")
Back to Journals » Infection and Drug Resistance » Volume 13
Metagenomic Next-Generation Sequencing in Diagnosis of a Case of Pneumocystis jirovecii Pneumonia in a Kidney Transplant Recipient and Literature Review
Authors Chen J , He T, Li X, Wang X, Peng L , Ma L
Received 9 April 2020
Accepted for publication 21 July 2020
Published 13 August 2020 Volume 2020:13 Pages 2829—2836
DOI https://doi.org/10.2147/IDR.S257587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Jie Chen,1,* Ting He,1,* Xiujun Li,2,* Xue Wang,1 Li Peng,1 Liang Ma3
1Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Pathology, College of Basic Medicine, Chongqing Medical University, Chongqing, People’s Republic of China; 3Critical Care Medicine Department, NIH Clinical Center, Bethesda, MD, USA
*These authors contributed equally to this work
Correspondence: Li Peng
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, 1 Youyi Road, Yuzhong District, Chongqing, People’s Republic of China
Email [email protected]
Background: Despite the increasing incidences of Pneumocystis jirovecii pneumonia (PCP) in renal transplant recipients, diagnosis of PCP remains challenging due to its nonspecific clinical presentation and the inadequate performance of conventional diagnostic methods. There is a need for novel diagnostic methods.
Case Presentation: A 27-year-old woman developed acute pneumonia 4 months after renal transplantation. Blood tests revealed a low CD4 count, a normal 1,3-beta-D-glucan level and other changes typical of inflammatory responses. Chest imaging showed bilateral diffuse infiltrates. Microscopic examination of stained sputum and bronchoalveolar lavage fluid (BALF) smear specimens did not find Pneumocystis organisms. There was also no evidence for other pathogens known to cause pneumonia in various antibody and culture tests. Direct metagenomic next-generation sequencing (mNGS) analysis of a BALF specimen identified a large number of P. jirovecii reads, allowing to confirm the diagnosis of PCP. Following treatment with trimethoprim-sulfamethoxazole for two weeks, the patient was cured and discharged.
Conclusion: This case report supports the value of mNGS in diagnosing PCP, highlights the inadequate sensitivity of conventional diagnostic methods for PCP, and calls for the need to add PCP prophylaxis to the current Diagnosis and Treatment Guideline of Invasive Fungal Infections in Solid Organ Transplant Recipients in China.
Keywords: Pneumocystis jirovecii pneumonia, renal transplant, diagnosis, metagenomic next-generation sequencing
Introduction
Pneumocystis pneumonia (PCP) is a major opportunistic infection in immunocompromised patients. With the introduction of antiretroviral therapy and prophylaxis of PCP, the morbidity and mortality of PCP in HIV-infected patients has decreased significantly, but the incidence of PCP in non-HIV infected patients is increasing gradually,1–4 especially in renal transplant recipients.5 Following the first report of a cluster of 5 cases in Switzerland in 1991, at least 393 cases of PCP in renal transplant recipients have been reported in approximately 50 studies across the world (Table S1).
To date, the causative agent of PCP in humans, Pneumocystis jirovecii, still cannot be reliably grown in vitro, and thus clinical diagnosis of PCP depends largely on microscopic detection of P. jirovecii organisms in respiratory specimens following chemical or immunofluorescence staining.6,7 However, these methods suffer from low sensitivity and specificity. Detection of serum 1,3-beta-D-glucan (BDG) appears to be sensitive but lack specificity for P. jirovecii.8 Development of various polymerase chain reaction (PCR)-based diagnostic assays has significantly improved the sensitivity and specificity;9,10 several commercially available P. jirovecii PCR kits have been approved for clinical use in some countries, primarily in Europe, but not in other countries, such as the United States and China.
Recently, metagenomic next-generation sequencing (mNGS) has rapidly emerged as a promising single, universal (or hypothesis-free), culture-independent pathogen detection tool that can be performed directly on clinical specimens.11,12 mNGS determines sequences of all nucleic acids in a sample (regardless of their origins) and then assigns sequence reads to their reference genomes to determine which microbes are present and in what proportions.13 In contrast to the current molecular assays including PCR and microarray which target only one or a limited number of known pathogens using specific primers or probes, mNGS targets all DNA or RNA present in a sample, allowing to detect the entire microbiome (including atypical or novel microbes) as well as the human host genome or transcriptome in patient samples. This method has been successfully used as a diagnostic tool for various infectious diseases including PCP.14–17 Its application to diagnose PCP in renal transplant recipients has been attempted in one study,18 and its value awaits further evaluation. Here we report a case of PCP diagnosed by mNGS following negative results in multiple conventional diagnostic tests. In addition, we provide a literature review of diagnostic methods for PCP in renal transplant recipients.
Case Report
A 27-year-old woman was admitted to our hospital (Nov 2, 2018), complaining of two weeks of cough, intermittent low fever and dyspnea during daily activity. Four months prior to the admission, she underwent a renal transplantation because of kidney failure caused by chronic glomerulonephritis. Following successful transplantation, she took immunosuppressive medication, including tacrolimus (2.5 mg twice a day), mycophenolate mofetil (750 mg twice a day) and methylprednisolone (12 mg daily) for four months. During this period, she did not receive influenza immunization or prophylaxis for opportunistic infections including Pneumocystis and cytomegalovirus (CMV) infections as per the Diagnosis and Treatment Guideline of Invasive Fungal Infections in Solid Organ Transplant Recipients in China (2016 edition).19 Two weeks prior to admission to our hospital, she presented to a local community hospital with complaints of fever, cough and dyspnea during daily activity. Chest X-ray showed bilateral patchy, cloudy opacities in the lower lungs with some adjacent pleural thickening and adhesion (Figure 1A). After empiric treatment with oral moxifloxacin for 7 days, there was no apparent improvement, with fever remaining high (38°C) and dyspnea aggravated.
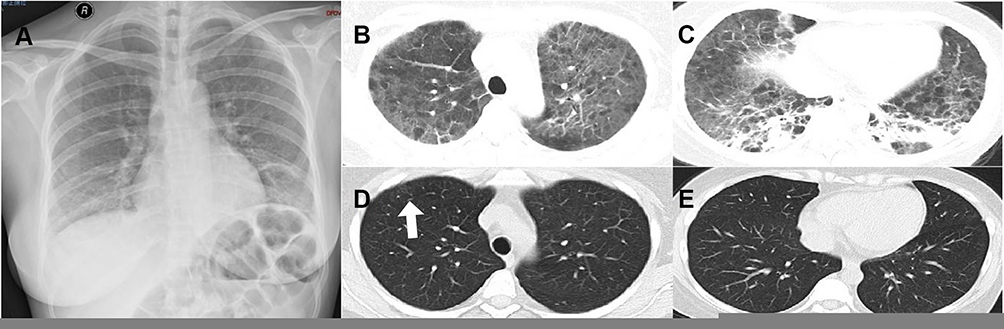 |
Figure 1 Chest images. (A) Chest X-ray showing bilateral patchy, cloudy opacities in the lower lungs with some adjacent pleural thickening and adhesion before treatment. (B and C) Chest HRCT showing diffused stripes as well as reticular and ground-glass opacities with honeycomb structures, primarily in the lower lungs before treatment. (D and E) Chest HRCT scan showing a faint patchy opacity in the lateral segment (white arrow). |
Upon admission to our hospital, physical examination found a normal body temperature of 36.7°C, blood pressure of 143/93 mm Hg, pulse of 116 beats per minute, and respiration rate of 24 per minute. Moist rales appeared bilaterally, with no lower-extremity edema. Due to hypoxemia (PO2: 63 mmHg, PCO2: 29 mmHg, SO2: 90%), she was given oxygen therapy with mask hydrogen inhalation shortly after admission. High-resolution computed tomography (HRCT) demonstrated diffused stripes and reticular and ground-glass opacity with honeycomb structures, primarily in the lower lungs (Figure 1B and C). Other laboratory tests revealed abnormal values for almost all parameters tested elevated levels of several biomarkers for inflammatory responses and decreased counts of lymphocyte and CD4 cells, as detailed in Table 1. Electrocardiogram was normal while echocardiogram showed left ventricular hypertrophy with decreased diastolic dysfunction. Serological assays showed positive results for IgM antibodies to Parainfluenza virus, but negative results for antibodies to respiratory syncytial virus, influenza virus (types A and B), cytomegalovirus (CMV), Adenovirus, Legionella pneumophila, Mycoplasma pneumonia, Chlamydia pneumoniae, Q-rickettsia, and Cryptococcus neoformans. Serum galactomannan and BDG levels were both normal (Table 1). Diff-Quick staining of sputum smear did not find Pneumocystis organisms. Blood culture was negative. Mycobacterium tuberculosis was negative based on blood test with T-SPOT.TB (Oxford Immunotec Ltd. UK) as well as acid-fast staining of sputum smear.
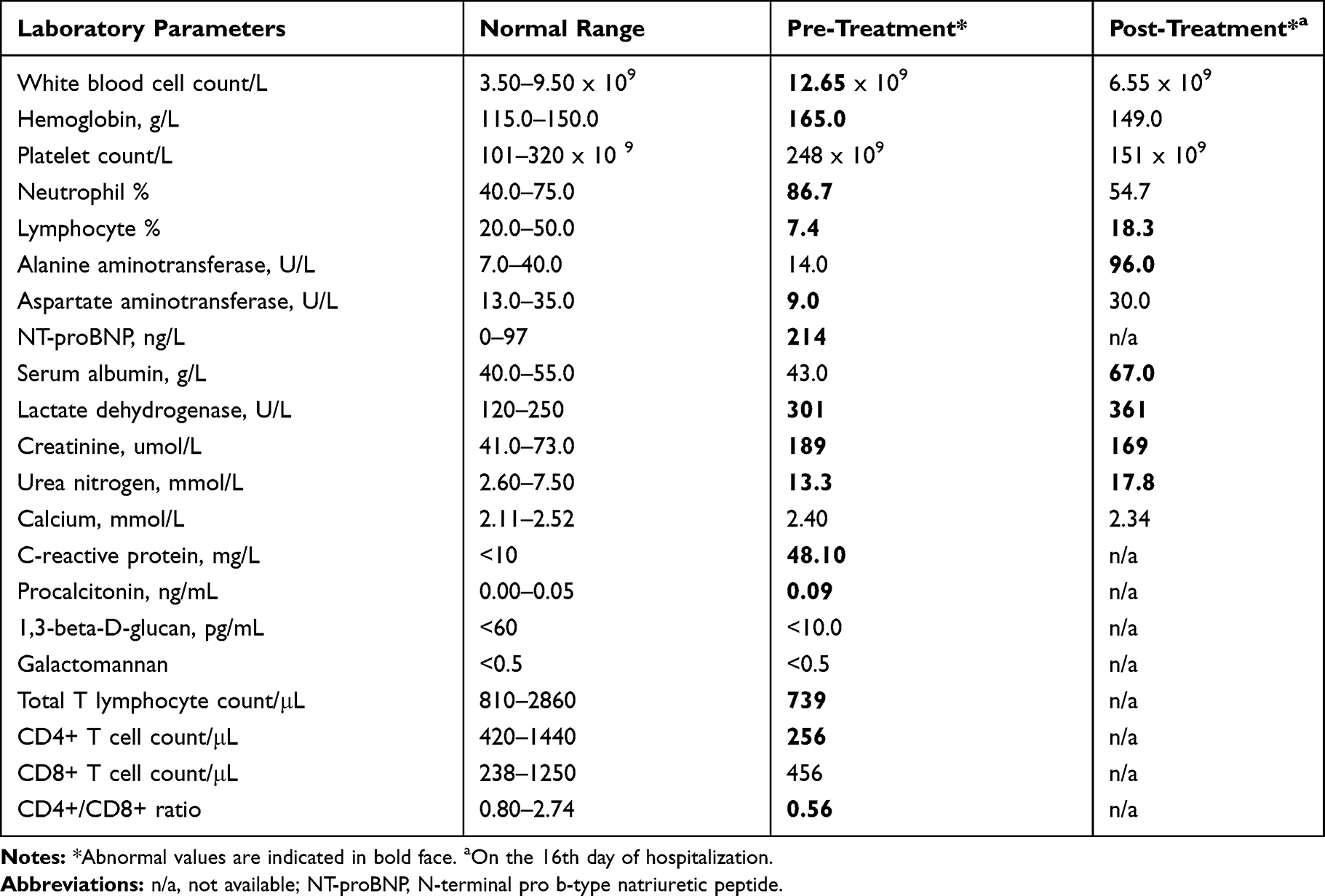 |
Table 1 Main Laboratory Test Results Before and After Treatment |
Considering the patient was at the high-risk stage to develop opportunistic infections, she was firstly given intravenous antibacterial (meropenem 1g thrice a day) and antiviral (ganciclovir 125g twice a day) treatment on the first day of hospitalization. After 3 days of treatment, she still had fever (38°C) and dyspnea. The antimicrobial treatment was changed to intravenous caspofungin (50mg daily), oral trimethoprim-sulfamethoxazole (TMP-SMX, 320/1600mg quadruple a day), and intravenous methylprednisolone (40mg daily), which resulted in improvement of general conditions and abatement of fever and dyspnea in 3 days. However, chest HRCT showed worsening of the opacity in the lower lungs.
On the 13th day of hospitalization, she underwent endobronchial ultrasound transbronchial lung biopsy combined with bronchoalveolar lavage fluid (BALF) collection under laryngeal mask airway instead of a regular bronchoscopy examination due to respiratory failure. Subsequent microbiological tests of BALF were negative for M. tuberculosis and P. jirovecii by the GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, CA, US) and Diff-Quick staining, respectively. In addition, BALF culture revealed no growth of bacteria or fungi; galactomannan level was in the normal range (OD index <0.5).
The consistently negative results in all etiological tests prompted us to submit 3 mL of BALF for mNGS by the Beijing Genomics Institute (Wuhan, Hubei Province, China) using the MGISeq 2000 platform (MGI Tec, Shenzhen, China). The results of mNGS were received <72h after shipping out the BALF sample. Based on the mNGS report (Table S2), there were 10 bacterial species (5 to 1406 reads per species), 1 fungal species (1,665,693 reads) and 1 viral species (12 reads). None of these species are well-established pathogenic organisms causing respiratory infections in humans except for the fungus P. jirovecii, which is the most dominant species, accounting for 99% of all microbial reads (6.8% of the total filtered reads including human DNA reads). The reads for P. jirovecii allowed assembly of the complete mitogenome of P. jirovecii (35,285 bp, GenBank accession number MT319762), which is 98–99% identical to 13 known P. jirovecii mitogenomes.20,21 In addition, these reads allowed assembly of the partial nuclear genome of P. jirovecii, which is ~90% complete compared to the P. jirovecii RU7 reference genome22 and which is included in a separate manuscript to be published elsewhere. Examination of the mitochondrial and nuclear genome assemblies showed no known nonsynonymous mutations in the dihydropteroate synthase (dhps), dihydrofolate reductase (dhfr) and cytochrome b (cob) genes.6
One week after transbronchial lung biopsy (5 days after receiving mNGS report), pathological examination of lung biopsy with hematoxylin-eosin (HE) stain (Figure S1a) reported that alveolar spaces were filled with abundant foamy or granular eosinophilic exudate as well as a few lymphocytes infiltrate; the alveolar septa became thickened due to edema and dilated capillaries. Gomori methenamine-sliver staining of the lung biopsy displayed a plenty of dark brown oval or cup-shaped organisms in alveolar spaces, consistent with the morphology of P. jirovecii (Figure S1b).
After completion of the treatment regimen with caspofungin for 14 days and TMP-SMX for 16 days, her symptoms disappeared, general conditions returned to normal and laboratory findings improved (Table 1). The patient was discharged after 16 days of hospitalization. She continued to take oral TMP-SMX for another two weeks. At her 2-week follow-up visit, she had no symptoms and chest HRCT scan exhibited no abnormal finding except for a faint patchy opacity in the lateral segment (Figure 1D and E). At her 9-month follow up, she appeared healthy with no symptoms and chest HRCT was normal.
Discussion
Despite its high prevalence in immunocompromised individuals, diagnosis of PCP remains challenging due to its nonspecific clinical manifestations and the inadequate performance of current conventional diagnostic methods. This challenge is well reflected in the present case report. As a renal transplant recipient without prophylaxis for opportunistic infections, the patient in this report was apparently at high risk for PCP, as further supported by the low CD4 count (192/μL). However, the P. jirovecii organism was consistently missed in microscopic examination of stained sputum smear and BALF samples. In addition, serum BDG level was completely normal (Table 1). These findings point out the inadequate sensitivity of microscopic examination of stained samples and serum BDG assay for diagnosing PCP.
In literature review, we noted a total of 393 reported PCP cases in renal transplant recipients, of which 70% (275) were detected by microscopic examination, 42% (164) by PCR and 6% (23) by pathological examination (Table S1).18,23–67 At least 16 of these cases in 4 studies were tested for serum BDG levels, with 11 of them being normal. The observation of normal BDG levels in these PCP studies including our present case is in contrast to the high sensitivity of serum BDG test (91% to 96%) demonstrated in three meta-analyses.68–70 Given the high load of P. jirovecii organisms in BALF in our patient as revealed by mNGS, the finding of a very low level of serum BDG is unexpected but consistent with the report of Zhang et al18 in which one renal transplant patient with PCP showed a normal serum BDG level (<31 pg/mL) and a high load of P. jirovecii organisms in BALF (9092 reads). The reasons for this are unclear and may be due to the failure of the BDG test or the lack of circulating BGD in the blood.
The observation of the very low level of serum BDG, together with the consistently negative results in microscopic examination of sputum and BALF smear samples in this case had led us to think that the pneumonia was likely to be caused by a pathogen other than P. jirovecii (which is one reason we did not seek to perform PCR for P. jirovecii). To look for other potential pathogens, we performed mNGS to this case directly using a single BALF sample (3 mL) without depletion of human DNA or enrichment of P. jirovecii DNA. Unexpectedly, a large number of P. jirovecii reads (1,665,693) was obtained, accounting for 6.8% of the total filtered mNGS reads (including human DNA reads), which is substantially higher than the ratio (<0.4–1%) described previously in NGS sequencing of DNA directly extracted from lung tissue or BALF samples from patients heavily infected by P. jirovecii.20–22 This finding, combined with the medical history and clinical manifestations as well as the results of pathological examination of lung biopsy firmly established P. jirovecii as the causative agent of pneumonia in this case. The successful assembly of the complete mitogenome and partial nuclear genome of P. jirovecii from this case suggests a potential to directly sequence the complete or a large proportion of the P. jirovecii genome using BALF specimens from heavily infected patients.
To date, there have been 5 reports on successful use of mNGS to diagnose pulmonary infections involving P. jirovecii (Table 2).14–18 While the sample size is small (1 to 13 specimens each), these studies involve the use of different types of specimens (BALF, sputum, lung biopsy and blood) and different NGS platforms. The numbers of sequence reads for P. jirovecii are highly variable (2 to 303,572) among studies though all are less than the P. jirovecii reads identified from our case (1,665,693). Two of these studies reported that mNGS is more sensitive than conventional methods (non-PCR based).14,18 Theoretically, PCR should be not only more sensitive but also simpler, faster and less expensive than mNGS. However, PCR testing depends on hypothesis (presumptive diagnosis) and currently, there is no PCR assay available and approved for clinical diagnosis of PCP in China. Under the current Chinese Guidelines for Diagnosis and Treatment of HIV/AIDS (2018),71 microscopic detection of Pneumocystis cysts or trophozoites in stained respiratory samples is the only way to confirm PCP diagnosis, without including PCR or other molecular methods. Compared to PCR as well as other conventional diagnostic methods, mNGS has the main advantages of hypothesis-free testing and unbiased samples, allowing identification of all potential known and new or unexpected pathogens.11–13 The whole process of mNGS in our case took less than 72h (from shipping out the BAL sample to receiving the mNGS report). These advantages enabled us to identify P. jirovecii as the cause of the disease in our patient. Another advantage of mNGS is its capacity to provide genome-wide information that may be useful for strain identification and drug resistance prediction. In our case, analysis of mNGS data revealed no nonsynonymous mutations in dhps, dhfr or cob gene.6 Nevertheless, the application of mNGS to clinical diagnosis is still challenging due to its fairly high cost, difficulty to obtain high-quality samples, demand for sophisticated bioinformatics analysis, and barriers in standardization of the entire process from sample collection to result interpretation. Clearly, all these issues warrant further investigation in the future.
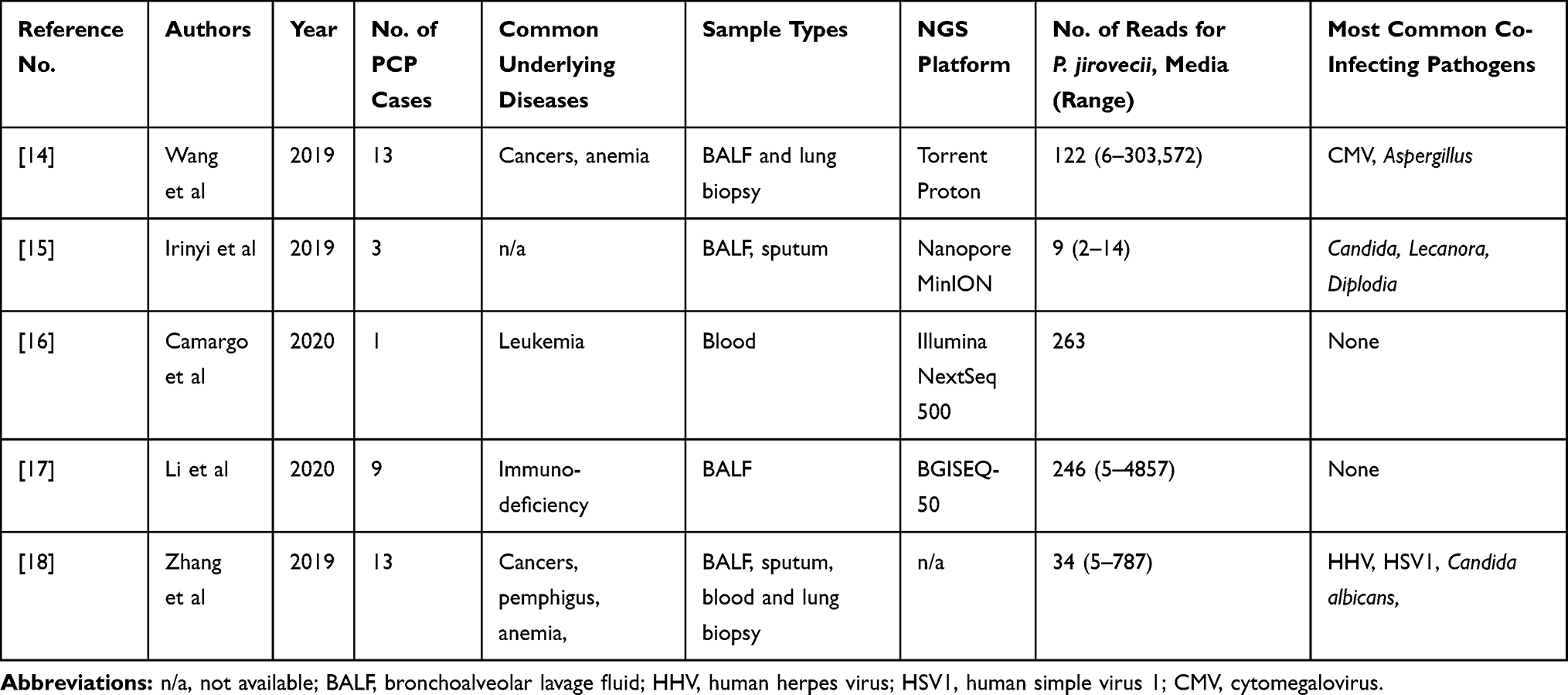 |
Table 2 Reports of PCP Cases Detected by Metagenomics Next-Generation Sequencing (mNGS) |
The increasing incidence of PCP outbreaks in renal transplant recipients worldwide has underscored the necessity of prophylaxis in this patient population.72 The patient in this report was not given any prophylaxis according to the Diagnosis and Treatment Guideline of Invasive Fungal Infections in Solid Organ Transplant Recipients in China (2016 edition).19 Even in the most recent edition (2019) of this guideline, PCP prophylaxis is still not recommended.73 Our case report, together with the widespread adoption of PCP prophylaxis in solid organ transplant recipients in many countries,72,74,75 highlights the need to add PCP prophylaxis to the relevant guideline in China.
In summary, we presented a case of PCP in a Chinese patient who developed acute pneumonia after renal transplantation but showed negative results for P. jirovecii and other common known respiratory pathogens in multiple conventional diagnostic tests. Direct mNGS analysis of a single BALF specimen identified a large number of P. jirovecii reads, allowing to confirm the diagnosis of PCP. This case report supports the value of mNGS in diagnosing infectious diseases, highlights the inadequate sensitivity of conventional diagnostic methods for PCP, and calls for the need to add PCP prophylaxis to the current Diagnosis and Treatment Guideline of Invasive Fungal Infections in Solid Organ Transplant Recipients in China.
Statement of Ethics
This research complies with the guidelines for human studies and is in accordance with the Declaration of Helsinki. This work was approved by Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University, China (No. 20172901). Written informed consent was obtained from the patient for the participation in this study and the publication of associated data including radiological and histological images. The authors confirmed that personal identity information of the patient data was unidentifiable from this report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Brown GD, Denning DW, Gow NA, Levitz SM, Netea MG, White TC. Hidden killers: human fungal infections. Sci Transl Med. 2012;4(165):165rv13. doi:10.1126/scitranslmed.3004404
2. Kelley CF, Checkley W, Mannino DM, Franco-Paredes C, Del Rio C, Holguin F. Trends in hospitalizations for AIDS-associated Pneumocystis jirovecii pneumonia in the United States (1986 to 2005). Chest. 2009;136(1):190–197. doi:10.1378/chest.08-2859
3. Maini R, Henderson KL, Sheridan EA, et al. Increasing Pneumocystis pneumonia, England, UK, 2000–2010. Emerg Infect Dis. 2013;19(3):386–392. doi:10.3201/eid1903.121151
4. Wickramasekaran RN, Jewell MP, Sorvillo F, Kuo T. The changing trends and profile of pneumocystosis mortality in the United States, 1999–2014. Mycoses. 2017;60(9):607–615. doi:10.1111/myc.12636
5. Le Gal S, Toubas D, Totet A, et al. Pneumocystis infection outbreaks in organ transplantation units in France: a nation-wide survey. Clin Infect Dis. 2020;70(10):2216–2220. doi:10.1093/cid/ciz901
6. Ma L, Cisse OH, Kovacs JA. A molecular window into the biology and epidemiology of Pneumocystis spp. Clin Microbiol Rev. 2018;31(3):e00009–18.
7. Desoubeaux G, Franck-Martel C, Caille A, et al. Use of calcofluor-blue brightener for the diagnosis of Pneumocystis jirovecii pneumonia in bronchial-alveolar lavage fluids: a single-center prospective study. Med Mycol. 2017;55(3):295–301. doi:10.1093/mmy/myw068
8. Del Corpo O, Butler-Laporte G, Sheppard DC, Cheng MP, McDonald EG, Lee TC. Diagnostic accuracy of serum (1-3)-β-D-glucan for Pneumocystis jirovecii pneumonia: a systematic review and meta-analysis. Clin Microbiol Infect. 2020;
9. Fan LC, Lu HW, Cheng KB, Li HP, Xu JF. Evaluation of PCR in bronchoalveolar lavage fluid for diagnosis of Pneumocystis jirovecii pneumonia: a bivariate meta-analysis and systematic review. PLoS One. 2013;8(9):e73099. doi:10.1371/journal.pone.0073099
10. Summah H, Zhu YG, Falagas ME, Vouloumanou EK, Qu J. Use of real-time polymerase chain reaction for the diagnosis of Pneumocystis pneumonia in immunocompromised patients: a meta-analysis. Chin Med J (Engl). 2013;126(10):1965–1973.
11. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
12. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14(1):319–338. doi:10.1146/annurev-pathmechdis-012418-012751
13. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
14. Wang J, Han Y, Feng J. Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis. BMC Pulm Med. 2019;19(1):252. doi:10.1186/s12890-019-1022-4
15. Irinyi L, Hu Y, Hoang MTV, et al. Long-read sequencing based clinical metagenomics for the detection and confirmation of Pneumocystis jirovecii directly from clinical specimens: a paradigm shift in mycological diagnostics. Med Mycol. 2019:myz109. doi:10.1093/mmy/myz109.
16. Camargo JF, Ahmed AA, Lindner MS, et al. Next-generation sequencing of microbial cell-free DNA for rapid noninvasive diagnosis of infectious diseases in immunocompromised hosts. F1000Res. 2019;8:1194. doi:10.12688/f1000research.19766.3
17. Li Y, Sun B, Tang X, et al. Application of metagenomic next-generation sequencing for bronchoalveolar lavage diagnostics in critically ill patients. Eur J Clin Microbiol Infect Dis. 2020;39(2):369–374. doi:10.1007/s10096-019-03734-5
18. Zhang Y, Ai JW, Cui P, Zhang WH, Wu HL, Ye MZ. A cluster of cases of Pneumocystis pneumonia identified by shotgun metagenomics approach. J Infect. 2019;78(2):158–169. doi:10.1016/j.jinf.2018.08.013
19. Branch of Organ Transplantation of Chinese Medical Association. Diagnosis and treatment guideline of invasive fungal infections in solid organ transplant recipients. Chin J Organ Transplant. 2016;37(5):300–305. (in Chinese).
20. Ma L, Huang DW, Cuomo CA, et al. Sequencing and characterization of the complete mitochondrial genomes of three Pneumocystis species provide new insights into divergence between human and rodent Pneumocystis. FASEB J. 2013;27(5):1962–1972. doi:10.1096/fj.12-224444
21. Cisse OH, Ma L, Wei Huang D, et al. Comparative population genomics analysis of the mammalian fungal pathogen Pneumocystis. mBio. 2018;9(3):e00381–18. doi:10.1128/mBio.00381-18
22. Ma L, Chen Z, Huang da W, et al. Genome analysis of three Pneumocystis species reveals adaptation mechanisms to life exclusively in mammalian hosts. Nat Commun. 2016;7(1):10740. doi:10.1038/ncomms10740
23. Coche S, Cornet G, Morelle J, Labriola L, Kanaan N, Demoulin N. Hypercalcemia associated with Pneumocystis jirovecii pneumonia in renal transplant recipients: case report and literature review. Acta Clin Belg. 2019;1–4. doi:10.1080/17843286.2019.1655233
24. Hamroun A, Lenain R, Bui Nguyen L, Chamley P, Loridant S. Hypercalcemia is common during Pneumocystis pneumonia in kidney transplant recipients. Sci Rep. 2019;9(1):12508. doi:10.1038/s41598-019-49036-w
25. Kim JE, Han A, Lee H, Ha J, Kim YS, Han SS. Impact of Pneumocystis jirovecii pneumonia on kidney transplant outcome. BMC Nephrol. 2019;20(1):212. doi:10.1186/s12882-019-1407-x
26. Pan D, Arkell P, Stone NRH, Parkinson B, Tinwell B, Cosgrove CA. Delayed strongyloides stercoralis hyperinfection syndrome in a renal transplant patient with Pneumocystis jirovecii pneumonia receiving high-dose corticosteroids. Lancet. 2019;393(10180):1536. doi:10.1016/S0140-6736(19)30708-1
27. Szydlowicz M, Jakuszko K, Szymczak A, et al. Prevalence and genotyping of Pneumocystis jirovecii in renal transplant recipients − preliminary report. Parasitol Res. 2019;118(1):181–189. doi:10.1007/s00436-018-6131-0
28. Taylor LN, Aesif SW, Matson KM. A case of Pneumocystis pneumonia, with a granulomatous response and vitamin D-mediated hypercalcemia, presenting 13 years after renal transplantation. Transpl Infect Dis. 2019;21(3):e13081. doi:10.1111/tid.13081
29. Mascia G, Argiolas D, Carta E, Michittu MB, Piredda GB. Acute kidney injury secondary to hypercalcemia in a kidney transplant patient with Pneumocystis jirovecii pneumonia: a case report. Transplant Proc. 2019;51(1):220–222. doi:10.1016/j.transproceed.2018.04.077
30. Prasad P, Lo KB, Ram P. Late presentation of Pneumocystis jirovecii pneumonia after renal transplant: a case report. Med Mycol Case Rep. 2018;20:33–34. doi:10.1016/j.mmcr.2018.01.006
31. Lee PH, Fu PK. Coinfection of Pneumocystis jiroveci pneumonia and pulmonary aspergillosis in a non-HIV-infected patient. J Microbiol Immunol Infect. 2018;51(6):860–861. doi:10.1016/j.jmii.2018.11.001
32. Kono M, Kojima K, Wakai S, Shirakawa H. A case of a Pneumocystis pneumonia twenty-four years after living kidney transplantation due to withdrawal of sulfamethoxazole/trimethoprim prophylaxis. Transplant Direct. 2018;4(6):e359. doi:10.1097/TXD.0000000000000796
33. Nieto-Rios JF, Zuluaga-Quintero M, Aristizabal-Alzate A, et al. Severe hypoxemic respiratory failure caused by Pneumocystis jirovecii in a late kidney transplant recipient. Biomedica. 2018;38(1):32–36. doi:10.7705/biomedica.v38i0.3589
34. Ling J, Anderson T, Warren S, et al. Hypercalcaemia preceding diagnosis of Pneumocystis jirovecii pneumonia in renal transplant recipients. Clin Kidney J. 2017;10(6):845–851. doi:10.1093/ckj/sfx044
35. Goto N, Takahashi-Nakazato A, Futamura K, et al. Lifelong Prophylaxis with trimethoprim-sulfamethoxazole for prevention of outbreak of pneumocystis jirovecii pneumonia in kidney transplant recipients. Transplant Direct. 2017;3(5):e151. doi:10.1097/TXD.0000000000000665
36. Brakemeier S, Durr M, Bachmann F, Schmidt D, Gaedeke J, Budde K. Risk evaluation and outcome of Pneumocystis jirovecii pneumonia in kidney transplant patients. Transplant Proc. 2016;48(9):2924–2930. doi:10.1016/j.transproceed.2016.05.017
37. Macken E, de Jonge H, Van Caesbroeck D, et al. Rhodococcus equi sepsis in a renal transplant recipient: a case study. Transplant Direct. 2015;1(3):e11. doi:10.1097/TXD.0000000000000519
38. Gits-Muselli M, Peraldi M, Castro N, et al. New short tandem repeat-based molecular typing method for Pneumocystis jirovecii reveals intrahospital transmission between patients from different wards. PLoS One. 2015;10(5):e0125763. doi:10.1371/journal.pone.0125763
39. Deborska-Materkowska D, Kozinska-Przybyl O, Mikaszewska-Sokolewicz M, Durlik M. Fatal late-onset Pneumocystis pneumonia after rituximab: administration for posttransplantation recurrence of focal segmental glomerulosclerosis – case report. Transplant Proc. 2014;46(8):2908–2911. doi:10.1016/j.transproceed.2014.09.010
40. Chandola P, Lall M, Sen S, Bharadwaj R. Outbreak of Pneumocystis jirovecii pneumonia in renal transplant recipients on prophylaxis: our observation and experience. Indian J Med Microbiol. 2014;32(3):333–336. doi:10.4103/0255-0857.136594
41. Ramalho J, Bacelar Marques ID, Aguirre AR, et al. Pneumocystis jirovecii pneumonia with an atypical granulomatous response after kidney transplantation. Transpl Infect Dis. 2014;16(2):315–319. doi:10.1111/tid.12198
42. Tu GW, Ju MJ, Xu M, et al. Combination of caspofungin and low-dose trimethoprim/sulfamethoxazole for the treatment of severe Pneumocystis jirovecii pneumonia in renal transplant recipients. Nephrology (Carlton). 2013;18(11):736–742. doi:10.1111/nep.12133
43. Borstnar S, Lindic J, Tomazic J, et al. Pneumocystis jirovecii pneumonia in renal transplant recipients: a national center experience. Transplant Proc. 2013;45(4):1614–1617. doi:10.1016/j.transproceed.2013.02.107
44. Wu YS, Lin NC, Chen IM, et al. Extracorporeal membrane oxygenation as treatment for acute respiratory failure and subsequent pneumothorax caused by Pneumocystis jirovecii pneumonia in a kidney transplant recipient. Transpl Infect Dis. 2013;15(1):E5–8. doi:10.1111/tid.12039
45. Muhammad Iqbal AH, Lim SK, Ng KP, Tan LP, Chong YB, Keng TC. Pneumocystis jirovecii pneumonia 13 years post renal transplant following a recurrent cytomegalovirus infection. Transpl Infect Dis. 2012;14(4):E23–26. doi:10.1111/j.1399-3062.2012.00738.x
46. Phipps LM, Chen SC, Kable K, et al. Nosocomial Pneumocystis jirovecii pneumonia: lessons from a cluster in kidney transplant recipients. Transplantation. 2011;92(12):1327–1334. doi:10.1097/TP.0b013e3182384b57
47. De Castro N, Xu F, Porcher R, Pavie J, Molina JM, Peraldi MN. Pneumocystis jirovecii pneumonia in renal transplant recipients occurring after discontinuation of prophylaxis: a case-control study. Clin Microbiol Infect. 2010;16(9):1375–1377. doi:10.1111/j.1469-0691.2010.03143.x
48. Camara B, Martin-Blondel G, Desloques L, et al. Pneumocystis jiroveci infection associated with organizing pneumonia in a kidney transplant patient. Rev Pneumol Clin. 2010;66(6):347–350. doi:10.1016/j.pneumo.2009.09.004
49. Gianella S, Haeberli L, Joos B, et al. Molecular evidence of interhuman transmission in an outbreak of Pneumocystis jirovecii pneumonia among renal transplant recipients. Transpl Infect Dis. 2010;12(1):1–10. doi:10.1111/j.1399-3062.2009.00447.x
50. Shelton E, Yong M, Cohney S. Late onset Pneumocystis pneumonia in patients receiving rituximab for humoral renal transplant rejection. Nephrology (Carlton). 2009;14(7):696–699. doi:10.1111/j.1440-1797.2009.01168.x
51. Yazaki H, Goto N, Uchida K, Kobayashi T, Gatanaga H, Oka S. Outbreak of Pneumocystis jiroveci pneumonia in renal transplant recipients: P. jiroveci is contagious to the susceptible host. Transplantation. 2009;88(3):380–385. doi:10.1097/TP.0b013e3181aed389
52. Arichi N, Kishikawa H, Mitsui Y, et al. Cluster outbreak of Pneumocystis pneumonia among kidney transplant patients within a single center. Transplant Proc. 2009;41(1):170–172. doi:10.1016/j.transproceed.2008.10.027
53. Kumar D, Gourishankar S, Mueller T, et al. Pneumocystis jirovecii pneumonia after rituximab therapy for antibody-mediated rejection in a renal transplant recipient. Transpl Infect Dis. 2009;11(2):167–170. doi:10.1111/j.1399-3062.2008.00345.x
54. Li JY, Yong TY, Grove DI, Coates PT. Late-onset and atypical presentation of Pneumocystis carinii pneumonia in a renal transplant recipient. Clin Exp Nephrol. 2009;13(1):92–95. doi:10.1007/s10157-008-0079-9
55. Boothpur R, Brennan DC. Didactic lessons from the serum lactate dehydrogenase posttransplant: a clinical vignette. Am J Transplant. 2008;8(4):862–865. doi:10.1111/j.1600-6143.2008.02151.x
56. Aguirre AR, Balbo BE, Ianhez LE, da Costa MC, Andrade L. Hypercalcemia and suppressed PTH levels in a renal transplant patient infected with Pneumocystis carinii. Ren Fail. 2007;29(4):513–516. doi:10.1080/08860220701275014
57. de Boer MG, Bruijnesteijn van Coppenraet LE, Gaasbeek A, et al. An outbreak of Pneumocystis jiroveci pneumonia with 1 predominant genotype among renal transplant recipients: interhuman transmission or a common environmental source? Clin Infect Dis. 2007;44(9):1143–1149. doi:10.1086/513198
58. Verma N, Soans B. Cryptogenic organizing pneumonia associated with Pneumocystis carinii infection and sirolimus therapy in a renal transplant patient. Australas Radiol. 2006;50(1):68–70. doi:10.1111/j.1440-1673.2005.01529.x
59. Hung YM. Pneumocystis carinii pneumonia with hypercalcemia and suppressed parathyroid hormone levels in a renal transplant patient. Transplantation. 2006;81(4):639. doi:10.1097/01.tp.0000185461.21901.5b
60. Totet A, Westeel PF, Nevez G. Severe Pneumocystis pneumonia in a renal transplant recipient after long term mycophenolate mofetil treatment. Rev Inst Med Trop Sao Paulo. 2005;47(5):303–304. (). doi:10.1590/S0036-46652005000500012
61. Hocker B, Wendt C, Nahimana A, Tonshoff B, Hauser PM. Molecular evidence of Pneumocystis transmission in pediatric transplant unit. Emerg Infect Dis. 2005;11(2):330–332. doi:10.3201/eid1102.040820
62. Morosi S, De Socio GV, Fiorio M, Stagni G. Late onset opportunistic infections in a renal allograft recipient: a case report. Infez Med. 2004;12(2):136–138.
63. Radisic M, Lattes R, Chapman JF, et al. Risk factors for Pneumocystis carinii pneumonia in kidney transplant recipients: a case-control study. Transpl Infect Dis. 2003;5(2):84–93. doi:10.1034/j.1399-3062.2003.00018.x
64. Chen WC, Chang SC, Wu TH, Yang WC, Tarng DC. Hypercalcemia in a renal transplant recipient suffering with Pneumocystis carinii pneumonia. Am J Kidney Dis. 2002;39(2):E8. doi:10.1053/ajkd.2002.30578
65. Lufft V, Kliem V, Behrend M, Pichlmayr R, Koch KM, Brunkhorst R. Incidence of Pneumocystis carinii pneumonia after renal transplantation. Impact of immunosuppression. Transplantation. 1996;62(3):421–423. doi:10.1097/00007890-199608150-00022
66. Hennequin C, Page B, Roux P, Legendre C, Kreis H. Outbreak of Pneumocystis carinii pneumonia in a renal transplant unit. Eur J Clin Microbiol Infect Dis. 1995;14(2):122–126. doi:10.1007/BF02111870
67. Chave JP, David S, Wauters JP, Van Melle G, Francioli P. Transmission of Pneumocystis carinii from AIDS patients to other immunosuppressed patients: a cluster of Pneumocystis carinii pneumonia in renal transplant recipients. AIDS. 1991;5(8):927–932. doi:10.1097/00002030-199108000-00002
68. Onishi A, Sugiyama D, Kogata Y, et al. Diagnostic accuracy of serum 1,3-beta-D-glucan for Pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: systematic review and meta-analysis. J Clin Microbiol. 2012;50(1):7–15. doi:10.1128/JCM.05267-11
69. Karageorgopoulos DE, Qu JM, Korbila IP, Zhu YG, Vasileiou VA, Falagas ME. Accuracy of beta-D-glucan for the diagnosis of Pneumocystis jirovecii pneumonia: a meta-analysis. Clin Microbiol Infect. 2013;19(1):39–49. doi:10.1111/j.1469-0691.2011.03760.x
70. Li WJ, Guo YL, Liu TJ, Wang K, Kong JL. Diagnosis of Pneumocystis pneumonia using serum (1-3)-beta-D-glucan: a bivariate meta-analysis and systematic review. J Thorac Dis. 2015;7(12):2214–2225. doi:10.3978/j.issn.2072-1439.2015.12.27
71. AIDS and Hepatitis C Professional Group, Society of Infectious Diseases, Chinese Medical Association, Chinese Center for Disease Control and Prevention. Chinese guidelines for diagnosis and treatment of HIV/AIDS (2018). Chin J Intern Med. 2018;57(12):867–884. (in Chinese).
72. Brakemeier S, Pfau A, Zukunft B, Budde K, Nickel P. Prophylaxis and treatment of Pneumocystis jirovecii pneumonia after solid organ transplantation. Pharmacol Res. 2018;134:61–67. doi:10.1016/j.phrs.2018.06.010
73. Branch of Organ Transplantation of Chinese Medical Association. Diagnosis and treatment guideline of invasive fungal infections in solid organ transplant recipients. Organ Transplant. 2019;10(3):227–236. (in Chinese).
74. Fishman JA, Gans H, Practice A. Pneumocystis jiroveci in solid organ transplantation: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13587. doi:10.1111/ctr.13587
75. Transplantation EEGoR. European best practice guidelines for renal transplantation. Section iv: long-term management of the transplant recipient. IV.7.1 late infections. Pneumocystis carinii pneumonia. Nephrol Dial Transplant. 2002;17(Suppl 4):36–39.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.