")
Back to Archived Journals » Research and Reports in Focused Ultrasound » Volume 2
Microfocused ultrasound for facial rejuvenation: current perspectives
Authors Day D
Received 20 January 2014
Accepted for publication 17 March 2014
Published 5 December 2014 Volume 2014:2 Pages 13—17
DOI https://doi.org/10.2147/RRFU.S49900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Doris Day
Day Dermatology and Aesthetics, New York, NY, USA
Abstract: In contrast with ultrasound imaging, therapeutic ultrasound uses high energy levels >5 W/cm2 and is tightly focused into a small point to rapidly heat and coagulate targeted tissues. The use of high intensity focused ultrasound has recently expanded from high-precision surgical procedures into the field of noninvasive cosmetic medicine. Microfocused ultrasound (MFU) differs from other energy technologies used for skin rejuvenation. A concave disk within the transducer focuses ultrasound energy with very high intensity at specific locations below the epidermis and can specifically target the dermis or superficial musculoaponeurotic system, a fibrous network consisting of collagen fibers, elastic fibers, and fat cells that connects the facial muscles with the dermis and is tightened during a facelift. Where applied, the temperature at the focal point rapidly rises while tissue above and below the focal zone are unaffected. Application of MFU causes collagen fibers to denature and contract and stimulates de novo synthesis of new collagen. MFU combined with visualization (MFU-V) can be applied to the skin with a high degree of precision to noninvasively lift and tighten the dermis and subdermal tissues. The desired treatment depth and the rate of heating can be selected by altering the ultrasound frequency and rate and intensity of energy delivery. One MFU-V device has been approved by the US Food and Drug Administration to noninvasively lift and tighten lax face and neck skin. Common adverse events associated with MFU-V include momentary discomfort during the treatment session, transient erythema and edema, and occasional bruising. Ongoing studies by independent investigators are evaluating the safety and efficacy of MFU-V for lifting and tightening lax skin in other anatomical areas.
Keywords: high intensity focused ultrasound, microfocused ultrasound, noninvasive, facial rejuvenation, skin laxity, skin tightening
Introduction
Therapeutic ultrasound is defined as the use of ultrasound for the treatment of diseased or injured organs or bodily structures.1 It is different from ultrasonography, which uses very low energy ultrasound to penetrate the body and capture reflected ultrasound waves with a transducer to create an image of internal structures. For therapeutic applications, high energy ultrasound with energy levels >5 W/cm2 is tightly focused into a small point that can rapidly heat and coagulate targeted tissues. This high intensity focused ultrasound technology is being used to perform noninvasive surgical procedures with great precision, and is currently being applied in the fields of cardiology, neurology, oncology, and gynecology.2–6
The medical applications of focused ultrasound have also expanded into the field of noninvasive cosmetic surgery. High intensity focused ultrasound is being used as a noninvasive method of body sculpting by coagulating unwanted subcutaneous adipose.7 In contrast, microfocused ultrasound (MFU) can be applied to the skin with much greater precision to noninvasively lift and tighten the dermis and subdermal tissues.8 When combined with ultrasonography for visualization, as in MFU with visualization (MFU-V), specific layers underneath the epidermis can be targeted during treatment. MFU-V differs from other forms of energy technology used for skin rejuvenation, such as radiofrequency, cryolipolysis, and lasers.9–11
General principles
Sound is a wave of mechanical compression that propagates through a medium and is perceptible in the range of human hearing. Ultrasound is a similar wave of mechanical compression, but at frequencies above the range of human hearing (>20 MHz).12 Ultrasound can be characterized by the same physical properties used to describe sound, such as frequency, wavelength, amplitude or intensity, and absorption or energy transfer.13 The frequency of focused ultrasound is measured in cycles per second (or Hz) and energy is expressed in J/cm2.
When used for diagnostic imaging, beams of divergent, low energy ultrasound are rapidly scanned over relatively broad areas of the body. The ultrasound energy is not directed at any one area for long enough to have an effect on tissues;12 however, a concave disk within a transducer can be used to focus ultrasound energy in a highly convergent manner analogous to focusing sunlight with a magnifying glass.1 The properties of sound energy enable it to be focused with very high intensity at specific locations and in a very small volume below the epidermis. There, the focused ultrasound eventually becomes absorbed and the waves of ultrasound are converted into molecular vibrations resulting in heat.13 If sufficiently high levels of energy are used, the temperature at the focal point quickly rises to levels above 60°C, causing coagulation of tissue and denaturation of collagen; however, the temperature immediately above and below the focal zone remains relatively unchanged.14
Unlike other hyperthermia technologies, such as radiofrequency, the attenuation of sound through tissue at ultrasound frequencies is sufficiently low that adequate amounts of energy can reach the necessary tissue depth during clinical treatment. Increasing the ultrasound frequency increases attenuation and heat release, but decreases the depth of penetration,13 increasing the margin of safety when focused ultrasound is used clinically. Frequencies near 4–7 MHz have been found to be most useful for heat deposition, with frequencies as low as 0.5 MHz being used for deep treatments and frequencies as high as 10 MHz being used for shallower treatments. The optimal choice of focused ultrasound frequency is therefore application-specific and represents a balance between the desired treatment depth and the rate of heating.
The total dose of focused ultrasound energy and amount of time required to deliver the total dose of energy can be adjusted as needed. The ability to change the energy provides the flexibility needed to make focused ultrasound suit different clinical requirements. At ultrasound frequencies of approximately 1 MHz, the focal point is only a few cubic millimeters. Because the lesions produced by focused ultrasound are isolated within the treated tissue with no surrounding damage, they are often referred to as “trackless” lesions.15 As the frequency increases, the ability to focus the waves of ultrasound also increases. Together, these relationships make focused ultrasound extremely well suited for performing noninvasive cosmetic therapy.
Preclinical studies
In addition to local tissue coagulation, application of heat using MFU-V causes collagen fibers to denature and contract in the subcutaneous layers.16 Heat contracts collagen by breaking intramolecular hydrogen bonds, causing the chains of collagen to fold and assume a more stable configuration. The result is a thickening and shortening of collagen fibers. Application of high intensity focused ultrasound in adipose tissue has demonstrated partial denaturing of collagen fibers (septae) at a frequency of 1 MHz and diffuse contraction of collagen fibers at 2–3 MHz.16
The superficial musculoaponeurotic system (SMAS) is a fibrous network consisting of collagen fibers, elastic fibers, and fat cells, which connects the facial muscles with the dermis.17 It was hypothesized that targeting the facial SMAS with MFU-V would produce focused thermal denaturation of collagen, which would subsequently stimulate collagen synthesis de novo, resulting in skin tightening and lifting. This required the development of a new ultrasound device that could deliver MFU transcutaneously to the facial SMAS to produce discrete thermal coagulative zones while sparing adjacent nontarget layers above and below the targeted tissue.18 In addition to emitting MFU, this unique device also incorporates diagnostic ultrasound using the same transducers that permit tissue visualization (MFU-V) prior to treatment (Ulthera® system; Ulthera Inc., Mesa, AZ, USA).19
Preclinical studies were performed using nonfixed human cadavers. Using the MFU-V device, the SMAS layer was visualized and targeted using microfocused ultrasound in several facial areas with various combinations of power and exposure time.18 Subsequent histology studies demonstrated reproducible, discrete thermal coagulative zones at depths of up to 7.8 mm, while the skin and surrounding tissue were unaffected. Applying increased energy settings and higher-density lines of exposure produced a greater degree of tissue shrinkage. In a similar study, cadaver skin samples were exposed to a range of MFU up to 45 W at 7.5 MHz with a nominal focal distance of 4.2 mm from the transducer membrane and exposure pulse durations of 50–200 milliseconds.20 By adjusting the treatment exposure parameters, it was possible to create individual and highly confined coagulated lesions up to a depth of 4 mm within the dermis. A precise pattern of individual thermal coagulative zones could be achieved in the deep dermis by applying the transducer sequentially at different exposure locations. The results of these preclinical studies provided evidence that MFU-V could be an effective modality for noninvasive skin lifting and tightening as well as reduction of wrinkles.
Facial rejuvenation
An initial clinical trial assessed the ability of MFU-V to tighten the brow by treating the full face and neck.21 Subjects were medicated with topical anesthetic, and MFU-V was applied to the forehead, temples, cheeks, submental region, and side of the neck using three transducers emitting 4 MHz and 7 MHz at a focal depth of 4.5 mm and 7 MHz at a focal depth of 3.0 mm. At 90 days after treatment, 30 (86%) of 35 evaluable subjects were judged by blinded observers to show clinically significant brow lift, with a mean elevation in eyebrow height of 1.7 mm (P=0.00001). Facial skin biopsies obtained before and 2 months after treatment with MFU-V showed more dermal collagen, with thickening of the dermis and straightening of the elastic fibers in the reticular dermis after treatment.22 These changes coincided with objective improvements in the nasolabial folds, and the jaw lines were improved in all patients. Examples of improvements in skin laxity in periorbital and neck areas are apparent in Figures 1 and 2.
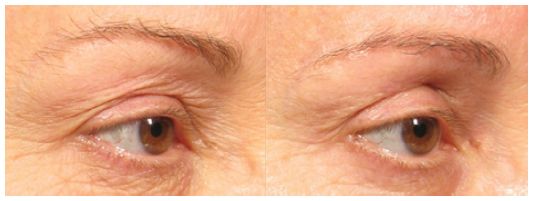 | Figure 1 Improvements in periorbital skin laxity after microfocused ultrasound with visualization. |
 | Figure 2 This patient achieved significant skin tightening in the neck area following microfocused ultrasound with visualization. |
Since 2009, when the currently available MFU-V device was approved by the US Food and Drug Administration,19 numerous studies, totaling over 35 to date, have reported on its safe and effective use for tightening lax facial skin and skin in other anatomical regions. Subsequently, indications for the device have expanded to include tightening of lax skin on the neck and regulatory approval for further indications is expected by the time this paper is published.
Several investigators have reported improved efficacy when multiple treatment passes were used.23 In one study, areas of the face and neck were treated with a 4 MHz 4.5 mm transducer followed by a 7 MHz 3.0 mm transducer. Two blinded clinicians determined that eight of ten evaluable patients showed clinical improvement 90 days after treatment, while nine subjects reported improvement. Another study compared the effectiveness of treating patients with MFU-V at either one or two treatment depths and the effects of varying the number and orientation of treatment lines and total applied energy.24 They reported the 15 vertically oriented treatment lines at tissue depths of 3.0 mm and 4.5 mm produced significantly greater lifting of the opposing brows and marionette lines than 15 horizontally placed treatment lines. Overall, sites receiving treatment lines and higher energy at dual depths showed significantly greater lifting.
MFU-V has also been used as an effective, nonsurgical, tissue-tightening procedure for the treatment of infraorbital skin laxity.25 Because the skin around the eye is relatively thin, a 7.0 MHz 3.0 mm focal depth transducer was used to deliver a single pass over the area to generate microthermal coagulation zones spaced approximately 3.0–5.0 mm apart. Treated patients (n=15) were evaluated after 6 months. Based on objective assessments, two patients were much improved, eleven were improved, and two were unchanged. Based on subjective assessments, three were much improved and 12 were improved.
Safety
Commonly reported adverse events associated with MFU-V include transient discomfort during the treatment session and transient erythema, edema, and occasional bruising.21,23–25 In one study, a single pass of MFU using three transducers emitting 4 MHz and 7 MHz at a focal depth of 4.5 mm and 7 MHz at a focal depth of 3.0 mm caused transient erythema and edema in most patients and focal bruising in up to 25%.26 Two patients were reported to experience post-inflammatory hyperpigmentation 1 month after treatment. Transient dysesthesia lasting 3–10 days has been reported.22,24 Striated linear skin patterns are rare but resolve spontaneously.21,22,24 Following treatment of the cheeks and submentum with a 4.4 MHz 4.5 mm transducer with 1.0 J of energy and a 7.5 MHz 3.0 mm transducer with 0.45 J of energy, the patient developed numbness along the right mandible immediately after the procedure which developed into partial paralysis of the right perioral area the next day, but spontaneously resolved 2 months later.27 The most recent methodology for application of ultrasound energy while using MFU-V substantially improves patient comfort with no loss of efficacy.
Patient selection
Not everyone will achieve maximum benefit from MFU-V treatment, and patient satisfaction will be increased by proper patient selection. MFU-V is best suited for patients with mild to moderate skin and soft tissue laxity. Since the clinical response to MFU-V treatment is partly dependent on de novo collagen synthesis and the so-called “wound healing response”, younger patients are likely to have better outcomes.11 Although this treatment will provide some benefit for all patients, results will also vary with the condition of the skin, such as the amount of skin laxity. Older patients and those with excessively photodamaged skin, extensive skin ptosis/laxity, heavy lipoptosis with jowling, and marked platysmal banding skin may require higher energy density during a single treatment or more than one treatment to achieve maximum benefit.10
Absolute contraindications are relatively few, and include infections or open skin lesions at the proposed treatment area, active severe or cystic acne, and active implants (eg, pacemakers, defibrillators) or metallic implants in the treatment area. Relative contraindications include treatment directly over keloids, implants, dermal fillers, and the presence of factors that could alter or impair wound healing such as smoking.10,11
Conclusion
Microfocused ultrasound has emerged as a safe and effective technology and is currently the only method of achieving lift and tightening of lax skin on the face and neck. Its use in cosmetic medicine continues to grow. Following the success of MFU-V for facial rejuvenation, several independent investigators have evaluated its use for lifting and tightening lax skin in other areas with good results. These include noninvasive lifting of the skin on the upper arms,28 thighs,28 knees,28,29 and décolleté.30
Acknowledgment
The author gratefully acknowledges the editorial assistance of Dr Carl Hornfeldt during preparation of the manuscript.
Disclosure
The author reports no conflicts of interest in this work.
References
Mason TJ. Therapeutic ultrasound an overview. Ultrason Sonochem. 2011;18:847–852. | |
Huisman M, van den Bosch MA. MR-guided high-intensity focused ultrasound for noninvasive cancer treatment. Cancer Imaging. 2011;11:S161–S166. | |
Voogt MJ, van Stralen M, Ikink ME, et al. Targeted vessel ablation for more efficient magnetic resonance-guided high-intensity focused ultrasound ablation of uterine fibroids. Cardiovasc Intervent Radiol. 2012;35:1205–1210. | |
Orsi F, Arnone P, Chen W, Zhang L. High intensity focused ultrasound ablation: a new therapeutic option for solid tumors. J Cancer Res Ther. 2010;6:414–420. | |
Schopka S, Schmid C, Keyser A, et al. Ablation of atrial fibrillation with the Epicor system: a prospective observational trial to evaluate safety and efficacy and predictors of success. J Cardiothorac Surg. 2010;5:34. | |
Foley JL, Little JW, Vaezy S. Effects of high-intensity focused ultrasound on nerve conduction. Muscle Nerve. 2008;37:241–250. | |
Jewell ML, Baxter RA, Cox SE, et al. Randomized sham-controlled trial to evaluate the safety and effectiveness of a high-intensity focused ultrasound device for noninvasive body sculpting. Plast Reconstr Surg. 2011;128:253–262. | |
Dobke MK, Hitchcock T, Misell L, Sasaki GH. Tissue restructuring by energy-based surgical tools. Clin Plast Surg. 2012;39:399–408. | |
Woolery-Lloyd H, Kammer JN. Skin tightening. Curr Probl Dermatol. 2011;42:147–152. | |
Brobst RW, Ferguson M, Perkins SW. Ulthera: initial and six month results. Facial Plast Surg Clin North Am. 2012;20:163–176. | |
MacGregor JL, Tanzi EL. Microfocused ultrasound for skin tightening. Semin Cutan Med Surg. 2013;32:18–25. | |
Kim YS, Rhim H, Choi MJ, Lim HK, Choi D. High-intensity focused ultrasound therapy: an overview for radiologists. Korean J Radiol. 2008;9:291–302. | |
ter Haar GT, Coussios C. High intensity focused ultrasound: physical principles and devices. Int J Hyperthermia. 2007;23:89–104. | |
Dubinsky TJ, Cuevas C, Dighe MK, Kolokythas O, Hwang JH. High-intensity focused ultrasound: current potential and oncologic applications. AJR Am J Roentgenol. 2008;190:191–199. | |
ter Haar GT, Coussios C. High intensity focused ultrasound: past, present and future. Int J Hyperthermia. 2007;23:85–87. | |
Ferraro GA, De Francesco F, Nicoletti G, Rossano F, D’Andrea F. Histologic effects of external ultrasound-assisted lipectomy on adipose tissue. Aesthetic Plast Surg. 2008;32:111–115. | |
Ghassemi A, Prescher A, Riediger D, Axer H. Anatomy of the SMAS revisited. Aesthetic Plastic Surgery. 2003;27:258–264. | |
White WM, Makin IR, Barthe PG, Slayton MH, Gliklich RE. Selective creation of thermal injury zones in the superficial musculoaponeurotic system using intense ultrasound therapy: a new target for noninvasive facial rejuvenation. Arch Facial Plast Surg. 2007;9:22–29. | |
Ulthera, Inc. Ulthera® Operation and Maintenance Manual. Mesa, AZ, USA: Ulthera, Inc. | |
Laubach HJ, Makin IR, Barthe PG, Slayton MH, Manstein D. Intense focused ultrasound: evaluation of a new treatment modality for precise microcoagulation within the skin. Dermatol Surg. 2008;34:727–734. | |
Alam M, White LE, Martin N, Witherspoon J, Yoo S, West DP. Ultrasound tightening of facial and neck skin: a rater-blinded prospective cohort study. J Am Acad Dermatol. 2010;62:262–269. | |
Suh DH, Shin MK, Lee SJ, et al. Intense focused ultrasound tightening in Asian skin: clinical and pathologic results. Dermatol Surg. 2011;37:1595–1602. | |
Lee HS, Jang WS, Cha YJ, et al. Multiple pass ultrasound tightening of skin laxity of the lower face and neck. Dermatol Surg. 2011;38:20–27. | |
Sasaki GH, Tevez A. Clinical efficacy and safety of focused-image ultrasonography: a 2-year experience. Aesthet Surg J. 2012;32:601–612. | |
Suh DH, Oh YJ, Lee SJ, et al. A intense-focused ultrasound tightening for the treatment of infraorbital laxity. J Cosmet Laser Ther. 2012;14:290–295. | |
Chan NP, Shek SY, Yu CS, Ho SG, Yeung CK, Chan HH. Safety study of transcutaneous focused ultrasound for non-invasive skin tightening in Asians. Lasers Surg Med. 2011;43:366–375. | |
Jeong KH, Suh DH, Shin MK, Lee SJ. Neurologic complication associated with intense focused ultrasound. J Cosmet Laser Ther. 2014;16(1):43–44. | |
Alster TS, Tanzi EL. Noninvasive lifting of arm, thigh, and knee skin with transcutaneous intense focused ultrasound. Dermatol Surg. 2012;38:754–759. | |
Gold MH. A prospective, single-center study of the efficacy and safety of micro-focused ultrasound with visualization for the non-invasive treatment of skin wrinkles and laxity above the knee. Presented at the annual meeting of the American Society for Dermatologic Surgery, Atlanta, GA, USA, October11–14, 2012. | |
Fabi SG, Massaki A, Eimpunth S, Pogoda J, Goldman MP. Evaluation of microfocused ultrasound with visualization for lifting, tightening, and wrinkle reduction of the décolletage. J Am Acad Dermatol. 2013;69:965–971. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.