")
Back to Journals » Patient Preference and Adherence » Volume 15
Motivational Factors for Smoking Behaviors in Individuals with Metabolic Syndrome
Authors Park M , Kang B , Ryu A , Li Y , Song R
Received 22 October 2021
Accepted for publication 7 December 2021
Published 23 December 2021 Volume 2021:15 Pages 2847—2854
DOI https://doi.org/10.2147/PPA.S343874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Moonkyoung Park, Baram Kang, Ahyun Ryu, YueLin Li, Rhayun Song
College of Nursing, Chungnam National University, Daejeon, Republic of Korea
Correspondence: Baram Kang Tel +1 512 839 7227
Fax +82 42 580 8309
Email [email protected]
Purpose: Smoking, which is one of the major risk factors for metabolic syndrome that causes cardiovascular disease or diabetes, is a crucial risk factor, which is modifiable. This study aimed to determine the factors that promote smoking behaviors according to smoking status among adults with metabolic syndrome.
Patients and Methods: A survey of structured self-reported questionnaires was conducted on 152 adults with metabolic syndrome. Outcome variables included cognitive motivations (self-efficacy, and perceived benefits and barriers), emotional motivation (emotional salience), and autonomous and controlled motivation based on self-determination theory. The participants were categorized by their smoking status (never smoking, quit smoking, or current smoking). Their sociodemographic and motivational factors were examined using one-way analysis of variance, analysis of covariance, and multinomial logistic regression analysis.
Results: Data on 152 individuals with metabolic syndrome with a mean age of 57.5 years were included. The findings indicated that the motivational factors for the never-smoking and quit-smoking groups significantly differed from those for the current-smoking group in terms of self-efficacy, perceived benefits, perceived barriers, and autonomous motivation. Based on multinomial logistic regression with current smoking as the reference group, sex (being female, OR=57.69) and perceived barriers (OR=0.39) were the significant predictors for the never-smoking group, while autonomous motivation (OR=1.96) was the significant predictor for the quit-smoking group.
Conclusion: The motivational factors for smoking behaviors varied according to the smoking status of adults with metabolic syndrome. Autonomous motivation was the significant predictor of smoking cessation for individuals who successfully quit, whereas cognitive motivation was influential in the prevention of smoking by individuals who have never smoked. Further studies are warranted to develop smoking cessation strategies, which should focus on specific motivational factors to lead effective smoking prevention programs in this population.
Keywords: smoking cessation, motivation, metabolic syndrome, health behavior
Introduction
Metabolic syndrome represents the presence of three or more of the following cluster of conditions in a person: central obesity, hypertension, dyslipidemia, and impaired fasting glucose, which is associated with increased mortality and the development of chronic illnesses such as cardio-cerebrovascular disease and type 2 diabetes.1,2 Although the pathogenic mechanism of metabolic syndrome is unclear, central obesity and insulin resistance are considered to be its major causes.3
Health behavior modification is essential in controlling risk factors for individuals with metabolic syndrome.4 Smoking, which is one of the main risk factors of metabolic syndrome, increases insulin resistance,5 elevates triglyceride levels by affecting lipid metabolism,6,7 and increases central obesity by altering the fat distribution even when the body mass index of the individual remains consistent.8 Smoking hinders the quality of life and affects disease processes and the treatment of chronic illnesses including metabolic syndrome, diabetes, and cardiovascular and inflammatory diseases.9 For current smokers, life expectancy is at least 10 years shorter compared with non-smokers. Smoking cessation before the age of 40 reduces the risk of premature death from the smoking-induced disease by nearly 90%,10 which indicates that smoking can be a major preventable risk factor of cardiovascular diseases. Globally, cardiovascular disease is the leading cause of death.11 In line with that, heart disease has occupied second place among the top 10 primary causes of death in South Korea.12 Despite the active efforts of the government public health sector, the smoking rate among Korean adults in 2018 was 22.4%,13 which was higher than those in the United States and Japan.14
Quitting smoking could be beneficial for individuals with diabetes or cardiovascular disease, yet less than 50% of the smokers in this population have been reported to have successfully ceased smoking.15 Cognitive motivational factors have been indicated to play key roles in individuals with metabolic syndrome performing various health behaviors, which could encourage individuals to progress from the preparatory stage to the action or maintenance stage of behavioral change.16 However, that study found that smoking-related behaviors were not sufficiently explained by cognitive motivational factors, possibly due to the addictive nature of smoking.17 More research is needed to conclusively identify the factors influencing the performance of specific health behaviors.
Individual motivation is a pivotal factor for changing health behaviors in individuals.18 According to social cognitive theory, the behavior of an individual is determined by their ability, internal and external reinforcement, self-efficacy, and the interactions of various cognitive factors such as perceived benefits and barriers.19 There is also contention about positive or negative emotions affecting health behaviors, which are integrated and reflected when implementing behaviors.20 While cognitive and emotional processes precede the actual performing of specific health behaviors by an individual, the transtheoretical model addresses behavioral changes by considering factors such as planning and decision-making during behavioral transitions.21,22 Intention and motivational factors to quit smoking appear to not be sufficient preconditions for successful smoking cessation.23 Cognitive motivational factors such as self-efficacy may motivate for individuals to initiate health behaviors, but competence alone may not be sufficient to ensure the maintenance of this modification.24
As a way to explain why an individual initiates and maintains health-related behaviors, self-determination theory focuses on autonomous motivation, which is considered an influencing factor that leads to positive behavioral changes in humans.24 While it is plausible that there is a unique set of motivational factors that influence addictive smoking-related behaviors, it has not been verified. Given that multiple motivational factors affect smoking behaviors according to behavioral changes, applying diverse motivation strategies depending on smoking status, such as current smoking, quitting smoking, or having never smoked, might be an effective method for behavioral modification.
This study aimed to identify if and how cognitive, emotional, and autonomous motivations influence the smoking status of individuals diagnosed with metabolic syndrome, and present suggestions for providing intervention strategies based on smoking status that can be applied to each behavior for smoking prevention and cessation.
Materials and Methods
Study Design
This cross-sectional, correlational study explored the motivational factors for smoking behaviors among individuals with metabolic syndrome.
Participants
This study selected individuals with metabolic syndrome as a target population. As a leading cause of death for decades, cardiovascular diseases attributed to smoking are closely interrelated with the cluster of clinical conditions of metabolic syndrome. Metabolic syndrome may be the most appropriate health condition given its close connection to smoking. Convenience sampling of adults with metabolic syndrome at the outpatient clinics of a university hospital recruited 152 patients, who completed a questionnaire on demographic information, smoking history, and motivational factors for smoking-related health behaviors. Quit smoking group was defined as those who quitted smoking more than 6 months. Those who either currently smoke or quitted recently (less than 6 months prior) were categorized as current smokers. Never smoking group was defined as those who responded that they never smoked before or never smoked within the past 5 years. The subjects were categorized into three groups based on their smoking status: never smoking (n=82), current smoking (n=23), or quit smoking (n=47). Power analysis was performed to determine the sample size required for the analysis of variance (ANOVA),25 and applied an effect size of 0.25 based on a previous study of motivations for smoking behavior.16 The required sample size was 147 cases for a power of 0.80, and the obtained data on 152 adults were therefore sufficient for the analysis.
Instruments
General Characteristics
The sociodemographic characteristics of the subjects were assessed using questions relating to age, sex, education duration, economic status, marital status, and chronic diseases including metabolic syndrome diagnoses. The smoking status was assessed with specific categories from never smoked, quit smoking (6–12 months, 1–5 years, or 5 years or more) to current smoking with the number of cigarettes per day, then finally categorized into three categories of (1) those who currently smoke, (2) those who had quit smoking for more than 6 months, and (3) those who had never smoked before or never smoked within the past 5 years.
Cognitive and Emotional Motivational Factors
Motivational factors were assessed using a motivation scale for health behaviors based on social learning theory and emotional motivation.26 The scale consisted of self-efficacy (ten items), perceived benefits (seven items), perceived barriers (ten items), and emotional salience (eleven items), which were scored from 1 (“completely disagree”) to 7 (“completely agree”). The negative items of the emotional salience subscale were reverse coded so that higher scores reflected a preference for performing specific health behaviors. Cronbach’s alpha for the current study was 0.89 (0.72 to 0.82 for the subscales).
Autonomous Motivation
Autonomous motivation for smoking behaviors was measured using the Treatment Self-Regulation Questionnaire (TSRQ), which is based on self-determination theory.27 The TSRQ for smoking behaviors assessed the motivational factors based on the performance of smoking-related health behaviors, and consisted of non-self-determined extrinsic motivation and self-determined extrinsic motivation (six items each) on a 7-point Likert-type scale (1 for “not at all” to 7 for “definitely yes”). Higher scores on the TSRQ reflect high autonomous or controlled motivation in performing smoking-related health behaviors. Cronbach’s alpha for the internal consistency of the scale in the original development study was 0.80,27 while that in the current study it was 0.88 (0.84 for each of the subscales of autonomous and controlled motivation).
Statistical Analysis
The statistical analysis in this study was conducted using SPSS for Windows (version 26). Cronbach’s alpha coefficients were used to determine the reliability of the scales. Descriptive statistics were used to describe the sociodemographic characteristics of the subjects and study outcome variables using means, standard deviations, frequencies, and percentages. One-way ANOVA was used to compare sociodemographic characteristics according to smoking statuses. Analysis of covariance (ANCOVA) was used to compare motivational factors according to smoking status while considering covariates, but the perceived benefits and autonomous and controlled motivation variables that did not conform to a normal distribution were analyzed using ranked ANCOVA. Multinomial logistic regression was conducted to identify the motivational factors for the never-smoking and quit-smoking groups while using the current-smoking group as the reference.
Results
General Characteristics According to Smoking Status
Age, education duration, sex, and chronic diseases differed significantly with the smoking status (Table 1). The mean age of the study participants was 57.5 years, while those who had never smoked were older than those who had quit or were currently smoking. The current-smoking group had the longest mean education duration of 14.4 years. The never-smoking group was mostly female (79.3%), whereas males comprised 87% of those in the quit-smoking and current-smoking groups. Among the markers of metabolic syndrome, 89% of the never-smoking group had central obesity, 73.9% of the current-smoking group had high triglyceride levels, and 56.9% of the quit-smoking group had low HDL cholesterol. However, no significant differences were found in metabolic syndrome markers by smoking status.
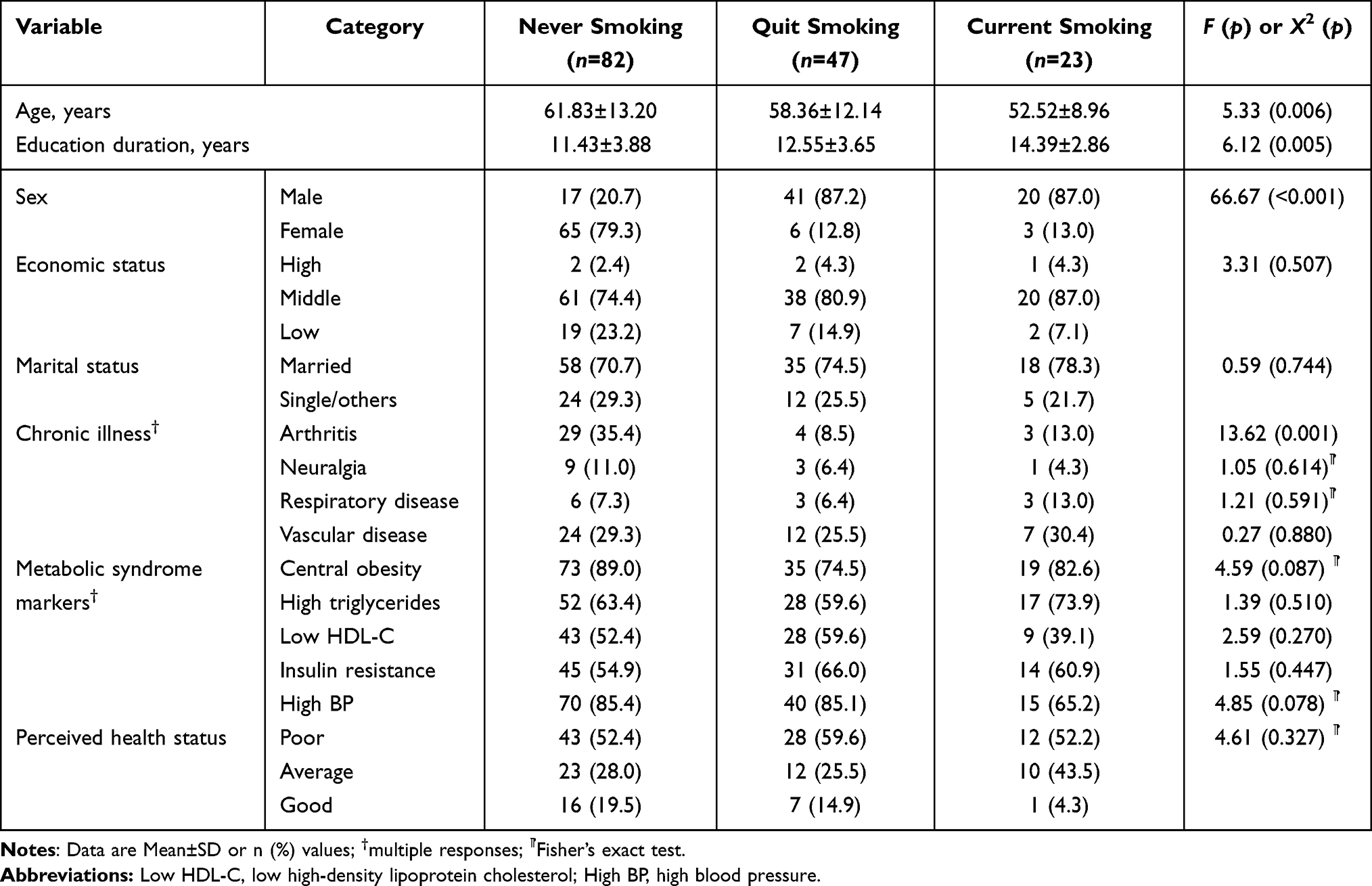 |
Table 1 General Characteristics of the Participants According to Smoking Status (N=152) |
Differences in Motivational Factors According to Smoking Status
Different sets of motivational factors affected the never-smoking, quit-smoking, and current-smoking groups (Table 2). Individuals in the never-smoking group had higher self-efficacy (F=5.23, p=0.006) and lower perceived barriers (F=3.28, p=0.004) than those in the current-smoking group. Individuals in the quit-smoking group had higher self-efficacy, lower perceived barriers, higher perceived benefits (F=4.92, p=0.009), and higher autonomous motivation (F=8.77, p<0.001) than those in the current-smoking group. Emotional salience and controlled motivation did not differ significantly between the smoking status groups.
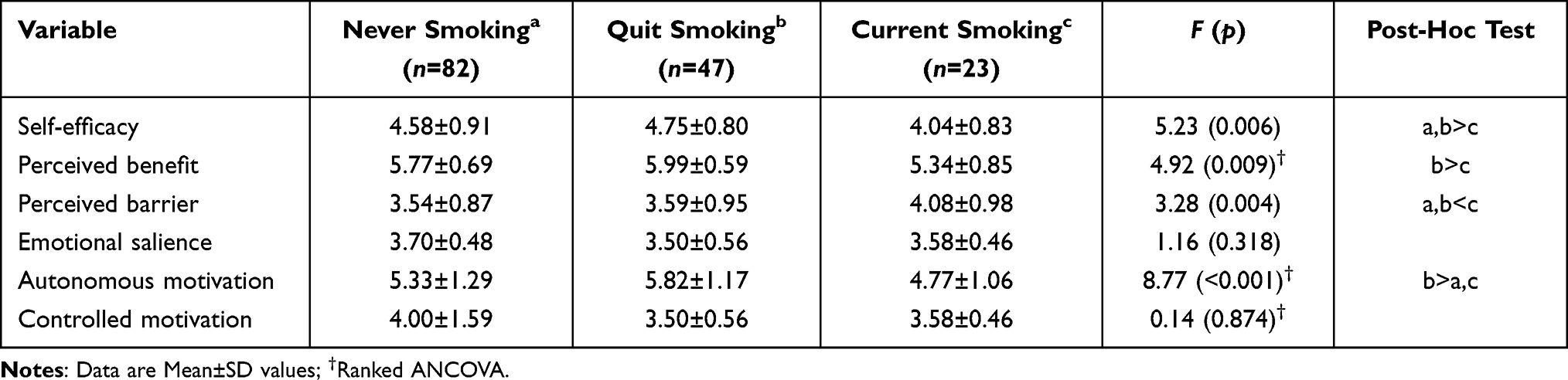 |
Table 2 Differences in Motivational Factors According to Smoking Status (N=152) |
Predictors of Smoking Status
Predictors of smoking status (never smoking or quit smoking vs current smoking) were examined using multinomial logistic regression (Table 3). The general characteristics of age, sex (female), and education duration (years) were controlled to identify the motivational factors that predict each smoking status. The model with motivational factors and covariates explained from 53.2% (Cox and Snell R2) to 61.9% (Nagelkerke R2) of the variance in smoking status (X2[14]=115.33, p<0.001). With the current-smoking group as a reference, being female (OR=57.69, 95% CI=8.85–375.98) and perceived barriers (OR=0.39, 95% CI=0.15–0.99) were the most significant predictors for the never-smoking group (n=82) after controlling for age, sex, and education duration. However, autonomous motivation (OR=1.96, 95% CI=1.13–2.11) was the most significant predictor for the quit-smoking group (n=47) after controlling for general characteristics.
 |
Table 3 Predictors of Smoking Behaviors from Multinomial Logistic Regression (N=152) |
Discussion
Modifying health behaviors, specifically smoking cessation, is crucial for managing the markers of metabolic syndrome. This study was conducted to identify the effects of cognitive, emotional, and autonomous motivations that could induce smoking-related behavioral changes according to the smoking status of an individual. The findings indicated that different sets of motivational factors were associated with performing smoking-related health behaviors in the never-smoking, quit-smoking, and current-smoking groups.
Cognitive motivation is required to change how individuals implement health behaviors.19 Analyzing motivational factors according to smoking status indicated that self-efficacy and perceived barriers were significant for individuals in the never-smoking and quit-smoking groups. Self-efficacy, or the confidence of individuals in their ability to abstain from smoking, is associated with a likelihood of initiating and maintaining changes in smoking behaviors.28 A meta-analysis found a strong relationship between self-efficacy and future smoking abstinence, but suggested the importance of controlling for concurrent smoking status as a potential confounding variable.29 Self-efficacy was hypothesized to vary over time, and to predict proximal behaviors better than distal behaviors.29 Previous studies support the role of self-efficacy in the attempts of current smokers to quit.30 There was a bidirectional relationship between current smoking status and self-efficacy. Increasing confidence in quitting smoking after an attempt is important for increasing and maintaining the probability of successful cessation.31 However, the motivation to attempt to quit differed from the motivation that leads to success in quitting.30
Among cognitive motivational factors, perceived benefits were significantly higher in the quit-smoking group than in the current-smoking group. Similarly, the perceived benefits of quitting smoking had a positive correlation with intentions of quitting among newly diagnosed cancer patients.32 Perceived benefits have a positive association with the motivations involved in smoking cessation, regardless of sex.33
Perceived barriers were significantly higher in the current-smoking group than in the never-smoking or quit-smoking groups. Barriers are often conceptualized as either structural psychosocial factors (ie, lack of accessible smoking cessation programs) or individual psychosocial factors (ie, subjective experience of physical nicotine addiction).34 A study involving a socially disadvantaged population in Poland found that the most common barriers perceived by current smokers were lack of support, addiction and withdrawal symptoms, and stress.35 Similarly, a national survey of 699 young adult current smokers identified “loss of a way to handle stress” and “cravings or withdrawal” as barriers to quitting.36
A previous systematic literature review identified a broad range of barriers for smoking cessation, including social, socioeconomic, and environmental factors that are interconnected with individual lifestyle factors.37 Those individual lifestyle factors could be modified by interventions to motivate individuals to attempt to quit smoking. Given the result of the current study that perceived barriers was a significant factor differentiating the never-smoking and current-smoking groups, intervention strategies should focus on modifiable psychological and behavioral barriers that hinder decisions when selecting and initiating smoking-related health behaviors. Community social support and policy establishment may reduce barriers for smoking cessation, along with an individual approaches such as stress management for diminishing the cognitive, social, and economic barriers that smokers experience when attempting to quit smoking.35
Autonomous motivation was significantly more important in the quit-smoking group than in the never-smoking or current-smoking groups. Multinomial logistic regression indicated that autonomous motivation was the most significant predictor (OR=1.96) for the quit-smoking group after controlling for age, sex, and education duration. A previous study on smoking behaviors indicated that, while self-efficacy was an independent variable for cessation at an early stage, autonomous motivation was positively correlated with an increased intention to quit.38 In a motivational interview-based study on smoking cessation, Cupertino et al also indicated that higher self-efficacy and higher autonomous motivation at the baseline can lead to smoking cessation.39 Self-determination theory suggests that behavioral changes might be initiated by controlled motivation, which induces engagement in certain behaviors, but complete behavioral changes can ultimately be accomplished by self-directed determination, which is a form of autonomous motivation.24 In other words, individuals would become capable of making changes independently and would be more likely to maintain behavioral changes through internalizing motivations.38
These cognitive and autonomous motivations eventually play meaningful roles in encouraging smokers to initiate smoking cessation and to ultimately quit, which should be the focus when designing programs for smoking cessation. By utilizing relevant motivational factors according to smoking status, more effective intervention strategies can be implemented for the health behavior modification of individuals with metabolic syndrome. This approach potentially will persuade them into maintaining a healthier lifestyle and enhance their quality of life. While our findings indicated that controlled motivation was not a statistically significant factor in smoking behaviors according to smoking status, Cupertino et al suggested that controlled motivation can lead to enhanced self-efficacy, which in turn predicts smoking cessation.39 Individual smoking behaviors are influenced by smoking legislation, the environment, or even by a peer group’s attitude toward smoking behaviors.40 For example, in Korea, smoking is forbidden inside of buildings and at most of public places, which in turn likely affects the smoking behaviors of people in Korea. Therefore, the role of controlled motivation along with environmental factors in smoking-associated behaviors requires further investigation.
There are some limitations that should be considered when interpreting the findings of this study. We identified different sets of motivational factors to predict smoking behaviors. While smoking behaviors were difficult to predict with cognitive or emotional motivational factors in previous studies, our findings suggested that autonomous motivation predicts smoking cessation specifically in the quit-smoking group. Cognitive and emotional motivations could play a role in initiating health behaviors, but autonomous motivation could help the current smokers to quit smoking. However, our findings from the survey design of this study proposed a further study with a randomized clinical trial to see the effect of autonomous motivation on quitting smoking. Since information about smoking history, including smoking status, was self-reported by participants in our study, the number of actual smokers may have been underestimated. We suggest that further studies including biochemical confirmation would be beneficial in order to examine whether there is a discrepancy between the self-reported abstinence and the actual state of smoking abstinence.
We categorized the smoking statuses of the participants based on the transtheoretical model of behavior change after completion of the sampling procedure, which resulted in an uneven number of subjects with each smoking status. The assumptions for descriptive statistics were confirmed prior to the statistical analysis, yet the relatively small number of subjects in the current-smoking group may have compromised the power of the study. Additionally, the motivational factors for smoking cessation might also be influenced by smoking behavior attributes such as smoking dependency or frequency,30 which were not included in our analysis. Further studies are warranted to examine the specific roles of cognitive and autonomous motivations on the initiation and maintenance of smoking behaviors with larger samples that better represent each smoking status or with data from other groups such as the general population or individuals with different diseases.
Conclusion
This research was conducted to identify the motivational factors for smoking-associated health behaviors of individuals with metabolic syndrome. The different sets of motivational factors played different roles in the smoking status of the individuals. Cognitive motivations such as self-efficacy and perceived barriers may influence smoking prevention for those who have never smoked, while autonomous motivation could lead to successful cessation. This implies that cognitive and autonomous motivations need to be included in order to induce smoking cessation. We suggest to develop and evaluate smoking cessation programs containing cognitive and autonomous motivations in further research.
Ethics Approval and Informed Consent
The Institutional Review Board of Chungnam National University approved the survey (no. 2-1046881-AN-01-210401-HR-002), which was conducted according to the guidelines of the Declaration of Helsinki. Informed consent was obtained from all study subjects.
Acknowledgments
The authors appreciate all participants who contribute to this research work for their dedication and meaningful insight.
Funding
This study was supported by the National Research Foundation in Korea (Grant number: 2017R1A2B4006775).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oh JE. Association between smoking status and metabolic syndrome in men. Korean J Obes. 2014;23(2):99–105. doi:10.7570/kjo.2014.23.2.99
2. Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005;28(7):1769–1778. doi:10.2337/diacare.28.7.1769
3. Eckel RH, Alberti KG, Grundy SM, et al. The metabolic syndrome. Lancet. 2010;375(9710):181–183. doi:10.1016/S0140-6736(09)61794-3
4. Jellinger PS, Handelsman Y, Rosenblit PD, et al. American Association of Clinical Endocrinologists and American College of Endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. 2017;23:1–87. doi:10.4158/EP171764.APPGL
5. Chiolero A, Faeh D, Paccaud F, et al. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am J Clin Nutr. 2008;87(4):801–809. doi:10.1093/ajcn/87.4.801
6. Babushkina EA, Belokopytova LV, Grachev AM, et al. Variation of the hydrological regime of Bele-Shira closed basin in Southern Siberia and its reflection in the radial growth of Larix sibirica. Regional Environ Change. 2017;17(1):1725–1737. doi:10.1007/s10113-017-1137-1
7. Jo A, Oh H. Incidence of colon cancer related to cigarette smoking and alcohol consumption in adults with metabolic syndrome: prospective cohort study. J Korean Acad Nurs. 2019;49(6):713–723. doi:10.4040/jkan.2019.49.6.713
8. Tran BT, Jeong BY, Oh J-K. The prevalence trend of metabolic syndrome and its components and risk factors in Korean adults: results from the Korean National Health and Nutrition Examination Survey 2008–2013. BMC Public Health. 2017;17(1):71. doi:10.1186/s12889-016-3936-6
9. Ford ES, Li C. Metabolic syndrome and health-related quality of life among US adults. Ann Epidemiol. 2008;18(3):165–171. doi:10.1016/j.annepidem.2007.10.009
10. Centers fro Disease Control and Prevention. Tobacco-Related Mortality. CDC; 2020. Available from: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/tobacco_related_mortality/index.htm#death.
11. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
12. Causes of Death Statistics in 2020. Statistics Korea; 2021. Available from: http://kostat.go.kr/portal/eng/pressReleases/8/10/index.board?bmode=read&bSeq=&aSeq=414516&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt=.
13. Trends in Smoking Rate. KOSIS; 2020. Available from: https://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_11702_N001.
14. Reitsma MB, Fullman N, Ng M, et al. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885–1906. doi:10.1016/s0140-6736(17)30819-x
15. Rigotti NA, Singer DE, Mulley AG, et al. Smoking cessation following admission to a coronary care unit. J Gen Intern Med. 1991;6(4):305–311. doi:10.1007/BF02597426
16. Song R, Park MK. Motivation factors for stages of behavioral change among individuals with metabolic syndrome. Korean J Adult Nurs. 2018;30(1):60–69. doi:10.7475/kjan.2018.30.1.60
17. Joe K, Kim D. Smoking as an addictive disorder. J Korean Neuropsychiatr Assoc. 2009;48(4):213–219.
18. Bassi N, Karagodin I, Wang S, et al. Lifestyle modification for metabolic syndrome: a systematic review. Am J Med. 2014;127(12):
19. Tougas ME, Hayden JA, McGrath PJ, et al. A systematic review exploring the social cognitive theory of self-regulation as a framework for chronic health condition interventions. PLoS One. 2015;10(8):e0134977. doi:10.1371/journal.pone.0134977
20. Song R. Analyzing motivational factors to predict health behaviors among older adults. Korean J Adult Nurs. 2006;18(4):523–532.
21. Bledsoe LK. Smoking cessation: an application of theory of planned behavior to understanding progress through stages of change. Addict Behav. 2006;31(7):1271–1276. doi:10.1016/j.addbeh.2005.08.012
22. Atak N. A transtheoretical review on smoking cessation. Int Q Community Health Educ. 2007;28(2):165–174. doi:10.2190/IQ.28.2.f
23. Smit ES, Hoving C, Schelleman-Offermans K, et al. Predictors of successful and unsuccessful quit attempts among smokers motivated to quit. Addict Behav. 2014;39(9):1318–1324. doi:10.1016/j.addbeh.2014.04.017
24. Ryan RM, Patrick H, Deci EL, et al. Facilitating health behaviour change and its maintenance: interventions based on self-determination theory. Eur Health Psychol. 2008;10(1):2–5.
25. Faul F, Erdfelder E, Lang AG, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
26. Song R, June KJ, Kim CG, et al. Comparisons of motivation, health behaviors, and functional status among elders in residential homes in Korea. Public Health Nurs. 2004;21(4):361–371. doi:10.1111/j.0737-1209.2004.21410.x
27. Levesque CS, Williams GC, Elliot D, et al. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ Res. 2007;22(5):691–702. doi:10.1093/her/cyl148
28. Prochaska JO, DiClemente CC. Self change processes, self efficacy and decisional balance across five stages of smoking cessation. Prog Clin Biol Res. 1984;156:131–140.
29. Gwaltney CJ, Metrik J, Kahler CW, et al. Self-efficacy and smoking cessation: a meta-analysis. Psychol Addict Behav. 2009;23(1):56–66. doi:10.1037/a0013529
30. Klemperer EM, Mermelstein R, Baker TB, et al. Predictors of smoking cessation attempts and success following motivation-phase interventions among people initially unwilling to quit smoking. Nicotine Tob Res. 2020;22(9):1446–1452. doi:10.1093/ntr/ntaa051
31. Clyde M, Pipe A, Reid R, et al. A bidirectional path analysis model of smoking cessation self-efficacy and concurrent smoking status: impact on abstinence outcomes. Addict Biol. 2019;24(5):1034–1043. doi:10.1111/adb.12647
32. Hall DL, Neil JM, Ostroff JS, et al. Perceived cancer-related benefits of quitting smoking and associations with quit intentions among recently diagnosed cancer patients. J Health Psychol. 2021;26(6):831–842. doi:10.1177/1359105319845131
33. McKee SA, O’Malley SS, Salovey P, et al. Perceived risks and benefits of smoking cessation: gender-specific predictors of motivation and treatment outcome. Addict Behav. 2005;30(3):423–435. doi:10.1016/j.addbeh.2004.05.027
34. Melnyk KA. Barriers: a critical review of recent literature. Nurs Res. 1988;37(4):196–201. doi:10.1097/00006199-198807000-00002
35. Milcarz K, Polańska K, Ł B, et al. Perceived barriers and motivators to smoking cessation among socially-disadvantaged populations in Poland. Int J Occup Med Environ Health. 2019;32(3):363–377. doi:10.13075/ijomeh.1896.01377
36. Villanti AC, Bover Manderski MT, Gundersen DA, et al. Reasons to quit and barriers to quitting smoking in US young adults. Fam Pract. 2016;33(2):133–139. doi:10.1093/fampra/cmv103
37. Twyman L, Bonevski B, Paul C, et al. Perceived barriers to smoking cessation in selected vulnerable groups: a systematic review of the qualitative and quantitative literature. BMJ Open. 2014;4(12):e006414. doi:10.1136/bmjopen-2014-006414
38. Williams GC, Gagné M, Ryan RM, et al. Facilitating autonomous motivation for smoking cessation. Health Psychol. 2002;21(1):40–50. doi:10.1037/0278-6133.21.1.40
39. Cupertino AP, Berg C, Gajewski B, et al. Change in self-efficacy, autonomous and controlled motivation predicting smoking. J Health Psychol. 2012;17(5):640–652. doi:10.1177/1359105311422457
40. Yang JJ, Song M, Yoon HS, et al. What are the major determinants in the success of smoking cessation: results from the health examinees study. PLoS One. 2015;10(12):e0143303. doi:10.1371/journal.pone.0143303
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.