")
Back to Journals » OncoTargets and Therapy » Volume 11
Metabolic syndrome and the incidence of hepatocellular carcinoma: a meta-analysis of cohort studies
Authors Chen Y, Li X, Wu S, Ye W, Lou L
Received 23 October 2017
Accepted for publication 10 February 2018
Published 27 September 2018 Volume 2018:11 Pages 6277—6285
DOI https://doi.org/10.2147/OTT.S154848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Yongxin Chen, Xiaofei Li, Shuang Wu, Weiwei Ye, Lianqing Lou
Department of Infectious Diseases, Yiwu Central Hospital, Yiwu, China
Background: Patients with metabolic syndrome (MetS) were suggested to have a higher risk of hepatocellular carcinoma (HCC), although the results of previous cohort studies are not consistent.
Aim: To perform an updated meta-analysis to evaluate the association between MetS and subsequent incidence of HCC.
Methods: Relevant cohort studies were identified by searching PubMed and Embase databases. Cochrane’s Q-test and I2 statistic were used to analyze the heterogeneity. Random effects model was used for the meta-analysis.
Results: Six cohort studies with 127,198 participants and 1,293 HCC cases during follow-up were included. Patients with MetS had a significantly higher incidence of HCC in studies with MetS defined by the revised National Cholesterol Education Program’s Adults Treatment Panel III (risk ratio [RR]: 1.43, 95% CI: 1.19–1.72, p<0.001; I2=29%) or International Diabetes Federation criteria (RR: 1.59, 95% CI: 1.13–2.23, p=0.008; I2=0%). Results of subgroup analysis showed that the presence of MetS was associated with a higher incidence of HCC in males (RR: 1.75, 95% CI: 1.28–2.38, p<0.001) but not in females (RR: 1.18, 95% CI: 0.76–1.84, p=0.46), and the association between MetS and higher risk of HCC was consistent regardless whether alcohol intake was adjusted. Although both were significant, MetS conferred higher risk of HCC in carriers of hepatitis B virus when compared with general population (p=0.06).
Conclusion: The presence of MetS is associated with significantly increased incidence of HCC in male participants.
Keywords: metabolic syndrome, hepatocellular carcinoma, cohort study, meta-analysis
Introduction
Although different diagnostic criteria are applied, metabolic syndrome (MetS) is defined as the presence of a cluster of disorders of metabolism, including obesity, hypertension, hyperglycemia, and dyslipidemia.1–3 Pathophysiologically, one of the key mechanisms underlying the development of MetS is insulin resistance, and a chronically activated inflammatory status has been involved in the pathogenesis of many other clinical disorders in patients with MetS.4,5 Since the prevalence of MetS is reported to be relatively high (between 10% and 30% in adult population) in both the developed and developing countries,6–8 intensive understanding of the risks of chronic diseases in these patients is important for improving the general health status in the global population. Accumulating evidence from epidemiological studies indicates that the patients with MetS are at higher risk for the development of chronic diseases, including cardiovascular diseases,9 stroke,10 osteoporosis,11 and venous thromboembolism.12 Moreover, since low-grade inflammatory response has to be involved in the pathogenesis of cancer,13 patients with MetS have been suggested to be with higher risk for the development of cancer. Indeed, patients with Mets are indicated to be of higher risks of colorectal, pancreatic, breast, endometrial, and prostate cancers as evidenced by the results of previous observational studies.14–19 However, the association between MetS and the subsequent risk of hepatocellular carcinoma (HCC) is not completely determined according to findings of previous studies.15,20 Although results of early meta-analyses of observational studies suggested that the presence of MetS may be associated with higher risk of HCC,15,20 they included both the cohort20–23 and the case–control24 studies, and therefore, a sequential relationship between the presence of MetS at baseline and subsequent incidence of HCC could not be indicated. Moreover, one15 of the previous meta-analyses included a cohort study with the outcome of HCC-related mortality25 instead of HCC incidence. Since many potential factors may influence the outcome of HCC-related mortality, such as the application of anticancer treatments, the potential association between MetS and HCC risk may be confounded. In addition, the available studies included in the previous meta-analyses are limited, which prevented the investigations regarding the potential study characteristics on the association between MetS and HCC risk. Since some recently published related cohort studies have not been included in the previous meta-analyses,26,27 we aimed to perform an updated meta-analysis to evaluate the association between MetS and subsequent incidence of HCC. Moreover, whether the association between MetS and HCC is confounded by established risk factors for HCC, including alcohol intake28 and hepatitis viruses,29 is also explored in this study.
Methods
The meta-analysis was performed in accordance with the Meta-analysis of Observational Studies in Epidemiology30 and Cochrane’s Handbook31 guidelines.
Literature searching
Databases of PubMed and Embase were searched for relevant records, using the terms “metabolic syndrome”, “insulin resistance syndrome”, or “syndrome X”, combined with “cancer”, “neoplasm”, “carcinoma”, and “hepatocellular”, “hepatic”, “intrahepatic”, “interlobular”, or “liver”, as well as “prospective”, “prospectively”, “retrospective”, “retrospectively”, “followed”, “follow-up”, “cohort”, or “cohorts”. The searching was limited to studies in humans and those published in English language. The reference lists of original and review articles were also analyzed using a manual approach. The final literature search was performed on October 22, 2017.
Study selection
Articles were included in the meta-analysis if they met all of the following criteria: 1) published as full-length article in English; 2) reported as cohort studies (prospective or retrospective, regardless of sample size) with the follow-up duration of at least 1 year; 3) included adult population (≥18 years of age) without HCC at baseline; 4) MetS defined according to the criteria of the original articles was identified as exposure of interest at baseline; 5) participants without MetS at baseline were used as controls; 6) documented the incidences of HCC during follow-up; and 7) reported the adjusted risk ratios (RRs, at least adjusted for age) and their corresponding 95% CIs for the incidence of HCC comparing individuals with MetS at baseline to those without MetS. Reviews, letters, editorials, and studies with designs other than cohort study were excluded.
Data extraction and quality evaluation
Literature searching, data extraction, and quality assessment of the included studies were performed according to the predefined inclusion criteria. Discrepancies were resolved by consensus. Data that were extracted include 1) name of first author, year of publication, and country where the study was performed; 2) design characteristics (prospective or retrospective); 3) characteristics and numbers of the participants; 4) criteria for the diagnosis of MetS; 5) follow-up period; 6) number of HCC cases in each study; and 7) variables adjusted when presenting the results. The quality of each study was evaluated using the Newcastle–Ottawa Scale (NOS),32 which ranges from 1 to 9 stars and judges each study regarding three aspects: selection of the study groups; the comparability of the groups; and the ascertainment of the outcome of interest.
Statistical analyses
We used RRs as the general measure for the association between MetS at baseline and the incidence of HCC. Data of RRs and their corresponding standard errors (SEs) were calculated from 95% CIs or p-values and were logarithmically transformed to stabilize variance and normalize the distribution.31 The Cochrane’s Q-test and I2-test were used to evaluate the heterogeneity among the included cohort studies.31,33 A significant heterogeneity was considered if I2>50%. We used a random effects model to synthesize the RR data because this model is considered as a more generalized method that incorporates the potential heterogeneity.31 Sensitivity analyses, by removing individual study one at a time, were performed to test the robustness of the results.34 Predefined subgroup analyses were performed to evaluate whether the association between MetS and HCC incidence was affected by gender of the participants, locations of the studies, study design characteristics, population characteristics, and adjustment for alcohol intake, in view of the fact that alcohol intake has been proven to be an important risk factor for HCC.28 Moreover, potential publication bias was assessed by funnel plots with the Egger regression asymmetry test.35 We used the RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and STATA software for the meta-analysis and statistics.
Results
Literature searching
The flowchart of database searching is presented in Figure 1. Briefly, 1,392 articles were found via initial literature searching of the PubMed and Embase databases, and 1,362 were excluded through screening of the titles and abstracts mainly because they were not relevant to the purpose of the meta-analysis. Subsequently, 30 potential relevant records underwent full-text review. Of these, 24 were further excluded because two of them were case–control studies, three were not with exposure of MetS, 16 reported the risks of total or other types of cancer, and the other three reported the incidence of HCC-related mortality. Finally, six cohort studies were included.20–23,26,27
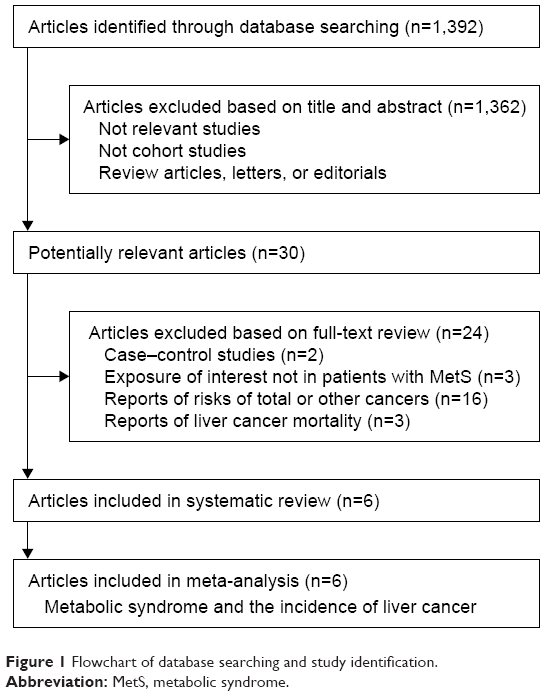 | Figure 1 Flowchart of database searching and study identification. |
Study characteristics and quality evaluation
The characteristics of the included studies are summarized in Table 1. Overall, we included six cohort studies20–23,26,27 with 127,198 participants. During follow-up, 1,293 HCC cases were reported. Briefly, four21,23,26,27 of the included cohort studies were performed in Asian countries, while the other two were performed in Western countries.20,22 As for the study design, four20–22,27 were prospective cohorts, while the other two23,26 were retrospective cohort studies. Five studies20–23,26 included general population, while the other one27 included male participants carrying hepatitis B virus (HBV). All of the included studies were adjusted for age and gender when reporting the association between MetS and HCC incidence, while other potential confounding factors such as smoking status, alcohol intake, and physical activities were adjusted in a few other studies. MetS was defined based on the criteria of revised National Cholesterol Education Program’s Adults Treatment Panel III (NCEP-ATP III) in all of the included cohorts,2 while two studies also applied the diagnostic criteria of International Diabetes Federation (IDF) for MetS.1 Gender-specific associations between MetS at baseline and incidence of HCC during follow-up were reported in all of the included cohorts. The qualities of the included studies were generally good, with the NOS varying between 7 and 9 points.
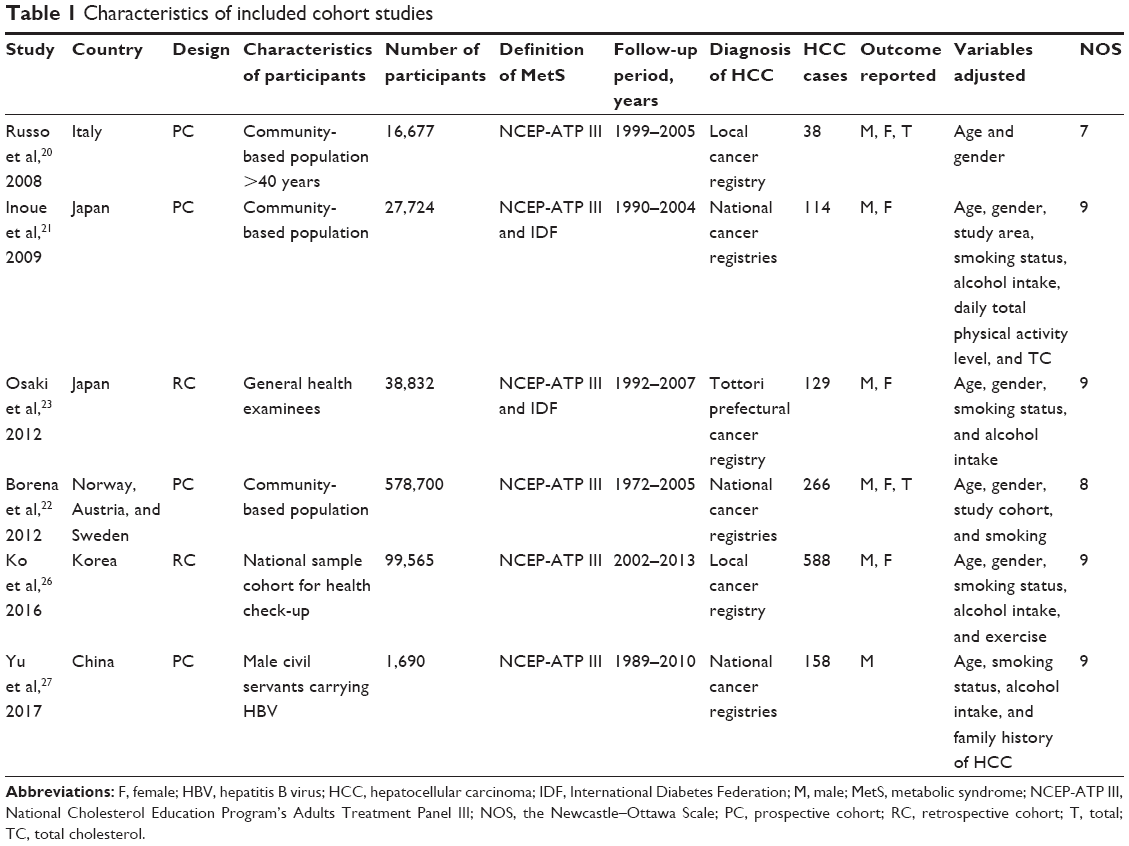 | Table 1 Characteristics of included cohort studies |
Association between the revised NCEP-ATP III-defined MetS and HCC risk
The pooled results of six cohorts consisted of nine data sets indicating that MetS defined by the revised NCEP-ATP III criteria was associated with significantly increased risk of HCC incidence (adjusted RR: 1.43, 95% CI: 1.19–1.72, p<0.001; Figure 2A) with moderate heterogeneity (p for Cochrane’s Q-test=0.19, I2=29%). Results of subgroup analysis according to the gender of the participants showed that MetS at baseline was associated with higher incidence of HCC during follow-up in men (adjusted RR: 1.75, 95% CI: 1.28–2.38, p<0.001, I2=65%; Figure 2B) but not in women (adjusted RR: 1.18, 95% CI: 0.76–1.84, p=0.46, I2=57%; Figure 2B). However, the differences between the two subgroups were not significant (p for subgroup difference=0.16). Results of subsequent subgroup analysis indicated that MetS at baseline was significantly associated with higher incidence of HCC in studies of Asian countries (adjusted RR: 1.58, 95% CI: 1.18–2.12, p=0.002), or in studies of prospective design (adjusted RR: 1.41, 95% CI: 1.15–1.72, p<0.001), but not in studies of Western countries, or in studies of retrospective design (Table 2). Moreover, we found that the association between MetS at baseline and increased risk of HCC was stronger in studies of HBV carriers (adjusted RR: 2.61, 95% CI: 1.34–5.08, p=0.005) when compared with those of general population (adjusted RR: 1.36, 95% CI: 1.16–1.58, p<0.001; p for subgroup difference=0.06; Table 2). However, the association between MetS at baseline and the increased risk of HCC was not significantly affected by whether alcohol intake was adjusted (p for subgroup difference=0.26; Table 2).
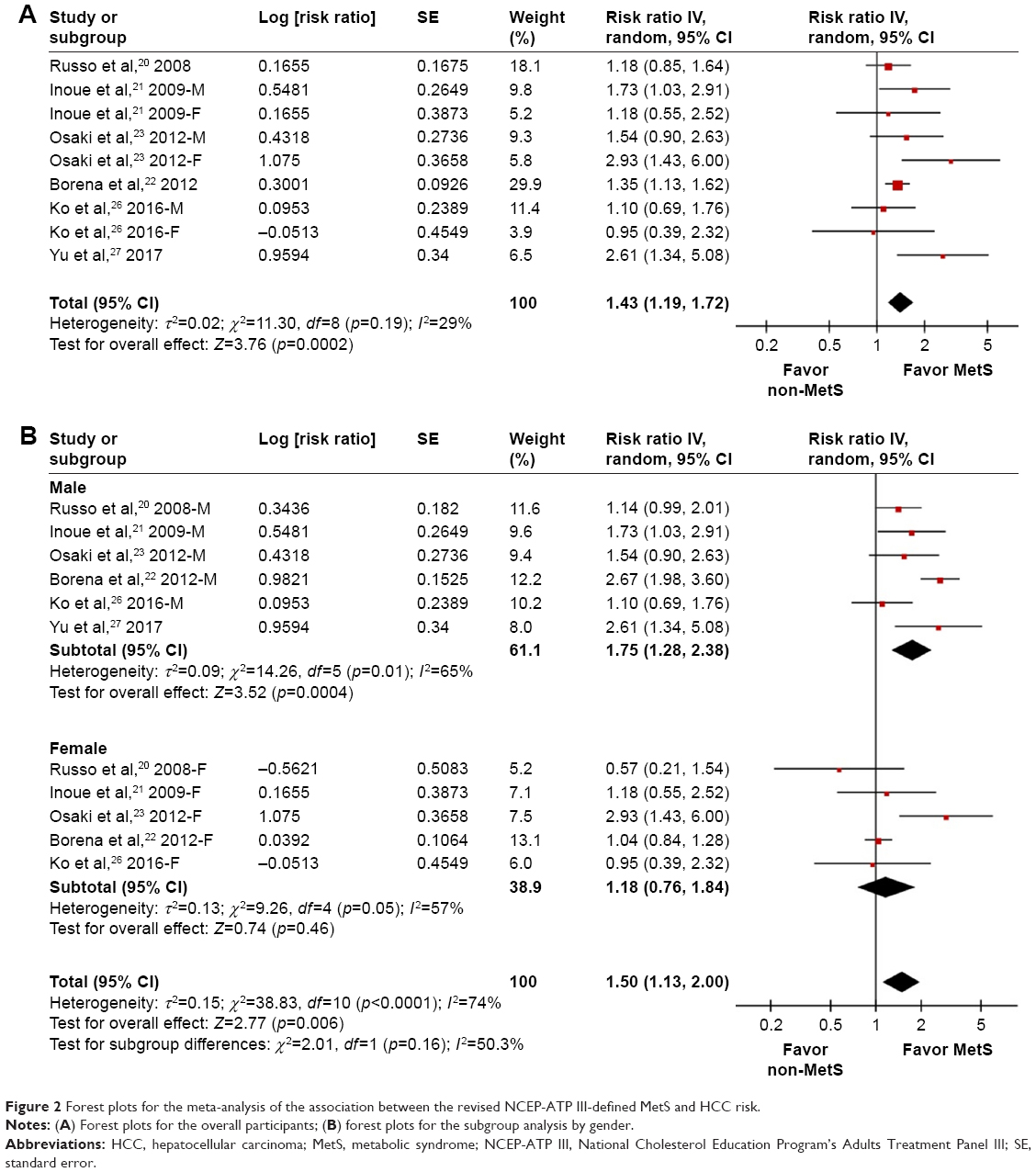 | Figure 2 Forest plots for the meta-analysis of the association between the revised NCEP-ATP III-defined MetS and HCC risk. |
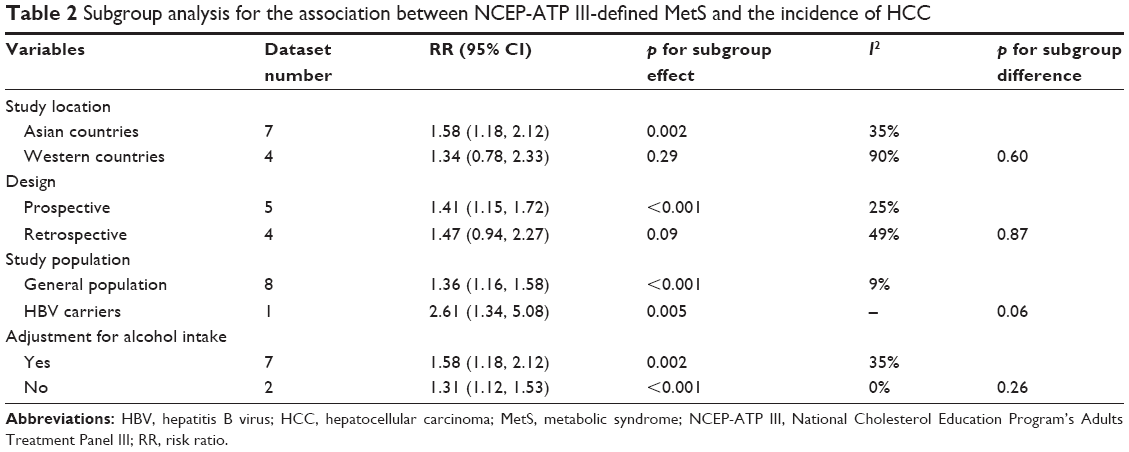 | Table 2 Subgroup analysis for the association between NCEP-ATP III-defined MetS and the incidence of HCC |
Association between IDF-defined MetS and HCC risk
Two studies21,23 reported the association between IDF-defined MetS and HCC risk. The results of pooled analysis indicated that IDF-defined MetS was associated with significantly increased risk of HCC incidence (adjusted RR: 1.59, 95% CI: 1.13–2.23, p=0.008, I2=0%; Figure 3). The association between IDF-defined MetS and the risk of HCC incidence was not significantly affected by the gender of participants (p for subgroup difference=0.96; Figure 3).
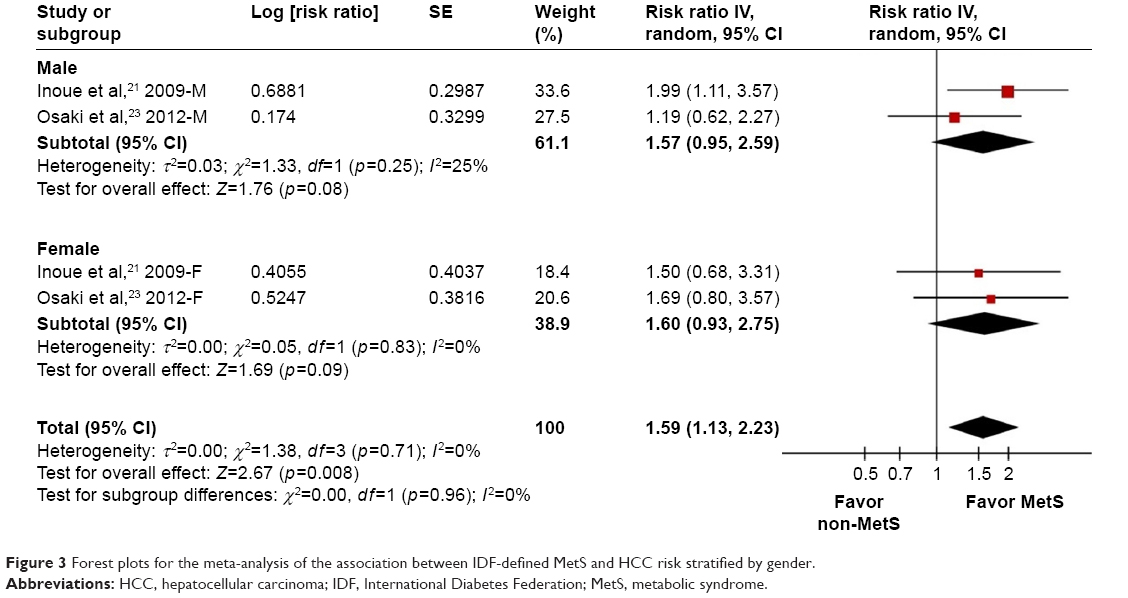 | Figure 3 Forest plots for the meta-analysis of the association between IDF-defined MetS and HCC risk stratified by gender. |
Publication bias
The funnel plots regarding MetS diagnosed by revised NCEP-ATP III or IDF criteria at baseline and risk of HCC incidence are shown in Figure 4A and B. The funnel plots are symmetric on visual inspection, suggesting low chance of significant publication bias. Results of Egger’s regression test suggested that no significant publication bias was detected for the meta-analysis of the association between MetS diagnosed by revised NCEP-ATP III and HCC risk (p=0.64). Egger’s regression test was not performed for the meta-analysis of association between IDF-defined MetS and the subsequent risk of HCC since limited cohorts were included.
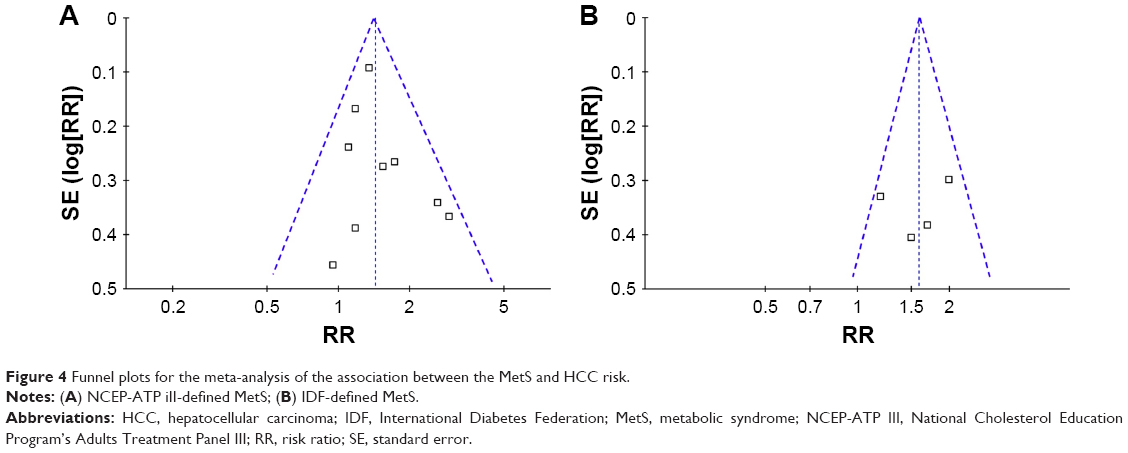 | Figure 4 Funnel plots for the meta-analysis of the association between the MetS and HCC risk. |
Discussion
In this updated meta-analysis, by pooling the results of all available cohort studies, results of our meta-analysis showed that baseline presence of MetS defined by either the revised NCEP-ATP III or the IDF criteria is associated with significantly higher risk of HCC incidence when compared with general population without MetS at baseline. Moreover, results of subsequent subgroup analysis by gender showed that MetS increased the risk of HCC incidence in male participants, but not in the females. Results of other subgroup analyses indicated that the association between MetS and higher risk of HCC was consistent in studies from Asian countries, of prospective design, and those with or without adjustment for alcohol intake when presenting the results. Importantly, although both are significant, we found that MetS confers higher risk of HCC incidence in HBV carriers when compared with the general population. These results suggested that participants with MetS are at higher risk for the development of HCC, particularly in male participants and in those of HBV carriers.
Our meta-analysis has the following strengths when compared with the previous ones.15,36 First, we included cohort studies only. Therefore, a sequential association between baseline presence of MetS and the incidence of HCC could be confirmed. Second, cohort studies with HCC-related mortality as the primary outcome were excluded. Therefore, the potential confounding effects of mortality-related factors such as the anticancer treatment could be avoided. Third, we evaluated the associations between MetS defined by two different criteria and the risk of HCC incidence, and the consistent results indicated the robustness of our findings. Lastly, two recently published cohort studies were included, which enables us to perform the subgroup analysis to explore the influences of study or patient characteristics on the association between MetS and HCC incidence.
Overall, the results of our study indicated that the presence of MetS is associated with significantly increased risk of HCC incidence compared with those without MetS. These results suggest that intensified prevention of HCC in patients may be needed. The potential association between MetS and HCC risk may be explained by the findings that some components of MetS may have a close relationship with HCC risk. Indeed, a recently published meta-analysis showed that premorbid obesity may be independently associated with a twofold risk of HCC-related mortality.37 Moreover, patients with type 2 diabetes mellitus (T2DM) are also found to be at higher risk for development of HCC,38 and some medications against T2DM, such as metformin,39 may be preventative against HCC. Although the association between dyslipidemia and HCC risk was not fully understood, the classic cholesterol-lowering medication statins were found to be preventative of HCC development.40 As for the potential mechanisms underlying the association between MetS and the increased risk of HCC development, further researches are needed because the exact mechanisms remain to be determined. The low-grade inflammatory response may be responsible for the carcinogenesis in patients with MetS.13 Moreover, with the presence of MetS in the liver, occurrence of nonalcoholic fatty liver disease may also expose the patients to increased risk of HCC.41,42 Besides, as a key pathophysiological mechanism of MetS, insulin resistance has also been suggested to be an important risk factor of HCC pathogenesis.43,44 Further studies are needed to clarify the dominant mechanisms.
Results of subgroup analysis suggested that MetS may increase the risk of HCC in men but not in women. This is consistent with the findings of some previous studies which indicated that components of MetS may confer higher risk of HCC in male participants than in females. For example, results of a previous meta-analysis showed that the association between obesity and HCC risk was more pronounced in men than in women.45 However, the underlying mechanisms remain unclear. Furthermore, we found that the association between MetS and increased risk of HCC remains significant in studies with alcohol intake adjusted and more pronounced in carriers of HBV. These results suggest that MetS also increased the risk of HCC in high-risk patients including HBV carriers. Again, these results highlight the importance of intensified HCC prevention in MetS, particularly in high-risk patients, such as the HBV carriers.
Besides above strengths and implications, our meta-analysis has limitations that should be considered when interpreting the results. First, the number of the included cohort studies was relatively small. Therefore, results of subgroup analyses should be interpreted with caution, and large-scale cohort studies are needed to confirm these findings. Second, although most-adequately adjusted results were pooled, we could not exclude other factors, such as the treatment against the components of MetS, which may confound the association between MetS and increased risk of HCC. Third, as inherited in meta-analysis of observational studies, results of our study could only support a sequential association between MetS at baseline and increased risk of HCC incidence subsequently. A causative relationship between MetS and HCC pathogenesis could not be indicated by our findings. Fourth, although MetS defined by revised NCEP-ATP III or IDF criteria was associated with higher HCC incidence, association between MetS defined by other criteria and subsequent HCC incidence remains undetermined. Fifth, studies in our meta-analysis mostly included general population, of which the prevalence of cirrhosis was not reported. Moreover, the prevalence of cirrhosis at baseline for participants with and without MetS was not adjusted when reporting the association between MetS and risk of HCC. Since cirrhosis is one of the primary risk factors for the development of HCC, we were unable to determine if the prevalence of cirrhosis may confound the association between MetS and HCC. Finally, the prevalence of hepatitis B and C of the participants was not reported in most of our included studies, and these factors were not adjusted when reporting the results. The potential higher prevalence of hepatitis B and C in Asian participants when compared with the participants from Western countries may at least partially be the reason that MetS and increased risk of HCC were significant in studies from Asian countries but not in Western countries. These hypotheses should be evaluated in future studies.
Conclusion
Results of our meta-analysis showed that the presence of MetS is significantly associated with increased risk of HCC incidence when compared with those without MetS at baseline. Intensified HCC prevention in MetS patients, particularly in high-risk patients such as the HBV carriers, may be clinically important.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Alberti KG, Zimmet P, Shaw J. Metabolic syndrome–a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23(5):469–480. | ||
Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227–239. | ||
Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428. | ||
Gluvic Z, Zaric B, Resanovic I, et al. Link between metabolic syndrome and insulin resistance. Curr Vasc Pharmacol. 2017;15(1):30–39. | ||
Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28(4):629–636. | ||
He YN, Zhao WH, Zhao LY, et al. Prevalence of metabolic syndrome in Chinese adults in 2010–2012. Zhonghua Liu Xing Bing Xue Za Zhi. 2017;38(2):212–215. | ||
Li R, Li W, Lun Z, et al. Prevalence of metabolic syndrome in Mainland China: a meta-analysis of published studies. BMC Public Health. 2016;16:296. | ||
Yamagishi K, Iso H. The criteria for metabolic syndrome and the national health screening and education system in Japan. Epidemiol Health. 2017;39:e2017003. | ||
Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56(14):1113–1132. | ||
Li X, Lin H, Fu X, et al. Metabolic syndrome and stroke: a meta-analysis of prospective cohort studies. J Clin Neurosci. 2017;40:34–38. | ||
Zhou J, Zhang Q, Yuan X, et al. Association between metabolic syndrome and osteoporosis: a meta-analysis. Bone. 2013;57(1):30–35. | ||
Ageno W, Di Minno MN, Ay C, et al. Association between the metabolic syndrome, its individual components, and unprovoked venous thromboembolism: results of a patient-level meta-analysis. Arterioscler Thromb Vasc Biol. 2014;34(11):2478–2485. | ||
Fernandes JV, Cobucci RN, Jatoba CA, Fernandes TA, de Azevedo JW, de Araujo JM. The role of the mediators of inflammation in cancer development. Pathol Oncol Res. 2015;21(3):527–534. | ||
Rosato V, Tavani A, Bosetti C, et al. Metabolic syndrome and pancreatic cancer risk: a case-control study in Italy and meta-analysis. Metabolism. 2011;60(10):1372–1378. | ||
Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. 2012;35(11):2402–2411. | ||
Esposito K, Chiodini P, Capuano A, et al. Colorectal cancer association with metabolic syndrome and its components: a systematic review with meta-analysis. Endocrine. 2013;44(3):634–647. | ||
Bhandari R, Kelley GA, Hartley TA, Rockett IR. Metabolic syndrome is associated with increased breast cancer risk: a systematic review with meta-analysis. Int J Breast Cancer. 2014;2014:189384. | ||
Esposito K, Chiodini P, Capuano A, Bellastella G, Maiorino MI, Giugliano D. Metabolic syndrome and endometrial cancer: a meta-analysis. Endocrine. 2014;45(1):28–36. | ||
Gacci M, Russo GI, De Nunzio C, et al. Meta-analysis of metabolic syndrome and prostate cancer. Prostate Cancer Prostatic Dis. 2017;20(2):146–155. | ||
Russo A, Autelitano M, Bisanti L. Metabolic syndrome and cancer risk. Eur J Cancer. 2008;44(2):293–297. | ||
Inoue M, Noda M, Kurahashi N, et al. Impact of metabolic factors on subsequent cancer risk: results from a large-scale population-based cohort study in Japan. Eur J Cancer Prev. 2009;18(3):240–247. | ||
Borena W, Strohmaier S, Lukanova A, et al. Metabolic risk factors and primary liver cancer in a prospective study of 578,700 adults. Int J Cancer. 2012;131(1):193–200. | ||
Osaki Y, Taniguchi S, Tahara A, Okamoto M, Kishimoto T. Metabolic syndrome and incidence of liver and breast cancers in Japan. Cancer Epidemiol. 2012;36(2):141–147. | ||
Welzel TM, Graubard BI, Zeuzem S, El-Serag HB, Davila JA, McGlynn KA. Metabolic syndrome increases the risk of primary liver cancer in the United States: a study in the SEER-Medicare database. Hepatology. 2011;54(2):463–471. | ||
Matthews CE, Sui X, LaMonte MJ, Adams SA, Hebert JR, Blair SN. Metabolic syndrome and risk of death from cancers of the digestive system. Metabolism. 2010;59(8):1231–1239. | ||
Ko S, Yoon SJ, Kim D, Kim AR, Kim EJ, Seo HY. Metabolic risk profile and cancer in Korean men and women. J Prev Med Public Health. 2016;49(3):143–152. | ||
Yu MW, Lin CL, Liu CJ, Yang SH, Tseng YL, Wu CF. Influence of metabolic risk factors on risk of hepatocellular carcinoma and liver-related death in men with chronic hepatitis B: a large cohort study. Gastroenterology. 2017;153(4):1006.e5–1017.e5. | ||
Chuang SC, Lee YC, Wu GJ, Straif K, Hashibe M. Alcohol consumption and liver cancer risk: a meta-analysis. Cancer Causes Control. 2015;26(9):1205–1231. | ||
Raffetti E, Fattovich G, Donato F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: a systematic review and meta-analysis. Liver Int. 2016;36(9):1239–1251. | ||
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012. | ||
Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0) [homepage on the Internet]. The Cochrane Collaboration 2011. Available from: http://www.cochranehandbook.org. Accessed October 1, 2017. | ||
Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2010 [webpage on the Internet]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed October 1, 2017. | ||
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. | ||
Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol. 2008;37(5):1148–1157. | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. | ||
Jinjuvadia R, Patel S, Liangpunsakul S. The association between metabolic syndrome and hepatocellular carcinoma: systemic review and meta-analysis. J Clin Gastroenterol. 2014;48(2):172–177. | ||
Xue K, Li FF, Chen YW, Zhou YH, He J. Body mass index and the risk of cancer in women compared with men: a meta-analysis of prospective cohort studies. Eur J Cancer Prev. 2017;26(1):94–105. | ||
Mantovani A, Targher G. Type 2 diabetes mellitus and risk of hepatocellular carcinoma: spotlight on nonalcoholic fatty liver disease. Ann Transl Med. 2017;5(13):270. | ||
Ma S, Zheng Y, Xiao Y, Zhou P, Tan H. Meta-analysis of studies using metformin as a reducer for liver cancer risk in diabetic patients. Medicine (Baltimore). 2017;96(19):e6888. | ||
Pradelli D, Soranna D, Scotti L, et al. Statins and primary liver cancer: a meta-analysis of observational studies. Eur J Cancer Prev. 2013;22(3):229–234. | ||
Argyrou C, Moris D, Vernadakis S. Hepatocellular carcinoma development in non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Is it going to be the “Plague” of the 21st century? A literature review focusing on pathogenesis, prevention and treatment. J BUON. 2017;22(1):6–20. | ||
Shetty K, Chen J, Shin JH, Jogunoori W, Mishra L. Pathogenesis of hepatocellular carcinoma development in non alcoholic fatty liver disease. Curr Hepatol Rep. 2015;14(2):119–127. | ||
Kim JH, Sinn DH, Gwak GY, et al. Insulin resistance and the risk of hepatocellular carcinoma in chronic hepatitis B patients. J Gastroenterol Hepatol. 2017;32(5):1100–1106. | ||
Montesi L, Mazzotti A, Moscatiello S, Forlani G, Marchesini G. Insulin resistance: mechanism and implications for carcinogenesis and hepatocellular carcinoma in NASH. Hepatol Int. 2013;7(Suppl 2):814–822. | ||
Gupta A, Das A, Majumder K, et al. Obesity is independently associated with increased risk of hepatocellular cancer-related mortality: a systematic review and meta-analysis. Am J Clin Oncol. Epub 2017 May 23. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.