")
Back to Journals » Clinical Interventions in Aging » Volume 12
Minor positive effects of health-promoting senior meetings for older community-dwelling persons on loneliness, social network, and social support
Authors Gustafsson S , Berglund H, Faronbi J, Barenfeld E, Ottenvall Hammar I
Received 14 June 2017
Accepted for publication 7 September 2017
Published 7 November 2017 Volume 2017:12 Pages 1867—1877
DOI https://doi.org/10.2147/CIA.S143994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Susanne Gustafsson,1,2 Helene Berglund,1,3 Joel Faronbi,1,4 Emmelie Barenfeld,1,2,5 Isabelle Ottenvall Hammar1,2
1Frail Elderly Research Support Group (FRESH), Institute of Neuroscience and Physiology, Sahlgrenska Academy at Gothenburg University, 2Gothenburg University Centre for Ageing and Health (AgeCap), 3Institute of Health and Care Sciences, Sahlgrenska Academy at Gothenburg University, Gothenburg, Sweden; 4Department of Nursing Science, College of Health Science, Obafemi Awolowo University, Ile-Ife, Nigeria; 5Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden
Objective: The aim of this study was to evaluate the 1-year effect of the health-promoting intervention “senior meetings” for older community-dwelling persons regarding loneliness, social network, and social support.
Methods: Secondary analysis of data was carried out from two randomized controlled studies: Elderly Persons in the Risk Zone and Promoting Aging Migrants’ Capabilities. Data from 416 participants who attended the senior meetings and the control group at baseline and the 1-year follow-up in the respective studies were included. Data were aggregated and analyzed with chi-square test and odds ratio (OR) to determine the intervention effect.
Results: The senior meetings had a positive effect on social support regarding someone to turn to when in need of advice and backing (OR 1.72, p=0.01). No positive intervention effect could be identified for loneliness, social network, or other aspects of social support.
Conclusion: Health-promoting senior meetings for older community-dwelling persons have a minor positive effect on social support. The senior meetings might benefit from a revision to reinforce content focused on loneliness, social network, and social support. However, the modest effect could also depend on the lack of accessible social resources to meet participants’ identified needs, a possible hindrance for a person’s capability. This makes it necessary to conduct further research to evaluate the effect of the senior meetings and other health-promoting initiatives on social aspects of older community-dwelling people’s lives, since these aspects are of high importance for life satisfaction and well-being in old age.
Keywords: aged, quality of life, health promotion, prevention, group intervention, evaluation studies
Introduction
Health promotion, as a targeted intervention for older community-dwelling persons, has become increasingly important to enable the growing population of older persons (65+) to increase control over and to improve their health, in line with the World Health Organization (WHO) directive.1,2 The prominence of health care organizations to provide health promotion is underpinned by principles of aging in place – to be able to live at home for as long as possible, which is supported by the wishes of older persons themselves3 and political strategies, for example in Sweden.4 In order to target aging in place, health promotion needs to address a plethora of goals to provide strategies to counteract loneliness and to propone social network and social support. These goals are motivated by the fact that enhanced social conditions have demonstrated a positive impact on life satisfaction and the well-being of older people.5
The general increase in single-person households as people age poses an increased risk of loneliness.6 Loneliness is always unwanted, unlike the more desirable concept of aloneness, which implies making a choice to being alone.7 The prevalence of loneliness in older people depends on its conceptual definition, but proportions between 20% and 50% have been reported.8 Loneliness increases with age, predicts lower life satisfaction,9 and implies a higher risk of mortality.10 It is also correlated to depression,7 which is considered to be an important public health problem among older people.11 Research has shown that loneliness can be positively affected in older people,12 and that interventions tailored to counteract loneliness in older persons can be effective.13 This provides important insights for health-promoting initiatives targeting loneliness, and the need to evaluate its effect.
It has been suggested that loneliness increases in the oldest age groups due to loss of close attachments.7 An older person’s social network and social support are therefore vital. Social network is traditionally defined as the number of social contacts/personal relationships (structural support) a person has,14 which can consist of family, friends, and colleagues, weak ties such as acquaintances,15 and contacts with health care and community services. Social support can be described as buffering individuals’ well-being from the potential negative influence of stressful events.16 It can also be explained as the individual’s perceptions of the degree to which social relations offer different forms of resources such as material aid or emotional support.17 Social network and social support are closely intertwined since support is exchanged in the relationships within a person’s social network.18 Thus, some definitions of social network also include the characteristics of relational linkages (ie, mutual social support) within a social network.19 One study reported that absence of social support is associated with poorer mental health and reduced cognitive performance,20 and another that having social support has a health-promoting effect on disease outcomes.21
A health-promoting intervention called senior meetings, with the aim of maintaining older community-dwelling persons’ independence and ability to maintain or improve different aspects of health and quality of life, has been studied in two randomized controlled studies: Elderly Persons in the Risk Zone (EPRZ)22 and Promoting Aging Migrants’ Capabilities (PAMC).23 Senior meetings is a group-based intervention in which a part of the content is directed toward issues of loneliness, social network, and social support. The intervention was earlier shown to have favorable effects on slowing down the deterioration of self-rated health and comorbidity,24 and dependence in activities of daily living (ADL) in both short- and long-term.25,26 Qualitative evaluations of the senior meetings show that the participants learned from each other and shared good examples from everyday life.27 In addition, participants perceived the senior meetings as a “key to action,” giving them knowledge to take action when needed. Another qualitative study of the senior meetings concluded that the intervention enabled participants to become aware of their life situation in a longitudinal time perspective.28 It also found that one main reason for attending the senior meetings was the possibility to meet others and to socialize.
Taken together, the health-promoting intervention senior meetings might have the potential to counteract loneliness, and positively affect social network and social support in the long-term for older community-dwelling persons. These outcomes have not been previously studied in connection to the EPRZ and the PAMC studies, and overall, there are few published empirical studies evaluating social aspects of health-promoting initiatives for older community-dwelling persons. For example, a recently published scoping review only found nine studies combining health promotion and social support, several among them addressing a general population or persons aged <65 years.29 Consequently, it is clear that loneliness, social network, and social support are important aspects to target in health-promoting interventions for older persons, and to evaluate such initiatives. Accordingly, seeking to support advancement of knowledge on this subject, the aim of the present study was to evaluate the 1-year effect of the health-promoting intervention senior meetings for older community-dwelling persons on loneliness, social network, and social support.
Methods
Study design
This study involved secondary analysis of data from two randomized controlled studies: EPRZ22 and PAMC.23 These studies involved 459 and 131 participants, respectively. In the EPRZ study, two different health promotion interventions were investigated: a preventive home visit and senior meetings. In the PAMC study, only senior meetings were evaluated. Senior meetings is a standardized intervention. It was implemented equally in the EPRZ and the PAMC.30 In the present study, to enable a more extensive evaluation on a larger group of community-dwelling older persons, data from participants in the EPRZ and PAMC studies that attended the health-promoting intervention senior meetings and the control group at baseline and the 1-year follow-up in the respective studies were included (n=285 and 131, respectively). Data were aggregated and analyzed. The Regional Ethical Review Board in Gothenburg approved both studies: EPRZ (# 650-07) and PAMC (# 821-11). Written informed consent was obtained from the participants. Trial registrations for EPRZ and PAMC, respectively, are ClinicalTrials.gov NCT00877058 and NCT01841853.
Participants and setting
The aggregated dataset contained a total of 416 community-dwelling persons aged ≥70 years, n=227 in the senior meeting group and n=189 in the control group. The inclusion criteria in the EPRZ study22 were ≥80 years, living in ordinary housing, not dependent on the community home help service or care, independent of help from another person in ADL, and cognitively intact (defined as having a score of ≥25, assessed with the Mini Mental State Examination31). The inclusion criteria in the PAMC study23 were the same except for age, which was ≥70 years and older, and that participants should have migrated to Sweden from Finland or the Western Balkan region. The only exclusion criterion in PAMC was impaired cognition, Mini Mental State Examination <80% of administered items, an adjustment of the scale made due to the occurrence of illiteracy.
The setting for the studies were three out of ten urban districts in a large city in western Sweden. EPRZ was implemented in an urban district with high and middle socioeconomic parameters (eg, general income level, sickness rate), while PAMC was implemented in two districts with middle and low socioeconomic parameters. In all three urban districts, there was a mix of self-owned houses and apartment blocks, a local health center, and a variety of social activities offered by community or private (eg, church, local associations) actors.
Intervention
Senior meetings
The senior meetings comprised four weekly, 2-hour group meetings involving four to six participants. Within the group meetings, the participants received information on and discussed the aging process, possible health consequences, and were provided with strategies for solving various problems that might arise in the home environment. A key intent of the intervention was to acknowledge older persons’ expertise and offer an arena for the exchange of knowledge rather than knowledge transfer.32 A person-centered approach33 was applied and peer learning was the main pedagogical method.34 The idea was to encourage people to make their own decisions and, as far as possible, control their own lives.35 A collaborative multi-professional intervention team in the urban districts comprising a registered occupational therapist (OT), a registered nurse (RN), a registered physiotherapist (PT), and a qualified social worker (SW), each responsible for one occasion, administered the four group meetings. The role of the leader in the respective group meeting was to encourage and guide participants in the learning process. Themes from a booklet (Table 1), written in a popular style by researchers in the field and especially designed for the intervention, were used as a basis for the meetings.36 The main part of the intervention content concerning loneliness, social network, and social support was scheduled in the fourth senior meeting administrated by the qualified SW. Two chapters in the booklet, “Life events and quality of life during aging” and “Anyone that needs help can get help,” formed the basis for information, discussions, and strategies in these issues. For instance, in discussing who to turn to if in need of help, alternative sources of support was one topic. Participants in the PAMC study could choose to attend meetings either in Swedish or with interpretation resources. In addition to taking part in the group meetings, each participant was followed up with an individually tailored home visit about 2–3 weeks after the senior meetings in which he/she had the opportunity to discuss group topics in more depth.
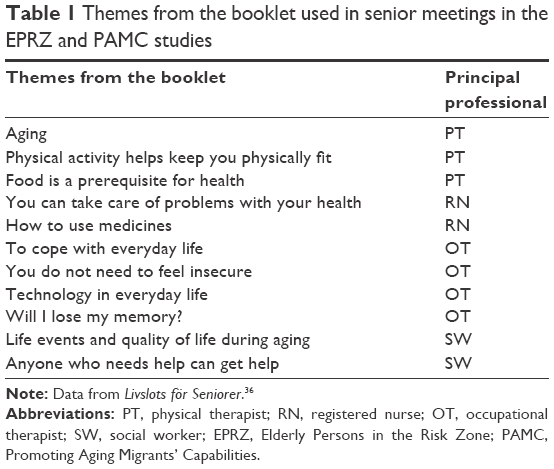 | Table 1 Themes from the booklet used in senior meetings in the EPRZ and PAMC studies |
The senior meetings were largely implemented according to plan in the EPRZ study, while compliance was somewhat lower in the PAMC study. In total, in the aggregated dataset for this study, 87% of the participants in the senior meetings group (n=197) attended all four meetings, while 6% (n=13) attended three meetings, 3% (n=7) two, and 3% (n=6) attended one meeting. Four persons attended no meeting. No known organized co-intervention took place within the periods in question, and no adverse events were reported during the implementation of the interventions in either study.
Control group
Participants in the control group had access to the ordinary range of community services offered by the community care for the aged, which they approached entirely on their own initiative whenever they felt the need. The aim of these services is to ensure that older persons are able to live as independently as possible in their own homes. In Sweden, when older persons are no longer able to manage daily life independently, they can apply for assistance from the community home help service. The extent of such support is subject to an assessment of needs and may include meals on wheels, help with cleaning and shopping, assistance with personal care, safety alarms, transportation services, and home health care. If the research assistant, at baseline or follow-up assessment, discovered that a person in the control group had an urgent need of community or health care service, he/she informed him/her where to turn to receive help.
Data collection
Data in the EPRZ study were collected between 2007 and 2010 and in the PAMC study between 2012 and 2016. For the purpose of this study, data from baseline and the 1-year follow-ups were used. Research assistants (OT, PT, RN, or SW) performed data collection face-to-face in the participant’s home, or in another place if the participant so wished. The items and the response alternatives were read to the participant and, if needed, shown on a paper. For participants in the PAMC study, all materials were available in the participants’ mother tongue and the research assistants were bilingual. All research assistants, in both EPRZ and PAMC, were trained in how to administer the assessments. To ensure as much standardization of the assessments as possible, study protocol meetings were held regularly throughout both studies.
Sample size, randomization, and blinding
The two studies were randomized controlled trials (RCTs) and had completed preparations for their respective implementation by the calculation of power and sample size according to the CONSORT guidelines.37,38 For details, please see the respective study protocol.22,23 Regarding randomization, an independent researcher, not involved in enrolling participants or in the intervention, organized the allocation system used in both studies. Opaque, sealed envelopes were used to randomly assign participants to either the control or the intervention group. Randomization was performed after baseline assessment. To enable blinding of those assessing the outcomes, the intent was that different parties conduct baseline assessments and follow-ups, which was met for a majority of the participants.
Outcome measures
Both the EPRZ and PAMC studies used the same questionnaire. The outcome measures for this study were the change between baseline and the 1-year follow-up regarding loneliness, social network, and social support. For each single query, the authors decided what constituted a positive intervention outcome based on 1) the literature or 2) relevant difference for the older person. The concepts of social network and social support partly overlap. Thus, for pragmatic reasons, we chose to sort queries concerning these outcomes under one of them on the basis of their main content (see Social network and Social support).
Loneliness
Loneliness was assessed by the question “Do you feel lonely?” with four answering alternatives dichotomized into “no” (“no never”) and “yes” (“yes, rarely,” “yes, sometimes,” and “yes, often”). In the final analysis, a change from feeling lonely at baseline to not feeling lonely at the 1-year follow-up, and to continue not feeling lonely at the 1-year follow-up, constituted positive intervention outcomes.
Social network
To measure different aspects of social network, five questions were used. Participants who had no children answered three of these five questions. The first was “How often do you meet and spend time with your child/children?” and the second “How often do you have contact in other ways, for instance telephone, Skype, email or letters, with your child/children?” The seven response options in both questions were similar, and were dichotomized into “often” (“every day” and “once or several times a week”) and “not often” (“once or several times a month,” “once or several times a quarter,” “once or twice per year,” “more seldom,” and “never”). The next two questions were of the same formulation as the former but involved relatives other than child/children. These four questions were in general consistent with questions in a national survey about living conditions/social relations conducted by Statistics Sweden,39 and the dichotomization of the response scale followed the directions outlined in another study concerning older persons.40 A positive intervention outcome connoted maintained estimation of “often” at the 1-year follow-up or a change from “not often” to “often.”
Regarding contacts with friends and acquaintances, a single sub-question from the validated LiSat-11 scale41,42 was used to determine the level of satisfaction with contacts; “The contact with friends and acquaintances are…?” The six response options were dichotomized into “not being satisfied” (“very dissatisfied,” “dissatisfied,” “rather dissatisfied,” and “rather satisfied”) and “being satisfied” (“satisfied” and “very satisfied”), which is a recommended strategy.41,42 A positive intervention outcome was operationalized as maintained estimation of “being satisfied” at the 1-year follow-up or a change from “not being satisfied” to “being satisfied.”
Social support
Social support was measured by five different questions. The first question was “How many persons do you have that you can trust and confide in?” to which participants could answer “none,” “one,” “two,” and “three or more.” For the purpose of this study, the responses to this question were operationalized into “reduced” (including those responding “none” at both baseline and the 1-year follow-up) or “maintained/increased” number of persons, comparing the responses at baseline with those of the 1-year follow-up.
The next question was “Who do you turn to first to ask for help if you become ill and bedridden?” The answers to this question (husband/wife/partner, partner living apart, children, other relative, friend, neighbor, home help/home care/primary care, voluntary organization, and other) were quantified and dichotomized into “have no one”/“have someone.” In the final analysis, a change from “have no one” to “have someone” and still having someone at the 1-year follow-up constituted positive intervention outcomes. In addition, a compilation of data was done in order to describe if the answer listed by participants could be classified as “family” (husband/wife/partner, partner living apart, children, and other relative), “friend” (friend and neighbor), or “health care/community service” (home help/home care/primary care and voluntary organization). Then, an analysis was carried out to determine if there were any differences between the distribution of these groups between participants in the intervention group and the control group at baseline and the 1-year follow-up.
Finally, three different questions regarding kind of support were asked: Sometimes you need help and support from someone. Do you have a relative, friend, or other person you can turn to if you need 1) practical help; 2) advice and backing; and 3) someone to talk to about your personal concerns. The number of different categories of persons and organizations (husband/wife/partner, partner living apart, children, other relative, friend, neighbor, home help/home care/primary care, voluntary organization, and other) was counted. A positive intervention outcome connoted “maintained/increased” number of categories as opposed to “reduced” (including those not having anyone at baseline and the 1-year follow-up). Participants’ values at baseline and those at the 1-year follow-up were then compared.
Statistical analyses
Analyses were carried out on the basis of the intention-to-treat principle (ITT).43 To provide as broad and comprehensive picture of the result as possible, two different approaches to the imputation of missing data were implemented. The first approach was the median change of deterioration (MCD). The basic assumption for using MCD is that older persons are expected to deteriorate over time as a natural course of the aging process. Therefore, missing values were replaced with a value based on the MCD between the two measuring points (baseline and the 1-year follow-up) of all who participated at both occasions. The second approach was the last observation carried forward (LOCF). This method is based on an assumption that no or little change will occur, and therefore, a missing value at the 1-year follow-up was replaced by the value at baseline. In both analyses, for values missing due to a person’s death at the time of the 1-year follow-up, the single imputation method of the worst case was used.44 In addition, sensitivity analyses using complete cases (CC) were also performed and are presented.45
Baseline characteristics for participants that completed the study and dropouts at the 1-year follow-up were compared using chi-square test for dichotomous variables and t-test for continuous variables. In the final analyses, the outcome measures were analyzed using an overall chi-square test, and thereafter compared groupwise by the odds ratio (OR). A p-value ≤0.05 was considered significant and a 95% confidence interval is provided for analysis when appropriate. Statistical analyses were performed using IBM SPSS version 22.0 (IBM Corporation, Armonk, NY, USA).
Results
The 416 participants’ ages ranged from 70 to 97 years with a mean age of 81 years. Sixty percent (n=247) were women and 53% (n=220) lived alone. Nineteen percent (n=78) of the participants had tertiary education (initiated or completed university or college) and 78% (n=321) rated their health as good at baseline (Table 2). There were no statistically significant differences between the participants in the senior meetings group and the control group in terms of gender, having children, education, and self-rated health. However, participants in the intervention group were significantly older and lived alone to a higher proportion compared to those in the control group (Table 2).
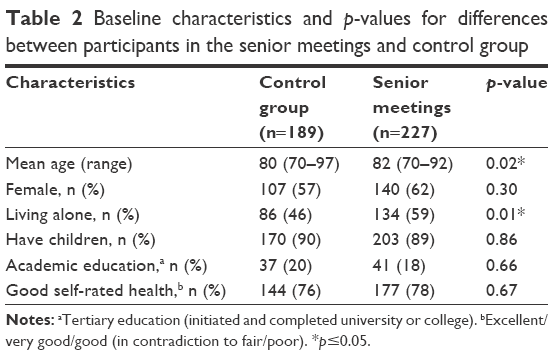 | Table 2 Baseline characteristics and p-values for differences between participants in the senior meetings and control group |
In total, the dropout rate at the 1-year follow-up was 18% (n=76), 22% (n=41) in the control group and 15% (n=35) in the senior meetings group. There was no statistically significant difference in proportions between the groups (p=0.10). “Not interested” was the main reason for declining participation in the control group, while the main reasons for declining participation in the senior meetings were more varied. No significant differences were found between participants that competed the study and dropouts at the 1-year follow-up concerning age, gender, education, having children, living alone, or self-rated health at baseline. Finally, at 1 year, seven persons (2%) had died (results not shown).
Loneliness
At baseline, 47% of participants felt lonely to some extent, and there was no statistically significant difference between the study arms (p=0.31) (Table 3). Regarding proportions of positive outcome between the groups at the 1-year follow-up, no statistically significant difference could be found for any of the two imputation methods, or for CC (Table 4).
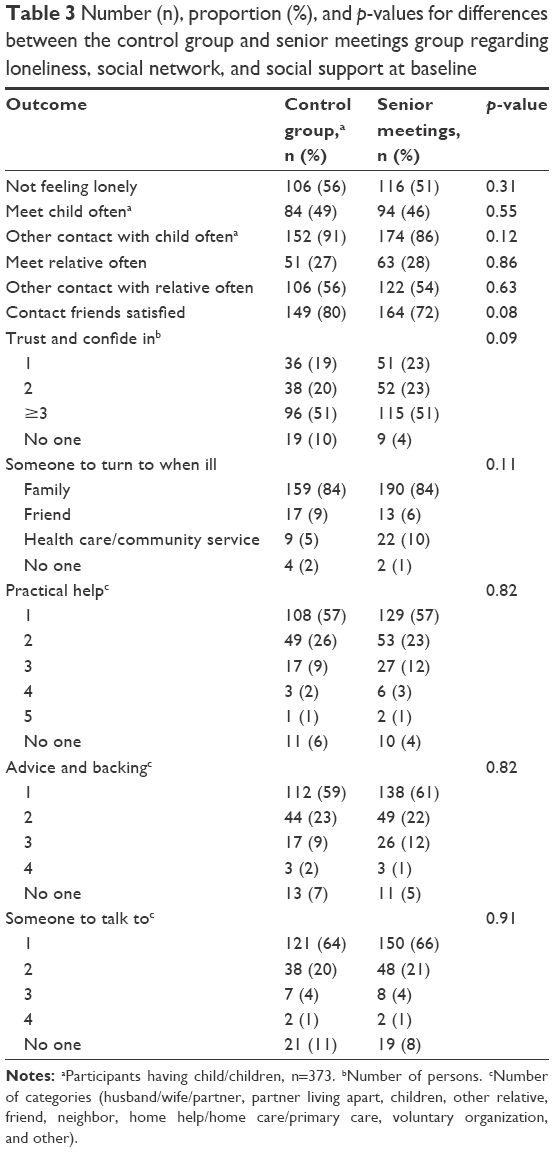 | Table 3 Number (n), proportion (%), and p-values for differences between the control group and senior meetings group regarding loneliness, social network, and social support at baseline |
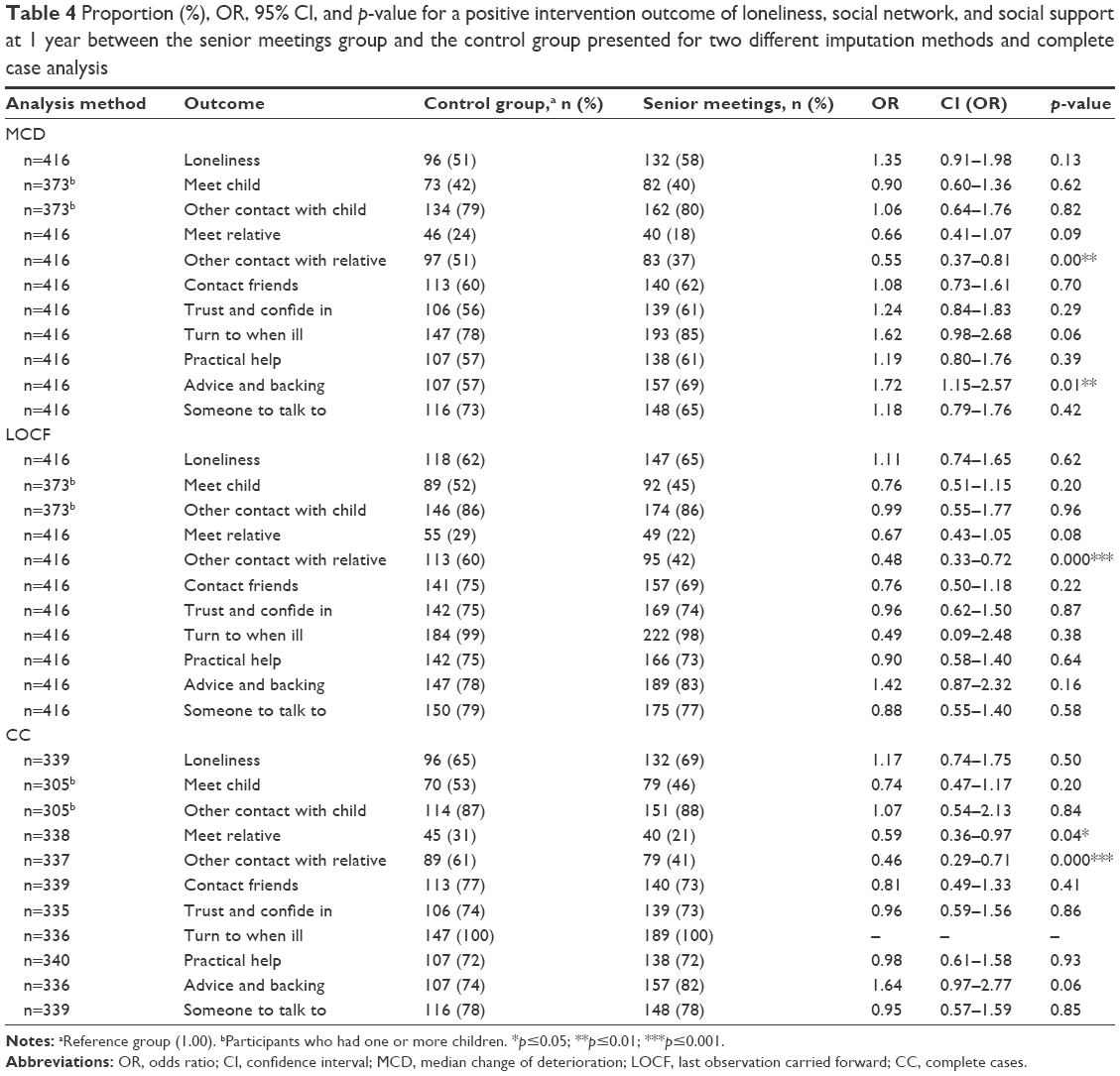 | Table 4 Proportion (%), OR, 95% CI, and p-value for a positive intervention outcome of loneliness, social network, and social support at 1 year between the senior meetings group and the control group presented for two different imputation methods and complete case analysis |
Social network
Ninety percent of the participants (n=373) had one or more children, mean 2.3 and median 2. At baseline, almost half of the participants met with their child/children often, and a large proportion (87%) often had contact with them in other ways (eg, telephone, Skype). No statistically significant differences were found between the groups at baseline (Table 3), nor any intervention effect at the 1-year follow-up (Table 4). Concerning contacts with relatives other than child/children at baseline, just over a quarter (27%) of the participants met with them often, and around half of the participants often had contact in other ways (eg, telephone, Skype). There was no statistically significant difference between the two study arms at baseline (Table 3). At the 1-year follow-up, analysis of contacts with relatives other than child/children showed a trend of negative intervention effect (MCD OR 0.66, p=0.09/LOCF OR 0.67, p=0.08), which became statistically significant when analyzing CC (OR 0.59, p=0.04) (Table 4). In addition, all analytical methods showed a non-favorable intervention effect for the senior meetings concerning contact with relatives other than child/children in other ways (Table 4). Regarding satisfaction with contacts with friends and acquaintances, three quarters of participants were satisfied at baseline and there was no significant difference between the study arms (Table 3). No intervention effect could be demonstrated at the 1-year follow-up (Table 4).
Social support
A vast majority of the participants had someone to trust and confide in at baseline, but 7% (n=28) had no one. There was no statistically significant difference in terms of number of persons between the study arms at baseline (Table 3), and no intervention effect could be demonstrated at the 1-year follow-up (Table 4). In response to the question, “who do you turn to first to ask for help if you become ill and bedridden?” 84% stated that they turned to a family member at baseline, while 7% stated that they first turned to the health care/community service. The proportions were equally distributed between the two study arms at baseline (Table 3), and there was no intervention effect at the 1-year follow-up (Table 4).
At baseline, all but 21 participants (5%) had someone to turn to for practical help. Most participants (57%) had one category of persons or organization to turn to and in 94% of these cases this was a family member. Only 2% stated that they turned to health care/community service (result not shown). There was no statistical difference between the study arms at baseline (Table 3), and no intervention effect at the 1-year follow-up (Table 4). Concerning having someone to turn to for advice and backing, 60% had one category of persons or organization to turn to, while 6% (n=24) had no one. There was no statistical difference between the study arms at baseline (Table 3). However, at the 1-year follow-up, analysis with MCD showed a favorable effect for the senior meetings (OR 1.72, p=0.01), and the analysis with LOCF and CC showed positive trends (OR 1.42/1.64), but were not statistically significant (p=0.16/0.06) (Table 4). The responses to if participants had someone to talk to about his/her personal concerns at baseline showed that 10% had no one, while 65% had one category of persons or organization to turn to. There was no statistical difference between the study arms at baseline (Table 3), nor could any intervention effect be demonstrated (Table 4).
Discussion
The results show that the health-promoting intervention senior meetings for older community-dwelling persons had a positive effect on social support regarding someone to turn to when in need of advice and backing. No intervention effect could be identified for other aspects of social support and for loneliness. Regarding features of social network, the senior meetings had no or non-favorable effects.
The positive intervention effect concerning someone to turn to when in need of advice and backing indicates that the information and discussions regarding this issue during the senior meetings have led to enhanced knowledge and skills among the participants. They may have, in line with health-promoting theoretical underpinnings, been empowered,35 and have the competence to expand the number of persons and organizations to turn to when in need of advice and backing. This positive finding is in line with an earlier study where participants described the intervention as a “key to action,” giving them knowledge to take action when needed.27 It is also in line with a recently published study which found that a group-based program promoting social capital (social support and participation) among lonely older people was effective.46
On the contrary, the senior meetings had no effect on other evaluated aspects of social support such as someone to turn to for practical help and someone to talk to. The simplest explanation to this null result is that the intervention was not effective in these respects, and needs to be revised to reinforce program content. For example, deepened information on, or study visits to, community resources and meeting places in the vicinity could be added to the intervention in order to further empower the participants to take actions. However, there are also other possible explanations for the modest results of the senior meetings. In order to reach a personal goal, for instance social support, a person needs not only own capacity at an individual level (micro), but also adequate resources in his/her environment (meso and macro level) that can respond, since a person’s capability to achieve health goals of value (eg, social support) is shaped by the interplay between internal and external factors.47 If both internal and external factors are not adequate, a person’s ability to “do” and “be” the things he/she regards as important in life, capability, can be reduced.48 The results of this study show that the vast majority of participants turned to family members (spouse, children, or other relative) for social support, few turned to health care, community services, or voluntary organizations. As older people’s social networks decrease with increasing age, they might not have equal opportunities for social support. It may be that the senior meetings led to increased knowledge and skills of participants, empowerment on the micro level, but that lack of resources at the meso and macro level constituted obstacles for participants’ capability, that they are not able to influence their own situation despite their own actions. Recently published qualitative results from the PAMC study support this argumentation by describing how participants are challenged by available resources in order to satisfy health needs in everyday life.49 Consequently, this implies amplification of the society’s responsibility to offer adequate and accessible resources for older people in line with a justice perspective.50 Implementing this reasoning in relation to the present study, it means that society needs to provide sufficient and accessible resources for social support regardless of age and extent of personal network. In addition, considering the fact that participants in one of the studies (PAMC) were born outside Sweden, community services must also be accessible on equal terms regardless of the country of birth and their understanding of the Swedish language.
The result also showed that senior meetings did not have a positive effect on participants’ social networks. On the contrary, regarding two aspects, meetings and time spent, and contacts in other ways with relatives other than child/children, the intervention demonstrated a non-favorable effect. This result was unexpected. It can indicate that the intervention was not effective in maintaining and expanding participants’ social network, but other possible explanations need to be discussed. The information and discussions in the senior meetings highlight the importance of social networks and their significance for life satisfaction and well-being while aging. This increases the awareness of social networks among participants and makes them pay attention to their own needs. In addition, a qualitative study regarding the intervention proved the social value of seeing and socializing with peers and personnel in the senior meetings and found that this was one main reason for attending the sessions.28 Considering these facts, participants may desiderate the possibility to socialize at the senior meetings in combination with raised awareness of the importance of social networks, resulting in lower estimations of their situation when assessed at the 1-year follow-up. Such interpretation underlines the importance of offering accessible community meeting places providing continued opportunities for socialization and social networking after participation in the senior meetings. In addition, 1 year is a short time for a person to actively work on improving one’s social network. A longer time may need to have passed before follow-up in order to capture any intervention effect on social network. Finally, it is possible that building social networks in later life will be harder due to reduced social interaction caused by increasing functional impairments (eg, hearing and mobility).19 Even so, in order to provide as varied opportunities as possible for social networking, community meeting places should be easily accessible and intergenerational, a recommendation also supported by WHO in its guidelines for age-friendly cities and communities.51
The senior meetings did not demonstrate any effect on loneliness. As argued earlier, this implies that the intervention was insufficient in affecting this outcome. Nevertheless, in line with earlier argumentation, participants might have directed more attention to loneliness, making them extra aware of feelings and needs resulting in lower estimations when assessed at the 1-year follow-up. Another possible explanation of the null result is related to the study design, a potential bias due to the Hawthorn effect.52 The Hawthorne effect is a form of reactivity whereby subjects improve or modify an aspect of their behavior being measured experimentally simply in response to the fact that they are being studied, not in response to any intervention. Consequently, the result of measurements in the control group may have been biased by the attention given to the participants, making them feel less lonely, resulting in reduced opportunity to detect any differences between the study arms at the 1-year follow-up. This explanation increases in credibility when taking into account the outcome variables possible sensitivity to personal contacts and the fact that another intervention study demonstrated that half of the improvement in their primary outcome was found to be attributed to the Hawthorne effect.53
Furthermore, it is important to bear in mind that this is a quantitative study. It says little about the meaning of loneliness or quality of participants’ social networks and social support. There is a possibility that the senior meetings might have had a positive impact on qualitative aspects of the outcomes, which has not been demonstrated in this study. For this reason, additional studies are needed in order to find out more about the effects of senior meetings and other health-promoting initiatives on loneliness, social support, and social network of older community-dwelling persons.
There is also a need to discuss possible methodological shortcomings in this secondary analysis of data from the EPRZ and PAMC studies. This research is an aggregation of data from two studies with partially different inclusion criteria; lower limits for age, ≥70 and ≥80 years, and participants’ countries of origin with cultural diversity. Almost all EPRZ study participants were born in Sweden and lived in an urban district with high or middle socioeconomic status, while the PAMC study participants were born in either Finland or the Western Balkan region and lived in more socioeconomic disadvantaged areas. The heterogeneity between, and within, the participants in the studies might have affected the results making it harder to demonstrate intervention effects. One possibility could have been to analyze subgroups but that was never an option since subgroups would become small and analyses uncertain. In addition, the main purpose of this study was to evaluate the intervention effect in a large group of community-dwelling older persons whose demographics matched the characteristics of the increasingly heterogeneous aging population in Sweden, enhancing generalization of results.
Finally, another possible methodological shortcoming is the statistically significant difference at baseline in the disadvantage of the senior meetings group regarding higher mean age and proportion of participants living alone. We chose not to adjust the analyses to control for these differences, which might have contributed to the modest result. This is because both the EPRZ and the PAMC studies were pragmatic RCTs mirroring a diverse older population in real life contexts, and the ambiguity concerning any such adjustment is justified.54 However, we analyzed data according to ITT and used two different methods for the imputation of missing data, and reported results from analyses of CC, an approach providing a broad picture of the intervention effect possibly partially compensating for differences at baseline. Despite the highlighted possible methodological shortcomings, our study constitutes a valuable addition to the lack of knowledge concerning the benefits with health-promoting intervention for the target group. Hence, more high-quality evaluative studies within this field are needed.
Conclusion
Health-promoting senior meetings for older community-dwelling persons have a minor positive effect on social support. The senior meetings might benefit from a revision to reinforce content focused on loneliness, social network, and social support. However, the modest effect could also depend on lack of accessible social resources to meet participants’ identified needs, a possible hindrance for a person’s capability. This makes it necessary to conduct further research to evaluate the effect of senior meetings and other health-promoting initiatives on social aspects of older community-dwelling people’s lives, since these aspects are of high importance for life satisfaction and well-being in old age.
Acknowledgments
We would like to thank the Gothenburg University Centre for Ageing and Health (AgeCap) (grant number 2013–2300), the Swedish Institute for Health Sciences (Vardalinstitutet), and the Hjalmar Svensson Foundation for financing and supporting this study. We also want to thank our collaborators, the City of Gothenburg, Sweden, and the Region of Vastra Gotaland, Sweden, for supporting the implementation of both the EPRZ and PAMC studies. Finally, our warmest thanks to the older persons contributing data by participating in the two studies.
Author contributions
SG was primarily responsible for designing the study and drafting the manuscript. IOH was involved in designing the study, drafting the manuscript, and contributing to critical revisions during the writing process. HB, JF, and EB were involved in designing the study and contributing to critical revisions during the writing process. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Ottawa Charter for Health Promotion. 1986. Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/. Accessed November 11, 2009. | ||
World Health Organization. Milestones in Health Promotion: Statements from Global Conferences. Geneva: WHO Press; 2009. | ||
Chippendale TL, Bear-Lehman J. Enabling “aging in place” for urban dwelling seniors: an adaptive or remedial approach. Phys Occup Ther Geriatr. 2010;28(1):57–62. | ||
Larsson K. Kvarboende eller flyttning på äldre dagar – En kunskapsöversikt. Stockholm: Stiftelsen Stockholms läns Äldrecentrum; 2006. Swedish. | ||
Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: three decades of progress. Psychol Bull. 1999;125(2):276–302. | ||
Beard JR, Bloom DE. Towards a comprehensive public health response to population ageing. Lancet. 2015;385(9968):658–661. | ||
Luanaigh CÓ, Lawlor BA. Loneliness and the health of older people. Int J Geriatr Psychiatry. 2008;23(12):1213–1221. | ||
Dykstra PA. Older adult loneliness: myths and realities. Eur J Ageing. 2009;6(2):91–100. | ||
Ní Mhaoláin AM, Gallagher D, Connell HO, et al. Subjective well-being amongst community-dwelling elders: what determines satisfaction with life? Findings from the Dublin Healthy Aging Study. Int Psychogeriatr. 2012;24(2):316–323. | ||
Tabue Teguo M, Simo-Tabue N, Stoykova R, et al. Feelings of loneliness and living alone as predictors of mortality in the elderly: the PAQUID study. Psychosom Med. 2016;78(8):904–909. | ||
Barg FK, Huss-Ashmore R, Wittink MN, Murray GF, Bogner HR, Gallo JJ. A mixed-methods approach to understanding loneliness and depression in older adults. J Gerontol B Psychol Sci Soc Sci. 2006;61(6):S329–S339. | ||
Dahlberg L, Andersson L, McKee KJ, Lennartsson C. Predictors of loneliness among older women and men in Sweden: a national longitudinal study. Aging Ment Health. 2015;19(5):409–417. | ||
Saito T, Kai I, Takizawa A. Effects of a program to prevent social isolation on loneliness, depression, and subjective well-being of older adults: a randomized trial among older migrants in Japan. Arch Gerontol Geriatr. 2012;55(3):539–547. | ||
Smith KP, Christakis NA. Social networks and health. Annu Rev Sociol. 2008;34:405–429. | ||
Granovetter M. The strength of weak ties. Am J Sociol. 1973;78:1360–1380. | ||
Cohen S. Psychosocial models of the role of social support in the etiology of physical disease. Health Psychol. 1988;7(3):269–297. | ||
Fontanini H, Marshman Z, Vettore M. Social support and social network as intermediary social determinants of dental caries in adolescents. Community Dent Oral Epidemiol. 2015;43(2):172–182. | ||
Seeman TE. Social ties and health: the benefits of social integration. Ann Epidemiol. 1996;6(5):442–451. | ||
Caetano SC, Silva CM, Vettore MV. Gender differences in the association of perceived social support and social network with self-rated health status among older adults: a population-based study in Brazil. BMC Geriatr. 2013;13(1):122. | ||
Cacioppo S, Capitanio JP, Cacioppo JT. Toward a neurology of loneliness. Psychol Bull. 2014;140(6):1464–1504. | ||
Tomaka J, Thompson S, Palacios R. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J Aging Health. 2006;18(3):359–384. | ||
Dahlin-Ivanoff S, Gosman-Hedstrom G, Edberg A-K, et al. Elderly persons in the risk zone. Design of a multidimensional, health-promoting, randomised three-armed controlled trial for “prefrail” people of 80+ years living at home. BMC Geriatr. 2010;10:27. | ||
Gustafsson S, Lood Q, Wilhelmson K, Häggblom-Kronlöf G, Landahl S, Dahlin-Ivanoff S. A person-centred approach to health promotion for persons 70+ who have migrated to Sweden: promoting aging migrants’ capabilities implementation and RCT study protocol. BMC Geriatr. 2015;15(1):10. | ||
Behm L, Wilhelmson K, Falk K, Eklund K, Ziden L, Dahlin-Ivanoff S. Positive health outcomes following health-promoting and disease-preventive interventions for independent very old persons: long-term results of the three-armed RCT elderly persons in the risk zone. Arch Gerontol Geriatr. 2014;58(3):376–383. | ||
Gustafsson S, Eklund K, Wilhelmson K, et al. Long-term outcome for ADL following the health-promoting RCT – elderly persons in the risk zone. Gerontologist. 2013;53(4):654–663. | ||
Gustafsson S, Wilhelmson K, Eklund K, et al. Health-promoting interventions for persons aged 80 and older are successful in the short term-results from the randomized and three-armed elderly persons in the risk zone study. J Am Geriatr Soc. 2012;60(3):447–454. | ||
Behm L, Zidén L, Dunér A, Falk K, Dahlin-Ivanoff S. Multi-professional and multi-dimensional group education – a key to action in elderly persons. Disabil Rehabil. 2013;35(5):427–435. | ||
Barenfeld E, Gustafsson S, Wallin L, Dahlin-Ivanoff S. Understanding the “black box” of a health-promotion program: keys to enable health among older persons aging in the context of migration. Int J Qual Stud Health Well-being. 2015;10:29013. | ||
Duplaga M, Grysztar M, Rodzinka M, Kopec A. Scoping review of health promotion and disease prevention interventions addressed to elderly people. BMC Health Serv Res. 2016;16(5):278. | ||
Barenfeld E, Wallin L, Bjork Bramberg E. Moving from knowledge to action in partnership: a case study on program adaptation to support optimal aging in the context of migration. J Appl Gerontol. Epub 2017 Aug 1. | ||
Folstein MF, Folstein SE, McHugh PR. ‘Mini mental state’. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. | ||
Adolfsson ET, Smide B, Gregeby E, Fernström L, Wikblad K. Implementing empowerment group education in diabetes. Patient Educ Counsel. 2004;53(3):319–324. | ||
Ekman I, Swedberg K, Taft C, et al. Person-centered care – ready for prime time. Eur J Cardiovasc Nurs. 2011;10(4):248–251. | ||
Shiner M. Defining peer education. J Adolesc. 1999;22(4):555–566. | ||
Tengland PA. Empowerment: a goal or a means for health promotion? Med Health Care Philos. 2007;10(2):197–207. | ||
Vårdalinstitutet. Livslots för Seniorer. Dahlin Ivanoff S, editor. Vårdalinstitutet; 2009. Available from: http://agecap.gu.se/digitalAssets/1565/1565362_manual-till-livslots-f--r-seniorer.pdf. Accessed October 20, 2017. Swedish. | ||
Moher D, Schulz KF, Altman D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. J Am Med Assoc. 2001;285(15):1987–1991. | ||
Zwarenstein M, Treweek S, Gagnier JJ, et al. Improving the reporting of pragmatic trials: an extension of the CONSORT statement. BMJ. 2008;337(7680):1223–1226. | ||
Statistiska Central Byrån (SCB) [Statistics Sweden]. Undersökningarna av levnadsförhållanden (ULF/SILC). 2017. Available from: http://www.scb.se/hitta-statistik/statistik-efter-amne/levnadsforhallanden/levnadsforhallanden/undersokningarna-av-levnadsforhallanden-ulf-silc/. Accessed October 20, 2017. Swedish. | ||
Berglund H, Hasson H, Wilhelmson K, Dunér A, Dahlin-Ivanoff S. The impact of socioeconomic conditions, social networks, and health on frail older people’s life satisfaction: a cross-sectional study. Health Psychol Res. 2016;4(5578):26–31. | ||
Borg T, Berg P, Fugl-Meyer K, Larsson S. Health-related quality of life and life satisfaction in patients following surgically treated pelvic ring fractures. A prospective observational study with two years follow-up. Injury. 2010;41(4):400–404. | ||
Fugl-Meyer AR, Bränholm I-B, Fugl-Meyer K. Happiness and domain-specific life satisfaction in adult northern Swedes. Clin Rehabil. 1991;5(1):25–33. | ||
Altman DG. Practical Statistics for Medical Research. London: Chapman & Hall; 1999. | ||
Committee for Medicinal Products for Human Use. Guideline on Missing Data in Confirmatory Clinical Trials. London: European Medicines Agency; 2009. | ||
Bennett DA. How can I deal with missing data in my study? Aust N Z J Public Health. 2001;25(5):464–469. | ||
Coll-Planas L, del Valle Gómez G, Bonilla P, Masat T, Puig T, Monteserin R. Promoting social capital to alleviate loneliness and improve health among older people in Spain. Health Soc Care Community. 2017;25(1):145–157. | ||
Ruger JP. Health and Social Justice. Oxford: Oxford University Press; 2010. | ||
Sen A. Capability and Well-being. Oxford: Clarendon; 1993. | ||
Barenfeld E, Gustafsson S, Wallin L, Dahlin-Ivanoff S. Supporting decision-making by a health promotion program: experiences of persons aging in the context of migration. Int J Qual Stud Health Well-being. 2017;12(1):1337459. | ||
Sen A. The Idea of Justice. Cambridge: Belknap Press of Harvard University Press; 2009. | ||
World Health Organization. Global Age-friendly Cities: A Guide. Geneva, Switzerland: WHO; 2007. | ||
McCarney R, Warner J, Iliffe S, Van Haselen R, Griffin M, Fisher P. The Hawthorne effect: a randomised, controlled trial. BMC Med Res Methodol. 2007;7:30. | ||
Wolfe F, Michaud K. The Hawthorne effect, sponsored trials, and the overestimation of treatment effectiveness. J Rheumatol. 2010;37(11):2216–2220. | ||
de Boer MR, Waterlander WE, Kuijper LDJ, Steenhuis IHM, Twisk JWR. Testing for baseline differences in randomized controlled trials: an unhealthy research behavior that is hard to eradicate. Int J Behav Nutr Phys Act. 2015;12(1):4. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.