")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
National Trends In Kidney, Heart And Liver Transplants Among Patients With And Without Chronic Obstructive Pulmonary Disease In Spain (2001–2015)
Authors de Miguel-Díez J , Jiménez-García R , Hernández-Barrera V , de Miguel-Yanes JM, Méndez-Bailón M, López-de-Andres A
Received 24 April 2019
Accepted for publication 9 August 2019
Published 26 September 2019 Volume 2019:14 Pages 2235—2243
DOI https://doi.org/10.2147/COPD.S213257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Javier de Miguel-Díez,1 Rodrigo Jiménez-García,2 Valentín Hernández-Barrera,2 José M de Miguel-Yanes,3,4 Manuel Méndez-Bailón,5 Ana López-de-Andres2
1Respiratory Department, Hospital General Universitario Gregorio Marañón, Facultad de Medicina, Universidad Complutense de Madrid (UCM), Instituto de Investigación Sanitaria Gregorio Marañón (IiSGM), Madrid, Spain; 2Preventive Medicine and Public Health Teaching and Research Unit, Health Sciences Faculty, Rey Juan Carlos University, Alcorcón, Madrid, Spain; 3Internal Medicine Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain; 4Facultad de Medicina, Universidad Complutense De Madrid (UCM), Madrid, Spain; 5Internal Medicine Department, Hospital Universitario Clínico San Carlos, Facultad De Medicina, Universidad Complutense de Madrid (UCM), Madrid, Spain
Correspondence: Rodrigo Jiménez-García
Preventive Medicine and Public Health Teaching and Research Unit, Health Sciences Faculty, Rey Juan Carlos University, Avenida de Atenas s/n, Alcorcón, Madrid 28922, Spain
Tel +34 91 4888853
Email [email protected]
Background: To describe trends and outcomes during admission for solid organ transplants, excluding lungs, in people with or without COPD in Spain (2001–2015).
Methods: We used national hospital discharge data to select all hospital admissions for kidney, heart and liver transplants. We estimated admission rates stratified by COPD status. We analyzed the Charlson Comorbidity Index, therapeutic procedures and outcomes.
Results: We identified 52,020 admissions (33,293 for kidney transplant, 3,937 for heart transplant and 14,790 for liver transplant). Patients with COPD accounted for 2.5%, 4.2% and 3.5% of kidney, heart and liver transplant patients, respectively. The number of kidney and liver transplants increased among COPD patients over the study period, whereas the number of heart transplants remained stable. In all cases, COPD patients were significantly older and had more coexisting medical conditions than those without COPD. Among patients who underwent a kidney transplant, there were no significant differences in the clinical characteristics analyzed between the groups, but the overall in-hospital mortality (IHM) rate was significantly higher in COPD patients than in those without COPD (2.22% vs 0.58%, p=0.008). There were no differences for any of the study variables or for the IHM rate in patients who underwent a heart transplant (14.63% in both groups). Among patients who underwent a liver transplant, COPD patients had lower prevalences of infection and complications than those without COPD. The IHM rate was also significantly lower in COPD patients than in non-COPD controls who underwent a liver transplant (4.07% vs 8.91%, p=0.002).
Conclusion: COPD prevalence in patients undergoing renal, heart and liver transplants is lower than it has been described in the general population. However, we did not find differences in the clinical characteristics analyzed between COPD and non-COPD patients. Furthermore, the IHM rate was only higher in COPD patients who underwent a kidney transplant but not in those undergoing a heart or liver transplant.
Keywords: solid organ transplant, COPD, comorbidities, in-hospital mortality
Background
Solid organ transplantation is the therapy of choice for patients with end-stage organ disease. The most frequently transplanted organs include the kidney, liver, heart, and lung.1 In recent decades, the rate of solid organ transplantation has significantly increased worldwide.2,3 In addition, improved organ allocation, donor selection, surgical techniques, and technology; refined corticosteroid and immunosuppressive regimens; and better diagnosis and treatment of complications have contributed to increasing the success rate of these transplants.4,5
As organ transplantation has become more common, the average age of transplant recipients has increased, thus increasing the potential for multiple comorbidities.6 These include chronic obstructive pulmonary disease (COPD), which is a major public health concern and a leading cause of morbidity and mortality worldwide, affecting approximately 10% of the general adult population.7,8
The prevalence and impact of COPD on the outcomes of patients undergoing lung transplantation has been previously described.9,10 Less well known is the prevalence and influence of this disease in recipients of transplants of other solid organs. However, it has been reported that COPD patients may experience higher mortality rates and may undergo fewer of some of these types of transplants.11 Furthermore, no definitive guidelines exist to guide when these patients have levels of operative risk that are too high, prohibiting safe transplantation.12
Using the Spanish National Hospital Discharge Database (SNHDD), we aimed to 1) examine the characteristics and in-hospital outcomes of kidney, heart and liver transplant patients among patients with or without COPD in Spain from 2001 to 2015 and 2) compare the clinical variables and in-hospital outcomes between people with and without COPD matched by sex, age and year who were hospitalized for kidney, heart and liver transplants.
Methods
We performed a retrospective, observational study using the SNHDD, which compiles all public hospital data, covering more than 95% of hospital admissions. The SNHDD includes patient variables (sex, date of birth), admission and discharge dates, up to 14 discharge diagnoses, and up to 20 procedures performed during the hospital stay.13 We analyzed data collected between January 1, 2001, and December 31, 2015. The SNHDD uses the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) for coding.
We selected admissions for patients whose medical procedures included kidney transplant (ICD-9-CM codes 55.6, 55.61), heart transplant (ICD-9-CM codes 37.51) and liver transplant (ICD-9-CM codes 50.5, 50.51, 50.59) in any procedure field.
We grouped admissions by COPD status. COPD sufferers were defined as those with any of the following ICD-9-CM codes in any diagnostic position: 490, 491, 491.0, 491.1, 491.2x, 491.8, 491.9, 492, 492.0, 492.8, 496; those without any of those codes were considered non-COPD sufferers.
The clinical characteristics included information on overall comorbidity at the time of discharge, which was assessed by calculating the Charlson comorbidity index (CCI).14 The calculation of the CCI was performed excluding COPD as a disease.
Irrespective of position on the diagnoses or procedures coding lists, we retrieved data about in-hospital infections (ICD-9-CM codes: 997.39, 486, 995.91, 995.92, 998.5, 998.51, 998.52, 998.53, 998.54, 998.55, 998.59, 998.50, 599.0, 008.45). We additionally sought specific complications of the transplanted recipients or graft rejection (ICD-9-CM code 996.8 and codes 996.81 for transplanted kidney; 996.83 for transplanted heart and 996.82 for liver transplant).
Additionally, we specifically identified the following procedures: hemodialysis/dialysis (ICD-9-CM codes 39.95, 54.98) and heart assist device implantation (ICD-9-CM codes 37.6, 37.60, 37.61, 37.62, 37.63, 37.64, 37.65, 37.66, 37.67, 37.68).
We estimated the mean length of hospital stay (LOHS) and hospital mortality (IHM). The IHM rate was defined as the proportion of patients who died during admission for each year of study.
Matching
To control for the possible confounding effects of age and sex, we selected a matched control non-COPD patient for each COPD patient who underwent each type of transplant. The matching variables included age, sex, year of surgery and province of residence. If more than one control was available, the selection was performed randomly. We found controls for over 98% of COPD patients (857/863 for lung transplant165/167 for heart transplant and 516/525 for liver transplant).
Statistical Analysis
A descriptive statistical analysis was performed for all continuous variables and categories by stratifying patients admitted for kidney, heart and liver transplant according to COPD status.
Variables are expressed as proportions or as the means with standard deviations. Time was categorized into five 3-year periods.
For each recipient transplant (kidney, heart and lung), we performed bivariable analyses according to COPD status using the χ2 test for linear trend (proportions), Fisher exact text and ANOVA (means), as appropriate.
We constructed bivariable conditional logistic regression models to compare the study variables between patients with COPD and the matched controls. The analyses were stratified according to the organ transplanted (kidney, heart and liver).
Matching and statistical analyses were performed using Stata version 10.1 (Stata, College Station, Texas, USA). Statistical significance was set at p<0.05 (2-tailed).
Ethical Aspects
Data confidentiality was maintained at all times as patient identifiers were deleted before the database was provided to the authors to maintain patient anonymity. It is not possible to identify patients on an individual level, either in this article or in the database. Given the anonymous and mandatory nature of the dataset, it was not necessary to obtain informed consent or approval by the ethics committee, in accordance with Spanish law.
Results
From 2001 to 2015, we identified 33,293 admissions for kidney transplants, 3,937 for heart transplants and 14,790 for liver transplants in Spain. Patients with COPD accounted for 2.5% (n=863) of the total kidney transplant recipients, 4.2% (n=167) of the total heart transplant recipients and 3.5% (n=525) of the total liver transplant recipients.
Table 1 shows the demographic and clinical characteristics and in-hospital outcomes of patients with kidney, heart and liver transplants.
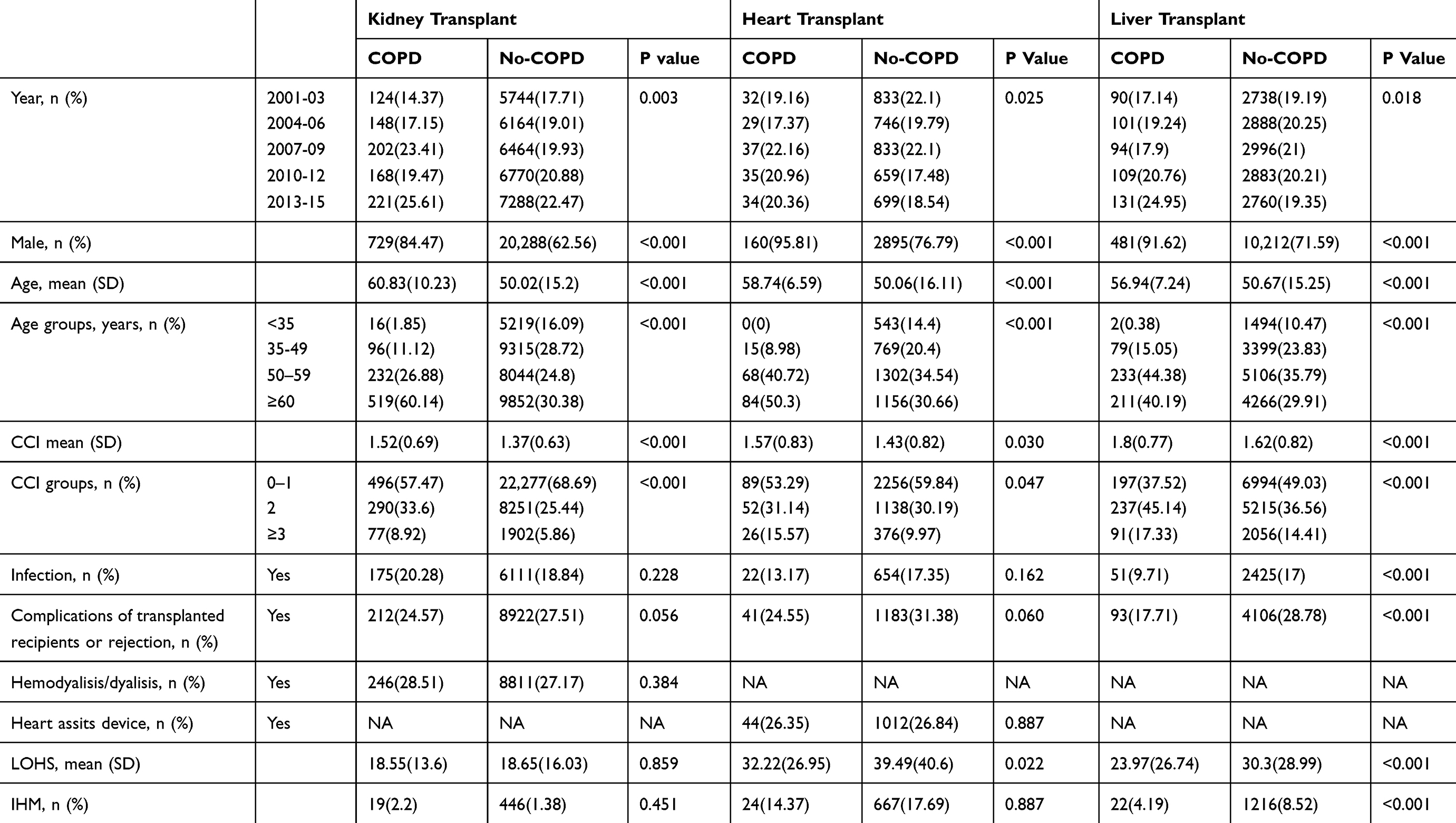 |
Table 1 Clinical Characteristics Of Hospital Admissions For Kidney, Heart And Liver Transplants Among Patients With Or Without COPD In Spain, 2001–2015 |
As shown in Table 1, the number of kidney and liver transplants increased among COPD patients over the study period, whereas the number of heart transplants remained stable.
For all types of transplants, we found a male predominance (84.47% for COPD and 62.56% for non-COPD in kidney transplants; 95.81% for COPD and 76.79% for non-COPD in heart transplants; and 91.62% for COPD and 71.59 for non-COPD in liver transplants; all p<0.05).
In COPD patients who underwent kidney transplantation, the mean age was 10 years older than that in those without COPD (60.83; SD 10.23 vs 50.02; SD 15.2, p<0.001). Patients with COPD had more coexisting medical conditions according to the CCI (p<0.001).
Almost 20% of patients who underwent kidney transplantation, in addition to COPD status, suffered infections, and approximately 25% suffered complications of the transplanted kidney or organ rejection. No differences were found between the groups of patients in the use of hemodialysis. The LOHS was similar (approximately 18 days in both groups), and the IHM rate was not significantly different (2.2% in COPD and 1.38% in non-COPD patients).
In patients who underwent heart transplantation, patients with COPD were significantly older than those without COPD (58.74 years vs 50.06 years) and had more comorbidities (mean CCI 1.57 vs 1.43; p=0.030). No differences were found between the groups of patients with regard to complications of the transplant (infections and complications of the heart transplant or organ rejection). Approximately 26% of patients, in addition to COPD, needed a heart assist device. The LOHS was significantly lower in COPD patients than in those without COPD (32.22 days vs 39.49 days). The crude IHM rate was 14.37% in COPD patients and 17.69% in non-COPD patients (p=0.887).
In patients who underwent liver transplantation, patients with COPD were significantly older and had more comorbidities than those without COPD, as shown in Table 1. COPD patients had significantly lower rates of infections and complications of the liver transplant than non-COPD patients (9.71% and 17.71% vs 17% and 28.78%, respectively; both p<0.001). The LOHS was significantly shorter in COPD patients than in those without COPD (23.97 days vs 30.3 days; p<0.001). Non-COPD patients had an IHM rate that was twice as high as that of COPD patients (8.52% vs 4.19%; p<0.001).
Table 2–4 show the distributions and IHM rates stratified according to the study variables in COPD patients and matched non-COPD controls who underwent kidney (Table 2), heart (Table 3) and liver transplants (Table 4).
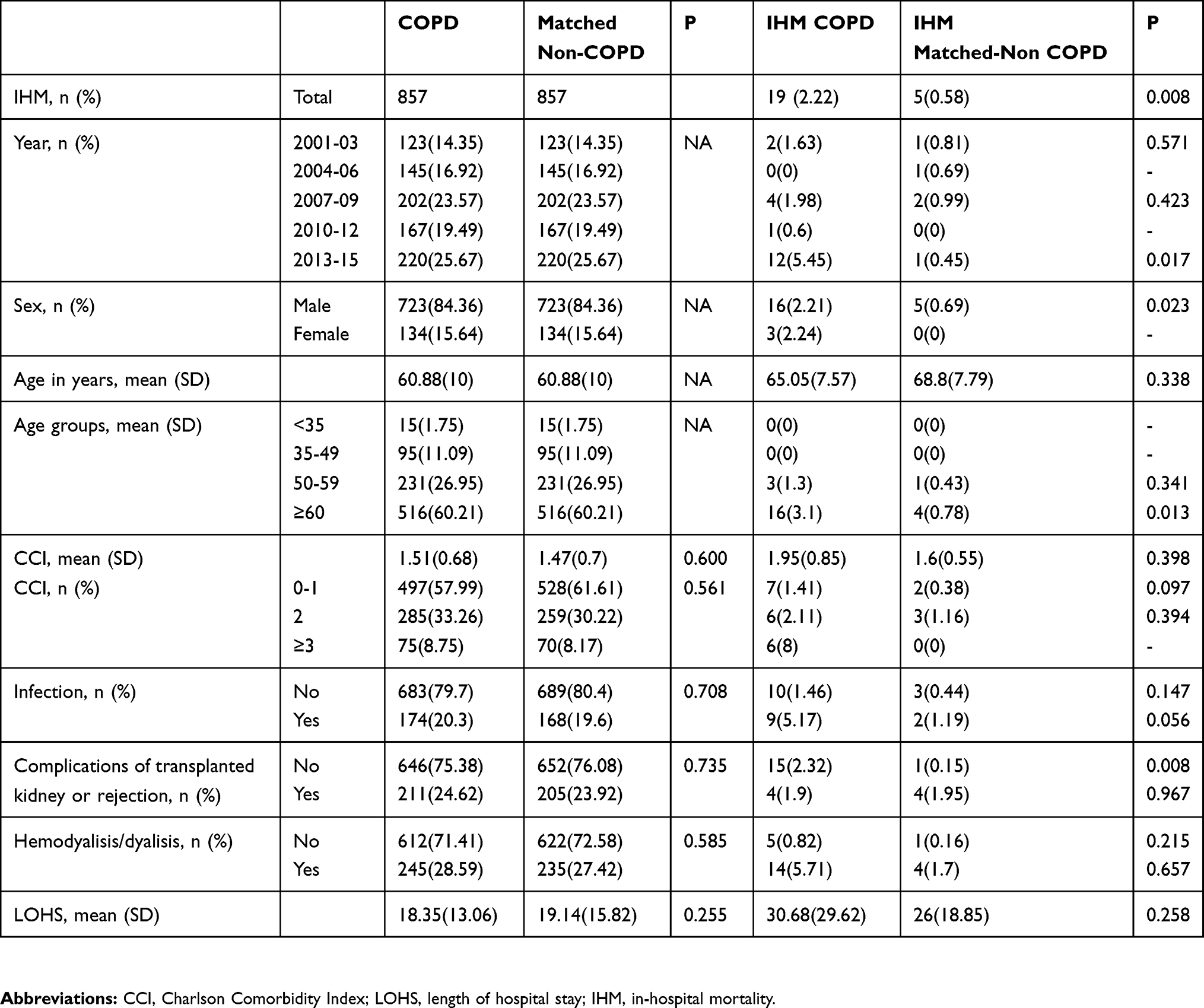 |
Table 2 Distribution And In-Hospital Mortality According To Study Variables Of COPD Patients And Matched Non-COPD Controls With A Kidney Transplant |
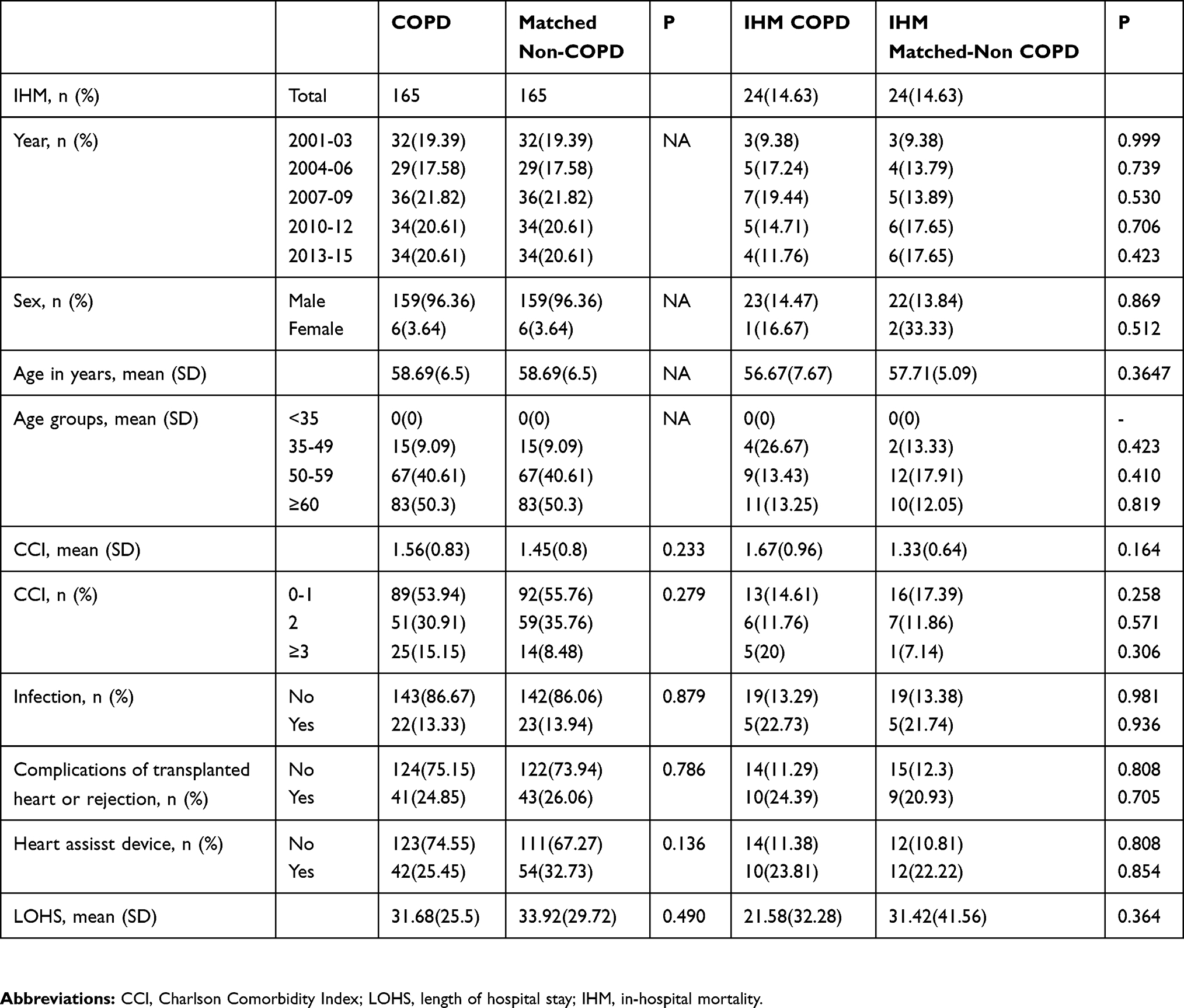 |
Table 3 Distribution And In-Hospital Mortality According To Study Variables Of COPD Patients And Matched Non-COPD Controls With A Heart Transplant |
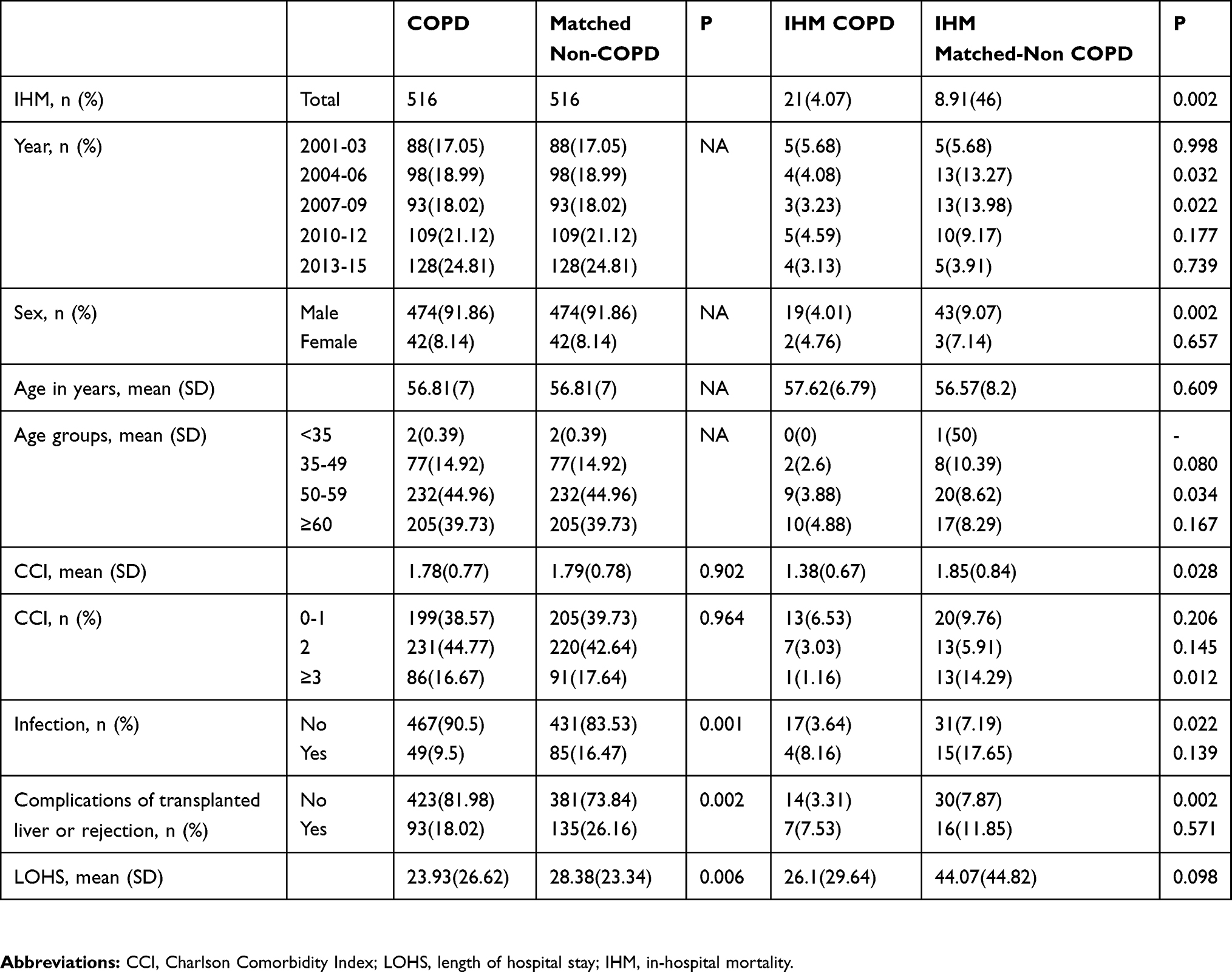 |
Table 4 Distribution And In-Hospital Mortality According To Study Variables Of COPD Patients And Matched Non-COPD Controls With A Liver Transplant |
After matching, patients who underwent kidney transplants with and without COPD had no significant differences in the prevalence of any clinical characteristics analyzed, including the LOHS. However, we found that overall IHM rate was significantly higher in COPD patients than in the matched non-COPD patients (2.22% vs 0.58%) (p=0.008). As shown in Table 2, this difference was also significant for the 2013–15 period and in the ≥60 age group. The IHM rate was higher for men with COPD than for men without COPD (2.21% vs 0.69%; p=0.023).
Table 3 shows the distribution and IHM rates for patients with COPD and the matched controls who underwent a heart transplant. After matching, no differences were found for any of the study variables, the LOHS or the IHM (14.63% in both groups).
As shown in Table 4, among the patients who underwent liver transplantation, patients with COPD had lower prevalences of infection (16.47% vs 9.5%, p=0.001) and complications of transplanted liver (26.16% vs 18.02%, p=0.002) than non-COPD controls. The mean LOHS was shorter in patients with COPD (23.93 days vs 28.38 days; p=0.006).
We found that the IHM rate was significantly lower in COPD patients than in the matched controls (4.07% vs 8.91%, p=0.002) who underwent a liver transplant. IHM had lower values for men with COPD than for men without COPD (4.01% vs 9.07%; p=0.002).
Discussion
Our study shows that the COPD prevalence in patients undergoing kidney, heart and liver transplants is lower than has been described in the general population.15 Thus, patients with COPD accounted for 2.5%, 4.2% and 3.5% of kidney, heart and liver transplant recipients, respectively. Nevertheless, the number of kidney and liver transplants performed in patients with COPD increased over the study period, whereas the number of heart transplants remained stable.
Kent et al also demonstrated that COPD patients who begin dialysis therapy in the United States experience lower rates of kidney transplantation than those without COPD.11 They reported that the prevalence of COPD was 7.5% overall and increased from 6.7 to 8.1% from 1995 to 2004. COPD correlated significantly with the following factors: older age, cardiovascular conditions, cancer, malnutrition, poor functional status, and tobacco use. Similarly, we also found that COPD patients who underwent kidney transplantation were significantly older and had more comorbidities than those without COPD.11
With regard to heart transplants, in a recent study in which 45 patients who had received this type of transplant were retrospectively evaluated, only 2 had COPD (4.4%).16 However, the Spanish Cardiac Transplant Registry has reported an increase in the prevalence of moderate-severe COPD in patients undergoing heart transplantation, from 6% in the period 1984–1988 to 8.5% in the period 2009–2013.17 It has previously been reported that patients with pretransplant vascular disease compared to those without vascular disease are older at the time of the heart transplant and have more comorbidities, including a history of COPD.18 Among the patients who underwent heart transplantation in our study, COPD patients had a higher mean age and more coexisting medical conditions than those without COPD.
In relation to liver transplantation, Hourani et al published a study of 116 consecutive patients admitted for evaluation for this type of transplant and found that only 3% had airway obstruction.19 In contrast, Rybak et al showed that 18% of new patients undergoing liver transplant evaluation in the United Sates had COPD.20 However, 80% of COPD patients had the diagnosis of this disease made for the first time during their liver transplant evaluation. Older age and any history of smoking increased the risk of COPD in this population. Among the patients who underwent liver transplantation in our study, COPD patients were also significantly older than those without COPD.
The low prevalence of COPD in patients undergoing kidney, heart and liver transplants in our study suggests that this disease is considered a possible contraindication for the surgery. However, we did not find differences in the clinical characteristics analyzed between COPD and non-COPD patients. Furthermore, COPD was associated with a higher IHM only in patients undergoing kidney transplant, although the figures were very low in both groups, but not in those undergoing a heart or liver transplant.
Kent et al also found, among patients who began dialysis therapy in the United States and subsequently received a kidney transplant, that the mortality risk was significantly higher for those with COPD.11 This disease has also been identified as a predictive feature of 5-year mortality in patients referred for kidney transplantation.21 In any case, as Laging et al have previously indicated, patient survival after kidney transplantation is remarkably good, so patients with extensive comorbidities should still be considered for this type of transplant.22
It has been described that COPD is an added risk factor for mortality in patients undergoing heart transplantation in the surgical period and a factor contributing to a poor prognosis in the future.23 However, COPD patients undergoing heart transplantation in the present study did not have a higher IHM rate than those without COPD. In contrast, Stepanova et al showed that COPD was independently associated with a lower posttransplant survival rate in the period 1995–2013.24
In patients undergoing liver transplantation in our study, the presence of COPD was associated with a lower IHM rate. Similarly, Rybak et al did not find differences in short-term survival in patients with advanced liver disease undergoing lung transplant evaluation.20 Conversely, in a cohort of 624 patients, Volk et al demonstrated that pretransplantation COPD independently contributed to decreased post-transplantation survival (median follow-up time of 4.3 years).25
The strength of our findings lies in the large sample size, with data from more than 50,000 transplants, the 15-year recruitment period covering the population of an entire country, and the standardized methodology, which has been used to investigate COPD and its complications in Spain and elsewhere.26 However, our study also has some limitations. Our data source was the SNHDD, an administrative database that contains discharge data for hospitalizations in Spain and necessarily relies on the information that physicians include in the discharge report. Therefore, we were unable to analyze the impacts of other variables that may play a role in post-transplant survival, including spirometric values, nutritional status, psychological factors or adherence to medications. Another relevant limitation is the lack of information on the duration or severity of COPD (including FEV1 values), which could be selection criteria for transplant indication. Thus, we cannot rule out the possibility that subjects with milder disease were included in the transplant protocols, whereas the more severe patients were excluded.
Despite these limitations, our study has addressed major issues related to solid organ transplantations.
In conclusion, our study indicates that the COPD prevalence in patients undergoing kidney, heart and liver transplants is lower than has been described in the general population, suggesting that this disease is considered a possible contraindication for surgery. However, we did not find differences in the clinical characteristics analyzed between COPD and non-COPD patients. Furthermore, we found that COPD only increased the IHM rate in patients undergoing kidney transplant, although the figures were very low regardless of the presence or absence of COPD. Screening and appropriate management may be warranted to minimize the short- and long-term impact of COPD on patients undergoing solid organ transplantations.
Abbreviations
CCI, Charlson comorbidity index; COPD, chronic obstructive pulmonary disease; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; IHM, in-hospital mortality; LOHS, length of hospital stay; SNHDD, Spanish National Hospital Discharge Database.
Acknowledgments
This study forms part of research funded by the FIS (Fondo de Investigaciones Sanitarias—Health Research Fund, Instituto de Salud Carlos III) and co-financed by the European Union through the Fondo Europeo de Desarrollo Regional (FEDER, “Una manera de hacer Europa”): grant no. PI16/00564. The authors would like to thank NEUMOMADRID (XVIII Awards Edition, 2018) for grant support.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tsai HI, Yu HP. A review of nationwide population study of organ transplantation in Taiwan. Acta Anaesthesiol Taiwan. 2016;54(2):70–74. doi:10.1016/j.aat.2016.05.003
2. Daga Ruiz D, Fernández Aguirre C, Segura González F, Carballo Ruiz M. Indications and long-term outcomes for solid organ transplant. Quality of life in solid organ transplant recipients. Med Intensiva. 2008;32(6):296–303.
3. Navale SM, Szubski CR, Klika AK, Schiltz NK, Desai PP, Barsoum WK. The impact of solid organ transplant history on inpatient complications, mortality, length of stay, and cost for primary total hip arthroplasty admissions in the United States. J Arthroplasty. 2017;32(4):1107–16.e1. doi:10.1016/j.arth.2016.10.017
4. Bloom RD, Goldberg LR, Wang AY, Faust TW, Kotloff RM. An overview of solid organ transplantation. Clin Chest Med. 2005;26(4):529–543. doi:10.1016/j.ccm.2005.06.002
5. Lodhi SA, Lamb KE, Meier-Kriesche HU. Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. Am J Transplant. 2011;11(6):1226–1235. doi:10.1111/j.1600-6143.2011.03539.x
6. Manoushagian S, Meshkov A. Evaluation of solid organ transplant candidates for coronary artery disease. Am J Transplant. 2014;14(10):2228–2234.
7. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD study): a population-based prevalence study. Lancet. 2007;370(9589):741–750.
8. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of COPD 2018. 2018 Global Initiative for Chronic Obstructive Lung Disease, Inc. Fontana, USA. Available from: https://goldcopd.org.
9. Aziz F, Penupolu S, Xu X, He J. Lung transplant in end-staged chronic obstructive pulmonary disease (COPD) patients: a concise review. J Thorac Dis. 2010;2(2):111–116.
10. Zeriouh M, Mohite PN, Sabashnikov A, et al. Lung transplantation in chronic obstructive pulmonary disease: long-term survival, freedom from bronchiolitis obliterans syndrome, and factors influencing outcome. Clin Transplant. 2015;29(4):383–392. doi:10.1111/ctr.12528
11. Kent BD, Eltayeb EE, Woodman A, Mutwali A, Nguyen HT, Stack AG. The impact of chronic obstructive pulmonary disease and smoking on mortality and kidney transplantation in end-stage kidney disease. Am J Nephrol. 2012;36(3):287–295. doi:10.1159/000342207
12. McAvoy NC, Hayes PC. Cardiac and pulmonary issues in LT assessment candidates. Clin Liver Dis. 2014;18(3):529–541. doi:10.1016/j.cld.2014.05.001
13. Instituto Nacional de Gestión Sanitaria, Ministerio de Sanidad, Servicios Sociales e Igualdad. Conjunto Mínimo Básico De Datos. Hospitales del INSALUD. Available from: http://www.ingesa.msssi.gob.es/estadEstudios/documPublica/CMBD-2001.htm. [accessed June 16, 2018.
14. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383.
15. Miravitlles M, Soriano JB, García-Río F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–868. doi:10.1136/thx.2009.115725
16. Savaş Bozbaş Ş, Ulubay G, Öner Eyüboğlu F, Sezgin A, Haberal M. Prevalence, cause, and treatment of respiratory insufficiency after orthotopic heart transplant. Exp Clin Transplant. 2015;13(Suppl 3):140–143. doi:10.6002/ect.tdtd2015.P76
17. González-Vílchez F, Gómez-Bueno M, Almenar L, et al. Spanish heart transplantation registry. 25th official report of the Spanish Society of Cardiology. Working group on heart failure and heart transplantation (1984–2013). Rev Esp Cardiol (Engl Ed). 2014;67(12):1039–1051. doi:10.1016/j.rec.2014.09.005
18. Takayama H, Salerno CT, Aldea GS, Verrier ED. Characteristics of extracoronary vascular disease in heart transplant recipient. J Card Surg. 2008;23(5):459–463. doi:10.1111/j.1540-8191.2008.00586.x
19. Hourani JM, Bellamy PE, Tashkin DP, Batra P, Simmons MS. Pulmonary dysfunction in advanced liver disease: frequent occurrence of an abnormal diffusing capacity. Am J Med. 1991;90(6):693–700.
20. Rybak D, Fallon MB, Krowka MJ, et al. Pulmonary vascular complications of liver disease study group. Risk factors and impact of chronic obstructive pulmonary disease in candidates for liver transplantation. Liver Transpl. 2008;14(9):1357–1365. doi:10.1002/lt.21545
21. Chen LX, Josephson MA, Hedeker D, Campbell KH, Stankus N, Saunders MR. A clinical prediction score to guide referral of elderly dialysis patients for kidney transplant evaluation. Kidney Int Rep. 2017;2(4):645–653. doi:10.1016/j.ekir.2017.02.014
22. Laging M, Kal-van Gestel JA, van de Wetering J, et al. A high comorbidity score should not be a contraindication for kidney transplantation. Transplantation. 2016;100(2):400–406. doi:10.1097/TP.0000000000000973
23. Copeland JG, Emery RW, Levinson MM, et al. Selection of patients for cardiac transplantation. Circulation. 1987;75(1):2–9. doi:10.1161/01.cir.75.1.2
24. Stepanova M, Locklear T, Rafiq N, Mishra A, Venkatesan C, Younossi ZM. Long-term outcomes of heart transplant recipients with hepatitis C positivity: the data from the U.S. transplant registry. Clin Transplant. 2016;30(12):1570–1577. doi:10.1111/ctr.12859
25. Volk ML, Hernandez JC, Lok AS, Marrero JA. Modified Charlson comorbidity index for predicting survival after liver transplantation. Liver Transpl. 2007;13(11):1515–1520. doi:10.1002/lt.21172
26. De Miguel-Díez J, López-de-Andrés A, Hernández-Barrera V, et al. Postoperative pneumonia among patients with and without COPD in Spain from 2001 to 2015. Eur J Intern Med. 2018;53:66–72. doi:10.1016/j.ejim.2018.02.011
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.