")
Back to Journals » Journal of Asthma and Allergy » Volume 9
Nasal polyps in patients with asthma: prevalence, impact, and management challenges
Received 1 October 2015
Accepted for publication 5 January 2016
Published 14 March 2016 Volume 2016:9 Pages 45—53
DOI https://doi.org/10.2147/JAA.S86251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Cristobal Langdon,1,2 Joaquim Mullol1–3
1Rhinology Unit and Smell Clinic, Otorhinolaryngology Department, Hospital Clínic, 2Clinical and Experimental Respiratory Immunoallergy (IRCE), Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), 3Centre for Biomedical Research in Respiratory Diseases (CIBERES), Barcelona, Catalonia, Spain
Abstract: Patients with chronic rhinosinusitis with nasal polyps (CRSwNP) often have coexisting asthma under the concept of “United Airway Disease”, being the combination of both diseases, which is one of the most challenging phenotypes to treat. Although clinicians have recognized this difficult-to-treat phenotype for many years, it remained poorly characterized. There is increasing epidemiological evidence linking chronic rhinosinusitis and asthma, but a good understanding of the pathophysiology and the combined management is still lacking. Bronchial asthma is more prevalent in patients who suffer chronic rhinosinusitis, while asthmatic patients have a greater prevalence of CRSwNP than patients without asthma. The effect of CRSwNP treatment, whether medical or surgical, in asthma is today less controversial after some studies have shown improvement of asthma after medical and/or surgical treatment of CRSwNP. However, direct comparisons between surgical and medical treatments are limited. Further randomized clinical trials are, however, still needed to better understand the management when both asthma and CRSwNP occur together. This review aims at summarizing the prevalence, impact, and management challenges regarding both asthma and CRSwNP.
Keywords: chronic rhinosinusitis, asthma, united airways, rhinosinusitis, corticosteroids, sinus surgery
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a chronic inflammatory disease of the upper airways. It is defined as the presence of two or more symptoms that persist for more than 12 weeks. Symptoms include facial pain/pressure, purulent nasal discharge, nasal obstruction, and decreased sense of smell during chronic inflammation and confirmed the presence of nasal polyps through endoscopy.1 On the other hand, asthma is a chronic inflammation of the lower airways involving episodic breathlessness and wheezing, with airway hyperresponsiveness to environmental stimuli, with a prevalence of 5%–10% in the general population.2 Asthmatic patients have a higher rhinosinusitis severity score than nonasthmatic patients, and more presence of nasal polyps regardless of atopic status, indicative of a strong relationship between CRSwNP severity and chronic airway inflammatory diseases.3
Since the introduction of the “United Airway Disease” concept,4 a large body of evidence from clinical epidemiology, pathophysiology, histology, and treatment outcomes has correlated asthma and CRSwNP. CRSwNP and asthma frequently coexist,1 both conditions sharing similar features of inflammation and remodeling. This association has been supported by numerous observations of similar histopathological changes5 and common inflammatory mediator infiltration.6 Typical histopathological findings of asthma, including airway remodeling (epithelial shedding and basement membrane thickening), eosinophilic infiltration, T-helper cell involvement, and IL-5 production are present in both asthma and CRSwNP, suggesting similar physiopathological processes.7,8
Although the argument for the existence of a link between upper and lower airway diseases is strong, the mechanism that underlies this connection remains under investigation. In this review, we will analyze the prevalence and the impact of management challenges regarding both asthma and CRSwNP.
Epidemiology and prevalence
CRSwNP is an inflammatory condition of the nose and paranasal sinuses of unknown cause, which is present in 2%–4% of the adult population.1,9 CRSwNP is often associated with other respiratory diseases such as asthma,10 aspirin sensitivity,11,12 and idiopathic bronchiectasis.13 It has been reported that 20%–60% of patients with CRSwNP have asthma.14–16
The association between CRSwNP and asthma patients can be considered from two different perspectives: percentage of asthmatic patients developing CRSwNP and patients diagnosed with CRSwNP and with asthma. Bronchial asthma is more prevalent in patients suffering from CRS.1,9,17 On the other hand, patients with asthma have a greater prevalence of CRS than patients without asthma.18 Jarvis et al9 included over 52,000 adults, aged 18–75 years, recruited in 19 centers from 12 European countries. In all centers and at all ages, a strong association between asthma and CRS (adjusted OR: 3.47; 95% CI: 3.20–3.76) was observed. The association with asthma was stronger in patients reporting both CRS and allergic rhinitis (adjusted OR: 11.85; 95% CI: 10.57–13.17). Dixon et al19 included 2,031 asthmatic patients and demonstrated that the association with CRS was related to severe asthma, poorly controlled asthma, and asthma exacerbations, but not to decreased lung function. Interestingly, most patients with CRS without clinical asthma showed bronchial hyperresponsiveness when a methacholine challenge test was performed. Furthermore, up to 45% of CRSwNP patients have or will develop asthma.1,9,20 The prevalence of CRSwNP is higher in asthmatics (7%) compared to the general population (4%),21 and females present a greater proportion of CRSwNP in combination with asthma.19 In addition, Caucasian patients have shown a greater prevalence of CRSwNP and asthma than Asiatic patients,22,23 while the severity of CRS is higher when concomitant asthma exists.3,24–26 In nonatopic asthma and late-onset asthma, CRSwNP was found even more frequently, from 15% to 26% depending on the study,27,28 while more than 60% of CRSwNP patients have some level of lower airway involvement.29
Aspirin-exacerbated respiratory disease (AERD), a syndrome characterized by the presence of aspirin sensitivity/intolerance, asthma, and CRSwNP, has an estimated prevalence of 1% in the general population and 10%–20% among asthmatics.1,12,30 During the natural evolution of the disease, a clinical history of rhinitis or CRS usually precedes asthma and the development of aspirin hypersensitivity. In the European Network on Aspirin-Induced Asthma cohort study, the disease followed a typical pattern: persistent rhinitis/rhinosinusitis appeared first (mean age 30 years), being associated to a flulike infection in half of the patients. This was followed by asthma after 2 years (mean age 32 years), and aspirin-induced respiratory reactions and nasal polyposis after 4 years (mean age 34 years).11 The clinical presentation in the different European countries was remarkably similar. In women, who outnumbered men by a ratio of 2.3:1, the onset of symptoms occurred significantly earlier, and the disease was more severe than in men. Once developed, CRSwNP and asthma evolution is usually independent of the aspirin and nonsteroidal anti-inflammatory drug avoidance.31
The typical clinical picture of patients with CRSwNP and asthma has been characterized by older age, longer duration of nasal symptoms, higher incidence of allergic rhinitis, bronchial obstruction, higher computed tomography (CT) and endoscopy scores, and higher number of sinonasal surgeries.3,32,33 Bilodeau et al34 showed that, among asthmatic subjects, those with CRSwNP presented more poorly controlled asthma, increased airway obstruction, and more marked lower airway inflammation than those without CRSwNP. The same authors have suggested that a subgroup of asthmatic patients may have a more intense lower airway inflammation in relation to the presence of CRSwNP. They observed that asthmatic subjects using intranasal corticosteroids (ICS) to treat nasal polyps had a more intense inflammation and a poorer asthma control compared to patients with chronic rhinosinusitis without nasal polyps, reflecting a more severe subset of asthma.
Asthma and CRSwNP have been also linked with an impaired quality of life (QoL); patients suffering from asthma and CRS reporting a poorer quality QoL.32 Alobid et al35 reported 109 patients with CRSwNP who were randomized to either receive oral prednisone for 2 weeks or to undergo endoscopic sinus surgery, all patients being treated with intranasal budesonide for 12 months. They observed a considerable impact of CRSwNP on patients’ QoL, this being even worse in patients with concomitant asthma mainly on physical functioning, body pain, and vitality (P<0.05). The same group10 evaluated different outcomes of patients with CRSwNP and found that asthma and especially persistent asthma have an accumulative impact on the loss of smell, proposing the loss of smell as a predictive symptom to identify severe asthma. Other authors have also found lower olfactory outcomes in patients who have associated CRSwNP and asthma36 or AERD.37
Management challenges
The European position paper on rhinosinusitis and nasal polyps provides a specific treatment guideline for patients with CRSwNP with and without asthma.1 On the basis of available evidence, medical therapy for CRSwNP should begin with daily application of a topical ICS in conjunction with high-volume saline irrigation, and subsequent therapies are based on the patient’s polyp status, severity of symptoms, and/or QoL impairment. Regarding the question about how sinus surgery and medical CRSwNP treatment may modify the course of bronchial asthma, different authors38,39 have concluded that the weight of evidence suggests a beneficial effect. A recent systematic review40 analyzed the effect of upper airway intervention in the subpopulation of patients with coexisting CRSwNP and asthma and did not find marked differences between outcomes after endoscopic sinus surgery (ESS) or medical treatment with montelukast, omalizumab, or erythromycin.
Medical treatments
When analyzing the evidence of medical treatment specifically for patients with CRSwNP and coexisting asthma, there are a few randomized controlled trials and uncontrolled prospective interventional studies that evaluated the efficacy of different treatments. Alobid et al35 prospectively studied 109 patients with CRSwNP with and without asthma. They observed that patients with CRSwNP have a significantly worse QoL than the general population and that steroid treatment and ESS lead to similar QoL improvement in CRSwNP, either with or without asthma; both steroid and ESS treatments improve nasal symptoms in patients with CRSwNP. Two montelukast trials with follow-up times of 10 weeks and 13 weeks were done. Schäper et al41 investigated the effect of montelukast (10 mg/d) in a double-blinded, placebo-controlled crossover trial (6 weeks of intervention, 4 weeks of placebo) in 24 patients. Short acting β-agonists and baseline doses of inhaled steroids were allowed. Ragab et al42 studied 44 patients with montelukast (10 mg/d) treatment for 3 months as an add-on therapy to inhaled steroids and intranasal steroids (INCS) in an uncontrolled prospective trial. Significant improvements in nasal and pulmonary symptoms, results of endoscopy and CT scanning of the paranasal sinuses, and asthma medication intake were reported in both trials. Nevertheless, no significant improvements were found in nasal and pulmonary function test results; however, Schäper et al41 found montelukast to increase peak expiratory flow significantly (P<0.05).
Immunoglobulin E (IgE) activates mast cells, and its levels are elevated in people with allergic diseases.1 The monoclonal antibody omalizumab lowers the level of IgE through selective binding, and anti-IgE is used in the treatment of uncontrolled allergic asthma. Omalizumab significantly improved nasal outcomes (symptoms, nasal endoscopy, and CT results) and QoL but did not significantly improve pulmonary outcomes (symptoms and pulmonary function test results). Gevaert et al43 studied 24 patients with and without allergy in a 16-week double-blinded, placebo-controlled trial. Omalizumab was given as an add-on to “standardized asthma treatment”, and during the trial oral steroids and antibiotics were prohibited. They observed significant improvements in nasal symptoms, endoscopy results, and opacification on CT scans in the omalizumab group over those in the placebo group, irrespective of allergy status. Vague results in the omalizumab group were seen in relation to the lower airways; significant improvements were found in two of three pulmonary symptoms, but no significant changes were found in pulmonary function test results. The same group,44 in a randomized, double-blind, placebo-controlled trial of 30 patients with severe nasal polyposis, observed in 12 patients who received mepolizumab (two doses) radiographic and endoscopic improvement in nasal polyp burden compared to patients in the placebo arm, after 8 weeks of treatment. Although mepolizumab led to a reduction in loss of smell, postnasal drip, and nasal congestion, these results did not reach statistical significance, and the benefit in nasal symptoms normalized after a period of time, except for improvement in olfaction. Gevaert et al45 showed that a single injection of reslizumab, another anti-IL-5 monoclonal antibody, improved nasal polyp scores in 50% of patients with CRSwNP, and nasal IL-5 levels predicted the response to treatment. These studies support that a select population of patients with severe nasal polyposis may benefit from anti-IL-5 therapy, although, once again, larger studies are needed to corroborate these findings.
Finally, in addition to the known antimicrobial effects, long-term low-dose treatment with a macrolide such as erythromycin is believed to have immunomodulatory effects. Erythromycin improved nasal symptoms and was superior to ESS in improving pulmonary outcomes (symptoms and pulmonary function test results).40 Ragab et al46 randomized a heterogeneous group of chronic rhinosinusitis without nasal polyps and CRSwNP patients with asthma who failed initial medical therapy with INCS and nasal lavage to continued medical therapy or surgery. Patients randomized to continued medical therapy received erythromycin for 12 weeks, nasal lavage, and fluticasone drops, and some patients with CRSwNP received oral steroids. Both the medical and the surgery groups had improved asthma at 12-month follow-up; evermore the continued medical therapy group (erythromycin group) had greater improvement in objective pulmonary function tests. When analyzing treatments used in both CRSwNP and asthma, the most used treatments are leukotriene antagonists, monoclonal antibodies, and macrolide antibiotics.
Surgical treatments
The surgical treatment of nasal polyps by means of ESS leads to a subjective improvement of asthma symptoms and a decrease in hospital admissions, emergency department visits, asthma exacerbations, and the need of medication for disease control. There is also growing evidence supporting that aggressive surgical management of CRSwNP can consequently lead to a greater improvement of asthma severity.47–49 Palmer et al50 retrospectively re-evaluated the clinical histories of 15 subjects who had both CRS and steroid-dependent asthma, investigating the asthma relapse days and total dose of oral corticosteroid or antibiotics needed before and after ESS. They observed that 93% of patients significantly reduced their postoperative prednisone or antibiotic needs by total number of days. Senior et al51 reported that 90% of asthmatic patients (n=30) who underwent ESS for CRS reduced the number of asthma exacerbations and need for medication after a follow-up period of 6.5 years. In the same line of research, Manning et al52 found that children with CRS and asthma (n=14) who underwent ESS had a decreased number of asthma hospitalizations and missed schooldays. Other authors36,53 have observed that asthma patients undergoing ESS for CRSwNP had a significant improvement in pulmonary function and a reduction of systemic medication, respectively, but they failed to show improvement in AERD patients. Trials studying impact of CRSwNP treatment on asthma are summarized in Table 1. Recently, Leung et al54 simulated an evidence-based risk analysis using literature-reported complication rates, QoL changes, and Medicare costs to identify the threshold at which the risks of repeated courses of corticosteroid exceeded the risks of surgery. They found that the risks of oral corticosteroid exceed the risks of ESS when patients exceed 0.20 (CRSwNP), 0.53 (CRSwNP/asthma), or 1.81 (Samter´s triad) courses of oral corticosteroids per year or need oral corticosteroid more frequently than every 5 years, 2 years, or 6 months, respectively. In ESS trials, all nasal outcomes (symptoms, nasal endoscopy, and pulmonary function test results) and QoL improved significantly although ambiguous results were reported for pulmonary outcomes (symptoms, pulmonary function test results, and asthma medication intake). A systematic review has found that ESS improves asthma control while decreasing asthma exacerbations, hospitalizations, and use of systemic and inhaled corticosteroids, pulmonary function being however unchanged.55 According to these findings, the current widespread belief is that comorbid asthmatic conditions of CRSwNP patients improve after ESS.
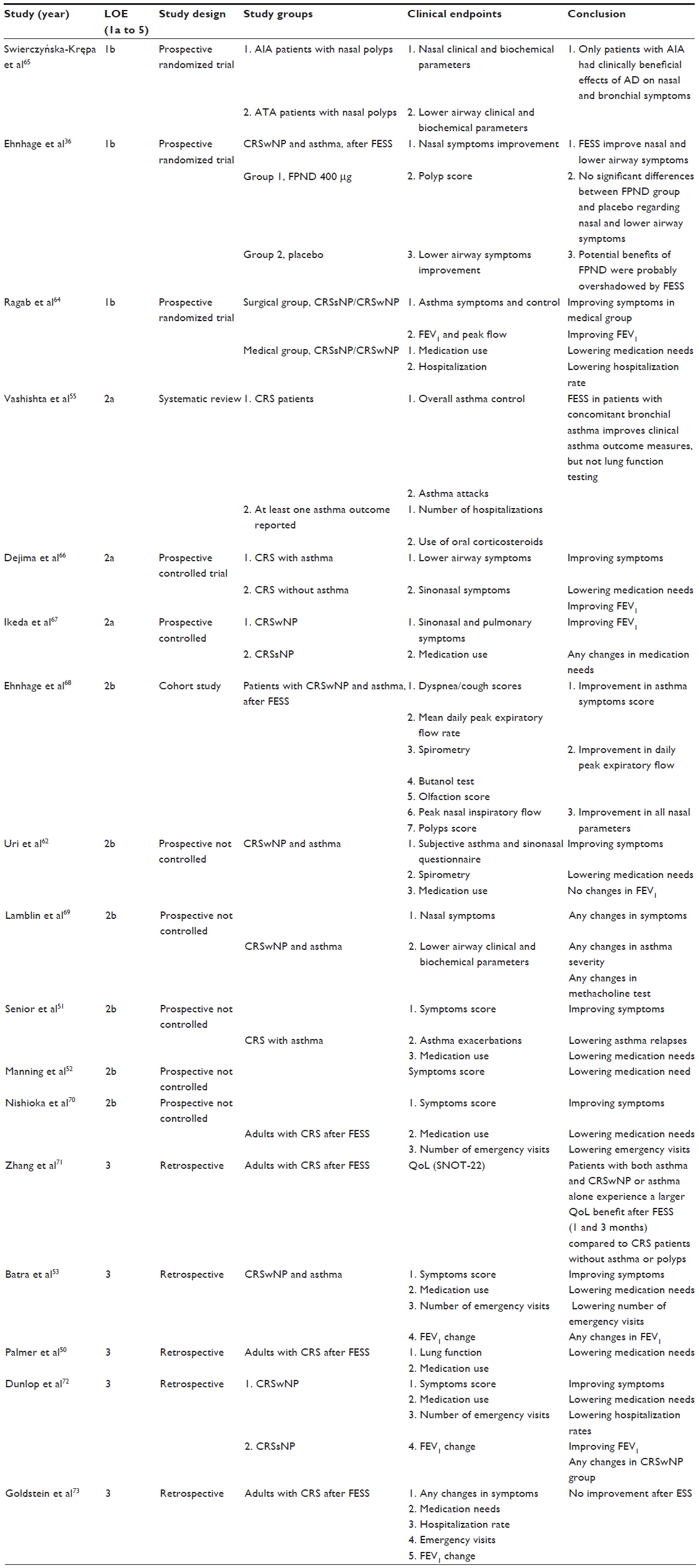 | Table 1 Trials evaluating the impact of CRS surgical treatment on asthma |
On the other hand, some authors have reported that asthma does not represent a predictor of poor symptomatic outcome after primary56,57 or revision58 ESS. Concomitant asthma was associated with worse postoperative endoscopic findings in two retrospective analyses, but had no significant weight on other objective outcomes. Symptoms improved significantly in both asthmatics and nonasthmatics postoperatively, but asthmatics exhibited worse postoperative endoscopic outcomes.59,60 In a series of 120 patients undergoing ESS, Kennedy26 reported that asthma did not affect the surgical outcomes when comparing patients with similar sinonasal disease severity, excluding the worst patients in whom asthma negatively affected the outcome. Seybt et al61 did not find differences in CRS patients with or without asthma in terms of the need for primary sinonasal surgery, but they observed that asthmatics had a significantly increased number of secondary surgeries. Uri et al62 reported that in patients with CRSwNP and asthma, ESS did not affect the asthma status. Lin et al,24 in a prospective trial including 224 CRS patients, could not confirm the beneficial effect of ESS on modifying the severity of asthma measured by objective lung function.
These findings suggest a benefit of early therapy for CRS in asthmatics if CRS is considered a reason for poor asthma control. Similarly, asthmatics with difficult-to-control illness should be assessed for unsuspected CRS, with CT scanning or nasal endoscopy, since CRS signs and symptoms may be subtle and overlooked if not specifically sought. We have highlighted that there exist only a few good quality studies of the treatment for CRSwNP with coexisting asthma, which underlines the need for further research in terms of both quality and quantity of the studies. The effect of ESS on pulmonary outcomes has been a question of great debate. We found low evidence to support a positive effect of both ESS and medical intervention on pulmonary function tests and asthma medication intake. Rix et al40 and Vashishta et al55 observed that patients who underwent ESS had an improvement in clinical asthma outcomes, but no significant change in pulmonary function test results. The effect of montelukast and other leukotriene antagonists on CRSwNP was evaluated in a recent systematic review and meta-analysis;63 improvements in symptoms and clinical outcomes were described by all 12 included studies after leukotriene antagonist treatment, but pulmonary function test results were sparse. Ragab et al64 published a randomized, prospective trial on patients with chronic rhinosinusitis without nasal polyps or CRSwNP and asthma comparing surgical versus medical treatment. They found that medical as well as surgical treatments for CRS showed improvements in asthma status with a good correlation to the improvement achieved in upper airway symptoms. Exhaled nitric oxide levels and forced expiratory volume in 1 second (FEV1) improved in both groups with predominance in the medical treatment group of patients with CRSwNP.
Conclusion
Although there has been major advances in this field, there is still a lack of consistent evidence to reach firm conclusions about the relationship between upper and lower airway inflammatory diseases, their natural history, pathophysiology, and medical/surgical management. Research on the basic pathophysiology of the nose and demonstration of the unified airway concept are mandatory. Clarification is also required concerning whether CRS management affects other comorbid lower airway diseases such as asthma, chronic obstructive respiratory disease, and bronchiectasis. Randomized clinical trials with a good level of scientific evidence need to be performed to better understand the available treatments for comorbid upper and lower inflammatory diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
Fokkens WJ, Lund VJ, Mullol J, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinology. 2012;23:1–298. | |
Bousquet J. Global initiative for asthma (GINA) and its objectives. Clin Exp Allergy. 2000;(Suppl 1):2–5. | |
Pearlman AN, Chandra RK, Chang D, et al. Relationships between severity of chronic rhinosinusitis and nasal polyposis, asthma, and atopy. Am J Rhinol Allergy. 2009;23:145–148. | |
Bousquet J, Khaltaev N, Cruz A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63 (Suppl 86):8–160. | |
Gaga M, Lambrou P, Papageorgiou N, et al. Eosinophils are a feature of upper and lower airway pathology in non-atopic asthma, irrespective of the presence of rhinitis. Clin Exp Allergy. 2000;30:663–669. | |
Braunstahl GJ, Kleinjan A, Overbeek SE, Prins JB, Hoogsteden HC, Fokkens WJ. Segmental bronchial provocation induces nasal inflammation in allergic rhinitis patients. Am J Respir Crit Care Med. 2000;161:2051–2057. | |
Ponikau JU, Sherris DA, Kephart GM, et al. Features of airway remodeling and eosinophilic inflammation in chronic rhinosinusitis: is the histopathology similar to asthma? J Allergy Clin Immunol. 2003;112:877–882. | |
Bachert C, Nan Z, Gabriele H, et al. Presence of IL-5 protein and IgE-antibodies to staphylococcal enterotoxins in nasal polyps is associated with co-morbid asthma. J Allergy Clin Immunol. 2010;126:962–968. | |
Jarvis D, Newson R, Lotvall J, et al. Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy. 2012;67:91–98. | |
Alobid I, Cardelus S, Benítez P, et al. Persistent asthma has an accumulative impact on the loss of smell in patients with nasal polyposis. Rhinology. 2011;49:519–524. | |
Szczeklik A, Nizankowska E, Duplaga M. Natural history of aspirin-induced asthma. AIANE Investigators. European Network on Aspirin-Induced Asthma. Eur Respir J. 2000;16:432–436. | |
Mullol J, Picado C. Rhinosinusitis and nasal polyps in aspirin-exacerbated respiratory disease. Immunol Allergy Clin North Am. 2013;33:163–176. | |
Guilemany JM, Angrill J, Alobid I, et al. United airways: the impact of chronic rhinosinusitis and nasal polyps in bronchiectasic patient’s quality of life. Allergy. 2009;64:1524–1529 | |
Larsen K. The clinical relationship of nasal polyps to asthma. Allergy Asthma Proc. 1996;17:243–249. | |
Zhang N, Van Zele T, Perez-Novo C, et al. Different types of T-effector cells orchestrate mucosal inflammation in chronic sinus disease. J Allergy Clin Immunol. 2008;122:961–968. | |
Klossek JM, Neukirch F, Pribil C, et al. Prevalence of nasal polyposis in France: a cross-sectional, case-control study. Allergy. 2006;60:233–237. | |
Mullol J, Guilemany JM, Alobid I. Relación de la rinitis y la rinosinusitis con la gravedad del asma. Rev Rinol. 2011;11:23–27. | |
Thorstensen WM, Bugten V, Sue-Chu M, Fossland NPW, Romundstad PR, Steinsvåg SK. Sino-nasal characteristics in asthmatic patients. Otolaryngol Head Neck Surg. 2012;147:950–957. | |
Dixon AE, Kaminsky DA, Holbrook JT, Wise RA, Shade DM, Irvin CG. Allergic rhinitis and sinusitis in asthma: differential effects on symptoms and pulmonary function. Chest. 2006;130:429–435. | |
Bousquet J, Schünemann HJ, Samolinski B; World Health Organization Collaborating Center for Asthma and Rhinitis. Allergic Rhinitis and its Impact on Asthma (ARIA): achievements in 10 years and future needs. J Allergy Clin Immunol. 2012;130:1049–1062. | |
Settipane GA, Chafee FH. Nasal polyps in asthma and rhinitis. A review of 6,037 patients. J Allergy Clin Immunol. 1977;59:17–21. | |
Bachert C, Claeys SEM, Tomassen P, van Zele T, Zhang N. Rhinosinusitis and asthma: a link for asthma severity. Curr Allergy Asthma Rep. 2010;10:194–201. | |
Bachert C, Zhang N. Chronic rhinosinusitis and asthma: novel understanding of the role of IgE “above atopy.” J Intern Med. 2012;272:133–143. | |
Lin DC, Chandra RK, Tan BK, et al. Association between severity of asthma and degree of chronic rhinosinusitis. Am J Rhinol Allergy. 2011;25:205–208. | |
Zhang Z, Linkin DR, Finkelman BS, et al. Asthma and biofilm forming bacteria are independently associated with revision sinus surgeries for chronic rhinosinusitis. J Allergy Clin Immunol. 2011;128:221–223. | |
Kennedy DW. Prognostic factors, outcomes and staging in ethmoid sinus surgery. Laryngoscope. 1992;102(Suppl 57):1–18. | |
Mariño FS, Alobid I, Guilemany JM, Mullol J, Obando A. Tratamiento médico y quirúrgico de la poliposis nasal. Efecto sobre el asma. Rev Rinol. 2009;9:26–32. | |
Hedman J, Kaprio J, Poussa T, Nieminen M. Prevalence of asthma, aspirin intolerance, nasal polyposis and chronic obstructive pulmonary disease in a population-based study. Int J Epidemiol. 1999;4:717–722. | |
Ragab A, Clement P, Vincken W. Objective assessment of lower airway involvement in chronic rhinosinusitis. Am J Rhinol. 2004;18:15–21. | |
Szczeklik A, Stevenson DD. Aspirin-induced asthma: advances in pathogenesis, diagnosis, and management. J Allergy Clin Immunol. 2003;111:913–921. | |
Berges-Gimeno MP, Simon RA, Stevenson DD. The natural history and clinical characteristics of aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol. 2002;89:474–478. | |
Lehrer E, Mullol J, Agredo F, Alobid I. Management of chronic rhinosinusitis in asthma patients: is there still a debate? Curr Allergy Asthma Rep. 2014;14:440. | |
Staikniene J, Vaitkus S, Japertiene LM, Ryskiene S. Association of chronic rhinosinusitis with nasal polyps and asthma: clinical and radiological features, allergy and inflammation markers. Med (Kaunas). 2008;44:257–265. | |
Bilodeau L, Boulay ME, Prince P, Boisvert P, Boulet LP. Comparative clinical and airway inflammatory features of asthmatics with or without polyps. Rhinology. 2010;48:420–425. | |
Alobid I, Benítez P, Bernal-Sprekelsen M, et al. Nasal polyposis and its impact on quality of life: comparison between the effects of medical and surgical treatments. Allergy. 2005;60:452–458. | |
Ehnhage A, Olsson P, Kölbeck K-G, et al. Functional endoscopic sinus surgery improved asthma symptoms as well as PEFR and olfactionin patients with nasal polyposis. Allergy. 2009;64:762–769. | |
Alobid I, Benítez P, Cardelús S, et al. Oral plus nasal corticosteroids improve smell, nasal congestion, and inflammation in sino-nasal polyposis. Laryngoscope. 2014;124:50–56. | |
Lund VJ. The effect of sinonasal surgery on asthma. Allergy. 1999; 54(Suppl 57):141–145. | |
Scadding G. The effect of medical treatment of sinusitis upon concomitant asthma. Allergy. 1999;54(Suppl 57):136–140. | |
Rix I, Håkansson K, Larsen CG, Frendø M, von Buchwald C. Management of chronic rhinosinusitis with nasal polyps and coexisting asthma: a systematic review. Am J Rhinol Allergy. 2015;29:193–201. | |
Schäper C, Noga O, Koch B, et al. Anti-inflammatory properties of montelukast, a leukotriene receptor antagonist in patients with asthma and nasal polyposis. J Investig Allergol Clin Immunol. 2011;21:51–58. | |
Ragab S, Parikh A, Darby YC, Scadding GK. An open audit of montelukast, a leukotriene receptor antagonist, in nasal polyposis associated with asthma. Clin Exp Allergy. 2001;31:1385–1391. | |
Gevaert P, Calus L, Van Zele T, et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J Allergy Clin Immunol. 2013;131:110–116. | |
Gevaert P, Van Bruaene N, Cattaert T, et al. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J Allergy Clin Immunol. 2011;128:989–995. | |
Gevaert P, Lang-Loidolt D, Lackner A, et al. Nasal IL-5 levels determine the response to anti-IL-5 treatment in patients with nasal polyps. J Allergy Clin Immunol. 2006;118:1133–1141. | |
Ragab SM, Lund VJ, Scadding G. Evaluation of the medical and surgical treatment of chronic rhinosinusitis: a prospective, randomised, controlled trial. Laryngoscope. 2004;114:923–930. | |
DeMarcantonio MA, Han JK. Nasal polyps: pathogenesis and treatment implications. Otolaryngol Clin North Am. 2011;44:685–695. | |
Ebbens FA, Toppila-Salmi SK, Renkonen JA, et al. Endothelial L-selectin ligand expression in nasal polyps. Allergy. 2010;65:95–102. | |
van Drunen CM, Reinartz S, Wigman J, Fokkens WJ. Inflammation in chronic rhinosinusitis and nasal polyposis. Immunol Allergy Clin North Am. 2009;29:621–629. | |
Palmer JN, Conley DB, Dong RG, Ditto AM, Yarnold PR, Kern RC. Efficacy of endoscopic sinus surgery in the management of patients with asthma and chronic sinusitis. Am J Rhinol. 2001;15:49–53. | |
Senior BA, Kennedy DW, Tanabodee J, Kroger H, Hassab M, Lanza DC. Long-term impact of functional endoscopic sinus surgery on asthma. Otolaryngol Head Neck Surg. 1999;121:66–68. | |
Manning SC, Wasserman RL, Silver R, Phillips DL. Results of endoscopic sinus surgery in pediatric patients with chronic sinusitis and asthma. Arch Otolaryngol Head Neck Surg. 1994;120:1142–1145. | |
Batra PS, Kern RC, Tripathi A, et al. Outcome analysis of endoscopic sinus surgery in patients with nasal polyps and asthma. Laryngoscope. 2003;113:1703–1706. | |
Leung RM, Dinnie K, Smith TL. When do the risks of repeated courses of corticosteroids exceed the risks of surgery? Int Forum Allergy Rhinol. 2014;4:871–876. | |
Vashishta R, Soler ZM, Nguyen SA, et al. A systematic review and meta-analysis of asthma outcomes following endoscopic sinus surgery for chronic rhinosinusitis. Int Forum Allergy Rhinol. 2013;3:788–794. | |
Mehanna H, Mills J, Kelly B, McGarry GW. Benefit from endoscopic sinus surgery. Clin Otolaryngol Allied Sci. 2002;27:464–471. | |
Chambers DW, Davis WE, Cook PR, Nishioka GJ, Rudman DT. Long-term outcome analysis of functional endoscopic sinus surgery: correlation of symptoms with endoscopic examination findings and potential prognostic variables. Laryngoscope. 1997;107:504–510. | |
Kountakis SE, Bradley DT. Effect of asthma on sinus computed tomography grade and symptom scores in patients undergoing revision functional endoscopic sinus surgery. Am J Rhinol. 2006;17:215–219. | |
Smith TL, Mendolia-Loffredo S, Loehrl TA, Sparapani R, Laud PW, Nattinger AB. Predictive factors and outcomes in endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope. 2005;115:2199–2205. | |
Marks SC, Shamsa F. Evaluation of prognostic factors in endoscopic sinus surgery. Am J Rhinol. 1997;11:187–191. | |
Seybt MW, McMains KC, Kountakis SE. The prevalence and effect of asthma on adults with chronic rhinosinusitis. Ear Nose Throat J. 2007;86:409–411. | |
Uri N, Cohen-Kerem R, Barzilai G, Greenberg E, Doweck I, Weiler-Ravell D. Functional endoscopic sinus surgery in the treatment of massive polyposis in asthmatic patients. J Laryngol Otol. 2002;116:185–189. | |
Wentzel JL, Soler ZM, DeYoung K, et al. Leukotriene antagonists in nasal polyposis: a meta-analysis and systematic review. Am J Rhinol Allergy. 2013;27:482–489. | |
Ragab S, Scadding GK, Lund VJ, et al. Treatment of chronic rhinosinusitis and its effects on asthma. Eur Respir J. 2006;28:68–74. | |
Swierczyska-Krpa M, Sanak M, Bochenek G, et al. Aspirin desensitization in patients with aspirin-induced and aspirin-tolerant asthma: a double-blind study. JACI. 2014;134:883–890. | |
Dejima K, Hama T, Miyazaki M, et al. A clinical study of endoscopic sinus surgery for sinusitis in patients with bronchial asthma. Int Arch Allergy Immunol. 2005;138:97–104. | |
Ikeda K, Tanno N, Tamura G, et al. Endoscopic sinus surgery improves pulmonary function in patients with asthma associated with chronic sinusitis. Ann Otol Rhinol Laryngol. 1999;108:355–359. | |
Ehnhage A, Olsson P, Kölbeck KG, Skedinger M, Stjärne P; NAFS Study Group. One year after endoscopic sinus surgery in polyposis: asthma, olfaction, and quality-of-life outcomes. Otolaryngol Head Neck Surg. 2012;146:834–841. | |
Lamblin C, Brichet A, Perez T, Darras J, Tonnel AB, Wallaert B. Long-term follow-up of pulmonary function in patients with nasal polyposis. Am J Respir Crit Care Med. 2000;161:406–413. | |
Nishioka GJ, Cook PR, Davis WE, McKinsey JP. Functional endoscopic sinus surgery in patients with chronic sinusitis and asthma. Otolaryngol Head Neck Surg. 1994;110:494–500. | |
Zhang Z, Adappa ND, Doghramji LJ, et al. Quality of life improvement from sinus surgery in chronic rhinosinusitis patients with asthma and nasal polyps. Int Forum Allergy Rhinol. 2014;4:885–892. | |
Dunlop G, Scadding GK, Lund VJ. The effect of endoscopic sinus surgery on asthma: management of patients with chronic rhinosinusitis, nasal polyposis, and asthma. Am J Rhinol. 1999;13:261–265. | |
Goldstein MF, Grundfast SK, Dunsky EH, Dvorin DJ, Lesser R. Effect of functional endoscopic sinus surgery on bronchial asthma outcomes. Arch Otolaryngol Head Neck Surg. 1999;125:314–319. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.