")
Back to Journals » Infection and Drug Resistance » Volume 16
Molecular Epidemiology of Community-Acquired Methicillin-Resistant Staphylococcus aureus and Clinical Characteristics of Different Sites of Infection
Authors Zhong J, Wei M , Yang C, Yin Y, Bai Y, Li R, Gu L
Received 29 December 2022
Accepted for publication 9 February 2023
Published 15 March 2023 Volume 2023:16 Pages 1485—1497
DOI https://doi.org/10.2147/IDR.S401998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jingjing Zhong, Ming Wei, Chunxia Yang, Yudong Yin, Yu Bai, Ran Li, Li Gu
Department of Infectious Diseases and Clinical Microbiology, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Li Gu, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100000, People’s Republic of China, Email [email protected]
Purpose: Since community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) was recognized, the molecular epidemiology of CA-MRSA in China has been diverse. It is unclear whether different sites of CA-MRSA infection differ in antimicrobial resistance and clinical characteristics. The purpose of this study was to identify the molecular types, virulence factors and antimicrobial resistance of CA-MRSA strains and to analyze the clinical characteristics of different sites of CA-MRSA infection.
Methods: 26 CA-MRSA strains were screened from Beijing Chao-Yang Hospital from 2014 to 2022. SCCmec type, MLST type, spa type, Panton–Valentine leukocidin (PVL), hemolysin α (Hla), phenolic soluble regulatory protein α (PSMα), toxic shock syndrome toxin-1 (TSST-1), and enterotoxin (SE) A to E were detected by PCR and gene sequencing. Antimicrobial susceptibility tests and the clinical features of CA-MRSA infection cases were collected for statistical analysis.
Results: The predominant type of CA-MRSA was ST59-t437-IV. New non-epidemic types, SCCmec VII, were also found. PVL was seen in 65.4% of CA-MRSA strains and TSST-1 was only be detected in 3.8% of CA-MRSA strain which caused poor prognosis. There were three types of infections: pneumonia (61.5%), infective endocarditis (7.7%), and skin and soft tissue infections (SSTIs) (30.8%). CA-MRSA pneumonia cases were secondary to influenza infection (37.5%). Patients with CA-MRSA-associated infective endocarditis were more likely to have underlying cardiac diseases. Patients with CA-MRSA-associated SSTIs were more likely to have a history of diabetes mellitus, and strains in this group were more susceptible to erythromycin and clindamycin.
Conclusion: ST59-t437-IV was the primary CA-MRSA type in our research and in China. We proposed that TSST-1 might be one of the indicators to predict the severity and prognosis of CA-MRSA infection. Different sites of CA-MRSA infection had difference in antibiotics susceptibility testing and underlying diseases of patients. It could provide a new perspective on treating different types of CA-MRSA infection.
Keywords: community, acquired methicillin, resistant Staphylococcus aureus, staphylococcal chromosomal cassette mec type, Panton-Valentine leukocidin, antibiotic resistance, pneumonia
Introduction
Staphylococcus aureus is a Gram-positive bacterium that can secrete several infection-related toxins and invasive enzymes, such as Panton–Valentine leukocidin (PVL), hemolysin, phenol-soluble modules (PSM), and enterotoxins.1 It is one of the leading causes of human bacterial infection around the world.2 In the past 70 years, the epidemics of antibiotic-resistant S. aureus have risen.3 Penicillin stopped being effective in treating most S. aureus infections because of the acquisition of plasmid-encoded β lactamase.4 Methicillin-resistant Staphylococcus aureus (MRSA) was first reported at a hospital in England in 1961,5 and it started being regarded as one of the leading pathogens of nosocomial infection that normally does not occur in the community.6
This view has changed with the discovery in recent decades of community-acquired MRSA (CA-MRSA). The number of CA-MRSA infections in healthy populations lacking infectious risk factors in the community has exploded since the 1990s. This new kind of MRSA strain is called community-associated MRSA (CA-MRSA). CA-MRSA differs from hospital-associated MRSA (HA-MRSA) in some aspects. Most HA-MRSA strains carry the staphylococcal chromosomal cassettes mec (SCCmec) element I, II, or III, and few carry the PVL gene. By contrast, most CA-MRSA strains carry smaller SCCmec elements, most commonly SCCmec type IV or type V, and frequently carry the genes for PVL.5 HA-MRSA isolates are multidrug-resistant, while CA-MRSA strains are susceptible to most non-β-lactam antibiotics.7 Infections caused by CA-MRSA could be various, ranging from skin and soft tissue infections (SSTIs) to invasive diseases, such as pneumonia, endocarditis, and osteomyelitis.5 The severity of these infections also covers a wide range, from minor SSTIs to necrotizing pneumonia.8 Although plenty of differences between CA-MRSA and HA-MRSA have been shown, there are no clear and specific guidelines on the epidemiology, clinical characteristics, and targeted treatment of CA-MRSA. It is also unknown whether there are differences in clinical features and antibiotic treatments among different types of infection.9 Therefore, we studied the molecular epidemiology and clinical characteristics of CA-MRSA cases and compared them with the different sites of infection to provide a basis for targeted treatment in the future.
Methods
Twenty-six cases of CA-MRSA infection were screened from 2014 to 2022 in Beijing Chao-Yang Hospital. The strains were obtained from the Beijing Chao-Yang Hospital microbiology laboratory, and the clinical data of inpatients were collected.
Participants
The Beijing Chao-Yang Hospital microbiology database includes 1506 strains of MRSA collected between 2014 and 2022. All of the strains were collected from sputum, blood, alveolar lavage fluid (BLAF) and secretion from patients diagnosed with MRSA infection in Beijing Chao-Yang Hospital. The inclusion criteria that were applied to participants were those listed in the Centers for Disease Control and Prevention (CDC) definition of CA-MRSA:6 Outpatients with positive MRSA culture or inpatients within 48 hours of admission have no history of hospitalization, surgery, long-term care in the past one year, no indwelling catheter, and no previous positive MRSA culture. Patients with the following criteria were excluded: MRSA culture was positive but lacking infectious symptoms, no radiographic evidence of MRSA infection,10 and the condition improved without using anti-MRSA antibiotics.
Molecular Typing
CA-MRSA strains were found in the microbial laboratory for culture. Species reconfirmation was performed using Vitek MALDI-TOF mass spectrometry. A DNA extraction kit (TIANGEN, DP302, China) was used to extract DNA.
SCCmec typing, MLST typing, and spa typing were analyzed by PCR sequencing. The primers of SCCmec typing, MLST typing, and spa typing and their references are shown in Table 1.11–14 The reaction system was as follows: 0.4 μL of each forward and reverse primer, 12.5 μL of 2×Taq PCR Mix (TIANGEN, China), 2 μL of DNA template, and 9.7 μL of deionized water. Amplification of SCCmec typing was performed using a GeneAmp1 PCR System 9700 (Applied Biosystems, USA) under the following conditions: activation of the enzyme at 94°C for 4 min; 30 cycles of denaturation at 94°C for 30s, annealing at 55°C for 30s, and extension at 72°C for 1 min; and a final extension at 72°C for 10 min.11 Amplification of MLST typing was performed under the following conditions: activation of the enzyme at 94°C for 5 min; 40 cycles of denaturation at 94°C for 15s, annealing at 55°C for 30s, and extension at 72°C for 1 min; and a final extension at 72°C for 10 min.14 Amplification of spa typing was performed under the following conditions: activation of the enzyme at 80°C for 5 min; 35 cycles of denaturation at 94°C for 45s, annealing at 60°C for 45s, and extension at 72°C for 90s; and a final extension at 72°C for 10 min. All PCR products were stored at 4°C.13 The PCR products were sequenced bidirectionally using an ABI 3730XL DNA sequencer (Applied Biosystems). All PCR products were subjected to agarose gel electrophoresis. The bands were observed under UV light.
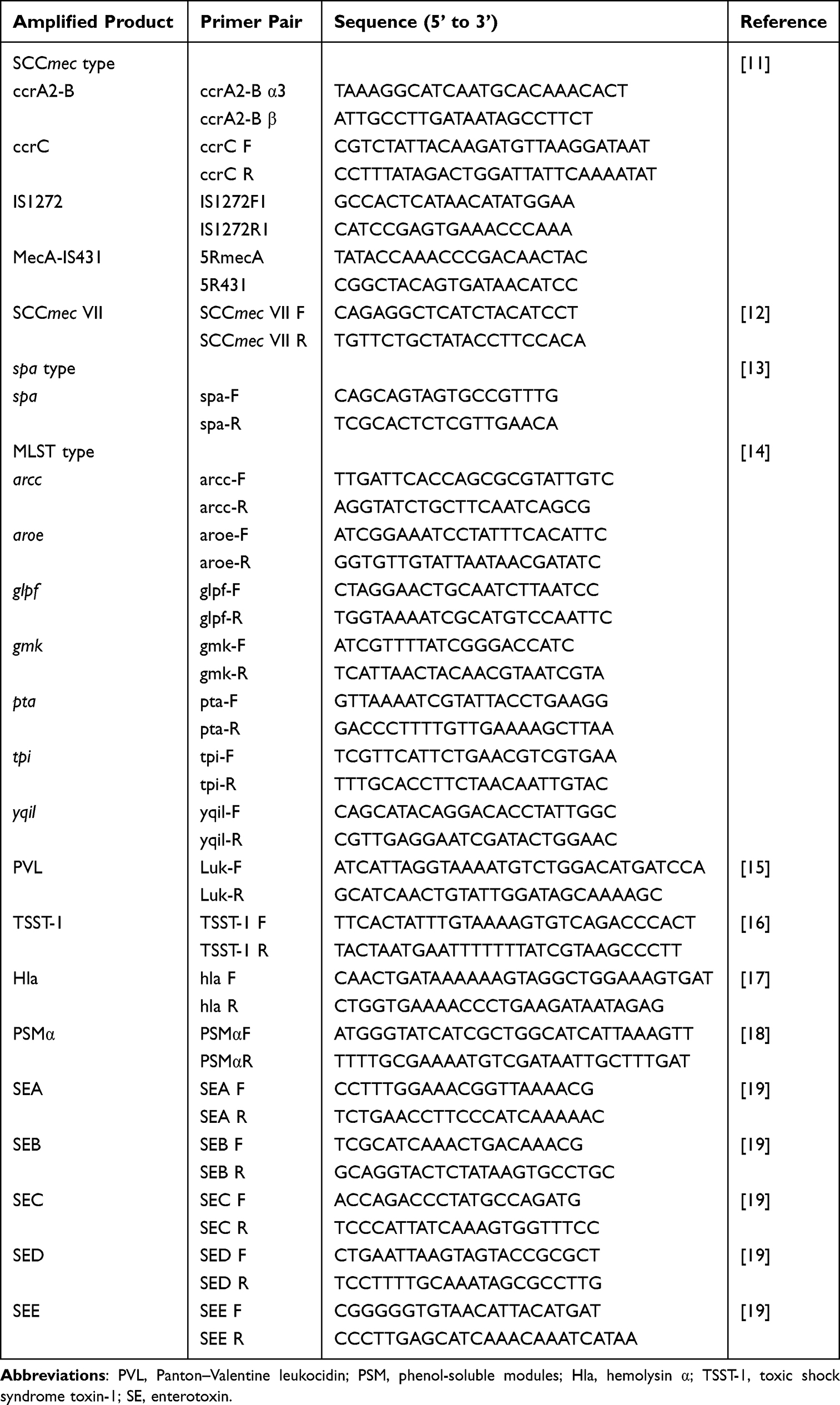 |
Table 1 CA-MRSA Primer Sequences and the Respective References Used in Our Study |
The criteria for SCCmec typing are shown in Table 2. We sent MLST and spa typing PCR products to the Ruibiotech Company for gene sequencing. The results were uploaded to online databases (https://pubmlst.org/ and https://cge.food.dtu.dk/services/spaTyper/).
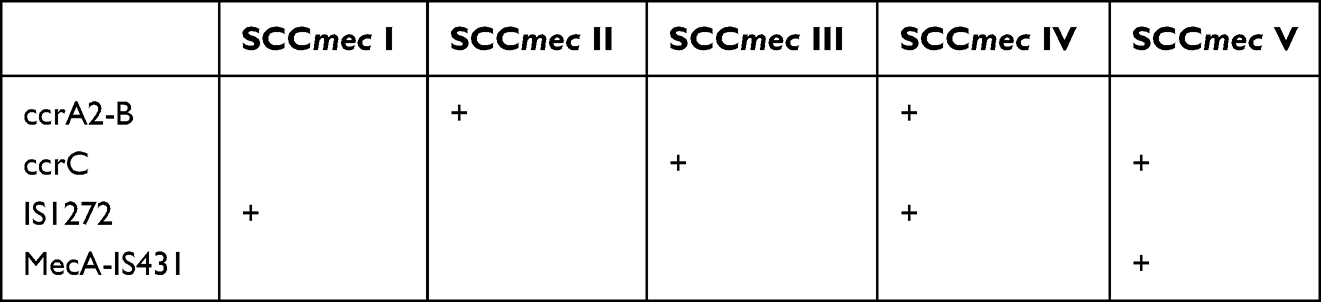 |
Table 2 The SCCmec Typing Criteria of CA-MRSA11 |
Detection of Virulence Factor
We detected nine virulence factors, namely PVL, hemolysin α (Hla), PSMα, toxic shock syndrome toxin-1 (TSST-1), and enterotoxin (SE) A–E, by using independent PCR assays. The PCR reaction system contained 0.4 μL of each forward and reverse primer, 12.5 μL of 2×Taq PCR Mix (TIANGEN, China), 2 μL of DNA template, and 9.7 μL of deionized water. All PCR products were detected by 1.0% agarose gel electrophoresis. Primers of virulence factors and their references are shown in Table 1.15–19
Antibiotics Susceptibility Testing
We performed the antibiotics susceptibility testing to 26 CA-MRSA for 15 kinds of antibiotics, including Teicoplanin, Penicillin, Oxacillin, Levofloxacin, Tetracycline, Linezolid, Tigecycline, Erythromycin, Clindamycin, Ciprofloxacin, Gentamicin, trimethoprim-sulfamethoxazole (TMP-SMZ), Vancomycin, Rifampicin and Moxifloxacin. Teicoplanin disk (30 ug) was purchased from Thermo Scientific ™ Oxoid, USA as well as other antibiotics using the commercial VITEK® AST-GP67 cards purchased from bioMérieux, France. The results of antibiotics susceptibility test were determined by BMD using the commercial Sensititre™ RAPMYCOI (Thermo Scientific, the United States) and the results were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) guideline.20
Clinical Data
We found the CA-MRSA inpatients’ data through the Hospital Information System. The data included sex, age, smoking history, drinking history, length of hospital stay, time of discharge/death, length of hospital stay, underlying diseases, previous operation history, admission blood routine, procalcitonin (PCT), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), biochemical tests, cheat imaging, and antimicrobial susceptibility testing. We collected data contemporaneously with the first detection of CA-MRSA.
Statistical Analysis
All data were processed using SPSS 25.0 statistical software. Enumeration data were expressed as N (%). If normally distributed, measurement data were represented as mean ± standard error and median (quartile) if not. Enumeration data were analyzed by χ2 test. The Fisher test analyzed measurement data conforming to a normal distribution, and measurement data not conforming to normal distribution were analyzed by the Kruskal–Wallis test. P < 0.05 was considered statistically significant.
Results
Molecular Typing
Twenty-six CA-MRSA strains were included in our study, excluding hospital-associated MRSA and MRSA of colonization according to inclusion and exclusion criteria. SCCmec IV was the predominant SCCmec type, accounting for 73.1%, followed by SCCmec VII (11.5%) and SCCmec V (7.7%). One strain of SCCmec I was in the SSTIs group, which was not found in the other two groups. One strain of CA-MRSA in the pneumonia group did not belong to SCCmec I ~ V or VII. Among 26 CA-MRSA strains, ST59 (69.2%) was the predominant MLST type, followed by ST88 (3.8%). A total of ten spa types were found in this study, among which the t437 type was the predominant type (53.8%). The predominant type of 26 CA-MRSA strains was ST59-t437-IV (46.15%). The genetic phenotype distribution for CA-MRSA strains is shown in Table 3.
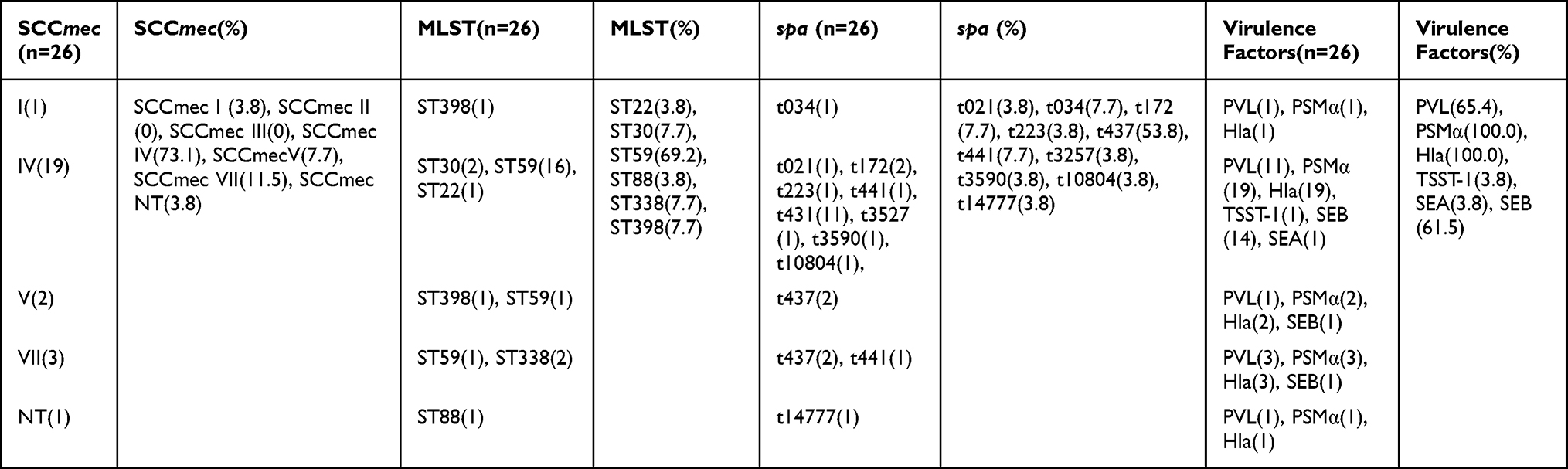 |
Table 3 Molecular Typing and Virulence Factors of CA-MRSA Strains Obtained from the Beijing Chao-Yang Hospital Microbiology Laboratory |
Virulence Factors
Nine virulence factors were detected in our study. Hla and PSMα were found in all CA-MRSA strains. PVL was not found in the infective endocarditis group but could be seen in the pneumonia group (75.0%) and the SSTIs group (62.5%). Only one strain of CA-MRSA was found to have TSST-1 in the pneumonia group. TSST-1-positive CA-MRSA infection was associated with sepsis (P=0.037), septic shock (P=0.005), acute renal insufficiency (P<0.001), and death (P<0.001). The presentation of virulence factors for these CA-MRSA strains is shown in Table 4, and the association between infective complications and PVL or TSST-1 of CA-MRSA strains is shown in Table 5.
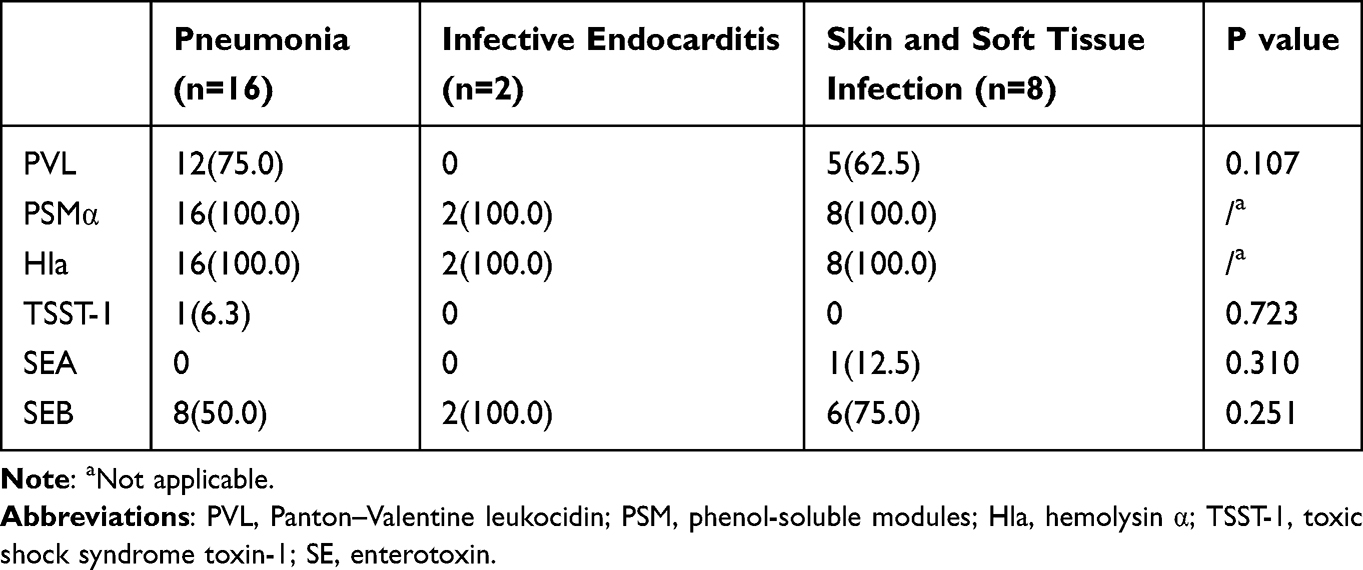 |
Table 4 Virulence Factors of CA-MRSA Strains Caused Different Sites of Infection Obtained from the Beijing Chao-Yang Hospital Microbiology Laboratory |
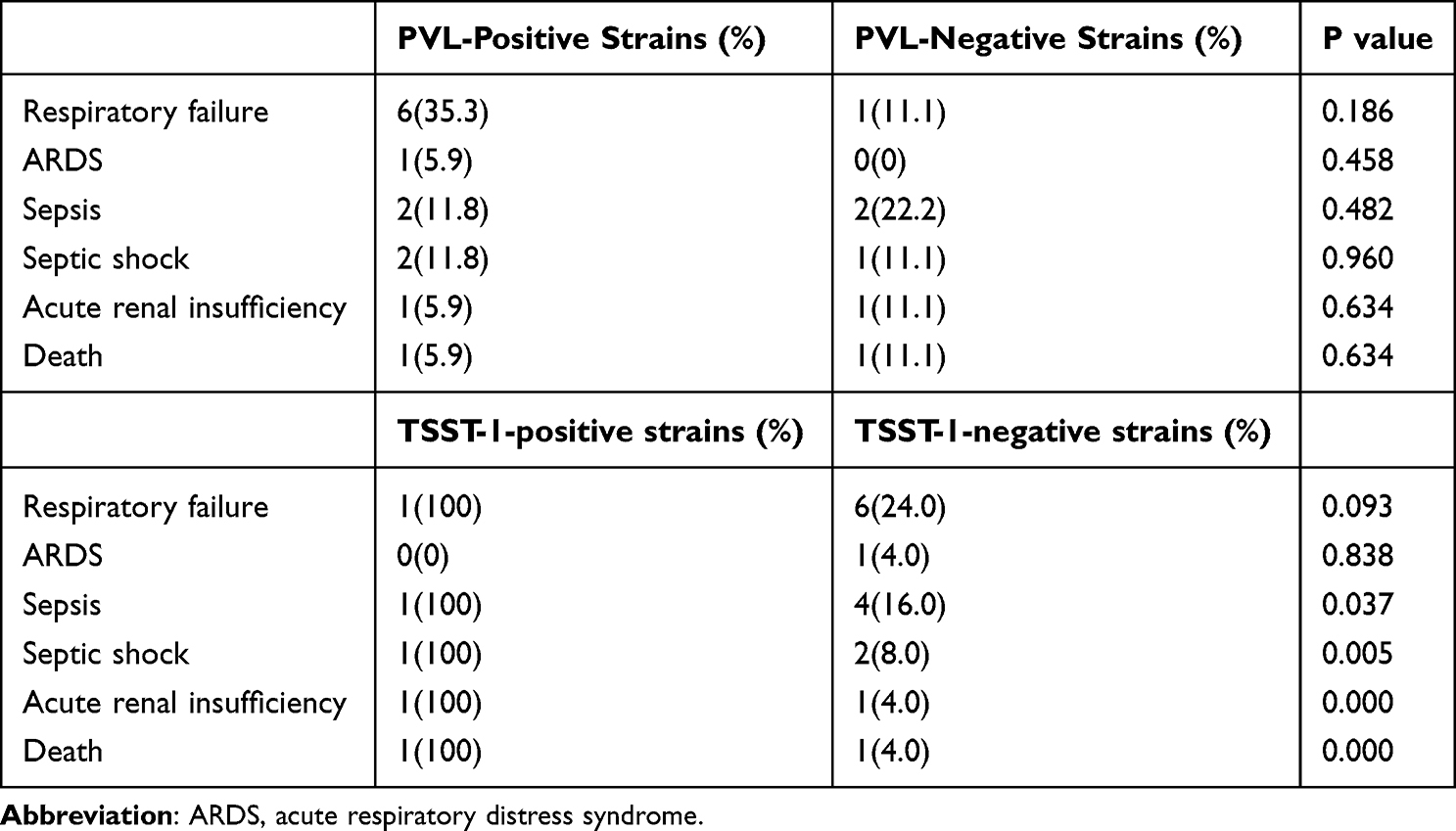 |
Table 5 The Association Between Infective Complications PVL or TSST-1 of CA-MRSA Strains |
Antibiotic Susceptibility Testing
All CA-MRSA strains were susceptible to teicoplanin, levofloxacin, moxifloxacin, tigecycline, ciprofloxacin, vancomycin, and linezolid. No vancomycin-resistant S. aureus (VRSA) or vancomycin-intermediate S. aureus (VISA) was found. We found that 69.2% of CA-MRSA were resistant to erythromycin and clindamycin. The macrolides resistance rate of the pneumonia group was 69.2%, that of the infective endocarditis group was 100%, and that of the SSTIs group was 12.5% (P<0.001). Only 7.7% of CA-MRSA strains were resistant to TMP-SMX, all of which were in the pneumonia group. CA-MRSA strains of the pneumonia group and the infective endocarditis group were susceptible to ciprofloxacin, while 37.5% of CA-MRSA strains in the SSTIs group were intermediate to ciprofloxacin (P=0.022). The type of two CA-MRSA strains mediated ciprofloxacin was ST59-t3590-IV and ST59-t172-IV, respectively. The antibiotic resistance rates for all CA-MRSA isolates are presented in Table 6.
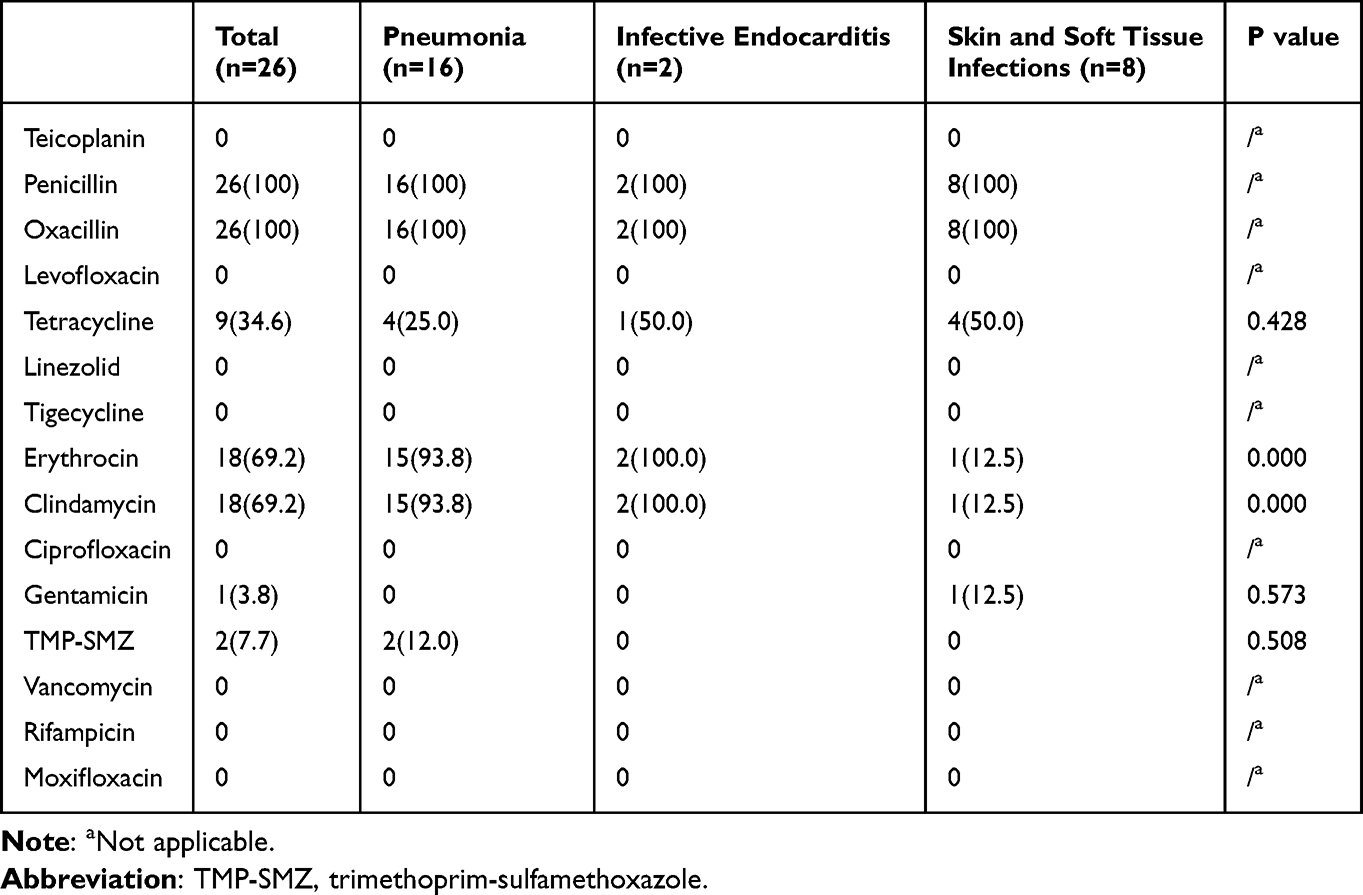 |
Table 6 The Antimicrobial Resistance Rate of CA-MRSA Obtained from the Beijing Chao-Yang Hospital Microbiology Laboratory in Different Infection Types |
Clinical Characteristics
We found that 37.5% of cases in the pneumonia group were secondary to influenza infection. Pleural effusion was found in 81.3% of the pneumonia group, 0 in the infective endocarditis group and 12.5% in the SSTIs groups (P=0.06). There were 62.5% of patients with diabetes mellitus in the SSTIs group, 12.5% of cases with diabetes mellitus in the pneumonia group, and no cases with diabetes mellitus in the infective endocarditis group (P=0.023). There were two severe cases in the SSTIs group. Both of them developed bacteremia and progressed to osteomyelitis. One severe SSTIs case was cured, and the other had a poor prognosis. The infection site of the case with a better prognosis was the lumbar vertebra, and that of the other case was the cervical vertebra. Vancomycin and linezolid were successively used for the anti-infective treatment of two cases. Surgery was only performed in the case with a poor prognosis, and the outcome of this case was high paraplegia. All patients in the infective endocarditis group had cardiovascular diseases, while 18.8% of patients in the pneumonia group and 12.5% in the SSTIs group had cardiovascular diseases (P=0.025).
Treatment and Outcomes
Vancomycin was used for treatment in 66.7% of CA-MRSA cases. Common anti-CA-MRSA antibiotics were not used in 33.3% of patients. A total of 34.6% of cases were treated with invasive mechanical ventilation, among which 43.8% of cases in the pneumonia group and 100% of cases in the infective endocarditis group were treated with invasive mechanical ventilation. No patients in the SSTIs group were treated with invasive mechanical ventilation (P=0.014). All patients in the infective endocarditis group received surgery (P < 0.001), so gastrojejunal catheterization, drainage tube indwelling, and invasive mechanical ventilation were used in patients of the infective endocarditis group. In the pneumonia group, 43.8% of the patients had respiratory failure treated with invasive mechanical ventilation. All of the death cases were in the pneumonia group, and one case was positive for TSST-1. The clinical features for all CA-MRSA isolation are shown in Table 7.
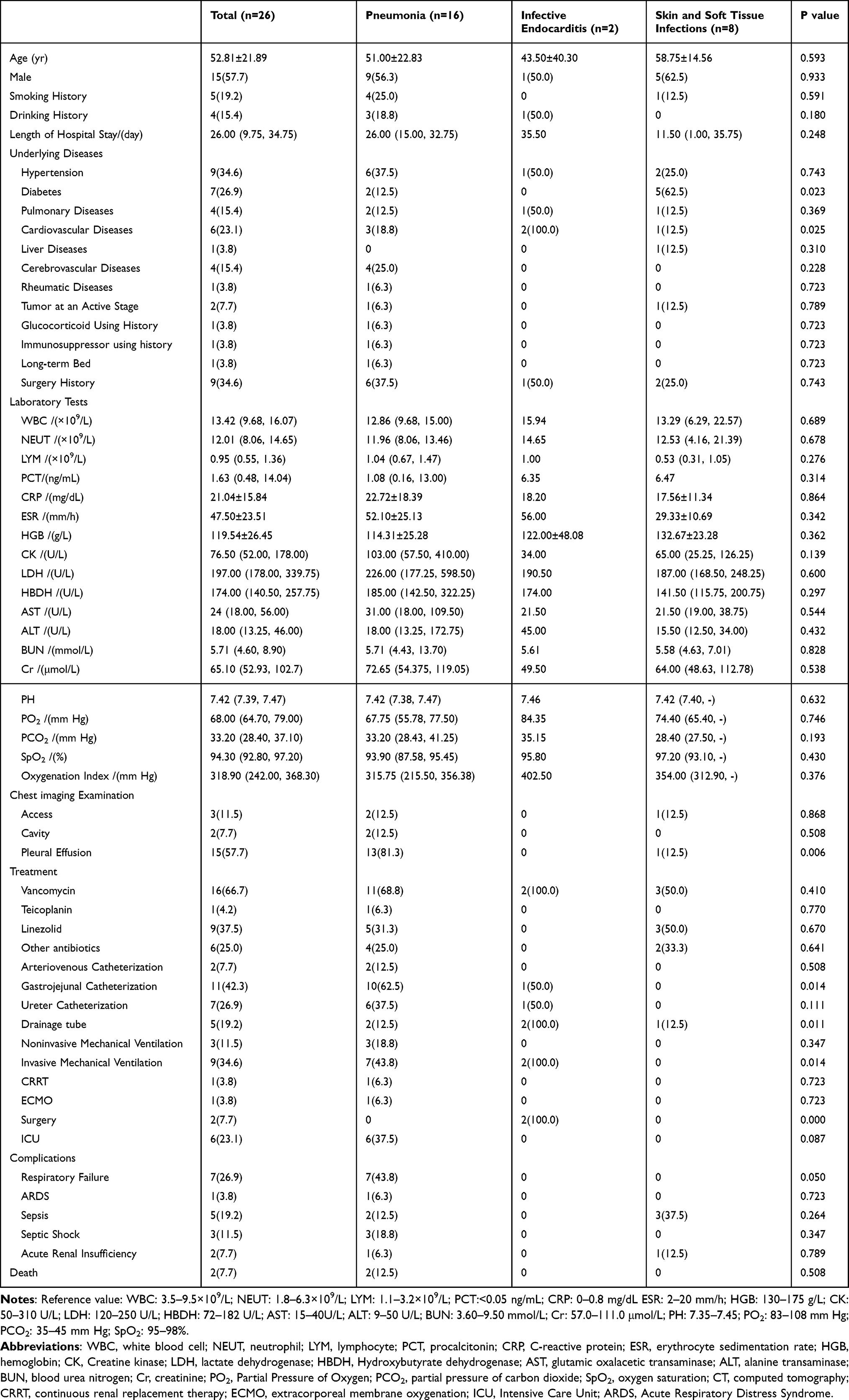 |
Table 7 Clinical Characteristics of Patients in Different CA-MRSA Infection Groups |
Discussion
There are various molecular types of MRSA, including SCCmec type, MLST type, spa type, and PFGE type. There are also differences in the prevalence of CA-MRSA in different regions.21 The predominant epidemic strain in the United States is USA300,5 while the molecular epidemiology of CA-MRSA in China is diverse. ST59-t437-IV was the primary CA-MRSA type (46.15%, 12/26) in our research, which was also the predominant CA-MRSA epidemic type in China.22 SCCmec IV and SCCmec V were the predominant types in CA-MRSA. Among the 26 CA-MRSA strains in our study, the predominant SCCmec type was SCCmec IV, followed by SCCmec VII, and only 7.7% were SCCmec V. In 2022, Wang et al23 sequenced the whole genome of 565 MRSA strains from several hospitals in different provinces of China and found six kinds of SCCmec types, among which SCCmec IV was the primary SCCmec type (48.8%, 276/565), and SCCmec VII was also found. However, the association between SCCmec VII and CA-MRSA is still unclear.
SCCmec IV and PVL are CA-MRSA-related molecular markers worldwide,24 but PVL is not necessarily present in all CA-MRSA strains. PVL was found in 65.4% of CA-MRSA included in our study, while PVL was not detected in 34.6% of the CA-MRSA strains. Several studies in the United States have found that PVL is mostly associated with SSTIs and severe invasive infections, such as community-acquired necrotizing pneumonia,25 severe sepsis,5 and other fatal infections. Montgomery et al26 found that PVL did not affect toxic or inflammatory transcriptional responses in a rat model of USA300 necrotizing pneumonia. PVL-positive CA-MRSA strains were found in 75.0% of the pneumonia group and 62.5% of the SSTIs group, while PVL was not found in the CA-MRSA strains of the infective endocarditis group. PVL was not statistically associated with infectious complications and death in our study, either. Therefore, the role of PVL in CA-MRSA infection is still controversial. The association between PVL and CA-MRSA still needs to be confirmed by additional studies.
Hla, a pore-forming toxin of S. aureus, was shown to be essential for the severity of pneumonia caused by USA300 and USA400 in a mouse model of pneumonia.27 PSM is also a kind of S. aureus pore-forming toxin, mainly expressed by highly virulent S. aureus, and is closely related to its pathogenic mechanism.28 PSM can be divided into α and β types and α-type PSM can promote and lyse neutrophils and other host cells, expressed in most staphylococci and released at high levels in CA-MRSA.29 Hla and PSMα were found in all CA-MRSA included in our study, indicating that Hla and PSMα are not only associated with pneumonia but may be associated with other types of infection caused by CA-MRSA strains. However, the relationship between Hla and PSMα and the disease severity is unknown.
Toxic shock syndrome toxin (TSST-1), a type of S. aureus superantigen, is mainly associated with toxic shock syndrome. Its characteristic clinical manifestations are fever, rash, hypotension, and multiple organ system dysfunctions.30 Among the 26 CA-MRSA strains included in our study, only one patient was found to be positive for TSST-1. This patient experienced severe pneumonia with fever, hypotension, respiratory failure, sepsis, septic shock, and acute renal insufficiency, and eventually died. TSST-1 might have a specific correlation with infection complications and the presence of TSST-1 may indicate the severity of the disease and poor prognosis. However, there is only one strain carries TSST-1 and it is hard to eliminate the host factors and to conduct the statistical analyze. Further experiments will be conducted in the future to test this hypothesis.
Among the CA-MRSA infection cases in our study, the most common infections were pneumonia, followed by SSTIs and infective endocarditis. Pneumonia caused by CA-MRSA is prone to be secondary to influenza virus infection.31,32 In our research, 37.5% of CA-MRSA pneumonia cases had an influenza virus infection, and 83.3% caused severe pneumonia. Before we recognized CA-MRSA, necrotizing fasciitis, necrotizing pneumonia, and severe sepsis caused by S. aureus were rarely reported; however, there are many reports of CA-MRSA infections now.5 The CA-MRSA included in our study mainly caused lung infections, among which 43.8% were severe pneumonia. These severe pneumonia cases were treated with invasive mechanical ventilation, 6.3% with continuous renal replacement therapy (CRRT), and 6.3% with extracorporeal membrane oxygenation (ECMO). However, there were no specific infectious indicators of CA-MRSA pneumonia. The chest imaging of the pneumonia group mainly was pleural effusion, while the characteristics of CA-MRSA infection, such as cavity and abscess,33 were rare. Early diagnosis of CA-MRSA pneumonia is more difficult, and early identification and anti-CA-MRSA treatment are particularly critical due to the severity of CA-MRSA pneumonia.
We found that diabetes was a risk factor for SSTIs caused by CA-MRSA. Diabetic patients have changes in immune function. For example, hyperglycemia will affect the operation of white blood cells and increase the resting level of proinflammatory factors,22 which makes diabetes a risk factor for a variety of infections. In addition, skin damage and ulcers are more prone to CA-MRSA infection.22 Suppurative SSTIs are the most common clinical manifestation of CA-MRSA infection.34 Recent studies have shown that patients with diabetes are twice as likely to develop CA-MRSA SSTIs as those without diabetes.35 Patients with diabetes are more likely to create SSTIs complications. Our study found two cases of developed osteomyelitis, and the outcome of one of them was high paraplegia. This warns us that CA-MRSA-associated SSTIs could range from minor, superficial to severe infections36 and may have a poor prognosis. Therefore, early treatment of SSTIs caused by CA-MRSA is essential.
S. aureus is one of the most common pathogens of infective endocarditis. In developed countries, 20–30% of S. aureus infective endocarditis has been attributed to MRSA.37,38 According to epidemiological information, CA-MRSA infective endocarditis is mainly acquired in the community, associated with young and healthy people, and has no known risk factors for infective endocarditis.39 All infective endocarditis cases included in our study had underlying cardiac conditions, such as atrial fibrillation and congenital heart disease, and all patients in the infective endocarditis group accepted surgery. This suggests that people with underlying heart diseases are more likely to develop infective endocarditis caused by CA-MRSA, and surgical treatment should be performed if necessary.
Unlike HA-MRSA, CA-MRSA is susceptible to various non-β-lactam antibiotics.40 All CA-MRSA strains in our study were susceptible to vancomycin and linezolid. In actual treatment, vancomycin anti-CA-MRSA therapy was preferred in 66.7% of cases after pathogen identification. Vancomycin is the first-line intravenous drug for treating MRSA infection.41 Still persistent or recurrent bacteremia, high treatment failure rate, nephrotoxicity, and the emergence of vancomycin-resistant strains during vancomycin treatment are becoming increasingly common.5 Linezolid was chosen for anti-CA-MRSA treatment in 37.5% of cases due to substandard blood concentration of vancomycin and poor treatment effect. A prospective randomized controlled study on MRSA hospital-acquired pneumonia42 showed that the linezolid group had a better clinical response and less nephrotoxicity than the vancomycin group. Still, there was no difference in 60-day mortality between the two groups. Linezolid has adverse effects with prolonged therapy, including myelosuppression and neuropathy, but its overall incidence is rare.43 Several studies also suggested that linezolid was more efficient than vancomycin.44 However, vancomycin is still the first-line drug to treat MRSA infections. It is worth considering whether linezolid could replace vancomycin.
In our study, only 7.7% of CA-MRSA strains were resistant to TMP-SMX, and all were pneumonia pathogens. The infective endocarditis group and the SSTIs group were susceptible to TMP-SMX. TMP-SMX shows great bacterial activity against susceptible S. aureus, including MRSA, and its oral bioavailability is excellent. Several studies concluded that TMP-SMX was an orally available choice for treating MRSA infections, including SSTIs and endocarditis.45 However, Pallin et al46 found no difference in effectiveness between cephalexin-combined TMP-SMX and cephalexin alone in treating cellulitis without abscess. There are few studies on treating invasive CA-MRSA infection by intravenous TMP-SMX. More clinical trials are needed to explore whether TMP-SMX could be the first-line antibiotic for treating CA-MRSA infections.
Most CA-MRSA in the pneumonia group and the infective endocarditis group were resistant to macrolides such as erythromycin and clindamycin in our study. By contrast, all CA-MRSA strains in the SSTIs group were susceptible to macrolides. Vancomycin is still the first choice for the treatment of SSTIs in most cases. The efficacy of macrolide for SSTIs is unknown, but it can provide a new choice for the future treatment of SSTIs caused by CA-MRSA. CA-MRSA strains in our study were susceptible to quinolones such as levofloxacin and moxifloxacin, and 65.4% of CA-MRSA strains were susceptible to tetracycline. However, few cases of treating CA-MRSA infection used quinolones and tetracycline. The current guidelines do not explicitly cover the antibiotic treatment of CA-MRSA, and the treatment of severe pneumonia infection caused by CA-MRSA and HA-MRSA is usually the same.47 The findings of our study can provide new insights for different types of infections caused by CA-MRSA.
Conclusion
CA-MRSA can cause various infections, such as pneumonia, infective endocarditis, and SSTIs. About half of the cases of CA-MRSA pneumonia have infectious complications. The condition is severe, and the prognosis is poor. The infective endocarditis and SSTIs caused by CA-MRSA also have severe cases. CA-MRSA is highly susceptible to non-β-lactam antibiotics, and there seem to be more choices of antibiotics, but supporting data are still lacking. Therefore, early identification and specific treatment have become the top priority to prevent adverse consequences. More studies are needed to clarify the differences among different types of CA-MRSA infection, so we can establish a definitive treatment.
Ethical Standards
The Beijing Chao-Yang Hospital Ethics Committee (2015-KE-158) approved the study and written informed consent was obtained from every participant. All participants have been informed of the use of their samples and clinical tests results and have given their informed consent. The authors assert that all procedures contributing to this work comply with the ethical standards of relevant national and institutional committees on human experimentation and with Helsinki Declaration of 1975, revised in 2013.
Acknowledgments
We thank all those who have contributed S. aureus genome sequences to GenBank (https://www.ncbi.nlm.nih.gov/genbank), the MLST database (https://pubmlst.org/), and the spa database (https://cge.food.dtu.dk/services/spaTyper/). The authors would like to thank all Department of Infectious Diseases and Clinical Microbiology staff members at Beijing Chao-Yang Hospital (Beijing, China) for contributing to this work. We thank LetPub for its linguistic assistance during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Reform and Development Program of Beijing Institute of Respiratory Medicine. The funder played no role in the design of the study, nor in the collection, analysis, and interpretation of data, nor in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jenkins A, Diep BA, Mai TT, et al. Differential expression and roles of Staphylococcus aureus virulence determinants during colonization and disease. mBio. 2015;6(1):e02272–14. doi:10.1128/mBio.02272-14
2. Diekema DJ, Pfaller MA, Schmitz FJ, et al. Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997–1999. Clin Infect Dis. 2001;32:S114–S132. doi:10.1086/320184
3. DeLeo FR, Chambers HF. Reemergence of antibiotic-resistant Staphylococcus aureus in the genomics era. J Clin Invest. 2009;119(9):2464–2474. doi:10.1172/JCI38226
4. Kirby WM. Extraction of a highly potent penicillin inactivator from penicillin resistant Staphylococci. Science. 1944;99(2579):452–453. doi:10.1126/science.99.2579.452
5. David MZ, Daum RS. Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clin Microbiol Rev. 2010;23(3):616–687. doi:10.1128/CMR.00081-09
6. DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010;375(9725):1557–1568. doi:10.1016/S0140-6736(09)61999-1
7. Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279(8):593–598. doi:10.1001/jama.279.8.593
8. Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Clin Infect Dis. 2005;40(1):100–107. doi:10.1086/427148
9. Mandell LA, Wunderink R. Methicillin-resistant Staphylococcus aureus and community-acquired pneumonia: an evolving relationship. Clin Infect Dis. 2012;54(8):1134–1136. doi:10.1093/cid/cis045
10. American Thoracic S; Infectious Diseases Society of A. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. doi:10.1164/rccm.200405-644ST
11. Boye K, Bartels MD, Andersen IS, Moller JA, Westh H. A new multiplex PCR for easy screening of methicillin-resistant Staphylococcus aureus SCCmec types I-V. Clin Microbiol Infect. 2007;13(7):725–727. doi:10.1111/j.1469-0691.2007.01720.x
12. Funaki T, Yasuhara T, Kugawa S, et al. SCCmec typing of PVL-positive community-acquired Staphylococcus aureus (CA-MRSA) at a Japanese hospital. Heliyon. 2019;5(3):e01415. doi:10.1016/j.heliyon.2019.e01415
13. Koreen L, Ramaswamy SV, Graviss EA, Naidich S, Musser JA, Kreiswirth BN. spa Typing method for discriminating among Staphylococcus aureus isolates: implications for use of a single marker to detect genetic micro- and macrovariation. J Clin Microbiol. 2004;42(2):792–799. doi:10.1128/Jcm.42.2.792-799.2004
14. Jolley KA, Bray JE, Maiden MCJ. Open-access bacterial population genomics: bIGSdb software, the PubMLST.org website and their applications. Wellcome Open Res. 2018;3:124. doi:10.12688/wellcomeopenres.14826.1
15. Johnsson D, Molling P, Stralin K, Soderquist B. Detection of Panton-Valentine leukocidin gene in Staphylococcus aureus by LightCycler PCR: clinical and epidemiological aspects. Clin Microbiol Infect. 2004;10(10):884–889. doi:10.1111/j.1469-0691.2004.00976.x
16. Indrawattana N, Sungkhachat O, Sookrung N, et al. Staphylococcus aureus clinical isolates: antibiotic susceptibility, molecular characteristics, and ability to form biofilm. Biomed Res Int. 2013;2013:314654. doi:10.1155/2013/314654
17. Gowrishankar S, Kamaladevi A, Balamurugan K, Pandian SK. In vitro and in vivo biofilm characterization of methicillin-resistant Staphylococcus aureus from patients associated with pharyngitis infection. Biomed Res Int. 2016;2016:1289157. doi:10.1155/2016/1289157
18. Strommenger B, Kettlitz C, Weniger T, Harmsen D, Friedrich AW, Witte W. Assignment of Staphylococcus isolates to groups by spa typing, SmaI macrorestriction analysis, and multilocus sequence typing. J Clin Microbiol. 2006;44(7):2533–2540. doi:10.1128/JCM.00420-06
19. Cheng J, Wang Y, Cao Y, et al. The distribution of 18 enterotoxin and enterotoxin-like genes in Staphylococcus aureus strains from different sources in East China. Foodborne Pathog Dis. 2016;13(4):171–176. doi:10.1089/fpd.2015.1963
20. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Twentieth Informational Supplement. Clinical and Laboratory Standards Institute; 2010. Available from: https://clsi.org/.
21. Chuang YY, Huang YC. Molecular epidemiology of community-associated meticillin-resistant Staphylococcus aureus in Asia. Lancet Infect Dis. 2013;13(8):698–708. doi:10.1016/S1473-3099(13)70136-1
22. Geng W, Yang Y, Wu D, et al. Community-acquired, methicillin-resistant Staphylococcus aureus isolated from children with community-onset pneumonia in China. Pediatr Pulmonol. 2010;45(4):387–394. doi:10.1002/ppul.21202
23. Wang B, Xu Y, Zhao H, et al. Methicillin-resistant Staphylococcus aureus in China: a multicentre longitudinal study and whole-genome sequencing. Emerg Microbes Infect. 2022;11(1):532–542. doi:10.1080/22221751.2022.2032373
24. Vandenesch F, Naimi T, Enright MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton-Valentine leukocidin genes: worldwide emergence. Emerg Infect Dis. 2003;9(8):978–984. doi:10.3201/eid0908.030089
25. Boussaud V, Parrot A, Mayaud C, et al. Life-threatening hemoptysis in adults with community-acquired pneumonia due to Panton-Valentine leukocidin-secreting Staphylococcus aureus. Intens Care Med. 2003;29(10):1840–1843. doi:10.1007/s00134-003-1918-5
26. Montgomery CP, Daum RS. Transcription of inflammatory genes in the lung after infection with community-associated methicillin-resistant Staphylococcus aureus: a role for panton-valentine leukocidin? Infect Immun. May. 2009;77(5):2159–2167. doi:10.1128/IAI.00021-09
27. Bubeck Wardenburg J, Bae T, Otto M, Deleo FR, Schneewind O. Poring over pores: alpha-hemolysin and Panton-Valentine leukocidin in Staphylococcus aureus pneumonia. Nat Med. 2007;13(12):1405–1406. doi:10.1038/nm1207-1405
28. Zhou Y, Niu C, Ma B, et al. Inhibiting PSMalpha-induced neutrophil necroptosis protects mice with MRSA pneumonia by blocking the agr system. Cell Death Dis. 2018;9(3):362. doi:10.1038/s41419-018-0398-z
29. Cassat JE, Hammer ND, Campbell JP, et al. A secreted bacterial protease tailors the Staphylococcus aureus virulence repertoire to modulate bone remodeling during osteomyelitis. Cell Host Microbe. 2013;13(6):759–772. doi:10.1016/j.chom.2013.05.003
30. Zarei Koosha R, Mahmoodzadeh Hosseini H, Mehdizadeh Aghdam E, Ghorbani Tajandareh S, Imani Fooladi AA. Distribution of TSST-1 and mecA genes in Staphylococcus aureus isolated from clinical specimens. Jundishapur J Microbiol. 2016;9(3):e29057. doi:10.5812/jjm.29057
31. Adam H, McGeer A, Simor A. Fatal case of post-influenza, community-associated MRSA pneumonia in an Ontario teenager with subsequent familial transmission. Can Commun Dis Rep. 2007;33(4):45–48.
32. Wang J, Yun L, Zhao H, Li X. Combination therapy of polymyxin B and amikacin for community-acquired pseudomonas aeruginosa pneumonia with MODS in a Previously Healthy Patient: A Case Report. Infect Drug Resist. 2021;14:2895–2900. doi:10.2147/IDR.S312601
33. Self WH, Wunderink RG, Williams DJ, et al. Staphylococcus aureus community-acquired pneumonia: prevalence, clinical characteristics, and outcomes. Clin Infect Dis. 2016;63(3):300–309. doi:10.1093/cid/ciw300
34. Buck JM, Como-Sabetti K, Harriman KH, et al. Community-associated methicillin-resistant Staphylococcus aureus, Minnesota, 2000–2003. Emerg Infect Dis. 2005;11(10):1532–1538. doi:10.3201/eid1110.050141
35. Pallin DJ, Egan DJ, Pelletier AJ, Espinola JA, Hooper DC, Camargo CA. Increased US emergency department visits for skin and soft tissue infections, and changes in antibiotic choices, during the emergence of community-associated methicillin-resistant Staphylococcus aureus. Ann Emerg Med. 2008;51(3):291–298. doi:10.1016/j.annemergmed.2007.12.004
36. Olaniyi R, Pozzi C, Grimaldi L, Bagnoli F. Staphylococcus aureus-associated skin and soft tissue infections: anatomical localization, epidemiology, therapy and potential prophylaxis. Curr Top Microbiol Immunol. 2017;409:199–227. doi:10.1007/82_2016_32
37. Maor Y, Belausov N, Ben-David D, Smollan G, Keller N, Rahav G. hVISA and MRSA endocarditis: an 8-year experience in a tertiary care centre. Clin Microbiol Infect. 2014;20(10):O730–6. doi:10.1111/1469-0691.12498
38. Xing L, Chen Y, Ling X, et al. Genomic characterization of livestock-associated methicillin-resistant Staphylococcus aureus ST7 Isolates from a case of human bacteremia in China. Infect Drug Resist. 2022;15:7449–7457. doi:10.2147/IDR.S385061
39. Millar BC, Prendergast BD, Moore JE, Community-associated MRSA. CA-MRSA): an emerging pathogen in infective endocarditis. J Antimicrob Chemother. 2008;61(1):1–7. doi:10.1093/jac/dkm410
40. Tsouklidis N, Kumar R, Heindl SE, Soni R, Khan S. Understanding the fight against resistance: hospital-acquired methicillin-resistant Staphylococcus aureus vs community-acquired methicillin-resistant Staphylococcus aureus. Cureus. 2020;12(6):e8867. doi:10.7759/cureus.8867
41. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–S72. doi:10.1086/511159
42. Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clin Infect Dis. 2012;54(5):621–629. doi:10.1093/cid/cir895
43. Yeager SD, Oliver JE, Shorman MA, Wright LR, Veve MP. Comparison of linezolid step-down therapy to standard parenteral therapy in methicillin-resistant Staphylococcus aureus bloodstream infections. Int J Antimicrob Agents. 2021;57(5):106329. doi:10.1016/j.ijantimicag.2021.106329
44. Kato H, Hagihara M, Asai N, et al. Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus. J Glob Antimicrob Resist. 2021;24:98–105. doi:10.1016/j.jgar.2020.12.009
45. Sabol KE, Echevarria KL, Lewis JS. Community-associated methicillin-resistant Staphylococcus aureus: new bug, old drugs. Ann Pharmacother. 2006;40(6):1125–1133. doi:10.1345/aph.1G404
46. Pallin DJ, Binder WD, Allen MB, et al. Clinical trial: comparative effectiveness of cephalexin plus trimethoprim-sulfamethoxazole versus cephalexin alone for treatment of uncomplicated cellulitis: a randomized controlled trial. Clin Infect Dis. 2013;56(12):1754–1762. doi:10.1093/cid/cit122
47. Rubinstein E, Kollef MH, Nathwani D. Pneumonia caused by methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2008;46(Suppl 5):S378–S385. doi:10.1086/533594
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.