")
Back to Journals » International Journal of General Medicine » Volume 14
Minimum Seven-Year Follow-Up Outcomes of Percutaneous Endoscopic Lumbar Discectomy for Lumbar Degenerative Disease
Authors Li X, Bai J, Hong Y, Zhang J, Tang H, Lyu Z, Liu S, Chen S, Liu J
Received 25 November 2020
Accepted for publication 22 February 2021
Published 5 March 2021 Volume 2021:14 Pages 779—785
DOI https://doi.org/10.2147/IJGM.S293400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiang Li,1 Jinzhu Bai,2 Yi Hong,2 Junwei Zhang,2 Hehu Tang,2 Zhen Lyu,2 Shujia Liu,2 Shizheng Chen,2 Jiesheng Liu2
1Department of Orthopaedics, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 2Department of Spine and Spinal Cord Surgery, Beijing Bo’ai Hospital, China Rehabilitation Research Center; School of Rehabilitation, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Jinzhu Bai
Department of Spine and Spinal Cord Surgery, Beijing Bo’ai Hospital, China Rehabilitation Research Center; School of Rehabilitation, Capital Medical University, No. 10 North Jiaomen Road, Fengtai District, Beijing, 100068, People’s Republic of China
Email [email protected]
Purpose: To investigate the long-term (> 7 years) clinical outcomes of percutaneous endoscopic lumbar discectomy for lumbar degenerative disease to address postoperative problems including postoperative dysesthesia (POD), residual back pain and segmental instability.
Methods: Inclusion and exclusion criteria were established. All patients who met the above criteria were treated by PELD using the transforaminal approach. Limited discectomy was performed to preserve the disc material in the intervertebral space as much as possible. The Oswestry Disability Index (ODI), Japanese Orthopaedic Association (JOA) score, visual analog scale (VAS) score for back pain (VAS-B) and leg pain (VAS-L) and Modified MacNab’s criterion were used for clinical evaluation. Radiographic parameters including height of intervertebral disc and segmental instability were also evaluated.
Results: Forty-two patients (24 men and 18 women) who met our inclusion and exclusion criteria were included in our study. The average follow-up period was 95.71± 5.63 months (ranging from 87 to 105 months). There were no neurological complications associated with the operation. POD was found in 14.29% of patients, while only 2 patients (4.76%) complained of mild dysesthesia at final follow-up. Two patients (4.76%) required revision surgery during the follow-up period. The final follow-up ODI, JOA score, VAS-B and VAS-L were significantly better than preoperative values. The average disc-height ratio was 84.52± 5.66% of the preoperative disc height. No instability at the operation level was noted at final follow-up.
Conclusion: Our study showed that PELD using the transforaminal approach can provide favorable results after a long-term follow-up period. POD is a common complication at initial prognosis. Limited discectomy can preserve the disc height well and minimize the risk of residual back pain.
Keywords: percutaneous endoscopic lumbar discectomy, transforaminal approach, long-term follow-up, back pain
Microdiscectomy is one of the most popular techniques for the treatment of patients with symptomatic lumbar disc herniation (LDH) that has not resolved after conservative treatment.1–5 This procedure can provide favorable long-term follow-up outcomes. In recent years, the percutaneous endoscopic lumbar discectomy (PELD) technique has gained more and more attention. Compared with conventional techniques, PELD can provide comparable clinical outcomes with a lower risk of infections and shorter hospital stays.1–5 As a novel technique, most studies about PELD focused on the short-term follow-up outcomes, while the long-term follow-up results were rare. The only published long-term follow-up study of PELD included both the transforaminal and interlaminar approaches.9 In the present study, we reviewed 42 patients who underwent PELD in our center with at least 7 years postoperative follow-up. The transforaminal approach was the only procedure. We investigated the long-term outcomes of PELD to address postoperative problems including postoperative dysesthesia (POD), residual back pain and segmental instability.
Methods
Inclusion and Exclusion Criteria
The inclusion criteria were as follow: symptomatic lumbar disc herniation or lumbar spinal stenosis with predominant leg pain; the symptoms had not resolved after at least 3 months of conservative treatment; a single-level PELD procedure at L3-4, L4-5 or L5-S1; a length of follow-up of 7 years or longer.
The exclusion criteria were: previous history of lumbar back operation; severe central canal stenosis; cauda equina syndrome; metastatic lesion; tumor.
Surgical Treatment
The transforaminal approach was the only procedure for all patients. The PELD procedure was performed under local anesthesia (0.5% lidocaine), with the patient in a prone position on a radiolucent table The operated level was identified using fluoroscopy. The estimated lateral distance to the midline ranged from 10 to 14cm according to different index levels. An 18-gauge spinal needle was advanced in to the region of the herniated disc under fluoroscopic guidance. Ideally, the tip of the needle should locate at the posterior vertebral body on the lateral view and at the midline of the vertebral canal on the AP view. The guide wire was inserted through the spinal needle and a 7-mm incision was made. Then, series guide rods and reamers were used for foraminoplasty to advance the working cannula. The ideal position of the working cannula was identified by fluoroscopy. The endoscopy was inserted through the working cannula. If the foraminoplasty is adequate, the compressed nerve root and herniated disk can be easily recognized. Grasping forceps were introduced through the endoscopy and the herniated disc material was removed. Limited discectomy was performed, which meant that only extruded or free fragments in the spinal canal were removed, while the disc material in the disc space was preserved as much as possible.
For patients with lumbar spinal stenosis, the targeted patho-anatomy was the ventral surface of the superior article process. Compared with patients with simple LDH, more bone from the ventral surface of the facet joint was removed with percutaneous tooth trephines during the initial foraminoplasty procedure. After placing the working cannula, discectomy was performed routinely. The above procedures can provide adequate decompression for patients with lumbar spinal stenosis.
Drainage was not routinely placed after surgery unless there was extensive bleeding during the operation.
Evaluation
The Oswestry Disability Index (ODI), Japanese Orthopaedic Association (JOA) score, visual analog scale (VAS) score for back pain (VAS-B) and leg pain (VAS-L) were used for clinical evaluation. The VAS score for back pain and leg pain measures from 0, indicating no pain, to 10, the most severe pain ever experienced. The evaluations were conducted preoperatively, 6 months postoperation and at final follow-up. The follow-up scores were compared with preoperative scores. The Modified MacNab’s criterion was used to evaluate the patient’s satisfaction with the operation.14 There are 4 classes—excellent, good, fair, and poor.
Standing AP, lateral, flexion and extension radiographic films were taken preoperatively and at final follow-up. The disc-height ratio was measured on the lateral view films using Mochida’s method.9 Intervertebral instability was defined as more than a 10-degree change of angles of intervertebral disc space between flexion and extension films.9 The follow-up radiographs were compared with preoperative films (Figure 1A–L).
 |
Figure 1 A 37-year-old female had severe sciatica for more than one year due to LDH and was treated by PELD using the transforaminal approach. (A–D) Preoperative X-rays and MR images showed protrusion at the L5-S1 segment. (E, F) Photograph during the operation showed the disc material removed and adequate decompression of the nerve root. (G–L) X-ray and MR images 7 years postoperation showed complete decompression and good preservation of the disc height. |
Statistical Analysis
Factors in the criteria included the average ODI, JOA score, VAS-B, and VAS-L. Student’s t-test and nonparametric Wilcoxon’s rank-sum test were run using SPSS (IBM, Armonk, NY) and statistical significance was set as 0.05. Results were presented as means ± SE.
Results
Between January 2012 and June 2013, 51 patients underwent the PELD procedure in our center due to lumbar degenerative disease. Clinical records of 48 patients who met the above inclusion and exclusion criteria were reviewed. Six patients were excluded due to inadequate clinical data. Finally, 42 patients were included in our study. There were 24 men and 18 women, with an average age of 48.56±6.34 years (ranging from 17 to 73 years) at the time of operation. The preoperative diagnosis was LDH in 37 patients and lumbar spinal stenosis in 5 patients. For 37 patients with LDH, the type of herniation was classified according to lumbar disc nomenclature: version 2.0 under NASS (North American Spine Society) guidelines.15 There were 21 patients classified as protrusion, 13 patients as extrusion and 3 as sequestration. The operation levels included L3-4 in 2 cases, L4-5 in 27 cases and L5-S1 in 13 cases (Table 1).
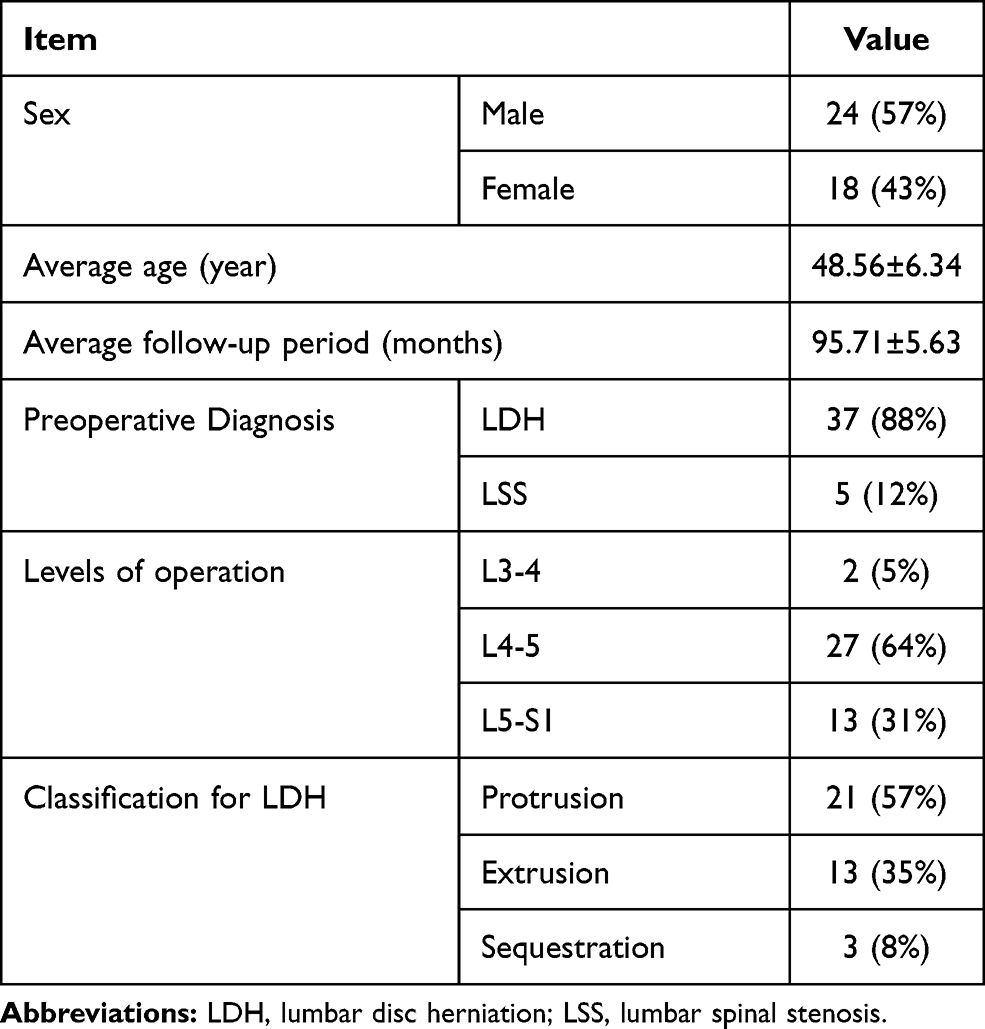 |
Table 1 Patient Demographic Data |
All of the patients tolerated the operation well and no patients were converted to open decompression. There were no neurological complications associated with the operations. The average follow-up period was 95.71±5.63 months (ranging from 87 to 105 months).
Two patients (4.76%) required revision surgery during the follow-up period. According to lumbar disc nomenclature, version 2.0 under NASS (North American Spine Society) guidelines,15 one patient was classified as extrusion and the other was sequestration. The operation levels were both in L5-S1. Both the patients reported leg pain relief immediately postoperative. Unfortunately, the leg pain reoccurred in one month and three months, respectively, because of residual compression. After the failure of conservative treatment, the patients underwent revision surgery by means of standard open discectomy three months and twelve months, respectively, after the initial surgery.
The average VAS score for leg pain improved from 6.86±1.64 preoperatively to 1.85±0.75 at 6 months postoperatively. The final follow-up average VAS score for leg pain was 1.75±0.75. Both the follow-up scores were significantly improved compared to the mean preoperative value (p<0.01).
The average VAS score for back pain was 4.05±1.25 preoperatively, 2.59±0.90 at 6 months postoperatively and 1.55±1.06 at the final follow-up. Both the follow-up scores were significantly improved compared to the mean preoperative value (p<0.05).
Residual back pain (VAS > 3) was found in 3 of the 42 patients (7.14%); however, only 1 patient (2.38%) complained of frequent or occasional moderate back pain (VAS score for back pain ≥ 5).
Six of forty-two (14.29%) patients presented symptoms of POD after their operations and none of these six patients showed motor weakness due to direct exiting root injuries. Four of six patients achieved full resolution of the symptoms within three months. At final follow-up, only 2 patients (4.76%) complained of mild dysesthesia, which did not affect work and recreation.
At the final follow-up, both the JOA score (23.62±4.67) and ODI score (12.68±3.54) were significantly better than preoperative scores (11.24±1.66 and 45.25±4.68, respectively, p<0.01) (Table 2).
 |
Table 2 Clinical Outcomes Preoperative, 6 Months Postoperative and at Final Follow-Up |
The Modified MacNab’s criterion at final follow-up evaluation revealed the following satisfaction levels: excellent in 24 patients, good in 12 patients, fair in 4 patients and poor in 2 patients.
The average final follow-up disc-height ratio in our patients was 84.52±5.66% of the preoperative disc height. There were no patients presenting with intervertebral disc instability at final follow-up at the level of operation.
Discussion
As a novel technique, PELD has gained attention in recent years. The advantages of PELD include lower risk of infection, shorter hospital stay and quicker recovery after surgery. Although favorable results of short-term outcomes have been reported extensively,6–13 the greatest limitation of the PELD technique is lack of long-term follow-up study data.6,9
To our knowledge, there was only one report on the long-term outcomes of PELD. In a series of 38 patients who underwent PELD with a minimum 10-year follow-up period, favorable long-term outcomes were achieved in terms of clinical and radiographic findings. The revision surgery rate was 9.6% at the same level and 27.4% at another level. No operation-induced instability was identified after long-term follow-up. But this study included the PELD procedure using both the transforaminal approach and the interlaminar approach.9
In the present study, we only reviewed patients who underwent PELD using the transforaminal approach. The POD, residual back pain and segmental instability were addressed in the present study.
POD due to irritation of DRG or exiting root injury is one of the most common postoperative complications associated with PELD. Up to 10% of patients who underwent PELD experienced POD.13 In the present study, the incidence of POD is 9%, which is comparable with the findings of other studies.13,16
The prognosis of POD is favorable. Yeung et al13 found that the majority of patients' POD symptoms resolved with conservative treatment within 2 to 3 weeks. In a series of 233 patients, Choi et al16 found that 20 patients presented exiting root injuries with POD or motor weakness. For 15 of 20 patients with POD, the symptoms resolved completely after 3–180 days (mean = 54 days). For five of twenty patients with both POD and motor weakness, full recovery was achieved after 4 to 240 days. Our study showed that 6 of 42 (14.29%) patients presented with symptoms of POD after PELD. Four of six patients achieved full resolution of the symptoms within 3 months. At final follow-up, only 2 patients complained of mild dysesthesia, which did not affect work and recreation. Various reasons, including postoperative hematoma, consistent compression on the exiting root by the working cannula, direct injury by the instrumentation and heat injury caused by radiofrequency, contributed to POD.13,16 No patients in our study showed motor weakness, so the most likely cause of POD was heat injury due to the use of radiofrequency.
Residual back pain and segmental instability are common consequences of standard discectomy or microdiscectomy. Though severe back pain was rare, long-term follow-up results (>10 years) showed that up to 70% of patients undergoing standard discectomy of microdiscectomy complained of mild to moderate back pain, while the incidence of segment instability was 6%.1
In a comparative cohort study with 5-year follow-up, Yong et al12 compared the clinical outcomes between transforaminal endoscopic lumbar discectomy (TELD) and open lumbar microdiscectomy. The results showed that, as a minimally invasive procedure, TELD had advantages including shorter operation time, hospital stay and recovery time. In terms of ODI, VAS-B and VAS-L, there were no significant differences between the two techniques. In a newly published article, Meshal et al17 found that both techniques can provide equivalent, satisfactory outcomes: the PELD technique demonstrated significant lower low back pain at 1 day and 3 months postoperatively compared with open lumbar microdiscectomy (1.48 vs 3.5, and 1.62 vs 2.72, respectively; p=0.01 and 0.026, respectively).
Our study showed that the average VAS-B was 2.59±0.90 at 6-month follow-up and 1.55±1.06 at seven-year follow-up after the PELD procedure. Residual back pain was found in 7.14% of patients, while only 2.38% of patients complained of frequent or occasional moderate back pain (VAS score for back pain ≥ 5). No segmental instability was found after the seven-year follow-up period. These results were comparable with those of the above studies.
In the present study, two cases (4.76%) requiring revision surgery occurred at an early stage of our learning curve. The operation levels were both in L5-S1 segments, with one classified as extrusion and the other as sequestration. The reason for revision surgery was reoccurring leg pain because of residual compression. Generally speaking, the transforaminal approach is difficult to get access to at the L5-S1 level because of shading of the iliac crest. In our opinion, LDH with extrusion or sequestration at the L5-S1 level is not a good indication for the transforaminal approach, especially for surgeons with little experience. The interlaminar approach of PELD is an alternative for this condition. For patients with LDH at the L4-5 level, the indication for the transforaminal approach can be expanded to extrusion or even sequestration due to easier access.
Several factors contribute to our satisfactory results. Firstly, as a minimally invasive technique, the PELD procedure can minimize structural damage and preserve stabilization as much as possible. This can minimize the risk of segmental instability after surgery. Secondly, only the extruded or free fragments in the spinal canal were removed and the nucleus material in the disc space was preserved as much as possible. Compared to more aggressive excision of disc material, the limited discectomy technique has advantages, including better preservation of intervertebral disc height, minimization of damage of the annulus fibrosus and lowering of the risk of reherniation. The preservation of intervertebral disc height can prevent the loosening of ligaments and articular capsules, which can prevent segmental instability and associated back pain.18
In conclusion, our study showed that PELD using the transforaminal approach can provide favorable results after a long-term follow-up period. POD is a common complication associated with the PELD procedure. Limited discectomy can preserved the disc-height well and minimize the risk of residual back pain. Although we cannot conclude that PELD is superior to open microdiscectomy for the treatment of lumbar degenerative disease with radicular pain, as a minimally invasive procedure, PELD had inherent advantages including shorter hospital stay and recovery time. Another important advantage of PELD is that this procedure can be performed under local anesthesia. This provides another option for patients with LDH who are deemed to require surgery when their general physical condition is not suitable for general anesthesia. Further high-quality, large-scale randomized clinical trials with long-term follow-up are warranted.
Ethics Approval and Consent to Participate
The study was approved by the ethical committee of the China Rehabilitation Research Center. Written informed consent was obtained from all patients.
Consent for Publication
The author grants Dove Press and the International Journal of General Medicine permission to publish this study.
Acknowledgments
We thank all of the patients who provided the follow-up photos and information.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Beijing Municipal Administration of Hospitals Incubating Program funded by Beijing Municipal Administration of Hospitals (Code PX2020003). The funding body has not been involved in the design, outcomes collection, interpretation or the writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yorimitsu E, Chiba K, Toyama Y, Hirabayashi K. Long-term outcomes of standard discectomy for lumbar disc herniation: a follow-up study of more than 10 years. Spine. 2001;26(6):652–657. doi:10.1097/00007632-200103150-00019
2. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the maine lumbar spine study. Spine. 2005;30(8):927–935. doi:10.1097/01.brs.0000158954.68522.2a
3. Casal-Moro R, Castro-Menéndez M, Hernández-Blanco M, Bravo-Ricoy JA, Jorge-Barreiro FJ. Long-term outcome after microendoscopic diskectomy for lumbar disk herniation: a prospective clinical study with a 5-year follow-up. Neurosurgery. 2011;68(6):1568–1575, 1575. doi:10.1227/NEU.0b013e31820cd16a
4. Benzakour A, Benzakour T. Lumbar disc herniation: long-term outcomes after mini-open discectomy. Int Orthop. 2019;43(4):869–874. doi:10.1007/s00264-019-04312-2
5. Burkhardt BW, Grimm M, Schwerdtfeger K, Oertel JM. The microsurgical treatment of lumbar disc herniation: a report of 158 patients with a mean follow-up of more than 32 years. Spine. 2019;44(20):1426–1434. doi:10.1097/BRS.0000000000003113
6. Nellensteijn J, Ostelo R, Bartels R, Peul W, van Royen B, van Tulder M. Transforaminal endoscopic surgery for symptomatic lumbar disc herniations: a systematic review of the literature. Eur Spine J. 2010;19(2):181–204. doi:10.1007/s00586-009-1155-x
7. Gempt J, Jonek M, Ringel F, Preuss A, Wolf P, Ryang Y. Long-term follow-up of standard microdiscectomy versus minimal access surgery for lumbar disc herniations. Acta Neurochir. 2013;155(12):2333–2338. doi:10.1007/s00701-013-1901-z
8. Gadjradj PS, van Tulder MW, Dirven CM, Peul WC, Harhangi BS. Clinical outcomes after percutaneous transforaminal endoscopic discectomy for lumbar disc herniation: a prospective case series. Neurosurg Focus. 2016;40(2):E3. doi:10.3171/2015.10.FOCUS15484
9. Eun SS, Lee SH, Sabal LA. Long-term follow-up results of percutaneous endoscopic lumbar discectomy. Pain Physician. 2016;19(8):E1161–E1166.
10. Gibson J, Subramanian AS, Scott C. A randomised controlled trial of transforaminal endoscopic discectomy vs microdiscectomy. Eur Spine J. 2017;26(3):847–856. doi:10.1007/s00586-016-4885-6
11. Chen Z, Zhang L, Dong J, et al. Percutaneous transforaminal endoscopic discectomy compared with microendoscopic discectomy for lumbar disc herniation: 1-year results of an ongoing randomized controlled trial. J Neurosurg Spine. 2018;28(3):300–310. doi:10.3171/2017.7.SPINE161434
12. Ahn Y, Lee SG, Son S, Keum HJ. Transforaminal endoscopic lumbar discectomy versus open lumbar microdiscectomy: a comparative cohort study with a 5-year follow-up. Pain Physician. 2019;22(3):295–304. doi:10.36076/ppj/2019.22.295
13. Yeung A, Lewandrowski KU. Five-year clinical outcomes with endoscopic transforaminal foraminoplasty for symptomatic degenerative conditions of the lumbar spine: a comparative study of inside-out versus outside-in techniques. J Spine Surg. 2020;6(Suppl 1):S66–S83. doi:10.21037/jss.2019.06.08
14. Singh K, Heller JG, Samartzis D, et al. Open vertebral cement augmentation combined with lumbar decompression for the operative management of thoracolumbar stenosis secondary to osteoporotic burst fractures. J Spinal Disord Tech. 2005;18(5):413–419. doi:10.1097/01.bsd.0000173840.59099.06
15. Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel RS, Sze GK. Lumbar disc nomenclature: version 2.0: recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J. 2014;14(11):2525–2545. doi:10.1016/j.spinee.2014.04.022
16. Choi I, Ahn JO, So WS, Lee SJ, Choi IJ, Kim H. Exiting root injury in transforaminal endoscopic discectomy: preoperative image considerations for safety. Eur Spine J. 2013;22(11):2481–2487. doi:10.1007/s00586-013-2849-7
17. Jarebi M, Awaf A, Lefranc M, Peltier J. A matched comparison of outcomes between percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for the treatment of lumbar disc herniation: a 2-year retrospective cohort study. Spine J. 2021;21(1):114–121. doi:10.1016/j.spinee.2020.07.005
18. Fakouri B, Patel V, Bayley E, Srinivas S. Lumbar microdiscectomy versus sequesterectomy/free fragmentectomy: a long-term (>2 y) retrospective study of the clinical outcome. J Spinal Disord Tech. 2011;24(1):6–10. doi:10.1097/BSD.0b013e3181bfdd07
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.