")
Back to Journals » Cancer Management and Research » Volume 10
MTHFR C677T and A1298C polymorphisms and lung cancer risk in a female Chinese population
Authors Tong W, Tong G, Jin D, Lv Q
Received 4 June 2018
Accepted for publication 11 July 2018
Published 3 October 2018 Volume 2018:10 Pages 4155—4161
DOI https://doi.org/10.2147/CMAR.S176263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Weiwei Tong,1 Guanghui Tong,1 Dongyan Jin,1 Qingjie Lv2
1Department of Laboratory Medicine, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 2Department of Pathology, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China
Objective: To examine the relationship between polymorphisms in the methylenetetrahydrofolate reductase (MTHFR) gene and susceptibility to lung cancer in a female Chinese population.
Method: A hospital-based case-control study of 388 cases and 388 controls was conducted. Two polymorphisms in MTHFR were detected using TaqMan methods.
Results: The MTHFR C677T polymorphism was associated with the risk of lung cancer and lung adenocarcinoma. Carriers with the TT genotype of C677T were observed to have an increased risk of lung cancer and lung adenocarcinoma (the ORs were 1.550 and 1.588, respectively). By contrast, the A1298C polymorphism had a negative relationship with the risk of lung cancer and lung adenocarcinoma; compared with the AA genotype carriers, the CC genotype carriers had a lower risk of lung cancer and adenocarcinoma in the female Chinese population (ORs were 0.302 and 0.215, respectively). In the stratified analyses, we observed only the A1298C polymorphism in the CC genotype carriers with a statistically significant reduction in the risk of non-small-cell lung cancer, compared to the AA genotype carriers. No significant statistical association was found between the MTHFR gene polymorphisms and risk of the residual subtype of lung cancer.
Conclusion: This study provides evidence that the MTHFR C677T polymorphism may contribute to the development of lung cancer and lung adenocarcinoma in a female Chinese population. However, the MTHFR A1298C polymorphism may be associated with the decreasing risk of lung cancer.
Keywords: MTHFR, single nucleotide polymorphism, lung cancer, genetic susceptibility
Introduction
Malignant tumors comprise the second leading cause of death among noninfectious diseases. Lung cancer is the leading cause of cancer-related death among males in both developed and developing countries and has surpassed breast cancer as the leading cause of cancer death among females in the developed countries.1 Lung cancer risk is not fully understood, but it has been commonly considered to be associated with many factors, including genetic and/or environmental factors. It is well known that smoking is an important risk factor for lung carcinoma. However, in China, the smoking rate for females is far lower than that for males. While females comprise ~52.4% of the total population, only ~2.9% of females are smokers,2 and ~53% of female lung cancer patients have no history of smoking,3 suggesting that genetic factors and other risk factors, such as occupational exposure and air pollution, may play very important roles in the development of lung cancer.4
The development of lung cancer is a complicated process that is affected by environmental risk factors and genetic factors. There are many genes that are associated with lung cancer, including methylenetetrahydrofolate reductase (MTHFR). MTHFR is a key enzyme that plays an important role in the metabolism of folate in the human body, by maintaining the normal metabolism of folate, which can regulate intracellular DNA.5 It also plays a part in maintaining the stability of single- and double-strand DNA, DNA methylation, and chromosomal integrity.6 The MTHFR gene is located on chromosome 1 at 1p36.3,7 and C677T (rs1801133) is present as a single nucleotide polymorphism (SNP) in the gene encoding region of the common MTHFR. The variation in the fourth gene exon consists of a cytosine (C) mutation to thymine (T) that results in an alanine-encoding amino acid substitution. The variation causes the thermal stability of MTHFR to become reduced, thereby reducing the enzyme activity. It has been reported that the MTHFR enzyme activity of the individual carrying homozygous mutant genotype is only 30% of that among the wild-type carriers.8 The reduction in enzyme activity can lead to low methylation of the genome, which is associated with susceptibility to many types of cancer, including lung carcinoma. The C677T (rs1801133) and A1298C (rs1801131) polymorphisms are the most common SNPs in the MTHFR gene. A previous study determined that MTHFR C677T can modify the enzyme activity of MTHFR.9 It has been reported that MTHFR C677T is associated with susceptibility to many malignancies, but the conclusion is not definitive.10–15 Hajiesmaeil et al reported that MTHFR 677TT genotype played a protective role and that MTHFR 1298CC genotype could be seen as a genetic risk factor for cervical cancer.16 However, the most recent meta-analysis indicated that no significant results were shown in C677T polymorphism analysis; nevertheless, MTHFR A1298C polymorphism could increase the risk of cervical cancer.17 In addition, several previous studies have reported the relationship between MTHFR C677T, A1298C polymorphisms, and colorectal cancer susceptibility.18–21 But Lin et al and Naghibalhossaini et al drew the opposite conclusion about MTHFR C677T.20,21 The association between MTHFR C677T, A1298C, and breast cancer has also been explored. Hardi et al reported that rs1801133TT genotype could increase the susceptibility of breast cancer comparing with wild-type genotype.22 A meta-analysis published in 2016 summarized that the MTHFR C677T polymorphism showed significant association with lung cancer in Asian and overall populations, but not in Caucasian populations. Xia et al have reported that MTHFR C677T polymorphism was a risk factor for gastric cancer and that A1298C played a protective role against gastric cancer.23 However, other articles showed exactly opposite results about these two polymorphisms.24,25 There are still many controversial results in other cancer types, including prostate cancer, bladder cancer, head and neck cancer, leukemia and lymphoma, nervous system cancers, etc.26–31
The purpose of our study was to explore the association between these two common polymorphisms in the MTHFR gene and the lung cancer risk.
Materials and methods
Data collection
This study was devised based on a molecular epidemiological case-control study. All patients in the case group were selected from Shengjing Hospital of China Medical University in Shenyang, China, from 2010 to 2015. The inclusion criteria of the case group were as follows: 1) patients with newly diagnosed lung cancers, 2) histopathologically confirmed disease as determined by experienced pathologists, 3) no previous radiation therapy or chemical therapy, 4) no history of cancer and metastatic carcinoma, and 5) only female patients. The controls were selected during the same period from the hospital’s physical examination center to assess the health of people who did not have cancer or respiratory diseases. The controls were matched to the cases by age (±5 years) and gender. Based on the calculation, a total of 388 patients and 388 controls were included. Five milliliters of venous blood was drawn from all subjects for SNP genotyping when they were included in the study. The study was approved by the ethics committee of Shengjing Hospital of China Medical University, and written informed consent was obtained from each participant. This study was conducted in 2016. The authors had no access to information that could identify individual participants during or after the data collection.
SNP genotyping
Genomic DNA was extracted from the venous blood of the participants using the classical phenol chloroform method. The TaqMan fluorescence probe method was used to genotype the samples of DNA using the Applied Biosystems 7500 Real-Time PCR System. Ten percent of the participants were randomly selected and divided into two groups, which were supervised by different managers in order to ensure the appropriate quantity for each assay. A 10% masked, random sample of subjects was tested twice by PCR-restriction fragment length polymorphism (RFLP) method, and the results were found to be concordant for all of the masked duplicate sets.
Statistical analysis
The chi-squared test was used to analyze the differences between the categorical variables of the two groups; the chi-squared goodness of fit test was used to calculate the Hardy–Weinberg equilibrium. Logistic regression was used to calculate the OR and 95% CI to evaluate the relationship between susceptibility to lung cancer and the MTHFR polymorphisms. The ORs were calculated for the homozygote model, heterozygote model, dominant model, recessive model, and additive model. The associations were also analyzed in subgroups of different pathologic types of lung cancer. All reported P-values were two-sided, and a probability of 0.05 or smaller was considered statistically significant. The statistical analyses were performed using the SPSS 20.0 software.
Results
A total of 388 patients and 388 controls were included in the present study. All of the subjects were females. Mean ages of cases and controls (mean ± SD) were almost identical (56.1±12.0 and 56.1±11.6 years, respectively) due to matching. There were no significant differences in the distribution of income and education between cases and controls. However, the distribution of smoking status was significantly higher in lung cancer cases (27.1%) than in healthy controls (20.1%) (P=0.006). The distribution of the MTHFR C677T and A1298C genotypes in the control group was in accordance with Hardy–Weinberg balance (P=0.777 and P=0.429). We analyzed the relationship between MTHFR and different lung cancer types, including lung cancer, non-small-cell lung carcinoma (NSCLC), lung adenocarcinoma, and squamous cell lung carcinoma.
First, we analyzed the association between MTHFR and the risk of lung cancer (see Table 1). For the C677T polymorphism (rs1801133), the association indicated that the TT genotype carriers of MTHFR had an increased risk of lung cancer compared with the CC genotype carriers (OR =1.550, 95% CI =1.026–2.342, P=0.037), and the recessive model (TT vs CC+CT) also showed a significantly increased risk of lung cancer (OR =1.401, 95% CI =1.038–1.891, P=0.028). The T allele had striking statistical significance toward enhancing the risk of cancer compared with the C allele (OR =1.262, 95% CI =1.031–1.544, P=0.024). For the A1298C polymorphism (rs1801131), however, the association revealed that the CC genotype carriers showed a decreased risk of lung cancer compared to the AA genotype carriers (OR =0.302, 95% CI =0.096–0.946, P=0.040), as did the dominant model (CA+CC vs AA: OR =0.671, 95% CI =0.483–0.930, P=0.017). In summary, the C allele, compared with the A allele, could be considered a protective factor against lung cancer and played a positive role in reducing the likelihood of lung cancer.
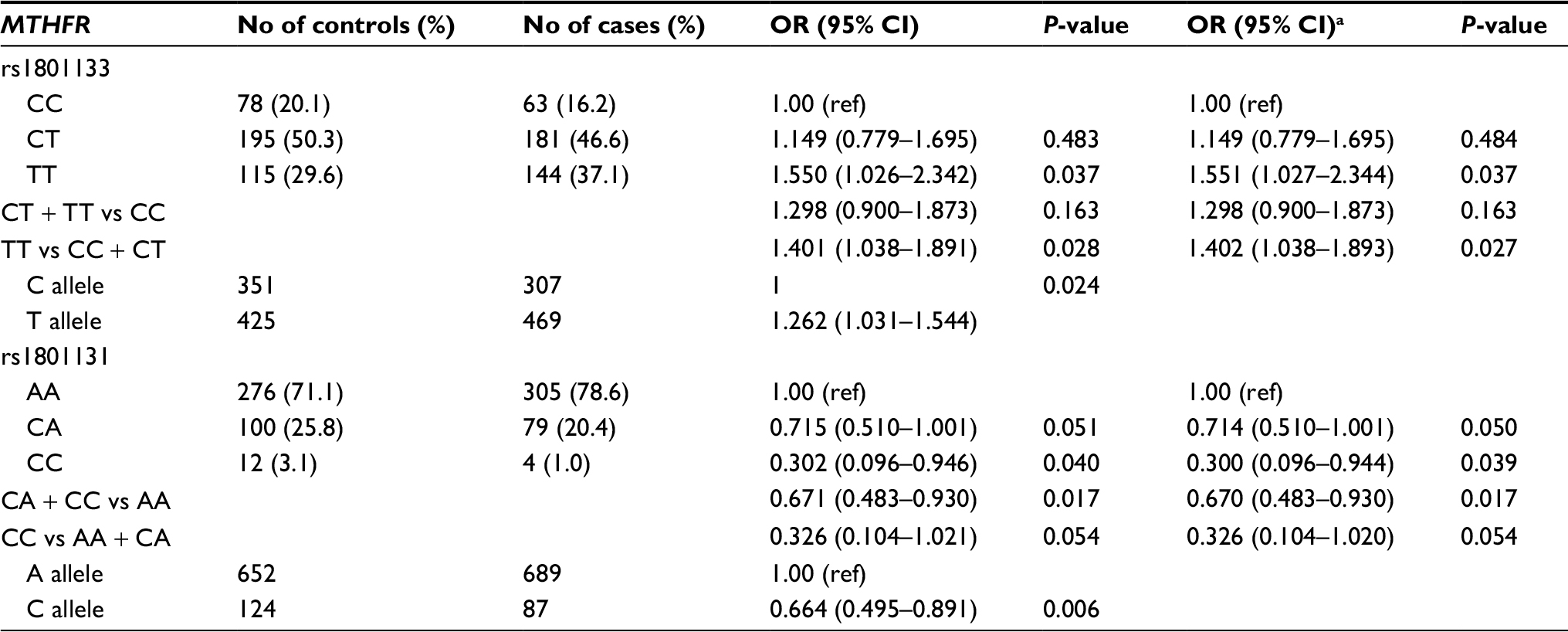 | Table 1 Relationship of MTHFR SNPs and lung cancer risk Note: aAdjusted by age and smoking history. Abbreviations: SNP, single nucleotide polymorphism; MTHFR, methylenetetrahydrofolate reductase. |
In the statistical analyses, we determined that the CC genotype in MTHFR A1298C showed statistical significance compared with the AA genotype in NSCLC (Table 2).
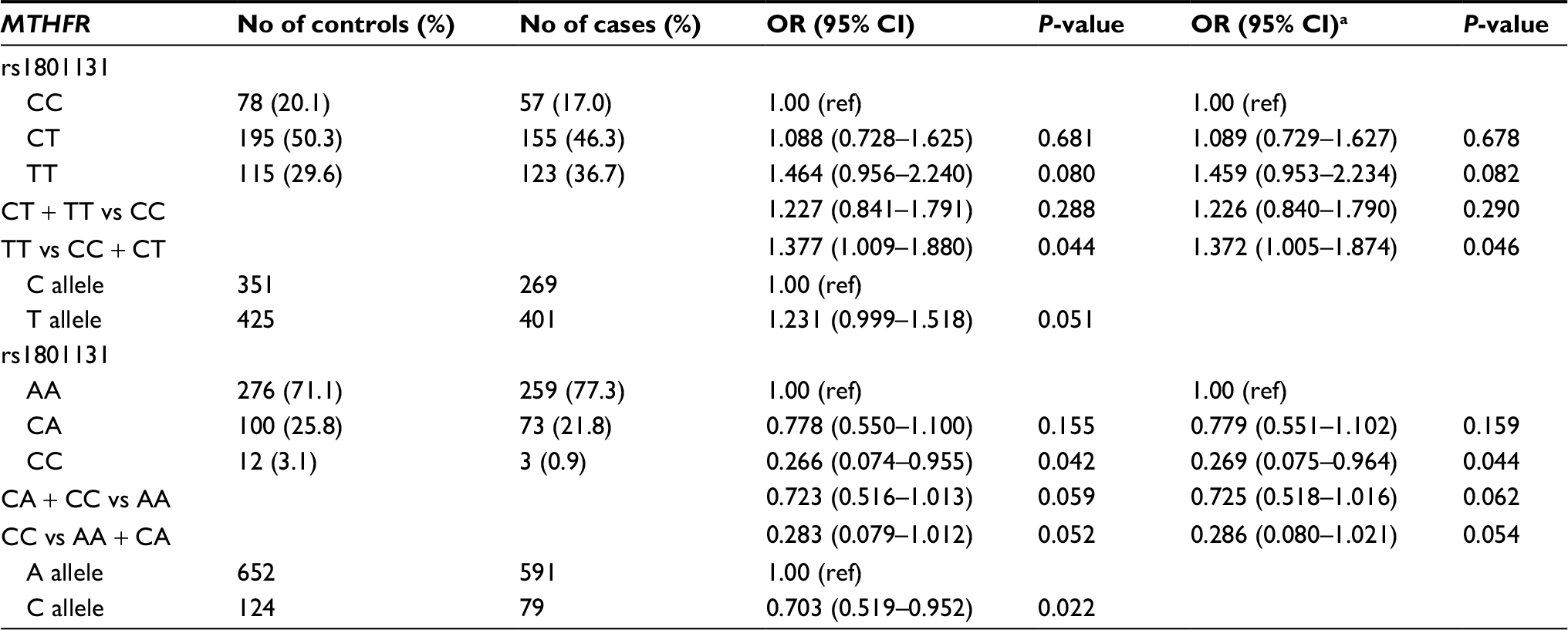 | Table 2 Association between MTHFR SNPs and NSCLC risk Note: aAdjusted by age and smoking history. Abbreviations: SNP, single nucleotide polymorphism; MTHFR, methylenetetrahydrofolate reductase; NSCLC, non-small-cell lung cancer. |
Next, we analyzed the effect of MTHFR polymorphisms on the subtypes of lung cancer, especially lung adenocarcinoma, as shown in Table 3. For the C677T polymorphism, the T allele was a risk factor compared to the C allele; the T allele showed a statistically significant increase in the incidence of lung adenocarcinoma (OR =1.281, 95% CI =1.026–1.601, P=0.029). Compared with the CC genotype, the TT genotype was statistically significantly associated with risk of lung adenocarcinoma (OR =1.588, 95% CI =1.007–2.503, P=0.047), as did the recessive model (TT vs CC+CT: OR =1.438, 95% CI =1.036–1.996, P=0.030). For the A1298C polymorphism, the C allele was a protective factor compared with the A allele (OR =0.661, 95% CI =0.476–0.918, P=0.013). The statistics showed that the CC and CA genotypes of MTHFR 1298 polymorphism were associated with a significant decrease in the risk of lung adenocarcinoma, compared to the AA genotype (OR =0.215, 95% CI =0.048–0.971, P=0.046; OR =0.679, 95% CI =0.473–0.976, P=0.037).
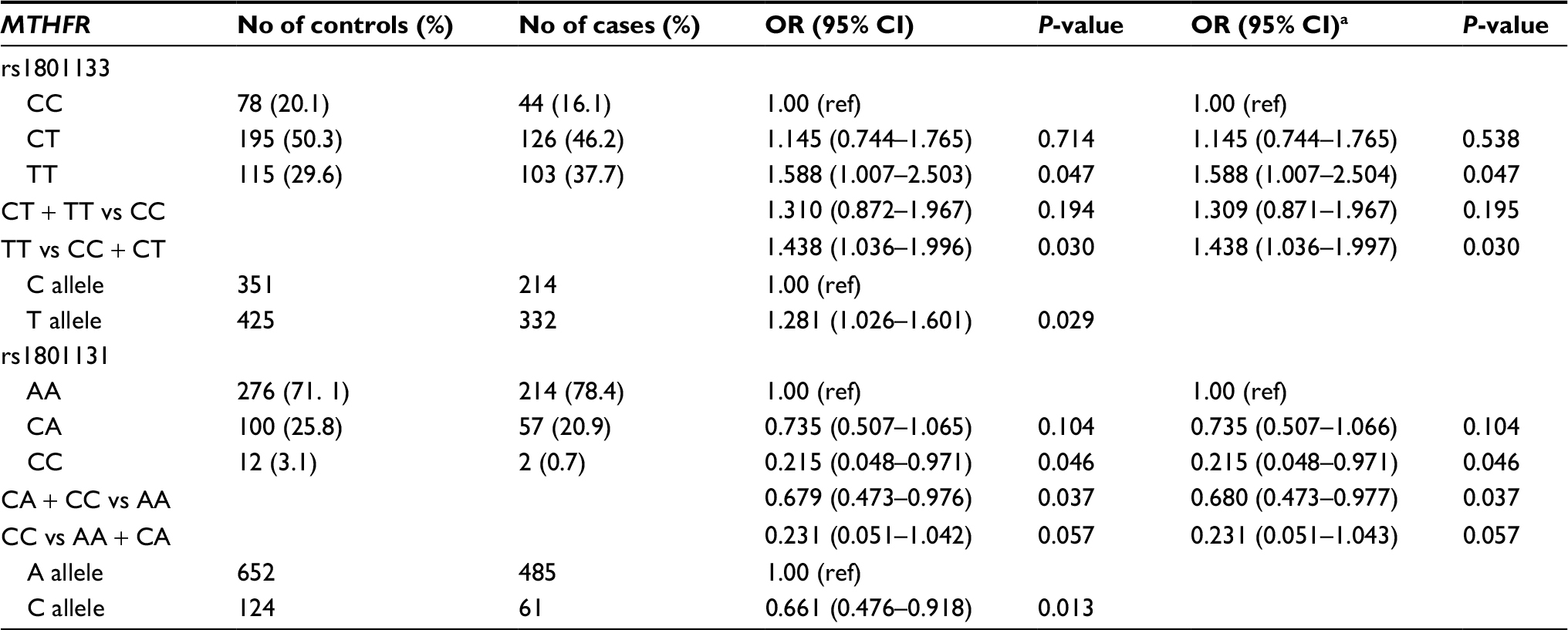 | Table 3 The relationship between the SNPs and lung adenocarcinoma risk Note: aAdjusted by age and smoking history. Abbreviations: SNP, single nucleotide polymorphism; MTHFR, methylenetetrahydrofolate reductase. |
In addition, we also analyzed the relationship between MTHFR polymorphisms and the risk of squamous cell lung carcinoma, as shown in Table 4. No association was found between the MTHFR genetic polymorphisms and risk of squamous cell lung carcinoma.
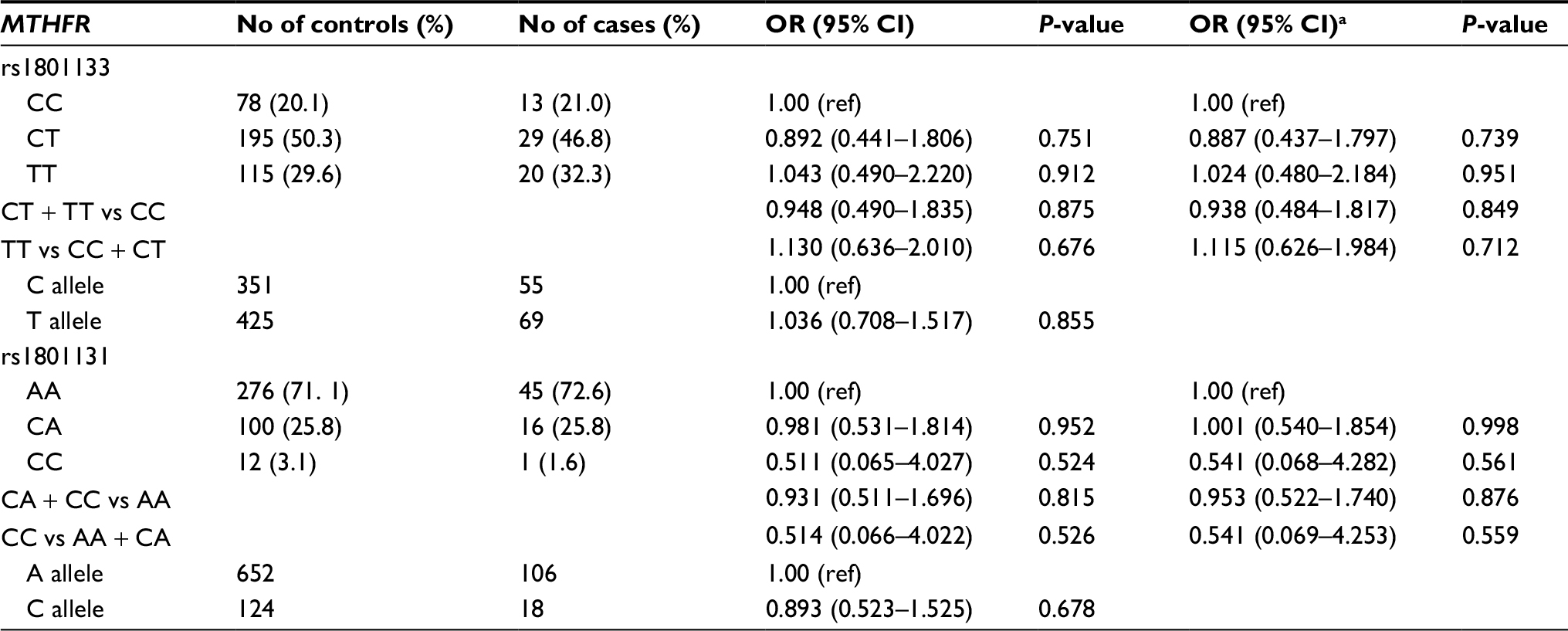 | Table 4 Correlation between MTHFR SNPs and lung squamous cell carcinoma risk Notes: aAdjusted by age and smoking history. Abbreviations: SNP, single nucleotide polymorphism; MTHFR, methylenetetrahydrofolate reductase. |
Discussion
Folate is a micronutrient that provides protection against lung carcinogenesis.32 MTHFR plays an important role in folate metabolism in vivo, where it catalyzes the irreversible conversion of its substrate 5,10-methyltetrahydrofolic acid to 5-methyltetrahydrofolic acid. 5-Methyltetrahydrofolic acid is the main form of folate in circulation in the body, and it provides the methyl group for the synthesis of methionine. As the S-adenosine methionine (SAM) precursor, methionine is converted into SAM in vivo. The major function of SAM is to provide the methyl group for the majority of biological methylation reactions in the human body, including DNA methylation.10 Abnormal changes associated with various cancers will manifest as abnormal DNA methylation, including oncogene hypermethylation and hypomethylation in the genome. DNA methylation changes caused by the abnormal expression of corresponding genes may play an important role in the occurrence of cancer. Therefore, our study of the relationship between methylenetetrahydrofolate reductase and the risk of lung cancer shows significant biological plausibility.
From our data, we have obtained evidence that the MTHFR C677T gene polymorphism was significantly associated with increased lung cancer risk in the investigated population. The risk of lung cancer for carriers with the MTHFR C677 TT genotype is 1.550 times higher than the risk for carriers of the CC genotype. The reason may be that the MTHFR enzyme activity of TT genotype carriers is weak, which affects the regulation of folate metabolism by MTHFR with a subsequent effect on the development of cancer.10 Compared to the CC encoding enzyme activity, the encoding MTHFR enzyme activity of the CT and TT genotype carriers is less than 35% and 70%, respectively.8 The low activity of the CT and TT genotypes of MTHFR toward generating the catalytic reaction products of 5-methyltetrahydrofolate, the levels of which are consequently decreased in the body, may cause abnormal changes in DNA methylation, thereby increasing the risk of cancer. Therefore, the conclusions of this study are consistent with the results of previous studies.11–13 The MTHFR C677T gene polymorphism is a risk factor for lung cancer.
Compared with the C677T gene polymorphism, the number of studies pertaining to the MTHFR A1298C gene polymorphism is relatively small. After a massive relative literature and meta-analysis was conducted, no statistically significant association was found between the MTHFR A1298C gene polymorphism and susceptibility to lung cancer,9 but in this study, we reached the conclusion that the A1298C gene polymorphism is a protective factor in lung cancer. For example, the CC genotype carriers were at lower risk to develop lung cancer than carriers of the AA genotype. This is clearly inconsistent with previous findings, so a definitive conclusion cannot be easily drawn. The reasons for this difference might be as follows: 1) the sample size may not be large enough, generating an imperceptible error that is applied to an entire population, and 2) these participants may not be appropriate representatives of the overall population, which may result in a selection bias in the study.
Several important limitations of our study are as follows. First, the selection bias may not be avoidable because all subjects were exclusively recruited from hospitals. Second, the lack of environmental risk factors limits the analyses of the gene–environment interaction. Finally, our study is limited to Chinese women. In future studies, a larger population of lung cancer patients is needed to verify the conclusion in different races. Because the result is only a statistical estimation, further experimental studies concerning the biological validity of these results are required and urged.
In summary, this study indicates that there might be correlation between the polymorphisms of the MTHFR gene and the risk of lung cancer in the female Chinese population. Nevertheless, these results still need to be further verified in the future.
Acknowledgments
We are grateful to the patients for their participation. We would like to thank all the personnel at the hospitals in our study.
Disclosure
The authors report no conflicts of interest in this work.
References
Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends – an update. Cancer Epidemiol Biomarkers Prev. 2016;25(1):16–27. | ||
Li Q, Hsia J, Yang G. Prevalence of smoking in China in 2010. N Engl J Med. 2011;364(25):2469–2470. | ||
Sun S, Schiller JH, Gazdar AF. Lung cancer in never smokers – a different disease. Nat Rev Cancer. 2007;7(10):778–790. | ||
Shields PG. Molecular epidemiology of smoking and lung cancer. Oncogene. 2002;21(45):6870–6876. | ||
Frosst P, Blom HJ, Milos R, et al. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995;10(1):111–113. | ||
Robien K, Ulrich CM. 5,10-Methylenetetrahydrofolate reductase polymorphisms and leukemia risk: a HuGE minireview. Am J Epidemiol. 2003;157(7):571–582. | ||
Goyette P, Sumner JS, Milos R, et al. Human methylenetetrahydrofolate reductase: isolation of cDNA mapping and mutation identification. Nat Genet. 1994;7(4):551. | ||
Frosst P, Blom HJ, Milos R, et al. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995;10(1):111–113. | ||
Zhang XD, Li YT, Yang SY, Li W. Meta-analysis on MTHFR polymorphism and lung cancer susceptibility in East Asian populations. Biomed Rep. 2013;1(3):440–446. | ||
Zingg JM, Jones PA. Genetic and epigenetic aspects of DNA methylation on genome expression, evolution, mutation and carcinogenesis. Carcinogenesis. 1997;18(5):869–882. | ||
Jin C, Zhang YH, Peng MF, et al. [The association between MTHFR polymorphism and lung cancer]. Chin J Cancer Prev Treat. 2007;12:888–891. Chinese. | ||
Senses KM, Gonen M, Barutcu AR, et al. Cancer-testis gene expression is associated with the methylenetetrahydrofolate reductase 677 C>T polymorphism in non-small cell lung carcinoma. BMC Med Genet. 2013;14(1):14–97. | ||
Zhu N, Gong Y, He J, et al. Influence of methylenetetrahydrofolate reductase C677T polymorphism on the risk of lung cancer and the clinical response to platinum-based chemotherapy for advanced non-small cell lung cancer: an updated meta-analysis. Yonsei Med J. 2013;54(6):1384–1393. | ||
Liu NB, Li J, Qi JF, , et al. Methylenetetrahydrofolate reductase 677TT genotype may be associated with an increased lung cancer risk in North China: an updated meta-analysis. Med Sci Monit. 2014;20:2817–2823. | ||
Yang Y, Yang LJ, Deng MZ, et al. MTHFR C677T and A1298C polymorphisms and risk of lung cancer: a comprehensive evaluation. Genet Mol Res. 2016;15(2):gmr7615. | ||
Hajiesmaeil M, Tafvizi F, Sarmadi S. The effect of methylenetetrahydrofolate reductase polymorphisms on susceptibility to human papilloma virus infection and cervical cancer. Infect Genet Evol. 2016;46:1–6. | ||
Gong JM, Shen Y, Shan WW, YX H. The association between MTHFR polymorphism and cervical cancer. Sci Rep. 2018;8(1):7244. | ||
Osian G, Procopciuc L, Vlad L, Mocan T, Cristea PG. Correlation between C677T and A1298C mutations of the MTHFR gene and therapeutic prognostic elements in colorectal cancer. Chirurgia. 2010;105(3):373–378. | ||
Yeh CC, Lai CY, Chang SN, et al. Polymorphisms of MTHFR C677T and A1298C associated with survival in patients with colorectal cancer treated with 5-fluorouracil-based chemotherapy. Int J Clin Oncol. 2017;22(3):484–493. | ||
Lin KM, Yang MD, Tsai CW, et al. The role of MTHFR genotype in colorectal cancer susceptibility in Taiwan. Anticancer Res. 2018;38(4):2001–2006. | ||
Naghibalhossaini F, Mokarram P, Khalili I, et al. MTHFR C677T and A1298C variant genotypes and the risk of microsatellite instability among Iranian colorectal cancer patients. Cancer Genet Cytogenet. 2010;197(2):142–151. | ||
Hardi H, Melki R, Boughaleb Z, El Harroudi, Aissaoui S, Boukhatem N. Significant association between ERCC2 and MTHR polymorphisms and breast cancer susceptibility in Moroccan population: genotype and haplotype analysis in a case-control study. BMC Cancer. 2018;18(1):292. | ||
Xia LZ, Liu Y, Xu XZ, et al. Methylenetetrahydrofolate reductase C677T and A1298C polymorphisms and gastric cancer susceptibility. World J Gastroenterol. 2014;20(32):11429–11438. | ||
Lv L, Wang P, Sun B, Chen G. The polymorphism of methylenetetrahydrofolate reductase C677T but not A1298C contributes to gastric cancer. Tumour Biol. 2014;35(1):227–237. | ||
Lin J, Zeng RM, Li RN, Cao WH. Aberrant DNA methylation of the P16, MGMT, and hMLH1 genes in combination with the methylenetetrahydrofolate reductase C677T genetic polymorphism and folate intake in gastric cancer. Genet Mol Res. 2014;13(1):2060–2068. | ||
Chen PL, Li WT, Wang J, et al. Association between MTHFR gene polymorphisms (C677T, A1298C) and genetic susceptibility to prostate cancer: a meta-analysis. Genet Mol Res. 2015;14(4):19191–19202. | ||
You W, Li Z, Jing C, et al. MTHFR C677T and A1298C polymorphisms were associated with bladder cancer risk and disease progression: a meta-analysis. DNA Cell Biol. 2013;32(5):260–267. | ||
Kałużna EM, Strauss E, Świątek-Kościelna B, et al. The methylenetetrahydrofolate reductase 677T-1298C haplotype is a risk factor for acute lymphoblastic leukemia in children. Medicine. 2017;96(51):e9290. | ||
Mashhadi MA, Miri-Moghaddam E, Arbabi N, et al. C677T and A1298C polymorphisms of methylene tetrahydrofolate reductase in non-Hodgkin lymphoma: southeast Iran. Tumori. Epub 2017 Apr 1. | ||
Zhang J, Zhou YW, Shi HP, et al. 5,10-Methylenetetrahydrofolate reductase (MTHFR), methionine synthase (MTRR), and methionine synthase reductase (MTR) gene polymorphisms and adult meningioma risk. J Neurooncol. 2013;115(2):233–239. | ||
Liu N, Jiang J, Song YJ, et al. Impact of MTHFR polymorphisms on methylation of MGMT in glioma patients from Northeast China with different folate levels. Genet Mol Res. 2013;12(4):5160–5171. | ||
Voorrips LE, Goldbohm RA, Brants HA, et al. A prospective cohort study on antioxidant and folate intake and male lung cancer risk. Cancer Epidemiol Biomarkers Prev. 2000;9(4):357–365. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.