")
Back to Journals » Journal of Healthcare Leadership » Volume 11
Network analysis of the structure of inter-professional knowledge exchange related to Electronic Health Record Medication Reconciliation within a Social Knowledge Networking system
Authors Rangachari P , Dellsperger KC , Rethemeyer RK
Received 4 April 2019
Accepted for publication 11 June 2019
Published 1 July 2019 Volume 2019:11 Pages 87—100
DOI https://doi.org/10.2147/JHL.S211109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
P Rangachari,1 KC Dellsperger,2 RK Rethemeyer3
1Department of Interdisciplinary Health Sciences, College of Allied Health Sciences, Augusta University, Augusta, GA 30912, USA; 2Cardiovascular Division, AU Health, Department of Medicine, Medical College of Georgia, Augusta University, Augusta, GA 30912, USA; 3Rockefeller College of Public Affairs and Policy, University at Albany, Albany, NY 12222, USA
Background: In fall 2016, a 2-year grant was secured to pilot a Social Knowledge Networking (SKN) system pertaining to Electronic Health Record (EHR) Medication Reconciliation (MedRec), to enable Augusta University Health System to progress from “limited use” of EHR MedRec technology, to “meaningful use” (MU). A total of 50 “SKN users” (practitioners), participated in discussing practice issues related to EHR MedRec, over a 1-year period. These discussions were moderated by five “SKN moderators” (senior administrators). The pilot study, completed in fall 2018, found that inter-professional knowledge exchanges on the SKN, enabled several collective learning (“aha”) moments to emerge. These learning dynamics in turn, were associated with distinct improvement trends in two measures of MU of EHR MedRec technology, identified for the study. A key takeaway was that an SKN could be a valuable tool in enabling MU of EHR MedRec technology.
Purpose: The study’s key findings related to the content and dynamics of inter-professional knowledge exchange on the SKN system, and their association with trends in measures of MU of EHR MedRec technology, have been described in a separate publication. This paper seeks to describe the structure of inter-professional knowledge exchange (or the pattern of connections) related to EHR MedRec, over the 1-year SKN period.
Methods: Social network analysis (SNA) techniques were used to describe the structure of inter-professional knowledge exchange on the SKN system.
Results: Results revealed that three of the five SKN moderators played a strong “collective brokerage” role in facilitating inter-professional knowledge exchange related to EHR MedRec, to enable learning and practice change. Together, they played complementary roles in reinforcing best-practice assertions, providing IT system education, and synthesizing collective learning moments, to enable “champions for change” to emerge from among SKN users.
Conclusion: Results provide insight into the structure of effective knowledge-sharing networks for enabling inter-professional learning and practice change in health care organizations.
Keywords: inter-professional learning, social network analysis, electronic health records, medication reconciliation, meaningful use, change implementation
Introduction
Patient safety advocates have long promoted the use of medication reconciliation to help prevent medication discrepancies and errors during transitions-of-care, eg, outpatient-to-inpatient-to-outpatient care transitions, for chronic disease patients on multiple medications. Medication reconciliation refers to the process of creating the most complete and accurate list of a patient’s current medications, comparing the list to those in the patient’s records, modifying the list as appropriate, and communicating the final up-to-date list to the patient, family, caregivers, and the next providers of care.1,2 Since 2005, “Medication Reconciliation” (MedRec) has been part of the Joint Commission’s hospital accreditation program, and more recently, it has become part of the Electronic Health Record (EHR) meaningful use (MU) requirements.3,4 Given the heightened risk of medication errors during transitions-of-care, the “MU” of EHR MedRec technology has potential to significantly improve quality and patient safety, reduce costs and health disparities, and engage patients/families in care delivery.
At a national level however, hospital adherence to MU of EHR MedRec technology has continued to lag; and studies in turn, have ascribed this trend to low physician engagement in EHR MedRec, emanating from an absence of shared understanding of 1) the responsibilities of each professional subgroup (eg, hospitalist vs community doctor) in managing a patient’s medication list, and 2) the value of MedRec as a clinical tool for promoting patient safety.5–10 Not surprisingly therefore, several recent studies have found that although federal vendors of EHR systems have been enhancing functionalities associated with MedRec over time, hospitals are continuing to use partially paper-based processes during care tranistions.11–13 In other words, there is “limited use” of EHR MedRec technology in hospitals and health systems across USA, as opposed to “MU”.14,15
In 2016, the Augusta University Health System, AU Health, a comprehensive health care system providing primary, specialty, and subspecialty care in Augusta, Georgia, faced challenges (similar to those described previously), with the use and implementation of its EHR MedRec system (which is powered by Cerner Inc., a federally certified EHR vendor). Although MedRec was often marked as “complete” before patient discharge from the hospital, by the press of a button on the EHR, the patient’s active medication list, was estimated by the AU Health leadership, to be inaccurate and incomplete, with numerous discrepancies between patient’s home and hospital medication lists, for a vast majority of discharged patients. These estimates emanated from a variety of sources, including medical record reviews to examine discrepancies in patients’ medication lists during care transitions, and anecdotal evidence from patients and providers, including frustrations expressed by patients and providers alike, in regard to inaccurate and incomplete medication lists. The Chief Medical Officer (CMO) and Chief Medical Information Officer (CMIO) who participated in this (Social Knowledge Networking [SKN]) study, were part of the AU Health Leadership team that developed these estimates, prior to this study.
Importantly, there was consensus among senior administrators at AU Health, that providers were not using the EHR MedRec system meaningfully, to communicate changes in the patient’s active medication list to the next provider of care and to patients/families. This problem was attributed to physicians’ reluctance to discontinue medications that they did not originally order from the patient’s active medication list, which in turn, led to both medication discrepancies during care transitions, and frustrations associated with inaccurate and incomplete medication lists among patients/families and providers of care, across the continuum. Therefore, AU Health faced a scenario that was reflective of national concerns related to use and implementation of EHR MedRec technology in hospitals and health systems, ie, low physician engagement, translating to limited use of EHR MedRec technology.
In fall 2016, Augusta University secured a 2-year grant from the Agency for Healthcare Research and Quality (AHRQ) to pilot an SKN system pertaining to EHR MedRec, to enable AU Health to progress from “limited use” of EHR MedRec Technology, to “MU”.16,17
The rationale for an SKN system, is that it could provide a platform for knowledge exchange on practice issues related to EHR MedRec, across diverse provider subgroups and care settings, to highlight adverse consequences of gaps in practice for patient safety (eg, not using the External Rx History function resulted in an error in recording patient’s dosage admission, which resulted in an adverse event). This, in turn, is expected to increase physician engagement in addressing issues related to EHR MedRec; and promote collective learning of best practices (eg, using the External Rx History function during each encounter, to generate the patient’s current medication list), to provide a foundation for practice change (improvement) ie, MU of EHR MedRec technology. The theoretical foundation for using an SKN system to facilitate provider engagement, inter-professional learning, and practice change, has been described in detail, in the earlier publication from this study, in the Journal of Healthcare Leadership.18 The following is a link to this open-access publication: https://doi.org/10.2147/JHL.S198951.
The essence of the theoretical framework, is that communication network structures rich in “brokerage” and “hierarchy” may be most effective for enabling engagement, collective learning, and change (improvement) in “professional complex systems”, ie, organizations exhibiting properties of both professional organizations and complex systems, like health care organizations (HCOs).20–28 To summarize, this theoretical framework suggests that an SKN system moderated by senior administrators, to engage provider subgroups in tacit knowledge exchange on practice issues (related to EHR MedRec), while also facilitating proactive, periodic, top-down communication on best practices related to EHR MedRec, can foster collective learning and practice change (eg, MU of EHR MedRec), in HCOs.
Purpose of this paper
The pilot-implementation of the SKN system on EHR MedRec, was successfully completed at AU Health, over a 1-year period, ie, April 1, 2017 to March 31, 2018 (Q2 2017 to Q1 2018). A total of 50 practitioners or “SKN users” (ie, physicians, nurses, and pharmacists based in outpatient and inpatient medicine settings at AU Health), participated in discussing practice issues pertaining to EHR MedRec, over the 1-year period. These discussions in turn, were moderated by five “SKN moderators” (senior administrators). Thematic (qualitative) analysis was used to understand dynamics of inter-professional knowledge exchange; while descriptive analysis was used to describe trends in two measures of MU of EHR MedRec, which were identified for the study, based on inter-professional discussions on the SKN system: 1) “Proportion of patient encounters with External Rx History import (Higher is Better)”, and 2) “Proportion of patients’ active medications that are missing documentation of Compliance Status (Lower is Better)”. The essential findings of this pilot study were that inter-professional knowledge exchange related to EHR MedRec on the SKN system, began with “problem statements” and then progressed to “problem solving statements (the how-to)”, followed by “IT system education (the what)”, and then to “best-practice assertions (the why)”, followed by “culture change assertions (the way-to)”, and “collective learning (aha) moments”, to provide a foundation for practice change (improvement). These inter-professional learning dynamics in turn, coincided with distinct improvement trends in both measures of MU of EHR MedRec technology, ie, an increasing trend in the first measure and a declining trend in the second measure. A key takeaway from this pilot study, was that an SKN system could be a valuable tool in enabling MU of EHR MedRec technology. An important gleaning was that the SKN enabled progress toward MU of EHR MedRec, by addressing implementation challenges in the correct sequence, ie, by facilitating collective learning of the value of best practices in EHR MedRec for patient safety (ie, the “big picture”), before IT training of providers to address socio-technical challenges of EHR implementation.
The key findings from this study related to the content and dynamics of inter-professional knowledge exchange and learning related to EHR MedRec (ie, “what” was discussed among practitioners over time on the SKN system), and the associations between these inter-professional learning dynamics and trends observed in the two measures of MU of EHR MedRec, over the 1-year SKN period, are described in detail in the earlier publication.18
- The aim of this paper, was to describe the structure of inter-professional knowledge exchange (or the patterns of connections among SKN participants) related to EHR MedRec, during the 1-year SKN period (ie, “who” spoke to whom), which in turn, provided a foundation for collective learning and practice change (ie, MU of EHR MedRec) at AU Health. It would be relevant to clarify at this juncture, that while the earlier publication focused on the “content” and “dynamics” of inter-professional knowledge exchange and learning related to EHR MedRec (ie, “what” was discussed among practitioners over time on the SKN system that in turn, contributed to collective learning), this paper focused on the “structure” of inter-professional knowledge exchange (or the patterns of connections among SKN participants) related to EHR MedRec, during the 1-year SKN period (ie, “who” spoke to whom on the SKN system).
An important purpose of this paper therefore, was to validate the theoretical framework (summarized earlier) related to the structure of effective knowledge sharing networks in professional complex systems like healthcare organizations (HCOs). The process of validating this framework in turn, helps gain insight into strategies for 1) the design of effective knowledge sharing networks; and 2) the role of select participants (senior administrators and provider champions), in enabling collective learning and practice change (improvement) in HCOs.
Methods
This paper used social network analysis (SNA), specifically, two-mode network analysis and ego-network analysis, to examine the structure of inter-professional knowledge exchange related to EHR MedRec, on the SKN system, over the 1-year pilot period.29,30 Key details related to the design of the SKN system and participant recruitment procedures, are provided in the following sections, prior to describing the methods associated with data collection and data analysis for this study.
Design of the SKN system
The key components of the SKN system piloted at AU Health are outlined in the following sections.
SKN reporting tool
The reporting tool was a form that was made available online. It allowed providers participating in the SKN system (SKN users) to report issues faced in clinical practice, related to EHR MedRec (eg, challenges in obtaining complete information for compiling the patient’s active medication list, at the time of admission). The form enabled SKN users to briefly describe the practice issue, and indicate the settings and patient conditions that the issue applied to.
SKN discussion tool (Yammer)
Microsoft Yammer was an online system that was independent of the SKN Reporting Tool. The purpose of Yammer was to facilitate moderated discussions on issues encountered in clinical practice related to EHR MedRec. Microsoft Yammer is considered to be a classic example of an “enterprise SKN system.” Our study used the basic version of Yammer (that was available to our enterprise as a component of the Office 365 package).
SKN lunch-and-learn sessions
A total of five SKN lunch-and-learn sessions were conducted over the 1-year pilot period. The purpose of these sessions was to enable SKN participants to meet in person and discuss highlights, gleanings, and takeaways, from the inter-professional knowledge on Yammer. All SKN participants received advance invitations to these lunch-and-learn sessions.
SKN periodic email updates
All SKN participants also received approximately 15 periodic progress email updates from the principal investigator (PI) during the course of the 1-year SKN period.
The SKN system had two types of participants.
SKN moderators
SKN moderators consisted of five senior administrators who played the crucial role of moderating discussions on issues encountered in clinical practice (related to EHR MedRec), among SKN users, during the 1-year period. The five SKN moderators included the CMO, two chief hospitalists, the CMIO, and the PI. SKN moderators’ main responsibility was to upload issues reported on the SKN Reporting Tool (pertaining to EHR MedRec), by SKN users, for discussion on Yammer, by all SKN users. Correspondingly, a majority of discussion threads on Yammer began with report of an issue (ie, statement of a problem) introduced by SKN moderators. SKN moderators were also expected to proactively initiate discussions on best practices related to EHR MedRec (eg, described in the literature), and bring key takeaways and learnings from Yammer, for discussion at ongoing meetings of the health system, including the Hospital Quality & Patient Safety Council.
SKN users
SKN users consisted of 50 practitioners (physicians, nurses, and pharmacists based in outpatient and inpatient medicine settings), who agreed to participate in the SKN system. SKN users’ main responsibilities were to: 1) report issues encountered in clinical practice related to EHR MedRec, via the SKN Reporting Tool, as often as possible; 2) participate in Yammer discussions (moderated by SKN moderators), over the 1-year period; and 3) share the key takeaways and learnings from their SKN participation, with colleagues in the health system. However, SKN users were prohibited from initiating new discussion threads directly on SKN Yammer. This particular capability was reserved only for SKN moderators, to enable coordination of issue discussions on the SKN system.
Participant recruitment
SKN participants were recruited after Institutional Review Board (IRB) approval for the project was obtained from Augusta University. All providers in three subgroups, ie, physicians, nurses, and pharmacists, based in five medicine service lines (inpatient and outpatient) at AU Health, including Cardiology, Hospitalist, Family Medicine, Internal Medicine, and Emergency Medicine service lines, were approached for recruitment using an informed consent process that was approved by the IRB. A total of 50 providers were recruited as SKN users, including 15 physicians, 20 pharmacists, and 15 nurses, from inpatient and outpatient medicine service lines. All physicians who agreed to participate from Internal Medicine, Cardiology, and Family Medicine, practiced in both inpatient and outpatient settings. Only Hospitalists exclusively practiced in the inpatient setting.
Written informed consent was obtained from all participants, prior to data collection. Individuals who agreed to participate, were requested to sign the following documents 1) Informed Consent, 2) Privacy and Confidentiality Agreement, which stressed that use of Protected Health Information on the SKN, was strictly prohibited; 3) Statement of Ethical and Professional Conduct on the SKN system; and lastly 4) Custom Usage Policy, clarifying that SKN users were prohibited from initiating discussion threads directly on Yammer. SKN users could only report issues through the SKN Reporting Tool and participate in threads launched by SKN moderators for the purpose of coordination, the ability to initiate discussion threads on Yammer would be restricted to SKN moderators. Following the signing of documents, SKN participants received a detailed orientation to the SKN system, including the process for accessing the Reporting Tool and Yammer, both of which were made available to participants through separate links on the EHR system. Both tools were also accessible through the enterprise web portal and through mobile devices; and Yammer was downloadable as an App.
Data collection
Inter-professional knowledge exchanges related to EHR MedRec on the SKN system
The primary source of data on inter-professional knowledge exchanges on the SKN, was Yammer, which included a record of all communications posted by SKN users, on various threads-of-discussion related to EHR MedRec, over the 1-year period. As described earlier, a majority of these threads-of-discussion in turn, stemmed from issues reported by SKN users via the SKN Reporting Tool, brought to Yammer for discussion by SKN moderators. All threads-of-discussion on Yammer, were open and available to all SKN users, without restriction. Yammer recorded the name, date, and time associated with each posting.
Data analysis
Social network analysis (SNA) of inter-professional knowledge exchanges
Of the 50 practitioners who signed up as SKN users, 25 were active users of SKN Yammer, with 12 or more posts over the 1-year SKN period. Active users of Yammer came from all professional subgroups and care settings represented on SKN, including eight physicians, nine nurses, and eight pharmacists. Additionally, three of the five SKN moderators (including the CMO, CMIO, and PI), each posted 40 or more messages on Yammer.
Over the 1-year SKN period there were a total of 485 posted communications on Yammer, divided into 62 threads-of-discussion. Of these, 45 threads had three or more posts; among which, 12 threads had ten or more posts; of which three threads had 25 or more posts, including one thread with 45 posts. There were a total of 32 issues related to EHR MedRec reported on the SKN Reporting Tool, over the 1-year period. Of the 45 threads with three or more posts, 32 began with issues reported on the SKN Reporting Tool, brought to Yammer by SKN moderators. As such, all reported issues were used to launch threads-of-discussion on Yammer.
Two types of SNA were used to describe the structure of inter-professional knowledge exchange related to EHR MedRec on the SKN system:
- Two-mode network analysis: the essential purpose of two-mode analysis is to understand the relationship between two separate sets of entities – here, “SKN participants” and “threads-of-discussion” – or the implicit relationship between individuals through their joint membership in a group or some other collective. For this study, two-mode analysis serves the particular purpose of examining the structure of participation across various threads-of-discussion, over the 1-year SKN period.
- Ego-network analysis: the essential purpose of ego-network analysis in this paper, was to describe the SKN participants and their characteristics, within each thread-of-discussion (the “ego” in this study), over the 1-year SKN period.
Results
Summary of key findings from the study
As mentioned in the Introduction, a key takeaway from this pilot study, was that an SKN system can be a valuable tool in enabling MU of EHR MedRec technology. As discussed in the Introduction, the content and dynamics of inter-professional knowledge exchange related to EHR MedRec on the SKN system, were examined using thematic analysis techniques. Broadly speaking, the thematic analysis process helped identify six repetitive themes across several threads-of-discussion, in the following chronological order: 1) problem statements; 2) problem-solving statements (“the how-to”); 3) IT system education (“the what”); 4) best-practice assertions (“the why”); 5) culture change assertions (“the way-to”); and 6) collective learning (“aha”) moments.
Over the 1-year period, there were two specific problem areas, ie, issues encountered in clinical practice related to EHR MedRec, for which inter-professional knowledge exchange progressed through the full spectrum of six themes from “problem statements” to “collective learning (aha) moments,” to lay a foundation for practice change (ie, MU of EHR MedRec). Both areas pertained to the broader theme of “improving communication across the continuum of providers,” to promote accuracy of the active medication list, during transitions-of-care. The two areas were 1) importing External Rx History during patient encounters, to improve accuracy of the patient’s medication history and current medication list to be used for reconciliation; and 2) ensuring documentation of “Compliance Status” for patients’ active medications, to facilitate discontinuation of appropriate medications from the list, during transitions-of-care.
The two threads of inter-professional knowledge exchange on the SKN system pertaining to these areas, ie, THREAD 1 and THREAD 2, respectively, in turn, provided a foundation for identifying two measures of MU of EHR MedRec, with MEASURE 1 being the “proportion of encounters with external Rx history import” (Higher is Better); and MEASURE 2 being the “proportion of patients’ total active medications that are missing documentation of compliance status” (Lower is Better). Data for both measures were obtained from the health system’s EHR for a period of 6 quarters, ie, Q1 2017 to Q2 2018, which translated to 1 quarter before SKN was launched, extending to 1 quarter after SKN implementation was concluded.
MEASURE 1 was defined as the aggregate proportion of patient encounters during which the external Rx history was imported before the inpatient or outpatient encounter ended. The “External Rx History Import” refers to the importation of the patient’s history of medications filled at their pharmacy. This history can be imported when the provider activates the External Rx History button on the EHR, which in turn would access an external (“Surescripts”) system to pull the patient’s Rx history. Data for MEASURE 1 were calculated quarterly for patient encounters, for 6 quarters, for each of the five medicine lines represented on the SKN. These data were then aggregated, to examine trends in the proportion of External Rx History Import. Since Cardiology was the only subspecialty of medicine on SKN, MEASURE 1 was restricted to patient encounters for a Cardiology-relevant chronic condition, ie, patients who had a primary or secondary diagnosis of congestive heart failure (CHF).
MEASURE 2 was defined as the aggregate proportion of patients’ active medications that are missing documentation of Compliance Status. It is essential for all active medications to have a documented (non-missing) Compliance Status, so that the next provider has information necessary to update the list accurately, before the following transition point. Data for MEASURE 2 were obtained quarterly, for 6 quarters, for all patients who had a primary or secondary diagnosis of CHF, and at least one encounter with any one of the five medicine service lines represented on the SKN, over the 6-quarter period. The aggregate proportion of missing documentation (of Compliance Status) was calculated quarterly, for all CHF patients with active medications reported, over a period of 6 quarters.
Both discussion threads began with problem statements reported by SKN users (frontline providers). For example, THREAD 1 began with a problem statement from an Emergency Department (ED) nurse in regard to the challenge of obtaining the correct medication history from the patient upon arrival, to formulate the current medication list, for reconciliation with new prescriptions. In response, an outpatient nurse put forth a problem-solving statement by suggesting use of “External Rx History Import,” a functionality within the EHR, for obtaining a current medication list for reconciliation. However, this suggestion was initially met with resistance from some of the providers. For example, the ED nurse argued that the External Rx History was not completely accurate, and therefore could not be trusted, and another provider, a cardiology physician argued that relying on the External Rx History when the patient does not have all the “pill bottles”, could create errors. These disagreements were met with more problem-solving statements from other providers, eg, a hospitalist physician argued that even if an electronic list of medications cannot be fully trusted, it can provide a template that can serve as a starting point for discussing with patients what they are actually taking.
Such statements were then followed by IT system education (eg, clarifications related to the External Rx History functionality on the EHR by the CMIO/SKN moderator, which in turn, was followed by best-practice assertions, ie, benefits of adhering to and consequences of not adhering to the best-practice of External Rx History Import during patient encounters. The latter type of statements were often initiated by SKN users (frontline providers) and actively reinforced by SKN moderators. For example, a pharmacist argued that importing “External Rx History,” preferably as close to admission as possible, is essential since it includes 90% plus of what actually occurred in the community. While there may be some gaps, it would at least allow providers to know what the patient has been prescribed and help them question why they are not taking certain medications. The CMO/SKN moderator then helped to reinforce the pharmacist’s message by providing examples of recent cases where dosing errors could have been averted during patient admission, if the External Rx History option had been used.
Another pharmacist then put forth a culture change assertion, urging participants not to allow “perfection to become the enemy of the good or the better.” When prescribers do not act to reconcile a medication owing to insufficient information, they are making a decision to “do nothing.” The CMO/SKN moderator helped to reinforce this message from the pharmacist by arguing that transferred patients and ED patients have limited ability to provide a medication history, making it all the more important to rely on the External Rx History Import. These discussions then culminated in a collective learning (aha) moment summarized by the PI/SKN moderator, ie, that incremental efforts to improve current medication list accuracy, through active use of the External Rx History Import functionality, could make a substantial contribution toward reducing medication discrepancies during transitions of care.
During the course of Yammer discussions in THREAD 1 and THREAD 2, SKN lunch-and-learn sessions were held during culminating points in these discussions, to allow SKN moderators to synthesize key takeaways and learnings from Yammer, and provide an opportunity for additional collective learning (aha) moments, among SKN users. These culminating points in inter-professional learning in THREAD 1 and THREAD 2 in turn, were found to be associated with distinct improvement trends in the respective measures of MU of EHR MedRec technology, ie, MEASURE 1 and MEASURE 2. While MEASURE 1 increased (improved) substantially, following the SKN lunch-and-learn session associated with THREAD 1, MEASURE 2 showed immediate decline (improvement) following the SKN lunch-and-learn session associated with THREAD 2, particularly among patients who had fewer active medications to manage.
A key takeaway from this pilot study, was that an SKN system could be a valuable tool in enabling MU of EHR MedRec technology. In particular, results suggest that SKN helped achieve progress in MU of EHR MedRec technology, by facilitating collective learning of the value of best practices (ie, big picture), before IT training of providers to address socio-technical challenges associated with implementing EHR. The lessons learned from this pilot study, related to content and dynamics of inter-professional knowledge exchange, in turn, providing a foundation for developing strategies for the creation of “learning health systems,” for enabling successful implementation of practice change in HCOs. Additionally, they serve to contribute to the literature and theory of change implementation in HCOs, by providing profound insights into how inter-professional learning occurs in the context of complex innovation implementation in HCOs.
The results described in the remaining sections, on the structure of inter-professional knowledge exchange related to EHR MedRec on the SKN system, provide several additional insights into the design of effective inter-professional knowledge sharing networks, as well as the roles of key participants (eg, SKN moderators), in enabling inter-professional learning and practice change in HCOs. These analyses in turn, provide a foundation for deriving additional implications for theory and practice of change implementation in HCOs.
Overall participation in the SKN system
Table 1 describes the essential characteristics of SKN participants, including participant type (ie, SKN moderators and SKN users), professional affiliation, and total number of posts on Yammer during the 1-year SKN period. The table also indicates the label used to distinguish each SKN participant on the network graphs depicted in Figures 1, 2, and 3.
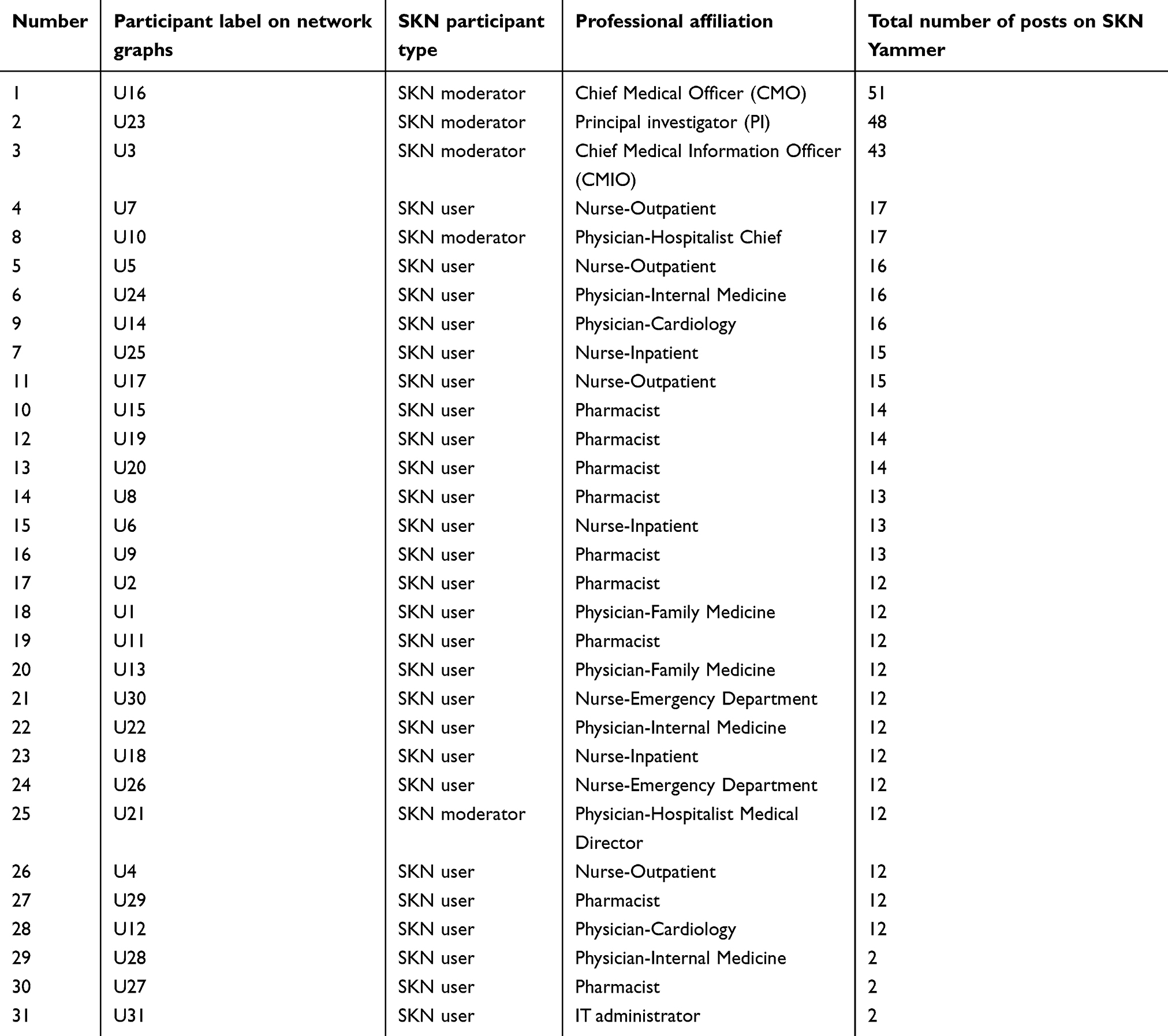 |
Table 1 Social Knowledge Networking (SKN) participant characteristics |
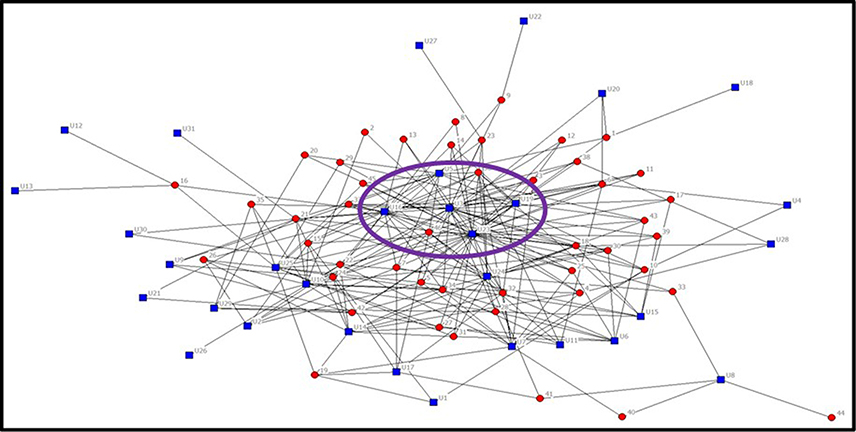 |
Figure 1 Two-mode analysis of structure of participation across all threads-of-discussion. |
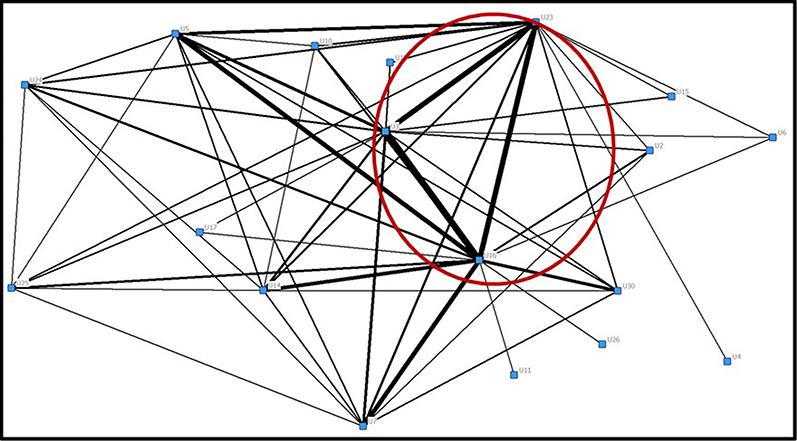 |
Figure 2 Network map of all Social Knowledge Networking system participants. |
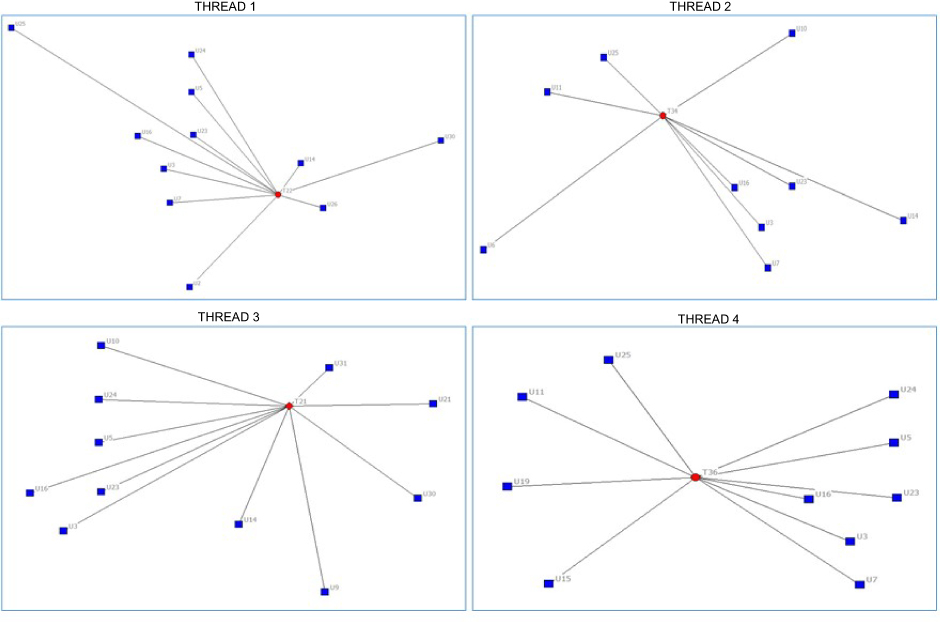 |
Figure 3 Ego network maps of participation within the four most voluminous threads-of-discussion. |
Table 1 is sorted by the total number of posts by SKN participants (last column), in descending order. Results on this column indicate that three of the five SKN moderators, posted 40 or more communications on Yammer over the 1-year SKN period, at least three times more than most SKN users. This suggests that SKN moderators (senior administrators) played a proactive role in “brokering” or facilitating inter-professional knowledge exchange on issues related to EHR MedRec, to promote collective learning of best practices, and create momentum for practice change (improvement). Further examination of the structure of inter-professional knowledge exchange, through SNA, provides additional insights related to the design of effective knowledge-sharing networks; and the roles played by select participants (eg, SKN moderators) over the 1-year SKN period, to enable collective learning and change (MU of EHR MedRec technology).
Two-mode network analysis of structure of participation across all threads-of-discussion
Figure 1 summarizes the structure of participation by all “SKN participants” in all “threads-of-discussion” on Yammer, over the 1-year SKN period. In the figure, “SKN participants” are represented by blue square nodes, while “threads-of-discussion” are represented by red circle nodes. A key takeaway from this figure, is the central “brokerage” (facilitation) role played by three of the five SKN moderators (U3, U16, and U23), across nearly all “threads-of-discussion” on the SKN system. As indicated in Table 1, node U3 represents the CMIO/SKN moderator, U16 represents the CMO/SKN moderator, and node U23 represents the PI/SKN moderator. The placement of the blue participant (person) nodes surrounded by red thread nodes, is a classic indicator that these persons are playing a central “brokerage” role – nearly all the red thread nodes lie between these three SKN moderators and the rest of the participants.
It would be relevant to note, that in addition to the function of “facilitation” of inter-professional knowledge exchange, “brokerage” refers to the ability of SKN moderators to transfer knowledge gained from members in one thread (eg, THREAD 1) to a different set of members in a separate thread (eg, THREAD 3), by virtue of their global view of the discussions.31 In addition to highlighting the central “brokerage” role of the three SKN moderators, Figure 1 indicates that these three SKN moderators consistently co-participated in a majority of threads, which in turn, suggests that they played a “collective brokerage” role in facilitating inter-professional knowledge exchange related to EHR MedRec, on the SKN system.
Figure 2 is a network graph of SKN participants only (minus any threads-of-discussion). This shows the implicit relationships between the participants by virtue of co-participating in a thread. This figure serves to effectively supplement Figure 1, in highlighting the strong “collective brokerage” role of the three SKN moderators (U3, U16, and U23). In Figure 2, a link between two SKN participants indicates that both participated together in at least one thread-of-discussion. The thicker the line, the more threads the two individuals participated in together. As indicated in Figure 2, the lines connecting the three SKN moderators are the thickest, relative to any of the other connecting lines, suggesting a strong “collective brokerage” role played by the three SKN moderators in facilitating inter-professional knowledge exchange related to EHR MedRec on the SKN system. Interestingly however, both Figures 1 and 2 indicate that two of the five participants originally designated as “SKN moderators” (ie, U10 and U21) did not emerge as having played a central “brokerage” role in facilitating knowledge exchange on the SKN system. This is corroborated by Table 1 which indicates that both these participants had considerably fewer total number of postings on SKN Yammer, compared to the other three SKN moderators.
On the other hand, Figures 1 and 2 reveal that five other individual SKN users (U5, U7, U19, U24, and U25), who were not officially designated as “SKN moderators” may have played a “brokerage” role, across several threads-of-discussion, similar to the three SKN moderators (U3, U16, and U23). As indicated in Table 1, U5 and U7 were outpatient nurses, U19 was a pharmacist, U24 was an internal medicine physician, and U25 was an inpatient nurse.
However, the results of ego-network analysis (summarized in Figure 3) showing participation within four of the most voluminous threads-of-discussion on SKN Yammer, reveals that while the three SKN moderators (U3, U16, and U23), participated together in all four threads, the five individual SKN users (U5, U7, U19, U24, and U25) did not consistently co-participate in all four threads, although they were present in one or two of them. For example, U19 did not participate in THREADS 1, 2, and 3 and U5 did not participate in THREAD 4. This suggests that the five SKN users, may have acted as “change champions,” thereby, brokering inter-professional knowledge exchange in some threads-of-discussion that they felt they had a stake in, but not all of the threads. In other words, each of the top four threads, had different sets of SKN users as “change champions,” whereas, the three SKN moderators were (U3, U16, and U23) consistently present in all of them. This serves to further emphasize the “collective brokerage” role of the three SKN moderators, in bringing together different sets of providers, to enable “change champions” to emerge on various threads related to EHR MedRec on the SKN system.
Ego-network analysis of participation within THREAD 1 and THREAD 2
Figure 3 summarizes the participation within each of the four most voluminous threads-of-discussion on SKN Yammer, including THREAD 1 and THREAD 2, which, respectively, were the threads-of-discussion (or inter-professional knowledge exchange) that provided the foundation for identifying two measures of MU of EHR MedRec for the study, as summarized in the Introduction, ie, “proportion of patient encounters with External Rx History import (Higher is Better) (MEASURE 1);” and “proportion of patients’ active medications that are missing documentation of Compliance Status (Lower is Better) (MEASURE 2).”
As indicated in Figure 3, in addition to the three SKN moderators (U3, U16, and U23) who participated in both THREAD 1 and THREAD 2, the additional participants in THREAD 1 included U2 (pharmacist), U5 (outpatient nurse), U7 (outpatient nurse), U14 (cardiology physician), U24 (internal medicine physician), U25 (inpatient nurse), U26 (ED nurse), and U30 (ED nurse). On the other hand, the additional participants in THREAD 2 included U6 (inpatient nurse), U7 (outpatient nurse), U10 (hospitalist), U11 (pharmacist), U14 (cardiology physician), and U25 (inpatient nurse). As such, while there was some overlap in individual participants between THREAD 1 and THREAD 2, overall, the two topics attracted and engaged different sets of provider stakeholders.
One of the key findings from the analysis of content and dynamics of inter-professional knowledge exchange in THREAD 1 and THREAD 2, was that champions for problem-solving and best-practice adherence initially emerged from among frontline providers.18 However, these types of messages, ie, “best-practice assertions” were actively reinforced by the CMO/SKN moderator (U16). On the other hand, the CMIO/SKN moderator (U3) played an important role in providing “IT system education” to participants, while the PI/SKN moderator (U23) played an important role in synthesizing lessons learned from inter-professional discussions to promote collective learning of the value of best practices, to provide a foundation for practice change. All SKN moderators also played an important role in the timely sharing of data and analytics related to both measures of MU of EHR MedRec technology on the SKN system, to enable data discussions and problem-solving. In contemplating the role played by SKN users (frontline providers), although champions for best-practice adherence often emerged from among pharmacists and nurses, physicians also actively participated in corroborating “best-practice assertions”, when they were presented with evidence linking practices to outcomes, to provide a clear rationale for practice change. Additionally, results suggest that five SKN users (U5, U7, U19, U24, and U25) served as champions for change, (thereby mimicking the “brokerage” role played by the three SKN moderators), in select threads-of-discussion that they felt they had a stake in.
Discussion
A key takeaway from the results of SNA in this paper, is that a knowledge sharing network rich in "brokerage" and "hierarchy," was effective in enabling inter-professional knowledge exchange and collective learning, to provide a foundation for practice change (MU of EHR MedRec). In other words, proactive, periodic top-down communication of best practices related to EHR MedRec was effective in engaging providers to share tacit knowledge on practice issues (related to EHR MedRec), and promote collective learning of the value of best practices, to lay a foundation for practice change. These results in turn, provide several implications for theory and practice of change implementation in HCOs.
Implications for theory
The results primarily serve to validate the theoretical framework on “effective communication network structures in professional complex systems”, discussed in the Introduction. In addition to reinforcing this framework, the results provide insights for refining and enhancing it, by suggesting that a strong “collective brokerage” role by senior administrators, with each one playing a unique role in facilitating inter-professional knowledge exchange, may be essential for enabling collective learning and change in HCOs, in the context of complex innovations (like MU of EHR MedRec technology).
For example, while the three key SKN moderators (U3, U16, and U23) played an important role in facilitating discussions of data related to the two practice measures, the CMO/SKN moderator (U16) played a key role in reinforcing problem-solving statements and best-practice assertions (emanating from SKN users), which often involved emphasizing the link between practices and outcomes. On the other hand, the CMIO/SKN moderator (U3) focused more on messages pertaining to IT system education; while the PI/SKN moderator (U23), played a role in synthesizing lessons learned from inter-professional discussions to develop collective learning (aha) moments. As such, taken together, the three SKN moderators played complementary roles in facilitating inter-professional knowledge exchange, to enable collective learning and practice change (improvement). Additionally, the various components of the SKN system; eg, SKN Yammer and SKN lunch-and-learn sessions, served to not only complement, but also reinforce each other, synergistically, to enable inter-professional learning, and create a foundation for practice change/improvement (MU of EHR MedRec technology).
Implications for practice
The previous discussion helps to identify management strategies for the design of effective knowledge sharing networks for inter-professional learning and change in HCOs. For example, the results suggest that during times of change, senior leaders must create mechanisms to facilitate (broker) knowledge exchange on practice issues, across professional subgroups and settings-of-care, while also proactively communicating the consequences of gaps in practices, to enable collective learning of the value of best practices. The latter in turn, enables shared understanding of the “big picture”, or the answer to the question of “why” practices need to change; which in turn, is essential for creating a foundation for practice change.
SNA of the structure of inter-professional knowledge exchange on the SKN system, also points to the potential effectiveness of a “collective brokerage” role by the SKN moderators. It suggests that a team of administrators playing complementary roles, to reinforce best-practice assertions; provide IT system education; and synthesize lessons learned to generate collective learning (aha) moments, can create a momentum for practice change. Specifically, such complementary efforts from senior administrators, can enable “champions for change” to emerge from among frontline providers, to initiate problem-solving statements and best-practice assertions, which in turn, can pave the way for senior administrators to reinforce these messages and enable learning and change.
In addition to playing proactive and complementary roles in facilitating inter-professional knowledge exchange, senior administrators also need to design the various components of the knowledge sharing (SKN) system (eg, SKN Yammer, SKN lunch-and-learn sessions, etc) to be complementary and synergistic in enabling collective learning and change. Importantly, the knowledge sharing system must incorporate the capacity for analyzing and disseminating data on measures of best practices, to provide a foundation for practice change (improvement).
Limitations and future research avenues
This study is limited in being restricted to one health system, and like any other implementation study, it is influenced by context in which the practice (EHR MedRec technology) is implemented at the institution. Correspondingly, the practice implications are also “context sensitive.” However, this may also be viewed as a strength of the study, in that, the prospective and exploratory study design helped gain insight into structure of inter-professional knowledge exchange and collective learning, within the context of implementing new practices in an HCO, which, in turn, provides insights into the design of effective knowledge sharing networks and other strategies for successful implementation of practice change in HCOs. Future research could help to evaluate the generalizability of results from this exploratory study, through large-scale controlled experiments to investigate causal relationships between SKN use and EHR MU, across a wide variety of HCOs.
Conclusion
The overall results of this study suggest that an SKN system could be a valuable tool in enabling inter-professional knowledge exchange and collective learning, to facilitate practice change (EHR MU) in HCOs. Results from SNA suggest that proactive, periodic top-down communication of best practices related to EHR MedRec, was effective in enabling inter-professional exchange of tacit knowledge on practice issues, and collective learning of the value of best practices, to lay a foundation for practice change. These results, in turn, provide several insights into the design of effective knowledge sharing networks, including the roles of SKN moderators and provider champions in enabling collective learning and change in HCOs. Future large-scale studies of SKN use in HCOs, could help to generate a systematic evidence-base of management strategies for promoting EHR MU, which in turn, could be used to prompt federal EHR vendors to incorporate SKN features into EHR systems.
IRB approval
The study was approved by the IRB at Augusta University. IRB approval was obtained prior to data collection.
Acknowledgments
This study was supported by grant number R21HS024335 from the Agency for Healthcare Research and Quality (AHRQ). Augusta University received funding for this project from AHRQ.
Disclosure
The authors report no conflicts of interest in this work.
References
1. AHRQ, Agency for Healthcare Research and Quality. Patient safety primer: medication reconciliation; 2016. Available from: https://psnet.ahrq.gov/primers/primer/1/medication-reconciliation
2. Barnsteiner JH. Medication Reconciliation. In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Clinicians. Rockville (MD): Agency for Healthcare Research and Quality (US); 2008. Chapter 38. Available from. http://www.ncbi.nlm.nih.gov/books/NBK2648/. Accessed October 15, 2015.
3. CMS Centers for Medicare and Medicaid Services. Stage 2 eligible professional meaningful use core measures measure 14 of 17; 2012 Available from: https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/Stage2_EPCore_14_MedicationReconciliation.pdf. Accessed October 15, 2015.
4. HealthIT.Gov. Achieving meaningful use stage 2: medication reconciliation; 2014. Available from: https://www.healthit.gov/providers-professionals/achieve-meaningful-use/core-measures-2/medication-reconciliation. Accessed October 01, 2015.
5. Boockvar KS, Santos SL, Kushniruk A, Johnson C, Nebeker JR. Medication reconciliation: barriers and facilitators from the perspectives of physicians and pharmacists. J Hosp Med. 2011;6:329–337. doi:10.1002/jhm.891
6. Clay BJ, Halasyamani L, Stucky ER, Greenwald JL, Williams MV. Results of a medication reconciliation survey from the 2006 Society of hospital medicine national meeting. J Hosp Med. 2008;3(6):465–472. doi:10.1002/jhm.295
7. Rose AJ, Fischer SH, Pasche-Orlow MK. Beyond medication reconciliation: the correct medication list. J Am Med Assoc. 2017;317(20):2057–2058. doi:10.1001/jama.2017.4628
8. Sanchez HS, Sadie SS, Santos SL, Boockvar K. Implementing medication reconciliation from the planner’s perspective: a qualitative study. BMC Health Serv Res. 2014;14:290. doi:10.1186/1472-6963-14-290
9. Greenwald JL, Halasyamani L, Greene J, et al. Making inpatient medication reconciliation patient centered, clinically relevant and implementable: a consensus statement on key principles and first steps. J Hosp Med. 2010;5(8):477–485. doi:10.1002/jhm.791
10. Van Sluisveld N, Zegers M, Natsch S, Wollersheim H. Medication reconciliation at hospital admission and discharge: insufficient knowledge, unclear task reallocation and lack of collaboration as major barriers to medication safety. BMC Health Serv Res. 2012;12:170. doi:10.1186/1472-6963-12-170
11. Grossman J, Gourevitch R, Cross DA. Hospital experiences using electronic health records to support medication reconciliation. Nat Inst Healthcare Reform (NIHCR) Res Brief Number. 2014;17:1–13.
12. Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172:1057–1069. doi:10.1001/archinternmed.2012.2246
13. Porcelli PJ, Wlatman LR, Brown SH. A review of medication reconciliation issues and experiences with clinical staff and information systems. Appl Clin Inform. 2010;1:442–461. doi:10.4338/ACI-2010-01-RA-0005
14. Rangachari P. Overcoming the unintended adverse consequences of implementing health IT through human resource and knowledge management. In: Blair JD, Fottler MD, Savage GT, editors. Advances in Health Care Management. Vol. 9. Bingley, UK: Emerald; 2010a:163–194.
15. Smith P. Med wreck: proposing a solution for the nightmare of medication reconciliation; eBook; 2017. Available from: https://healthitaccelerator.com/med-wreck/.
16. AHRQ, Agency for Healthcare Research and Quality. Using Social Knowledge Networking (SKN) technology to enable meaningful use of EHR technology; 2016. Available from: https://healthit.ahrq.gov/ahrq-funded-projects/using-social-knowledge-networking-skn-technology-enable-meaningful-use-ehr.
17. Rangachari P. Implementing a Social Knowledge Networking (SKN) system to enable meaningful use of an EHR medication reconciliation system: a study protocol. Risk Manag Healthc Policy. 2018a;11:45–53. PMID: 29618941. doi:10.2147/RMHP.S152313
18. Rangachari P, Dellsperger KC, Rethemeyer R. A qualitative study of inter-professional learning related to Electronic Health Record (EHR) medication reconciliation within a Social Knowledge Networking (SKN) System. J Healthcare Leadersh. 2019;11:23–41. doi:10.2147/JHL.S198951
19. Plsek P. Redesigning Health Care with Insights from the Science of Complex Adaptive Systems (Appendix B, 309Y322). In Institute of Medicine, Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
20. Anderson A, McDaniel R. Managing health care organizations: where professionalism meets complexity science. Health Care Manage Rev. 2000;25(1):83–92.
21. Burt R. Network structure of social capital. In: Sutton RI, Staw BM, editors. Research in Organizational Behavior. Vol. 22. Greenwich, CT: JAI Press; 2000:345–423.
22. Hansen MT. The search-transfer problem: role of weak ties in sharing knowledge across organizational units. Adm Sci Q. 1999;44(1):82–111. doi:10.2307/2667032
23. Rangachari P. Knowledge sharing networks related to hospital quality measurement and reporting. Health Care Manage Rev. 2008;33(3):253–263. doi:10.1097/01.HMR.0000324910.26896.91
24. Rangachari P. Knowledge sharing networks in professional complex systems. J Knowl Manage. 2009;13(3):132–145. doi:10.1108/13673270910962923
25. Rangachari P. Knowledge sharing and organizational learning in the context of hospital infection prevention. Qual Manag Health Care. 2010b;19(1):34–45. doi:10.1097/QMH.0b013e3181ccbd1d
26. Rangachari P. Using social knowledge networking technology to enable meaningful use of electronic health record technology in hospitals and health systems: a review article. J Hosp Adm. 2014;3(6):66–78. doi:10.5430/jha.v3n6p66
27. Rangachari P, Madaio M, Rethemeyer RK, et al. The evolution of knowledge exchanges enabling successful practice change in two intensive care units. Health Care Manage Rev. 2015a;40(1):65–78. doi:10.1097/HMR.0000000000000001
28. Rangachari P, Madaio M, Rethemeyer RK, et al. Cumulative impact of periodic top-down quality improvement communications on infection prevention practices and outcomes in two units. Health Care Manage Rev. 2015b;40(4):324–336. doi:10.1097/HMR.0000000000000038
29. Borgatti SP, Everett MG, Johnson JC. Analyzing Social Networks. Chapter 13. Los Angeles: Sage Publications; 2013a.
30. Borgatti SP, Everett MG, Johnson JC. Analyzing Social Networks. Chapter 15. Los Angeles: Sage Publications; 2013b.
31. Fernandez RM, Gould RV. A dilemma of state power: brokerage and influence in the national health policy domain. Am J Sociol. 1994;99(6):1455–1499. doi:10.1086/230451
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.