")
Back to Journals » Infection and Drug Resistance » Volume 15
More Than Three-Fourths of AstraZeneca (ChAdox1 COV-19) COVID-19 Vaccinated Individuals Develop Post Immunization Adverse Event in Northwest Ethiopia
Authors Muluneh AG , Merid MW, Gelaye KA , Tilahun SY, Teshager NW, Abereha AY, Sugamo KS, Yimer MA , Kassa GM
Received 30 January 2022
Accepted for publication 21 April 2022
Published 3 May 2022 Volume 2022:15 Pages 2409—2416
DOI https://doi.org/10.2147/IDR.S360605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Atalay Goshu Muluneh,1 Mehari Woldemariam Merid,1 Kassahun Alemu Gelaye,1 Sewbesew Yitayih Tilahun,2 Nahom Worku Teshager,3 Aklilu Yiheyis Abereha,4 Kalkidan Samuel Sugamo,5 Mulugeta Ayalew Yimer,3 Getahun Molla Kassa1
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Psychiatry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Pediatrics and Child health, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Surgery, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 5Department of Internal medicine, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Atalay Goshu Muluneh, Email [email protected]
Background: Ethiopia was using the ChAdOx1 COV-19 vaccine, and health professionals were targets of the first phase of the vaccination strategy. Evidence on the adverse events following immunization (AEFI) was barely available. The study aimed to assess the magnitude and associated factors of adverse events following ChAdOx1 COV-19 immunization among health professionals of the University of Gondar Specialized and Comprehensive Hospital, 2021.
Methods: An institution-based cross-sectional study was conducted among health professionals of the University of Gondar Comprehensive and specialized referral hospital. All health professionals who took the ChAdOx1 COV-19 vaccine in the 1st phase were surveyed. A total of 314 health professionals who took the ChAdOx1 COV-19 vaccine were included. The EpiData version 4.6.0.0 and Stata 16 were used for data entry and analysis, respectively. A binary logistic regression was used to identify statistically significant factors associated with AEFI. Chi-square and multicollinearity assumptions were tested. A p-value < 0.2 and 0.05 were used as cut-off values of significance in the bi- and multivariable logistic regression models, respectively. An adjusted odds ratio (AOR) with 95% CI was reported for statistically significant variables.
Results: Among 314 study participants, 263 of them had at least one mild to severe AEFI of ChAdOx1 COV-19 with a prevalence of AEFI of 83.76% (95% CI: 79.23, 87.46). The commonest AEFI observed were injection site tenderness (n=198/263), fatigue (114/263), headache (n=107/263), and muscle pain (n=85/263). Females (AOR=2.75, 95% CI: 1.15, 6.58), and participants who felt the vaccine was unsafe (AOR=2.84, 95% CI: 1.03, 7.85) were having nearly three times more odds of AEFI immunization as compared to males and those who felt the vaccine was safe, respectively.
Conclusion: Adverse event following immunization has been a public health problem in Northwest Ethiopia. Being female and having a feeling that the vaccine is unsafe were statistically significantly associated with AEFI.
Keywords: adverse event, ChAdOx1 COV-19, associated factors, Ethiopia
Background
COVID-19 pandemic remains a global public health threat claiming more than two hundred million cases and 4.7 million deaths until September 19, 2021.1,2 Ethiopia has reported more than three hundred thousand cases, and five thousand deaths.1 The World Health Organization and other local health authorities have design different mitigation strategies such as vaccines, and other non-medical interventions to combat spread of the disease. Still, risk perception and behavioral responses are different among different regions.3–16 Different types of vaccines have been distributed to different continents including Africa, but the utilization rate has remained low as compared to different targets set by the World Health Organization and regional health institutes.17–20 Countries in Africa including Ethiopia have the lowest vaccinated population in the world.20 Concerns related to vaccine safety and efficacy, the difficulty of accessing the vulnerable populations,21 wars, and conflicts, the use of different vaccines, and other access-related constraints are the major concerns of very low vaccine rollout in Africa.20 Other articles also claimed that vaccine hesitancy, distributed misinformation, religious fanaticism, attitude and uptake of vaccine among health care workers, social influences, and environments wherein people looking for trusted icons response and involvement are major obstacles of COVID-19 vaccine roll out to achieve the target.22 According to the vaccine’s safety profile within the product information, the most common side effects include mild-to-moderate symptoms of one or more of the following: headache (52.6%), fatigue (53.1%), muscle or joint pain (44%), fever (33.6%), chills (31.9%), and nausea (21.9%).23,24 Additionally, symptoms of an allergic reaction including hives, a rash, swelling, and respiratory issues may occur.25
Recent evidence noted that people who have not received a COVID-19 vaccine were faced 10, and 11 times higher risk of hospitalization and death due to COVID-19 than those who have undergone vaccination, respectively.23 Getting vaccinated protects against severe illness and mortality from COVID-19, including the Delta variant. Monitoring COVID-19 incidence by vaccination status might provide early signals of changes in vaccine-related protection that can be confirmed through a well-controlled vaccine effectiveness (VE) study.24 Some of the side effects associated with the use of the COVID-19 vaccine are reported in different countries as mentioned above. However, there is still controversy and evidence gap regarding the magnitude and extent of the adverse events associated with the COVID-19 vaccine. As a result, countries are facing challenges in expanding the uptake of the vaccine among citizens. Therefore, this study aimed to assess the common post-COVID-19 vaccine (AstraZeneca) immunization adverse events among the health care workers at the university of Gondar Comprehensive Specialized Hospital.
Methods
Study Design and Period
An institution-based cross-sectional study was conducted from June 1, 2021, to August 21, 2021.
Study Setting
This study was undertaken at the University of Gondar Comprehensive Specialized Hospital which is found in the Central Gondar Zone of the Amhara region, Ethiopia. It serves more than 7 million people and is one of the COVID-19 diagnosis and treatment centers in the country. It is also one of the major sites of COVID-19 vaccine delivery for the targeted population, ie health professionals and medical intern doctors.
Study Population
The study population included all health professionals (medical doctors, medical intern doctors, nurses, pharmacists, psychiatrists, midwives, and others) who took at least 1st dose of the ChAdOx1COV-19 vaccine.
Sample Size and Sampling Technique
We surveyed all health professionals who took the ChAdOx1COV-19 vaccine in the first round.
Inclusion and Exclusion Criteria
All health professionals who took at least the first dose of ChAdox1 COV-19 were included while those health professionals on monthly leave were excluded.
Data Collection and Quality Control
Data was collected using a semi-structured self-administered questionnaire (Supplementary Table 4). Data completeness and consistency were checked daily by one general practitioner and three specialist medical doctors. The data was entered using EpiData 4.6.0.0 software and exported to Stata 16 for further cleaning and analysis.
Variables and Measurement
The dependent variable was adverse event following immunization as subjectively reported by the health professionals, ie, if they report at least one of these symptoms following immunization: injection site tenderness, redness or swelling, systemic reaction, seizure, abscess, high-grade fever, anaphylaxis, bleeding, thrombocytopenia, fatigue, chills, joint pain, muscle pain, headache, malaise, flu-like symptom, vomiting, and/or nausea. Independent variables were age, educational status, religion, gender, specialty, comorbidity, number of doses of the vaccine, previous history of COVID-19 infection, and feeling about the vaccine.
Data Analysis
Data was analyzed using Stata 16 software. Descriptive findings were reported using proportions, frequencies, and medians. Binary logistic regression was fitted to identify statistically significant factors. Chi-square and multicollinearity assumptions were tested. A P-values less than 0.2 and 0.05 were used as a cut-off value for statistical significance for bi and multivariable logistic regression, respectively. Finally, the Adjusted Odds Ratio (AOR) with 95% CI was reported in the final model.
Results
Socio-Demographic Characteristics
Of the total 335 self-administered questionnaires, we excluded 21 questionnaires (four were incomplete, and 17 respondents’ vaccination status was missed). All the data obtained from the 314 participants were included in the final analysis. Of which 71.34% were males and the median age was 25 (inter-quartile range [IQR]: 23, 28) years. About 76.75% were Orthodox Christians and, 56.05% were interning medical doctors while others were health professionals. More than half of the participants reported that they felt the vaccine is safe (54.48%) (Supplementary Table 1).
Adverse Events Following Immunization (AEFI) ChAdOx1 COV-19 Vaccinations
The overall prevalence of AEFI was 83.76% (95% CI: 79.23, 87.46 (n=263/314)). The commonest AEFI observed were injection site tenderness (n=198/263), fatigue (n=114/263), headache (n=107/263), and muscle pain (n=85/263). There were no seizures, injection site abscesses, shock, or bleeding disorders following the immunization (Figure 1).
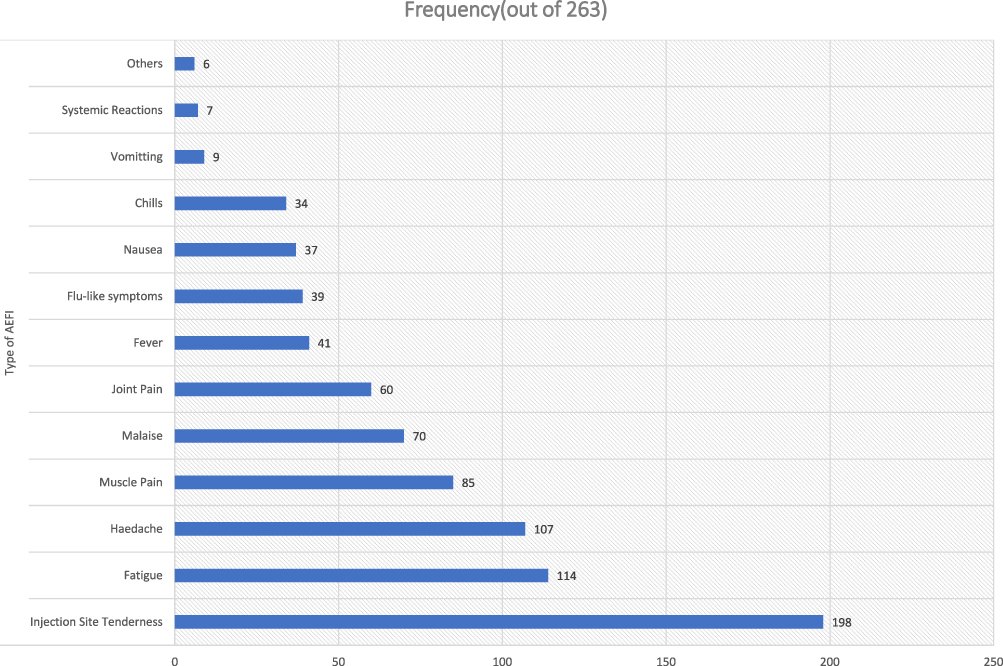 |
Figure 1 Type and frequency of adverse events developed following ChAdOx1 COVID-19 immunization among medical and health care professionals in University of Gondar (n=263). |
The majority of the AEFI was developed in the first (n=191/232, 82.33%) and second (n=31/232, 13.36%) days of immunization. The minimum and maximum days of symptom resolution were 1 and 22 days after the onset. Nearly ninety percent of the AEFI resolved within three days (Figure 2A and B).
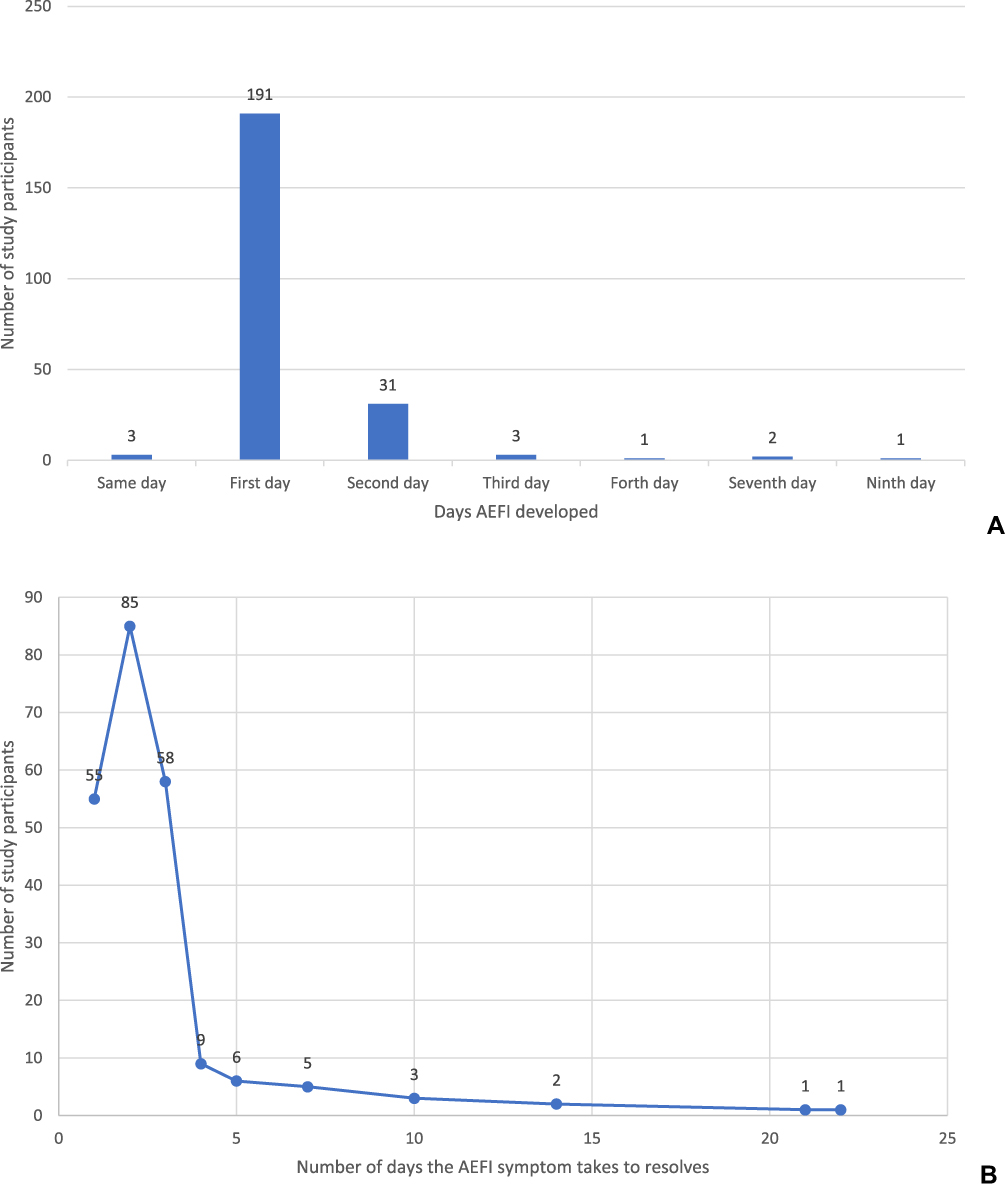 |
Figure 2 (A) Number of days the study participants developed AEFI and (B) number of days the AEFI symptom takes to resolve. |
Ninety percent (90%, n=235/261), 4.98% (n=13/261), and 4.98% (n=13/261) of all the AEFIs were reported after the first, second, and both doses of the vaccine, respectively. Out of 263 respondents who experienced AEFI 257 scaled the severity of symptoms as follows: mild (n=162/257, 63.04%), moderate (n=73/257, 28.40%), severe (20/257, 7.78%), and difficult to scale (n=2/257, 0.78%). Most of the respondents with AEFI (51.70%) took paracetamol for symptom relief. Other drugs taken were diclofenac (12.50%) and Ibuprofen (5.68%). Above a quarter (28.98%) of those respondents with AEFI reported that they have taken an unspecified drug to relieve the symptoms. Two-thirds of those respondents with AEFI (66.40%) recovered without intervention and one-third (31.60%) recovered with minor intervention. There were four admissions following adverse events, of which three recovered without sequelae, and one developed sequelae.
History of Drug, Food, or Other Reactions and COVID-19 Infection
All participants who were tested positive for COVID-19 had AEFI symptoms. Of those with current AEFI, 3.10% (8/258) had a history of past vaccine-related AEFI for meningitis A, hepatitis B, swine-flu vaccine, and tetanus vaccines). Of those 259 respondents who had had previous COVID-19 test results, 21 (8.11%) had a history of positive results (Supplementary Table 2).
Binary Logistic Regression to Identify Factors Associated with AEFI Development
From the descriptive statistics participants’ sex, religion, highest educational status, number of vaccine doses taken, and feeling towards the vaccine safety satisfied the chi-squared assumption. Bivariable and multivariable binary logistic regression models were fitted in the multivariable regression we found participants’ sex and feelings towards the safety of the vaccine positively associated with the development of AEFI at a p. value of less than 0.05. Females had three times higher odds of AEFI than males had (AOR: 2.75, 95% CI: 1.15, 6.58), and those participants who felt the vaccine is not safe had approximately three times (AOR: 2.84, 95% CI: 1.03, 7.85) higher odds of AEFI when compared to those who felt the vaccine is safe (Supplementary Table 3).
Discussion
This study aimed to measure the magnitude and associated factors of adverse events following ChAdOx1 immunization among health professionals working at the University of Gondar. We found that more than three-fourths of the study participants had mild to severe adverse events following immunization. This finding is comparable with other studies conducted in Nepal, and Korea26 where 79.8%, and 81% of health professionals had an adverse event following immunizations, respectively, but higher than studies on Indian health professionals where 57% of the health professionals had adverse events.27,28 It is also higher than findings reported from Saudi Arabia where two-thirds of the study participants reported at least one AEFI.29 Similarly, it was higher than the findings of the studies conducted in the United Kingdom where 58.7% of the study population who took the 1st dose of the ChAdOx1 vaccine developed local symptoms,30 and the one conducted in Togo.31 This might be justified by the variations in study population, for the Saudi Arabia, and United Kingdom studies were on the general public that may not report mild symptoms while ours was on health professionals that can report every simple adverse event. While the communities/general public may not report mild symptoms.
On the other side, the magnitude of AEFI was lower than web-based study findings from Korea where more than 90% of the health professionals reported at least one AEFI.32 This might be due to variations of outcome ascertainment techniques. Accordingly, the Korean study was a mobile-based daily report from the participants while we collected the data from the respondents a week after they took the vaccine, which may lead to missing mild symptoms. This might have caused underestimation of the AEFI in our study compared to daily reports of the symptoms in the Saudi Arabian study. It was also lower than the other study’s findings in Saudi Arabia, where more than 95% of the participants had at least one AEFI symptom.33
The majority of the adverse events were reported within the first 48 hours. This is comparable with reports findings of a study on Indian health professionals where more than three-fourths of the adverse events were reported within the first 48 hrs.27
The commonly reported adverse events were injection site tenderness, and fatigue as compared to others. This is supported by another study conducted in Korea where the pain, injection site tenderness, and fatigue were the top adverse events of health professionals experienced.32 It is also supported by findings of other studies on health professionals from Togo,31 and Nepal.34 Compared to other brands of COVID-19 vaccines, ChAdOx1 had a lower AEFI than Moderna (94%) but higher AEFI than Pfizer vaccine (53%). Nevertheless, higher number of patients who took ChAdOx1 developed series AEFI compared to patients who took Moderna and Pfizer vaccine.35 Another study finding indicate that among all immunized individuals more than half (58.1%) of the AEFI, and nearly half (49.5%) of severe adverse events were reported following ChAdOx1 vaccination compared to Moderna and Pfizer vaccines.36
Those who felt the vaccine was unsafe had nearly three times higher odds of AEFI as compared to those who felt the vaccine is safe. Unfortunately, we failed to find comparable pieces of evidence that incorporate the participants’ feelings about vaccine safety. Still, one study reported the association between vaccine perception and adverse events by stating those participants who think the vaccines are useless and with side effects have more chances of developing adverse events.37 Another study reported that students who had fear of side effects reported seven times higher AEFI as compared to those who did not fear the vaccine.38 This might be justified by those individuals who feel the vaccine is unsafe might be very suspicious and report and remember every mild symptom after vaccination.
Female health professionals had more than double the odds of AEFI as compared to male health professionals. This is in line with study findings reported from India where females had two times more odds of AEFI as compared with males.28 Similarly, our finding was comparable with findings from the Vietnamese study where female participants reported more AEFI.39 Another study’s finding from Israel also supported this evidence by stating that females had nearly double risks of developing adverse events following 1st and 2nd dose of Pfizer-BioNTech COVID-19 vaccine as compared to males.40 This may give clues for health professionals to give more attention to female vaccinees, and researchers to conduct further investigation on gender differences in terms of adverse events.
Strength and Limitation of the Study
We are confident that our study was strong enough to conclude but subjective measurements based on participants’ reports were used for outcome ascertainment that may bias some specific adverse events.
Conclusion
More than three-fourths of the health professionals taking the ChAdOx1 COVID-19 vaccine developed minor to severe adverse events following immunization. Of these, nearly one-third of symptomatic participants recovered intervention such as antipain but nearly a tenth of them had severe symptoms. Being female and having a feeling that the vaccine is unsafe were statistically significantly associated with AEFI.
Abbreviations
AEFI, adverse event following immunization; AOR, adjusted odds ratio.
Data Sharing Statement
The data used for the preparation of this manuscript can be available from the corresponding author with formal request.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Ethical Review Committee of the University of Gondar. A permission letter was sought from the University of Gondar Hospital’s chief executive director. The purpose, the risks and benefits of the study were explained, and written informed consent was taken from all study participants. Anonymity was maintained throughout the whole process. All activities were conducted based on the declaration of Helsinki ethical guidelines.
Acknowledgments
The authors acknowledge the Institute of Public Health and the School of Medicine, College of Medicine and Health Sciences, University of Gondar. Our thanks also extend to study participants and data collectors.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. INSA. Ethiopia Covid-19 monitoring platform; 2020 Available from: https://www.covid19.et/covid-19/.
2. COVID-19 Coronavirus Pandemic; 2020. Available from: https://www.worldometers.info/coronavirus/.
3. Adalja AA, Toner E, Inglesby TV. Priorities for the US health community responding to COVID-19. JAMA. 2020;323:1343. doi:10.1001/jama.2020.3413
4. Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. 2020;395(10228):931–934. doi:10.1016/S0140-6736(20)30567-5
5. Atchison CJ, Bowman L, Vrinten C, et al. Perceptions and behavioural responses of the general public during the COVID-19 pandemic: a cross-sectional survey of UK adults. medRxiv. 2020. doi:10.1136/bmjopen-2020-043577
6. Betsch C, Wieler L, Bosnjak M, et al. Germany COVID-19 Snapshot MOnitoring (COSMO Germany): monitoring knowledge, risk perceptions, preventive behaviours, and public trust in the current coronavirus outbreak in Germany. 2020.
7. De La Vega R, Barquín RR, Boros S, Szabo A. Could attitudes toward COVID-19 in Spain render men more vulnerable than women? Global Public Health. 2020;15:1278–1291. doi:10.1080/17441692.2020.1791212
8. Deng SQ, Peng HJ. Characteristics of and public health responses to the coronavirus disease 2019 outbreak in China. J Clin Med. 2020;9(2):575. doi:10.3390/jcm9020575
9. Huynh TLD. The COVID-19 risk perception: a survey on socioeconomics and media attention. Econom Bull. 2020;40(1):758–764.
10. Khosravi M. Perceived risk of COVID-19 pandemic: the role of public worry and trust. Electron J Gen Med. 2020;17(4):em203. doi:10.29333/ejgm/7856
11. Kwok KO, Li KK, Chan HH, et al. Community responses during the early phase of the COVID-19 epidemic in Hong Kong: risk perception, information exposure and preventive measures. medRxiv. 2020. doi:10.1101/2020.02.26.20028217
12. Lohiniva A-L, Sane J, Sibenberg K, Puumalainen T, Salminen M. Understanding coronavirus disease (COVID-19) risk perceptions among the public to enhance risk communication efforts: a practical approach for outbreaks, Finland, February 2020. Eurosurveillance. 2020;25(13):2000317. doi:10.2807/1560-7917.ES.2020.25.13.2000317
13. Qian M, Wu Q, Wu P, et al. Psychological responses, behavioral changes and public perceptions during the early phase of the COVID-19 outbreak in China: a population based cross-sectional survey. medRxiv. 2020. doi:10.1101/2020.05.05.20091553
14. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A Nationwide Survey of Psychological Distress Among Chinese People in the COVID-19 Epidemic: Implications and Policy Recommendations. BMJ Publishing Group Ltd; 2020.
15. Wise T, Zbozinek TD, Michelini G, Hagan CC. Changes in risk perception and protective behavior during the first week of the COVID-19 pandemic in the United States. 2020.
16. World Health Organization. Coronavirus disease 2019 (COVID-19) situation report – 59. 2020.
17. Tagoe ET, Sheikh N, Morton A, et al. COVID-19 vaccination in lower-middle income countries: national stakeholder views on challenges, barriers, and potential solutions. Front Public Health. 2021;9:709127. doi:10.3389/fpubh.2021.709127
18. Sharma P, Pardeshi G. Rollout of COVID-19 vaccination in India: a SWOT analysis. Disaster Med Public Health Prep. 2021;2021:1–4.
19. Sarkar SK, Morshed MM. Spatial priority for COVID-19 vaccine rollout against limited supply. Heliyon. 2021;7(11):e08419. doi:10.1016/j.heliyon.2021.e08419
20. Ayenigbara IO, Adegboro JS, Ayenigbara GO, Adeleke OR, Olofintuyi OO. The challenges to a successful COVID-19 vaccination programme in Africa. Germs. 2021;11(3):427–440. doi:10.18683/germs.2021.1280
21. Braganza BB, Capulong HG, Gopez JM, Gozum IE, Galang JR. Prioritizing the marginalized in the COVID-19 vaccine rollout. J Public Health. 2021;43(2):e368–e9. doi:10.1093/pubmed/fdab083
22. Wirsiy FS, Nkfusai CN, Ako-Arrey DE, Dongmo EK, Manjong FT, Cumber SN. Acceptability of COVID-19 vaccine in Africa. Int J MCH AIDS. 2021;10(1):134–138. doi:10.21106/ijma.482
23. Scobie HM, Johnson AG, Suthar AB, et al.Monitoring incidence of COVID-19 cases, hospitalizations, and deaths, by vaccination status—13 US Jurisdictions, April 4–July 17, 2021. Morbid Mortal Wkly Rep. 2021;70:1284.
24. Skelly DT, Gilbert-Jaramillo J, Knight ML. Two doses of SARS-CoV-2 vaccination induce more robust immune responses to emerging SARS-CoV-2 variants of concern than does natural infection. 2021.
25. Agency EM. COVID-19 Vaccine AstraZeneca: PRAC investigating cases of thromboembolic events - vaccine’s benefits currently still outweigh risks - update. 2021.
26. Song JE, Oh GB, Park HK, Lee SS, Kwak YG. Survey of adverse events after the first dose of the ChAdOx1 nCoV-19 vaccine: a single-center experience in Korea. Infect Chemother. 2021;53(3):557–561. doi:10.3947/ic.2021.0044
27. Kamal D, Thakur V, Nath N, Malhotra T, Gupta A, Batlish R. Adverse events following ChAdOx1 nCoV-19 vaccine (COVISHIELD) amongst health care workers: a prospective observational study. Med J. 2021;77:S283–s8. doi:10.1016/j.mjafi.2021.06.014
28. Kaur U, Ojha B, Pathak BK, et al. A prospective observational safety study on ChAdOx1 nCoV-19 Corona virus vaccine (recombinant) use in healthcare workers- first results from India. EClinicalMedicine. 2021;38:101038. doi:10.1016/j.eclinm.2021.101038
29. Adam M, Gameraddin M, Alelyani M, et al. Evaluation of post-vaccination symptoms of two common COVID-19 vaccines used in Abha, Aseer Region, Kingdom of Saudi Arabia. Patient Prefer Adherence. 2021;15:1963–1970. doi:10.2147/PPA.S330689
30. Menni C, Klaser K, May A, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. Lancet Infect Dis. 2021;21(7):939–949. doi:10.1016/S1473-3099(21)00224-3
31. Konu YR, Gbeasor-Komlanvi FA, Yerima M, et al. Prevalence of severe adverse events among health professionals after receiving the first dose of the ChAdOx1 nCoV-19 coronavirus vaccine (Covishield) in Togo, March 2021. Archiv Public Health. 2021;79(1):207. doi:10.1186/s13690-021-00741-x
32. Jeon M, Kim J, Oh CE, Lee JY. Adverse events following immunization associated with the first and second doses of the ChAdOx1 nCoV-19 vaccine among healthcare workers in Korea. Vaccines. 2021;9(10):1096. doi:10.3390/vaccines9101096
33. Abu-Hammad O, Alduraidi H, Abu-Hammad S, et al. Side effects reported by Jordanian healthcare workers who received COVID-19 vaccines. Vaccines. 2021;9(6):577. doi:10.3390/vaccines9060577
34. Subedi P, Yadav GK, Paudel B, Regmi A, Pyakurel P. Adverse events following the first dose of Covishield (ChAdOx1 nCoV-19) vaccination among health workers in selected districts of central and western Nepal: a cross-sectional study. PLoS One. 2021;16(12):e0260638. doi:10.1371/journal.pone.0260638
35. Kant A, Jansen J, van Balveren L, van Hunsel F. Description of frequencies of reported adverse events following immunization among four different COVID-19 vaccine brands. Drug Safety. 2022;45:1–13. doi:10.1007/s40264-021-01134-3
36. Tobaiqy M, MacLure K, Elkout H, Stewart D. Thrombotic adverse events reported for moderna, Pfizer and Oxford-AstraZeneca COVID-19 vaccines: comparison of occurrence and clinical outcomes in the EudraVigilance database. Vaccines. 2021;9(11):1326.
37. Santangelo OE, Provenzano S, Grigis D, Migliore CB, Firenze A. Adverse events following immunization and vaccine perception in nursing students. Annali di igiene. 2021;33(2):123–130. doi:10.7416/ai.2021.2418
38. Provenzano S, Santangelo OE, Lanza GLM, Raia DD, Alagna E, Firenze A. Factors associated with reporting adverse reactions after immunization, study in a sample of university students. Annali di igiene. 2018;30(5):436–442. doi:10.7416/ai.2018.2244
39. Tran VN, Nguyen HA, Le TTA, Truong TT, Nguyen PT, Nguyen TTH. Factors influencing adverse events following immunization with AZD1222 in Vietnamese adults during first half of 2021. Vaccine. 2021;39(44):6485–6491. doi:10.1016/j.vaccine.2021.09.060
40. Green MS, Peer V, Magid A, Hagani N, Anis E, Nitzan D. Gender differences in adverse events following the Pfizer-BioNTech COVID-19 vaccine. Vaccines. 2022;10(2):233. doi:10.3390/vaccines10020233
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.