")
Back to Journals » Open Access Journal of Sports Medicine » Volume 10
Musculoskeletal injuries in real tennis
Authors Humphrey JA, Humphrey PP, Greenwood AS , Anderson JL , Markus HS, Ajuied A
Received 17 December 2018
Accepted for publication 3 April 2019
Published 23 May 2019 Volume 2019:10 Pages 81—86
DOI https://doi.org/10.2147/OAJSM.S198500
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Andreas Imhoff
JA Humphrey,1 PP Humphrey,2 AS Greenwood,3 JL Anderson,4 HS Markus,5 A Ajuied6
1Orthopaedic Department, Milton Keynes University Hospital, Milton Keynes, MK65LD, UK; 2School of Pharmacy, University College London, London, WC1N 1AX, UK; 3Department of Sport and Exercise Sciences, St Mary’s University, Twickenham, TW1 4SX, UK; 4Medical Education Department, University of Brighton, Brighton, BN1 9PH, UK; 5Department of Clinical Neurosciences, University of Cambridge, Cambridge CB2 2PY, UK; 6Orthopaedic Department, Guys’ and St Thomas’ NHS Trust, London SE1 9RT, UK
Introduction: Real tennis is a growing, unique, and well-established sport. To date, there has been no epidemiological data on real tennis injuries. The primary aim of this retrospective study is to record the incidence and document any trends in real tennis musculoskeletal injuries, so as to improve injury awareness of common and possibly preventable injuries.
Methods: A surveillance questionnaire e-mailed to 2,036 Tennis & Rackets Association members to retrospectively capture injuries sustained by amateur and professional real tennis players over their playing careers.
Results: A total of 485 (438 males and 47 females) questionnaires were fully completed over 4 weeks. A total of 662 musculoskeletal injuries were recorded with a mean of 1.4 injuries per player (range 0–7). The incidence of sustaining an acute real tennis musculoskeletal injury is 0.4/1000 hrs. The three main anatomical locations reported injured were elbow 15.6% (103/662), knee 11.6% (77/662), and face 10.0% (66/662). The most common structures reported injured were muscle 24% (161/661), tendon 23.4% (155/661), ligament 7.0% (46/661), soft tissue bruising 6.5% (43/661), and eye 6.2% (41/661). The majority of the upper limb injuries were gradual onset (64.7%, 143/221), and the lower limb injuries were sudden onset (72.0%, 188/261).
Conclusion: This study uniquely provides valuable preliminary data on the incidence and patterns of musculoskeletal injuries in real tennis players. In addition, it highlights a number of reported eye injuries. The study is also a benchmark for future prospective studies on academy and professional real tennis players.
Keywords: epidemiology, musculoskeletal injuries, real tennis
Introduction
“To see Good Tennis! What divine joy
Can fill our leisure, or minds employ?
Let other people play at other things:
The King of Games is still the Game of Kings.”1
Real tennis is an original racquet sport from which the modern game of lawn tennis is derived. It is played indoors involving high-skill levels and strategy, and has essentially remained unchanged over the last five centuries. Real tennis was the first sport to be described as “the beautiful game”.2 Currently, there are over 10,000 officially registered players in the UK, US, Australia, and France. The International Real Tennis Professional Association (IRTPA) supports real tennis professionals and drives the development of the sport worldwide. The main governing body in the UK is the Tennis & Rackets Association (T&RA).
Over the years, there have been several studies describing lawn tennis injuries.3,4 Other racquet sports including squash, badminton, and even paddle-tennis have followed suit.5,6,7 However, there are no data on the epidemiology of injuries in this unique and well-established sport. The primary aim of this retrospective study is to record the incidence of real tennis musculoskeletal injuries, and determine factors associated with injuries, so as to improve both injury awareness and strategies for prevention among amateur and professional players.
Methods
This retrospectively cross-sectional study captured data from active real tennis players over their playing careers to date. An email was sent to real tennis players >18 years old identified through T&RA members’ database requesting participation in the study and to complete an injury surveillance questionnaire through the anonymous Bristol On-Line Survey online and a hard copy is attached in the supplementary material. E-mail reminders were sent at one and two weeks, and the online link was active for a month from the original participation request.
Terminology, definitions, and methods were adapted from the published consensus statement describing the methodology for epidemiological assessment of medical conditions in lawn tennis.8 An injury was defined as any “musculoskeletal complaint directly related to playing real tennis irrespective of the severity.” The International Tennis Federation (ITF) differentiate between the incidence of acute musculoskeletal injuries (number of injuries/1,000 playing hours) and the all prevalence of gradual onset injuries (number of injured players in the season x 100/number players in the study).8 A retrospective study design means only the incidence of acute musculoskeletal injuries can be calculated.
Players’ demographics, baseline playing information, and details of injuries sustained (if any) were recorded. Each specific musculoskeletal injury was classified into anatomical location, structure/system injured, injury presentation (acute/gradual onset), and nature of injury (new/recurrent). Musculoskeletal injury severity was determined by days required off playing before return to the sport, and by participants rating their injury from 0 (insignificant) to 10 (life-threatening). Details on the management on each musculoskeletal injury were also captured.
Ethical approval for the study was granted by Brighton and Sussex Medical School Research & Governance Ethical Committee. T&RA members by completing the online injury surveillance questionnaire inferred their informed consent into the study.
Statistical analysis
Factors associated with injuries were explored. The following factors were investigated: Demographic characteristics (age, gender, height, weight), dominant hand, number of years played, hours played per week, whether they usually stretched pre-game, warmed-up and warmed-down, and real tennis handicap. Each player has a handicap, which determines their individual level of play. Associations with a total number of injuries were initially examined by univariate analysis using Chi-square for categorical data, or Pearsons or Spearman’s correlation according to whether data were normally distributed or not for continuous data. Variables which met a P≤0.1 were entered into multivariate analysis using logistic regression to determine which associations were independently associated with the number of injuries. All statistical analysis was performed in Statistical Package for the Social Sciences (SPSS) version 25 for Mac.
Results
Player characteristics
In total, 2,036 real tennis players were e-mailed and invited to participate in the study, with 485 (438 males and 47 females) fully completed questionnaires were returned (response rate 23.8%). Baseline demographics and play metrics are shown in Table 1.
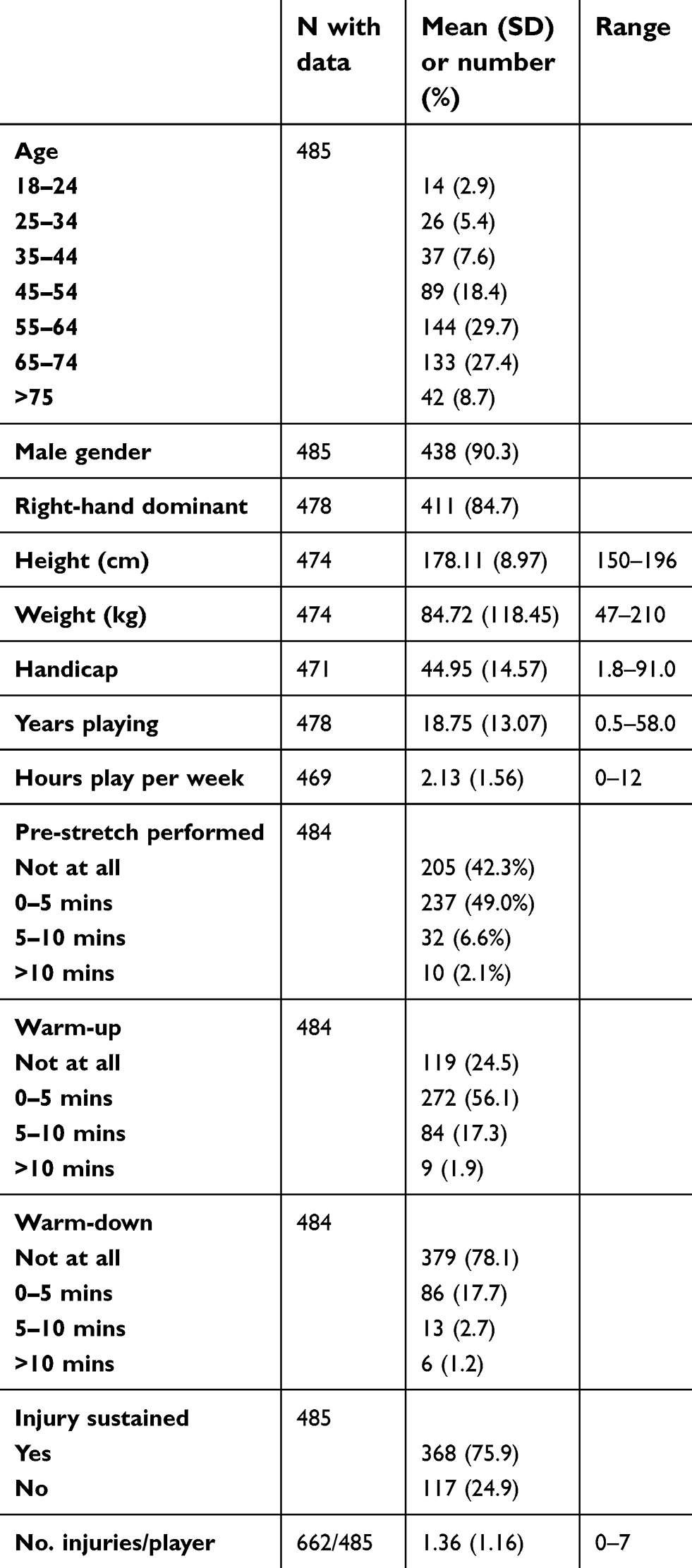 | Table 1 Baseline demographics and playing details |
The players participating in the study represented 30 real tennis clubs worldwide, including all the 24 real tennis clubs in England, but also clubs from the US (four) and Australia (two). The most represented club was the Royal Tennis Court, Hampton Court Palace with 45 participants.
The mean number of years played per respondent was 18.8 (range <1–56), with a mean of 2 hrs (range <1–12) playing time per week. The cohort had a player handicap mean of −44.9 and median of −46 (range +8 to −91).
Hand dominance was right for 419 players (86.4%) and left for 66 players (13.6%). All players (485) used single-handed forehand strokes. The majority of players (469, 96.7%) used single- handed backhand strokes, and the remaining players (16, 3.3%) used double-handed backhand strokes.
The percentage of players that engaged in pre-game stretching was 55.8% (271/484), players that warmed-up before commencing play was 75% (364/485), and players that warmed-down after completing play was only 21% (102/485) (Table 1).
Musculoskeletal injury details
Out of the 485 players, 368 (75.9%) sustained at least one real tennis musculoskeletal injury during their playing career to date. A total of 662 musculoskeletal injuries were recorded with a mean of 1.4 injuries per player (range 0–12). The incidence of sustaining an acute real tennis musculoskeletal injury was 0.4/1,000 playing hours. The 55–64 age category had the highest percentage of injuries sustained 29.7% (144/485).
The five most frequently injured anatomical locations were: elbow 15.6% (103/662), knee 11.6% (77/662), face 10.0% (66/662), lower leg (calf) 8.8% (57/662), and shoulder 8.2% (54/662) (Table 2). Injury location was further stratified as lower limb 39.4% (261/662), upper limb 33.3% (221/662), head and face 15.7% (104/662), trunk and spine 8.5% (51/662), and other 3.8% (25/662). The most commonly injured tissue structures were: muscle 24% (161/661), tendon 23.4% (155/661), ligament 7.0% (46/661), soft tissue bruising 6.5% (43/661), and eye 6.2% (41/661) (Table 2).
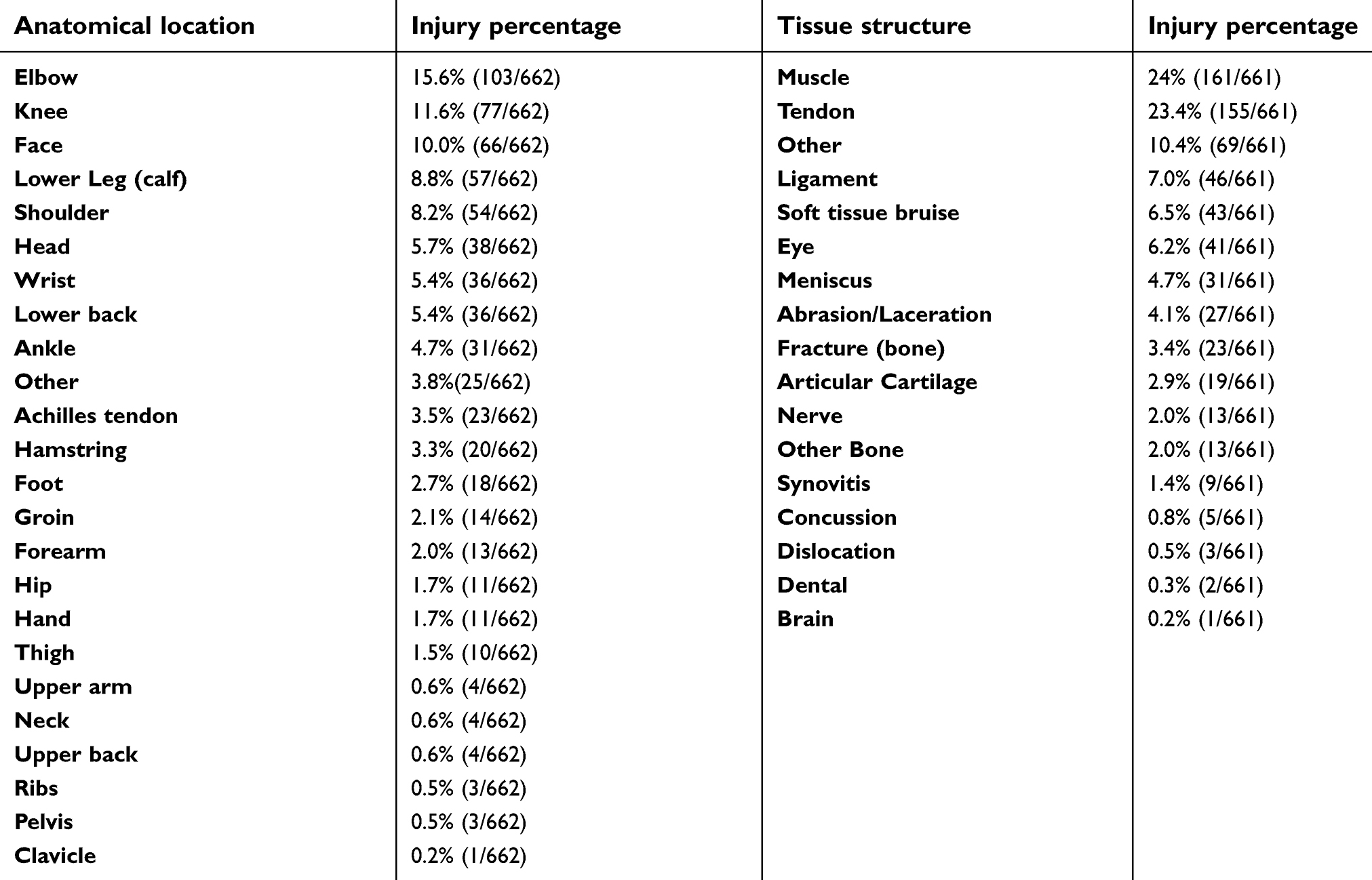 | Table 2 Anatomical locations and tissue structures involved in real tennis injuries |
More new musculoskeletal injuries (76%, 504/660) were recorded than recurrent musculoskeletal conditions (24%, 156/660). Sudden onset (acute) musculoskeletal conditions (64%, 418/656) were more common than gradual onset (overuse) musculoskeletal conditions (36%, 238/656). The majority of the upper limb injuries were gradual onset (64.7%, 143/221), and the lower limb injuries were sudden onset (72.0%, 188/261).
Severity of musculoskeletal conditions determined through time off playing real tennis was categorized as follows: 7.3% no days off (48/655), 7.7% 1–3 days off (51/655), 11.0% 4–7 days off (72/655), 31% 8–28 days off (203/655), 32.7% 1–6 months off (214/655), and 10.2% >6 months off (67/655). The mean subjective musculoskeletal condition severity rating was 3.8 (range 1–10).
The health care systems that players were treated in included – State-funded health care (eg, The UK’s National Health Service) 21.5% (142/662), privately funded health care 33.5%, both State and private health care 11.8% (78/662) and was not applicable in 33.2% (220/662) of injuries. Only 29.2% (193/662) of the reported injuries were not assessed by a health care or medical practitioner. The remaining 70.8% (469/662) of reported injuries were assessed by one or more of the following health care or medical practitioners–physiotherapist 35.8% (240/670), medical doctor 35.2% (236/670), orthopaedic surgeon 18.7% (125/670), other 7.0% (47/670) and chiropractor 3.3% (22/670).
In total, 65.7% (435/662) of the reported injuries did not require any medical imaging. The remaining 34.3% (227/662) of reported injuries required one or more of the following medical imaging- X-ray 39.1% (115/294), CT scan 7.5% (22/294), MRI scan 29.6% (87/294), ultrasound scan 18.0 (53/294), and other modality 5.8 (17/294).
Treatment was self-administered in 36.3% (240/662) of the reported injuries. The remaining 63.7% (422/662) of injuries required formal treatment with one or more of the following – rest/ice/compression/elevation 39.7% (292/736), physiotherapy 32.2% (237/736), surgery 12.0% (88/736), other 12.0% (87/736), hydrotherapy 0.3% (2/736), and acupuncture 4.1% (30/736).
Factors associated with injuries
On univariate analysis, the following variables were associated with the number of injuries with a p≤0.1 and were entered into the multivariable analysis; namely height, number of years played, hours play per week, pre-match stretch, warm-up, and warm-down. The strongest independent predictor of the number of injuries was the hours of play per week. Number of years played and the amount of pre-stretch were also positively associated with a number of injuries. There was an inverse relationship between height and number of injuries. The amount of warm-up and warm-down exercises were not independently found to correlate with the number of injuries. Table 3 shows the results of multivariate analysis determining which factors were independently associated with the number of injuries.
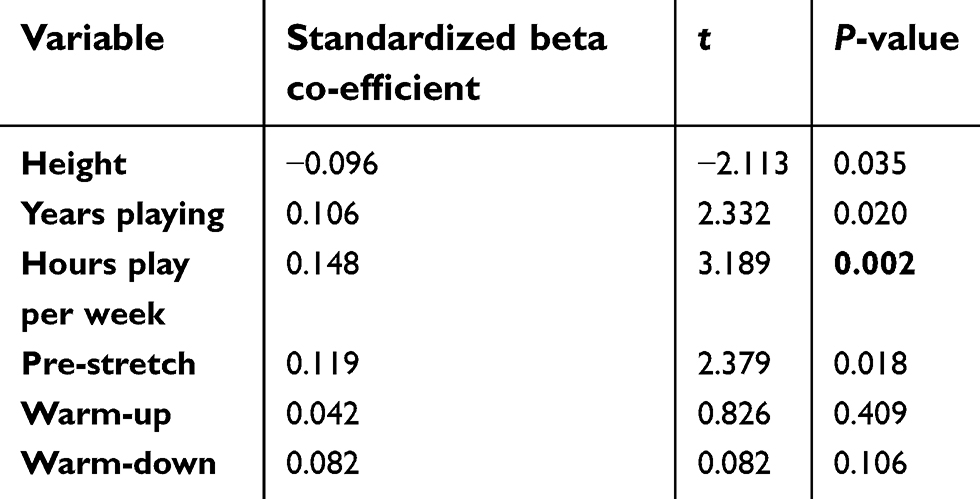 | Table 3 Results of multivariate analysis determining which factors were independently associated with the number of injuries |
Discussion
Our inaugural epidemiology study on real tennis injuries documents the incidence and details of musculoskeletal injuries sustained among amateur and professional players. The ITF recommended that their consensus statement for epidemiological studies in lawn tennis can be applied to other racquet sports8 and here we have uniquely adapted it to real tennis. We have captured well over 600 real tennis injuries. The incidence of acute musculoskeletal injuries is 0.4/1000 playing hours, which is low. This is not surprising given the retrospective design and the long recall period. Less serious self-diagnosed injuries sustained may have been under-reported. Our results though are comparable with lawn tennis as their reported incidence in the literature varies from 0.04 to 3.0 injuries/1,000 playing hours.4
All indoor racquet sports have an intrinsic risk of eye injuries.9,10 We have reported a high number of facial and eye injuries that have been sustained whilst playing real tennis. The only other real tennis injury described in the academic literature to-date is an isolated eye injury.11 In real tennis, the unique combination of hard balls hit with heavy spin within an asymmetrical court with sloping roofs, posted openings, and an angulated wall, means the ball rebounds at unexpected/unpredictable angles and deflections into the player’s face can occur off the small racquet head. However, courts are well-lit, the balls are colored “optic yellow” to improve visual recognition and some players routinely wear eye protection in order to minimize the risk of facial injuries. The T&RA is currently further exploring eye injury prevention strategies.
The most common structures injured were muscles and tendons, which is similar to the findings of epidemiological studies on lawn tennis injuries.12,13 These observations are compatible with the sports technical requirements. New musculoskeletal injuries were more commonly reported than recurrent musculoskeletal conditions. This correlates with our other findings that players were appropriately seeking medical attention and formally managing their injuries prior to returning to play.
Real tennis injuries also have a similar pattern to lawn tennis with upper limb gradual onset injuries and sudden onset lower limb injuries.14
Real tennis is played with a hand-made ball composed of a cork core surrounded by felt and a rigid wood-based racquet with tight strings, which are both significantly heavier than their lawn tennis equivalents. Essentially this means the ball travels at high velocity and with a low bounce, so requires a bent elbow and a cocked wrist to play repetitive strokes. Some serves, most notably “the railroad” and volleying require overhead movements. All these factors contribute to players sustaining gradual onset injuries of the elbow, shoulder, and wrist.
The forces on the lower limbs draw similarities to a combination of lawn tennis with running side-to-side across court and squash with bending the knees close to the playing surface whilst retrieving low bouncing balls. These active movements correlate with findings that players are sustaining sudden onset lower limb injuries mainly affecting the knee and lower leg (calf).
Our results highlight the main factor associated with real tennis injuries is hours played per week. Unusually pre-game stretch was associated with an increased injury risk and warm-up or warm-down exercises did not reduce the risk of injury. These findings may be a result of limited information requested, with players potentially changing their pre- and post-match routines over the years, and no information was obtained on exact exercises and stretches eg, static vs dynamic stretching. More robust evidence is required prior to proposing formal pre-stretch, warm-up, and warm-down recommendations.
Strengths and limitations
Real tennis is a niche sport, and the players are quite engaged, so as envisaged we achieved a good response rate of 23.8%. By comparison, a similar study investigating musculoskeletal injuries in lawn tennis-teaching professionals only achieved a response rate of 8.7%.12
The study participants are a representative sample of the real tennis population, with low numbers of females and younger players (<25 years old). This trend is most likely related to lack of real tennis exposure, limited courts, cost, and other competing racquet sports. The T&RA endeavor to make sure the sport is well publicized and accessible to everyone.
A nuance of real tennis is the global handicap system, which determines a player’s level. Although players were not asked whether they were amateur or professional, it can be deduced that professional players participated given some of the elite handicaps recorded.
Our study had limitations secondary to the retrospective design being susceptible to recall bias. This can lead to inaccurate injury details and potential underreporting. Also, the self-reporting questionnaire did not require injuries to have a formal diagnosis from a medical practitioner. We aimed to capture musculoskeletal injuries directly related to playing real tennis. However, some injuries are multi-factorial and could have been influenced if real tennis players were participating in other sporting activities.
In addition, the study cohort incorporated a broad spectrum of ages and abilities. So the next step would be to perform prospective seasonal studies, focused on academy and professional players. This will provide more accurate information on specific player groups to focus on injury prevention.
Conclusion
This study uniquely provides valuable preliminary data on the incidence and patterns of musculoskeletal injuries in real tennis players. In addition, it highlights a high number of reported eye injuries. The majority of the upper limb injuries were gradual onset, and the lower limb injuries were sudden onset. The study is also a benchmark for future prospective studies on academy and professional real tennis players.
Acknowledgments
We would like to thank Nick Wood (Head Real Tennis Professional, Royal Tennis Court) and Chris Davies (Chief Executive, Tennis & Rackets Association) for their support and input throughout the project. To improve study participation, the players who completed the questionnaire could choose to be placed into a confidential randomly allocated drawer for a bottle of Champagne, which was supplied and sent directly to the winner by Pol Roger. No other financial assistance with the project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ward TH. The English Poets. New York, London: Macmillan and Co., 1880–1918; Bartleby.com; 2013.
2. Barcellon P. Rules and Principles of Tennis. 1800. Hamilton R, English translation, Ronaldson Publications. 1987.
3. Powell RW. Lawn tennis leg. Lancet. 1883;2:44.
4. Pluim BM, Staal JB, Windler GE, Jayanth N. Tennis injuries: occurrence, aetiology, and prevention. Br J Sports Med. 2006;40:415–423. doi:10.1136/bjsm.2005.023184
5. Reeves J, Hume PA, Gianotti S, Wilson B, Ikeda E. A retrospective review from 2006 to 2011 of lower extremity injuries in badminton in New Zealand. Sports. 2015;3:77–86. doi:10.3390/sports3020077
6. Berson BL, Passoff TL, Nagelberg S. Thornton J.Injury patterns in squash players. Am J Sports Med. 1978;6(6):323–325. doi:10.1177/036354657800600603
7. Castillo-Lozano R, Casuso-Holgado MJ. Incidence of musculoskeletal sport injuries in a sample of male and female recreational paddle-tennis players. J Sports Med Phys Fitness. 2017;57(6):816–821. doi:10.23736/S0022-4707.16.06240-X
8. Pluim BM, Fuller CW, Batt ME, et al. Consensus statement on epidemiological studies of medical conditions in tennis, April 2009. Br J Sports Med. 2009;43:893–897. doi:10.1136/bjsm.2009.064915
9. Jao KK, Atik A, Jamieson MP, et al. Knocked by the shuttlecock: twelve sight-threatening blunt-eye injuries in Australian badminton players. Clin Exp Optom. 2017;100(4):365–368. doi:10.1111/cxo.12501
10. Genovese MT, Lenzo NP, Lim RK, Morkel DR, Jamrozik KD. Eye injuries among pennant squash players and their attitudes towards protective eyewear. Med J Aust. 1990;153(11–12):655–658.
11. Jones N. One year of severe eye injuries in sport. Eye. 1998;2:484–487. doi:10.1038/eye.1988.97
12. Colberg R, Aune K, Propst M. Prevalence of musculoskeletal conditions in tennis-teaching professionals. Orthop J Sports Med. 2017;4(10):2325967116668138.
13. Gescheit DT, Cormack SJ, Duffield R, Kovalchik WTO, Omizzolo M, Ried M. Injury epidemiology of tennis players at the 2011–2016 Australian open grand slam. Br J Sports Med. 2017;51:1289–1294. doi:10.1136/bjsports-2016-097283
14. Abrams G. Epidemiology of musculosketal injury in the tennis player. Br J Sports Med. 2012;46:492–498. doi:10.1136/bjsports-2012-091164
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.