")
Back to Journals » Journal of Pain Research » Volume 13
Mirogabalin in Japanese Patients with Renal Impairment and Pain Associated with Diabetic Peripheral Neuropathy or Post-Herpetic Neuralgia: A Phase III, Open-Label, 14-Week Study
Authors Baba M, Takatsuna H, Matsui N, Ohwada S
Received 24 March 2020
Accepted for publication 23 June 2020
Published 17 July 2020 Volume 2020:13 Pages 1811—1821
DOI https://doi.org/10.2147/JPR.S255345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Masayuki Baba,1 Hiroshi Takatsuna,2 Norimitsu Matsui,3 Shoichi Ohwada4
1Aomori Prefectural Central Hospital, Aomori, Japan; 2Medical Science Department, Daiichi Sankyo Co., Ltd., Tokyo, Japan; 3Clinical Development Department, Daiichi Sankyo Co., Ltd., Tokyo, Japan; 4Biostatistics and Data Management Department, Daiichi Sankyo Co., Ltd., Tokyo, Japan
Correspondence: Hiroshi Takatsuna
Medical Science Department, Daiichi Sankyo Co., Ltd., Tokyo 103-8425, Japan
Tel +81 3-6225-1053
Fax +81 3-6225-1959
Email [email protected]
Purpose: Mirogabalin was recently approved in Japan for the treatment of peripheral neuropathic pain, based on data from clinical trials in diabetic peripheral neuropathic pain (DPNP) and post-herpetic neuralgia (PHN), common clinical conditions which cause intense distress for patients. We characterized the safety and tolerability of mirogabalin in Japanese patients with renal impairment.
Patients and Methods: This multicenter, open-label study (ClinicalTrials.gov identifier NCT02607280) enrolled renally impaired individuals aged ≥ 20 years diagnosed with DPNP or PHN, and with an average daily pain score (ADPS) of ≥ 4 over the 7 days prior to treatment initiation. Mirogabalin dosage was titrated for 2 weeks, followed by a fixed dose for 12 weeks according to degree of renal impairment: 7.5 mg twice daily for moderate impairment and 7.5 mg once daily for severe impairment. The primary endpoint was safety and tolerability of mirogabalin, evaluated via treatment-emergent adverse events (TEAEs). Secondary efficacy endpoints included change in ADPS from baseline to Week 14.
Results: Overall, 35 patients were enrolled (30 with moderate and 5 with severe renal impairment). Most TEAEs were mild or moderate in severity; the most commonly reported were nasopharyngitis (22.9%) and somnolence (11.4%). Only 4 patients (11.4%) discontinued treatment due to TEAEs. Mirogabalin significantly decreased ADPS from baseline in patients with renal impairment; least squares mean change from baseline at Week 14 was − 1.9 (95% confidence interval: − 2.8, − 1.0).
Conclusion: Mirogabalin was well tolerated and significantly reduced pain levels when used to treat DPNP/PHN at a fixed dose of 7.5 mg once or twice daily in patients with renal impairment.
Keywords: peripheral neuropathic pain, mirogabalin, creatinine clearance, dose adjustment, safety, tolerability
Introduction
Neuropathic pain is a common clinical problem, affecting approximately 1 in 10 of the general population, and is associated with a number of underlying conditions, including diabetes mellitus, infection, surgery, and cancer.1,2 The symptoms may include burning pain, sensations of pressure, electric shock, or stabbing pain, and mechanical allodynia.3 Neuropathic pain causes intense distress for patients, and is commonly associated with depression, anxiety, and sleep disturbances.4,5
Despite the high prevalence of conditions such as diabetic peripheral neuropathic pain (DPNP) and post-herpetic neuralgia (PHN), treatment remains challenging and patient dissatisfaction is high.6,7 Current therapeutic recommendations include antidepressants (duloxetine), anticonvulsants (pregabalin, gabapentin), topical analgesics (lidocaine, capsaicin), and even opioids (tapentadol).2,8,9 However, not all of these agents are approved for treatment by regulatory authorities; of those that are approved, optimal administration may be compromised by the occurrence of adverse events (AEs), and efficacy is limited.10,11 Polypharmacy and off-label treatment is common,12 but can be risky for patients, especially for the elderly, who may have additional comorbidities.13
Mirogabalin besylate (herein referred to as mirogabalin; Daiichi Sankyo Co., Ltd., Tokyo, Japan) was developed for the treatment of peripheral neuropathic pain (PNP), which includes DPNP and PHN, and was recently approved in Japan as monotherapy for adults with PNP.14 It is an orally administered gabapentinoid which acts via α2δ calcium channel subunits to modulate pain transmission and processing.15 In a Phase II study in patients with DPNP in the United States, mirogabalin provided statistically significant reductions in average daily pain score (ADPS) and a clinically meaningful effect, compared with placebo.16 In a recently published Phase III, randomized, controlled trial (RCT) in Asian patients with DPNP, mirogabalin (30 mg/day) provided significant pain relief vs placebo and was well tolerated.17 In a second Phase III RCT, in Asian patients with PHN, mirogabalin efficacy was superior to placebo at all doses tested (15, 20, or 30 mg/day), with no new safety signals.18
PNP is common in the elderly, with an increased prevalence of both DPNP and PHN associated with increasing age.19,20 Since renal function is also often impaired in elderly patients,21,22 mirogabalin could, potentially, be widely used by PNP patients with renal impairment. Findings from a single-dose clinical pharmacology study in healthy individuals with varying degrees of renal function indicated that mirogabalin was excreted primarily in the urine, and that the pharmacokinetic parameters were affected by renal function. The area under the plasma concentration–time curve up to the last quantifiable time (AUClast) increased with the severity of renal impairment; compared with individuals with normal renal function, the geometric least squares mean was 1.9 and 3.6 for subjects with moderate and severe renal impairment, respectively.23 Based on these data, a dose reduction of 50% to 75% was deemed necessary in individuals with moderate or severe renal impairment. Thus, the objective of this study was to characterize the safety and tolerability of an adjusted dose of mirogabalin in patients with moderate or severe renal impairment.
Patients and Methods
Study Design
This was a multicenter, open-label study (ClinicalTrials.gov identifier NCT02607280) conducted at 35 centers in Japan between January 21, 2016, and March 1, 2017 (Figure 1). A full list of study investigators and institutions is provided as Appendix 1. No randomization was performed, but patients were enrolled in this study using an interactive web response system according to degree of renal impairment. All study medication was supplied to patients by the investigator at each study site.
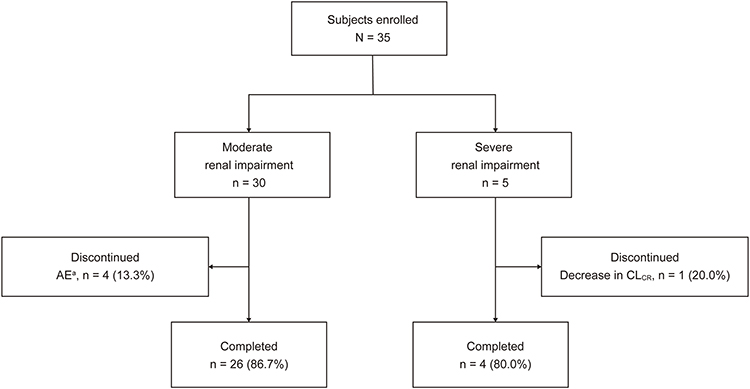 |
Figure 1 Patient disposition. Note: aOne event each of angina pectoris, hepatitis E, myelitis, and somnolence. Abbreviations: AE, adverse event; CLCR, creatinine clearance. |
The study duration per patient was approximately 16 weeks (comprising a 1-week observation period, a 2-week titration period, a 12-week fixed-dose period, and a 1-week follow-up period) (Figure 2). Patients using prohibited concomitant medications or prohibited concomitant therapies were required to undergo a ≥7-day washout period prior to screening.
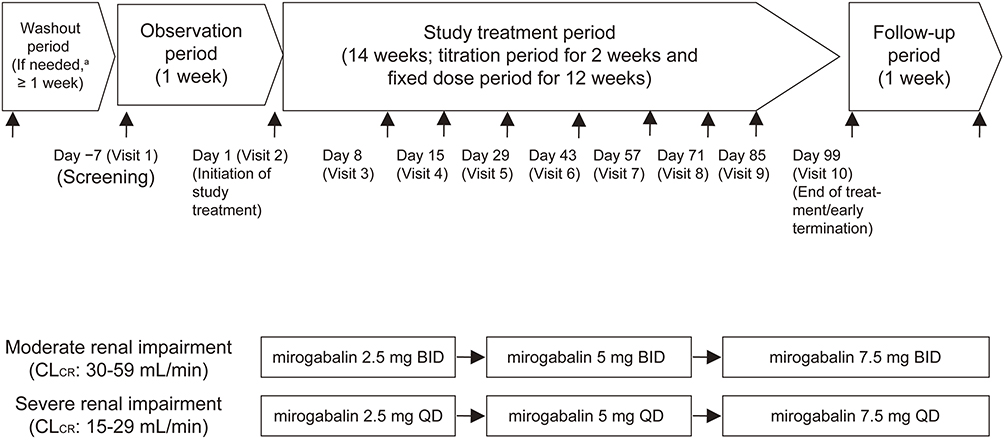 |
Figure 2 Study design. Notes: aAfter obtaining informed consent, patients who were treated with prohibited concomitant medications (DPNP and PHN) or prohibited concomitant therapies (PHN) underwent a washout period of ≥7 days. Abbreviations: BID, twice daily; CLCR, creatinine clearance; DPNP, diabetic peripheral neuropathic pain; PHN, post-herpetic neuralgia; QD, once daily. |
Patients
Eligible patients were aged ≥20 years, with DPNP (defined as type 1 or type 2 diabetes mellitus at screening and painful distal symmetric polyneuropathy, diagnosed at least 6 months prior to screening) or PHN (defined as pain present for 3 months or more after herpes zoster skin rash at screening). The DPNP assessment was conducted in accordance with the simplified diagnostic criteria for diabetic neuropathy established in Japan, and the diagnosis was made by a trained physician. At screening, patients were required to have creatinine clearance (CLCR; Cockcroft-Gault equation24) 15–59 mL/min, and a pain score of ≥40 mm but <90 mm on the visual analog scale (VAS) of the short-form McGill Pain Questionnaire (SF-MPQ).25 At initiation of study treatment, patients were required to have an SF-MPQ VAS score of ≥40 mm and <90 mm, plus completion of at least 4 days of daily electronic patient diaries (for pain) and ADPS of ≥4 (on an 11-point numerical rating scale) over the prior 7 days.
Key exclusion criteria for patients with DPNP were glycated hemoglobin (HbA1c) >10.0% at screening (in accordance with the National Glycohemoglobin Standardization Program); uncontrolled blood glucose that could necessitate changes in diabetes treatment during the study; any lower limb amputation (with the exception of toes); and a change in restricted concomitant medications (Appendix 2) within 30 days prior to screening. Key exclusion criteria for patients with PHN were prior neurolytic block or neurosurgery for PHN; a change in restricted concomitant medications (Appendix 2) within 14 days prior to screening; and known immunocompromised status.
Additional exclusion criteria which applied to all patients were ADPS ≥9 during the observation period; any non-DPNP/PHN-related severe pain or neurologic disorder, or skin conditions, that could confound the assessment of DPNP or PHN; hemodialysis, acute renal failure or a history of kidney transplant; suicidality (assessed using the Mini-international Neuropsychiatric Interview [MINI; version 6.0]26 and the Columbia-Suicide Severity Rating Scale [C-SSRS]27) at screening; current or previous history of major psychiatric disorder, malignancy (except for basal cell carcinoma), pernicious anemia, untreated hypothyroidism, or any other clinically significant illness; hepatitis B or C or human immunodeficiency virus positive; prior treatment with drugs that could cause irreversible retinal degeneration; use of prohibited concomitant therapies (Appendix 2) within 7 days prior to screening; drug or alcohol abuse within 12 months prior to screening; participation in another clinical study within 30 days of screening or in any previous mirogabalin clinical study; hypersensitivity to, or previous lack of efficacy with, pregabalin or gabapentin; pregnancy, lactation, or unwillingness to use contraception; any other clinical or laboratory finding that rendered the subject ineligible at the discretion of the investigator.
Treatment
Mirogabalin dose levels are expressed as the free form. Patients with moderate renal impairment (CLCR 30–59 mL/min) received mirogabalin 2.5 mg twice daily (BID) for the first week of the titration period and 5 mg BID for the second week, followed by a fixed dose of 7.5 mg BID for 12 weeks. Patients with severe renal impairment (CLCR 15–29 mL/min) received mirogabalin 2.5 mg once daily (QD) for the first week of the titration period and 5 mg QD for the second week, followed by a fixed dose of 7.5 mg QD for 12 weeks. Based on the results of a prior study in healthy Japanese subjects individuals with varying degrees of renal function,23 Phase III studies in Asian patients,17,18 plus modeling and simulation analyses,28 the dosages of 7.5 mg BID in patients with moderate renal impairment and 7.5 mg QD in patients with severe impairment administered in this study were expected to produce exposures equivalent to 15 mg BID in patients with normal renal function.
Study Endpoints and Measurements
The primary endpoint was safety and tolerability of mirogabalin in patients with renal impairment. Evaluations included AEs; laboratory assessments, vital signs, and electrocardiogram; body weight; Hospital Anxiety and Depression Scale (HADS)29 and C-SSRS;27 and neurologic examination (gait/station and muscle strength).
Secondary study endpoints included the effect of mirogabalin on ADPS; ADPS responder rate (defined as the percentage of patients with ≥30% and ≥50% reduction from baseline to Week 14); results of pain questionnaires (SF-MPQ:25 sensory, affective, and total subscales, VAS, present pain intensity); impact on sleep interference (based on the average daily sleep interference score [ADSIS]); and patient global impression of change (PGIC) in pain.30
AEs were recorded throughout the duration of the study and follow-up period, regardless of perceived relationship to the study drug. AEs were coded using the Medical Dictionary for Regulatory Activities Version 17.1. Treatment-emergent AEs (TEAEs) were defined as any AE that emerged during study treatment (having been absent prior to treatment) or worsened relative to the pre-treatment state. Adverse drug reactions (ADRs; defined as TEAEs considered to be related to the study drug) were evaluated as any AE for which a causal relationship to the study drug could not be ruled out, according to the International Conference on Harmonisation Tripartite Guideline E2A. Pain and sleep interference were recorded in the electronic patient diary once daily (upon awakening, prior to receiving study drug) from the day after the screening visit to the end of treatment/early termination visit. The subject selected the number describing their pain over the past 24 hours on a scale of 0 (no pain) to 10 (worst possible pain); weekly mean ADPS was calculated using these scores. The subject selected the number describing how their pain had interfered with sleep over the past 24 hours on a scale of 0 (no interference) to 10 (complete interference); weekly mean ADSIS was calculated using these scores. Most other efficacy parameters were measured weekly.
Statistical Analysis
The sample size of 35 patients was determined to provide >95% probability that at least one AE of moderate/severe dizziness and somnolence was observed, assuming the true AE rate was 10%. Both the safety and efficacy analysis sets included all enrolled patients who received at least one dose of study drug.
TEAEs and ADRs were summarized as a frequency table. Missing weekly ADPS data were handled using the multiple imputation (MI) method. In the MI data generation, the Markov Chain Monte Carlo method with age, sex, and CLCR group as covariates, was used to produce a monotone missing data pattern, followed by regression with predictive mean matching (REGPMM) with the same set of covariates applied to the monotone missing data. A pattern mixture model with different shift parameters according to reasons for study discontinuation (AE, lack of efficacy or other reason) was applied to the imputed weekly ADPS data by REGPMM to impose a penalty on the study discontinuation under a missing, not at random, mechanism.31 To estimate the change from baseline in ADPS at Week 14 for each CLCR group, a mixed-effects model with repeated measures (MMRM), which included CLCR group, week and CLCR group-by-week as fixed effects and baseline ADPS as a covariate, was used for the imputed datasets.32 The results of MMRM analysis from each imputed dataset were combined using Rubin’s rule.33 ADPS responder rates (≥30% and ≥50% improvement in ADPS) at Week 14 were calculated. Those patients who discontinued the study were considered non-responders and a last observation carried forward (LOCF) approach was used for the imputation for patients who completed the study but did not have week 14 ADPS. Continuous responder analysis,34 representing cumulative distribution of the percent reduction from baseline in ADPS, was provided. For SF-MPQ and ADSIS, the changes from baseline at Week 14 were summarized using the LOCF approach. PGIC was also tabulated.
All statistical analyses were performed using Statistical Analysis Software®, Version 9.3 (SAS Institute, Cary, NC, USA).
Results
Patients
Overall, 35 patients were enrolled (30 with moderate renal impairment and 5 with severe renal impairment), received at least one dose of study drug, and were included in the safety and efficacy analysis sets.
Subject disposition is shown in Figure 1. Four patients with moderate renal impairment discontinued treatment due to AEs: one event each of angina pectoris (severe, not deemed by the investigator to be related to the study drug), hepatitis E (mild, not related to the study drug), myelitis (mild, not related to the study drug), and somnolence (moderate, related to the study drug). All four AEs were reported as resolved/resolving subsequent to treatment cessation. One subject with severe renal impairment discontinued due to a decrease in CLCR <15 mL/min (a prespecified discontinuation criterion); no patients in this group discontinued due to AEs.
Baseline demographic and clinical characteristics are shown in Table 1. Six patients (17.1%) had PHN, and 29 (82.9%) had DPNP. All patients with DPNP had type 2 diabetes, no patients with type 1 diabetes were enrolled. All patients with severe renal impairment had DPNP. Overall, the mean (standard deviation [SD]) age was 73.4 (7.3) years, and the majority (80.0%) of patients were male. Mean baseline ADPS was 5.7 (1.1) and mean SF-MPQ VAS scores at screening and at initiation of treatment were 58.2 (9.4) and 59.6 (9.6), respectively. Characteristics were similar between the two renal impairment groups, with the exception of baseline CLCR, which was 51.8 (9.6) mL/min in patients with moderate impairment and 22.0 (6.2) mL/min in patients with severe impairment.
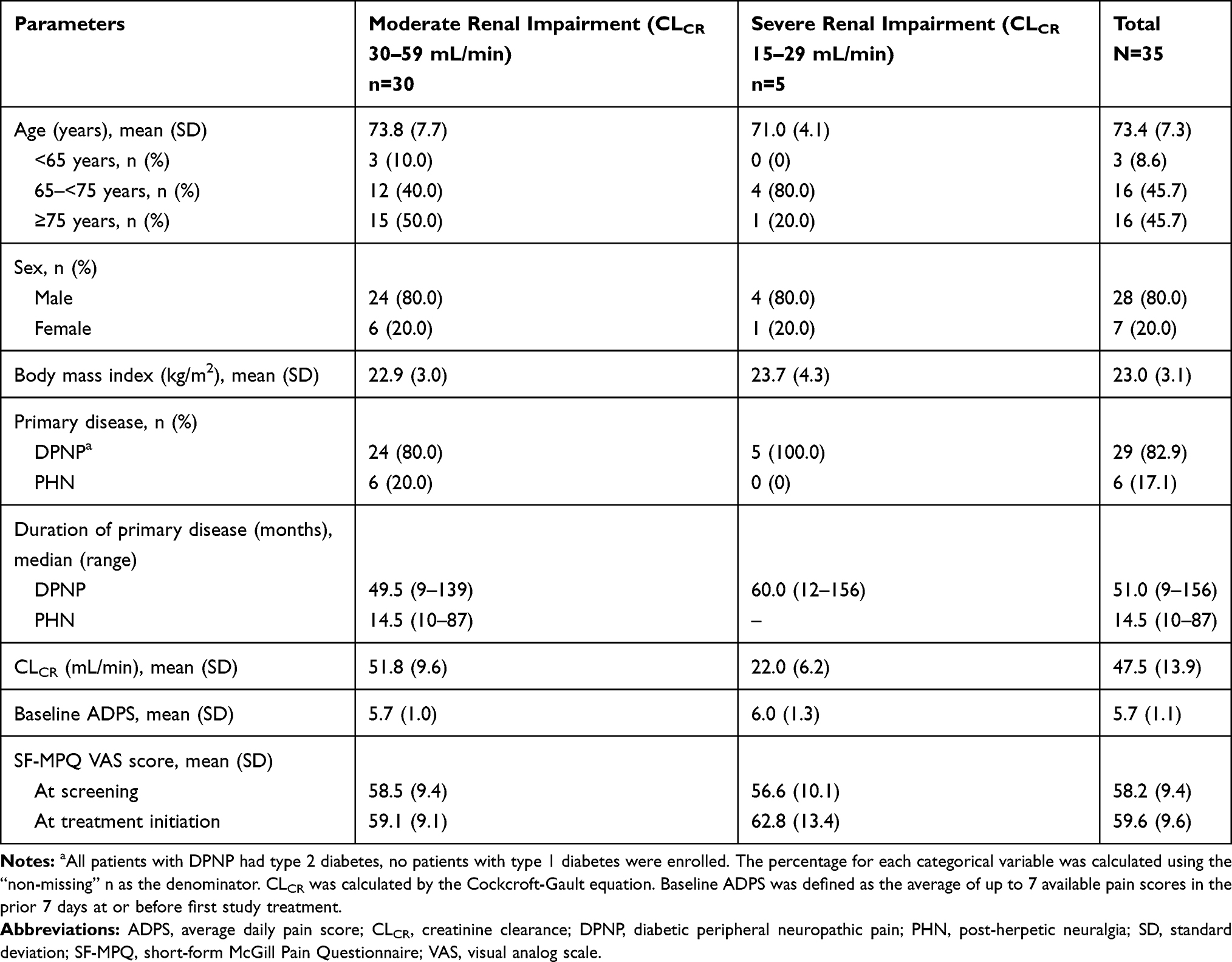 |
Table 1 Demographic and Other Baseline Characteristics (Safety Analysis Set) |
Safety Outcomes
The median treatment duration was 98.0 days in patients with moderate renal impairment and 97.0 days in patients with severe renal impairment. The mean treatment compliance rate was high: 99.9% in patients with moderate renal impairment and 78.7% in patients with severe renal impairment (primarily due to the subject who discontinued treatment due to meeting a prespecified discontinuation criterion: a decrease in CLCR <15 mL/min).
The overall incidence of TEAEs was 82.9% (29/35 patients) (Table 2); all were mild or moderate in severity with the exception of one severe TEAE (angina pectoris, considered unrelated to the study drug) reported in a subject with moderate renal impairment. Serious TEAEs were reported in one subject (3.3%; angina pectoris) with moderate renal impairment, but in no subject with severe impairment. Only four patients (11.4%) discontinued due to TEAEs; all were in the moderate renal impairment group. No deaths were reported during the study.
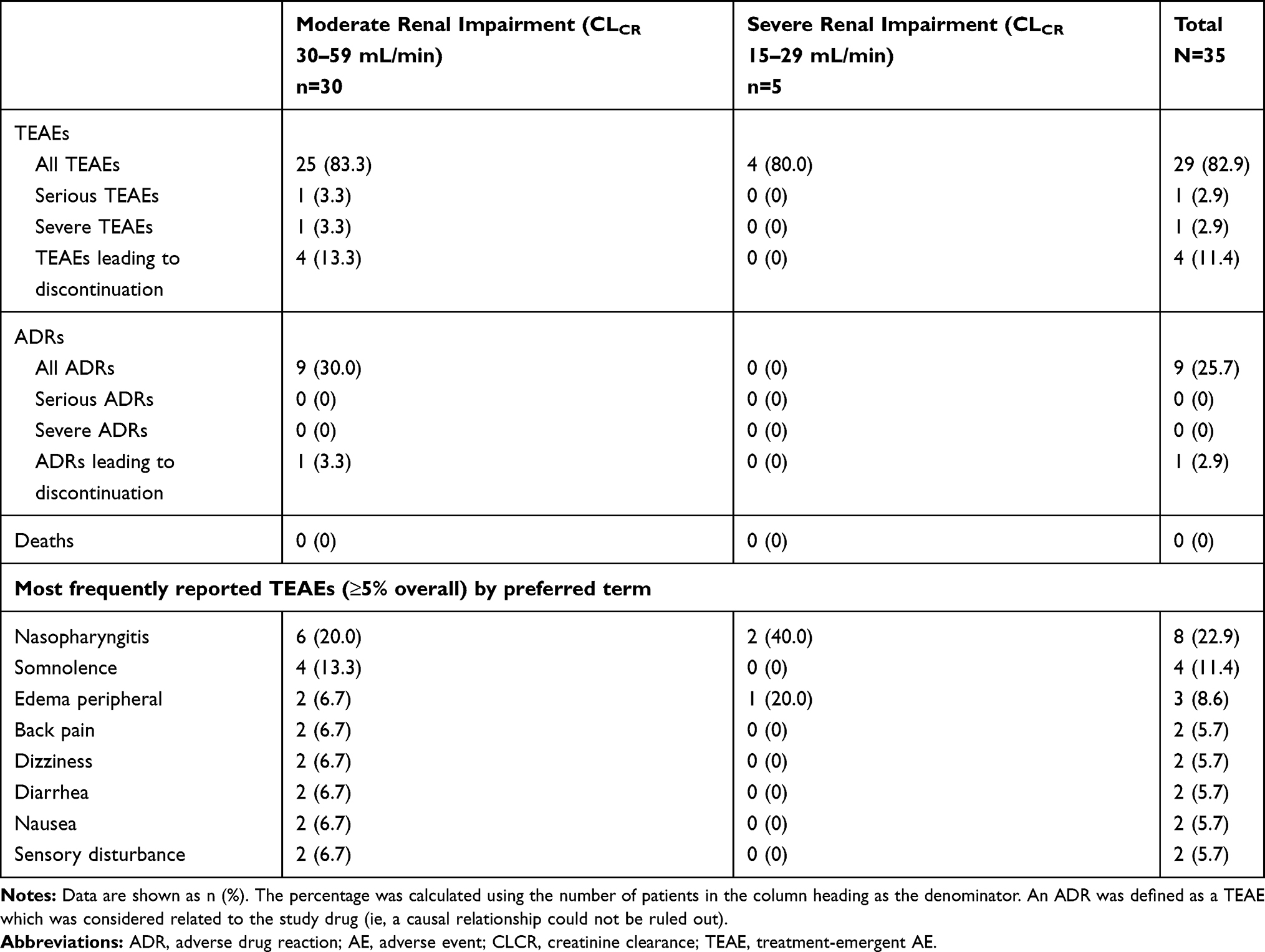 |
Table 2 Summary of TEAEs and ADRs (Safety Analysis Set) |
The most commonly reported TEAEs were nasopharyngitis (22.9% [8/35]), somnolence (11.4% [4/35]), and edema peripheral (8.6% [3/35]) (Table 2). ADRs occurred in 25.7% (9/35) of patients overall; this included 30.0% (9/30) of patients with moderate renal impairment and 0% of patients with severe impairment. The most common ADRs were somnolence (11.4% [4/35]) and dizziness (5.7% [2/35]). No suicide-related TEAEs were reported. At Week 14, no clinically significant changes from baseline were found in the HADS subscales of depression and anxiety. In addition, no clinically significant changes or trends over time were found in any physical or neurological examination data or laboratory test values.
Efficacy Outcomes
The mean baseline ADPS was 5.7 overall (5.7 and 6.0 in patients with moderate and severe renal impairment, respectively). The least squares mean change from baseline in the imputed ADPS at Week 14 for the 35 renally impaired patients was −1.9 [95% confidence interval [CI] −2.8, −1.0]; by group, the changes were −1.8 (95% CI −2.5, −1.1) in patients with moderate renal impairment and −2.1 (95% CI −3.8, −0.4) in patients with severe renal impairment (Table 3). Most of the missing values of ADPS occurred due to AE-related discontinuations (four due to AEs and one due to reduction in CLCR <15 mL/min). No trends were found related to the timing of discontinuations. Mirogabalin significantly decreased the ADPS at Week 14 from baseline in both renal impairment groups (Figure 3).
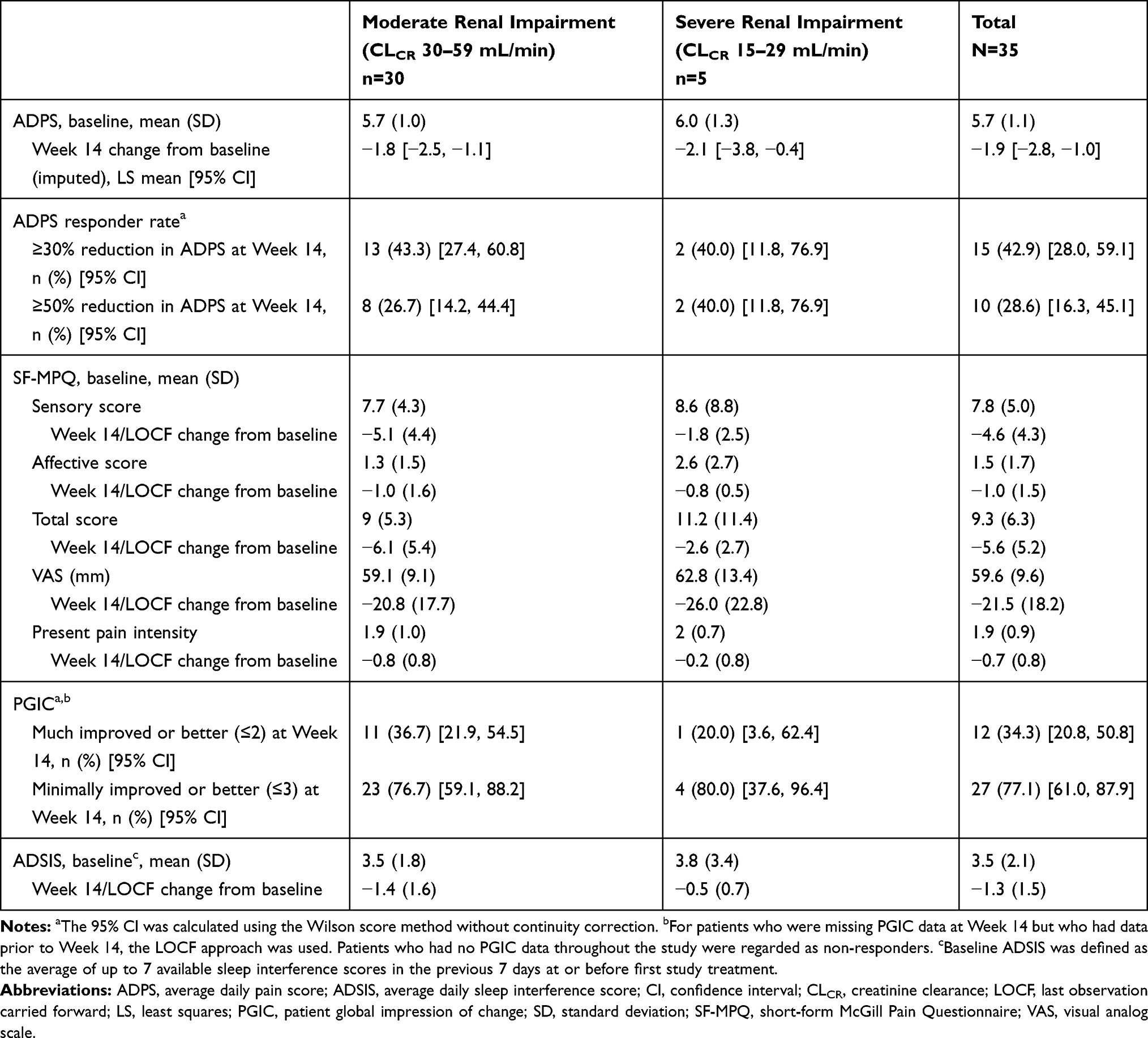 |
Table 3 Efficacy Outcomes (Efficacy Analysis Set) |
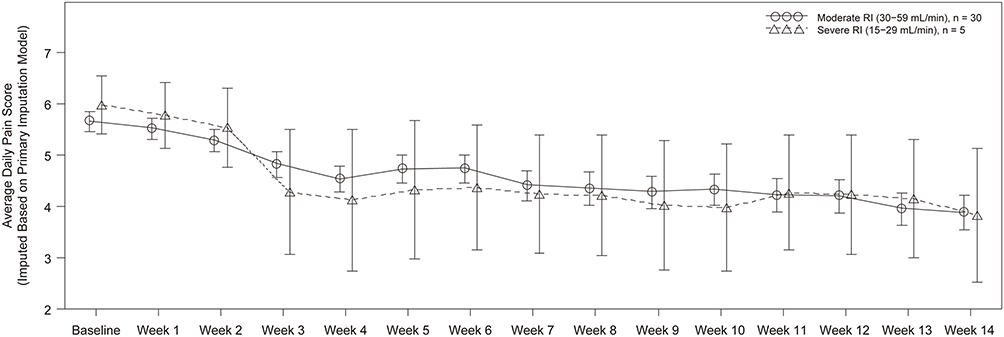 |
Figure 3 Time course of average daily pain scoresa (efficacy analysis set). Notes: aData are shown as least squares mean ± SE. The MI method using pattern mixture model with different shifting parameters according to the reason for treatment discontinuation was applied. The MMRM with CLCR group, week and CLCR group-by-week as fixed effects and baseline ADPS as a covariate was performed to estimate the least squares means and the corresponding SE for each week. Abbreviations: ADPS, average daily pain score; CLCR, creatinine clearance; MI, multiple imputation; MMRM, mixed-effects model with repeated measures; RI, renal impairment; SE, standard error. |
At Week 14, 42.9% (15/35) of patients achieved a ≥30% reduction from baseline in ADPS; this equated to 43.3% (13/30) of patients with moderate renal impairment and 40.0% (2/5) of patients with severe renal impairment. At Week 14, 28.7% (10/35) of patients achieved a ≥50% reduction from baseline in ADPS; this included 26.7% (8/30) of patients with moderate renal impairment and 40.0% (2/5) of patients with severe renal impairment (Table 3).
The results of the SF-MPQ are also shown in Table 3. For the VAS score, the mean (SD) changes from baseline at Week 14 were −20.8 (17.7) in patients with moderate impairment and −26.0 (22.8) in patients with severe impairment. For the total score, the mean (SD) changes from baseline at Week 14 were −6.1 (5.4) and −2.6 (2.7) in patients with moderate and severe impairment, respectively. The difference between groups was largely driven by changes in the sensory score.
At Week 14, the percentage of patients with a PGIC score of much improved or better (score ≤2) was 36.7% (11/30) in patients with moderate renal impairment and 20.0% (1/5) in patients with severe impairment. At Week 14, the percentage of patients with a PGIC score of minimally improved or better (score ≤3) was 76.7% (23/30) and 80.0% (4/5), respectively (Table 3).
The mean (SD) changes from baseline in ADSIS at Week 14 were −1.4 (1.6) in patients with moderate renal impairment and −0.5 (0.7) in patients with severe impairment (Table 3).
Discussion
Despite the fact that PNP (including DPNP and PHN) is highly prevalent in the general population, treatment for these conditions is often suboptimal,6,7 and patient dissatisfaction remains high.35,36 The orally administered gabapentinoid mirogabalin was recently approved for the treatment of PNP in Japan, and the results of Phase III RCTs demonstrated that mirogabalin was able to provide significant pain relief and was generally well tolerated.17,18
This study aimed to characterize mirogabalin in patients with renal impairment, a characteristic common in the elderly patients who will likely make up a large proportion of mirogabalin users. The results indicate that mirogabalin was safe and well tolerated in patients with DPNP or PHN and renal impairment when used at a fixed dose of 7.5 mg BID (moderate renal impairment) or 7.5 mg QD (severe renal impairment).
The key finding from our study in patients with renal impairment was that the safety outcomes in this population were comparable with those from non-impaired patients in the Phase III studies, with no new safety signals. In the Phase III studies in DPNP17 and PHN,18 the most frequently reported TEAEs with mirogabalin 15 mg BID were nasopharyngitis (16.4% and 12.9%, respectively), somnolence (14.5% and 23.9%), and dizziness (10.9% and 15.5%). While the frequency of nasopharyngitis was slightly increased in our study (22.9%), rates of somnolence (11.4%) and dizziness (5.7%) were slightly lower. Treatment compliance in our study was high, and most TEAEs were mild or moderate in severity. Discontinuations due to TEAEs were low (11.4%), and consistent with discontinuation rates due to TEAEs observed with mirogabalin 15 mg BID in the Phase III studies (9.7%17 and 7.7%18).
In addition, despite the reduced dosages, mirogabalin significantly decreased ADPS, reduced ADSIS, and improved PGIC scores over 14 weeks of treatment. The least squares mean reduction in ADPS of −1.9 at Week 14 in this study was consistent with the improvements reported in the recent Phase III studies,17,18 although differences in study design and population size mean that comparisons should be made with caution. For patients without moderate or severe renal impairment receiving mirogabalin 15, 20, and 30 mg/day, the least squares mean changes in ADPS at Week 14 were −1.6, −1.7, and −2.0, respectively, in the DPNP study17 and −1.3, −1.5 and −1.8, respectively, in the PHN study.18
Dosage adjustment for renally impaired individuals is often necessary for therapeutic agents which are renally excreted, and regulatory authorities recommend pharmacokinetic evaluation during clinical development.37 The doses used in this study were selected to produce exposures equivalent to those observed in patients with normal renal function receiving mirogabalin 15 mg BID, based on previously published data.17,18,23,28 The requirement for a reduced dosage of mirogabalin in patients with renal impairment was not unexpected, given that reduced dosages are also recommended for the gabapentinoids pregabalin38 (indicated for DPNP and PHN in the US38 and for neuropathic pain in Japan39) and gabapentin (approved for PHN in the US)40 in this context. It is worth noting, however, that duloxetine (indicated in the US for DPNP) is contraindicated for use in patients with severe renal impairment.41
Since this was an uncontrolled study in patients with renal impairment, it was deemed necessary to be able to compare safety outcomes with a control group of patients with relatively normal renal function. The prior Phase III RCTs of mirogabalin in patients with DPNP and PHN, which enrolled patients without moderate or severe renal impairment,17,18 provided a suitable historical control population. Background factors of the patients in our study, such as ADPS at baseline (5.7), mean age (73.4 years), and duration of DPNP (51.0 months) or PHN (14.5 months) were broadly consistent with those of patients in the Phase III DPNP study (5.6, 61.4 years, and 35.0 months, respectively)17 and the Phase III PHN study (5.7, 66.5 years, and 18.0 months, respectively).18 However, to facilitate inter-study comparisons, study designs must be similar. Since the Phase III studies utilized a 12-week fixed-dose period, in accordance with the recommendation from the European Medicines Agency,42 the current study was also designed with a 12-week fixed-dose period. In addition, taking subject safety into consideration, the current study incorporated a 2-week titration period prior to the fixed-dose period.
We recognize that our study has several limitations; namely, that it was an open-label study in which all patients were aware of their treatment regimen, and no directly comparable control cohort was enrolled. However, the use of a similar study design to the Phase III mirogabalin RCTs was intended to partially mitigate against this potential weakness, by allowing comparison of our study data with results from two larger, methodologically robust studies, thus placing our results into the wider context of therapeutic evidence for mirogabalin use. The small study size also potentially limits extrapolation of the data to the wider population of patients with DPNP or PHN, although the demographic data indicate that the patients enrolled in this analysis were representative of individuals seen in general practice. In particular, the small number of patients enrolled with severe renal impairment means that the study lacks statistical power to definitively demonstrate efficacy and safety in this population; although we consider that mirogabalin 7.5 mg QD can be safely administered and will provide benefit to patients with severe renal impairment, additional data are needed to confirm this. Despite these caveats, we believe that the data accruing from our study extend the evidence base for optimal mirogabalin use in special populations with PNP, and elucidate key therapeutic aspects for clinicians treating patients with neuropathic pain and renal impairment.
Conclusion
Mirogabalin was safe and well tolerated in patients with DPNP or PHN and renal impairment when used at a fixed dose of 7.5 mg QD (severe impairment) or 7.5 mg BID (moderate impairment). Furthermore, these reduced doses of mirogabalin were able to reduce pain from baseline to Week 14 in renally impaired patients with DPNP or PHN.
Abbreviations
ADPS, average daily pain score; ADSIS, average daily sleep interference score; AE, adverse event; AUClast, area under the plasma concentration–time curve up to the last quantifiable time; BID, twice daily; CLCR, creatinine clearance; C-SSRS, Columbia-Suicide Severity Rating Scale; DPNP, diabetic peripheral neuropathic pain; HADS, Hospital Anxiety and Depression Scale; HbA1c, glycated hemoglobin; LOCF, last observation carried forward; MI, multiple imputation; MINI, Mini-international Neuropsychiatric Interview; MMRM, mixed-effects model with repeated measures; PGIC, patient global impression of change; PHN, post-herpetic neuralgia; QD, once daily; RCT, randomized, controlled trial; REGPMM, regression with predictive mean matching; SD, standard deviation; SF-MPQ, short-form McGill Pain Questionnaire; TEAE, treatment-emergent adverse event; VAS, visual analog scale.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was conducted in compliance with the ethical principles that have their origin in the Declaration of Helsinki, the International Council for Harmonisation consolidated Guideline E6 for Good Clinical Practice (CPMP/ICH/135/95), and all applicable national and international regulatory requirements. The protocol, amendments, the informed consent forms, and information sheets were approved by the Institutional Review Boards at each participating study center. All patients provided written informed consent prior to initiation of any study procedures.
Acknowledgments
The authors wish to acknowledge editorial assistance provided by Sally-Anne Mitchell, PhD (McCANN HEALTH CMC), funded by Daiichi Sankyo Co., Ltd. (Tokyo, Japan). The authors also thank the study investigators (Appendix 1), and all participating patients and their families. Some data included in this manuscript were previously presented at the 53rd Annual Meeting of the Japan Pain Clinic Society, July 18–20, 2019, Kumamoto, Japan (Abstract J313).
Disclosure
All authors have received personal fees from Daiichi Sankyo Co., Ltd. HT, NM, and SO are employees of Daiichi Sankyo Co., Ltd. The authors report no other conflicts of interest in this work.
References
1. Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3(1):17002. doi:10.1038/nrdp.2017.2
2. Sumitani M, Sakai T, Matsuda Y, et al. Executive summary of the clinical guidelines of pharmacotherapy for neuropathic pain: second edition by the Japanese society of pain clinicians. J Anesth. 2018;32(3):463–478. doi:10.1007/s00540-018-2501-0
3. Truini A, Garcia-Larrea L, Cruccu G. Reappraising neuropathic pain in humans–how symptoms help disclose mechanisms. Nat Rev Neurol. 2013;9(10):572–582. doi:10.1038/nrneurol.2013.180
4. Ferini-Strambi L. Neuropathic pain and sleep: a review. Pain Ther. 2017;6(Suppl 1):19–23. doi:10.1007/s40122-017-0089-y
5. Descalzi G, Mitsi V, Purushothaman I, et al. Neuropathic pain promotes adaptive changes in gene expression in brain networks involved in stress and depression. Sci Signal. 2017;10(471):eaaj1549. doi:10.1126/scisignal.aaj1549
6. Hwang S, van Nooten F, Wells T, et al. Neuropathic pain: a patient-centred approach to measuring outcomes. Health Expect. 2018;21(4):774–786. doi:10.1111/hex.12673
7. Scholz J, Finnerup NB, Attal N, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
8. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
9. Amescua-Garcia C, Colimon F, Guerrero C, et al. Most relevant neuropathic pain treatment and chronic low back pain management guidelines: a change pain Latin America advisory panel consensus. Pain Med. 2018;19(3):460–470. doi:10.1093/pm/pnx198
10. Javed S, Alam U, Malik RA. Mirogabalin and emerging therapies for diabetic neuropathy. J Pain Res. 2018;11:1559–1566. doi:10.2147/JPR.S145999
11. Hadley GR, Gayle JA, Ripoll J, et al. Post-herpetic neuralgia: a review. Curr Pain Headache Rep. 2016;20(3):17. doi:10.1007/s11916-016-0548-x
12. Yang M, Qian C, Liu Y. Suboptimal treatment of diabetic peripheral neuropathic pain in the United States. Pain Med. 2015;16(11):2075–2083. doi:10.1111/pme.12845
13. Ali A, Arif AW, Bhan C, et al. Managing chronic pain in the elderly: an overview of the recent therapeutic advancements. Cureus. 2018;10(9):e3293.
14. Deeks ED. Mirogabalin: first global approval. Drugs. 2019;79(4):463–468. doi:10.1007/s40265-019-01070-8
15. Domon Y, Arakawa N, Inoue T, et al. Binding characteristics and analgesic effects of mirogabalin, a novel ligand for the alpha2delta subunit of voltage-gated calcium channels. J Pharmacol Exp Ther. 2018;365(3):573–582. doi:10.1124/jpet.117.247551
16. Vinik A, Rosenstock J, Sharma U, et al. Efficacy and safety of mirogabalin (DS-5565) for the treatment of diabetic peripheral neuropathic pain: a randomized, double-blind, placebo- and active comparator-controlled, adaptive proof-of-concept Phase 2 study. Diabetes Care. 2014;37(12):3253–3261. doi:10.2337/dc14-1044
17. Baba M, Matsui N, Kuroha M, Wasaki Y, Ohwada S. Mirogabalin for the treatment of diabetic peripheral neuropathic pain: a randomized, double-blind, placebo-controlled phase III study in Asian patients. J Diabetes Investig. 2019;10(5):1299–1306. doi:10.1111/jdi.13013
18. Kato J, Matsui N, Kakehi Y, Murayama E, Ohwada S, Sugihara M. Mirogabalin for the management of postherpetic neuralgia: a randomized, double-blind, placebo-controlled Phase 3 study in Asian patients. Pain. 2019;160(5):1175–1185. doi:10.1097/j.pain.0000000000001501
19. Zorzoli E, Pica F, Masetti G, Franco E, Volpi A, Gabutti G. Herpes zoster in frail elderly patients: prevalence, impact, management, and preventive strategies. Aging Clin Exp Res. 2018;30(7):693–702. doi:10.1007/s40520-018-0956-3
20. Pai YW, Lin CH, Lee IT, Chang MH. Prevalence and biochemical risk factors of diabetic peripheral neuropathy with or without neuropathic pain in Taiwanese adults with type 2 diabetes mellitus. Diabetes Metab Syndr. 2018;12(2):111–116. doi:10.1016/j.dsx.2017.09.013
21. Dutra MC, Uliano EJ, Machado DF, Martins T, Schuelter-Trevisol F, Trevisol DJ. Assessment of kidney function in the elderly: a population-based study. J Bras Nefrol. 2014;36(3):297–303. doi:10.5935/0101-2800.20140043
22. Schmitt R, Melk A. Molecular mechanisms of renal aging. Kidney Int. 2017;92(3):569–579. doi:10.1016/j.kint.2017.02.036
23. Kato M, Tajima N, Shimizu T, et al. Pharmacokinetics and safety of a single oral dose of mirogabalin in Japanese subjects with varying degrees of renal impairment. J Clin Pharmacol. 2018;58(1):57–63. doi:10.1002/jcph.974
24. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
25. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
26. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33.
27. Posner K, Brown GK, Stanley B, et al. The Columbia-suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266–1277. doi:10.1176/appi.ajp.2011.10111704
28. Yin OQ, Merante D, Truitt K, Miller R. Population pharmacokinetic modeling and simulation for assessing renal impairment effect on the pharmacokinetics of mirogabalin. J Clin Pharmacol. 2016;56(2):203–212. doi:10.1002/jcph.584
29. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
30. Farrar JT, Young JP
31. Kenward MG, Molenberghs G, Thijs H. Pattern-mixture models with proper time dependence. Biometrika. 2003;90(1):55–71. doi:10.1093/biomet/90.1.53
32. Mallinckrodt CH, Lane PW, Schnell D, Peng Y, Mancuso JP. Recommendations for the primary analysis of continuous endpoints in longitudinal clinical trials. Drug Inf J. 2008;42(4):303–319. doi:10.1177/009286150804200402
33. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York: John Wiley & Sons, Inc.; 1987.
34. Kim Y. Missing data handling in chronic pain trials. J Biopharm Stat. 2011;21(2):311–325. doi:10.1080/10543406.2011.550112
35. Butler S, Eek D, Ring L, Gordon A, Karlsten R. The utility/futility of medications for neuropathic pain - an observational study. Scand J Pain. 2019;19(2):327–335. doi:10.1515/sjpain-2018-0317
36. Oster G, Harding G, Dukes E, Edelsberg J, Cleary PD. Pain, medication use, and health-related quality of life in older persons with postherpetic neuralgia: results from a population-based survey. J Pain. 2005;6(6):356–363. doi:10.1016/j.jpain.2005.01.359
37. Verbeeck RK, Musuamba FT. Pharmacokinetics and dosage adjustment in patients with renal dysfunction. Eur J Clin Pharmacol. 2009;65(8):757–773. doi:10.1007/s00228-009-0678-8
38. Lyrica (pregabalin) [prescribing information]. New York: Pfizer Inc.; 2019.
39. Honda M, Murata T, Ebata N, Fujii K, Ogawa S. Treatment patterns of postherpetic neuralgia patients before and after the launch of pregabalin and its effect on medical costs: analysis of Japanese claims data provided by Japan Medical Data Center. J Dermatol. 2017;44(7):767–773. doi:10.1111/1346-8138.13784
40. Neurontin (gabapentin) [prescribing information]. New York: Pfizer Inc.; 2018.
41. Cymbalta (duloxetine) [prescribing information]. Indianapolis: Eli Lilly and Company, Inc.; 2017.
42. European Medicines Agency. Guideline on the clinical development of medicinal products intended for the treatment of pain; 2016. Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-medicinal-products-intended-treatment-pain-first-version_en.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.