")
Back to Journals » Clinical Ophthalmology » Volume 14
Modified Low Power Mode Laser for the Treatment of Central Serous Chorioretinopathy
Authors Miura M , Wakita R, Iwasaki T
Received 25 September 2020
Accepted for publication 12 November 2020
Published 30 November 2020 Volume 2020:14 Pages 4109—4113
DOI https://doi.org/10.2147/OPTH.S284005
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Masahiro Miura, Ryo Wakita, Takuya Iwasaki
Department of Ophthalmology, Tokyo Medical University, Ibaraki Medical Center, Inashiki, Ibaraki 3000395, Japan
Correspondence: Masahiro Miura
Department of Ophthalmology, Tokyo Medical University, Ibaraki Medical Center, 3-20-1 Chuo, Ami, Inashiki, Ibaraki 300395, Japan
Tel +81-298871161
Fax +81-298877656
Email [email protected]
Purpose: Low power mode (LPM) can be used for subthreshold retinal laser treatment by simply adjusting the laser parameters. Herein, we report the use of a modified LPM laser treatment for four cases of central serous chorioretinopathy (CSCR).
Patients and Methods: We retrospectively reviewed the medical records of four patients (four eyes) with persistent CSCR who underwent modified LPM laser for leakage. The laser power was first titrated with a barely visible burn, and then treatment was applied using 33% laser energy by manually adjusting the laser power and duration.
Results: Serous retinal detachment completely resolved in all cases by 2 months after treatment. Autofluorescence images did not show any specific changes induced by laser burns.
Conclusion: A modified LPM laser may provide a feasible treatment for persistent CSCR.
Keywords: central serous chorioretinopathy, subthreshold laser, low power mode, photocoagulation
Introduction
Central serous chorioretinopathy (CSCR) is a chorioretinal disorder characterized by serous retinal detachment, and it is associated with leakage from the choroid through the outer blood-retinal barrier at the retinal pigment epithelium (RPE) layer.1 This disease typically has a self-limiting course, and serous retinal detachment spontaneously resolves within 3–4 months. However, in some cases, persistent or recurrent serous retinal detachment can cause permanent structural damage in the retina, with irreversible visual disturbance.1
Several therapies have been used to seal the leakage from the choroid. For example, suprathreshold laser photocoagulation was an effective treatment option for persistent CSCR.2 However, suprathreshold laser therapy may cause untoward effects, including retinal atrophy or choroidal neovascularization at the laser scar.2 Subthreshold laser photocoagulation was developed to reduce retinal damage by adjusting the laser power, pulse duration or pulse repetition.3 Nevertheless, an essential consideration when using subthreshold laser treatment is adjustment of the laser energy under the condition of invisible laser burn. Without proper adjustment, subthreshold laser treatment may cause under-treatment or accidental retinal damage.
A recent approach for subthreshold laser treatment involves titration based on a barely visible laser burn outside of the treatment site.3 In many studies, a micropulse laser with a titration algorithm was used for subthreshold laser treatment in persistent CSCR.3 However, micropulse laser treatment is not achievable with the widely used continuous laser systems. EndPoint Management is a subthreshold laser treatment with a continuous laser system.4 The EndPoint Management program is built into the PASCAL laser system (Topcon Medical Laser Systems, Santa Clara, CA), and automatically adjusts laser power and exposure time based on the Arrhenius integral.4 The utility of this system for the treatment of CSCR was reported previously.4 However, because EndPoint Management is available only with the PASCAL laser system, it is not applicable to other continuous laser systems.
The low power mode (LPM) in the MC-500ViXi laser system (Nidek Co., Gamagori, Japan) is a new approach for laser titration, involving simple adjustment of the laser power only. Importantly, the LPM can be performed with other continuous laser systems by manual adjustment of the laser parameter. In this case series, we report the use of modified LPM laser treatment for four cases of persistent CSCR with favorable therapeutic effects.
Patients and Methods
We retrospectively evaluated four eyes of four Japanese patients with persistent CSCR (one male, three females; age range 43–72 years). The clinical characteristics of these patients are summarized in Table 1. The clinical diagnosis of persistent CSCR was made based on serous retinal detachment of the macula for 12 months or more, with fluid leakage on fundus fluorescein angiography.
 |
Table 1 Summary of Subjects |
The leakage point was treated with modified LPM using the MC-500ViXi laser system with a wavelength of 577 nm. In the original LPM configuration, the laser energy was simply reduced by adjusting the laser power. However, Lavinski et al reported that simultaneous adjustment of both laser power and pulse duration is required for proper subthreshold laser treatment.4 Thus, we estimated the optimum laser power and pulse duration at 33% laser energy, based on that study.4 We used the 100-µm spot size based on previous reports about subthreshold laser treatment for CSR.3 A 10-ms shot with 50% laser power was used for the 33% laser energy treatment, based on a 15-ms titration shot. The titration laser shot was applied to produce a barely visible burn, outside the retinal vascular arcade, at 3 sec after the laser shot. Laser treatment was then applied to the leakage point, with the following parameters: 50% laser power, 10-ms duration and four to eight shots of laser using a 0.25 diameter spacing.
This retrospective case study was performed according to the tenets of the Declaration of Helsinki, and was approved by the Institutional Review Board of the Tokyo Medical University (T2019-0181). Written informed consent was obtained from all patients regarding the potential use of their medical records for a scientific study. The confidentiality of patient data was maintained with data anonymization.
Results
The durations of serous retinal detachments prior to treatment ranged from 12 to 60 months (Table 1). Each eye had a single leakage point (Figures 1 and 2), and the distances from the leakage points to the fovea ranged from 1960 to 3600 μm. Each leakage point was treated with modified LPM. Laser shots with 33% laser energy, based on a titration shot, were performed at the leakage points. In all cases, the serous retinal detachment had completely resolved at 2 months post-treatment (Figures 1 and 2), and the best-corrected visual acuity had improved at 6 months after treatment (Table 1). Autofluorescence images (488-nm excitation, emission >500 nm) were obtained before laser treatment and at 3 months after treatment, using a Heidelberg Retina Angiograph 2 (Heidelberg Engineering, Heidelberg, Germany). Autofluorescence images did not show any specific changes at the location of the laser shots after treatment (Figures 1 and 2).
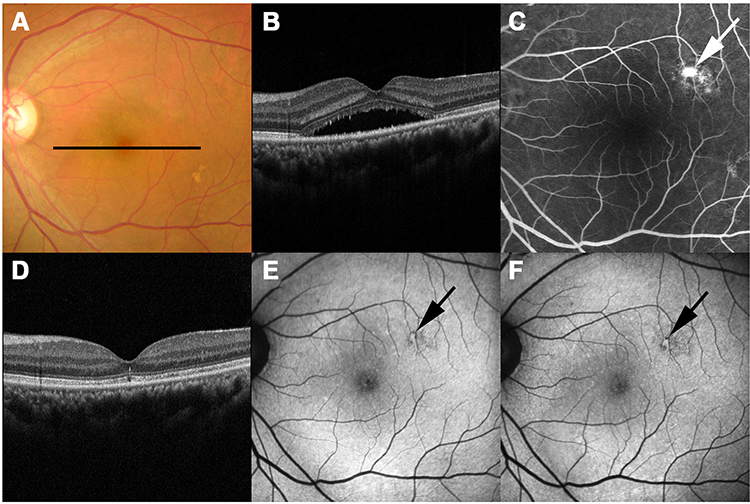 |
Figure 1 Case 1. Images from the left eye of a 46-year-old woman with persistent central serous chorioretinopathy. Color fundus photograph (A), optical coherence tomography (OCT) image (B) and fluorescein angiography (FA) image (C) before treatment. The black line in the color fundus photograph indicates the scanning line for the OCT images (B, D). The OCT image (B) shows serous retinal detachment at the macula, while the FA image (C) shows a leakage point (white arrow). Serous retinal detachment had disappeared at 2 months after laser treatment in the OCT image (D). Autofluorescence images at 3 months after treatment (F) did not show any specific changes compared with those before treatment (E) at the location of the laser shots (black arrows). |
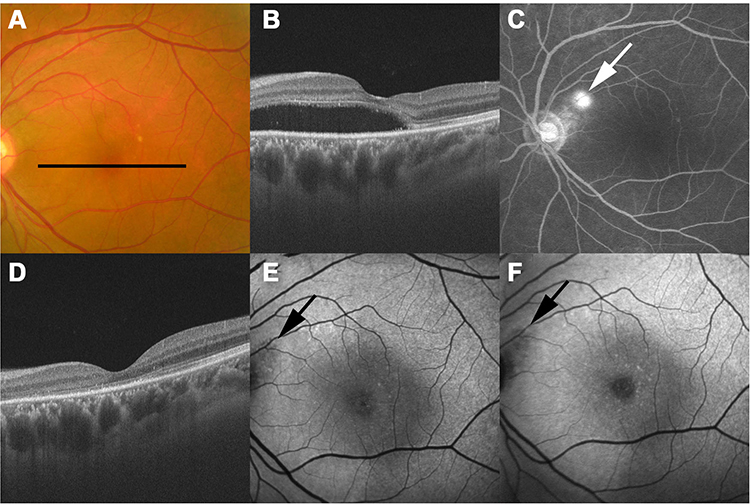 |
Figure 2 Case 2: Images from the left eye of a 43-year-old woman with persistent central serous chorioretinopathy. Color fundus photograph (A), optical coherence tomography (OCT) image (B), and fluorescein angiography (FA) image (C) before treatment. The black line in the color fundus photograph indicates the scanning line for the OCT images (B, D). The OCT image (B) shows serous retinal detachment at the macula, while the FA image (C) shows a leakage point (white arrow). Serous retinal detachment had disappeared at 2 months after laser treatment in the OCT image (D). Autofluorescence images at 3 months after treatment (F) did not show any specific changes compared with those before treatment (E) at the location of the laser shots (black arrows). |
Discussion
In this case series, modified LPM laser treatment was successfully performed in four cases of persistent CSCR. Autofluorescence images did not demonstrate any obvious RPE damage from the laser. With the minimally invasive nature of modified LPM laser treatment, it might be applicable for leakage points near the fovea. Even for leakage far from the fovea, modified LPM laser treatment has the advantage over suprathreshold laser of avoiding complications, including retinal atrophy or choroidal neovascularization.2 Furthermore, our simple approach was based on manual adjustment of laser parameters, which can also be applied to other commonly used retinal laser systems. This general versatility is important for dissemination of subthreshold laser treatment.
There are several hypotheses about the cellular mechanism of subthreshold laser treatment for CSCR, including migration of RPE cells to restore the outer blood-retinal barrier5 and activation of RPE function.6 Expression of heat shock proteins after subthreshold laser treatment has been reported, and heat shock protein might enhance fluid pumping by the RPE cells.4,6 However, the experiments performed in those studies were unrelated to the treatment of CSCR; hence, the cellular mechanisms for the treatment of CSCR are still unclear. In this study, focal laser treatment for leakage was performed for CSCR by reference to previous studies,7,8 whereas other studies performed diffuse grid-pattern laser across the area of serous retinal detachment.4 The mechanisms of action leading to therapeutic benefits remain under debate.3 Thus, further studies are required to confirm the optimum protocol for modified LPM laser treatment of CSCR.
There are some other potential limitations of this case series. For example, the number of cases is small, with relatively short follow-up periods. Thus, more cases, with longer follow-up, are required to confirm the success and determine the recurrence rate when using modified LPM. Another limitation is the lack of a control group and, therefore, lack of randomization. The resolution of subretinal fluid might be part of the natural history of the disease process. In our case series, leakage points were located relatively far from the fovea, without diffuse leakage. To deal with the diverse spectrum of CSCR cases, further study is required with leakage points near the fovea, or with diffuse leakage area. The safety of the titration algorithm remains controversial,9 hence, further study is required to determine the optimum titration protocol. In addition, comparisons with other treatment options2 such as transpupillary thermotherapy, photodynamic therapy, micropulse laser and EndPoint Management will be important to confirm the clinical significance of our method.
Conclusion
In conclusion, this small case series suggests that modified LPM protocols can provide favorable treatment efficacy for persistent CSCR. Further studies are required to confirm the appropriate titration methods and to compare with other treatment options.
Abbreviations
RPE, retinal pigment epithelium; CSCR, central serous chorioretinopathy; LPM, low power mode.
Acknowledgments
The authors thank Hitoshi Abe from Nidek Co. for discussions regarding our patients.
Disclosure
Masahiro Miura reports grants from Alcon, fees for clinical trials from Allergan and Senju, grants from Novartis, grants from Santen, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82–118. doi:10.1016/j.preteyeres.2015.05.003
2. van Rijssen TJ, van Dijk EHC, Yzer S, et al. Central serous chorioretinopathy: towards an evidence-based treatment guideline. Prog Retin Eye Res. 2019;73:100770. doi:10.1016/j.preteyeres.2019.07.003
3. Wood EH, Karth PA, Sanislo SR, Moshfeghi DM, Palanker DV. Nondamaging retinal laser therapy for treatment of central serous chorioretinopathy: what is the evidence? Retina. 2017;37(6):1021–1033. doi:10.1097/IAE.0000000000001386
4. Lavinsky D, Wang J, Huie P, et al. Nondamaging retinal laser therapy: rationale and applications to the macula. Invest Ophthalmol Vis Sci. 2016;57(6):2488–2500. doi:10.1167/iovs.15-18981
5. Roider J, Michaud NA, Flotte TJ, Birngruber R. Response of the retinal pigment epithelium to selective photocoagulation. Arch Ophthalmol. 1992;110(12):1786–1792.
6. Sramek C, Mackanos M, Spitler R, et al. Non-damaging retinal phototherapy: dynamic range of heat shock protein expression. Invest Ophthalmol Vis Sci. 2011;52(3):1780–1787. doi:10.1167/iovs.10-5917
7. Koss MJ, Beger I, Koch FH. Subthreshold diode laser micropulse photocoagulation versus intravitreal injections of bevacizumab in the treatment of central serous chorioretinopathy. Eye (Lond). 2012;26(2):307–314. doi:10.1038/eye.2011.282
8. Gupta B, Elagouz M, McHugh D, Chong V, Sivaprasad S. Micropulse diode laser photocoagulation for central serous chorio-retinopathy. Clin Exp Ophthalmol. 2009;37(8):801–805. doi:10.1111/j.1442-9071.2009.02157.x
9. Gawęcki M. Micropulse laser treatment of retinal diseases. J Clin Med. 2019;8(2):242. doi:10.3390/jcm8020242
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.