")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Moderating role of self-efficacy on the associations of social support with depressive and anxiety symptoms in Chinese patients with rheumatoid arthritis
Received 16 March 2017
Accepted for publication 14 July 2017
Published 9 August 2017 Volume 2017:13 Pages 2141—2150
DOI https://doi.org/10.2147/NDT.S137233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Wai Kwong Tang
Li Liu,1 Neili Xu,2 Lie Wang1
1Department of Social Medicine, School of Public Health, China Medical University, 2Department of Rheumatology, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China
Purpose: Rheumatoid arthritis (RA) is significantly associated with depression and anxiety. Social support and self-efficacy are the coping resources of psychological distress. However, little research is available on the interaction of social support and self-efficacy in RA patients. This study aimed to identify the prevalence of depressive and anxiety symptoms and to examine whether or not self-efficacy moderates the associations of social support with depressive and anxiety symptoms in Chinese RA patients.
Methods: A multicenter, cross-sectional study was conducted in northeast of China from December 2014 to January 2016. A total of 297 RA patients completed the Center for Epidemiologic Studies Depression Scale, Zung Self-Rating Anxiety Scale, Multidimensional Scale of Perceived Social Support and General Self-Efficacy Scale. The associations of social support, self-efficacy and social support × self-efficacy interaction with depressive and anxiety symptoms were examined by hierarchical regression analysis. If the interaction was statistically significant, simple slope analysis was conducted.
Results: The prevalence of depressive symptoms was 58.2%, while 47.5% RA patients had anxiety symptoms. Social support and social support × self-efficacy interaction were significantly associated with depressive symptoms. Social support, self-efficacy and their interaction were significantly associated with anxiety symptoms. The association between social support and depressive symptoms was gradually reduced in the low (1 standard deviation [SD] below the mean, B=–0.614, β=–0.876, P<0.001), mean (B=–0.395, β=–0.563, P<0.001) and high (1 SD above the mean, B=–0.176, β=–0.251, P=0.002) groups of self-efficacy. For anxiety symptoms, the association was also gradually reduced in the low (B=–0.527, β=–0.774, P<0.001), mean (B=–0.288, β=–423, P<0.001) and high (B=–0.049, β=–0.071, P=0.447) groups of self-efficacy.
Conclusion: There was a high prevalence of depressive and anxiety symptoms in Chinese RA patients. Self-efficacy could attenuate the associations of social support with depressive and anxiety symptoms. Adequate social support and self-efficacy intervention should be provided to alleviate psychological distress.
Keywords: self-efficacy, social support, psychological distress, moderating role, rheumatoid arthritis
Introduction
As a common autoimmune disease, rheumatoid arthritis (RA) is mainly manifested as chronic, symmetric and progressive multi-arthritis that often leads to joint deformity and loss of function. It is often accompanied by extra-articular organ involvement, which can seriously damage the quality of life of patients.1 In reality, the long-term physical dysfunction of RA patients can result in psychological distress. Previous studies have mostly focused on depression and anxiety as poor mental health indicators. Specifically, the prevalence of subclinical depression in RA patients ranged from 33.8% to 44.7% across countries,2–4 while the prevalence of anxiety symptoms ranged from 13.4% to 33.7% worldwide based on different assessment scales.4–6 More importantly, these psychological disorders could lead to the increases in mortality and disability, reduced treatment response and poor compliance with treatment.7–10 Therefore, early screening and managing strategies may significantly reduce the adverse consequences of these psychological disorders in the patients.
Unsurprisingly, it is of great importance to identify the psychosocial factors of psychological distress in RA patients, and then, appropriate psychosocial inventions could be developed to modify them effectively. Social support, as a positive psychosocial factor, refers to the perception and/or actuality that individuals are cared for and have assistance available in times of need from three relationships in their supportive social networks, including family members, friends, colleagues and other communities in general.11 Typically, social support includes three basic levels, emotional, instrumental and informational, as a multidimensional concept. In the past 3 decades, the relationship between social support and mental health has been verified by empirical data.12–15 According to the “strain buffering hypothesis”,16 social support can act as a “direct agent” to strengthen individuals’ health and well-being. In addition, social support, as an “antecedent factor”, plays its positive effects on mental health by increasing patients’ psychological empowerment and positive coping styles. For example, the relationship between social support and depression was found to be mediated by appearance-related social anxiety and avoidance in RA patients.12 Moreover, as a “moderator”, social support may act as a coping strategy that helps patients to deal with stress and/or other threats to their psychological well-being. Dekkers et al13 reported that perceived support was a moderator of the relationship between daily hassles and psychological well-being in patients with recently diagnosed RA. In patients with short-term RA, disease-related factors and social support were important in determining psychological distress. In addition, a buffering effect of social companionship was found by Strating et al.14 The study of Benka et al15 showed that emotional support moderated the influence of functional disability on depressive feelings in patients with RA. There is strong empirical evidence that social support may have significant positive effect on psychological health in RA patients. Coupled with the deficiency often faced by RA patients in social support,17 it means that health care workers have sought ways to boost social support for their patients. However, the most intensive forms of social support are often difficult to provide for cost reasons. Therefore, further studies should be carried out to explore some positive psychological resources that on the one hand can directly improve the psychological well-being of patients with RA and on the other hand can reduce the dependence of RA patients on the positive effect of social support to develop effective intervention for psychological disorders in clinical practice.
In the past 3 decades, as an important psychological construct, self-efficacy has been attached increasing importance to play positive roles in clinical practice.18 According to the self-efficacy theory,19 first of all, self-efficacy can influence one’s behavior selection; second, when individuals have to face obstacles or painful experiences, self-efficacy determines the degree and duration of their efforts; third, self-efficacy influences people’s thinking pattern and emotional response pattern. Thus, self-efficacy can influence appraisal and coping processes and psychological symptoms in stressful transactions. In particular, general self-efficacy refers to the belief in one’s competence to cope with a broad range of stressful or challenging demands.20 Previous studies have reported that self-efficacy has direct positive effect on the psychological well-being of patients with RA.21 With lower self-efficacy, RA-related psychological symptoms such as depression and anxiety became more severe. In addition, lower self-efficacy was directly or indirectly significantly and negatively associated with physical and mental health-related quality of life among Chinese patients with RA.22 In addition, the positive link between social support and self-efficacy has been made clear. The mediating role of self-efficacy in the relationship between social support and its positive health-related outcomes has been confirmed widely in patients with chronic diseases.23,24 Moreover, self-efficacy can also act as a “moderator” to enhance or attenuate the effects of stressors and coping resources on psychological well-being. Yang et al25 found that self-efficacy moderated the relationships of persuasion/pressure with diabetes-related emotional distress and depressive symptoms among older adults with type 2 diabetes mellitus. Lowe et al also mentioned that self-efficacy, as an appraisal, may moderate the relationships between coping strategies and emotional outcomes. Among RA patients, the nature of associations between coping and emotional outcomes (depression and anxiety) was found to differ according to self-efficacy appraisals.26 In general, social support is considered as a potential resource for individuals dealing with stressful events. Therefore, self-efficacy seems like a relevant moderator on the associations between social support and depressive and anxiety symptoms in RA patients.
In view of the abovementioned statement, we put forward the hypothesis that the relationship between social support and mental health is weak for the RA patients with a high level of self-efficacy. In other words, the psychological well-being of these patients is less dependent on social support. This may have implications for clinical practice in that the adaptive significance of social support for psychological well-being may differ according to underlying self-efficacy in RA patients. To the best of our knowledge, in RA patients, no research has been conducted to evaluate the associations among social support, self-efficacy, and depressive and anxiety symptoms. Therefore, the objectives of this study were to identify the prevalence of depressive and anxiety symptoms in Chinese patients with RA and to examine whether or not self-efficacy moderates the associations of social support with depressive and anxiety symptoms.
Materials and methods
Study design and sample
A multicenter, cross-sectional study was carried out in successive inpatients diagnosed with RA from December 2014 through January 2016. All patients were recruited at the Department of Rheumatology at Shengjing Hospital of China Medical University, Central Hospital of Benxi, General Hospital of Fushun Mining Bureau and Sujiatun Central Hospital of Shenyang in Liaoning Province, northeastern China. The inclusion criteria included who 1) were diagnosed with RA on the basis of American College of Rheumatology/ European League Against Rheumatism 2010; 2) were at least 18 years or older and 3) could understand and communicate in Chinese well. The exclusion criteria included: 1) psychiatric history in the past; 2) intellectual and/or cognitive impairments and 3) suffering from some severe comorbidities simultaneously. All the eligible patients were requested to participate in the research voluntarily and anonymously by rheumatologists-in-charge. Participants were well informed about the objectives and procedures of the research. After obtaining their written informed consent for this study, a set of self-administered questionnaires was distributed to the participants, and clinical data were collected from their medical records. The protocol of research was inspected and authorized by the Committee on Human Experimentation of Shengjing Hospital of China Medical University, Central Hospital of Benxi, General Hospital of Fushun Mining Bureau, and Sujiatun Central Hospital of Shenyang and was in accordance with the ethical standards.
The minimum sample size was calculated before patient recruitment by the formula: n= (Zα/2)2P(1–P)/δ2. In the formula, α=0.05, Zα/2=1.96. P is the prevalence of depressive or anxiety symptoms in RA patients, which is estimated according to the results of previous studies and trial test. In this study, P=0.30. δ is tolerable error, and δ=0.06 in this study. Thus, we identified 224 as the minimum sample size for this study. There were 325 patients recruited as the potential subjects at the initial stage. In all, 12 patients refused to cooperate subsequently. Data with missing information concerning any item in the questionnaires were excluded from the final analysis. Thus, of the 313 eligible patients, 16 were excluded. In total, effective responses were received from 297 (91.4%) patients in this study.
Measurement of depressive symptoms
Depressive symptoms were measured with the Chinese version of the Center for Epidemiologic Studies Depression (CES-D) scale.27 The CES-D scale comprises 20 items, and each item includes 4-point Likert-type scale responses that describe the frequency of subjects’ feelings in the past week ranging from 0 (rarely or none of the time [less than 1 day]) to 3 (most or all of the time [5–7 days]). The summed score ranges from 0 to 60, with a higher score indicating more severe depressive symptoms. The presence of depressive symptoms was defined as a CES-D score ≥16. The Chinese CES-D scale has been widely used in previous studies.28,29 The Cronbach’s α coefficient for the CES-D scale was 0.90 in the present study.
Measurement of anxiety symptoms
Anxiety symptoms were measured with the Chinese version of the Zung Self-Rating Anxiety Scale (SAS).30 The SAS consists of 20 items, and each item is answered on a 4-point Likert-type scale responses ranging from 1 (never) to 4 (always). The summed raw score is standardized according to the formula: standardized score = int (1.25× raw score). A higher score means more severe anxiety symptoms. The presence of anxiety symptoms was defined as an SAS standardized score ≥50. The Chinese SAS has been extensively applied and validated among Chinese patients.6,28,29 In this study, the Cronbach’s α coefficient for the SAS was 0.82.
Measurement of social support
The Chinese version of the Multidimensional Scale of Perceived Social Support (MSPSS) was utilized to measure the level of social support.31 The 12-item MSPSS measures perceived support from three social relationships: family, friends and significant others (such as relatives and colleagues). The score of each item is given on a 7-point Likert-type scale in accordance with the patients’ personal experiences, ranging from 1 (very strongly disagree) to 7 (very strongly agree). The total score ranges from 12 to 84, with a higher score indicating higher social support. The MSPSS has good reliability and validity among various Chinese patients.28,32 In the present study, the Cronbach’s α coefficient for the scale was 0.95.
Measurement of self-efficacy
Self-efficacy was measured with the Chinese version of General Self-Efficacy Scale (GSES),20 which was widely used among patients in China.33,34 The GSES comprises 10 items, and each item includes 4-point Likert-type scale responses in accordance with the respondents’ personal perception ranging from 1 (completely incorrect) to 4 (completely correct). The summed score of GSES is from 10 to 40, and a higher score means higher self-efficacy. The Cronbach’s α coefficient for the GSES was 0.76 in the present study.
Demographic characteristics
In this study, demographic characteristics included age, gender, marital status, educational level, employment, household monthly income and residence. Marital status was categorized as married/cohabited and single/divorced/widowed/separated. Educational level was classified as junior high school or below, senior high school and junior college or above. Employment was divided into three groups as unemployment, part time and full time. Household monthly income (RMB) was categorized as <4,000 and ≥4,000 yuan. Residence was categorized as urban or rural.
Clinical variables
Clinical variables including duration of suffering from RA, anemia, early morning stiffness (EMS), tender joint counts (TJC), swollen joint counts (SJC), C-reactive protein (CRP), and other chronic comorbidities were collected in this study. The duration of suffering RA was classified as: 1, 2–5, 6–10 and >10 years. Anemia was categorized as yes or no. EMS was divided into three groups: no, ≤1 and >1 hour. The value of Disease Activity Score 28 (DAS28)-CRP was calculated to indicate the disease activity of RA patients. On the basis of TJC, SJC and CRP, DAS28-CRP was calculated according to the formula: DAS28-CRP =[0.56×sqrt (TJC28)+0.28×sqrt(SJC28)+0.36×ln(CRP+1)]×1.10+1.15. If the respondents were suffering from some severe comorbidities, such as osteoarthritis, sclerosis, hypertension, coronary heart disease, diabetes, or other chronic comorbidity, it was defined as “yes”; otherwise, it was categorized as “no”.
Statistical analysis
The demographic, clinical and psychological variables were described with mean, standard deviation (SD), number (n) and percentage (%) as appropriate. Group differences of continuous variables were examined using independent sample t-test or one-way ANOVA. Pearson’s correlation was used to examine correlations among continuous variables. Hierarchical regression analysis was applied to examine the associations of social support and self-efficacy with depressive and anxiety symptoms as well as to explore the moderating roles of self-efficacy on the associations of social support with depressive and anxiety symptoms, respectively. Besides age and gender, the demographic and clinical variables related to depressive and anxiety symptoms in univariate analysis (P<0.15) were adjusted. In step 1, age, gender, and potential control variables were added. Social support and self-efficacy were added in step 2. Ultimately, the product of social support and self-efficacy was added in step 3. If the interaction effect was statistically significant, simple slope analysis was conducted to visualize the interaction term.35 The variables in the models were centralized before regression analysis. Statistical analysis was carried out by SPSS 19.0 software, and a two-tailed P-value <0.05 was viewed as statistically significant.
Results
Descriptive statistics
Demographic and clinical characteristics and group differences in depressive and anxiety symptoms are displayed in Table 1. Of these subjects, 87.9% (261) were married/cohabited, and they reported lower depressive symptoms (t=3.027, P=0.003) and anxiety symptoms (t=2.651, P=0.008) than those of single/divorced/widowed/separated subjects. There were 65.6% (195) subjects with a senior high school or above education, and 61.3% (182) subjects were unemployed. In all, 230 (77.4%) subjects had a household monthly income level of <4,000 yuan RMB, and they had a higher level of depressive symptoms compared with patients who had a household monthly income level of ≥4,000 yuan RMB (t=2.011, P=0.045). With regard to clinical variables, 193 (65.0%) subjects with at least one other chronic disease reported higher depressive symptoms than those without comorbidities (t=2.097, P=0.037).
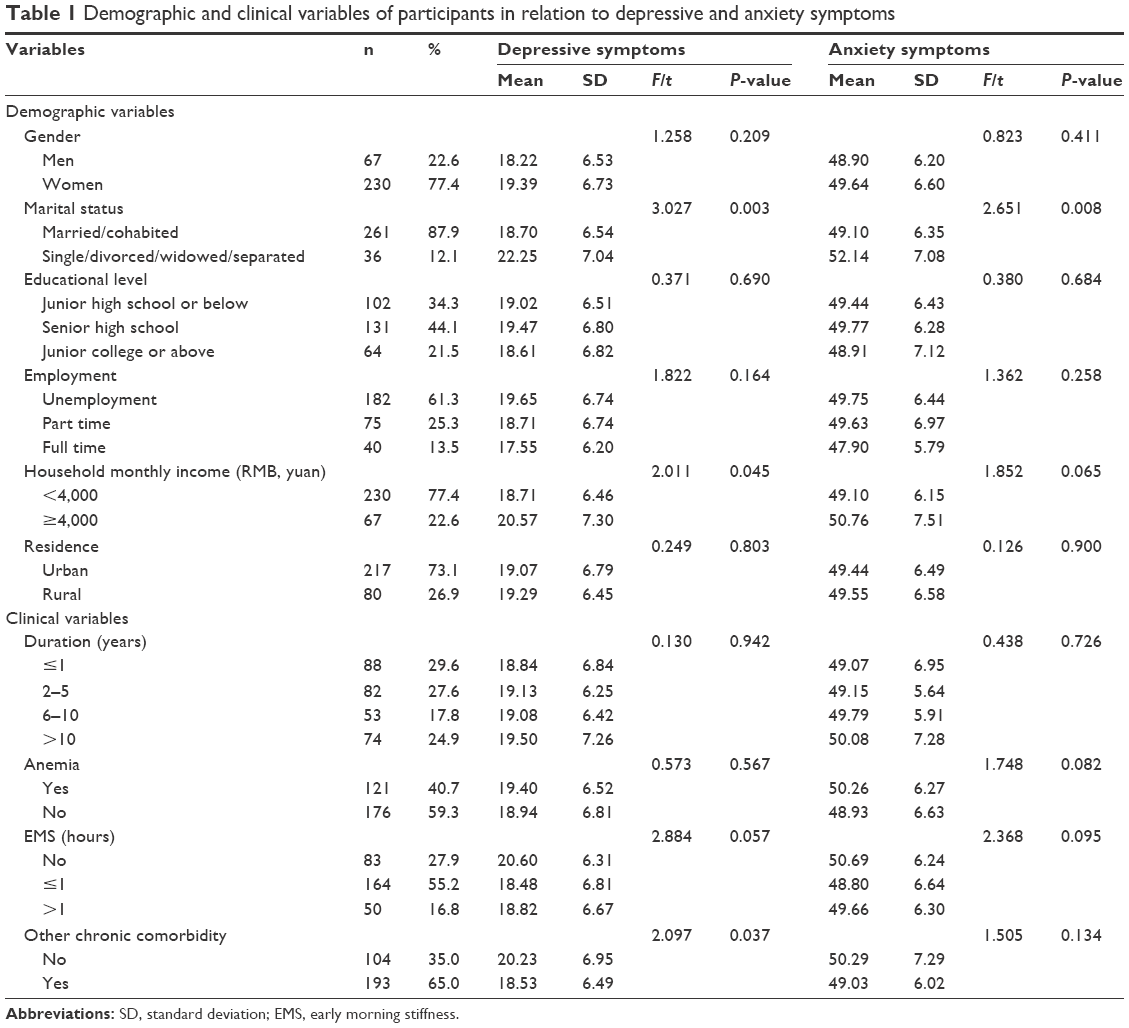 | Table 1 Demographic and clinical variables of participants in relation to depressive and anxiety symptoms |
The levels of depressive and anxiety symptoms, age, DAS28-CRP, social support and self-efficacy are provided in Table 2. The mean score of depressive symptoms was 19.13 (SD =6.69). Based on the cutoff value of 16, the prevalence of depressive symptoms in RA patients was 58.2%. The mean score of anxiety symptoms was 49.47 (SD =6.51). Based on the cutoff value of 50, the prevalence of anxiety symptoms in RA patients was 47.5%.
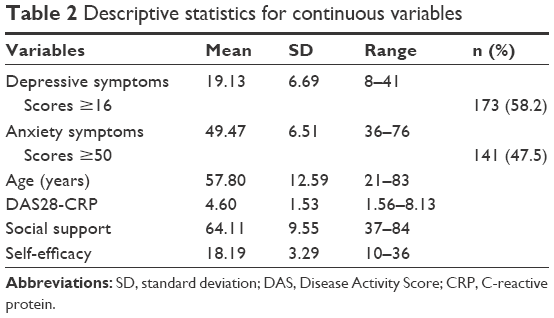 | Table 2 Descriptive statistics for continuous variables |
Correlations among continuous variables
The correlations among age, DAS28-CRP, social support, self-efficacy, depressive and anxiety symptoms are displayed in Table 3. Both depressive and anxiety symptoms were positively correlated with age and DAS28-CRP but negatively correlated with social support and self-efficacy. In addition, age was negatively correlated with social support and self-efficacy, and social support was positively correlated with self-efficacy.
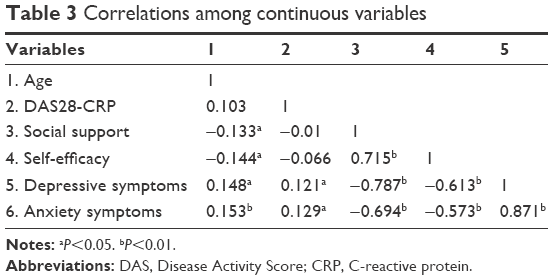 | Table 3 Correlations among continuous variables |
Hierarchical regression analyses
The results of hierarchical regression analyses are displayed in Tables 4 and 5 for depressive and anxiety symptoms, respectively. In the first step, the linear combination of demographic and clinical control variables (gender, age, marital status, household monthly income, anemia, EMS, DAS28-CRP, and other chronic comorbidity) significantly explained depressive symptoms (F=5.614, adjusted R2=0.123, P<0.01) and anxiety symptoms (F=4.890, adjusted R2=0.106, P<0.01). In the second step, adding social support and self-efficacy improved the model fits of depressive symptoms (F=50.888, adjusted R2=0.650, ΔR2=0.512, P<0.01) and anxiety symptoms (F=29.238, adjusted R2=0.512, ΔR2=0.397, P<0.01). Social support exhibited significant main effects on depressive symptoms (B=−0.484, β=−0.691, P<0.001) and anxiety symptoms (B=−0.386, β=−0.566, P<0.001), and self-efficacy exhibited a significant main effect on anxiety symptoms (B=−0.253, β=−0.128, P=0.030) only. For the depressive symptoms model, the social support × self-efficacy interaction term significantly explained an additional 4.9% of the variance (F=58.427, adjusted R2=0.700, ΔR2=0.049, P<0.01) in the third step. The interaction term was positively associated with depressive symptoms (B=0.066, β=0.244, P<0.001). Simple slope analysis revealed that when self-efficacy is higher, the association between social support and depressive symptoms becomes weaker. In other words, the associations between social support and depressive symptoms were gradually reduced in the low (1 SD below the mean, B=−0.614, β=−0.876, P<0.001), mean (B=−0.395, β=−0.563, P<0.001) and high (1 SD above the mean, B=−0.176, β=−0.251, P=0.002) groups of self-efficacy. The interaction is visualized in Figure 1. For the anxiety symptoms model, the interaction term also significantly explained an additional 6.2% of the variance (F=34.378, adjusted R2=0.575, ΔR2=0.062, P<0.01) in the third step. The interaction term was positively associated with anxiety symptoms (B=0.073, β=0.275, P<0.001). Simple slope analysis revealed that the associations between social support and anxiety symptoms were gradually reduced in the low (1 SD below the mean, B=−0.527, β=−0.774, P<0.001), mean (B=−0.288, β=−423, P<0.001) and high (1 SD above the mean, B=−0.049, β=−0.071, P=0.447) groups of self-efficacy. The interaction is visualized in Figure 2.
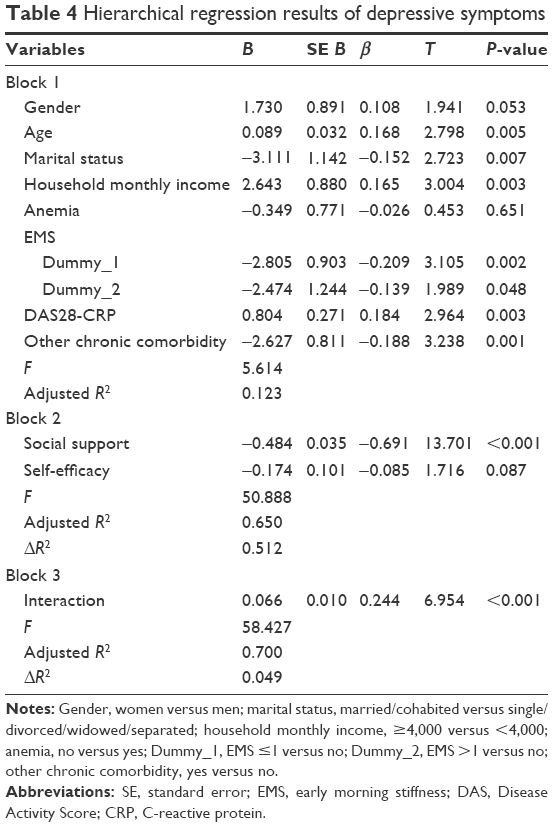 | Table 4 Hierarchical regression results of depressive symptoms |
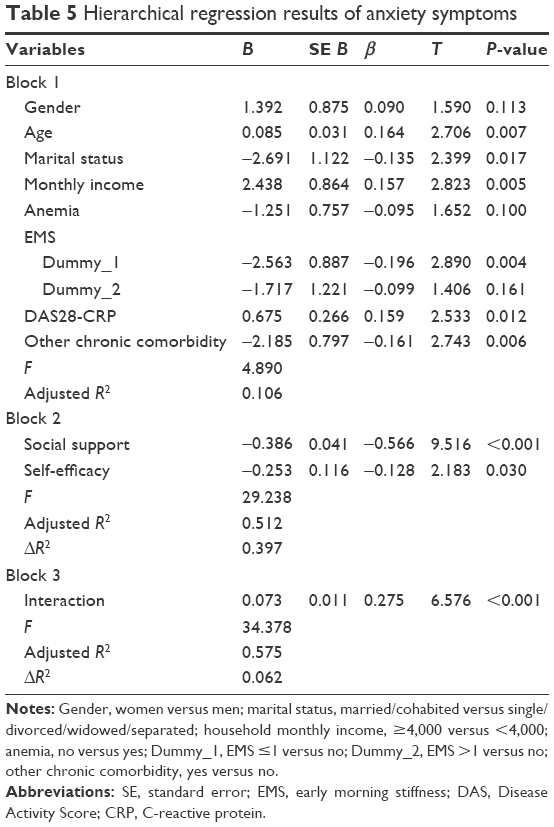 | Table 5 Hierarchical regression results of anxiety symptoms |
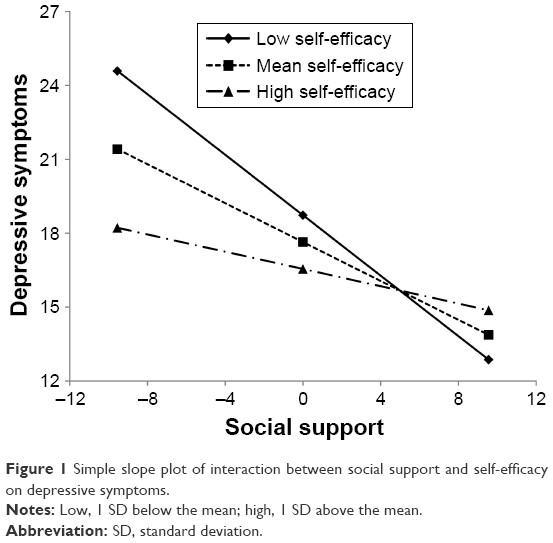 | Figure 1 Simple slope plot of interaction between social support and self-efficacy on depressive symptoms. |
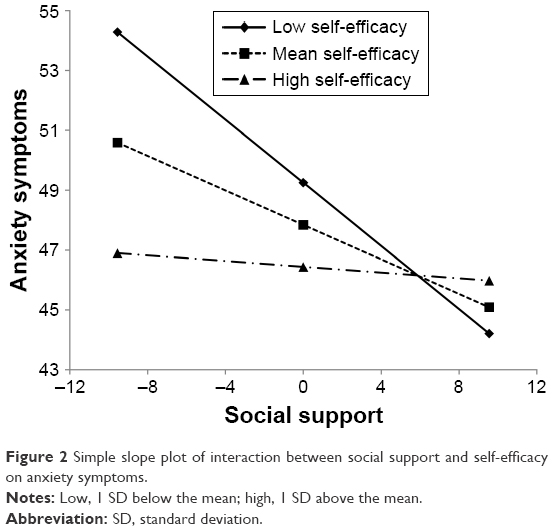 | Figure 2 Simple slope plot of interaction between social support and self-efficacy on anxiety symptoms. |
Discussion
This study investigated the prevalence of depressive and anxiety symptoms among Chinese RA patients. Almost 60% of the RA patients suffered from depressive symptoms, while ~50% suffered from anxiety symptoms. The mean level of depressive symptoms measured by the CES-D scale in this study was higher than that of RA patients in most previous studies across countries.36–39 In addition, the prevalence of depressive symptoms was 58.2% in this study, and it was higher than that of RA patients from previous studies mentioned earlier.36,37 In the present study, the mean level of anxiety symptoms measured by the Zung SAS was higher than that of RA patients in most previous studies from China.6,40 As a result, the prevalence of anxiety symptoms (47.5%) in this study was higher than that of RA patients from these previous studies.4–6,40 Moreover, although no patients suffering from other diseases were selected as control groups in this study, the scores of depressive and anxiety symptoms are considered to be at a medium–high level relative to the results of previous studies carried out in other patient populations.29,33,41 Therefore, the psychological disorders’ symptoms should be attached great importance in RA patients, and efforts should be done to reduce depressive and anxiety symptoms.
Among demographic and clinical variables, age, marital status, household monthly income, EMS, DAS28-CRP and chronic comorbidity were associated with depressive and anxiety symptoms. However, gender, education, employment, residence and duration of suffering from RA were not related to depressive and anxiety symptoms in univariate analyses. Thus, they were not adjusted in the following hierarchical regression analyses. These associations have been explored in previous studies.42–44 Understanding the demographic and clinical causes of depression and anxiety can facilitate a comprehensive pattern for targeting interventions in RA patients.
We found that, consistent with the findings of previous studies, social support was a positive coping resource both for depressive and anxiety symptoms in Chinese RA patients. Compared with RA patients who possessed adequate social support, those who could not seek help from their social networks suffered from more severe symptoms of psychological disorders.12–15 RA is often considered as a disease that only has a slightly threatening, and it is not obviously visible to others.45 However, RA is factually incurable with a prolonged course, even deformity and physical disability.17 As a result, the chance of obtaining social support could be reduced when the patients deal with the symptoms of RA.46 Conversely, the perceptions of social support may be confounded by depressive symptoms.47,48 Khalil and Abed48 found that depressive symptoms resulted in poor quality of life through reducing perceived social support in patients with end-stage renal disease. In a word, social support should be an important resource for managing psychological symptoms in RA patients. In addition to social support, self-efficacy was correlated with both depressive and anxiety symptoms in univariate analysis in this study. However, it was only significantly associated with anxiety symptoms, but not associated with depressive symptoms after controlling for other factors. One reason of this result may be the symptomatic distinctions of depressive and anxiety symptoms.49 Depressive symptoms mainly include sadness, hopelessness and worthlessness, whereas anxiety symptoms basically include worry, fear and avoidance. Reasonably, the belief in one’s competence to cope with a broad range of stressful or challenging demands is considered as one of the most important coping resources for overcoming anxiety. Some previous studies reported that patients with a higher level of self-efficacy suffered from less severity of psychological disorders’ symptoms than RA patients.21,22 Therefore, further research could be conducted to explore its exact effect in RA-related psychological disorders.
To our knowledge, this study was the first to explore the moderating role of self-efficacy on the association between social support and psychological disorders’ symptoms in RA patients. We hypothesized that self-efficacy might weaken the associations of social support with depressive and anxiety symptoms. We have found that self-efficacy and social support interact with each other in their associations with depressive and anxiety symptoms. This may indicate that if more self-efficacy is present, RA patients can better maintain their mental health at a lower social support level, possibly because these RA patients feel more other positive psychological resources, such as optimism and resilience. The finding that self-efficacy moderated the associations between social support and depressive and anxiety symptoms was somewhat similar to an earlier study regarding moderation of associations of perceived social and physical environmental correlates with physical activity in older adolescents by self-efficacy.50 Consistent with Lowe et al,26 the findings highlighted contributions to these psychological disorders’ symptoms from interactions between coping resources and self-efficacy. Moreover, psychological resources should be hypothesized to moderate the association between extrinsic resource and mental health in general. Although certain coping strategies can alleviate stress and promote positive psychological outcomes, the efficacy of the coping strategy depends on the personal psychological resources of subjects, such as self-efficacy and resilience.26,51 Therefore, self-efficacy, as a modifiable factor, should be improved by effective interventions in RA patients for coping with mental health problems. The application of self-efficacy theory to arthritis self-management intervention has been widely developed, which consistently has shown significant early and sustained benefits that are attributed to the change in self-efficacy.52 Both group-based and individual-based educational programs with various modalities, such as face to face, telephone and internet, were successfully explored in the past 3 decades.53–55 Cognitive-behavioral approach was used to enhance patient’s self-efficacy in these educational intervention programs. Specifically, four primary strategies have been suggested in clinical practice: 1) identify and facilitate patient’s performance accomplishments or skills mastery; 2) guide patient to observe vicarious experiences; 3) give social and verbal persuasion and 4) pay attention to patient’s physiological and emotional states.52,56 A group-based and face-to-face self-efficacy-enhancing intervention should be introduced by clinicians or nurses for the RA patients of this study.
However, several limitations should be illustrated in the present study. First, the cross-sectional design was unable to assess the causal relationships among study variables in this study and only provided a snapshot of depressive and anxiety symptoms that were experienced by the RA patients at the time of the survey. Therefore, longitudinal data should be achieved further to verify our findings. Second, psychosocial variables were mainly measured using self-report questionnaires. Owing to possible recall and reporting bias, the associations among the psychosocial variables might be confounded. The possibility of common-method bias has been minimized using some effective process control measures. Third, the sample of this study was recruited from a province of northeast China. Thus, the generalization of our findings should be further confirmed in other populations.
Conclusion
There was a high prevalence of depressive and anxiety symptoms in Chinese RA patients. Social support was negatively associated with depressive and anxiety symptoms, and self-efficacy was only negatively associated with anxiety symptoms. Self-efficacy could attenuate the associations of social support with depressive and anxiety symptoms. In addition to providing adequate social support, self-efficacy intervention should be integrated into the prevention and treatment strategies of depressive and anxiety symptoms among RA patients.
Acknowledgment
The authors would like to thank all the inpatients who voluntarily participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. | ||
Yang C, Wang J, Sun C, Zhang Q. The prevalence of depression in adult rheumatoid arthritis patients in China: a meta-analysis. Chin J Rheumatol. 2015;19(10):662–668. | ||
Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2013;52(12):2136–2148. | ||
Zhang L, Xia Y, Zhang Q, et al. The correlations of socioeconomic status, disease activity, quality of life, and depression/anxiety in Chinese patients with rheumatoid arthritis. Psychol Health Med. 2017;22(1):28–36. | ||
Isik A, Koca SS, Ozturk A, Mermi O. Anxiety and depression in patients with rheumatoid arthritis. Clin Rheumatol. 2007;26(6):872–878. | ||
Guo J, Li L, Yang J. Investigation and analysis of anxiety and depression of patients with rheumatoid arthritis. Rheum Arthritis. 2012;1(3):28–29. | ||
van den Hoek J, Boshuizen HC, Roorda LD, et al. Association of somatic comorbidities and comorbid depression with mortality in patients with rheumatoid arthritis: a 14-year prospective cohort study. Arthritis Care Res (Hoboken). 2016;68(8):1055–1060. | ||
Ormseth SR, Draper TL, Irwin MR, et al. Multidimensional model of disability and role functioning in rheumatoid arthritis. Arthritis Care Res (Hoboken). 2015;67(12):1686–1692. | ||
Matcham F, Norton S, Scott DL, Steer S, Hotopf M. Symptoms of depression and anxiety predict treatment response and long-term physical health outcomes in rheumatoid arthritis: secondary analysis of a randomized controlled trial. Rheumatology (Oxford). 2016;55(2):268–278. | ||
Xia Y, Yin R, Fu T, et al. Treatment adherence to disease-modifying antirheumatic drugs in Chinese patients with rheumatoid arthritis. Patient Prefer Adherence. 2016;10:735–742. | ||
Gottlieb BH, Bergen AE. Social support concepts and measures. J Psychosom Res. 2010;69(5):511–520. | ||
McBain H, Shipley M, Newman S. Appearance Research Collaboration (ARC). The impact of appearance concerns on depression and anxiety in rheumatoid arthritis. Musculoskeletal Care. 2013;11(1):19–30. | ||
Dekkers JC, Geenen R, Evers AW, Kraaimaat FW, Bijlsma JW, Godaert GL. Biopsychosocial mediators and moderators of stress-health relationships in patients with recently diagnosed rheumatoid arthritis. Arthritis Rheum. 2001;45(4):307–316. | ||
Strating MM, Suurmeijer TP, van Schuur WH. Disability, social support, and distress in rheumatoid arthritis: results from a thirteen-year prospective study. Arthritis Rheum. 2006;55(5):736–744. | ||
Benka J, Nagyova I, Rosenberger J, et al. Social support as a moderator of functional disability’s effect on depressive feelings in early rheumatoid arthritis: a four-year prospective study. Rehabil Psychol. 2014;59(1):19–26. | ||
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. | ||
Kostova Z, Caiata-Zufferey M, Schulz PJ. The impact of social support on the acceptance process among RA patients: a qualitative study. Psychol Health. 2014;29(11):1283–1302. | ||
Schönfeld P, Preusser F, Margraf J. Costs and benefits of self-efficacy: differences of the stress response and clinical implications. Neurosci Biobehav Rev. 2017;75:40–52. | ||
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. | ||
Luszczynska A, Scholz U, Schwarzer R. The general self-efficacy scale: multicultural validation studies. J Psychol. 2005;139(5):439–457. | ||
Gong G, Mao J. Health-related quality of life among Chinese patients with rheumatoid arthritis: the predictive roles of fatigue, functional disability, self-efficacy, and social support. Nurs Res. 2016;65(1):55–67. | ||
Barlow JH, Cullen LA, Rowe IF. Educational preferences, psychological well-being and self-efficacy among people with rheumatoid arthritis. Patient Educ Couns. 2002;46(1):11–19. | ||
Wang Y, Bao Y, Liu L, Ramos A, Wang Y, Wang L. The mediating effect of self-efficacy in the relationship between social support and post-traumatic stress disorder symptoms among patients with central system tumors in China: a cross-sectional study. Psychooncology. 2015;24(12):1701–1707. | ||
Maeda U, Shen BJ, Schwarz ER, Farrell KA, Mallon S. Self-efficacy mediates the associations of social support and depression with treatment adherence in heart failure patients. Int J Behav Med. 2013;20(1):88–96. | ||
Yang F, Pang JS, Cheng WJ. Self-care adherence and psychological functioning of older patients with type 2 diabetes: effects of persuasion, social pressure, and self-efficacy. J Clin Psychol Med Settings. 2016;23(4):389–401. | ||
Lowe R, Cockshott Z, Greenwood R, et al. Self-efficacy as an appraisal that moderates the coping-emotion relationship: associations among people with rheumatoid arthritis. Psychol Health. 2008;23(2):155–174. | ||
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. | ||
Yang YL, Liu L, Li MY, Shi M, Wang L. Psychological disorders and psychosocial resources of patients with newly diagnosed bladder and kidney cancer: a cross-sectional study. PLoS One. 2016;11(5):e0155607. | ||
Li M, Wang L. The associations of psychological stress with depressive and anxiety symptoms among Chinese bladder and renal cancer patients: the mediating role of resilience. PLoS One. 2016;11(4):e0154729. | ||
Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. | ||
Dahlem NW, Zimet GD, Walker RR. The Multidimensional Scale of perceived social support: a confirmation study. J Clin Psychol. 1991;47(6):756–761. | ||
Liu L, Yang YL, Wang ZY, Wu H, Wang Y, Wang L. Prevalence and positive correlates of posttraumatic stress disorder symptoms among Chinese patients with hematological malignancies: a cross-sectional study. PLoS One. 2015;10(12):e0145103. | ||
Wang ZY, Liu L, Shi M, Wang L. Exploring correlations between positive psychological resources and symptoms of psychological distress among hematological cancer patients: a cross-sectional study. Psychol Health Med. 2016;21(5):571–582. | ||
Yang YL, Liu L, Wang XX, Wang Y, Wang L. Prevalence and associated positive psychological variables of depression and anxiety among Chinese cervical cancer patients: a cross-sectional study. PLoS One. 2014;9(4):e94804. | ||
Hayes AF. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: Guilford Press; 2013. | ||
Goes AC, Reis LA, Silva MB, Kahlow BS, Skare TL. Rheumatoid arthritis and sleep quality. Rev Bras Reumatol. 2017;57(4):294–298. | ||
Sato E, Nishimura K, Nakajima A, et al. Major depressive disorder in patients with rheumatoid arthritis. Mod Rheumatol. 2013;23(2):237–244. | ||
Fusama M, Miura Y, Yukioka K, et al. Psychological state is related to the remission of the Boolean-based definition of patient global assessment in patients with rheumatoid arthritis. Mod Rheumatol. 2015;25(5):679–682. | ||
Taylor-Gjevre RM, Gjevre JA, Nair B, Skomro R, Lim HJ. Components of sleep quality and sleep fragmentation in rheumatoid arthritis and osteoarthritis. Musculoskeletal Care. 2011;9(3):152–159. | ||
Zhang G, Zhao MS, Xia RH, Wang YH, Zhang GH. Relationship between oxidative stress and depression in patients with rheumatoid arthritis. Beijing Da Xue Xue Bao. 2012;44(2):199–203. | ||
Lou Z, Li Y, Yang Y, Wang L, Yang J. Affects of anxiety and depression on health-related quality of life among patients with benign breast lumps diagnosed via ultrasonography in China. Int J Environ Res Public Health. 2015;12(9):10587–10601. | ||
Ho RC, Fu EH, Chua AN, Cheak AA, Mak A. Clinical and psychosocial factors associated with depression and anxiety in Singaporean patients with rheumatoid arthritis. Int J Rheum Dis. 2011;14(1):37–47. | ||
el-Miedany YM, el-Rasheed AH. Is anxiety a more common disorder than depression in rheumatoid arthritis? Joint Bone Spine. 2002;69(3):300–306. | ||
Katz PP, Yelin EH. Prevalence and correlates of depressive symptoms among persons with rheumatoid arthritis. J Rheumatol. 1993;20(5):790–796. | ||
Tiwana R, Rowland J, Fincher M, Raza K, Stack RJ. Social interactions at the onset of rheumatoid arthritis and their influence on help-seeking behaviour: a qualitative exploration. Br J Health Psychol. 2015;20(3):648–661. | ||
Brandstetter S, Riedelbeck G, Steinmann M, Ehrenstein B, Loss J, Apfelbacher C. Pain, social support and depressive symptoms in patients with rheumatoid arthritis: testing the stress-buffering hypothesis. Rheumatol Int. 2017;37(6):931–936. | ||
Maher MJ, Mora PA, Leventhal H. Depression as a predictor of perceived social support and demand: a componential approach using a prospective sample of older adults. Emotion. 2006;6(3):450–458. | ||
Khalil AA, Abed MA. Perceived social support is a partial mediator of the relationship between depressive symptoms and quality of life in patients receiving hemodialysis. Arch Psychiatr Nurs. 2014;28(2):114–118. | ||
Liu L, Pang R, Sun W, et al. Functional social support, psychological capital, and depressive and anxiety symptoms among people living with HIV/AIDS employed full-time. BMC Psychiatry. 2013;13:324. | ||
Deforche B, Van Dyck D, Verloigne M, De Bourdeaudhuij I. Perceived social and physical environmental correlates of physical activity in older adolescents and the moderating effect of self-efficacy. Prev Med. 2010;50(suppl 1):S24–S29. | ||
Smith MM, Saklofske DH, Keefer KV, Tremblay PF. Coping strategies and psychological outcomes: the moderating effects of personal resiliency. J Psychol. 2016;150(3):318–332. | ||
Marks R, Allegrante JP, Lorig K. A review and synthesis of research evidence for self-efficacy-enhancing interventions for reducing chronic disability: implications for health education practice (part II). Health Promot Pract. 2005;6(2):148–156. | ||
Shigaki CL, Smarr KL, Siva C, Ge B, Musser D, Johnson R. RAHelp: an online intervention for individuals with rheumatoid arthritis. Arthritis Care Res (Hoboken). 2013;65(10):1573–1581. | ||
Ndosi M, Johnson D, Young T, et al. Effects of needs-based patient education on self-efficacy and health outcomes in people with rheumatoid arthritis: a multicentre, single blind, randomised controlled trial. Ann Rheum Dis. 2016;75(6):1126–1132. | ||
Deng W, Hu J. The effects of a pilot intervention for community-dwelling adults with rheumatoid arthritis in Wuhan, China. Front Public Health. 2013;1:43. | ||
Allegrante JP, Marks R. Self-efficacy in management of osteoarthritis. Rheum Dis Clin North Am. 2003;29(4):747–768. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.