")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Moderate to Severe Diarrhea and Associated Factors Among Under-Five Children in Wonago District, South Ethiopia: A Cross-Sectional Study
Authors Tesfaye TS , Magarsa AU, Zeleke TM
Received 9 June 2020
Accepted for publication 4 September 2020
Published 19 October 2020 Volume 2020:11 Pages 437—443
DOI https://doi.org/10.2147/PHMT.S266828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Tinsae Shemelise Tesfaye,1 Abowak Ulfata Magarsa,2 Tadesse Mekonen Zeleke3
1Department of Public Health, College of Health Science and Medicine, Dilla University, Dilla, Ethiopia; 2Primary Health Care Unit, Adegalchati Health Center, Elwaye, Ethiopia; 3Food Science, and Nutrition Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia
Correspondence: Tinsae Shemelise Tesfaye
Department of Public Health, College of Health Science and Medicine, Dilla University, Dilla, Ethiopia
Tel +251910644517
Email [email protected]
Background: Diarrheal disease is the second leading cause of death in children under five years old and is responsible for killing around 525 000 children every year. Based on the world health organization estimates, diarrhea contributes to more than one in every ten (13%) child deaths in Ethiopia. Despite the emphasis given to improving child health, many children are still dying due to easily preventable and treatable diarrheal disease in Ethiopia.
Methods: A community cross-sectional study was conducted on randomly selected under-five children who live in Wonago district. Three hundred eighteen households were selected using a systematic sampling technique. Data were collected using a structured closed-ended questionnaire. Data were cleaned, coded, and entered into the statistical package for social sciences window version 20 statistical software analysis.
Results: The magnitude of moderate to severe diarrhea in the Wonago district was 30.9%. The number of family members (AOR: 2.7, 95% CI [1.277– 5.716]), presence of animals in households (AOR: 2.591, 95% CI [1.188– 5.650]), availability of latrine (AOR: 2.129, 95% CI [1.006– 4.505]), and hand washing practice during a critical time (AOR: 2.683, 95% CI [1.139– 6.319]) were strongly associated with moderate to severe diarrhea.
Conclusion: Childhood diarrhea remains an important health concern in the study area. This calls for a holistic and multimodal approach for the prevention, early identification, and intervention of diarrhea in children. More emphasis should also be given on personal, household, and environmental hygiene, as well as family planning.
Keywords: diarrhea, children, South, Wonago, Ethiopia
Introduction
In 2015, 5.9 million children died before reaching their fifth birthday. Of these 5.9 million deaths, diarrhea was responsible for 9%, making the disease the second leading cause of children worldwide. Together with pneumonia, it claimed the lives of nearly 1.5 million children under the age of 5 in a single year.1,2
Diarrhea mortality in young children continues to be disproportionately concentrated in a few countries. Even though they are home to only 55% of the world’s under-5 population, 72% of the global burden of diarrhea child deaths occur in just 15 countries.1–3 Diarrhea mortality disproportionately affects the youngest children; 70% of deaths associated with diarrhea occur during the first two years of life, and it can compromise health more broadly by leading to a vicious cycle of malnutrition, stunted growth, cognitive impairment, and poor immune response. Also, treatments for the illness can cause serious financial difficulties, contributing to the cycle of poverty.4
There has already been substantial progress in reducing diarrhea-related mortality. Deaths have dropped more significantly since 2000, falling from 1.2 million to 526,000 in 2015, which is a decline of 57%. The Integrated Global Action Plan for Pneumonia and Diarrhea (GAPPD) sets forth strategies and solutions for reducing the burden of these diseases by 2025 to reduce mortality from diarrhea in children less than five years of age to less than 1 death per 1000 live births. While diarrhea and pneumonia deaths have declined over the past decade, they still kill more children than all other infectious diseases combined. Continued lack of action on diarrhea will prevent many countries from achieving the new sustainable development health goals by 2030.5
Diarrhea is one of the major contributors to younger children’s deaths in Ethiopia. Based on the WHO estimates, diarrhea contributes to more than one in every ten (13%) child deaths in Ethiopia. Diarrhea is the 3rd most cause of mortality in under-five children in Ethiopia.6 According to the Ethiopia Demographic and Health Surveys (EDHS) of 2016, 13% of children aged < five had diarrhea. Similarly, this report showed that in the southern nation’s nationalities and people region 16.3% of children under the age of five had diarrhea, which had the highest prevalence of diarrhea in the county next to Benishangul-Gumuz and Gambela.7
Different studies in Ethiopia showed that socioeconomic status, number of children, methods of complementary feeding, types of water storage equipment, mother’s poor hand-washing practices, lack of hand-washing facilities, duration of breastfeeding, and improper waste disposal practices are significant factors for diarrhea occurrence.8
Despite the emphasis given by the Ethiopian Ministry of Health and the respective regional health offices to improve child health, many children are still dying due to easily preventable and treatable diarrheal disease in Ethiopia. Identifying the contributing factors of diarrhea is very important for the effective implementation of child health programs and prioritizations. In addition, there is a considerable variation in prevalence and determinant factors for diarrhea occurrence in Ethiopia. Therefore, this study aimed to assess the prevalence and associated factors of diarrheal diseases among children under the age of 5 years in Wonago district, South, Ethiopia.
Methods
Study Area and Setting
A community-based cross-sectional study was conducted in Wonago district, Gedeo zone, Southern Ethiopia, located 377 km to the south of Addis Ababa. The district is well known for being the most densely populated area in the country and having the highest total fertility rate. The district has 21 kebeles (the smallest local administrative classification in Ethiopia), of which 17 kebeles are rural administration and 4 are semiurban. This study was conducted from 1 October 2018 to 30 May 2019.
Source and Study Population
All under-five children who lived in the study area were the source population and the study population of the study was randomly selected under-five children who lived in Wonago district.
Eligibility Criteria
Inclusion Criteria
All under-five children lived in the study area for at least 6 months.
Exclusion Criteria
Children who were chronically ill and with persistent diarrhea for greater than two weeks were excluded.
Critically ill mothers or guardians of the selected children were excluded.
Sample Size Calculation
The sample size was determined using a single population proportion formula by considering these assumptions: p = 27% (prevalence of diarrhea and associated factors among under-five children in Jigjiga District9), 95% confidence interval, and 5% margin of error (d)
With the above parameters, the maximum sample size required was 303 and taking 5% contingency the final sample size was 318.
Sampling Technique
A multi-stage sampling technique was applied. There are 20 Kebele in the Wonago district and we stratified them into rural and urban kebeles. One urban and five rural kebeles were selected by simple random sampling using the lottery method. The study participants were selected by systematic random sampling. The total number of under-five children households was 2145. The first household was selected randomly at the center of the kebele, and the subsequent households were selected at every 7th interval until the sample size was fulfilled. When the selected households had no under-five children, the next neighborhood household was replaced.
Data Collection Tools and Methods
The structured questionnaire was developed after reviewing relevant literature to include all possible variables that address the objectives of the study. The questionnaire contains independent variables such as socio-demographic characteristics, behavioral factors, and environmental factors. The questionnaire was first prepared in English and then translated to the local language Gedeoffa and back-translated to English to maintain the consistency of the contents of the instrument. Face to face interviews was conducted to collect data about the above variables. The interview was conducted in the language that the respondent could understand and respond to.
Variables of the Study
Dependent variable: moderate to severe diarrhea
Independent Variables
Socio-demographic factors: age of the child, level of maternal education, ethnicity, family size, residency, monthly income of the family
Behavioral factors: immunization, access to clean water, hand wash station near latrine, soap or ash at hand wash station, breastfeeding
Environmental factors: facility type (flush latrine, VIP latrine, traditional pit latrine, and pour-flush latrine), access to any facility, facility sharing, open disposal of child’s feces, feces visible in defecation area, feces visible in house or yard.
Operational Definition
Moderate to severe diarrhea(MSD) was defined as a child with a diarrheal illness < 1-week duration with >/= 3 loose stools in 24h and >/=2 of the following conditions: lethargic, sunken eyes, drinking poorly, drinking eagerly, slow skin pinch, dysentery.10
Caregiver hygiene is the personal hygiene of caregivers like short fingernail cut or long fingernail, which could be factors for the occurrence of diarrheal disease among children.
Appropriate hand washing practice is the way of child-caregiver hand washing practice that shows clean hand palm, fingertip, and between-fingers observed by data collectors to determine its relationship with the occurrence of diarrheal disease.
Hand washing facilities refer to households having hand-washing facilities like plastic or metal with water seated nearest to latrine for children to wash their hands after latrine utilization, as observed by data collectors.
Hand washing during critical time refers to caregivers’ hand washing practice after utilization of latrine, before food preparation, and child-feeding as identified by caregivers’ oral report of their practice to identify its relationship with diarrheal occurrence.
Data Quality Management
To enhance instrument reliability, the pre-test was done on a 5% population in Abaya districts that have similar socio-demographic features as the study area. Data were collected using an interviewer-administered structured questionnaire, which was extruded from different literature. Unclear questions were explained for respondents during data filling and data were checked for its completeness before data filling. Each completed questionnaire was checked immediately at the site of data collection to ascertain all the questions had been answered consistently, and the number of returned questionnaires was counted.
Data Processing and Analysis
Data were cleaned, coded, and entered into SPSS Windows version 20 statistical software for analysis. Descriptive statistics were done to assess basic household characteristics and the prevalence of MSD. Bivariate analysis using a logistic regression technique was done to see the crude association between independent variables and the dependent variable. Factors that had a p-value of less than 0.25 were entered into multiple logistic regression models to control for confounding factors and to identify significant variables. The strength of statistical association was measured by the adjusted odds ratio at 95% CI, and a p-value < 0.05 was considered as a significant variable.
Ethical Consideration
The study was conducted after obtaining ethical clearance from the Institutional Review Board of the DURH. Oral consent was obtained from the participants before the interview. The verbal informed consent was acceptable and approved by the Ethics Research Review Board of Dilla University, and that this study was conducted under the Declaration of Helsinki. Also, all the responses were kept confidential and make the questionnaire anonymous. At the end of the interview, health information regarding MSD was provided. Children who had diarrhea during the interview were treated using ORS and zinc tablets and then sent to a nearby health institution.
Result
Socio-Demographic Characteristics
A total of 311 households were included in this study, yielding a response rate of 98%. 122 (39.2%) of the mothers were between the 25–31 ages group. Half of the mothers lived in a rural area 156 (50.2%). More than a quarter of the mothers 95 (30.5%) had completed elementary school. More than half of the households had more than or equal to five family members, 182 (58.5%). 127(40.8%) of children were < 1 year, and around half of the children were females 158 (50.8%). Around half of the household’s monthly income was above 1000.00 ETB 164 (52.7%) (Table 1).
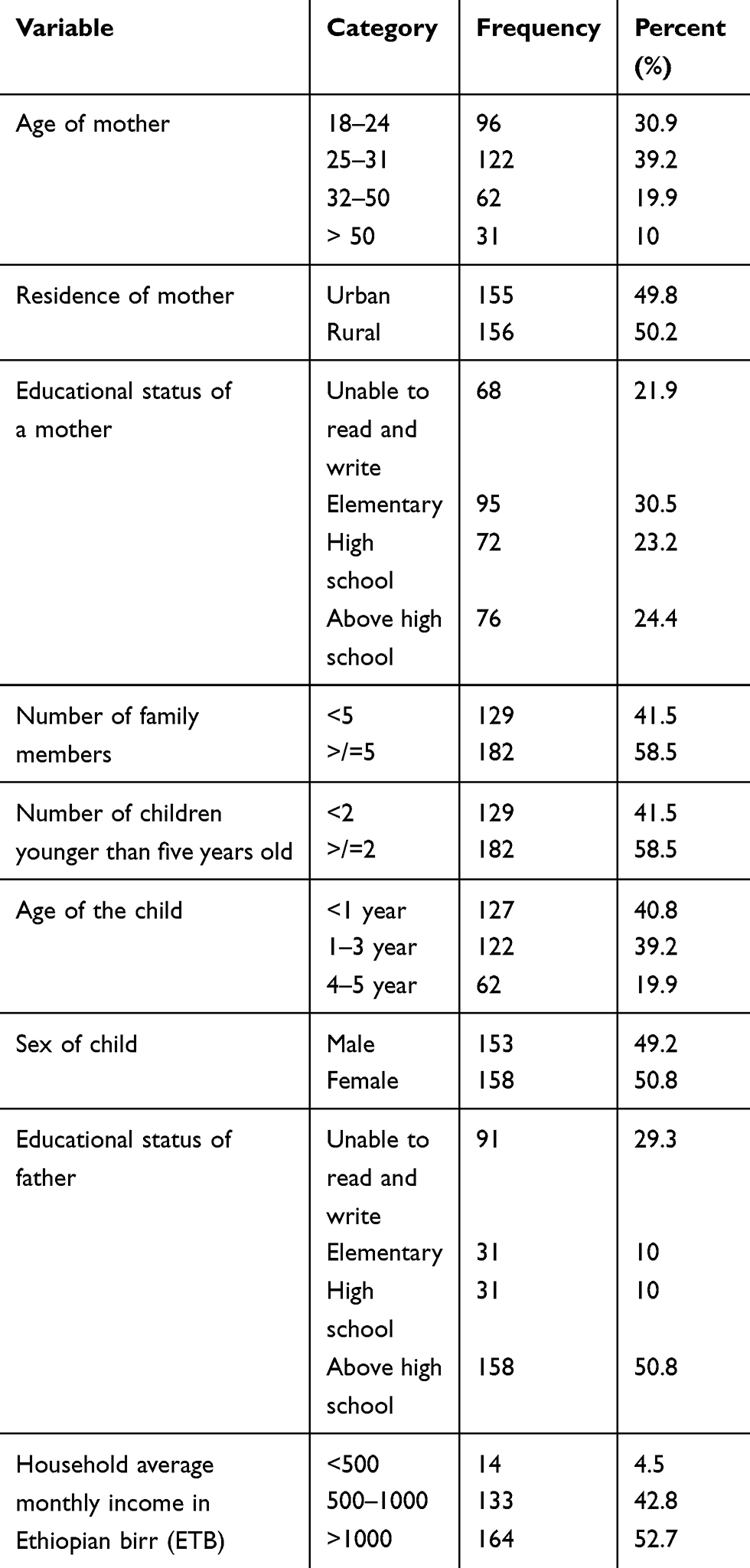 |
Table 1 Socio-Demographic Characteristics of Under-Five Children in Wonago District, South, Ethiopia, 2019 GC |
Environment-Related Factors
More than half of the respondent’s households had tap water 198 (63.7%) as drinking water sources. 223 (71.7%) of the mothers mentioned that it takes </= 30 minutes to fetch the drinking water. Among the households that had animals, 106 (34.1%) shared a house with their animals. The majority of respondents had latrine 235 (75.6%). Of those who own a latrine, 207 (66.6%) latrine type was a traditional pit latrine. Among latrine owners, 145 (46.6%) did not have handwashing facilities nearby the latrine. Half of the respondent’s households clean their compound every day 158 (50.8%). More than half of the household’s house floor was cleaned neatly 160 (51%). 218 (70.1%) of households’ compounds did not have feces in open field. Among those who own animals, 106 (34.1%) households contained animal feces.
Behavioral Factors
More than half of the households responded that their child started supplementary food at 6 months of age 202 (65%). Around half of the respondents stated that their child weaned at the age of two 153 (49.2%). Among the respondents, 138 (44.4%) mentioned they had been washing their hands at critical times, which means after utilization of latrine, before food preparation, and child-feeding. 121 (38.9%) households utilize soap or ashes for hand washing. Among the respondents, around 190 (61.1%) children had completed vaccination. 122 (39.2%) mothers had short fingernails, clean hand palms, and clean between fingers.
Prevalence of Moderate to Severe Diarrhea
The prevalence of moderate to severe diarrhea in the Wonago district was 30.9% with the majority of children diarrhea lasting for 4 days 64 (20.6%), and the majority of diarrheal frequency was 3 episodes per day 72 (23.2%).
Association Between Moderate to Severe Diarrhea with Independent Variables
In binary logistic regression seven variables (number of family members, animals in households, having latrine, cleaning household compound, supplementation food starting age, hand washing practice during a critical time, and household’s drinking water source) were p-value less than 0.25, so they were candidates for multivariate analysis.
But after controlling for the effects of confounding factors, four variables (number of family members, animal living in households, having latrine, and hand washing practice during a critical time) were strongly associated with moderate to severe diarrhea.
A child in households of family members greater than five were 3 times more likely to have moderate to severe diarrhea than those who have less than five family members [AOR: 2.7, 95% CI (1.277–5.716)] and children in households that have animals were 3 times more likely to have moderate to severe diarrhea than their encounter parts [AOR: 2.591, 95% CI (1.188–5.650)]. Children in households without latrine were 2 times more likely to have moderate to severe diarrhea than households who have Latrine [AOR: 2.129, 95% CI (1.006–4.505)].Children of a caregiver who did not practice hand washing during a critical time were 3 times more likely to develop moderate to severe diarrhea than respondents who did not wish their hand during a critical time [AOR: 2.683, 95% CI (1.139–6.319)] (Table 2).
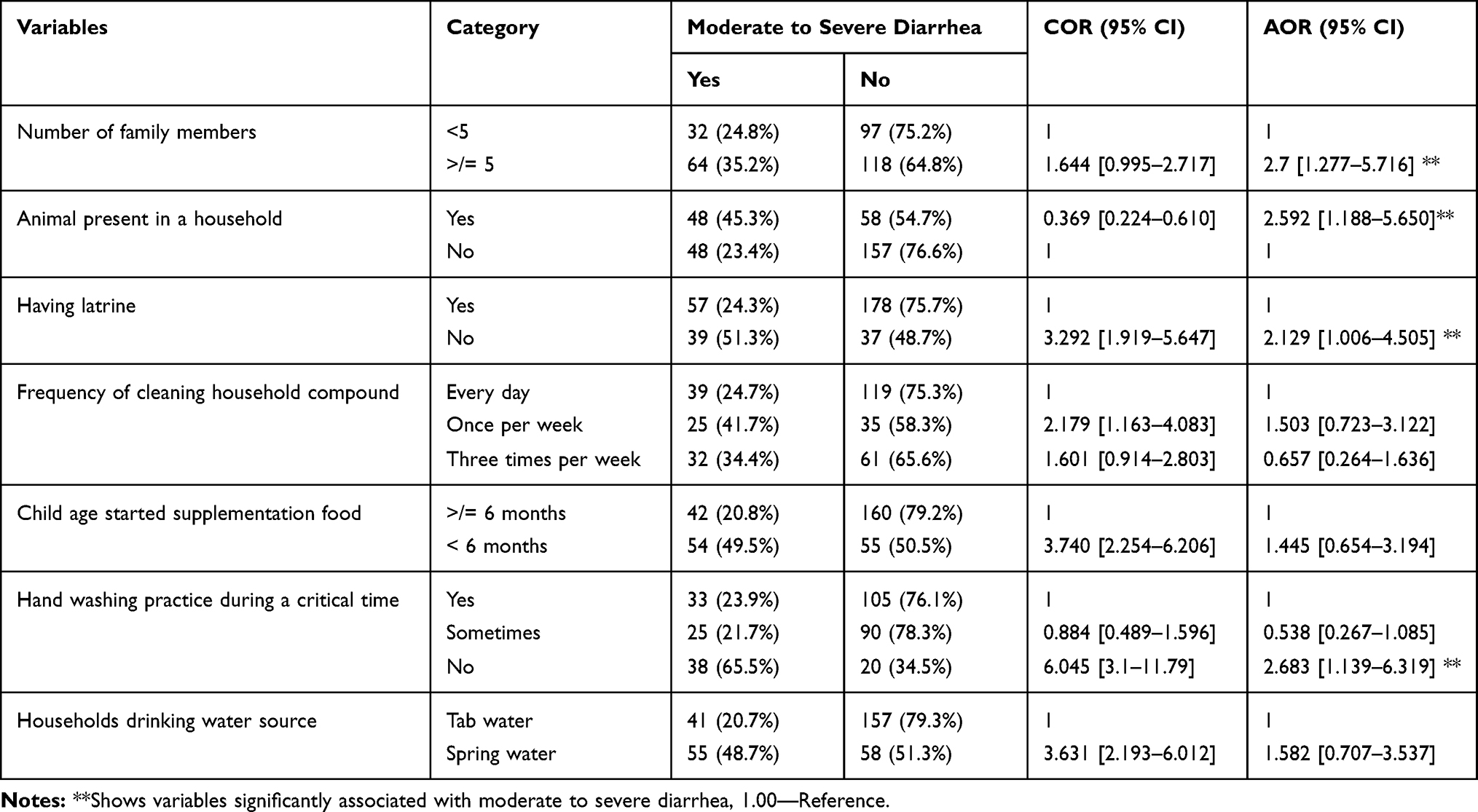 |
Table 2 Association Between Moderate to Severe Diarrhea and Independent Variables Among Under-Five Children in the Wonago District, South, Ethiopia, 2019 GC |
Discussion
The prevalence of moderate to severe diarrhea 30.9%. This is higher than the prevalence of diarrhea in Ethiopia (13%) and in the SNNPR region (16.3) observed in 2011 Ethiopian Demographic and Health Survey.7
This high prevalence of diarrhea is also higher compared to other studies done in other different parts of Ethiopia, 27.3% in Gigiga town9 11% in Wolaita sodo,11 14.9% in Jimma zone,12 and other studies conducted in Ethiopia.8,13 This might be due to study setting differences as well as our study area is a densely populated area with low socioeconomic status.
In this study number of family members is one of the predictors of moderate to severe diarrhea. A child in households of family members greater than five in numbers was 3 times more likely to have moderate to severe diarrhea. This might be due to overcrowding, which leads to family members being easily contracted by diarrhea. This result is supported by a study done in eastern Ethiopia.14
Another major predictor variable for the occurrence of diarrhea among under-five children in this study was latrine availability. The risk of having diarrhea was found to be significantly associated with latrine facilities, where children living in houses without latrine facilities were most likely to have a higher risk of diarrhea than children living in households with latrine facilities. These findings are supported by different studies.9,12,15
Hand washing practice during a critical time, which means that after the utilization of latrine, before food preparation, and child-feeding were found predictors of moderate to severe diarrhea. Children of caregivers who did not practice hand washing during critical time 3 times more likely to develop moderate to severe diarrhea. This might be due to those who did not practice hand washing during the critical time will be contaminated with human feces and microorganisms, so when they prepare food for children and feeding children, microorganisms might be transmitted to children; therefore this leads to diarrhea. These findings are supported by studies done in the Sidama zone,13 Gigiga District,9 Adama district,16 Arba Minch District,17 and also in Ibadan, Nigeria.18
Children in households that have animals were 3 times more likely to have moderate to severe diarrhea than their counterparts. This might be due to children exposed to animal feces that contain different microorganisms, and the child might be ingesting it; so this leads to diarrhea.
Conclusion
Childhood diarrhea remains an important health concern in the study area. The number of family members, animal presence within households, latrine availability, and hand washing practices during a critical time were strongly associated with the prevalence of diarrhea.
These findings have important policy implications for childhood diarrheal disease intervention programs. Government sectors and partners should work in collaboration to implement an intervention program focusing on the community to practice proper hand washing techniques at all appropriate times, and health extension workers need to give programmed health education regarding personal hygiene, environmental hygiene, and family planning for the community is also highly recommended.
Limitations of the Study
Our study has several limitations that are offered for consideration. First, the assessment of diarrhea prevalence was based on caregivers’ reports, which may have introduced some recall bias, second, determinant factors like nutritional factors were not included due to the limitation of time and resource.
Abbreviations
AGE, acute gastroenteritis; AOR, adjusted odds ratio; CI, confidence interval; DURH, Dilla University Referral Hospital; EDHS, Ethiopia Demographic and Health Survey; IRB, Institutional Review Board; MSD, moderate to severe diarrhea; SPSS, Statistical Package for Social Studies; U5C, under-five children; VIP, ventilated improved pit latrine; WASH, water sanitation and hygiene; WHO, World Health Organization.
Data Sharing Statement
All data and materials of this study are available and can be accessed with a reasonable request from Tinsae Shemelise (corresponding author) with the email address of “[email protected]”.
Ethics Approval and Consent to Participate
The paper of approval and letter of permission was obtained before the beginning of data collection from the research review board of Dilla University. After that, participants were oriented about the purpose and procedure of data collection, and that confidentiality and privacy were ensured. It is also clear that participation is fully based on participant’s willingness.
Acknowledgment
We would like to express our great appreciation to our study participants.
Author Contributions
AU and TS conceived and designed a study proposal, supervised data collection, cleaning, and feeding data to the commuter. AU, TS, and TM analyzed and interpreted the data and drafted the manuscript for important intellectual content.
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. All authors have read and approved the final manuscript.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. UNICEF. Estimates of child cause of death, acute respiratory infection (2015, December). [Data file]. Available from: https://data.unicef.org/wp-content/uploads/2015/12/CoD_ARI_Dec-2015_WHO_MCEE_236.xlsx.
2. UNICEF. Estimates of child cause of death, diarrhea, December, 2015. [Data file]. Available from: https://data.unicef.org/wp-content/uploads/2015/12/CoD_Diarrhoea_Dec-2015_WHO_MCEE_234.xlsx.
3. International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health. Pneumonia and diarrhea progress report 2016: reaching goals through action and innovation; 2016
4. McCormick BJJ, Lang DR. Diarrheal disease and enteric infections in LMIC communities: how big is the problem? Trop Dis Travel Med Vaccines. 2016;2(1):11. doi:10.1186/s40794-016-0028-7
5. UNICEF. One is Too Many: Ending Child Deaths from Pneumonia and Diarrhea. New York: UNICEF; 2016.
6. Deribew A, Tessema GA, Deribe K, et al. Trends, causes, and risk factors of mortality among children under 5 in Ethiopia, 1990–2013: findings from the Global Burden of Disease Study 2013. Popul Health Metr. 2016;14(1):42. doi:10.1186/s12963-016-0112-2
7. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
8. Dagnew AB, Tewabe T, Miskir Y, et al. Prevalence of diarrhea and associated factors among under-five children in Bahir Dar city, Northwest Ethiopia, 2016: a cross-sectional study. BMC Infect Dis. 2019;19(1):417. doi:10.1186/s12879-019-4030-3
9. Hashi A, Kumie A, Gasana J. Prevalence of diarrhoea and associated factors among under-five children in Jigjiga District, Somali Region, Eastern Ethiopia. Open J Prev Med. 2016;6(10):233–246. doi:10.4236/ojpm.2016.610022
10. Baker KK, O’Reilly CE, Levine MM, et al. Sanitation and hygiene-specific risk factors for moderate-to-severe diarrhea in young children in the global enteric multicenter study, 2007–2011: case-control study. PLoS Med. 2016;13(5):e1002010. doi:10.1371/journal.pmed.1002010
11. Alambo KA. The prevalence of diarrheal disease in under five children and associated risk factors in Wolitta Soddo Town, Southern, Ethiopia. ABC Res Alert. 2015;3(2). doi:10.18034/abcra.v3i2.295
12. Kasye DG, Garoma NH, Kassa MA. Assessment of the prevalence of diarrheal disease under-five children Serbo Town, Jimma Zone South West Ethiopia. Clin Mother Child Health. 2018;15(281):2. doi:10.4172/2090-7214.1000281
13. Melese B, Paulos W, Astawesegn FH, Gelgelu TB. Prevalence of diarrheal diseases and associated factors among under-five children in Dale District, Sidama zone, Southern Ethiopia: a cross-sectional study. BMC Public Health. 2019;19(1):1235. doi:10.1186/s12889-019-7579-2
14. Mengistie B, Berhane Y, Worku A. Prevalence of diarrhea and associated risk factors among children under-five years of age in Eastern Ethiopia: a cross-sectional study. Open J Prev Med. 2013;3(07):446. doi:10.4236/ojpm.2013.37060
15. Mihrete TS, Alemie GA, Teferra AS. Determinants of childhood diarrhea among underfive children in Benishangul Gumuz regional state, north West Ethiopia. BMC Pediatr. 2014;14(1):102. doi:10.1186/1471-2431-14-102
16. Regassa W, Lemma S. Assessment of diarrheal disease prevalence and associated risk factors in children of 6-59 months old at Adama District rural Kebeles, eastern Ethiopia, January/2015. Ethiop J Health Sci. 2016;26(6):581–588.
17. Mohammed S, Tamiru D. The burden of diarrheal diseases among children under five years of age in Arba Minch District, southern Ethiopia, and associated risk factors: a cross-sectional study. Int Scholarly Res Not. 2014;2014:1–6. doi:10.1155/2014/654901
18. Löfgren J, Tao W, Larsson E, Kyakulaga F, Forsberg BC. Treatment patterns of childhood diarrhoea in rural Uganda: a cross-sectional survey. BMC Int Health Hum Rights. 2012;12(1):19. doi:10.4314/ahs.v14i4.32
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.