")
Back to Journals » Infection and Drug Resistance » Volume 15
Model-Informed Precision Dosing of Antibiotics in Osteoarticular Infections
Authors Liu L, Wang J, Zhang H, Chen M , Cai Y
Received 5 August 2021
Accepted for publication 11 November 2021
Published 11 January 2022 Volume 2022:15 Pages 99—110
DOI https://doi.org/10.2147/IDR.S332366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lingling Liu,1 Jin Wang,1 Huan Zhang,1 Mengli Chen,2 Yun Cai1
1Center of Medicine Clinical Research, Department of Pharmacy, Medical Supplies Center, PLA General Hospital, Beijing, People’s Republic of China; 2Department of Pharmacy, Medical Supplies Center, PLA General Hospital, Beijing, People’s Republic of China
Correspondence: Yun Cai
Center of Medicine Clinical Research, Department of Pharmacy, Medical Supplies Center, PLA General Hospital, 28 Fu Xing Road, Beijing, 100853, People’s Republic of China
Tel +86-10-6693-7166
Email [email protected]
Mengli Chen
Department of Pharmacy, Medical Supplies Center, PLA General Hospital, 28 Fu Xing Road, Beijing, 100853, People’s Republic of China
Tel +86-10-6693-9610
Email [email protected]
Abstract: As a heterogeneous and wide inflammation, osteoarticular infection (OAI) shows an increasing incidence in recent years. Staphylococcus aureus is the most important pathogen causing OAI. The antibiotic treatment will affect the outcomes of OAI patients, and the drug selection and dosage regimen highly rely on patients’ variability, pathogen susceptibility, and drug property like bone permeability. Model-informed precision dosing (MIPD) provides options to describe and quantify the pharmacokinetic (PK) variability of the OAI population using different models, such as the population pharmacokinetic (PPK) model and physiological-based pharmacokinetic (PB/PK) model. In the present review, we highlighted that the MIPD of antibiotics played a critical role in OAI and listed the dose regimen recommended by the model. Collectively, our current study provided a valuable reference for the treatment of patients and improved the safety and efficiency of drug use.
Keywords: osteoarticular infection, antibiotic, PPK, PBPK, dose
Background
As a wide inflammation resulting from microbial invasions of bone and/or joint structures,1 osteoarticular infection (OAI) is a heterogeneous disease in its pathophysiology, clinical presentation, and treatment, which is frustrating for both patients and their doctors.2 OAI includes osteomyelitis, spondylodiscitis, septic arthritis, and prosthetic joint infection (PJI). With the rapid economic development, severe social aging problems, and the increase in artificial joint replacements, the incidence of OAI is rising worldwide.3–5 For example, the diagnosis of PJI has been steadily increasing in 2009–2018,6 which is associated with a 1-year mortality rate of 8–25.9%.7–9 For osteomyelitis, such rate is increased with the calendar year from 11.4 cases per 100,000 person-years in 1969–1979 to 24.4 per 100,000 person-years in 2000–2009 in the United States.10
The most common infection-causing pathogen for OAI is Staphylococcus aureus, including methicillin-susceptible S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA).4,11–13 Other pathogens that cause OAI, such as coagulase-negative staphylococci (CoNS) and aerobic Gram-negative bacilli, cannot be ignored.14,15 The resistances of CoNS isolated from OAI to vancomycin, teicoplanin, and linezolid are increased by 0–2.3%, 3.8–22%, and −3.5% between 2002 and 2011, respectively, while S. aureus is still sensitive to the above-mentioned antibiotics.16
The treatment of OAI requires antimicrobial therapy and surgical intervention, such as debridement and joint drainage.12,17–19 Infectious Diseases Society of America (IDSA) recommends vancomycin in combination with a third- or fourth-generation cephalosporin to cover the pathogens, including MRSA, streptococci, and Gram-negative bacilli, for patients with vertebral osteomyelitis as empirical administration.19 Insufficient antimicrobial treatment may induce secondary infections, deep vein thrombosis, and even secondary surgery.20,21 The success of antibiotic therapy depends on their permeability in bone tissue, the susceptibility of infected bacteria, and host-related factors.22 IDSA has issued the guidelines for the diagnosis and treatment of PJI in 2013 and native vertebral osteomyelitis in adults in 2015,19,23 which provide general antibiotic choices and dose regimens mainly based on experiences from cohort or case-controlled analytic studies. Notably, some essential oils can be a new antimicrobial frontier against multidrug-resistant bacteria, although most of the studies are still in the laboratory research stage.24,25
Model-informed precision dosing (MIPD) uses mathematical methods to integrate and quantitatively analyze information, such as physiology, pharmacology, and disease processes, through model simulations based on statistical principles, finally realizing the quantitative or at least semi-quantitative guidance for drug dosage individualization and increasing the safety and efficiency of drug use. Commonly used methods of models include the population pharmacokinetic (PPK) model, population pharmacodynamic (PopPD) model, pharmacokinetic/pharmacodynamic (PK/PD) model, physiological-based pharmacokinetic (PB/PK) model, and so on.26,27 PPK model can identify sources and correlates of PK variability in a target patient population receiving an agent of interest.28,29 PB/PK model uses “physiology room” to replace the compartmental model, and simulates the circulatory system blood flow to connect the body’s various tissues or organs, allowing simulation of the time course of drug concentrations in plasma and tissues, such as bone tissue.30,31
In the present work, we summarized the recently published studies to emphasize the potentiality of MIPD of antibiotics in individualization and precision medicine for OAI treatment.
MIPD of Antibiotics Against Gram-Positive Bacteria-Caused OAI
Penicillin
Cloxacillin is a time-dependent antibiotic against staphylococcal infections,32,33 with a plasma protein-binding (PB) rate of around 94% and a half-life (T1/2) of nearly 45 min.34 Its PK/PD target is the time above the MIC of greater than 50% of the dosing interval (50% fT>MIC). The label recommended dose of cloxacillin in OAI is 4–6 g/day, iv, divided into 2–4 times. A retrospective study35 included 82 patients with severe septic bursitis receiving cloxacillin (2 g, q4 h, iv until improvement, afterward 1 g,q6 h, po until resolution) alone or in combination with gentamicin 240 mg/day, iv or rifampicin 600 mg/day, po. They concluded that cloxacillin alone might be sufficient for patients without extensive cellulitis, and cloxacillin in combination with gentamicin seemed to be appropriate for the majority of severe patients.
Courjon et al36 recruited 11 patients with OAI caused by MSSA who received continuous infusion (CI) or intermittent infusion (II) of cloxacillin using a prospective crossover design and developed a PPK model. Tables 1 and 2 summarize the demographic data of patients and model parameters. They used a two-compartment model to describe the data, performed PK/PD simulations, and calculated the probability of target attainment (PTA) for several II and CI dosing regimens. Moreover, they suggested a prolonged infusion or CI of cloxacillin, ie, 2–3 g, q6 h, 2–4 h of infusions; 2 g, q4 h, 1–2 h of infusions; 6–12 g/day, and CI would achieve a PTA of 90% based on the PK/PD target of 50% fT>MIC against S. aureus at a MIC up to 0.5 mg/L. Those two studies both showed insufficient label dose in OAI.
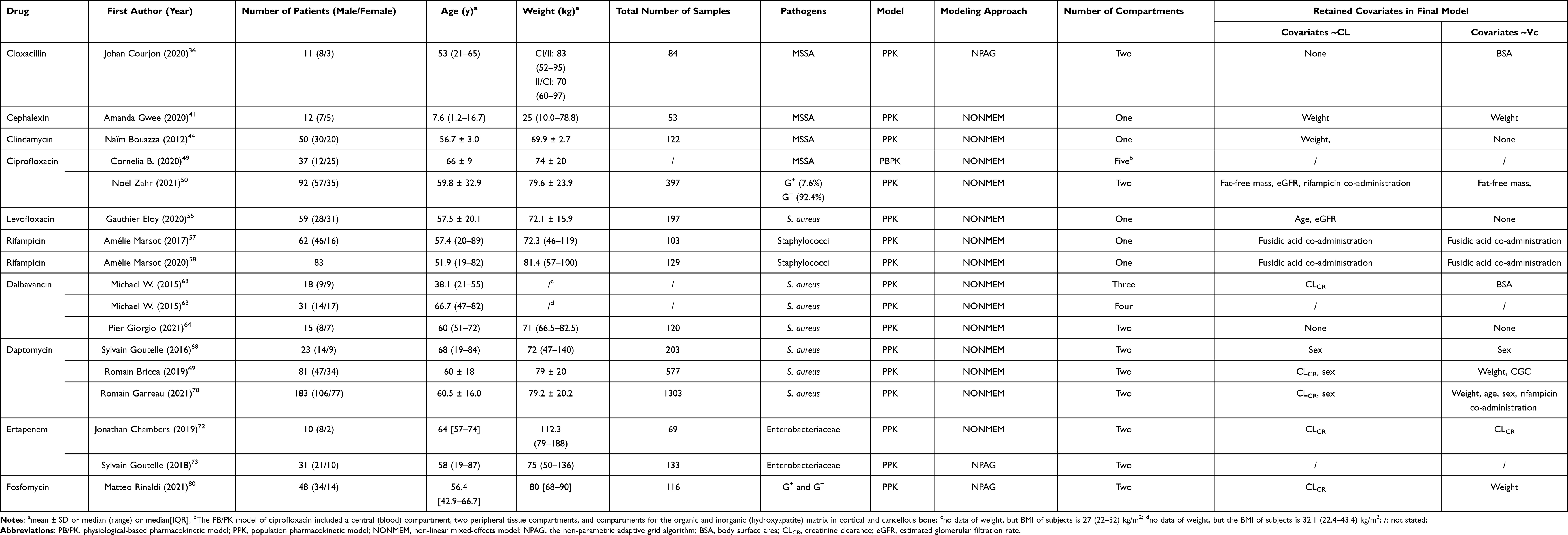 |
Table 1 Overview Characteristics of Included Studies |
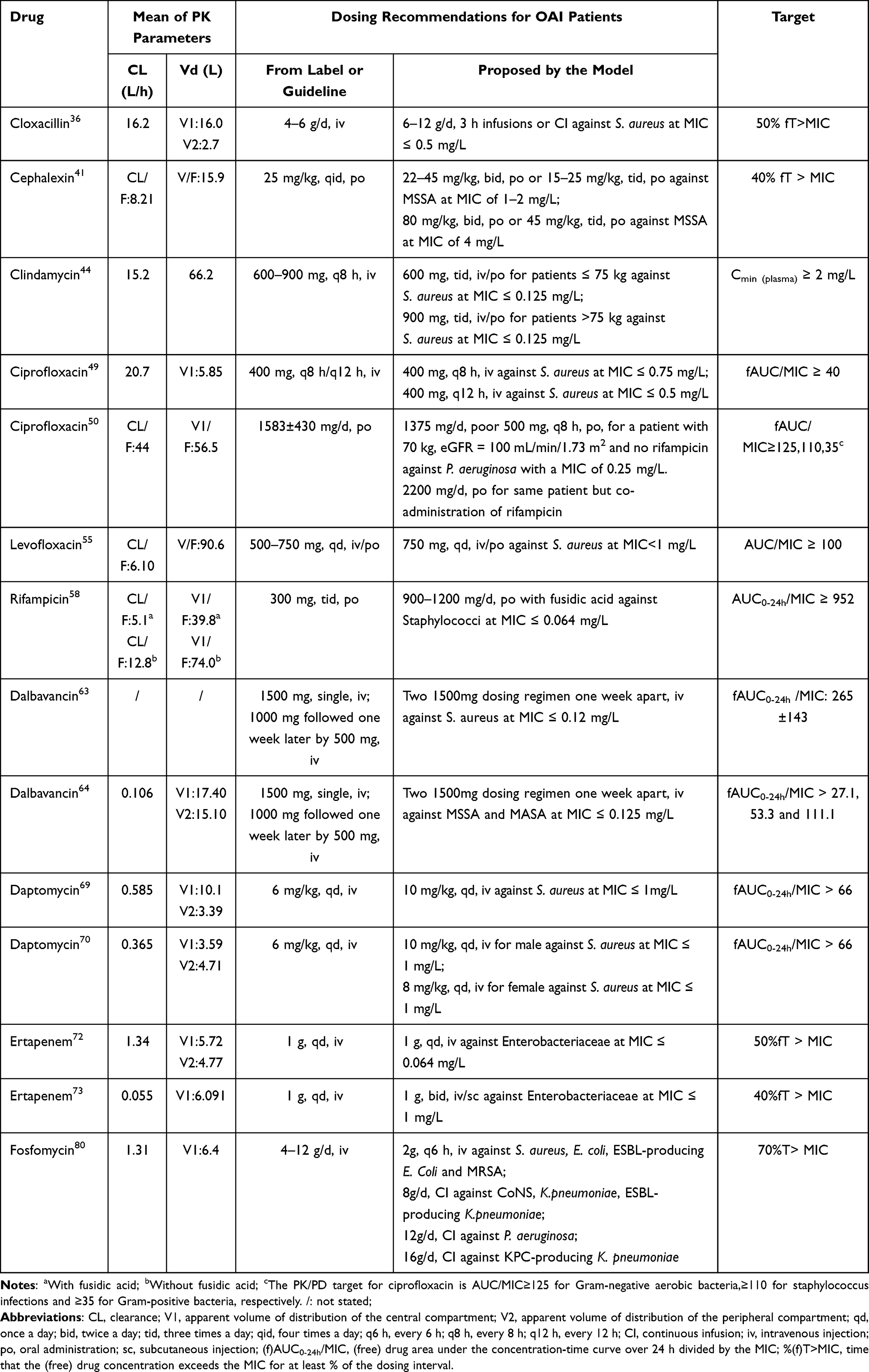 |
Table 2 Summary of Drug PK Parameters and Dosing Recommendations for OAI Patients |
Cephalosporin
Cephalexin shows a time-dependent bactericidal activity against MSSA, its oral bioavailability (F) is close to 100%, and its T1/2 is 49.5–76.5 min,37 with a PB of 10–15%34 and a PK/PD target of 40% fT >MIC. The recommended dose in the instruction is 250–500 mg, qid, po for adults and 25–50 mg/kg, qid, po for children.38 Moreover, the guideline also recommends cephalexin 500 mg, q6 h, as a followed-by oral therapy for an additional 7–14 days after parenteral antibiotics for at least 14 days in adults with MSSA septic arthritis.
One study39 showed that after a single dose of 1 g cephalexin orally, the samples of two patients were collected after 3–4 h, the bone concentrations were 1.3 and 3.1 μg/g, while the serum concentrations were 37.7 and 27.9 μg/mL, respectively. Given that the frequency of four times daily would lower treatment compliance with higher frequency in clinical practice, one PK/PD study40 showed the safety and efficiency of cephalexin at a median dose of 40 mg/kg, q8 h, po in 12 children with OAI, and the PTA was 100%, 90%, and 80% for MSSA with MICs at 0.25, 2, and 4 mg/L, respectively.
In 2020, Gwee et al41 established the first PPK model of cephalexin to optimize the dosing regimen, such as twice-daily and thrice-daily, with 12 OAI children caused by MSSA. Due to the delay in oral absorption, one compartment with a transit compartment model was used to fit the data of cephalexin adequately. They concluded that 22–45 mg/kg, bid, or 15–25 mg/kg, tid, po for MSSA with a MIC of 1–2 mg/L; 80 mg/kg, bid, or 45 mg/kg, tid, po for MSSA with a MIC of 4 mg/L could achieve a PTA of 90% at the target of 40% fT>MIC. They developed a more detailed and specific dosing regimen of cephalexin, showing the superiority of the PPK model.
Lincosamide
Clindamycin is a time-dependent killing antibiotic against anaerobic bacteria, Gram-positive cocci and bacilli, and Gram-negative bacilli,42 with a PB of 92–94% and a T1/2 of 2.5–3 h. The label recommended dose of clindamycin for adults’ infection is 600–2700 mg/day, divided into 2 or 3 times, iv; 150–300 mg, q6 h or q8 h, po. IDSA recommends it to treat native vertebral osteomyelitis in adults at a dose of 600–900 mg, q8 h, iv as a parenteral treatment.19 An observational study included 61 OAI patients receiving a median dose of 600 mg, q8 h. The measured median Cmin(plasma) was 1.39 mg/L, with 58% of patients below the target of 1.7 mg/L (due to Cbone /MIC > 2 at the MIC of 0.25 mg/L based on the penetration of 30% to bone), suggesting this dose regimen was not sufficient.43
In 2012, Bouazza et al44 developed a PPK model consisting of 50 osteomyelitis patients receiving clindamycin at a median dose of 26.0 mg/kg/d, iv/po, and these data were adequately described by a one-compartment model. F was estimated to be 87.6%. They chose a PK/PD target of Cmin (plasma) ≥ 2 mg/L due to Cbone /MIC > 5 at the MIC of 0.125 mg/L for S. aureus based on the penetration of 30% to the bone. Besides, Monte Carlo simulations showed that 600 mg, q8 h, iv/po was enough for patients with a bodyweight ≤75 kg. For those with a bodyweight >75 kg, the dose should be raised to 900 mg, q8 h, iv/po as the clearance was significantly increased with bodyweight. Adjusting the dose regimen according to the patient’s bodyweight may be more proper to ensure efficiency.
Fluoroquinolone
Ciprofloxacin produces its concentration-dependent activity against many Gram-negative and Gram-positive bacteria,45,46 including intracellular S. aureus,47,48 and its PK/PD target is fAUC0-24 h /MIC ≥ 40. With a PB of about 25% and a T1/2 of 4 h,34 FDA recommends 400 mg, iv,q8 h or q12 h, with a duration of 4 to 8 weeks for OAI patients. In 2020, Landersdorfer et al49 developed a PB/PK model consisting of 39 patients with a single dose of 400 mg, iv, at 0.5–20 h before orthopedic surgery to study the complete time-course of ciprofloxacin in bone. It included a central (blood) compartment, two peripheral tissue compartments, and compartments for the organic and inorganic (hydroxyapatite) matrix in cortical and cancellous bone. They found that at 0.5–2 h and 13–20 h, the average observed cortical bone/plasma concentration ratio (Ccort/Cplasma) was 0.67 and 5.1, and that for cancellous bone (Ccanc/Cplasma) was 0.77 and 4.4, respectively. Moreover, at the steady-state, AUCcort/AUCplasma and AUCcanc/AUCplasma were 1.62 and 2.53, respectively, with higher concentrations detected in bone compared with plasma. Monte Carlo simulations showed that with the maximum approved daily dose of 400 mg, q8 h, reverse engineered PK/PD breakpoints for plasma and bone were 0.75 mg/L and 0.5 mg/L, respectively, which was lower than the MIC of S. aureus (1 mg/L) based on the PK/PD target of AUCcort/MIC of ≥86 and AUCcanc/MIC of ≥135. Therefore, the currently approved dose regimen would not be sufficient, and it suggests that a combination with other classes of antibiotics would be more efficient for treating S. aureus osteomyelitis. Recently, Zahr et al50 developed a PPK model of ciprofloxacin with 92 OAI patients, which was fitted to a two-compartment. They made a specific dosing regimen according to the patient’s bodyweight, eGFR, co-administration of rifampicin, the PK/PD target for different infectious pathogens. For example, a patient with 70 kg, eGFR = 100 mL/min/1.73 m2 and no rifampicin, the corresponding dose is 1375 mg/d, po, based on the target of AUC/MIC ≥125 for P. aeruginosa with a MIC of 0.25 mg/L. Moreover, co-administration of rifampicin increases this dose by 60% (namely 2200 mg/d, po). Although the specific values of PK/PD target, the PK parameters, the probability of target attainment (PTA) of simulations have certain deviations in two model studies, and the dose of ciprofloxacin (400 mg, iv, q8 h) is a bit lower in the treatment of OAI.
Levofloxacin has a similar action mechanism as ciprofloxacin, its F is about 99%, and PK/PD target is AUC0-24 h/MIC ≥100, with a PB of 24–38% and a T1/2 of approximately 6–8 h.51,52 As for the penetration into bone, one study encompassed 12 subjects undergoing total hip replacement who received a single dose of levofloxacin 500 mg, iv. After 1.2 h, the samples were collected and analyzed. Results showed that the Cplasma was 7.5 ± 1.3 mg/L. The mean Ccort/Cplasma and Ccanc/Cplasma were 0.5 and 1.0, respectively, which achieved greater concentrations in cancellous and cortical bone tissues compared with the breakpoint of MIC ≤ 2 mg/L for susceptible organisms, such as S. aureus.53 The recommended dose of levofloxacin is 250–750 mg, qd, iv/po, while IDSA recommends 500–750 mg, qd, po for native vertebral osteomyelitis caused by MSSA in adults.19 A patient of periprosthetic knee infection caused by Streptococcus anginosus, was successfully treated by vancomycin (1 g, q12h, iv) and levofloxacin (750 mg, qd, iv) for 4 weeks, and then levofloxacin (750 mg, qd, po) for 2 weeks.54
In 2020, Eloy et al55 developed a PPK model of levofloxacin with 59 OAI patients, and the model consisted of a one-compartment model with first-order absorption and elimination. Monte Carlo simulations evaluated the PTA of levofloxacin at a dose of 750 mg, qd, with different ages and renal functions. They found that 750 mg, qd would provide an optimal exposure at the target of AUC0-24 h/MIC ≥100 for S. aureus at a MIC of <1 mg/L. If the patients were older than 60 years old with an eGFR <70 mL/min/1.73 m2, the dose should be decreased. Therefore, levofloxacin 750 mg, qd, iv/po seemed to be appropriate for most OAI patients.
Rifampicin
Rifampicin inhibits DNA-dependent RNA polymerase activity, which concentration-dependently kills most intracellular and extracellular Gram-positive and Gram-negative bacteria,34 with a PB of 89%. The PK/PD target of rifampicin is AUC0-24 h/MIC ≥952. One study demonstrated that the Ccort/Cserum and Ccanc/Cserum at 3 h after 600 mg, bid, po were 0.20 and 0.41, respectively, showing a good bone penetration of rifampicin.56 Moreover, rifampicin was recommended by IDSA to treat Staphylococcal OAI at a dosing regimen of 300–450 mg, bid, po.23
In 2016, Marsot et al57 established the first rifampicin PPK model consisting of 62 OAI patients, and this model was composed of a one-compartment model and a transit absorption model. They found that fusidic acid led to potential high drug exposure of rifampicin, presenting a decrease of CL (5.1 L/h vs 13.7 L/h) and Vd (23.8 L vs 61.1 L). Since fusidic acid inhibits the transporter OATP1B1, of which rifampicin is a sensitive substrate. In 2020, they58 enrolled 21 new patients to rebuild a PPK model, and this new dataset consisting of 83 patients used the same compartment model. They confirmed this drug-interaction by Monte Carlo simulations that rifampicin co-administration with fusidic acid achieved the target of AUC0-24 h/MIC ≥952 for staphylococci at a MIC of 0.004–0.064 mg/L with all tested dosing regimens (600 and 900 mg, qd; 450 and 600 mg, bid; or 300 mg, tid), except for 600mg, qd for Staphylococcus epidermidis OAI, whereas none of the tested dosing regimens achieved this target in the absence of fusidic acid. Those two studies showed that the co-administration of fusidic acid might improve the PTA of rifampicin in OAI.
Glycopeptide
As a second-generation lipoglycopeptide antibiotic, dalbavancin’s T1/2 is 346 h at a once-weekly dosing regimen, with a PB of 93%.34 Dalbavancin exhibits a dose-dependent activity, with a target of mean fAUC0-24 h/MIC 265 ± 143 against S. aureus, and it shows increased activity against Gram-positive bacteria, including MRSA, compared with natural glycopeptides, such as vancomycin and teicoplanin.59 FDA label recommends a single infusion dosage of 1500 mg or a two-dose regimen of 1000 mg followed by 1 week of 500 mg for patients with acute bacterial skin and skin structure infections with normal renal function.60 A retrospective cohort study of adults with OAI, or other infections receiving dalbavancin (1500 mg for two doses 1 week apart) or SOC (vancomycin 17.1 mg/kg and daptomycin 7.4 mg/kg) showed that compared with SOC, dalbavancin was related to a lower 90-day infection-related readmission, a shorter hospital stay before therapy, and a longer time to infection-related readmission.61 In a case-control study of prosthetic joint infections, 1500 mg for two doses with a 3-week interval showed no significant difference in efficacy and reduced toxicity compared with other drug combinations.62
In 2015, Dunne et al63 conducted two phase-I studies of dalbavancin. They developed a PPK model to describe the time course of dalbavancin in plasma with 18 healthy volunteers using a three-compartment model with zero-order iv input and first-order elimination. Subsequently, a four-compartment PPK model was expanded for the dalbavancin transfer between plasma and bone tissue with 31 healthy volunteers to characterize the bone penetration. They found that after a single dose of 1000 mg, iv, the dalbavancin concentrations in cortical bone were 6.3 and 4.1 μg/g at 12 h and 14 days, respectively, while those in plasma were 85.3 and 15.3 μg/mL, respectively. Moreover, the AUCbone/AUCplasma penetration ratio was 0.131. Besides, they concluded that two 1500 mg dosing once-weekly regimens provided tissue exposure over the MIC99 for S. aureus of 0.12 mg/L for 8 weeks and were well tolerated based on the target of fAUC0-24 h/MIC of 265 ± 143. In 2021, 15 Gram-positive OAI adult patients were recruited to develop another PPK model of dalbavancin using a two-compartment model with linear elimination to fit the data.64 Results showed that two licensed dosages granted an extension of desirable PTA up to 3 weeks at the target of fAUC0-24 h/MIC >27.1 or 53.3. Two 1500 mg dosing once-weekly regimens granted an extension of desirable PTA up to 5–7 weeks, 3–4 weeks, and 3 weeks at the target of fAUC0-24h/MIC >27.1, 53.3, and 111.1, respectively, against S. aureus. Finally, they concluded that two 1500 mg dosing once-weekly regimens might be continuously effective for up to 5 weeks against MSSA and MRSA in OAI patients. Studies of PPK models showed the potency of two 1500 mg dosing once-weekly in OAI.
Lipopeptide
Daptomycin is a concentration-dependent killing antibiotic against Gram-positive bacteria, and its PK/PD target is AUC0-24 h/MIC >666 against S. aureus.65 As a high plasma PB drug (90–93%),66 daptomycin’s bone penetration percentage is 9.0%.67 Moreover, its recommended dose is 6 mg/kg, qd for MRSA OAI patients in the guideline published by IDSA in 2013.23 In 2016, one PPK model consisting of 23 OAI patients described the data by a two-compartment model.68 The model showed that the CL of daptomycin was significantly higher in males compared with female patients, and suggested that Cmax(plasma)>50 μg/mL and Cmin (plasma)< 24 μg/mL could be considered as targets for TDM. Bricca et al made a series of studies for the PPK of daptomycin in OAI patients,69,70 both using a two-compartment model. They concluded that sex difference, rifampicin co-administration, and P-gp gene polymorphism might affect the probability of AUC0-24 h/MIC target attainment. Interestingly, contrary to clindamycin, the rifampicin co-administration improved daptomycin exposure, showing the decrease of the volume of distribution of the central compartment (V1) due to the P-gp induction effect of rifampicin. Besides, they recommended a dosing regimen of 8 mg/kg/d in women and 10 mg/kg/d in men by PK/PD simulations at the target of fAUC0-24 h/MIC >66 for S. aureus at a MIC ≤ 1 mg/L.
MIPD of Antibiotics Against Gram-Negative Bacteria-Caused OAI
Carbapenem
Ertapenem shows a time-dependent killing activity against Gram-negative bacteria, which is stable against hydrolysis by extended-spectrum beta-lactamases (ESBL), while it can be hydrolyzed by Metallo-beta-lactamases. With a PB of 85–95% and a T1/2 of 2.5–4 h, its PK/PD target is defined as 40% fT>MIC.71 The label recommended dose and guideline recommendation for Enterobacteriaceae-caused native vertebral osteomyelitis in adults are both 1 g, qd, iv. A PPK model of ertapenem72 performed a two-compartment model and showed a bone to plasma ratio of 0.025 over 24 h after a single dose of 1 g, iv in 10 obese OAI patients, and the PTA of bone is ~90%, ~80%, ~65%, ~45%, and ~30% for MICs of 0.064, 0.125, 0.25, 0.5, and 1.0 mg/L, respectively. Therefore, ertapenem is recommended to treat OAI at a dose of 1 g, qd, iv against Enterobacteriaceae at a MIC ≤ 0.064 mg/L. Another PPK model73 consisting of 31 subjects used a two-compartment model to compare subcutaneous injection (sc) with intravenous injection (iv) of 1 g, bid/qd of ertapenem. They found that sc administration lowered the peak concentration but prolonged the action of ertapenem, with a higher value of fT>MIC. For example, the regimen of 1 g, qd, iv failed to achieve 90% PTA for a MIC of 1 mg/L, whereas 1 g, qd, sc achieved this goal. Moreover, 1 g, bid, iv/sc provided 90% PTA for a MIC of 2 mg/L, which could achieve the PK/PD target for OAI patients.
MIPD of Broad-Spectrum Antibiotics in OAI
Fosfomycin
Fosfomycin is a time-dependent bactericidal antibiotic disrupting the first step of bacterial cell wall synthesis,74 and its PK/PD target is 70% T>MIC. With a wide range of bactericidal activity against Gram-positive bacteria and Gram-negative bacteria, including MRSA and MDR-enterobacteria,74,75 fosfomycin is also active against biofilms.76,77 With a PB of <5% and a T1/2 of 3–5 h, the label recommended dose of fosfomycin is 4–12 g/day, divided into 2–3 times for adults. Fosfomycin shows a good penetrating ability to the bone, and its ratio of the AUC0–6 h for the bone to plasma is 0.43±0.04 after a single intravenous dose of 100 mg/kg for diabetic patients presenting with bacterial foot infection.78 The available data suggested that 93.7% OAI patients (343/365) used fosfomycin (4–24 g/d) as a part of combination therapy showing well safety.79
In 2021, Rinaldi et al80 conducted a prospective study with 48 OAI patients and developed a PPK model of fosfomycin. A two-compartment open model with infusion input and first-order elimination best fitted the data. Monte Carlo simulations showed a daily dosage of 2 g, q6 h by II against S. aureus, E. coli, ESBL-producing E. Coli, and MRSA; 8 g by CI against CoNS, K. pneumonia, and ESBL-producing K. pneumoniae; 12 g by CI against P. aeruginosa, and 16 g by CI against KPC-producing K. pneumonia would achieve the optimal PTA of 70% T>MIC and the cumulative fraction of response (CFR) (≥90%).
Conclusions
In the present study, we summarized the characteristics of the relevant study population, model parameters, and recommended dosing regimens of the PPK and PBPK models of antibiotics in OAI patients. MIPD takes account of the individual characteristics adequately, and tailors antibiotic dose recommendations for each patient instead of the “one-dose-fits-all-approach”. The model achieves stratification of dose regimen based on the types of infectious pathogens and their respective susceptibility to different antibiotics. Moreover, it identifies other risk factors influencing treatment efficacy and safety of OAI, like drug bone permeability, T1/2, drug–drug interactions, and administration route. Although MIPD extrapolation should match the intended population and monitor dynamically, this review optimized antibiotic dose administration for OAI patients and advanced relevant information for the clinicians.
Data Sharing Statement
All data analyzed are included in this published article.
Funding
This work was supported by the National Natural Science Foundations of China (81770004 and 82073894) and the Cultivation Project of PLA General Hospital for Distinguished Young Scientists (2020-JQPY-004).
Disclosure
The authors declare no competing interests.
References
1. Zimmerli W, Sendi P. Orthopaedic biofilm infections. APMIS. 2017;125(4):353–364. doi:10.1111/apm.12687
2. Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364(9431):369–379. doi:10.1016/S0140-6736(04)16727-5
3. Gupta A, Kowalski TJ, Osmon DR, et al. Long-term outcome of pyogenic vertebral osteomyelitis: a cohort study of 260 patients. Open Forum Infect Dis. 2014;1(3):ofu107. doi:10.1093/ofid/ofu107
4. Pigrau C, Rodriguez-Pardo D, Fernandez-Hidalgo N, et al. Health care associated hematogenous pyogenic vertebral osteomyelitis: a severe and potentially preventable infectious disease. Medicine. 2015;94(3):e365. doi:10.1097/MD.0000000000000365
5. Uckay I, Holy D, Betz M, Sauer R, Huber T, Burkhard J. Osteoarticular infections: a specific program for older patients? Aging Clin Exp Res. 2021;33(3):703–710. doi:10.1007/s40520-019-01329-w
6. Walter N, Rupp M, Hinterberger T, Alt V. Prosthetic infections and the increasing importance of psychological comorbidities: an epidemiological analysis for Germany from 2009 through 2019. Orthopade. 2021. doi:10.1007/s00132-021-04088-7
7. Otto-Lambertz C, Yagdiran A, Wallscheid F, Eysel P, Jung N. Periprosthetic infection in joint replacement. Dtsch Arztebl Int. 2017;114(20):347–353. doi:10.3238/arztebl.2017.0347
8. Gundtoft PH, Pedersen AB, Varnum C, Overgaard S. Increased mortality after prosthetic joint infection in primary THA. Clin Orthop Relat Res. 2017;475(11):2623–2631. doi:10.1007/s11999-017-5289-6
9. Zmistowski B, Karam JA, Durinka JB, Casper DS, Parvizi J. Periprosthetic joint infection increases the risk of one-year mortality. J Bone Joint Surg Am. 2013;95(24):2177–2184.
10. Kremers HM, Nwojo ME, Ransom JE, Wood-Wentz CM, Melton LJ
11. Yeo A, Ramachandran M. Acute haematogenous osteomyelitis in children. Br Med J. 2014;348:g66. doi:10.1136/bmj.g66
12. Lazzeri E, Bozzao A, Cataldo MA, et al. Joint EANM/ESNR and ESCMID-endorsed consensus document for the diagnosis of spine infection (spondylodiscitis) in adults. Eur J Nucl Med Mol Imaging. 2019;46(12):2464–2487. doi:10.1007/s00259-019-04393-6
13. Ondusko DS, Nolt D. Staphylococcus aureus. Pediatr Rev. 2018;39(6):287–298. doi:10.1542/pir.2017-0224
14. Nolla JM, Ariza J, Gómez-Vaquero C, et al. Spontaneous pyogenic vertebral osteomyelitis in nondrug users. Semin Arthritis Rheum. 2002;31(4):271–278. doi:10.1053/sarh.2002.29492
15. Perrotti PP, Corrales JL, Popescu BM. [Pyogenic vertebral osteomyelitis]. Medicina. 2009;69(5):513–518. [Spanish]
16. Titécat M, Senneville E, Wallet F, et al. Microbiologic profile of Staphylococci isolated from osteoarticular infections: evolution over ten years. Surg Infect (Larchmt). 2015;16(1):77–83. doi:10.1089/sur.2013.258
17. Sharff KA, Richards EP, Townes JM. Clinical management of septic arthritis. Curr Rheumatol Rep. 2013;15(6):332. doi:10.1007/s11926-013-0332-4
18. Tsantes AG, Papadopoulos DV, Vrioni G, et al. Spinal infections: an update. Microorganisms. 2020;8(4):476. doi:10.3390/microorganisms8040476
19. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in Adults. Clin Infect Dis. 2015;61(6):e26–46. doi:10.1093/cid/civ482
20. Gelfand MS, Cleveland KO, Goswami RK, Heck R. Pathological fracture in acute osteomyelitis of long bones secondary to community-acquired methicillin-resistant Staphylococcus aureus: two cases and review of the literature. Am J Med Sci. 2006;332(6):357–360. doi:10.1097/00000441-200612000-00010
21. Kaandorp CJ, Krijnen P, Moens HJ, Habbema JD, van Schaardenburg D. The outcome of bacterial arthritis: a prospective community-based study. Arthritis Rheum. 1997;40(5):884–892. doi:10.1002/art.1780400516
22. Stepensky D, Kleinberg L, Hoffman A. Bone as an effect compartment: models for uptake and release of drugs. Clin Pharmacokinet. 2003;42(10):863–881. doi:10.2165/00003088-200342100-00001
23. Osmon DR, Berbari EF, Berendt AR, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2013;57(1):162–164. doi:10.1093/cid/cit189
24. Langeveld WT, Veldhuizen EJ, Burt SA. Synergy between essential oil components and antibiotics: a review. Crit Rev Microbiol. 2014;40(1):76–94. doi:10.3109/1040841X.2013.763219
25. Amorese V, Donadu M, Usai D, et al. In vitro activity of essential oils against Pseudomonas aeruginosa isolated from infected hip implants. J Infect Dev Ctries. 2018;12(11):996–1001. doi:10.3855/jidc.10988
26. Li J, Yang J, Wang Y. Applications of model-informed drug development (MIDD) on new drug research and development. Chin J Clin Pharmacol Ther. 2020;25(01):1-8. doi:10.12092/j.issn.1009-2501.2020.01.001
27. Darwich AS, Polasek TM, Aronson JK, et al. Model-informed precision dosing: background, requirements, validation, implementation, and forward trajectory of individualizing drug therapy. Annu Rev Pharmacol Toxicol. 2021;61(1):225–245. doi:10.1146/annurev-pharmtox-033020-113257
28. Kiang TK, Sherwin CM, Spigarelli MG, Ensom MH. Fundamentals of population pharmacokinetic modelling: modelling and software. Clin Pharmacokinet. 2012;51(8):515–525. doi:10.1007/BF03261928
29. Ludden TM. Population pharmacokinetics. J Clin Pharmacol. 1988;28(12):1059–1063. doi:10.1002/j.1552-4604.1988.tb05714.x
30. Miller NA, Reddy MB, Heikkinen AT, Lukacova V, Parrott N. Physiologically based pharmacokinetic modelling for first-in-human predictions: an updated model building strategy illustrated with challenging industry case studies. Clin Pharmacokinet. 2019;58(6):727–746. doi:10.1007/s40262-019-00741-9
31. El-Khateeb E, Burkhill S, Murby S, Amirat H, Rostami-Hodjegan A, Ahmad A. Physiological-based pharmacokinetic modeling trends in pharmaceutical drug development over the last 20-years; in-depth analysis of applications, organizations, and platforms. Biopharm Drug Dispos. 2021;42(4):107–117. doi:10.1002/bdd.2257
32. Ghathian K, Frimodt-Moller N. Beta-hemolytic streptococci A, C and G are susceptible to cloxacillin. APMIS. 2021;129(6):314–316. doi:10.1111/apm.13134
33. Ambrose PG, Bhavnani SM, Rubino CM, et al. Pharmacokinetics-pharmacodynamics of antimicrobial therapy: it’s not just for mice anymore. Clin Infect Dis. 2007;44(1):79–86. doi:10.1086/510079
34. Wishart DS, Feunang YD, Guo AC, et al. DrugBank 5.0: a major update to the DrugBank database for 2018. Nucleic Acids Res. 2018;46(D1):D1074–D1082. doi:10.1093/nar/gkx1037
35. Martinez-Taboada VM, Cabeza R, Cacho PM, Blanco R, Rodriguez-Valverde V. Cloxacillin-based therapy in severe septic bursitis: retrospective study of 82 cases. Joint Bone Spine. 2009;76(6):665–669. doi:10.1016/j.jbspin.2009.04.003
36. Courjon J, Garzaro M, Roger PM, et al. A population pharmacokinetic analysis of continuous infusion of cloxacillin during Staphylococcus aureus bone and joint infections. Antimicrob Agents Chemother. 2020;64(12). doi:10.1128/AAC.01562-20.
37. Gower PE, Dash CH. Cephalexin: human studies of absorption and excretion of a new cephalosporin antibiotic. Br J Pharmacol. 1969;37(3):738–747.
38. FDA Approved Drug Products: KEFLEX®(cephalexin) capsules. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2006/050405s097lbl.pdf. Accessed December 31, 2021.
39. Jalava S, Saarimaa H, Elfving R. Cephalexin levels in serum, synovial fluid and joint tissues after oral administration. Scand J Rheumatol. 1977;6(4):250–252. doi:10.3109/03009747709095460
40. Julie Autmizguine M, Watt KM, Théorêt Y, Kassir N, Laferrière C. Stefan parent bruce tapiéro and philippe ovetchkine. pharmacokinetics and pharmacodynamics of oral cephalexin in children with osteoarticular infections. Pediatr Infect Dis J. 2013;32(12):1340–1344. doi:10.1097/INF.0b013e3182a222a6
41. Gwee A, Autmizguine J, Curtis N, Duffull SB. Twice- and thrice-daily cephalexin dosing for staphylococcus aureus infections in children. Pediatr Infect Dis J. 2020;39(6):519–522. doi:10.1097/INF.0000000000002646
42. Spížek J, Řezanka T. Lincosamides: chemical structure, biosynthesis, mechanism of action, resistance, and applications. Biochem Pharmacol. 2017;133:20–28. doi:10.1016/j.bcp.2016.12.001
43. Curis E, Pestre V, Jullien V, et al. Pharmacokinetic variability of clindamycin and influence of rifampicin on clindamycin concentration in patients with bone and joint infections. Infection. 2015;43(4):473–481. doi:10.1007/s15010-015-0773-y
44. Bouazza N, Pestre V, Jullien V, et al. Population pharmacokinetics of clindamycin orally and intravenously administered in patients with osteomyelitis. Br J Clin Pharmacol. 2012;74(6):971–977. doi:10.1111/j.1365-2125.2012.04292.x
45. Pietsch F, Bergman JM, Brandis G, et al. Ciprofloxacin selects for RNA polymerase mutations with pleiotropic antibiotic resistance effects. J Antimicrob Chemother. 2017;72(1):75–84. doi:10.1093/jac/dkw364
46. Varshney A, Ansari Y, Zaidi N, et al. Analysis of binding interaction between antibacterial ciprofloxacin and human serum albumin by spectroscopic techniques. Cell Biochem Biophys. 2014;70(1):93–101. doi:10.1007/s12013-014-9863-1
47. Sisto F, Bonomi A, Cavicchini L, et al. Human mesenchymal stromal cells can uptake and release ciprofloxacin, acquiring in vitro anti-bacterial activity. Cytotherapy. 2014;16(2):181–190. doi:10.1016/j.jcyt.2013.11.009
48. Seral C, Van Bambeke F, Tulkens PM. Quantitative analysis of gentamicin, azithromycin, telithromycin, ciprofloxacin, moxifloxacin, and oritavancin (LY333328) activities against intracellular Staphylococcus aureus in mouse J774 macrophages. Antimicrob Agents Chemother. 2003;47(7):2283–2292. doi:10.1128/AAC.47.7.2283-2292.2003
49. Landersdorfer CB, Kinzig M, Hohl R, Kempf P, Nation RL, Sorgel F. Physiologically based population pharmacokinetic modeling approach for ciprofloxacin in bone of patients undergoing orthopedic surgery. ACS Pharmacol Transl Sci. 2020;3(3):444–454. doi:10.1021/acsptsci.0c00045
50. Zahr N, Urien S, Aubry A, et al. Ciprofloxacin population pharmacokinetics during long-term treatment of osteoarticular infections. J Antimicrob Chemother. 2021;76(11):2906–2913. doi:10.1093/jac/dkab275
51. Norrby SR. Levofloxacin. Expert Opin Pharmacother. 1999;1(1):109–119. doi:10.1517/14656566.1.1.109
52. FDA Approved Drug Products: levaquin (levofloxacin) oral tablets. Available from: https:// www.accessdata.fda.gov/ drugsatfda_docs/ label/2019/020634s071lbl.pdf. Accessed December 31, 2021.
53. Rimmelé T, Boselli E, Breilh D, et al. Diffusion of levofloxacin into bone and synovial tissues. J Antimicrob Chemother. 2004;53(3):533–535. doi:10.1093/jac/dkh110
54. Marongiu G, Conte M, Verderosa V, et al. Late onset periprosthetic joint infection of the knee caused by Streptococcus anginosus. Case presentation and literature review. J Infect Dev Ctries. 2021;15(3):436–441. doi:10.3855/jidc.12326
55. Eloy G, Lebeaux D, Launay M, et al. Influence of renal function and age on the pharmacokinetics of levofloxacin in patients with bone and joint infections. Antibiotics. 2020;9(7). doi:10.3390/antibiotics9070401.
56. Cluzel RA, Lopitaux R, Sirot J, Rampon S. Rifampicin in the treatment of osteoarticular infections due to staphylococci. J Antimicrob Chemother. 1984;13(suppl_C):23–29. doi:10.1093/jac/13.suppl_C.23
57. Marsot A, Ménard A, Dupouey J, Muziotti C, Guilhaumou R, Blin O. Population pharmacokinetics of rifampicin in adult patients with osteoarticular infections: interaction with fusidic acid. Br J Clin Pharmacol. 2017;83(5):1039–1047. doi:10.1111/bcp.13178
58. Marsot A, Ménard A, Dupouey J, Allanioux L, Blin O, Guilhaumou R. Evaluation of current dosing guidance for oral rifampicin treatment in adult patients with osteoarticular infections. Br J Clin Pharmacol. 2020;86(11):2319–2324. doi:10.1111/bcp.14319
59. Andes D, Craig WA. In vivo pharmacodynamic activity of the glycopeptide dalbavancin. Antimicrob Agents Chemother. 2007;51(5):1633–1642. doi:10.1128/AAC.01264-06
60. FDA Approved product label: DALVANCE(dalbavancin). Available from: https://www.accessdata.fda.gov/ drugsatfda_docs/ label/2018/021883s007lbl.pdf. Accessed December 31, 2021.
61. Veve MP, Patel N, Smith ZA, Yeager SD, Wright LR, Shorman MA. Comparison of dalbavancin to standard-of-care for outpatient treatment of invasive gram-positive infections. Int J Antimicrob Agents. 2020;56(6):106210. doi:10.1016/j.ijantimicag.2020.106210
62. Fiore V, De Vito A, Aloisio A, et al. Dalbavancin two dose regimen for the treatment of prosthetic joint infections: new possible options for difficult to treat infectious diseases. Infect Dis. 2021;53(6):473–475. doi:10.1080/23744235.2021.1893898
63. Dunne MW, Puttagunta S, Sprenger CR, Rubino C, Van Wart S, Baldassarre J. Extended-duration dosing and distribution of dalbavancin into bone and articular tissue. Antimicrob Agents Chemother. 2015;59(4):1849–1855. doi:10.1128/AAC.04550-14
64. Cojutti PG, Rinaldi M, Zamparini E, et al. Population pharmacokinetics of dalbavancin and dosing consideration for optimal treatment of adult patients with staphylococcal osteoarticular infections. Antimicrob Agents Chemother. 2021;65(5): e02260–20. doi:10.1128/AAC.02260-20.
65. Safdar N, Andes D, Craig WA. In vivo pharmacodynamic activity of daptomycin. Antimicrob Agents Chemother. 2004;48(1):63–68. doi:10.1128/AAC.48.1.63-68.2004
66. FDA Approved Drug Products: CUBICIN (daptomycin) injection. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/021572s063,064lbl.pdf. Accessed December 31, 2021.
67. Montange D, Berthier F, Leclerc G, et al. Penetration of daptomycin into bone and synovial fluid in joint replacement. Antimicrob Agents Chemother. 2014;58(7):3991–3996. doi:10.1128/AAC.02344-14
68. Goutelle S, Roux S, Gagnieu MC, et al. Pharmacokinetic variability of daptomycin during prolonged therapy for bone and joint infections. Antimicrob Agents Chemother. 2016;60(5):3148–3151. doi:10.1128/AAC.02597-15
69. Bricca R, Goutelle S, Roux S, et al. Genetic polymorphisms of ABCB1 (P-glycoprotein) as a covariate influencing daptomycin pharmacokinetics: a population analysis in patients with bone and joint infection. J Antimicrob Chemother. 2019;74(4):1012–1020. doi:10.1093/jac/dky541
70. Garreau R, Bricca R, Gagnieu MC, et al. Population pharmacokinetics of daptomycin in patients with bone and joint infection: minimal effect of rifampicin co-administration and confirmation of a sex difference. J Antimicrob Chemother. 2021;76(5):1250–1257. doi:10.1093/jac/dkab006
71. Chen M, Nafziger AN, Drusano GL, Ma L, Bertino JS
72. Chambers J, Page-Sharp M, Salman S, et al. Ertapenem for osteoarticular infections in obese patients: a pharmacokinetic study of plasma and bone concentrations. Eur J Clin Pharmacol. 2019;75(4):511–517. doi:10.1007/s00228-018-2597-z
73. Goutelle S, Valour F, Gagnieu MC, Laurent F, Chidiac C, Ferry T. Population pharmacokinetics and probability of target attainment of ertapenem administered by subcutaneous or intravenous route in patients with bone and joint infection. J Antimicrob Chemother. 2018;73(4):987–994. doi:10.1093/jac/dkx477
74. Veganzones J, Montero A, Maseda E; Servicio de Anestesia UdCCQ, Hospital Universitario La Paz, Madrid. New evidence on the use of fosfomycin for bacteremia and infectious endocarditis. Rev Esp Quimioter. 2019;32(Suppl 1):25.
75. Lepak AJ, Zhao M, VanScoy B, et al. In vivo pharmacokinetics and pharmacodynamics of ZTI-01 (Fosfomycin for Injection) in the neutropenic murine thigh infection model against Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2017;61(6). doi:10.1128/AAC.00476-17.
76. Docobo-Perez F, Drusano GL, Johnson A, et al. Pharmacodynamics of fosfomycin: insights into clinical use for antimicrobial resistance. Antimicrob Agents Chemother. 2015;59(9):5602–5610. doi:10.1128/AAC.00752-15
77. Morata L, Soriano A. The role of fosfomycin in osteoarticular infection. Rev Esp Quimioter. 2019;32(Suppl1):30–36.
78. Schintler MV, Traunmuller F, Metzler J, et al. High fosfomycin concentrations in bone and peripheral soft tissue in diabetic patients presenting with bacterial foot infection. J Antimicrob Chemother. 2009;64(3):574–578. doi:10.1093/jac/dkp230
79. Tsegka KG, Voulgaris GL, Kyriakidou M, Kapaskelis A, Falagas ME. Intravenous fosfomycin for the treatment of patients with bone and joint infections: a review. Expert Rev Anti Infect Ther. 2021;1–11. doi:10.1080/14787210.2021.1932463
80. Rinaldi M, Cojutti PG, Zamparini E, et al. Population pharmacokinetics and Monte Carlo simulation for dosage optimization of fosfomycin in the treatment of osteoarticular infections in patients without renal dysfunction. Antimicrob Agents Chemother. 2021;65(5). doi:10.1128/AAC.02038-20.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.