")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
N-Acetylcysteine to Combat COVID-19: An Evidence Review
Received 24 July 2020
Accepted for publication 8 October 2020
Published 2 November 2020 Volume 2020:16 Pages 1047—1055
DOI https://doi.org/10.2147/TCRM.S273700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Zhongcheng Shi,1,2 Carlos A Puyo3
1Department of Pathology and Immunology, Baylor College of Medicine, Houston, TX, USA; 2Department of Pathology, Texas Children’s Hospital, Houston, TX, USA; 3Department of Anesthesia and Critical Care, Holy Family Hospital, Steward Health Care, Methuen, MA, USA
Correspondence: Zhongcheng Shi Tel +1- 832-824-0814
Email [email protected]
Abstract: The novel coronavirus disease (COVID-19) is caused by a virus (SARS-Cov-2) and is known for inducing multisystem organ dysfunction associated with significant morbidity and mortality. Current therapeutic strategies for COVID-19 have failed to effectively reduce mortality rate, especially for elderly patients. A newly developed vaccine against SARS-Cov-2 has been reported to induce the production of neutralizing antibodies in young volunteers. However, the vaccine has shown limited benefit in the elderly, suggesting an age-dependent immune response. As a result, exploring new applications of existing medications could potentially provide valuable treatments for COVID-19. N-acetylcysteine (NAC) has been used in clinical practice to treat critically ill septic patients, and more recently for COVID-19 patients. NAC has antioxidant, anti-inflammatory and immune-modulating characteristics that may prove beneficial in the treatment and prevention of SARS-Cov-2. This review offers a thorough analysis of NAC and discusses its potential use for treatment of COVID-19.
Keywords: N-acetylcysteine, SARS-Cov-2, COVID-19
Introduction
According to the CDC, most SARS-Cov-2 infected individuals can recover from the disease at home. However, this virus can also cause serious illness in immune-compromised individuals, elderly patients, and in those with certain preexisting health conditions, such as hypertension, diabetes, and cardiovascular disease.1 It takes approximately 7 days to develop computed tomography (CT)-confirmed pneumonia (COVID-19) from the onset symptoms, such as fever or dry cough, and another 2 days to progress to acute respiratory distress syndrome (ARDS).2 ARDS is the major cause of death for COVID-19 patients and is associated with dysregulated host immune responses following viral infection.
One of the early immune responses during viral infection is the production of cytokines and chemokines from immune cells. High levels of IL-8, a strong chemoattractant for neutrophils, has been detected early in infected SARS patients.3 Once activated by infection, neutrophils are rapidly recruited to sites of inflammation in the lungs, where they produce and secrete cytokines, enzymes, including elastase (NE), reactive oxygen species (ROS) by oxidative burst, and finally release DNA to form neutrophil extracellular traps (NETs).4 In severe COVID-19 patients, an increased number of neutrophils has been associated with disease severity,5 most likely due to the production of large amounts of proinflammatory cytokines, creating a “cytokine storm”.
In neutrophils, NE can degrade a wide variety of architecturally and functionally important molecules, such as clotting factors and complement proteins.6 NE activity may, in part, explain the significant increase of D-dimer and pulmonary hemorrhage observed in COVID-19 patients.2 Additionally, NET-bound NE can degrade local plasminogen without generating plasmin onto fibrin, thus resulting in impaired fibrinolysis. This suggests that NE-bound NETs have the potential to serve as a platform for activation and formation of intravascular coagulation,7,8 which partly explains why pulmonary embolism usually occurs in critical COVID-19 patients in the intensive care unit (ICU).9 In some critically ill COVID-19 patients, the coexistence of thrombosis and hemorrhage was observed,10 indicating that suppression of NE production by stabilizing neutrophils could be beneficial for either condition. For instance, inhibiting neutrophil activation by an IL-8 antibody can effectively combat acute lung injury.11,12 In other words, any measure that can suppress neutrophil activation might improve the outcomes of COVID-19 patients.
Cellular immunity is also required for a host to fight a viral infection, which is regulated by an oxidant-antioxidant balance. This balance is maintained by antioxidants including glutathione. In the immune cells of senior or immune-compromised individuals, ROS is increased due to decreased glutathione, which causes dysregulation of immune responses, particularly of T cell-mediated functions. This may explain the depressed cell-mediated immunity and increased mortality found in elderly persons as a result of infectious diseases, such as pneumonia.13,14 In fact, in addition to depressed functions, the number of lymphocytes, including both CD4+ and CD8+ T cells, was found to decrease linearly with age.15 Furthermore, a reduced number of T cells as a result of apoptosis was also observed in critical COVID-19 patients, which further compromised cellular immunity and was associated with the higher mortality for these populations.2,16 Therefore, replenishing certain antioxidants may restore the normal responses of immune cells through inhibiting T cell apoptosis, potentially reducing incidence or severity of pneumonia due to virus infection.
Combining count changes of neutrophils and lymphocytes, several groups have recently revealed that a high neutrophil-to-lymphocyte ratio (NLR) predicts a more severe progression of the disease and worse outcomes for COVID-19 patients,17–19 suggesting that NLR may be used as a prognostic marker and a therapeutic guide during acute COVID-19 infection. Therefore, in addition to administration of anti-viral drugs, inhibiting neutrophil activation and protecting T cells could provide an effective therapeutic option for treating COVID-19 patients.
Theoretically, an effective vaccine would be the best solution to combat SARS-cov-2 infection. A recent study showed that a recombinant adenovirus type-5 (Ad5) vaccine was capable of inducing neutralizing antibodies at day 14 post-vaccination,20 suggesting that a quick control of the COVID-19 pandemic is a possibility. However, this study also found that the neutralizing antibodies were reduced between the ages of 45 to 60 when compared with younger people. Since younger people are widely considered the major carriers and spreaders of SARS-Cov-2, effective vaccines are still desperately needed to reduce virus transmission. Meanwhile, exogenous neutralizing antibodies may help those not responsive to the SARS-Cov-2 vaccines. Unfortunately, both vaccines and neutralizing antibodies are still under development. Therefore, a multimodal approach may be necessary when treating COVID-19 in elderly patients or in those with preexisting conditions.
Evidence and Discussions
N-Acetylcysteine, a Forgotten Immune-Modulating Agent
N-acetylcysteine (NAC), a precursor of the antioxidant glutathione, has been used to loosen thick mucus in the lungs and treat acetaminophen overdose for decades. However, NAC can also boost the immune system, suppress viral replication, and reduce inflammation. Despite these valuable features, NAC has been mostly overlooked throughout SARS-Cov and MERS-Cov epidemics, as well as the current COVID-19 pandemic.
In 1997, De Flora et al demonstrated that oral administration of NAC (600mg, bid) significantly improved cell-mediated immunity, shifting from anergy to normoergy in seniors (Figure 1A).21 Anergy represents a lack of reaction from immune cells to foreign substances, such as bacteria and viruses. Unsurprisingly, NAC treatment significantly decreased the frequency of influenza, as well as the severity and duration of most symptoms (Figure 1B). Although the infection rates of influenza virus (H1N1 Singapore 6/86) were similar in the two groups, only 25% of virus-infected subjects in NAC group developed flu symptoms, contrasting with 79% of the subjects in the placebo group. As a result, NAC may improve compromised cellular immunity and prevent development of certain respiratory virus-caused diseases, thus raising the question: Can NAC administration benefit COVID-19 patients?
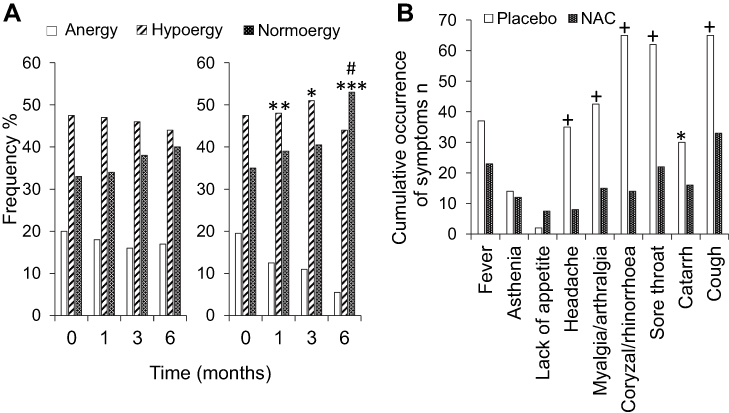 |
Figure 1 (A) Effect of NAC treatment on cell-mediated immunity. Left: Placebo group; Right: NAC-treated group. *p <0.05; **p<0.01; ***p<0.001, significance of difference in the frequency of anergy, within the NAC group, after 1, 3 and 6 months, compared to the start of the study (time 0); #p<0.05, significance of difference in the frequency of anergy between the NAC group and the placebo group. (B) Effect of NAC treatment on the cumulative occurrence of individual influenza-like signs and symptoms. *p<0.05; +p<0.0001, significance of difference between the frequency of symptoms in the NAC group and the placebo group. Reproduced with permission from De Flora S, Grassi C, Carati L. Attenuation of influenza-like symptomatology and improvement of cell-mediated immunity with long-term N-acetylcysteine treatment. European Respiratory Journal. 1997;10: 1535–1541.21 |
NAC Offers the Following Key Features to Combat COVID-19
Anti-Virus Functions of NAC
RNA viruses need active NF-κB pathway support within host cells in order to replicate. For human coronaviruses (HCoV-229E), suppression of NF-κB significantly reduced the replication rate.22 Therefore, drugs that inhibit NF-κB activation could potentially reduce viral replication.
NAC has been demonstrated to inhibit NF-κB, as well as the replication of human influenza viruses (H5N1, Vietnam/VN1203 strain) in human lung epithelial cells in a dose dependent manner (5 to 15 mM) (Figure 2). NAC also reduced the production of pro-inflammatory cytokines (IL-8, CXCL10, CCL5 and IL-6), thus reducing chemotactic migration of monocytes.23 In addition, NAC has also been showed to inhibit replication of other viruses, such as human immunodeficiency virus (HIV)24 and respiratory syncytial virus (RSV).25 This means that, theoretically, NAC has the potential to inhibit SARS-Cov-2 as well because of its ability to negatively regulate NF-κB.
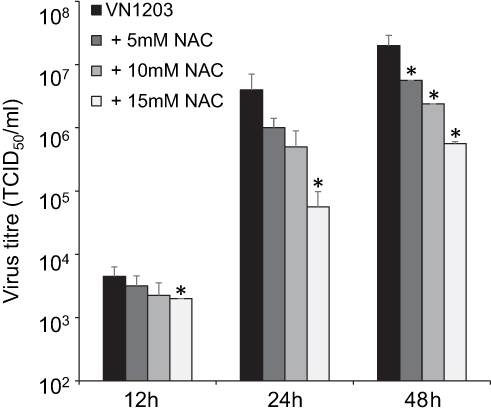 |
Figure 2 Influence of NAC on H5N1 virus replication in A549 cells. A549 cells were infected with A/Vietnam/1203/04 (VN1203) at a MOI of 0.01. NAC treatment (0 mM NAC: dark grey bars, 5 mM NAC: middle grey bars, 10 mM NAC: light grey bars, 15 mM NAC: white bars) was performed continuously starting 24 h prior to infection. H5N1 titres were determined 12, 24 and 48 h post-infection. *p<0.05 relative to untreated virus control. Reprinted from Biochemical Pharmacology, 79, Geiler J, Michaelis M, Naczk P, et al. N-acetyl-L-cysteine (NAC) inhibits virus replication and expression of pro-inflammatory molecules in A549 cells infected with highly pathogenic H5N1 influenza A virus. 413–420, Copyright (2010), with permission from Elsevier.23 |
In SARS-Cov-2, main protease (Mpro) is required for viral replication. As a result, many researchers have sought to develop inhibitors specifically targeting Mpro. Zhang et al provided the crystal structure of Mpro and designed the small compound 13b, which can efficiently inhibit SARS-CoV-2 replication in human lung cells.26 However, it will likely take years for this promising Mpro inhibitor to advance to clinical application. Guthappa suggested that NAC may bind to Cys-145, an active site of Mpro, which could potentially inhibit its protease activity and then inhibit viral replication.27 Thus, NAC could serve as a first-line drug specifically for SARS-Cov-2 due to its structural characteristics.
Immune-Modulating Properties of NAC
It has been demonstrated that NAC can change the redox balance towards reduced status inside neutrophils by replenishing reduced glutathione (GSH), which suppresses NF-κB activation at concentrations of 10mM or more, resulting in modulation of cytokine production and chemotactic signals.28 Moreover, neutrophils from healthy volunteers taking NAC (600 mg daily) for 14 days showed lower rates of oxidative burst and chemotaxis. NAC also suppressed elastase release from neutrophils induced by formyl-methionyl-leucyl-phenylalanine (fMLP) in a dose dependent manner, as the elastase was completely abolished by 10mM NAC (Figure 3). Monocyte chemotaxis can also be inhibited by clinically accessible concentrations of NAC.29 When it comes to considering even higher doses of NAC, another study showed that oral administration of 1200 mg of NAC significantly reduced oxidative bursts from neutrophils induced by the stimulants C. albicans, fMLP, and PMA. Interestingly, NAC did not compromise other functions of neutrophils, such as phagocytosis and bacterial killing.30 Collectively this data supports the notion that 1200 mg of oral NAC can effectively reduce ROS production without compromising phagocytosis of SARS-Cov-2 in neutrophils.
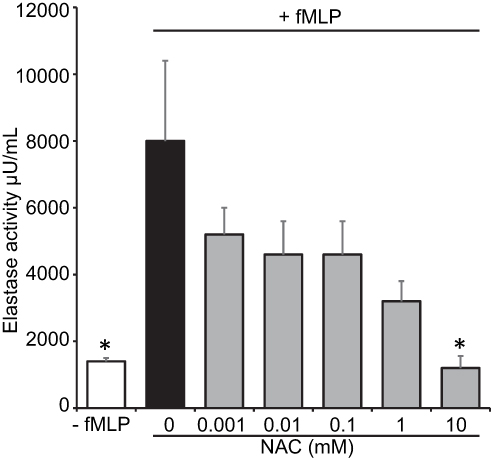 |
Figure 3 The effect of 30 min incubation of neutrophils with different NAC concentrations on the fMLP (10−7 M induced release of elastase by neutrophils in vitro. *p<0.05 when compared to the preincubation without NAC. Reprinted from Pharmacological Research, 53, Sadowskaa AM, Manuel-y-Keenoy B, Vertongen T, et al. Effect of N-acetylcysteine on neutrophil activation markers in healthy volunteers: In vivo and in vitro study. 216–225, Copyright (2006), with permission from Elsevier.28 |
In severe COVID-19 patients, a SARS-cov-2 infection frequently causes lymphopenia, especially for T cells.31 NAC can increase intracellular GSH in human T cells and block apoptosis induced by pro-apoptosis Fas antigen/Fas ligand lethal signal32 that is upregulated during virus infections, such as HIV, HCV and influenza. Lai et al demonstrated that 2400 mg of oral NAC (1200 mg, bid) quickly increased glutathione levels in lymphocytes during a chronic inflammatory disease, which was not achieved by a low-dose NAC (600 mg, bid).33 We therefore expect that high-dose oral NAC (1200 mg, bid) can improve adaptive immunity by elevating glutathione levels in lymphocytes, in addition to modulating neutrophil functions during COVID-19 development.
NAC Can Reduce the Incidence of Pneumonia
Given that oral NAC (600mg, bid) significantly decreased the frequency and severity of influenza, oral NAC may reduce the incidence of pneumonia as well. One study has demonstrated that about 37% of mechanically ventilated patients develop pneumonia, namely, ventilator-associated-pneumonia (VAP) in an intensive care unit. NAC (600 mg, bid) treated patients developed significantly less clinically confirmed pneumonia compared with placebo group patients (26.6% VS 46.6%).34 Another study showed that oral (600mg, bid) NAC significantly reduced the levels of TNF and malondialdehyde (MDA) and significantly improved oxidative stress.35 Modulation of the inflammatory process with antioxidants may have a mitigating effect in the development of pneumonia, potentially improving outcomes if high doses of NAC (1200mg, bid) are utilized.
Improve Lung Function to Reduce Mortality Rate by Intravenous NAC
Virus induced “Cytokine storm” has been closely linked with the mortality in COVID-19 patients.36 In addition to secreting cytokines, neutrophils also produce ROS radicals. ROS are chemically reactive oxygen-containing species, such as superoxide, peroxides, hydroxyl radical, singlet oxygen and alpha-oxygen, etc. Superoxide anion radicals (O2−) can cause injury directly and can be converted into more damaging oxidant species such as hydroxyl radical (OH−) and hypochlorous acid (HOCl).37 Of the two, OH− has been demonstrated as the key reactive oxygen species to cause pulmonary edema during acute lung injury.38 Hypoxemia secondary to Adult Respiratory Distress Syndrome (ARDS) and pulmonary edema may occur during COVID-19 infection.39 Besides causing tissue injury, ROS can also activate the NF-kB pathway to amplify inflammation through upregulation of expression of multiple genes, such as IL-6, TNF-α, and chemokines. NAC, a powerful scavenger of OH−,40 could effectively prevent cytokine storm and ROS-induced pulmonary edema and respiratory failure.
In patients with mild-to-moderate acute lung injury, intravenous (IV) NAC treatment (40mg/kg/day) for 3 days significantly improved systemic oxygenation, reduced the need for ventilatory support and also slightly reduced the mortality rate,41 suggesting that higher concentrations of IV NAC could be administrated, potentially improving clinical outcomes.
A case report revealed the significance of NAC treatment for a patient with septic shock from an influenza (H1N1) infection. Together with oseltamivir, intravenous infusion of NAC at 100 mg/kg/day for 3 days rapidly improved the patient’s sepsis conditions with resolution of lung infiltrates. However, the patient relapsed after cessation of the NAC infusion. Then, reinstating the infusion of NAC at the same dose rapidly improved the patient’s conditions again, until the viruses were eventually eradicated, and the patient was discharged.42 This case suggests that high concentration and enough exposure time of NAC is the key to treat virus-caused critical conditions, including pneumonia-mediated sepsis.
Another promising study revealed that in ARDS and acute ALI patients, IV NAC at a loading dose of 150 mg/kg at the first day, followed by a dose of 50 mg/kg/day for 3 days, not only improved oxygenation, but also decreased mortality rate (35.7% VS 76.9%) compared to control patients (p < 0.05).43 Although this cohort is relatively small, its results are dramatic, further suggesting that IV NAC can be used to treat severe COVID-19 and reduce mortality, given enough dosage and treating time.
Case Reports and Clinical Trials Using NAC to Treat COVID-19 Patients
A recent case report demonstrated that using low-dose hydroxychloroquine (HCQ) and IV NAC had a positive impact on a 54-year-old male COVID-19 patient, with a history of hypertension, hyperlipidemia, and obesity. Multi-system end-organ damage was diagnosed and the patient was given a low-dose oral HCQ (total 600 mg) in combination with IV NAC, at a loading dose of 75 mg/kg for 4 hours, then 35 mg/kg for 16 hours, followed by 17 mg/kg for 24 hours. The patient gradually recovered (NLR from 16.7 to 2.4) despite pulmonary embolism and short-term mechanical ventilation. He was then released from intensive care on day 7 and eventually discharged on post-admission day 12.44
In another case report, a 64-year-old male COVID-19 patient developed respiratory failure on day 13 post-admission, despite being treated with antibiotics, antiviral and respiratory support. Together with other treatments, a large dose (10–15 g) of NAC inhalation repeated for 11 days significantly improved his critical conditions. The patient was eventually discharged after 26 days of mechanical ventilation and 46 days of hospitalization.45 Another two COVID-19 patients with dyspnea were effectively treated with oral and IV glutathione, NAC and alpha lipoic acid,46 further suggesting that remediation of oxidative stress could be a key in combating COVID-19.
Recently, in a larger cohort study, Ibrahim et al have demonstrated that IV NAC significantly improved disease conditions in 10 severe respirator-dependent COVID-19 patients, aged from 38 to 71 years, including one with Glucose-6-phosphate dehydrogenase (G6PD) deficiency. IV NAC administration significantly reduced inflammatory markers, such as C-reactive protein (CRP) and ferritin, and also improved lung functions. Eight patients were eventually discharged, and two remaining patients showed improved conditions by the date of publication.47 This clinical practice further proves the effectiveness of NAC in COVID-19 treatment. Since NAC is a stronger antioxidant and less expensive than glutathione, the significance of NAC-mediated treatments for COVID-19 patients should be emphasized, at least as part of a multimodal approach.
To date, there are 6 clinical trials using NAC regarding COVID-19 treatments, 4 of them (NCT04545008; NCT04419025; NCT04455243; NCT04466657) have not recruited patients yet. In the other 2 trials that are recruiting patients, one of them (NCT04370288) was designed with the combination of NAC, Methylene Blue and vitamin C, making the interpretation of NAC effect difficult. And another study (NCT04374461) is scheduled for completion date in May 2021. Without effective treatments, COVID-19 could make severe consequences in terms of morbidity and mortality. As a dietary supplement, NAC has been used increasingly worldwide. During this COVID-19 pandemic, NAC can potentially prevent development of critical pneumonia for the people sensitive to SARS-CoV-2 infections. It also provides the potential references of how to use NAC for ongoing clinical trials. In addition, NAC features and its successful application for treating COVID-19 may encourage patients to enroll into the clinical trials using NAC.
Routes and Doses of NAC Administration
IV Infusion of NAC
To treat acetaminophen overdose for adults based on a FDA approved 3-bag regime, NAC (Molecular weight: 163) is administrated intravenously, initially 150 mg/kg in 200 mL of 5% dextrose for 60 minutes (first bag), followed by 50 mg/kg in 500 mL of 5% dextrose for 4 hours (second bag), and then 100 mg/kg in 1000 mL of 5% dextrose for 16 hours (third bag).48 Given that the average American male (20 years or older) weighs about 90 kg with about 7000 mL of blood, 13.5 g of NAC in 200 mL (414 mM) of 5% dextrose can be infused in one hour. Based on the calculations of two studies,49,50 the approximate NAC concentration in blood should be about 1 mM during infusion of the first bag, which is enough to neutralize the potent oxidant species, suppress oxidative burst, and substantially reduce neutrophil chemotaxis and cytokine storm.
Oral Administration of NAC
The gut is the largest immune organ we have,51 carrying 70% of all lymphocytes in the body. Absorbed in the small intestine, oral NAC interacts with epithelial cells and immune cells, potentially boosting our immune system to combat virus infection. One capsule of 600 mg NAC can reach a level of 16 μM NAC in the peripheral blood in half an hour after administration. Although it has been labeled as “low bioavailability” for decades, if administrated within 8–10 hours of acetaminophen overdose, oral administration of NAC displays the same capacity of detoxification as given by the IV route.52
NAC Inhalation
Under FDA guideline, to loosen mucus, MAYO clinic suggests inhaling 3 to 5 milliliters (mL) of a 20% solution or 6 to 10 mL of a 10% solution using a nebulizer, three or four times a day. For NAC, 10% is equivalent to 613 mM. Highly concentrated NAC can effectively reduce viral replication and significantly alleviate pneumocyte damage, as well as excessive immune responses.
Availability and Cost of NAC
The affordable generic NAC has been used increasingly as a dietary supplement in the US and Europe. For example, a 600 mg NAC capsule costs about 0.07–0.1 dollars on the market. The other acetylcysteine formulations are also commercially available in the US as generic and brand-name drugs, such as Mucomyst for nebulizer administration (prescription needed, 10mL of 10% NAC costs about $6 with insurance, and about $3.8 with an online coupon) and Acetadote for intravenous administration.
The Strategy of NAC Administration
To protect those who have not contracted SARS-Cov-2, oral NAC (600 mg, bid) could be an effective and economical measurement to modulate their immune systems against potential infection. Once onset symptoms appear, such as fever or dry cough, oral NAC (1200 mg, bid) could be taken to alleviate symptoms and accelerate recovery from virus infection.
For relatively severe patients without airway obstructions, an inhalable formula of NAC can be used with a nebulizer. Patients with allergies or asthma should take antihistamine before or during NAC inhalation, to prevent adverse reactions. Self-treatment with oral or inhalable NAC could help many SARS-Cov-2 infected patients safely recover at home.
Once patients develop clinically confirmed pneumonia or dyspnea, in addition to regular therapy, such as Remdesivir,53 IV NAC should be given intermittently or continuously. This could then prevent development of ARDS, which often entails invasive ventilation and intensive care unit support. For example, NAC can be infused at a dose of 100 mg/kg for at least 3 days, which equals to about 1/3 of the total dose during a 3-bag regime. There is no difference between intermittent and continuous infusion of NAC regarding patient outcomes.54
When a patient develops ARDS, along with regular antiviral therapy, 150 mg/kg at the first day, followed by a dose of 100 mg/kg/day for at least 3 days, should be administrated to avoid irreversibly fatal multiple organ failure (MOF). Once MOF or critical sepsis occurs, patients likely will not benefit from any NAC administration.55 A brief overview of a NAC therapeutic strategy to combat COVID-19 has been summarized in Figure 4.
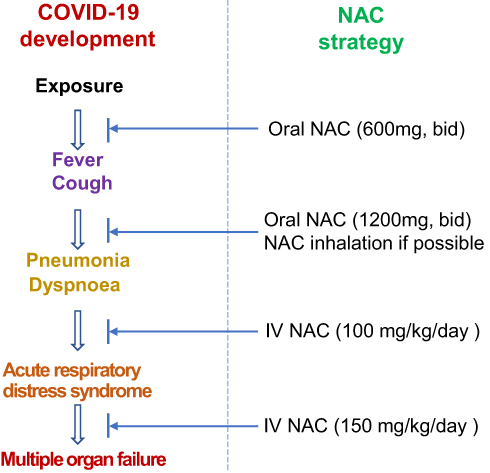 |
Figure 4 A brief overview of a NAC therapeutic strategy to combat COVID-19. |
Conclusions
N-acetylcysteine (NAC) is inexpensive, has very low toxicity, has been FDA approved for many years, and has the potential to improve therapeutic strategies for COVID-19. NAC administered intravenously, orally, or inhaled, may suppress SARS-CoV-2 replication and may improve outcomes if used timely. Potential therapeutic benefits of NAC include, extracellularly scavenging ROS radicals, replenishing intracellular GSH, suppression of cytokine storm, and T cell protection, thus mitigating inflammation and tissue injury. NAC administration in combination with other antiviral agents may dramatically reduce hospital admission rate, mechanical ventilation and mortality.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Jamwal S, Gautam A, Elsworth J, et al. An updated insight into the molecular pathogenesis, secondary complications and potential therapeutics of COVID-19 pandemic. Life Sci. 2020;257:118105. doi:10.1016/j.lfs.2020.118105
2. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
3. Huang KJ, Su IJ, Theron M, et al. An interferon-γ-related cytokine storm in SARS patients. J Med Virol. 2005;75:185–194. doi:10.1002/jmv.20255
4. Stegelmeier AA, van Vloten JP, Mould RC, et al. Myeloid Cells during Viral Infections and Inflammation. Viruses. 2019;11(2):168. doi:10.3390/v11020168
5. Schulte-Schrepping J, Reusch N, Paclik D, et al. Severe COVID-19 Is Marked by a Dysregulated Myeloid Cell Compartment. Cell. 2020;182(6):1419–1440. doi:10.1016/j.cell.2020.08.001
6. Janoff A. Elastase in tissue injury. Ann Rev Med. 1985;36:207–216. doi:10.1146/annurev.me.36.020185.001231
7. Thierry AR. Anti-protease Treatments Targeting Plasmin(ogen) and Neutrophil Elastase May Be Beneficial in Fighting COVID-19. Physiol Rev. 2020;100(4):1597–1598. doi:10.1152/physrev.00019.2020
8. Cruz DB, Helms J, Aquino LR, et al. DNA-bound elastase of neutrophil extracellular traps degrades plasminogen, reduces plasmin formation, and decreases fibrinolysis: proof of concept in septic shock plasma. FASEB J. 2020. doi:10.1096/fj.201901363RRR
9. Leonard-Lorant I, Delabranche X, Severac F, et al. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d-Dimer Levels. Radiology. 2020;296(3):E189–E191. doi:10.1148/radiol.2020201561
10. Xu J, Wang L, Zhao L, et al. Risk assessment of venous thromboembolism and bleeding in COVID-19 patients. Res Square. 2020. doi:10.21203/rs.3.rs-18340/v1
11. Mukaida N, Matsumoto T, Yokoi K, et al. Inhibition of neutrophil-mediated acute inflammatory injury by an antibody against interleukin-8 (IL-8). Inflammation Res. 1998;47:151–157. doi:10.1007/s000110050308
12. Bao Z, Ye Q, Gong W, et al. Humanized monoclonal antibody against the chemokine CXCL-8 (IL-8) effectively prevents acute lung injury. Int Immunopharmacol. 2010;10(2):259–263. doi:10.1016/j.intimp.2009.11.005
13. Wayne SJ, Rhyne RL, Garry PJ, et al. Cell-Mediated Immunity as a Predictor of Morbidity and Mortality in Subjects Over 60. J Gerontol. 1990;45(2):45–48. doi:10.1093/geronj/45.2.M45
14. Ohrui T. Interventions to prevent pneumonia in older adults. Geriatr Gerontol Int. 2004;4(s1):92–95. doi:10.1111/j.1447-0594.2004.00162.x
15. Saule P, Trauet J, Dutriez V, et al. Accumulation of memory T cells from childhood to old age, Central and effector memory cells in CD4+ versus effector memory and terminally differentiated memory cells in CD8+ compartment. Mech Ageing Dev. 2006;127(3):274–281. doi:10.1016/j.mad.2005.11.001
16. Li H, Wang S, Zhong F, et al. Age-dependent risks of Incidence and Mortality of COVID-19 in Hubei Province and Other Parts of China. Fron Med. 2015:214. doi:10.3389/fmed.2020.00190
17. Zhang B, Zhou X, Zhu C, et al. Immune phenotyping based on neutrophil-to-lymphocyte ratio and IgG predicts disease severity and outcome for patients with COVID-19. medRxiv. 2020. doi:10.1101/2020.03.12.20035048
18. Ma Y, Shi N, Fan Y, et al. Predictive Value of the Neutrophil-to-Lymphocyte Ratio (NLR) for diagnosis and worse clinical course of the COVID-19: findings from ten provinces in China. Lancet. 2020. doi:10.2139/ssrn.3569838
19. Qin C, Zhou L, Hu Z, et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin Infect Dis. 2015;14:148. doi:10.1093/cid/ciaa248
20. Zhu F, Li Y, Guan X, et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. Lancet. 2020. doi:10.1016/S0140-6736(20)31208-3
21. Flora SD, Grassi C, Carati L. Attenuation of influenza-like symptomatology and improvement of cell-mediated immunity with long-term N-acetylcysteine treatment. Eur Respiratory J. 1997;10(7):1535–1541. doi:10.1183/09031936.97.10071535
22. Poppe M, Wittig S, Jurida L, et al. The NF-κB-dependent and -independent transcriptome and chromatin landscapes of human coronavirus 229E-infected cells. PLoS Pathog. 2017;13(3):e1006286. doi:10.1371/journal.ppat.1006286
23. Geiler J, Michaelis M, Naczk P, et al. N-acetyl-L-cysteine (NAC) inhibits virus replication and expression of pro-inflammatory molecules in A549 cells infected with highly pathogenic H5N1 influenza A virus. Biochem Pharmacol. 2010;79(3):413–420. doi:10.1016/j.bcp.2009.08.025
24. Ho W, Douglas SD. Glutathione and N-Acetylcysteine suppression of human immunodeficiency virus replication in human Monocyte/Macrophages in vitro. AIDS Res Hum Retroviruses. 1992;8(7):1249–1253. doi:10.1089/aid.1992.8.1249
25. Mata M, Sarrion I, Armengot M, et al. Respiratory syncytial virus inhibits ciliagenesis in differentiated normal human bronchial epithelial cells: effectiveness of N-Acetylcysteine. PLoS One. 2012;7(10):e48037. doi:10.1371/journal.pone.0048037
26. Zhang L, Lin D, Sun X, et al. Crystal structure of SARS-CoV-2 main protease provides a basis for design of improved α-ketoamide inhibitors. Science. 2020;368:409–412.
27. Guthappa R. Molecular Docking Studies of N-Acetyl Cysteine, Zinc Acetyl Cysteine and Niclosamide on SARS Cov 2 Protease and Its Comparison with Hydroxychloroquine. Chemarxiv. 2020. doi:10.26434/chemrxiv.12161493.v1
28. Sadowskaa AM, Manuel-y-Keenoy B, Vertongen T, et al. Effect of N-acetylcysteine on neutrophil activation markers in healthy volunteers: in vivo and in vitro study. Pharmacol Res. 2006;53(3):216–225. doi:10.1016/j.phrs.2005.11.003
29. Kharazmi A. Nielsen H and Schiotx PO. N-acetylcysteine inhibits human neutrophil and monocyte chemotaxis and oxidative metabolism. Int J Lmmunopharmac. 1988;10(1):39–46. doi:10.1016/0192-0561(88)90148-8
30. Allegra L, Sasso MD, Bovio C, et al. Human Neutrophil Oxidative Bursts and their in vitro Modulation by Different N-Acetylcysteine Concentrations. Drug Res. 2002;52(9):669–676.
31. Tavakolpour S, Rakhshandehroo T, Wei EX, Rashidian M. Lymphopenia during the COVID-19 infection: what it shows and what can be learned. Immunol Lett. 2020;225:31–32. doi:10.1016/j.imlet.2020.06.013
32. Chiba T, Takahashi S, Sato N, et al. Fas-mediated apoptosis is modulated by intracellular glutathione in human T cells. Eur J Immunol. 1996;26(5):1164–1169. doi:10.1002/eji.1830260530
33. Lai Z, Hanczko R, Bonilla E, et al. N-acetylcysteine reduces disease activity by blocking mammalian target of rapamycin in T cells from systemic lupus erythematosus patients: A randomized, double-blind, placebo-controlled trial. Arthritis Rheumatology. 2012;64(9):2937–2946. doi:10.1002/art.34502
34. Sharafkhah M, Abdolrazaghnejad A, Zarinfar N, et al. Safety and efficacy of N-acetylcysteine for prophylaxis of ventilator-associated pneumonia: a randomized, double blind, placebo-controlled clinical trial. Mojtaba Med Gas Res. 2018;8(1):19–23. doi:10.4103/2045-9912.229599
35. Zhang Q, Ju Y, Ma Y, et al. N-acetylcysteine improves oxidative stress and inflammatory response in patients with community acquired pneumonia A randomized controlled trial. Medicine. 2018;97:e13087.
36. Ragab D, Eldin H, Taeimah M, et al. The COVID-19 cytokine storm; What we know so far. Front Immunol. 2020;11. doi:10.3389/fimmu.2020.01446
37. Hassett P, Curley GF, Contreras M, et al. Overexpression of pulmonary extracellular superoxide dismutase attenuates endotoxin induced acute lung injury. Intensive Care Med. 2011;37:1680–1687.
38. Fox RB. Prevention of granulocyte-mediated oxidant lung injury in rats by a hydroxyl radical scavenger, dimethylthiourea. J Clin Invest. 1984;74(4):1456–1464. doi:10.1172/JCI111558
39. Li L, Huang Q, Wang DC, et al. Acute lung injury in patients with COVID-19 infection. Clin Transl Med. 2020. doi:10.1002/ctm2.16
40. Aruoma OI, Halliwell B, Hoey BM, et al. The antioxidant action of N-acetylcysteine: its reaction with hydrogen peroxide, hydroxyl radical, superoxide, and hypochlorous acid. Free Radic Biol Med. 1989;6(6):593–597. doi:10.1016/0891-5849(89)90066-X
41. Suter PM, Domenighetti G, Schaller MD, et al. N-Acetylcysteine enhances recovery from acute lung injury in man: a randomized, double-blind, placebo-controlled clinical study. Chest. 1994;105(1):190–194. doi:10.1378/chest.105.1.190
42. Lai K, Ng W, Chan PK, et al. High-Dose N-Acetylcysteine Therapy for Novel H1N1 Influenza Pneumonia. Ann Intern Med. 2010;152(10):687. doi:10.7326/0003-4819-152-10-201005180-00017
43. Moradi M, Mojtahedzadeh M, Mandegari A, et al. The role of glutathione-S-transferase polymorphisms on clinical outcome of ALI/ARDS patient treated with N-acetylcysteine. Respir Med. 2009;103(3):434–441. doi:10.1016/j.rmed.2008.09.013
44. Puyo C, Kreig D, Saddi V, et al. Case Report: use of hydroxychloroquine and N-acetylcysteine for treatment of a COVID-19 positive patient [version 1; peer review: awaiting peer review]. F1000Research. 2020;9:491.
45. Liu Y, Luo G, Qian X, et al. Experience of N-acetylcysteine airway management in the successful treatment of one case of critical condition with COVID-19. Researchsquare. 2020. doi:10.21203/rs.3.rs-34193/v1
46. Nasia A, McArdleb S, Gaudernackc G, et al. Reactive oxygen species as an initiator of toxic innate immune responses in retort to SARS-CoV-2 in an ageing population, consider N-acetylcysteine as early therapeutic intervention. Toxicol Rep. 2020;7:768–771. doi:10.1016/j.toxrep.2020.06.003
47. Ibrahim H, Perl A, Smith D, et al. Therapeutic blockade of inflammation in severe COVID-19 infection with intravenous n-acetylcysteine. Clin Immunol. 2020;219:108544. doi:10.1016/j.clim.2020.108544
48. ACETADOTE® (acetylcysteine) Injection. NDA 21-539/S-004. FDA. 2006
49. Dósa E, Helta K, Radovits T, et al. Dose escalation study of intravenous and intra-arterial N-acetylcysteine for the prevention of oto- and nephrotoxicity of cisplatin with a contrast-induced nephropathy model in patients with renal insufficiency. Fluids and Barriers of the CNS. 2017;14(1):26. doi:10.1186/s12987-017-0075-0
50. Hong SY, Gil HW, Yang JO, et al. Effect of High-Dose Intravenous N-acetylcysteine on the Concentration of Plasma Sulfur-Containing Amino Acids. Korean J Intern Med. 2005;20:217–223. doi:10.3904/kjim.2005.20.3.217
51. MacDonald TT. The gut is still the biggest lymphoid organ in the body. Nature. 2008;1(4):246–247.
52. Green JL, Heard KJ, Reynolds KM, et al. Oral and Intravenous Acetylcysteine for Treatment of Acetaminophen Toxicity: A Systematic Review and Meta-analysis. West J Emerg Med. 2013;14(3):218–226. doi:10.5811/westjem.2012.4.6885
53. Grein J, Ohmagari N, Shin D, et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. NEJM. 2020;382(24):2327–2336. doi:10.1056/NEJMoa2007016
54. Yazdi AP, Razavi M, Sheikh S, et al. Clinical Trial Assessment of Intermittent and Continuous Infusion Dose of N-Acetylcysteine on Redox Status of the Body in Patients with Sepsis Admitted to the ICU. J Intensive Care Med. 2019. doi:10.1177/0885066618823152
55. Molnar Z, Shearer E, Lowe D, et al. N-Acetylcysteine treatment to prevent the progression of multisystem organ failure: a prospective, randomized, placebo-controlled study. Crit Care Med. 1999;27(6):1100–1104. doi:10.1097/00003246-199906000-00028
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.