LHA. When this so-called feeding center is lesioned or stimulated (eg, by means of high frequency electrical stimulation), both decreasing food intake and weight loss are observed. In this regard, it has been hypothesized that the hypothalamic nucleus might provide a target for modulating human energy balance in cases of refractory obesity.67
Only a total of 14 AN and three obese patients have been included in clinical studies based on DBS. Patients were heterogeneous, with different comorbidities and medications. In this regard, effects of DBS might be promising, but more studies are required.
Direct current stimulation (DCS) has been used in seven controlled studies. In these cases, DLPFC is the target due to the fact that food craving (as well as drug craving) is linked mostly with the left, right, or bilateral DLPFC (area in the PFC important for executive functioning), which is activated in response to cues that induce both food and drug cravings.68 The studies based on DCS have included 138 patients with overweight and obesity, BN, and frequent food craving. Therefore, a deficiency in the prefrontal cortical inhibitory networks might contribute to the pathophysiology of disordered eating. The mechanisms by which DLPFC stimulation decreases cravings are unknown, although data suggest that reduced function in the right PFC may lead to overeating. It must be noted that noninvasive techniques of brain stimulation seem to suppress cravings even when the right DLPFC is inhibited and/or the left DLPFC is excited.17,69 Generally, these studies have found a reduction in the calorie intake per day, mood improvements, a reduction in ED cognitions, and a reduction in food craving. Nevertheless, the study by Grundeis et al25 does not support the notion of prefrontal/frontal DCS as a promising treatment option for obesity. Controversial findings due to methodological differences deserve more research in this field. In addition, the discrepancy between the study by Grundeis et al25 and other more positive findings24 demands further studies, for example, combining repetitive DCS instead of just one single session. In this regard, Ljubisavljevic et al, using repeated tDCS, reduced craving even 30 days after the intervention.28 In this case, although based on a small sample size, the results strengthen the use of tDCS as an adjuvant intervention for overweight and obesity.
With respect to TMS, studies have included 90 patients with obesity and binge EDs, 206 patients with BN and EDNOS, and 49 AN patients. Again, DLPFC was the target. Therefore, reduced activity in the PFC might contribute to AN symptoms related to both impaired inhibitory control (ie, binge eating and purging) and poor cognitive flexibility (eg, compulsions such as body checking, exercising, and the obsessive pre-occupation with eating, weight and shape).31 The DLPFC seems to have a key role in such self-regulatory control mechanisms and has been a common target for neuromodulatory interventions in disorders of frontolimbic dysregulation (depression, addictions, etc.). The psychophysiological mechanisms explaining the effects of rTMS in AN remain unclear. The DLPFC is involved in 1) emotion regulation, so that rTMS could improve maladaptive emotion regulation strategies in AN (ie, dietary restraint); 2) changes in synaptic plasticity, which is in accordance with reported increases in BDNF, modulation of extrastriatal dopamine, and bilateral DLPFC levels of 5-hydroxytryptamine (5-HT) after rTMS. These neural substrates have been implicated in the etiopathogenesis of AN. Furthermore, high-frequency rTMS to the DLPFC might remediate hypoactivity within prefrontal brain regions that has been associated with poor inhibitory control and impaired cognitive flexibility in AN.53,54,70–77 Considering safety, tolerability, and acceptability, overall TMS could be considered an appropriate tool. In fact, 90% of people who had received real rTMS considered that if rTMS proved to be efficacious in treating AN, they would consider having it as a treatment (ie, 20 daily sessions).31
The use of TMS in bulimic symptoms is based on the fact that BN patients display aberrant patterns of PFC activity during a wide range of experimental tasks, and BN patients are assumed to have an addictive component.78 In this regard, it is possible that rTMS of the DLPFC could reduce overeating behaviors by reducing food cravings and by improving cognitive control.32
Generally, studies have found some different improvements by means of TMS. Nevertheless, the study by Gay et al concluded that, despite being well tolerated, no significant improvement in binging and purging symptoms was noted after 10 sessions of high-frequency rTMS to the left DLPFC.32 They proposed that future studies should consider methodological issues and alternative targets.
Despite methodological differences, small sample sizes (more than 50% of studies included less than 30 patients), and controversial results, neuromodulation seems to be a promising therapeutical approach in ED and obesity. Future studies should consider that above and beyond a specific diagnosis, other factors are relevant methodologically: medications taken, disease severity, comorbidity, evolution, history of previous treatments (and types of them), etc. Overall, craving has been reported to be reduced in several studies17,27,28,36 as well as the urge to eat and binge episodes.16,26,33 In addition, reduction in calorie intake and higher percentage of weight loss have been reported.24 As a controversial result, Gay et al reported no significant improvement in binging and purging symptoms after rTMS. They suggested that 10 sessions of high-frequency rTMS to the left DLPFC provided no greater benefit.32 In this regard, the number of sessions could be a relevant factor to be considered when applying neuromodulation techniques.
With respect to AN, core symptoms of this disorder and a decrease in fat-feeling and full-filling sensations have been observed in several neuromodulation studies.29,31 It is relevant that, in refractory AN, improvements in different psychological variables and quality of life have been shown. These findings undoubtedly highlight the promising role of neuromodulation in ED.22
Generally, patients who have been treated using DBS, tDCS, and TMS are heterogeneous with respect to symptoms and other aspects mentioned above. Often, different phases of disease (acute vs chronic) may be found, and results do not reveal a consistent pattern between structural alterations and behavior as it has been previously noted.15
ED and obesity are complex conditions that are difficult to treat given the underlying interplay between body homeostasis, reward pathways, and affective/limbic circuitry. DBS offers a way to treat these patients despite some aspects that need to be refined (eg, exact stimulation parameters, brain targets, patient selection, timing and precise indications).79 Overall, DBS seems to be a good option in patients with chronic, treatment-refractory AN.22 Noninvasive techniques are another promising way of treatment. Both tDCS and TMS show an excellent safety-feasibility profile and lack of severe side effects.79 Some authors state that tDCS has several practical advantages over TMS: it is portable, inexpensive, has a more safety-feasibility profile, and can be applied bilaterally.17 Clinically, the findings by Fregni et al27 extend the results of previous studies using TMS to inhibit craving as it suggests that excitability enhancing strategies of brain stimulation of the right hemisphere might be more effective in reducing food craving.
Despite not being “real” trials, two studies that were included in the current revision are a protocol for this field of study. Thus, the study by Bartholdy et al30 is a protocol, which includes a) a diagnosis based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria; b) an illness duration >3 years and a previous course of unsuccessful treatment; c) a range of outcome variables (BMI, ED psychopathology, other psychopathology [eg, depression, anxiety], quality of life, neuropsychological processes [eg, self-regulation, attentional bias, and food choice behavior], neuroimaging measures [changes in brain structure or function], tolerability and acceptability of rTMS, and additional service utilization). The same protocol considers that acceptability and tolerability of the treatment would be assessed by means of semistructured interviews. Finally, feasibility would be evaluated through assessment of recruitment and retention rates, acceptability of random allocation, blinding success (allocation concealment), completion of treatment sessions, and research assessments (baseline, posttreatment, and follow-up assessments). A relevant point of this protocol refers to the use of sham (placebo) vs real (active) high-frequency rTMS to the left DLPFC. The authors highlight the fact that no sham-controlled randomized control trials of therapeutic rTMS in AN have been conducted.30 The use of sham stimulation deserves some comments. Generally, sham stimulation approaches serve multiple purposes in neuromodulation research; they are used as both placebo and to control sensory side effects of neuromodulation. It must be noted that the concept of controlled conditions in neuromodulation research is not restricted to placebo and control of sensory side effects. In the light of this view, sham stimulation is limited, and its use has to be carefully balanced with other methodological considerations.80
The second study protocol aimed to be applied in patients with BED.38 Inclusion criteria for patients were as follows: 1) meeting DSM-5 criteria for BED; 2) age ranging from 18 to 55; 3) right-handed and able to write, read, and understand all elements of the study; 4) females; 5) BMI ≥35 kg/m2 and body weight ≤150 kg; and 6) laboratory blood tests within normal range at study enrollment. In this case, the current use of psychotropic drugs (except for antidepressants on a stable dose for at least 1 month), the current use of any antiobesity drug and medications that are known to reduce weight, and major psychiatric disorder requiring immediate treatment (eg, schizophrenia, bipolar disorder), substance dependence, and individuals currently receiving any psychological therapy for ED were exclusion criteria. With respect to outcome measures, primary (changes in binge eating episodes and urge to eat) and secondary (specific for BED and others such as impulsivity, depression, anxiety, and body shape) measures were considered along with anthropometric measures, several biomarkers, a cognitive evaluation, and neuroimaging. Finally, tolerability would be based on the number of adverse events reported and number of dropouts due to adverse events or other reasons. Safety would be measured based on the occurrence of serious adverse events such as seizures. The relevance of this protocol lies on the study of the rTMS effects on ED-related psychopathology linked to binge eating and craving. By using rTMS as a research tool, the authors extend the investigation of the examination of patterns of comorbidity, neurobiological, and neuropsychological underpinnings and of potential biomarkers.
Neuromodulation in ED seems to have clinical potentials and therefore constitutes a promising area for further research. Developments in neuromodulation in ED will be linked to neuroimaging to identify potential stimulation targets and possible biomarkers of treatment response. To date, TMS and/or DCS are not the first-line treatment but perhaps will be. In the future, smaller sample sizes and very different methodologies should be avoided. Neuromodulation techniques are in the experimental phase, and they are not an evidence-based treatment for ED.14
Abbreviations
AL/CR, anode left/cathode right; ALIC, anterior limb of the internal capsule; AN, anorexia nervosa; AR/CL, anode right/cathode left; ATQ, adult temperament questionnaire; BAI, Beck anxiety inventory; BDI, Beck depression inventory; BES, binge eating scale; BIS-15, 15-item Barrat impulsiveness scale; BMI, body mass index; BN, bulimia nervosa; BSQ, body shape questionnaire; CESD-R, center for epidemiologic studies depression scale-revised; CG, control group; CRS, cognitive restraint subscale; DBS, deep brain stimulation; DASS-21, 21-item depression anxiety stress scale; DERS, difficulties in emotional regulation scale; DMPFC, dorsomedial prefrontal cortex; dMRI, diffusion magnetic resonance imaging; DMTT, deterministic multitensor tractography; ED, eating disorder; EDE-Q, eating disorder examination questionnaire; EDNOS, eating disorders not otherwise specified; FCI, food craving inventory; FCQ-S, food craving questionnaire-state; FCQ-T, food craving questionnaire-trait; FCQ (T/S), food craving questionnaire (trait/state); FCT, food challenge task; GBES, Gormally binge eating scale; HADS, hospital anxiety and depression scale; HAMD, Hamilton depression inventory; HC, healthy control; HDRS, Hamilton depression rating scale; IWQL-LQ, impact of weight on quality of life-Lite questionnaire; LHA, lateral hypothalamic area; LOCES, loss of control over eating scale; MBMD, millon behavioral medicine diagnostic; MEDCQ-R, Mizes eating disorder cognition questionnaire-revised; PANAS, positive and negative affect schedule; PCL-C, PTSD Checklist-Civilian; POMS, profile of mood states; PTSD, posttraumatic stress disorder; QOL, quality of life; RCTs, randomized control trials; rTMS, repetitive transcranial magnetic stimulation; SCC, subcallosal cingulate cortex; SUD, substance use disorder; TD, temporal discounting; TFE-Q, three factor eating questionnaire; YBC-EDS, Yale-Brown-Cornell eating disorder scale; YBOCS, Yale-Brown obsessive-compulsive scale.
Acknowledgments
We acknowledge the economic support of “Fundación APE” (Zaragoza, Spain) and the support of the staff of the Behavioral Sciences Institute (Seville, Spain) in the searching process. Special thanks to Carlos Peralta for his support from “Fundación APE”.
Author contributions
Both authors have contributed to conception and design, acquisition of data, analysis and interpretation of data, and have revised the content; in addition, they have approved the final version and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Stock VM, Knotkova H, Nitsche MA, Rasche D. Principles of neuromodulation. In: Notkhova H, Rasche D, editors. Textbook of Neuromodulation: Principles, Methods and Clinical Applications. New York: Springer; 2014:3–6. | ||
Benabid AL, Pollak P, Louveau A, Henry S, de Rougemont J. Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Appl Neurophysiol. 1987;50(1–6):344–346. | ||
De Pittà M, Brunel N, Volterra A. Astrocytes: Orchestrating synaptic plasticity? Neuroscience. 2016;323:43–61. | ||
Gómez-Fernández L. Cortical plasticity and restoration of neurologic functions: an update on this topic. Rev Neurol. 2000;31(8):749–756. | ||
Bayona-Prieto J, Bayona EA, Leon-Sarmiento FE, Neurorehabilitación. In: Uribe CS, Arana A, Lorenzana P, editors. Fundamentos de medicina. Medellin: CIB. 2010:745. | ||
Pascual-Leone A, Tormos-Muñoz JM. Transcranial magnetic stimulation: the foundation and potential of modulating specific neuronal networks. Rev Neurol. 2008;46(Suppl 1):S3–S10. | ||
López-Rojas J, Almaguer-Melián W, Bergado-Rosado JA. Synaptic tagging and memory trace. Rev Neurol. 2007;45(10):607–614. | ||
León-Sarmiento FE, Gómez A, Kimura J. Neurofisiologia Clinica. In: Toro J, Yepes M, Palacios E, editors. Neurologia. Mexico DF: Manual Moderno; 2010:683–701. | ||
Chen XL, Xiong YY, Xu GL, Liu XF. Deep Brain Stimulation. Interv Neurol. 2012;1(3–4):200–212. | ||
Thoden U, Doerr M, Dieckmann G, Krainick JU. Medial thalamic permanent electrodes for pain control in man: an electrophysiological and clinical study. Electroencephalogr Clin Neurophysiol. 1979;47(5):582–591. | ||
Dodick DW, Schembri CT, Helmuth M, Aurora SK. Transcranial magnetic stimulation for migraine: a safety review. Headache. 2010;50(7):1153–1163. | ||
Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol. 2000;527 Pt 3(3):633–639. | ||
Shiozawa P, Raza R, Cordeiro Q, et al. Clinical applications of neuromodulation in psychiatry. In: Notkhova H, Rasche D, editors. Textbook of Neuromodulation: Principles, Methods and Clinical Applications. New York: Springer; 2014:171–185. | ||
Van den Eynde F, Guillaume S. Neuromodulation techniques and eating disorders. Int J Eat Disord. 2013;46(5):447–450. | ||
Hayes DJ, Lipsman N, Chen DQ, et al. Subcallosal cingulate connectivity in anorexia nervosa patients differs from healthy controls: A multi-tensor tractography study. Brain Stimul. 2015;8(4):758–768. | ||
Walpoth M, Hoertnagl C, Mangweth-Matzek B, et al. Repetitive transcranial magnetic stimulation in bulimia nervosa: preliminary results of a single-centre, randomised, double-blind, sham-controlled trial in female outpatients. Psychother Psychosom. 2008;77(1):57–60. | ||
Kekic M, McClelland J, Campbell I, et al. The effects of prefrontal cortex transcranial direct current stimulation (tDCS) on food craving and temporal discounting in women with frequent food cravings. Appetite. 2014;78:55–62. | ||
Fagundo AB, de La Torre R, Jiménez-Murcia S, et al. Executive functions profile in extreme eating/weight conditions: from anorexia nervosa to obesity. PLoS One. 2012;7(8):e43382. | ||
Romijn AR, Rucklidge JJ. Systematic review of evidence to support the theory of psychobiotics. Nutr Rev. 2015;73(10):675–693. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. | ||
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12. | ||
Lipsman N, Woodside DB, Giacobbe P, et al. Subcallosal cingulate deep brain stimulation for treatment-refractory anorexia nervosa: a phase 1 pilot trial. Lancet. 2013;381(9875):1361–1370. | ||
Whiting DM, Tomycz ND, Bailes J, et al. Lateral hypothalamic area deep brain stimulation for refractory obesity: a pilot study with preliminary data on safety, body weight, and energy metabolism. J Neurosurg. 2013;119(1):56–63. | ||
Gluck ME, Alonso-Alonso M, Piaggi P, et al. Neuromodulation targeted to the prefrontal cortex induces changes in energy intake and weight loss in obesity. Obesity. 2015;23(11):2149–2156. | ||
Grundeis F, Brand C, Kumar S, Rullmann M, Mehnert J, Pleger B. Non-invasive prefrontal/frontal brain stimulation is not effective in modulating food reappraisal abilities or calorie consumption in obese females. Front Neurosci. 2017;11(11):334. | ||
Kekic M, McClelland J, Bartholdy S, et al. Single-session transcranial direct current stimulation temporarily improves symptoms, mood, and self-regulatory control in bulimia nervosa: A randomised controlled trial. PLoS One. 2017;12(1):e0167606. | ||
Fregni F, Orsati F, Pedrosa W, et al. Transcranial direct current stimulation of the prefrontal cortex modulates the desire for specific foods. Appetite. 2008;51(1):34–41. | ||
Ljubisavljevic M, Maxood K, Bjekic J, Oommen J, Nagelkerke N. Long-term effects of repeated prefrontal cortex transcranial direct current stimulation (tDCS) on food craving in normal and overweight young adults. Brain Stimul. 2016;9(6):826–833. | ||
Van den Eynde F, Guillaume S, Broadbent H, Campbell IC, Schmidt U. Repetitive transcranial magnetic stimulation in anorexia nervosa: a pilot study. Eur Psychiatry. 2013;28(2):98–101. | ||
Bartholdy S, McClelland J, Kekic M, et al. Clinical outcomes and neural correlates of 20 sessions of repetitive transcranial magnetic stimulation in severe and enduring anorexia nervosa (the TIARA study): study protocol for a randomised controlled feasibility trial. Trials. 2015;16(1):548. | ||
McClelland J, Kekic M, Bozhilova N, et al. A randomised controlled trial of neuronavigated repetitive transcranial magnetic stimulation (rTMS) in anorexia nervosa. PLoS One. 2016;11(3):e0148606. | ||
Gay A, Jaussent I, Sigaud T, et al. A Lack of clinical effect of high-frequency rTMS to dorsolateral prefrontal cortex on bulimic symptoms: A randomised, double-blind trial. Eur Eat Disord Rev. 2016;24(6):474–481. | ||
Van den Eynde F, Claudino AM, Mogg A, et al. Repetitive transcranial magnetic stimulation reduces cue-induced food craving in bulimic disorders. Biol Psychiatry. 2010;67(8):793–795. | ||
Van den Eynde F, Claudino AM, Campbell I, et al. Cardiac safety of repetitive transcranial magnetic stimulation in bulimic eating disorders. Brain Stimul. 2011;4(2):112–114. | ||
Van den Eynde F, Claudino AM, Campbell IC, Schmidt U. Immediate cognitive effects of repetitive Transcranial Magnetic Stimulation in eating disorders: a pilot study. Eat Weight Disord. 2011;16(1):45–48. | ||
Claudino AM, Van den Eynde F, Stahl D, et al. Repetitive transcranial magnetic stimulation reduces cortisol concentrations in bulimic disorders. Psychol Med. 2011;41(6):1329–1336. | ||
Woodside DB, Colton P, Lam E, et al. Dorsomedial prefrontal cortex repetitive transcranial magnetic stimulation treatment of posttraumatic stress disorder in eating disorders: An open-label case series. Int J Eat Disord. 2017;50(10):1231–1234. | ||
Maranhão MF, Estella NM, Cury ME, et al. The effects of repetitive transcranial magnetic stimulation in obese females with binge eating disorder: a protocol for a double-blinded, randomized, sham-controlled trial. BMC Psychiatry. 2015;15(1):194. | ||
Van den Eynde F, Suda M, Broadbent H, et al. Structural magnetic resonance imaging in eating disorders: a systematic review of voxel-based morphometry studies. Eur Eat Disord Rev. 2012;20(2):94–105. | ||
Titova OE, Hjorth OC, Schiöth HB, Brooks SJ. Anorexia nervosa is linked to reduced brain structure in reward and somatosensory regions: a meta-analysis of VBM studies. BMC Psychiatry. 2013;13(1):110. | ||
Zhu Y, Hu X, Wang J, et al. Processing of food, body and emotional stimuli in anorexia nervosa: a systematic review and meta-analysis of functional magnetic resonance imaging studies. Eur Eat Disord Rev. 2012;20(6):439–450. | ||
Phillipou A, Rossell SL, Castle DJ. The neurobiology of anorexia nervosa: a systematic review. Aust N Z J Psychiatry. 2014;48(2):128–152. | ||
Brandys MK, Kas MJ, van Elburg AA, Campbell IC, Adan RA. A meta-analysis of circulating BDNF concentrations in anorexia nervosa. World J Biol Psychiatry. 2011;12(6):444–454. | ||
Kaye WH, Fudge JL, Paulus M. New insights into symptoms and neurocircuit function of anorexia nervosa. Nat Rev Neurosci. 2009;10(8):573–584. | ||
Friederich HC, Wu M, Simon JJ, Herzog W. Neurocircuit function in eating disorders. Int J Eat Disord. 2013;46(5):425–432. | ||
Lipsman N, Woodside DB, Lozano AM. Neurocircuitry of limbic dysfunction in anorexia nervosa. Cortex. 2015;62:109–118. | ||
Marsh R, Maia TV, Peterson BS. Functional disturbances within frontostriatal circuits across multiple childhood psychopathologies. Am J Psychiatry. 2009;166(6):664–674. | ||
Park RJ, Godier LR, Cowdrey FA. Hungry for reward: How can neuroscience inform the development of treatment for Anorexia Nervosa? Behav Res Ther. 2014;62:47–59. | ||
Sanders N, Smeets PA, van Elburg AA, et al. Altered food-cue processing in chronically ill and recovered women with anorexia nervosa. Front Behav Neurosci. 2015;9(Pt 3):46. | ||
Brooks SJ, Rask-Andersen M, Benedict C. A debate on current eating disorder diagnoses in light of neurobiological findings: is it time for a spectrum model? BMC Psychiatry. 2012;12(1):76. | ||
O’Hara CB, Campbell IC, Schmidt U. A reward-centred model of anorexia nervosa: a focussed narrative review of the neurological and psychophysiological literature. Neurosci Biobehav Rev. 2015;52:131–152. | ||
Oberndorfer TA, Kaye WH, Simmons AN, Strigo IA, Matthews SC. Demand-specific alteration of medial prefrontal cortex response during an inhibition task in recovered anorexic women. Int J Eat Disord. 2011;44(1):1–8. | ||
Wierenga C, Bischoff-Grethe A, Melrose AJ, et al. Altered BOLD response during inhibitory and error processing in adolescents with anorexia nervosa. PLoS One. 2014;9(3):e92017. | ||
Sato Y, Saito N, Utsumi A, et al. Neural basis of impaired cognitive flexibility in patients with anorexia nervosa. PLoS One. 2013;8(5):e61108. | ||
Andreason PJ, Altemus M, Zametkin AJ, et al. Regional cerebral glucose metabolism in bulimia nervosa. Am J Psychiatry. 1992;149(11):1506–1513. | ||
Nozoe SI, Naruo T, Yonekura R, et al. Comparison of regional cerebral blood flow in patients with eating disorders. Brain Res Bull. 1995;36(3):251–255. | ||
Uher R, Yoganathan D, Mogg A, et al. Effect of left prefrontal repetitive transcranial magnetic stimulation on food craving. Biol Psychiatry. 2005;58(10):840–842. | ||
Slotema CW, Blom JD, Hoek HW, et al. Should we expand the toolbox of psychiatric treatment methods to include repetitive transcranial magnetic stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J Clin Psychiatry. 2010;71(7):873–884. | ||
Van den Eynde F, Broadbent H, Guillaume S, Claudino A, Campbell IC, Schmidt U. Handedness, repetitive transcranial magnetic stimulation and bulimic disorders. Eur Psychiatry. 2012;27(4):290–293. | ||
Kelley AE, Schiltz CA, Landry CF. Neural systems recruited by drug- and food-related cues: studies of gene activation in corticolimbic regions. Physiol Behav. 2005;86(1–2):11–14. | ||
Aldao A, Nolen-Hoeksema S. Specificity of cognitive emotion regulation strategies: a transdiagnostic examination. Behav Res Ther. 2010;48(10):974–983. | ||
Kaye WH, Wierenga CE, Bailer UF, et al. Does a shared neurobiology for foods and drugs of abuse contribute to extremes of food ingestion in anorexia and bulimia nervosa? Biol Psychiatry. 2013;73(9):836–842. | ||
Val-Laillet D, Aarts E, Weber B, et al. Neuroimaging and neuromodulation approaches to study eating behavior and prevent and treat eating disorders and obesity. Neuroimage Clin. 2015;8:1–31. | ||
Mayberg HS, Lozano AM, Voon V, et al. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45(5):651–660. | ||
Smith GS, Laxton AW, Tang-Wai DF, et al. Increased cerebral metabolism after 1 year of deep brain stimulation in Alzheimer disease. Arch Neurol. 2012;69(9):1141–1148. | ||
Mennemeier M, Triggs W, Chelette K, Woods A, Kimbrell T, Dornhoffer J. Sham transcranial magnetic stimulation using electrical stimulation of the scalp. Brain Stimul. 2009;2(3):168–173. | ||
Tomycz ND, Whiting DM, Oh MY. Deep brain stimulation for obesity – from theoretical foundations to designing the first human pilot study. Neurosurg Rev. 2012;35(1):37–43. | ||
Tang DW, Fellows LK, Small DM, Dagher A. Food and drug cues activate similar brain regions: a meta-analysis of functional MRI studies. Physiol Behav. 2012;106(3):317–324. | ||
Boggio PS, Sultani N, Fecteau S, et al. Prefrontal cortex modulation using transcranial DC stimulation reduces alcohol craving: a double-blind, sham-controlled study. Drug Alcohol Depend. 2008;92(1–3):55–60. | ||
Ochsner KN, Gross JJ. The neural architecture of emotion regulation. In: Gross JJ, editor. Handbook of Emotion Regulation. New York, NY: Guilford Press; 2007:87–109. | ||
Kaye W. Neurobiology of anorexia and bulimia nervosa. Physiol Behav. 2008;94(1):121–135. | ||
Gersner R, Kravetz E, Feil J, Pell G, Zangen A. Long-term effects of repetitive transcranial magnetic stimulation on markers for neuroplasticity: differential outcomes in anesthetized and awake animals. J Neurosci. 2011;31(20):7521–7526. | ||
Medina FJ, Túnez I. Mechanisms and pathways underlying the therapeutic effect of transcranial magnetic stimulation. Rev Neurosci. 2013;24(5):507–525. | ||
Ridding MC, Rothwell JC. Is there a future for therapeutic use of transcranial magnetic stimulation? Nat Rev Neurosci. 2007;8(7):559–567. | ||
Zanardini R, Gazzoli A, Ventriglia M, et al. Effect of repetitive transcranial magnetic stimulation on serum brain derived neurotrophic factor in drug resistant depressed patients. J Affect Disord. 2006;91(1):83–86. | ||
Cho SS, Strafella AP. rTMS of the left dorsolateral prefrontal cortex modulates dopamine release in the ipsilateral anterior cingulate cortex and orbitofrontal cortex. PLoS One. 2009;4(8):e6725. | ||
Baeken C, De Raedt R, Bossuyt A, et al. The impact of HF-rTMS treatment on serotonin(2A) receptors in unipolar melancholic depression. Brain Stimul. 2011;4(2):104–111. | ||
Hadad NA, Knackstedt LA. Addicted to palatable foods: comparing the neurobiology of Bulimia Nervosa to that of drug addiction. Psychopharmacology. 2014;231(9):1897–1912. | ||
Lee DJ, Elias GJB, Lozano AM. Neuromodulation for the treatment of eating disorders and obesity. Ther Adv Psychopharmacol. 2018;8(2):73–92. | ||
Duecker F, Sack AT. Rethinking the role of sham TMS. Front Psychol. 2015;6(210). |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.