")
Back to Journals » Clinical Ophthalmology » Volume 16
Microbial Contamination of Soft Contact Lenses Among Medical School Students in Southern Iraq
Authors Alasadi SZ , Ibraheim W, Almusawi LA
Received 11 August 2022
Accepted for publication 13 October 2022
Published 4 November 2022 Volume 2022:16 Pages 3651—3660
DOI https://doi.org/10.2147/OPTH.S383086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Salah Zuhair Alasadi,1 Wijdan Ibraheim,2 Loay Abdulmutalib Almusawi1
1Department of Surgery, College of Medicine, University of Basrah, Basrah, Iraq; 2Department of Microbiology, College of Medicine, University of Basrah, Basrah, Iraq
Correspondence: Loay Abdulmutalib Almusawi, Department of Surgery, College of Medicine, University of Basrah, Basrah, 61022, Iraq, Tel +964 7705559205, Email [email protected]
Background: Contamination of CLs and accessories risks potentially devastating microbial keratitis. We aimed to explore the rate of microbial contamination and predisposing factors among a group of asymptomatic young medical students.
Methodology: The study included 115 healthy female medical students with a mean age of 21.64 ± 2.02 years between January and November 2021. Information about CL use, wear and care was gathered. Each participant’s CL and case were swabbed for microbiological identification. Univariable and multivariable analyses were conducted to look for associations with a range of factors.
Results: Overall, 91 participants (79.13%) had at least one contaminated sample (lens and/or case). The rates of contamination of CL and their cases were 66% and 76.5%, respectively. Higher contamination rates were caused by gram-negative bacteria (60% of the contaminated samples) with P. aeruginosa being the most common contaminant both for CL and cases, whereas S. epidermidis and S. aureus were the most common contaminants for the CL and cases, respectively, regarding gram-positive contamination. Multivariable analysis showed younger age as a significant predictor of pseudomonas contamination of the lenses and cases (OR: 12.302, 6.555 for CL & cases, respectively; P = 0.001 for both). Older age was a significant predictor of K. pneumoniae contamination (OR: 4.154, P = 0.007). Pseudomonas contamination of both lenses and cases was predicted by the type of solution used (OR: 10.8 and 13.5, P = 0.001 and 0.003 for bottled and distilled water vs commercially available solutions for CL; OR: 4.5 and 5.8, P = 0.045 and 0.004, respectively, for cases). Pseudomonas case contamination was associated with low frequency of solution change.
Conclusion: Microbial contamination rate of soft CL and their cases is high among young medical students in comparison to previously reported rates and was predisposed by several poor hygienic practices and wearing regimens.
Keywords: soft contact lens, contact lens case, microbial contamination, lens hygiene, lens wearing schedule, medical students
Introduction
The advances in contact lens and lens-care solutions, materials and design have contributed to an increase in contact lens wear, for refractive and aesthetic reasons, to about 140 million users worldwide.1 Nevertheless, CL wear is associated with a variety of potential complications including bacterial and fungal keratitis, acanthamoeba keratitis, papillary conjunctivitis, superior limbic keratoconjunctivitis, neurotrophic corneal ulceration and others.2–4
Contact lens-related bacterial keratitis has become a major cause of all new cases of bacterial keratitis, particularly in high socioeconomic populations such as the United Kingdom (65% of all new cases) and Japan (54.5%).5–7
Bacteria responsible for bacterial keratitis have been isolated from the surface of the contact lens or the contact lens-care solution.8–10
The contact lens disrupts the protective mechanism of the mucin layer of the tear film, hindering its antimicrobial activity on the corneal surface.11
Past studies have highlighted the rate of CL contamination and the variation of corneal pathogens with ambient temperature and humidity.12–14 Hot and humid weather such as in Southern Iraq, where the present study was conducted, as well as lens care regimens and practices imposed by our study population may contribute to variation in CL bacterial contamination.
The aim of the current study was to evaluate the rate of contamination and to determine the types of microorganism in soft contact lenses and their cases among medical school students, and to analyze associations between these and the wearer’s age, the type of contact lens, wearing schedule, frequency of change of CL, duration of wear, handling and cleaning processes, the type of CL solution, and its changing interval.
Methodology
Study Population
The study included 115 healthy female soft contact lens wearers attending medical colleges at the University of Basra between January and November 2021. The study followed the principles of the Declaration of Helsinki and was approved by the institutional review board at the University of Basrah (Ethical Standards and Professional Conduct Authority). Written informed consent was obtained from each participant before commencement of the study. Each participant was interviewed to complete a questionnaire related to their contact lens usage. Information involved personal data such as age, the type of contact lens, wearing schedule, frequency of change of CL, duration of wear, handling and cleaning processes, and the type of CL solution. Participants were excluded from the study if there were unwilling to participate or wearing daily disposable lenses (which do not require lens case) other types of CL (other than soft) or swimming with contact lens in or showing symptoms of ocular surface infection such as discharge and redness. The subjects were all females since no male subject had been encountered wearing soft contact lens during the study period.
Microbiological Technique
The contact lens was gently removed from one eye of each participant using sterile blunt tipped forceps by an experienced staff member at the same time the questionnaire was filled. In accordance with sterile aseptic technique, the concave side of the lens was swabbed using sterile cotton tipped swabs moistened with sterile 0.9% sodium chloride solution.
The lens case was also swabbed, and each was labelled, stored separately and transferred to the laboratory in less than 30 minutes to be incubated in a brain heart infusion broth at 37°C for 24–48 hours. Following this, 0.1 mL of the broth was inoculated into each of blood, MacConkey, chocolate and Sabouraud dextrose agar plates and incubated for 24–48 hours for bacterial isolation and for 2 weeks for fungi. A Vitek® system (bioMerieux Vitek, Hazelwood, Mo, USA) was used to isolate and identify bacterial colonies.
Statistical Analysis
All data entry and subsequent statistical tests were performed using SPSS v26 (SPSS Inc., Chicago, Illinois, USA). Continuous variables were expressed as mean ± standard deviation and categorical variables as frequencies and percentages. All percentages were calculated from the total number of participants. Crude association was tested using the chi-squared test or Fisher's exact test according to statistical assumptions. Predictors that were significant on univariable analysis were subsequently tested for association using binomial logistic regression analysis to calculate the adjusted odds ratio (OR). Significance was considered at P value less than 0.05.
Results
The total sample size was 115 female subjects, with mean age of 21.64 ± 2.02 years (range 18–26 years; median 22 years). Table 1 summarizes the age and CL wear characteristics of the study population. Overall, 91 participants (79.13%) had at least one contaminated sample (lens and/or case). Of these, 76 (66.08%) had a contaminated CL and 88 (76.52%) had a contaminated lens case, with 73 participants (63.5%) demonstrating contamination of both CL and case (Table 2).
 |
Table 1 Demographic and Contact Lens (CL) Wear Characteristics of the Study Population |
 |
Table 2 Contact Lens (CL) and Case Contamination Rates |
The bacteria S. epidermidis and S. aureus accounted for the highest rates of gram-positive contamination of CL (22 contaminated samples) and cases (15 contaminated samples), respectively (Figure 1). The highest rate of gram-negative infection was due to P. aeruginosa, for both lenses and cases where 27 and 39 samples were contaminated, respectively (Figure 2).
 |
Figure 1 Gram-positive bacterial contamination rates. |
 |
Figure 2 Gram-negative bacterial contamination rates. |
More samples were contaminated by gram-negative (n = 69, 60%) than gram-positive bacteria (n = 45, 39%). The causative agent could not be identified in only seven (6.1%) samples, and 29 (25.2%) showed mixed contaminations, as shown by Figure 3.
 |
Figure 3 Distribution of contamination according to gram-stain. |
Univariable analysis (Table 3) showed significant associations between S. aureus CL contamination and both CL change interval exceeding one month, and CL wear exceeding six hours per day (P = 0.015 and 0.035 respectively); however, no such association was found for case contamination. Staphylococcus epidermidis CL contamination was significantly negatively associated with solution change frequency (P = 0.016), but again no such association was found for case contamination.
 |
Table 3 Univariable Analysis of Gram-Positive Contamination |
Univariable analysis of gram-negative contamination (Tables 4 and 5) showed that P. aeruginosa contamination of both CL and case was significantly associated with younger age, longer interval (exceeding one month) between changes of CL, type of solution and its change frequency. E. coli contamination of CL was associated only with CL change intervals exceeding one month (P = 0.029), while K. pneumoniae contamination of the case was associated only with older age (P = 0.003).
 |
Table 4 Predictors of Pseudomonas Aeruginosa Contamination of Contact Lenses and Cases on Univariable Analysis |
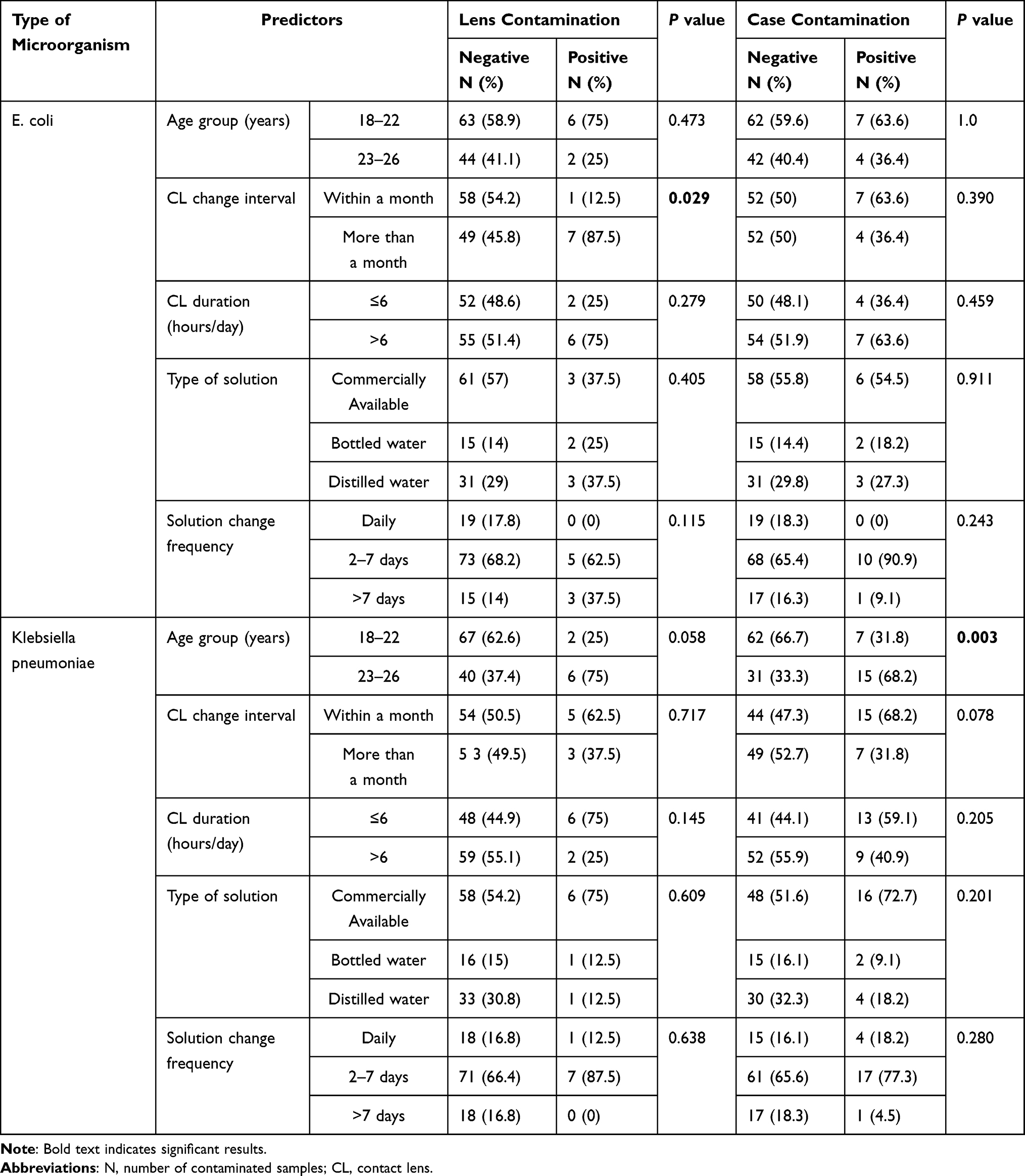 |
Table 5 Univariable Analysis of Other Gram-Negative Bacterial Contamination |
On multivariable analysis (Table 6), younger age was a significant predictor of P. aeruginosa contamination of both lenses and cases as well as K. pneumonia contamination of the cases. Conversely, Klebsiella contamination was associated with older age. In addition, Pseudomonas contamination of the lens was predicted by the type of solution used but not solution change frequency. Pseudomonas contamination of the case could be predicted by using distilled water or bottled water compared to commercially available solution and by lens solution change intervals exceeding one week compared to daily change. Other predictors that were significant on univariable analysis were not significant on multivariable analysis.
 |
Table 6 Multivariable Analysis of Bacterial Contamination of Contact Lenses (CL) and Their Cases |
Discussion
The results of the present study demonstrate a high rate of contact lens and case contamination among asymptomatic female medical students in Southern Iraq. Most of the participants (79.1%) had at least one contaminated sample. Previous related studies reported an overall rate of contamination ranging from 17% to 52%.15–19 However, the present and previous studies were carried out on different populations and samples were collected using a range of methodologies. Poor hygienic practices were present among our study population such as wetting the CL with saliva before applying it to the eye in at least one participant. The risks associated with this practice are well documented. Contact lens cases had a higher contamination rate in our study than the lenses themselves (88 vs 76 samples). It is possible that micro-organisms flourish in the contact lens case first followed by secondary contamination of the lens.19 Several other comparable studies from nearby regions have also reported a relatively high rate of contamination of CL cases (Table 7).16–19 However, several factors other than lens care practice could potentially influence the rate of microbial contamination, including population age, gender, type of contact lens, environmental temperature and microbial isolation techniques.
 |
Table 7 Rate of Microbial Contamination of Contact Lenses (CL) and Their Cases as Reported by Various studies16–19 |
It is known that bacterial adherence to contact lenses increases with decreased water content of the lens and that hydrophobic lenses are more susceptible to bacterial adherence than high water-content lenses.20 High ambient temperature in the range of 35 Celsius and above can contribute to dehydration of the lens and possibly increasing bacterial adherence and thereby account for the higher contamination rate observed in our study.21
Six different species of bacteria were identified in our study. Gram positive bacteria included Staph. aureus, Staph epidermidis and Bacillus species. Although these micro-organisms may provide a small contribution to the normal microbiome of the ocular surface, they can be involved in devastating keratitis especially under compromised ocular surface conditions which may be associated with chronic contact lens use.5,22,23 In fact, there is some evidence that epithelial cells of the ocular surface respond weakly to colonization by bacteria that contribute to normal microbial flora, perhaps allowing more severe ocular infection when caused by these micro-organisms.24 Multivariable analysis in the present study showed no significant association between the three identified species and any lens wear regimen or lens care practice.
Gram negative bacteria that were identified include Pseudomonas aeruginosa, Klebsiella pneumoniae and E. coli. These micro-organisms are thought to rarely contribute to normal flora of the ocular surface; however, recent genomic evidence suggests that they may contribute significantly to the normal ocular microbiome and may therefore cause severe keratitis with devastating outcomes.24 Pseudomonas in particular is known to be the most common cause of contact lens-related aggressive bacterial keratitis.5,17 Consequently, identifying and addressing risk factors for pseudomonas contamination could potentially decrease the incidence of such aggressive forms of keratitis.
In our study, Pseudomonas contamination was significantly associated with younger participants who were six to 12 times more likely to have CL and case contamination, respectively. This can be attributed to the possible lack of sufficient knowledge about the risks associated with poor contact lens care in this age group and that older medical students may be more aware of anterior segment pathology and the need for careful CL care practice. The use of bottled or distilled water significantly increased the odds of P. aeruginosa contamination of both CL and case when compared to commercially available solution. This is expected since commercially available solutions are preserved; however, no currently available solution is immune to contamination.25 Longer time intervals between solution changes were associated with pseudomonas contamination of cases only. The lack of significant association may be due to the limited number of contaminated CL samples.
Our study was limited by the number of samples contaminated by some species, and this may contribute to the lack of statistical significance with respect to those species.
Conclusion
Microbial contamination rate of soft CL and their cases is high among young medical students in comparison to previously reported rates and was predisposed by several poor hygienic practices and wearing regimens. We recommend further larger population-based studies to identify and confirm the association between certain poor hygienic practices and CL wear and to educate the population in general and soft CL wearers in particular regarding the possibility of serious microbial infections that can result from high contamination rates due to poor hygienic practices.
Funding
The study did not receive any grants and the funding was self-provided by authors.
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Sulley A, Young G, Hunt C. Factors in the success of new contact lens wearers. Cont Lens Anterior Eye. 2017;40(1):15–24. doi:10.1016/j.clae.2016.10.002
2. Lim CHL, Stapleton F, Mehta JS. Review of contact lens-related complications. Eye Contact Lens. 2018;44(Suppl 2):S1–S10. doi:10.1097/ICL.0000000000000481
3. Bischoff G, Kuhn D. Der ophthalmologe: Zeitschrift der deutschen [contact lens complications: diagnosis and treatment]. Ophthalmologischen Gesellschaft. 2018;115(12):1087–1102. German. doi:10.1007/s00347-018-0812-z
4. Batlle-Ferrando S, Marín-Martínez S, Boniquet S, Sabater N. Complicaciones asociadas al uso de lentes de contacto blandas [Complications associated with the use of soft contact lenses]. Semergen. 2020;46(3):208–213. Spanish. doi:10.1016/j.semerg.2019.09.004
5. Green M, Apel A, Stapleton F. Risk factors and causative organisms in microbial keratitis. Cornea. 2008;27(1):22–27. doi:10.1097/ICO.0b013e318156caf2
6. Dart JK, Stapleton F, Minassian D, Dart JKG. Contact lenses and other risk factors in microbial keratitis. Lancet. 1991;338(8768):650–653. doi:10.1016/0140-6736(91)91231-I
7. Toshida H, Kogure N, Inoue N, Murakami A. Trends in microbial keratitis in Japan. Eye Contact Lens. 2007;33(2):70–73. doi:10.1097/01.icl.0000237825.98225.ca
8. Mayo MS, Schlitzer RL, Ward MA, Wilson LA, Ahearn DG. Association of Pseudomonas and Serratia corneal ulcers with use of contaminated solutions. J Clin Microbiol. 1987;25:1398–1400. doi:10.1128/jcm.25.8.1398-1400.1987
9. Martins EN, Farah ME, Alvarenga LS, Yu MC, Hoflin-Lima AL. Infectious keratitis: correlation between corneal and contact lens cultures. CLAO J. 2002;28:146–148.
10. Mela EK, Giannelou IP, Koliopoulos JX, Gartaganis SP, John KX, Sotirios GP. Ulcerative keratitis in contact lens wearers. Eye Contact Lens. 2003;29:207–209. doi:10.1097/01.icl.0000078102.30635.A7
11. Tariq F, Koay P. The risk of contact lens wear and the avoidance of complications. Int J Med Stud. 2013;1(2):80–85. doi:10.5195/ijms.2013.209
12. Sweeney DF, Willcox MD, Sansey N, et al. Incidence of contamination of preserved saline solutions during normal use. CLAO J. 1999;25:167–175.
13. Yung MS, Cho P, Yap M. A market survey of contact lens practice in Hong Kong. Clin Exp Optom. 2005;88:165–175. doi:10.1111/j.1444-0938.2005.tb06690.x
14. Walkden A, Fullwood C, Tan SZ, et al. Association between season, temperature and causative organism in microbial keratitis in the UK. Cornea. 2018;37(12):1555–1560. doi:10.1097/ICO.0000000000001748
15. Panthi S, Paudel P, Chaudhary M, Sapkota K, Shah DN. Microbial contamination of contact lens care accessories and compliance with care regimens in Nepal. Cont Lens Anterior Eye. 2014;37(1):2–10. doi:10.1016/j.clae.2013.07.001
16. Thakur DV, Gaikwad UN. Microbial contamination of soft contact lenses & accessories in asymptomatic contact lens users. Indian J Med Res. 2014;140(2):307–309.
17. Waleed AM, Lua’i AI, Wisam S, Sana J. Antimicrobial susceptibility of bacterial isolates from the conjunctiva, storage cases and mobile phones of university students using contact lenses. Cont Lens Anterior Eye. 2021;44(1):62–66. doi:10.1016/j.clae.2019.10.139
18. Rahim N, Bano H, Naqvi BS. Bacterial contamination among soft contact lens wearer. Pak J Ophthalmol. 2008;24(2):93–96.
19. Yung MS, Boost M, Cho P, Yap M. Microbial contamination of contact lenses and lens care accessories of soft contact lens wearers (university students) in Hong Kong. Ophthalmic Physiol Opt. 2007;27(1):11–21. doi:10.1111/j.1475-1313.2006.00427.x
20. Dutta D, Cole N, Willcox M. Factors influencing bacterial adhesion to contact lenses. Mol Vis. 2012;18:14–21.
21. Chan VWY, Phan CM, Walther H, Ngo W, Jones L. Effects of temperature and blinking on contact lens dehydration of contemporary soft lens materials using an in vitro blink model. Transl Vis Sci Technol. 2021;10(8):11. doi:10.1167/tvst.10.8.11
22. Zhou Y, Holland MJ, Makalo P, et al. The conjunctival microbiome in health and trachomatous disease: a case control study. Genome Med. 2014;6(11):99. doi:10.1186/s13073-014-0099-x
23. Al-Shakarchi F. Initial therapy for suppurative microbial keratitis in Iraq. Br J Ophthalmol. 2007;91(12):1583–1587. doi:10.1136/bjo.2007.123208
24. Petrillo F, Pignataro D, Lavano MA, et al. Current evidence on the ocular surface microbiota and related diseases. Microorganisms. 2020;8(7):1033. doi:10.3390/microorganisms8071033
25. Szczotka-Flynn LB, Pearlman E, Ghannoum M. Microbial contamination of contact lenses, lens care solutions, and their accessories: a literature review. Eye Contact Lens. 2010;36(2):116–129. doi:10.1097/ICL.0b013e3181d20cae
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.