")
Back to Journals » Infection and Drug Resistance » Volume 15
Metagenomic Next-Generation Sequencing for Accurate Diagnosis of Acute HIV Infection with Aseptic Meningitis: A Case Report
Authors Zhou J, Fu M, Zhang D, Xu Y, Lian J, Xu H, Zhang Y, Chen H
Received 3 February 2022
Accepted for publication 12 May 2022
Published 16 May 2022 Volume 2022:15 Pages 2529—2536
DOI https://doi.org/10.2147/IDR.S361049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jing Zhou,1 Miao Fu,2 Dehe Zhang,1 Yejin Xu,1 Jiangshan Lian,3 Hanglu Xu,1 Yang Zhang,1 Haijun Chen1
1Department of Infectious Disease, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, 321000, People’s Republic of China; 2Department of Clinical Laboratory, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, 321000, People’s Republic of China; 3State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Department of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China
Correspondence: Haijun Chen, Department of Infectious Disease, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, 365 Renmin East Road, Jinhua, Zhejiang, 32100, People’s Republic of China, Email [email protected]
Background: Although individuals infected with HIV for the first time manifest a series of acute syndromes, most patients show mild or no symptoms, which complicates the initial clinical diagnosis. Early diagnosis is important for effective prevention and management of patients. Metagenomic next-generation sequencing technology (mNGS) can rapidly detect a wide range of pathogenic microorganisms, even in atypical cases. However, to date, few studies have reported the application of mNGS to diagnose acute HIV infection with aseptic meningitis.
Case Presentation: A 38-year-old man was admitted to the Department of Infectious Diseases due to repeated fever, headache, and scattered rashes on his limbs. Routine blood analysis revealed elevated absolute lymphocytes and monocytes. Moreover, monocytes were found to be significantly increased following a lumbar puncture and cerebrospinal fluid detection. mNGS results revealed the presence of the human immunodeficiency virus (HIV-1), with HIV RNA of 910 copies/mL in his cerebrospinal fluid. The HIV antigen/antibody test was negative. According to a study by Fie Big et al, a clear diagnosis of acute HIV infection at Fiebig stage I. The patient’s condition improved after treatment, and he was prescribed antiretroviral therapy (ART) after discharge.
Conclusion: Aseptic meningitis is easily misdiagnosed during the initial stages of acute HIV infection. mNGS can be used to identify the pathogen early, rapidly, and accurately, thereby improving the treatment of acute HIV infections.
Keywords: acute HIV infection, aseptic meningitis, Fiebig stage I, mNGS
Background Information
Previous studies have shown that 10% of patients with acute HIV infection may manifest neurological-related symptoms,1 among which aseptic meningitis is the most common. Clinically, acute HIV infection is characterized by symptoms such as fever, sore throat, muscle soreness, lymphadenopathy, and rashes,2 which may be easily overlooked or missed.3,4 This causes a delay between initial HIV infection and the onset of symptoms or diagnosis. To date, only a handful of studies have systematically described the manifestations of aseptic meningitis during the early stages of acute HIV infection. Herein, we report a case of acute HIV infection, with aseptic meningitis at FieBig I stage. The diagnosis was made using metagenomic next-generation sequencing (mNGS) of cerebrospinal fluid. mNGS is a high throughput and sensitive tool that employs next-generation sequencing technology to sequence all nucleic acid sequences in a specific specimen.5 Although this technology has been extensively used to diagnose various infections,6 its diagnostic value in HIV fever is largely unknown. The mNGS technology is more accurate compared with traditional pathogenic detection methods, making it ideal for clinical application.7–10 In the present case, mNGS enabled early diagnosis of acute HIV infection and meningitis.
Case Presentation
A 38-year-old man, who had no history of the disease, was admitted to the Department of Infectious Diseases due to repeated fever, headache, and scattered rashes on his limbs. The fever persisted 13 days before the hospital visit, his highest axillary temperature was 38.5℃, and this was accompanied by fatigue and headache. Routine blood examination at our hospital suggested the fever was due to infection, and he was put on ceftriaxone treatment for 1 week. However, the fever did not resolve, and scattered red rashes were seen on his limbs 7 days ago. The rashes subsided after self-administration of anti-allergic drugs. The headache worsened 1 day after the treatment, and this was accompanied by a slow response, thus he was admitted. He was healthy and had no history of bad habits such as drug abuse, having multiple sexual partners, and homosexual practice. The patient’s vital signs were as follows: 125/78 mmHg brachial artery blood pressure, 38°C axillary temperature, 84 bpm heart rate, and 22 bpm respiration rate. Additionally, the patient exhibited consciousness, slow reaction, negative neck resistance, pharyngeal hyperemia, no swelling of the tonsils, and no cardiac, pulmonary, or abdominal abnormalities. He did, however, have a few scattered rashes on his extremities, with no evidence of superficial lymph node swelling, normal muscle strength in his extremities, and negative nerve localization signs. A routine blood examination performed one day before admission, revealed a total white blood cell count of 10.89×10^9/L, a neutrophil percentage of 37.6%, a lymphocyte count of 6.22×10^9/L, as well as C-reactive protein (CRP) and Procalcitonin (PCT) levels of 0.93 mg/l and 0.13 ng/mL, respectively. Results from liver function analysis revealed an alanine aminotransferase (ALT) of 148 U/L and aspartate aminotransferase (AST) of 106 U/L. The antigen/antibody test for the human immunodeficiency virus was negative, while Chest CT showed no abnormalities.
Following hospitalization, routine blood tests revealed a total white blood cell count of 10.84×10^9/L, reduced neutrophil percentage (35.4%), an increased lymphocyte percentage (57.2%), a lymphocyte count of 6.20×10^9/L, a monocyte count of 0.69×10^9/L, a CRP of 1.54 mg/ L and PCT: 0.1 ng/ mL (Figure 1). The blood gas analysis indicated normal results, but the liver function test revealed ALT and AST levels of 92.4 and 50.3 U/L, respectively. HCMV and EBV antibody assays revealed positive and negative IgG and IgM respectively, but no HCMV or EBV DNA. A lumbar puncture revealed a cerebrospinal fluid pressure of 110 mmH2O, while results from CSF routine tests revealed negative occult-blood test, light yellow, transparent, Pan’s test 4+, nucleated cell counts of 380 /ul, neutral 1%, lymphoid 99%. Additionally, his lactate dehydrogenase increased (161 U/L), glucose levels decreased (2.0 mmol/ L), chloride level decreased (117.8 mmol/L), and his protein levels were >6000 mg/ L. Simultaneously, he had normal electrolyte and blood glucose levels, and the CSF smear test for Cryptococcus was negative. Adenosine deaminase activity in the CSF was 6.1 U/L and the electroencephalogram (EEG) was normal. Brain enhanced MRI+DWI scan showed no obvious abnormalities. Similarly, a Color Doppler ultrasound revealed no abnormalities in the lymph nodes in his neck, underarms, or both sides of the groin. Color Doppler ultrasound of the hepatobiliary, pancreas, and spleen revealed no obvious abnormalities.
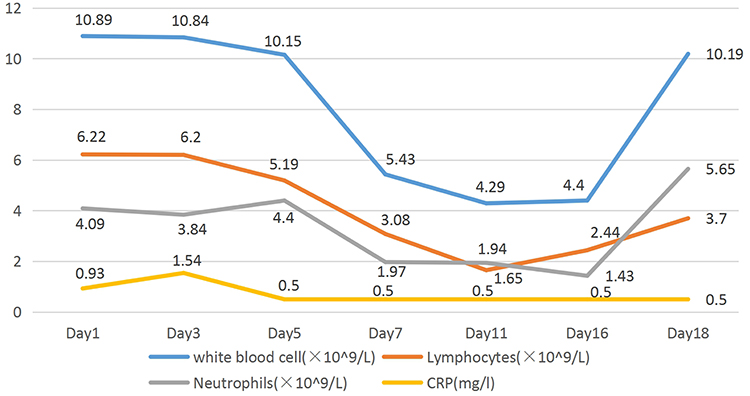 |
Figure 1 Inflammation indicators obtained in the patient during hospitalization. |
On the second day of hospitalization, we collected 3 mL of his CSF and sent it to Hangzhou Jieyi Medical Laboratory (Hangzhou, China) for metagenomic next-generation sequencing. On the 4th day, the mNGS report confirmed the presence of 12 human immunodeficiency virus type 1 (HIV-1) sequences (Figure 2), but no other pathogenic microorganisms (including bacteria, viruses, mycobacteria, fungi, and parasites, among others) were detected. On the third day, both the blood tuberculosis T cell spot test (T-SPOT. TB) and the CSF cryptococcal capsule antigen assays were negative. On the fifth day, mycobacterium tuberculosis DNA analysis from CSF revealed negative results, with no evidence of bacterial growth in either the cerebrospinal fluid or blood cultures.
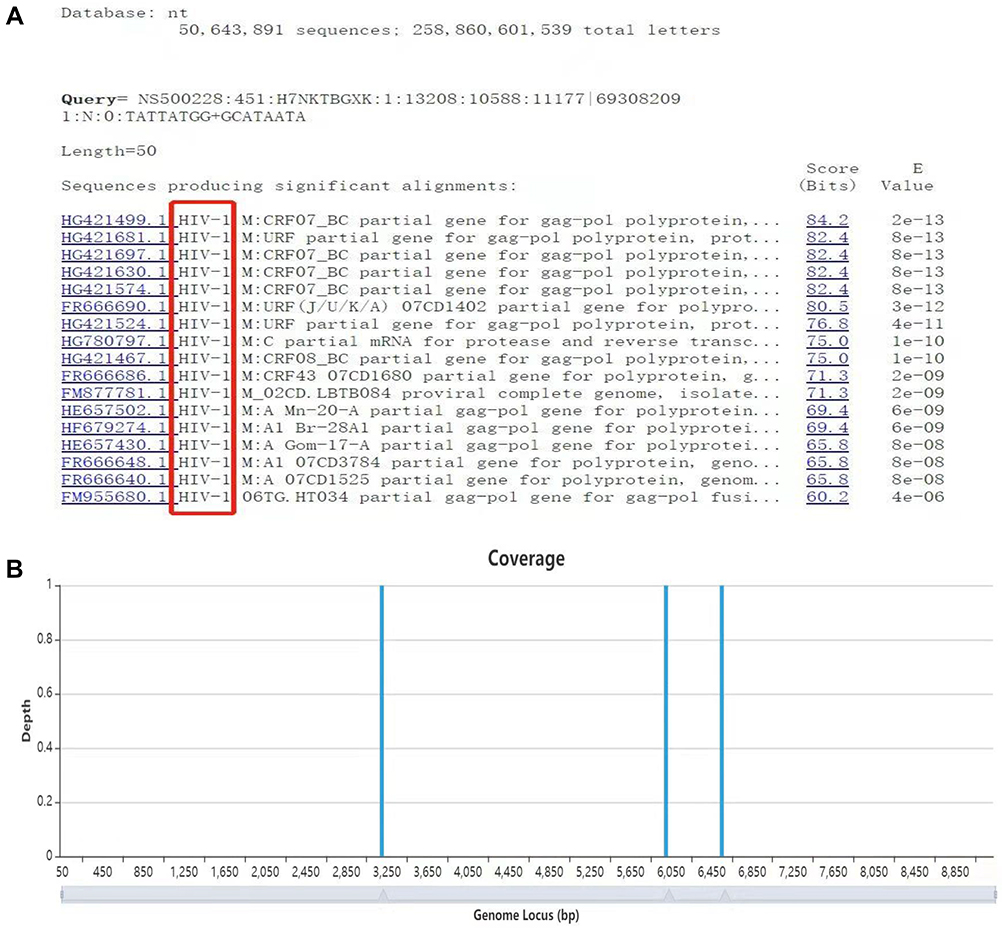 |
Figure 2 mNGS results of the patient. mNGS detected 12 HIV sequences in cerebrospinal fluid (A). The coverage and proportion of HIV detected by mNGS in cerebrospinal fluid (B). The blue ch2 and red ch1 lines denote the internal reference and specimen curve, respectively. mNGS, metagenomic next-generation sequencing. |
Lumbar puncture and cerebrospinal fluid examination were performed on the 6th, 9th, and 18th day respectively. The results indicated a progressive decrease in nucleated cell count, while sugar, chloride, and protein levels gradually returned to normal (Table 1). Additionally, CSF smears were negative for Cryptococcus. On the 6th day, 2 mL of CSF was collected and analyzed for the presence of HIV RNA qPCR 910 copies/mL, and blood HIV RNA qPCR 1.37×10^5 copies/mL (Figure 3). HIV antigen/antibody tests, performed between the 5th and 10th days, again showed negative results (the fourth generation), whereas a positive result was obtained on the 17th day. On the 18th day, a Western blot (gp120, gp160, gp41, P24) assay confirmed the presence of HIV in the blood (Table 2). On the 6th day, cell counts revealed CD4+ and CD8+ counts of 447 and 600/ul, respectively. On the 10th day, these counts had decreased, as shown by a CD4+ cell count of 293/ul, and a CD8+ cell count of 517/ul.
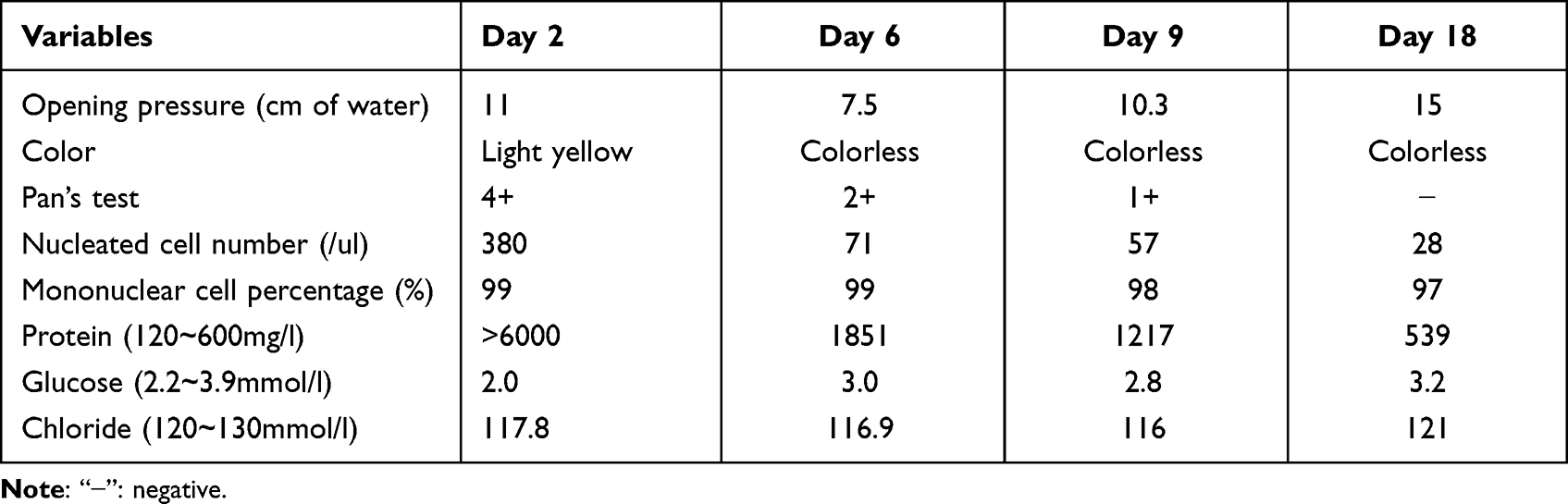 |
Table 1 Results of Cerebrospinal Fluid Examination During Hospitalization |
 |
Table 2 HIV-Related Testing |
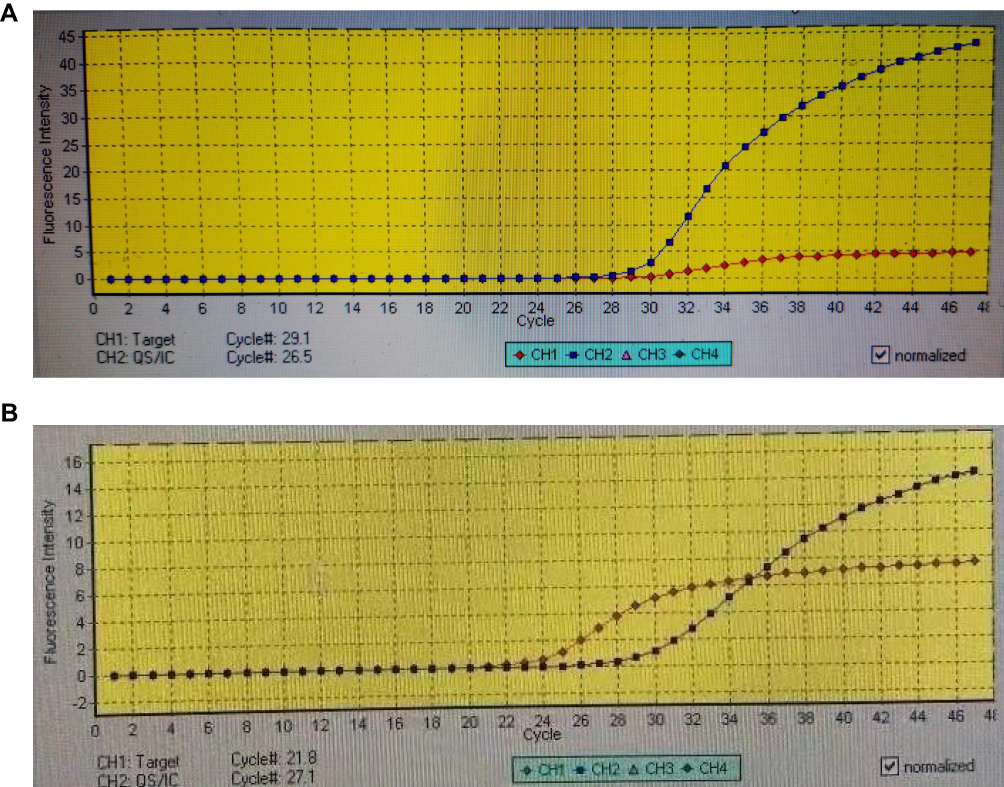 |
Figure 3 qPCR results of the patient. qPCR results in HIV in cerebrospinal fluid (A) and blood (B). qPCR, quantitative polymerase chain reaction. |
On the second day of hospitalization, tuberculous meningitis was considered based on relevant blood and CSF examination results. Consequently, the patient was administered four diagnostic anti-tuberculosis treatments: isoniazid, rifampicin, moxifloxacin, and linezolid. Additionally, he was administered an intravenous injection with an anti-inflammation dexamethasone needle and symptomatic treatment, which included compound glycyrrhizin for liver protection. On the 6th day, all anti-tuberculosis drugs and dexamethasone needles were discontinued, except for glycyrrhizin (for liver protection) and adequate fluid rehydration. On the second day of hospitalization, the patient’s body temperature gradually decreased, before returning to normal. His headache and condition improved, and he was transferred to an outpatient clinic on the 18th day for antiretroviral therapy (ART). His medical history was obtained regarding past protected same-and anal sex activities, 8 days before the onset of symptoms.
Discussion and Conclusion
Acute HIV infection (AHI) refers to the period following infection with the human immunodeficiency virus during which the body completes seroconversion before the appearance of HIV antibodies, and the HIV viral load rapidly increases to the peak level before stabilizing.11 HIV is generally diagnosed using a variety of detection techniques, including HIV RNA, HIV antigen/antibody (P24 antigen), and Western blot analysis, among others. The AHI stages, also referred to as Fiebig stages,12 are confirmed by diagnostic laboratory results. The eclipse period, which lasts approximately 10 days (range 7 to 21 days), refers to the period between virus exposure and the time when the first diagnostic test, HIV RNA PCR, detects virus presence. Fiebig stage I refers to the next stage, where HIV RNA PCR is detectable, whereas Fiebig stage II is where the p24 antigen, a transient core viral protein, becomes detectable Stages III–VI are defined by HIV-1 IgM enzyme-linked immunosorbent assay (ELISA) reactivity (stage III), HIV antibody Western blot indeterminate result (stage IV), HIV antibody Western blot positivity with a negative Western blot for a structural viral protein called p31 (stage V), and finally, antibody reactivity with a positive Western blot for p31 (stage V1).12
In this case, the patient developed symptoms associated with acute HIV infection on the 8th day after exposure, which was consistent with previous studies indicating that symptoms may manifest 1 to 6 weeks after exposure to the virus.13 We successfully detected the HIV-1 type sequence using mNGS, with viral loads of 910 and 1.37×10^5 c copies/mL in cerebrospinal fluid and blood HIV RNA, respectively. These findings unequivocally confirmed positive HIV-1 infection. Repeated detection of human immunodeficiency virus serum P24 antigen and HIV-1 antibody using two distinct HIV antigen/antibody reagents were negative, indicating that the patient had acute HIV infection at Fiebig stage I. Additionally, on the 17th day following hospitalization, HIV antigen/antibody testing revealed positive results, as did a blood Western blot test on day 18, confirming the previous diagnosis. Because there is a delayed antigen/antibody reaction in this case according to Fiebig staging, we believe that the following reasons should be considered: 1. The patient’s eclipse phase was prolonged, meaning the virus nucleic acid was detected in the blood for a longer time, up to 21 days, resulting in a prolonged antigen/antibody production time. Regrettably, this study did not perform viral nucleic acid detection during the early stages of the disease, rather, it performed nucleic acid detection after the HIV sequence was found using mNGS, hence this conclusion cannot be confirmed. 2. The sensitivity of the detection reagent is insufficient.
The majority of acute HIV symptoms and signs are non-specific, while disease development is self-limiting, both of which impede rapid HIV diagnosis. For example, Weintrob et al3 found that 83% of patients with acute HIV infections could not be diagnosed at the first visit. Additionally, HIV diagnostic tests encompass point-of-care (POC) and laboratory-based testing,14 as well as a variety of other testing methods applicable at various stages of infection. Typically, there is a delay between HIV infection and the onset of symptoms or diagnostic tests. Acute HIV infection continues to be a significant component exacerbating the epidemic, as the risk of transmission is greatest during the early stages of infection. Therefore, initiating ART at this stage can reduce the risk of transmission and the associated long-term complications.15 To date, however, only 17% of all symptomatic acute cases are accurately diagnosed, owing to this variable transmission.3 In the present case, we used the CSF mNGS detection technology to successfully detect the HIV-1 type sequence within 15 days of symptom onset, and further quantified the viral loads in both CSF and blood thereby accurately confirming the diagnosis at an early stage.
In recent years, the incidence of tuberculous meningitis (TBM) in non-AIDS-related TBM is between 2–5%, while that in AIDS patients has gradually increased to about 10%.16 Previous studies have shown that tuberculous meningitis is often misdiagnosed as viral, cryptococcal, or suppurative meningitis, among other subtypes,17 and its mortality rates remain as high as 10.0–36.5% even after receiving anti-tuberculosis drug treatment.18 In the present case, on the second day following the patient’s admission, we could not rule out tuberculous meningitis, based on symptoms and cerebrospinal fluid test results. Consequently, we administered active diagnostic anti-tuberculosis treatment to prevent disease progression. However, this was ruled out following an analysis of mNGS data from cerebrospinal fluid and other related tuberculosis DNA. On the 6th day, all anti-tuberculosis drugs were discontinued and a diagnosis of aseptic meningitis caused by acute HIV infection was considered. Previous research has demonstrated that acute HIV infections can be complicated by aseptic meningitis. For example, Hanson et al19 found that 5.3% of patients with acute HIV infection were positive for HIV RNA in their cerebrospinal fluid, findings that were clinically consistent with aseptic meningitis. Aseptic meningitis, which is typically characterized by headache and meningeal symptoms, is the most common central nervous system (CNS) manifestation of AHI and can occur within 2 weeks of infection, even before seroconversion.20 To date, the rate at which CNS reservoirs can form in AHI in humans remains unknown. Results from HIV macaque models with simian immunodeficiency virus (SIV) revealed the presence of viral RNA in the brain tissue as early as 10 days after infection.21 In the present case, mNGS detected HIV-1 RNA sequence on the 23rd day following exposure. At present, no clinical report has reported the use of this technology in the diagnosis of HIV infection in the CNS, indicating its potential utility.
The clinical presentation of aseptic meningitis in the initial phase of acute HIV infection is atypical, thus it can easily be misdiagnosed and missed, resulting in delayed patient prognosis and treatment. However, mNGS enables accurate and rapid pathogen diagnosis, which is critical for HIV management, because it aids in early detection and helps to reduce the risk of HIV transmission and long-term complications. It is expected that mNGS will be more automated, standardized, and significantly cheaper in the coming years enabling it to become a routine diagnostic and etiological analytic tool for infectious diseases.
Abbreviations
mNGS, metagenomic next-generation sequencing technology; CRP, C-reactive protein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CSF, cerebrospinal fluid; AHI, acute HIV infection; TBM, tuberculous meningitis; CNS, central nervous system; SIV, simian immunodeficiency virus.
Ethics Approval
Ethical approval for the study was granted by the ethics committee of Jinhua central hospital.
Consent to Participate
The patient voluntarily signed a written informed consent form prior to the study.
Consent for Publication
The patient in this study provided written informed consent for the publication of the clinical details and images.
Acknowledgments
We thank the patient for his participation and cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Key project of Social development of Jinhua Science and Technology Project (No. 2020-3-035).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Manji H, Miller R. The neurology of HIV infection. J Neurol Neurosurg Psychiatry. 2004;75(Suppl 1):i29–35. doi:10.1136/jnnp.2003.034348
2. Lin TY, Yang CJ, Liu CE, et al. Clinical features of acute human immunodeficiency virus infection in Taiwan: a multicenter study. J Microbiol Immunol Infect. 2019;52(5):700–709. doi:10.1016/j.jmii.2018.01.005
3. Weintrob AC, Giner J, Menezes P, et al. Infrequent diagnosis of primary human immunodeficiency virus infection: missed opportunities in acute care settings. Arch Intern Med. 2003;163(17):2097–2100. doi:10.1001/archinte.163.17.2097
4. Schacker T, Collier AC, Hughes J, et al. Clinical and epidemiologic features of primary HIV infection. Ann Intern Med. 1996;125(4):257–264. doi:10.7326/0003-4819-125-4-199608150-00001
5. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
6. Dekker JP. Metagenomics for clinical infectious disease diagnostics steps closer to reality. J Clin Microbiol. 2018;56(9):e00850–18. doi:10.1128/JCM.00850-18
7. Blauwkamp TA, Thair S, Rosen MJ, et al. Analytical and clinical validation of a microbial cell-free DNA sequencing test for infectious disease. Nat Microbiol. 2019;4(4):663–674. doi:10.1038/s41564-018-0349-6
8. Wilson MR, Naccache SN, Samayoa E, et al. Actionable diagnosis of neuroleptospirosis by next-generation sequencing. N Engl J Med. 2014;370(25):2408–2417. doi:10.1056/NEJMoa1401268
9. Fung M, Zompi S, Seng H, et al. Plasma CELL-FREE DNA next-generation sequencing to diagnose and monitor infections in allogeneic hematopoietic stem cell transplant patients. Open Forum Infect Dis. 2018;5(12):ofy301. doi:10.1093/ofid/ofy301
10. Du B, Tao Y, Ma J, et al. Identification of sparganosis based on next-generation sequencing. Infect Genet Evol. 2018;66:256–261. doi:10.1016/j.meegid.2018.10.005
11. Cohen MS, Shaw GM, McMichael AJ, et al. Acute HIV-1 Infection. N Engl J Med. 2011;364(20):1943–1954. doi:10.1056/NEJMra1011874
12. Fiebig EW, Wright DJ, Rawal BD, et al. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS. 2003;17(13):1871–1879. doi:10.1097/00002030-200309050-00005
13. Lavreys L, Thompson ML, Martin HL Jr, et al. Primary human immunodeficiency virus type 1 infection: clinical manifestations among women in Mombasa, Kenya. Clin Infect Dis. 2000;30(3):486–490. doi:10.1086/313718
14. Elliott T, Sanders EJ, Doherty M, et al. Challenges of HIV diagnosis and management in the context of pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP), test and start and acute HIV infection: a scoping review. J Int AIDS Soc. 2019;22(12):e25419. doi:10.1002/jia2.25419
15. De Salvador-Guillouët F, Sakarovitch C, Durant J, et al. Antiretroviral regimens and CD4/CD8 ratio normalization in HIV-infected patients during the initial year of treatment: a Cohort Study. PLoS One. 2015;10(10):e0140519. doi:10.1371/journal.pone.0140519
16. Rock RB, Olin M, Baker CA, et al. Central nervous system tuberculosis: pathogenesis and clinical aspects. Clin Microbiol Rev. 2008;21(2):243–61, table of contents. doi:10.1128/CMR.00042-07
17. Jain SK, Tobin DM, Tucker EW, et al. Tuberculous meningitis: a roadmap for advancing basic and translational research. Nat Immunol. 2018;19(6):521–525. doi:10.1038/s41590-018-0119-x
18. Wang YY, Xie BD. Progress on diagnosis of tuberculous meningitis. Methods Mol Biol. 2018;1754:375–386.
19. Hanson KE, Reckleff J, Hicks L, et al. Unsuspected HIV infection in patients presenting with acute meningitis. Clin Infect Dis. 2008;47(3):433–434. doi:10.1086/589931
20. Tambussi G, Gori A, Capiluppi B, et al. Neurological symptoms during primary human immunodeficiency virus (HIV) infection correlate with high levels of HIV RNA in cerebrospinal fluid. Clin Infect Dis. 2000;30(6):962–965. doi:10.1086/313810
21. Clements JE, Babas T, Mankowski JL, et al. The central nervous system as a reservoir for simian immunodeficiency virus (SIV): steady-state levels of SIV DNA in brain from acute through asymptomatic infection. J Infect Dis. 2002;186(7):905–913. doi:10.1086/343768
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.