")
Back to Journals » Substance Abuse and Rehabilitation » Volume 6
Motivation to maintain sobriety among residents of sober living recovery homes
Received 27 May 2015
Accepted for publication 6 July 2015
Published 11 September 2015 Volume 2015:6 Pages 103—111
DOI https://doi.org/10.2147/SAR.S89361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Li-Tzy Wu
Douglas L Polcin, Rachael Korcha
Alcohol Research Group, Public Health Institute, Emeryville, CA, USA
Background: The study of motivation in the substance abuse field has typically examined the extent to which substance users want to quit or reduce substance use. Less frequently examined is the desire to maintain sobriety after achieving abstinence. The current study examined motivation to maintain sobriety among residents of sober living houses (SLHs), a type of recovery home for individuals with alcohol and drug problems. Previous research on this population showed favorable longitudinal outcomes over 18 months. Resident views about the costs of not using substances (ie, the difficulties encountered when not using), as well as the perceived benefits of not using, were strong predictors of substance use outcomes.
Methods: This study adds to these findings by conducting two focus groups with individuals familiar with the structure and day-to-day operations of SLHs, including administrators of SLH organizations, owners, and peer managers
Results: Focus group results supported the importance of costs and benefits as motivational forces influencing abstinence. However, participants also emphasized characteristics of the sober living recovery environment as important factors influencing motivation. Interactions among recovering peers offer unique opportunities for feeling understood, recognizing vulnerability in others, identifying with the recovery processes of others, receiving supportive confrontation, and engaging in mutual accountability. These experiences are important elements of motivation that become activated by involvement in the SLH environment and are difficult to replicate outside of that context.
Conclusion: In addition to recognizing how motivation can be enhanced by addressing costs and benefits experienced by individuals, operators of recovery homes need to understand motivation as a function of the recovery home social environment. Additional studies are needed on motivation as a longitudinal construct in a variety of peer-oriented environments. Studies are also needed to better specify interactions within SLHs that increase and hinder motivation among different types of residents.
Keywords: recovery residence, sober living house, social model, social environment
Introduction
Studies assessing motivation for change in the literature on addiction have found significant but modest associations between motivation and subsequent treatment outcome.1,2 Most of these studies have been limited in a number of respects. First, studies typically measure motivation only at treatment entry and overlook how motivation can change over time. Second, studies on motivation have typically addressed motivation to stop or reduce use of alcohol and drugs. Motivation to maintain abstinence from drugs and alcohol among individuals who have ceased their substance use has largely been ignored. Finally, motivation has typically been studied within the context of formal treatment programs. We therefore know little about motivation after treatment completion or among persons participating in peer-oriented services, such as 12-step programs or residential recovery homes.
Research conducted by Korcha et al3 was an exception to the typical studies on motivation. They studied motivation at three 6-month intervals among 167 individuals entering residential recovery homes in California. They assessed motivation to maintain sobriety in addition to motivation to quit or reduce substance use. Motivation was measured using the costs and benefits subscales of the Alcohol and Drug Consequences Questionnaire (ADCQ),4 which was conceptualized using perceived costs and benefits of continuing sobriety. Examples of costs included items such as “I will have difficulty relaxing”, “I will get depressed”, and “I will feel bored”. Examples of benefits include items such as “I will have a better relationship with my family”, “I will feel better about myself”, and “I will be more active and alert”. Overall, participants expressed strong motivation for sobriety; they consistently reported higher perceptions of benefits than costs of sobriety at each interview.
With the use of lagged generalized estimating equation models across time, higher scores on the ADCQ costs scale consistently predicted increased substance use and severity of problems related to use. Higher scores on the benefits scale predicted better alcohol and drug outcomes, although the effects were less consistent and weaker than the costs scales. In a follow-up analysis, Korcha et al5 found that the cost scale was resilient; it was not moderated by a variety of social and demographic factors that the researchers examined. However, an analysis by Polcin et al6 found that high costs were particularly strong predictors among persons with high psychiatric severity. Korcha et al5 found that the benefits scale was particularly influential between two subgroups: persons who had low affiliation with 12-step recovery groups and persons who had large social networks. The authors concluded that involvement in 12-step programs was a strong, resilient predictor of good outcome and individual perceptions about benefits only became important when participants had decreased 12-step attendance and activities. Among persons with large social networks, recognition of benefits was thought to operate as a prophylaxis to the high-risk situations that one might be increasingly exposed to when engaged in a large social network.
Purpose
The purpose of the current study was to expand upon the quantitative findings reported earlier by eliciting views about motivation from persons who actively work with sober living houses (SLHs) and SLH residents on a daily basis, including administrators of SLH associations, owners of the homes, and house managers. While our findings for the influence of perceived costs and benefits on sobriety were compelling, we surmised there might be a variety of motivational influences not tapped by the ADCQ that could be identified by these individuals. In addition, we wanted to better understand our quantitative findings by hearing how our focus group participants viewed them. Based on our findings, we aimed to develop suggestions for maximizing motivation to maintain sobriety. Finally, we hoped our results would provide direction for additional research on motivation in SLHs and other types of recovery homes. Study procedures were reviewed and approved by the Public Health Institute Institutional Review Board. Informed consent procedures were approved by the Public Health Institute Institutional Review Board. As the study data was limited to perceptions about motivation in sober living recovery homes and did not involve disclosure of individual level personal information from focus group participants, informed consent was limited to description of focus group procedures and verbal agreement to participate.
Analysis
Data of two 1-hour focus groups were audiotaped and transcribed. Two raters independently hand coded text for dominant themes within specific content areas queried during the interview. Content areas included questions addressing general factors motivating residents, peer influences, family influences, views about costs and benefits of sobriety as motivational influences, and views about our quantitative findings showing how motivation varied by social network and psychiatric severity characteristics. The two coders then discussed the themes each area generated and discrepancies were resolved through discussion. Dominant themes within each area were finalized and examples of relevant text were selected for inclusion in the study.
Methods
Participants
The current study used a mixed method design, drawing on previous quantitative research in recovery homes3,5,6 and new qualitative data from two focus groups to create a broader, more comprehensive view of motivation. The first focus group consisted of six individuals associated with a sober living organization in Northern California: the owner of the houses, a longtime administrative coordinator, and four current or recent house managers. All of the participants except the administrative coordinator were men and all were in recovery from alcohol and drug problems. In addition to being a site for collection of focus group data, these were the houses used to collect the prior quantitative data on motivation.3,5,6
The program consists of 16 recovery homes divided into a beginning phase for new residents and a more advanced phase for residents who have established some period of sobriety, typically a month or more. House sizes range from three to 12 bedrooms, the latter being a large phase I house where entering residents benefit from more containment (eg, rules such as curfews) and support from the larger community. The houses use a “social model” approach to recovery7–9 that emphasizes peer support as the essential ingredient in recovery. No onsite services are offered but residents are encouraged to pursue services they need in the community, and all are required to attend 12-step meetings. While living at the house, residents are expected to be involved in work, school, or other productive activities. Residents are expected to abstain from alcohol and drugs, required to attend house meetings, and involved in upkeep of the facility. Costs associated with the homes are primarily covered through resident fees, although some criminal justice programs will pay 1 month or 2 months of rent for ex-offenders upon entry into the SLH. Residents are free to live in the homes for as long as they like, but most use it as transitional living into independent living in the community. The average length of stay is slightly over 5 months (mean =166 days; standard deviation =163). An evaluation of resident outcomes showed significant improvement on measures of alcohol and drug use, severity of drug and alcohol problems, employment, and arrests. Improvements were evident between baseline and 6-month follow-up and continued at 18 months even though the vast majority had left the homes at that point.10 Consistent with the social model view of recovery, social network characteristics and the level of involvement in 12-step groups predicted outcome. More detailed information about SLHs is available in Polcin and Henderson11 or Wittman and Polcin.12
The second focus group consisted of six individuals associated with the sober living network in Southern California. The operations of these houses are generally similar to those studied in Northern California, although there is no phase system that residents transition through as time in the home increases. Sober living network is an advocacy network for SLHs that provides certification and training for approximately 500 homes in California. Participants included an administrator and five house managers, four men and one woman. The houses they operated ranged in size from six to 16 bedrooms.
Process and content of focus groups
Both focus groups were audiotaped in private locations onsite at the SLH organizations. Interviews took slightly >1 hour to complete and began with a general, open-ended question about factors felt to influence motivation to remain abstinent from alcohol and drugs. Specific follow-up questions included inquiries about the influence of peers, family, and friends on motivation. We then presented findings from our quantitative studies of motivation and asked participants to comment on them. Results presented to them included our findings that both costs and benefits predicted whether an individual used substances. We also presented the finding that two factors appeared to moderate the impact of benefits (ie, 12-step involvement and size of the social network). Finally, we asked participants to comment on our finding that persons with high psychiatric severity had worse substance abuse outcomes, and costs, but not benefits, were particularly strong predictors of those worse outcomes. Table 1 identifies the questions asked.
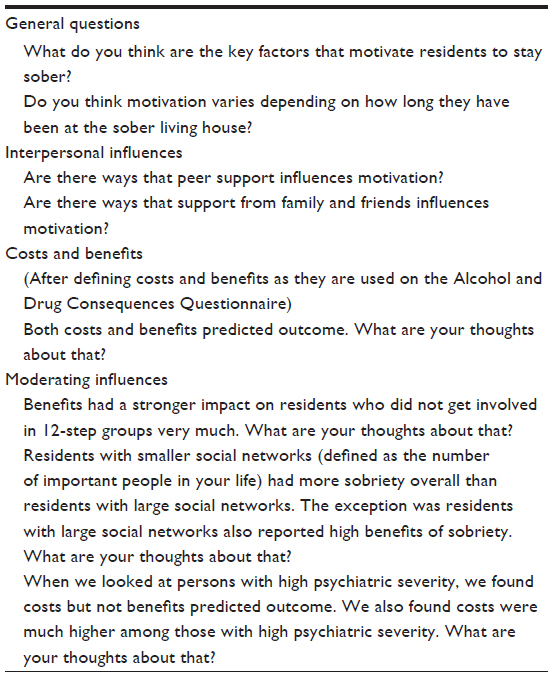 | Table 1 Focus group questions |
Results
Overall views about motivation
In response to the general question about motivation for maintaining sobriety, focus group participants emphasized many factors based on benefits and costs. For example, implementation of random and targeted urine screening, which could lead to eviction if positive for drug use, was viewed as an important motivator for keeping one’s sobriety. Many individuals enter the SLH with few if any other viable housing options. Participants also noted that costs related to substance use prior to entering the SLH were important motivators. Comments included, “I think one of the big motivators too is when most got here [they were] broken up. … ran into the ground”. “I’ve literally seen people come in here that look like they’re about two inches from dying”.
Consistent with studies of treatment entry for substance abuse problems,13 motivation to enter recovery homes was often viewed as a response to external pressure. Focus group participants pointed out there were significant costs for many residents if they did not take action to deal with their substance abuse. The consequences of inaction could include financial, legal, and interpersonal costs. One house manager stated, “I think the majority of people that come in their families, loved ones, employers, the courts are the motivator of them coming in here”. Several managers noted that financial pressures from families can increase motivation. This was particularly common for young persons who were still financially dependent on their parents.
… the fear of being homeless. And you know if we can get the parents to pull the cash away from them, then that becomes a very real fear and then you are motivated because it’s either there or the street.
Although family and other types of pressure were viewed as motivation to enter the recovery home, over time these sources of pressure came to be experienced as beneficial reasons to maintain abstinence. As residents rebuilt their lives over time, they often got their families back.
And so when most of the family are coming here they’re like dropping them off … We love you but we can’t watch you … if an individual makes it through at least the first sixty or ninety days [the] family starts coming back around and they become willing to help … they come to have dinner with them … even maybe come to a meeting. They become willing to come get them and take them out to eat or go to shopping or come home for the weekend.
Several house managers described motivation as a process where initially motivation was based on negative consequences associated with substance use, “deficit motivation”. However, for the resident to succeed over time, there needed to be a switch at some point to motivation that was based on the benefits of recovery.
Deficit motivation … the felonies and the evictions and the breakups … [When] the deficit motivation is gone … . see ya … But you’ve got to realize that you’ve got to get into a growth motivation so you start hearing about the benefits and a lot of the benefits are unactualized benefits. Because you have to work for them. They don’t just happen … you’re expected to do the work.
Examples of benefits included finding work, reengaging with one’s family, clearing up legal problems, and regaining a driver’s license. Several participants pointed out that achieving these goals typically required practical and emotional support from resident peers. One manager described a meeting labeled the “Been There, Done That” meeting. “We have the meetings where you can become of service and help people get to doctors, court appointments, I mean anything”. Another participant pointed out that the resident who developed that meeting received recognition in the household for his efforts, which furthered his commitment to the house as well as his individual recovery. Ways that residents supported one another resulted in a type of substitute family where persons could reside until they were able to begin reestablishing trust with their family.
Very few have family support that still want to engage when they first come in here and that’s what makes motivation too for someone to be here in this environment … this kind of becomes your replacement family but it gives you time to start mending with the family …
SLH social environment
The importance of the social environment within the SLH was emphasized as a motivator for sobriety in multiple ways. Peer support and experiences of comradery engaged residents in ways that would be difficult to replicate outside the SLH context. Over time, appreciation of the value of these experiences becomes a potent benefit of maintaining abstinence. One focus group participant stated:
… having instead of just a couple people they’ve got like this little town of peers here that are like-minded, that all have the same goal … we’ve got to leave our old places, people behind if we want to stay clean and sober. So if you have to do that you’ve got to have new people. And a sober living environment provides that.
Study participants felt residents were most likely to be receptive to feedback when it came from other residents rather than house managers. Within an interpersonal context of understanding and support, they were more motivated to address issues they needed to work on and acknowledge ways they were vulnerable to relapse. One participant stated, “They’re more apt to listen to their peers in regards to behavior or advice or criticism, whether it’s constructive you know whether it’s critical or just trying to be helpful”.
The SLH environment also created a context where residents could recognize vulnerability in others and take action to be helpful.
One of the things that I think is completely awesome is when somebody is having a bad day around here and you can kind of see … You kind of feel it, the aura … There [are] people that step up that ask you, hey, what’s going on?
One of the participants gave an example from her own recovery experience in a SLH. She described feeling upset and going for a walk. Suddenly, she was surrounded by her peers who stated they were going with her.
And part of me was like what the … Why are you going with me? What’s your problem? But the other part of me was like, wow, they’re showing they care for me … . And what they said was, you’re not okay. Everything on your face shows terror, anger and fear, and we just want to go with you … that’s what sober living is all about … I thought that things were okay that day but clearly I was not okay.
The care and concern experienced by this participant became an important motivator toward continuing sobriety. Experiences like this were felt to be examples of ways that mutual accountability was facilitated and supported sobriety within the household. Each individual in the household was accountable to other residents, not only in terms of their own behavior (eg, maintaining abstinence), but also in terms of contributing to a healthy recovery environment. The actions of the peers in the above case to reach out and help the resident who was upset and potentially vulnerable to relapse is an excellent example.
There were similar comments from other participants, including the contention that peers could often confront each other in ways that were experienced as helpful and supportive and resulted in increased motivation. One manager used the phrases “carefrontation” and “positive peer pressure”. “…you’ve got a group of guys around you trying to push you in a positive direction it can help motivate you to change your behavior …”
A final way that residents were thought to be motivated had to do with leadership of the house manager. One participant felt that the house manager “hopefully, is almost parentified. [Residents] want their approval … their validation”. Using residents’ motivation for approval, it was suggested that house managers make it a “goal to create a healthy family dynamic … How do we learn to communicate, express our feelings, have conflict resolution without getting loaded or punching a guy in the face?” Motivation based solely on compliance with external demands without learning these skills and without internal emotional work on oneself was felt to be short-lived.
Reflections on cost/benefit quantitative findings
In addition to general questions about motivation, we asked participants to comment on our quantitative findings.5 We presented to them the finding that perceived cost of sobriety was a robust predictor of substance use. We explained that when residents felt abstinence it would be difficult and would require them to tolerate high discomfort, they then tended to use substances more. This was particularly the case for persons with high psychiatric severity. We also noted that perceived benefits of abstinence were associated with sobriety overall, but benefits were particularly influential for persons who were less involved in 12-step meetings and persons who had a large number of persons in their social networks.
Reactions of focus group participants to our findings highlighted a number of points. Several participants thought perceived costs of sobriety were more prevalent in early recovery.
The costs I would say those are for somebody that is in very early recovery and hasn’t had some treatment … . hasn’t got any relief, emotional relief yet.
One participant noted that costs of abstinence subsided as one worked a recovery program and found new ways to manage the challenges of abstinence. “You’ve got to find a sufficient substitute”.
When we presented findings about ways the benefits operated differently for different groups (ie, interactions with 12-step involvement and size of one’s social network), participants mostly responded to the latter issue. The finding about differential effects of benefits for persons with high versus low 12-step involvement drifted into general discussions about how recovery through the 12-step program worked. There were also few reflections about why benefits would be more important for persons with larger social networks. However, there were interesting reflections about the overall finding that smaller social networks had better outcomes than large networks. Several participants felt that in early recovery, it was common to feel like you were friends with large numbers of fellow 12-step members. As recovery proceeded, many individuals become more discerning about their relationships and considered persons in their social network to be those they knew more intimately. As one participant put it, “find four people you can call at two in the morning and that’s more important than fifty people on speed dial”.
Reflections on psychiatric findings
We also asked participants to reflect on our finding that persons with more serious psychiatric problems had higher costs associated with sobriety and higher levels of substance use. One response was that standard SLHs were not a good option for some of these individuals. One participant in charge of overseeing a large group of houses pointed out that “some people with schizophrenia or mental health disorders do better in a small house that’s just like a six-bed house because of their psychosis and they’re paranoid they do much better with just a smaller group”. In addition, participants pointed out that persons with dual diagnosis needed a less demanding and more tolerant environment.
One manager described one of his facilities as primarily housing persons with dual diagnoses of psychiatric and substance use disorders. He felt many such residents were able to do well “if you can keep them medication compliant and you can get them introduced into co-occurring disorder groups”. He described the house as part of a “full service partnership”, where residents who were relapsing could readily be admitted to other types of housing without a sobriety requirement. However, his perception was that a significant number of dual diagnosed individuals preferred the modified SLH arrangement.
Discussion
Motivation has rarely been studied outside the context of formal treatment programs, and it has usually been studied in terms of desire to stop or cut down substance use. This study combined previously published quantitative data with new qualitative work to study motivation to maintain sobriety in SLHs. Unlike formal treatment, SLHs rely primarily on peer support rather than professionally delivered services as the primary therapeutic mechanism. The practice of social model recovery within the houses has important implications for understanding and enhancing motivation.
Motivation as a function of household relationships
In most studies, motivation is conceptualized as an individual’s desire to make changes, recognize problems, and take steps to address problems.14,15 Strategies to enhance motivation involve individual-based interventions such as motivational interviewing.16 A relatively novel but not unexpected finding in the current study was the conceptualization of motivation in terms of the SLH peer environment.
There are a number ways that peer dynamics within SLHs can facilitate motivation to maintain sobriety. Focus group participants felt there was often a level of understanding among peers that made it easy to recognize when a fellow resident was experiencing difficulty and was vulnerable to relapse. The typical response was to reach out to these individuals to find out what was wrong and be of assistance. Although residents sometimes initially rejected these overtures, they often came to experience them as supportive, as one manager put it, a type of “carefrontation”. Helping fellow residents was one way to receive acknowledgment and recognition that strengthened one’s commitment to the shared goal of abstinence.
Focus group participants also pointed out that residents were often able to consider feedback from their peers that they might reject if it came from others. It needs to be emphasized that the interactions they were referencing typically focused on potential harm to the resident, their areas of vulnerability, and were not personal attacks. Within the supportive environment of the SLH, residents were often able to acknowledge vulnerability and potential harm in ways that increased their commitment to abstinence and to the overall household. The emphasis on feedback about potential harm being experienced as supportive is consistent with previous research on supportive confrontation in SLHs.17–19 However, for individuals to feel supported by these interactions, it is important that the comments came from persons who are respected. They are particularly helpful when received from persons who have extensive recovery experience.18
Our study findings suggest that understanding motivation in SLHs requires a broader conceptualization. First, motivation exists at different levels, including individual, interpersonal, and household. One way to increase motivation is to facilitate self-reflection among individuals about reasons to maintain sobriety. However, residents of SLHs also enhance motivation in other ways, including ways they reach out to residents to help them avoid relapse. Initially, the resident may avoid relapse primarily as a response to external pressure. However, our focus group participants suggested that over time, and when coming from trusted peers, they may be more receptive to accepting the validity of potential harm. The care and concern from fellow residents becomes important reasons to stay sober, and relapse could result in the loss of valued personal relationships. The challenge to managers of SLHs and other types of recovery residences is facilitating an environment within the SLH where social interaction among peers facilitates motivation for recovery. Specific suggestions on ways to enhance social environments within SLHs are given in Polcin et al.8 Although motivation to change substance use has been discussed in terms of potential loss of intimate partners, friends, and family, it has typically not been examined in terms of desire to maintain relationships with peers in recovery.
Several house manager participants characterized life in a SLH as a family and that may be part of the reason household relationships can serve as important motivators. In terms of support for recovery, the SLH family can often provide more than actual families. Khantzian and Mack20 pointed out that fellow members of Alcoholics Anonymous often have a level of understanding about one another that creates the safety necessary to honestly discuss issues that otherwise might not be discussed at all, not even with intimate family members. The identification with other Alcoholics Anonymous members is a way persons in early recovery are able to regain the self-esteem necessary to move forward. This peer dynamic may be even more prevalent for recovering persons who live together in one household. The unique ways peers are able to give and receive support in SLHs appear to be important motivators to maintain sobriety.
View of costs and benefits
In addition to emphasizing the peer context of motivation, focus group participants emphasized the importance of a variety of well-established factors known to influence motivation. These included the important role of costs associated with substance use as motivation to seek help.4 In particular, they mentioned family pressures, legal problems, and periods of homelessness or the threat of homelessness. They also emphasized the important role of benefits associated with abstinence as a reason to continue sobriety. However, participants felt there were time-varying influences for some motivational factors. For example, they felt perceived costs of sobriety (ie, the challenges associated with not using) were more prominent early in recovery. Persons still using substances or those in early recovery were viewed as often not having confidence that they could manage without substances. In contrast, managers felt the benefits of sobriety were stronger influences at later time points. With the passing of time, residents in recovery regained important aspects of their lives that had been lost, particularly relationships with estranged family members. To date, there has been limited examination about the ebb and flow of motivation over time, particularly factors related to maintenance of sobriety.
Participants were not able to explain potential reasons for factors that moderated benefits (size of the social network and level of involvement in 12-step groups). However, there were general comments about how the size of one’s social network changed over time. They felt early in recovery a large number persons in 12-step recovery meetings were considered to be part of one’s social network. However, many persons felt differently over time. As the recovery process proceeded, they felt many persons were more discerning about whom they identified as a member of their social network. In general, it was felt to be more important to have strong relationships with a fewer number of persons than superficial connections with many.
When we presented our previous finding that persons with psychiatric disorders experienced higher costs associated with abstinence and those higher costs were associated with more substance use (ie, Polcin et al6), there was little surprise. Although persons with more psychiatric problems showed improvement on measures of alcohol and drug use, study group participants indicated that traditional SLHs might not be the best option for some of these individuals. Modifications were needed to reduce the level of stress and increase flexibility around relapse policies. One manager described a facility designed for these dual diagnosed persons that employed a “Housing Choice” model that offered a variety of housing options to individuals. Chronic homelessness occurring with substance abuse and mental illness further complicates housing choices. Although some of the dual diagnosed residents opt for housing funded by the Department of Housing and Urban Development that does not focus on abstinence, a significant number of residents desire a trial in a house with a focus on abstinence. A variety of housing providers targeting services for substance abuse, mental illness, and homelessness are debating which housing models best match individual needs. Waegemakers Schiff and Schiff21 provide a recent review of this literature.
Limitations
There are a number of limitations in our study. First, the data were limited to two focus groups in California and results might be different in other geographical areas. The N’s were small (N=6 for each group) and only included two women. Second, we only interviewed administrators and managers of the houses, not residents. However, most of the house managers who participated in the focus groups had at a previous time been residents themselves in sober houses and they were therefore able to draw upon their experiences as a resident as well as a manager when responding to focus group questions. Third, SLHs represent one type of residential setting and may not be generalizable to other recovery homes or residential treatment programs. Fourth, the focus group methods resulted in qualitative data that cannot be used to verify that the factors emphasized by participants caused increases in motivation. Fifth, we asked participants to comment on our findings about motivation that assessed motivation using the ADCQ. There are other measures of motivation that might have resulted in different findings. Finally, our questions asking participants to comment on the findings from our research on the ADCQ were difficult for some participants to understand.
Conclusion
Individuals who are intimately familiar with SLHs felt motivation to maintain sobriety among residents in their homes was influenced by factors known to affect motivation in formal treatment programs. These included the perceived costs and benefits associated with substance use and abstinence. However, motivation has typically been measured only at treatment entry and focus group participants felt the factors influencing motivation differed over time. Perceived costs were viewed to be more influential early in treatment and benefits were thought to be more influential as recovery time increased. More research is needed on the trajectories of costs and benefits across time for different populations of substance abusers.
Studies on motivation rarely identify peer relationships within service settings as important motivators to sustain recovery over time. However, focus group participants felt relationships within SLHs were potent motivators for continued sobriety. Fellow peers provided a level of understanding and support that to a large degree was viewed as uniquely supportive. Ways that residents reached out to fellow peers in distress were felt to facilitate motivation at individual and household levels. There is a serious need for research on the specific types of peer interactions that best facilitate motivation for different individuals. The content and intensity of peer interactions that are helpful might vary by resident characteristics (eg, age, sex, length of time in the residence, history of addiction and treatment, and severity of co-occurring problems). We also need information about destructive peer interactions that hinder motivation.
Housing service providers are struggling to identify housing models that best respond to the needs of specific subgroups, particularly persons with psychiatric disabilities and chronic homelessness who may not be motivated for abstinence. Focus group participants felt that standard SLHs may not be appropriate for some of these individuals and modifications were being made in SLHs designed to serve residents who presented serious psychiatric disorders in addition to substance abuse. There is a need for research on the effectiveness of different housing models for different populations and research that can inform placement of different residents across time. Housing choice should not be viewed as a single event for individual residents, but as an ongoing choice based on needs and motivation.
Acknowledgment
This research was supported by National Institute on Drug Abuse Grant R03 DA034961.
Disclosure
The authors report no conflicts of interest in this work.
References
Adamson SJ, Sellman JD, Frampton CMA. Patient predictors of alcohol treatment outcome: a systematic review. J Subst Abuse Treat. 2009;36: 75–86. | |
McKay JR, Weiss RV. Review of temporal effects and outcome predictors in substance abuse treatment studies with long-term follow-ups: preliminary results and methodological issues. Eval Rev. 2001;25: 113–161. | |
Korcha RA, Polcin DL, Bond JC, Lapp WM, Galloway G. Substance use and motivation: a longitudinal perspective. Am J Drug Alcohol Abuse. 2011;37:48–53. | |
Cunningham JA, Sobell LC, Gavin DR, Sobell MB, Breslin FC. Assessing motivation for change: preliminary development and evaluation of a scale measuring the costs and benefits of changing alcohol and drug use. Psychol Addict Behav. 1997;11:107–114. | |
Korcha R, Polcin DL, Bond J. Social Influences as Moderators of Motivation to Abstain from Alcohol and Drugs. Emeryville, CA: Alcohol Research Group [In press]. | |
Polcin DL, Korcha R, Bond J. Interaction of motivation and psychiatric symptoms on substance abuse outcomes in sober living houses. Subst Use Misuse. 2015;50:195–204. | |
Borkman TJ, Kaskutas LA, Room J, Bryan K, Barrows D. An historical and developmental analysis of social model programs. J Subst Abuse Treat. 1998;15:7–17. | |
Polcin DL, Mericle A, Howell J, Sheridan D, Christensen J. Maximizing social model principles in residential recovery settings. J Psychoactive Drugs. 2014;46:436–443. | |
Wright A. What is a social model? In: Shaw S, Borkman T, editors. Social Model Alcohol Recovery: An Environmental Approach. Burbank, CA: Bridge-Focus, Inc.; 1990:7–10. | |
Polcin DL, Korcha R, Bond J, Galloway G. What did we learn from our study on sober living houses and where do we go from here? J Psychoactive Drugs. 2010;42:425–433. | |
Polcin DL, Henderson DM. A clean and sober place to live: philosophy, structure, and purported therapeutic factors in sober living houses. J Psychoactive Drugs. 2008;40:153–159. | |
Wittman FD, Polcin DL. The evolution of peer run sober housing as a recovery resource for California communities. Int J Self Help Self Care. 2014;8:157–187. | |
Polcin DL, Korcha R, Greenfield TK, Bond J, Kerr W. Pressure to reduce drinking and reasons for seeking treatment. Contemp Drug Probl. 2012;39:687–714. | |
DiClemente CC, Hughes SO. Stages of change profiles in outpatient alcoholism treatment. J Subst Abuse. 1990;2:217–235. | |
Miller WR, Tonigan JS. Assessing drinkers’ motivation for change: the stages of change readiness and treatment eagerness (SOCRATES). Psychol Addict Behav. 1996;10:81–89. | |
Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. 2nd ed. New York, NY: Guilford Press; 2002. | |
Polcin DL, Greenfield TK. Confrontation about potential harm related to substance use: changes in and correlates of confrontation in sober living houses. Ther Communities. 2006;27:373–385. | |
Polcin DL, Mulia N, Jones L. Substance users’ perspectives on helpful and unhelpful confrontation: implications for recovery. J Psychoactive Drugs. 2012;44:144–152. | |
Polcin DL, Galloway GP, Bond J, Korcha R, Greenfield TK. How do residents of recovery houses experience confrontation between entry and 12-month follow-up? J Psychoactive Drugs. 2010;42:49–62. | |
Khantzian EJ, Mack JE. How AA works and why it’s important for clinicians to understand. J Subst Abuse Treat. 1994;11:77–92. | |
Waegemakers Schiff J, Schiff RA. Housing first: paradigm or program? J Soc Distress Homeless. 2014;23:80–104. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.