")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Mono-Lateral External Fixation for Treatment of Femoral Osteomyelitis
Authors Mohd Yusof N, Saleh AK , Abuomira IEAA, Attallah AA , Elshal EA, khames AAA
Received 26 July 2022
Accepted for publication 21 October 2022
Published 22 November 2022 Volume 2022:14 Pages 437—443
DOI https://doi.org/10.2147/ORR.S383863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Nazri Mohd Yusof,1 Ayman K Saleh,2,3 Ibrahim Elsayed Abdellatif A Abuomira,4 Abdehamid A Attallah,2 Ehab Abdelftah Elshal,4 Amr abdelhalem Amr khames4
1Advanced Trauma and Limb Reconstructive Surgery Department, International Islamic University of Malaysia, Gombak, Malaysia; 2Department of Orthopedic Surgery, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 3Department of Surgery, College of Medicine, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia; 4Department of Orthopaedic surgery, Al-Azhar University, Assiut, Egypt
Correspondence: Ayman K Saleh, Email [email protected]
Background and Aim: Maintenance of stability using external fixation devices is an important principle to ensure successful treatment of osteomyelitis (OM). In this study, we report our experience with femoral OM treated with acute compression and bone transport using the Orthofix limb reconstruction system (LRS).
Patients and Methods: This prospective study included 30 consecutive patients with femoral OM. LRS insertion and corticotomy were done according to the standard technique. Radiographic evaluation was performed every 2 weeks during the distraction phase and every 2– 4 weeks during the consolidation phase. The clinical outcome measurements included union time, limb length discrepancy, additional operative procedures, refracture and infection.
Results: The present study included 30 patients with femoral OM. They comprised 27 males (90.0%) and 3 females (10.0%) with an age of 28.1 ± 15.6 years. All, except one, achieved union with a mean union time of 8.6 months (range 4– 20 months). The mean union time for acute compression was 7.6 months (range 4– 20 months) while for patients with bone transport it was 14.5 months (range 12– 18 months). The mean limb length discrepancy was 1.8 cm (range 0– 4 cm). At the end of the follow=up, two patients were not able to ambulate without support; one due to non-union and one due to paraplegia.
Conclusion: The present study identified treatment of femoral OM using LRS as a feasible and effective technique with good outcomes. Reported complications could be adequately managed in most cases.
Keywords: osteomyelitis, external fixation, limb reconstruction system
Introduction
Chronic osteomyelitis (OM) is one of the most challenging conditions in orthopedic practise.1 OM is mostly caused by Staphylococcus aureus. Recent researches achieved significant progress in understanding the pathophysiology of OM. Studies have shed light on the role of osteocytes in the employment of immune cells and the mechanisms of microbial invasion and persistence in the cortical bone.2 The role of Staphylococcus aureus in orthopedic implant-associated infections was also demonstrated.3
Fundamental principles for successful OM treatment entail surgical debridement, administration of specific antibiotics, obliteration of dead space and maintenance of stability using external fixation devices.4
Applying external fixation to the femur is difficult because of the surrounding muscles and the proximity with the opposite limb. Lateral fixation offers the best solution because it is safe and more comfortable for patients.5 However, traditional fixation is not strong enough to overcome the strong deforming force of the adductor muscles which may lead to varus deformity. Although ring fixation provides a stable fixation of bone, it is bulky and uncomfortable for patients.6
The modern mono-lateral external fixation systems provide better stability by having a larger screw diameter with conical hydroxyapatite coated thread fixed in a rigid clamp that is connected to the rail. It allows compression at the fracture site and bone transport.5
In this study, we report our experience with femoral OM treated with acute compression and bone transport using the Orthofix limb reconstruction system (LRS).
Patients and Methods
This prospective cohort study was conducted at the Advanced Trauma and Limb Reconstruction Unit, Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia from 2010 till 2014. The local ethical committee approved the study protocol and all patients or their legal guardians, if they were younger than 18 years old, provided informed consent before enrolment, in accordance with the Helsinki Declaration on clinical research involving human subjects.
The study included 30 consecutive patients with femoral OM. Infection was diagnosed on the basis of history and physical examination. Infection was confirmed during operation with evidence of pus or a positive culture from bacteriological tests. Patients were excluded if they had other active systemic infections or immunocompromised states.
Antibiotic Protocol
Intraoperative specimens were sent for bacteriological studies and antibiotics were given on the basis of culture and sensitivity. Antibiotics were given intravenously for 2 weeks followed by oral form for 4 weeks. Tobramycin pellets 4.0% (Wright Medical Technology, Inc, Arlington, TN 38002 USA) were used in 14 cases and custom-made gentamycin beads (40 g of cement powder mixed with 2 g of vancomycin and made into beads connected to each other by suture) in one case. One patient whose culture grew Burkholderia pseudomallei received antibiotics for 6 months.
LRS Insertion
LRS insertion and corticotomy were done according to the technique described by Nayagam.7 Corticotomy and bone transport were done after infection had been controlled. Bone transport was started after a 1 week period of latency. Transport was done at the rate of a quarter turn four times per day. Bone grafting was done when docking of the transported segment had been achieved. Distraction is continued until an equal length to the contra-lateral femur was achieved. Antibiotics were only used during the perioperative period. Physiotherapy was started as soon as the patient could tolerate it, usually on the second post-operative day. Patients were encouraged to undergo partial weight bearing during treatment to prevent disuse osteoporosis and stimulate bone healing (Figure 1).
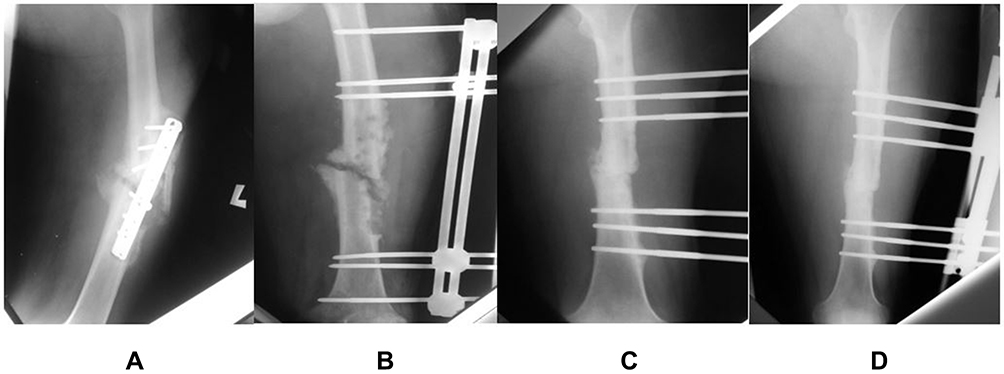 |
Figure 1 (A) X-ray showing osteomyelitis at presentation. (B) After removal of plate and insertion of standard monoliteral external fixator. (C) Resection of both fracture ends followed by acute compression using LRS fixation. (D) Fracture uniting after 5 months of treatment with LRS. |
Postoperative Evaluation
Radiographic evaluation was performed every 2 weeks during the distraction phase and every 2–4 weeks during the consolidation phase. Consolidation was diagnosed radiographically with ossification of at least three cortices and clinically when there is no pain on full weight bearing with a loosened frame. To avoid re-fracture from premature removal of the frame, the frame was dynamized first by removing the screw that fixes the proximal clamp to the rail. Then, patients were allowed to fully weight bear without support for six weeks before removing the whole frame.
Surgical Outcome
The clinical outcome measurements included union time, limb length discrepancy, additional operative procedures, refracture and infection.
Results
The present study included 30 patients with femoral OM. They comprised 27 males (90.0%) and 3 females (10.0%) with an age of 28.1 ± 15.6 years. OM was caused by hematogenous infection in 6 patients (20.0%) while it developed post-traumatically in 24 patients (80.0%). Infection was located at the proximal third in 1 patient (3.3%), at the midshaft in 25 patients (83.3%) and at the distal third in 4 patients (13.3%). Other baseline data are shown in Table 1. In patients with a pathological fracture due to haematogenous osteomyelitis, wound debridement and skeletal traction were done first and Orthofix LRS was inserted after 3 weeks of intravenous antibiotics. In patients with post-traumatic OM, LRS was inserted on the same surgery with debridement and removal of the implant.
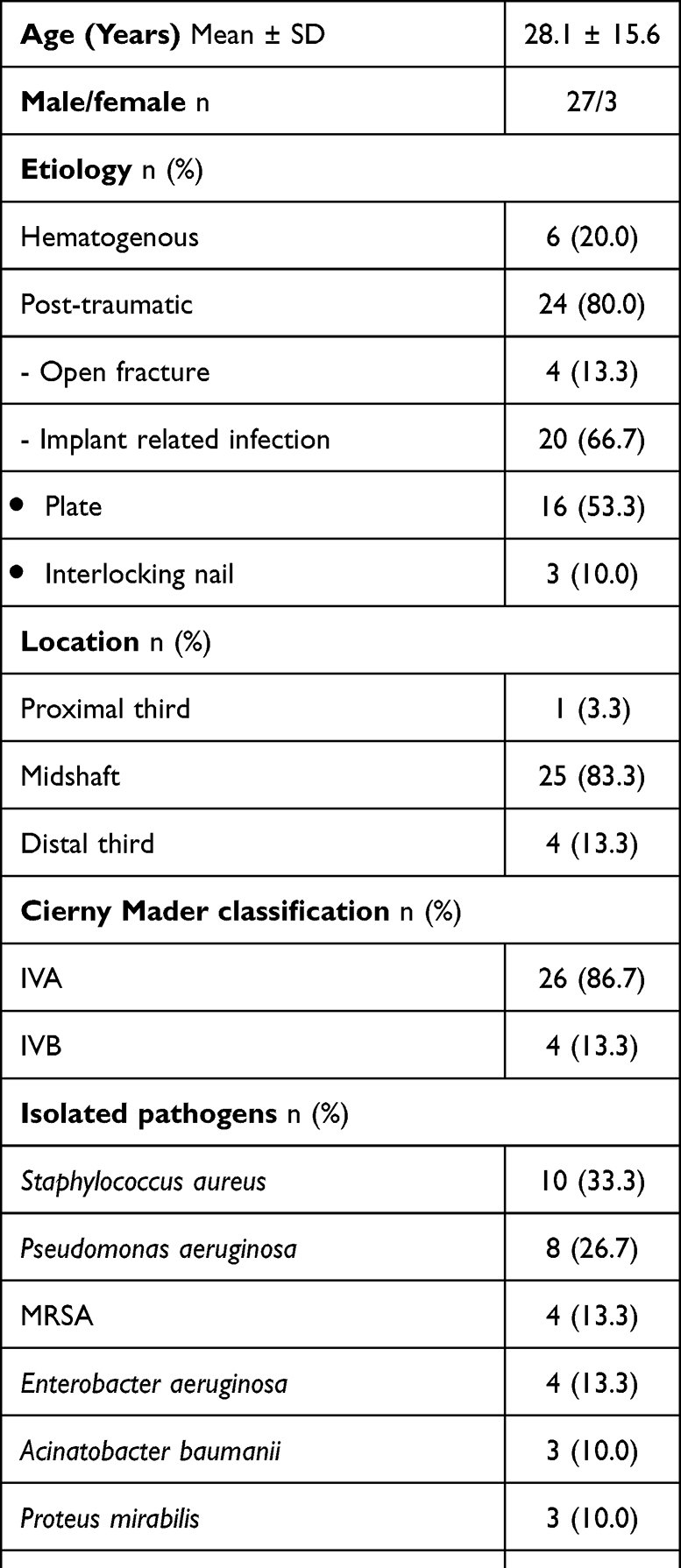 |
Table 1 Baseline Characteristics in the Studied Patients (n = 30) |
Acute compression was done in 25 cases, bone transport in 5 cases and autogenous bone graft in 1 case. One patient had a fracture at the thin bone segment which was allowed to be overlapped to get a bigger bone diameter and was treated with reinsertion of LRS and lengthening. One patient who had a bone graft at a 3 cm segmental defect had s persistent infection and required repeated bone resection and bone transport.
All infections were resolved at the end of follow-up (minimum 2 years). All, except one, achieved union with a mean union time of 8.6 months (range 4–20 months). The mean union time for acute compression was 7.6 months (range 4–20 months) while it was 14.5 months (range 12–18 month) for patients with bone transport.
The patient who had non-union was a 42-year-old man with a pathological fracture at the distal third of femur secondary to femoral OM and septic arthritis of the knee. He had no evidence of infection clinically and his blood parameters were normal at his 4-year follow-up.
The mean limb length discrepancy was 1.8 cm (range 0–4 cm). At the end of follow-up, two patients were not able to ambulate without support; one due to non-union and one due to paraplegia. Complications identified during follow-up and their management are illustrated in Table 2.
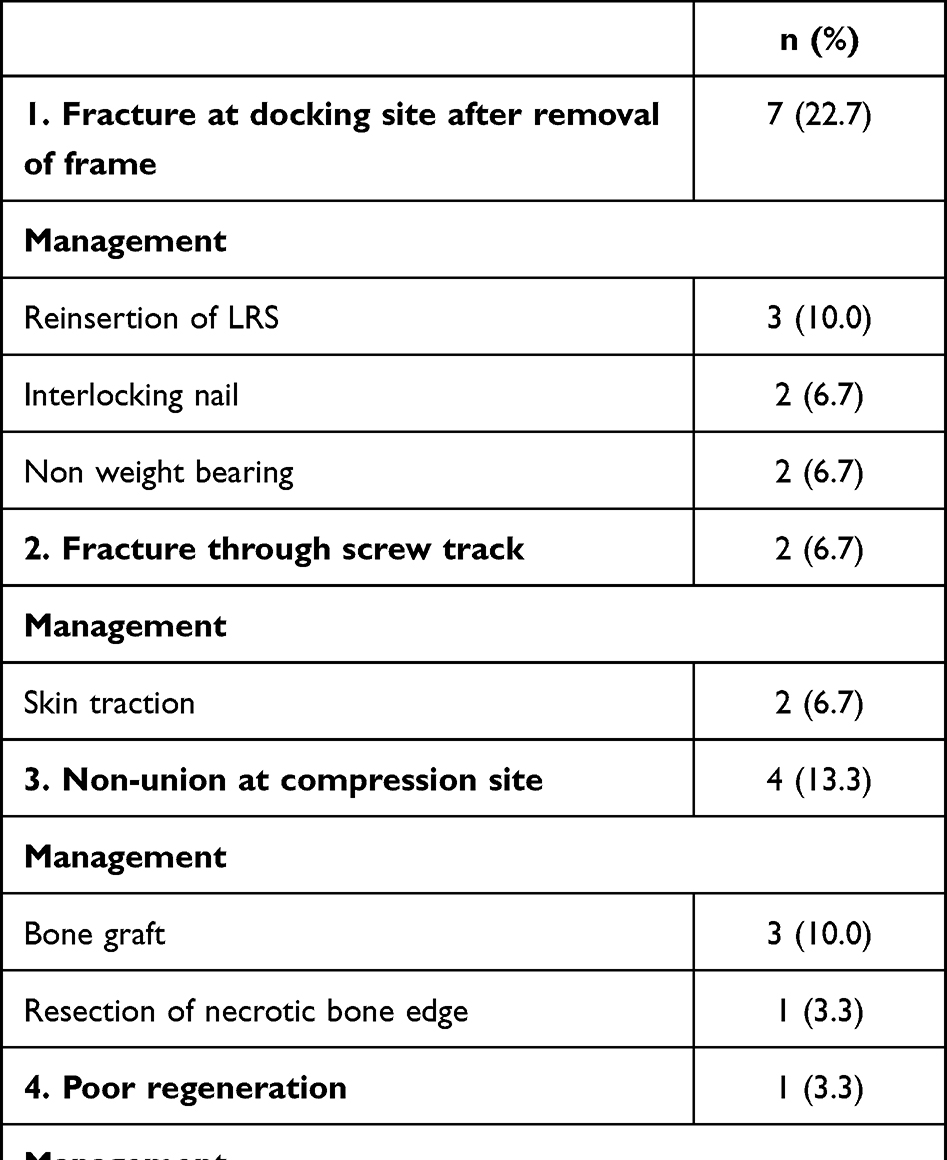 |
Table 2 Reported Treatment Complications and Their Management (n = 30) |
Discussion
External fixation is not commonly used to treat femoral fractures due to pin site infection. However, in the presence of an infection, external fixation is the only choice of treatment that provides stability and allows patients to ambulate.8
In the present study, using LRS, all infections were resolved at the end of follow up and apart from one patient, union was achieved in all patients. Our results are comparable with others. Arora et al5 achieved 100% infection-free and union rates in his 15 patients who underwent bone transport for post-traumatic OM of the femur using LRS.
In our series, we had one case of non-union in a patient with haematogenous OM of the femur with septic arthritis of the knee. Notably, treatment for haematogenous OM is more challenging because the infection is more widespread.
In our study, we used tobramycin pellets in some patients. They were found to be effective in controlling infection. McKee et al's9 study found that tobramycin pellets were as effective as antibiotic beads in controlling infection. In this study, we had 2 cases that required bone grafting 6 months after acute compression to achieve union. In comparison, Mekhail et al10 did 29 bone grafting procedures in their 19-patient series while Saleh and Rees11 performed additional bone grafting in their 16-patient study.
Also, we had 5 cases of fracture at the compression site following removal of the external fixation. Although many authors suggested that it is safe to remove the external fixation when three cortices have ossified, we still encountered this problem. Our fracture rate is higher than reported by Simpson and Kenwright12 who had a fracture rate of 9.4% especially at the regenerated bone. Krishnan et al6 had one case of fracture after removal but did not mention the location of the fracture.
In our work, all fractures occurred in patients who underwent acute compression following the resection of infected bone. We did not augment with bone grafts in the same procedure due to the presence of infection. We only performed bone grafting during follow up if we observed poor bone healing at the docking site. We identified the cause of refracture as the early removal of the frame in one case and reduced amount of bone contact due to partial bone loss at resected bone ends in the other 4 cases. We now perform delayed bone grafting when there is a reduced contact surface at the fracture end as described by Giotakis et al.13
In our study, one 14-year-old boy experienced fracture through the screw hole. A similar finding was reported by Simpson and Kenwright12 who suggested using smaller diameter screws for patients with small diameter bones.
Most of our patients were treated with reinsertion of LRS because the fracture occurred immediately after removal. However, three patients refused additional surgery and were treated with either skin traction or just non-weight bearing crutches because the fracture was “sticky” and did not displace much. We treated one patient who had a fracture 3 months after removal with intramedullary nailing without any complications in accordance with Krishnan et al.6 In contrast, Simpson and Kenwright12 noted deep infections among the 3 patients who underwent interlocking nails even though the screw tracks were healthy during the procedure. They preferred using plate to treat this complication.
Most of our patients had a shortening of less than 2 cm. Three had 4 centimetres shortening; one paraplegic patient, a 71-year-old man with a pathological fracture from haematogenous OM and a 43-year-old diabetic patient with infections following plate OM with poor social support. In fact, we felt these patients were not good candidates for bone transport.
Although patients who underwent acute compression had shortening, most of them were not bothered by it. Only one of our patients was not happy with the 2-cm shortening. He underwent lengthening of the tibia because there was very high soft tissue resistance during his femoral bone transport process. The main advantage of acute compression is to reduce the external fixation time. Patients who underwent bone transport united in twice the time of acute compression. This finding was similar to that reported by Saleh and Rees.11
In conclusion, the present study identified treatment of femoral OM using LRS as a feasible and effective technique with good outcomes. Reported complications could be adequately managed in most cases. However, these conclusions may be limited by the small sample size of the study and lack of comparison with other surgical interventions. Well-designed randomized clinical studies are recommended to compare LRS to other interventions.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This prospective study was conducted at the Advanced Trauma and Limb Reconstruction Unit, Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia from 2010 till 2014. The local ethical committee approved the study protocol and all patients provided informed consent before enrolment.
Consent for Publication
All authors reviewed the manuscript and approved its submission.
Acknowledgments
We heartfully thank all patients who agreed to participate in this work. We also express our gratitude to Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia and the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Barakat A, Schilling WH, Sharma S, Guryel E, Freeman R. Chronic osteomyelitis: a review on current concepts and trends in treatment. Orthop Trauma. 2019;33(3):181–187. doi:10.1016/j.mporth.2019.03.005
2. Hofstee MI, Muthukrishnan G, Atkins GJ, et al. Current concepts of osteomyelitis: from pathologic mechanisms to advanced research methods. Am J Pathol. 2020;190(6):1151–1163. doi:10.1016/j.ajpath.2020.02.007
3. Klein K, Schweizer TA, Siwy K, et al. Establishment of a localized acute implant-associated Staphylococcus aureus bone infection model in sheep. Pathog Dis. 2021;79(6):ftab032. doi:10.1093/femspd/ftab032
4. Lazzarini L, Mader JT, Calhoun JH. Osteomyelitis in long bone. J Bone Joint Surg Am. 2004;86A:2305–2318. doi:10.2106/00004623-200410000-00028
5. Arora S, Batra S, Gupta V, Goyal A. Distraction osteogenesis using a monolateral external fixator for infected non-union of the femur with bone loss. J Orthopaed Surg. 2012;20(2):185–190. doi:10.1177/230949901202000210
6. Krishnan A, Pamecha C, Patwa JJ. Modified ilizarov technique for infected nonunion of the femur: the principle of distraction –compression osteogenesis. J Orthop Surg. 2006;14:265–272. doi:10.1177/230949900601400307
7. Nayagam S. Femoral lengthening with a rail external fixator: tips and tricks. Strat Traum Limb Recon. 2010;5:137–144. doi:10.1007/s11751-010-0098-4
8. Beebe MJ, Kelly DM, Warner WC, Sawyer JR. Current controversies in the treatment of pediatric femoral shaft fractures. Curr Orthop Pract. 2009;20(6):634–640. doi:10.1097/BCO.0b013e3181baee8b
9. McKee MD, Li-Bland EA, Wild LM, Schemitsch EH. A prospective, randomised clinical trial comparing an antibiotic-impregnated bioabsorbable bone substitute with standard antibiotic-impregnated cement beads in the treatment of chronic osteomyelitis and infected nonunion. J Orthop Trauma. 2010;24(8):483–490. doi:10.1097/BOT.0b013e3181df91d9
10. Mekhail AO, Abraham E, Gruber B, Gonzalez M. Bone transport in the management of post traumatic bone defects in the lower extremity. J Trauma. 2004;56:368–378. doi:10.1097/01.TA.0000057234.48501.30
11. Saleh M, Rees A. Bifocal surgery for deformity and bone loss after lower-limb fractures. Comparison of bone-transport and compression-distraction methods. J Bone Joint Surg Br. 1995;77(3):429–434. doi:10.1302/0301-620X.77B3.7744930
12. Simpson AH, Kenwright J. Fracture after distraction osteogenesis. J Bone Joint Surg. 2000;82-B:659–665. doi:10.1302/0301-620X.82B5.0820659
13. Giotakis N, Narayan B, Nayagam S. Distraction osteogenesis and nonunion of the docking site: is there an ideal treatment option? Injury Int J Care Injured. 2007;38S1:S100–S107.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.