")
Back to Journals » OncoTargets and Therapy » Volume 9
Meta-analysis of outcomes of patients with stage IV colorectal cancer managed with chemotherapy/radiochemotherapy with and without primary tumor resection
Authors Lee KC, Ou YC, Hu WH, Liu CC, Chen HH
Received 17 May 2016
Accepted for publication 16 October 2016
Published 15 November 2016 Volume 2016:9 Pages 7059—7069
DOI https://doi.org/10.2147/OTT.S112965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Ko-Chao Lee,1 Yu-Che Ou,2 Wan-Hsiang Hu,1 Chia-Cheng Liu,3 Hong-Hwa Chen1
1Division of Colorectal Surgery, Department of Surgery, 2Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital, Kaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, 3Department of Surgery, Pingtung Christian Hospital, Pingtung, Taiwan
Background: Colorectal cancer is the third leading cause of death worldwide. Currently, novel chemotherapeutic agents are first-line therapy for unresectable stage IV colorectal cancer, while benefits of noncurative primary tumor resection in advanced disease remain debatable.
Objective: This meta-analysis evaluated outcomes of patients with unresectable stage IV colorectal cancer receiving systemic chemotherapy with or without primary tumor resection.
Materials and methods: A database search of PubMed and Cochrane Library databases identified 167 studies that were screened for relevance. After 119 were excluded, 48 were assessed for eligibility and 26 were included for meta-analysis, including 24 retrospective studies, one prospective study, and one randomized, controlled trial. Extracted data included patient demographics (age, sex), clinical data (tumor stage, metastasis), targeted therapy agents, and surgical data (with/without tumor resection). Patients’ overall and progression-free survival was compared between groups with/without primary tumor resection.
Results: The 26 studies included 43,903 patients with colorectal cancer, with 29,639 receiving chemotherapy/radiotherapy plus primary tumor resection, and 14,264 managed medically with chemotherapy/chemoradiotherapy alone without primary tumor resection. Patients receiving primary tumor resection plus chemotherapy/radiotherapy had longer overall survival (hazard ratio [HR 0.59], 95% confidence interval [CI] 0.51–0.68; P<0.001), with significant differences in overall survival between patients with and without primary tumor resection (HR 0.58, 95% CI 0.49–0.68; P<0.001). Longer overall survival was also found among patients receiving primary tumor resection who were treated with bevacizumab/cetuximab targeted therapy agents (HR 0.63, 95% CI 0.46–0.86; P=0.003). Patients from three studies who received primary tumor resection had longer progression-free survival (HR 0.73, 95% CI 0.58–0.91; P=0.005). Results are limited by retrospective data, inconsistent complications data, and publication bias.
Conclusion: Study results support primary tumor resection in stage IV colorectal cancer, but significant biases in studies suggest that randomized trials are warranted to confirm findings.
Keywords: chemotherapy, colorectal cancer, outcomes, tumor resection
Introduction
New cases of colorectal cancer (CRC) worldwide totaled 14.1 million in 2012, with 8.2 million deaths, making CRC the third leading cause of death worldwide after lung and liver cancers.1 In the US, ~134,490 adults will be diagnosed with CRC in 2016 (95,270 colon, 39,220 rectal), and ~49,190 will die from the disease.2 Many such CRC-related deaths can be prevented through early detection of precancerous polyps in the colon and rectum, identified during regular screening according to guidelines of the American Cancer Society. However, in 2010, only 59% of US adults aged ≥50 years actually reported undergoing CRC screening.3 Nevertheless, the death rate per 100,000 individuals per year has been dropping over the last two decades, due to overall increased screening and advances in treatment as well.4 As a result, >1 million survivors are now living in the US.
The traditional approach to managing incurable stage IV CRC has been surgical resection of the primary tumor or stoma. However, this has changed significantly during the last three decades, favoring a multidisciplinary approach that relies heavily on chemotherapy using novel third-generation targeted therapy agents in combination with second-generation agents.5,6 This change has led to a dramatic increase in the median overall survival (OS) of CRC patients from 6 months to ~2 years,7 while surgical resection of the primary tumor in these patients remains controversial.8–11 A systematic review concluded that resection of the primary tumor in asymptomatic patients with unresectable stage IV CRC who are managed with chemotherapy/radiotherapy was not either associated with prolonged OS or reduced the risk of complications.12 Ahmed et al asked appropriately if noncurative resection of the primary tumor was advisable in treating stage IV CRC, finding that some of the previous studies did support noncurative resection in advanced CRC.11 A systematic review indicated that primary tumor resection prognostic factors were found to be significantly associated with OS after multivariate analysis.13 Tumor-related complication rates remained as high as 29.7% in resected cases compared to 27.6% in the nonresection population.11 Even with the combined application of primary tumor resection and systemic chemotherapy, only 10%–15% of patients survive for 5 years.11 Therefore, when resection is being considered, the potential morbidity and effects on quality of life must be determined case by case.
The controversy continues among surgeons in oncology about the relative benefits of resection of primary tumors versus chemotherapy alone, and available data are insufficient to reach consensus. Therefore, this meta-analysis was conducted to evaluate outcomes of patients with unresectable stage IV CRC receiving either systemic chemotherapy alone or combined therapy of primary tumor resection and systemic chemotherapy.
Materials and methods
Search strategy
The PubMed and the Cochrane Library databases were searched until February 2015 for relevant studies using prespecified eligibility criteria. Only human-subject studies published from 1997 to 2015 were included. The search terms included two combinations: combination 1 (advanced OR stage IV) AND (colorectal cancer) AND (non-resection OR resection) AND (chemotherapy); and combination 2 (colorectal cancer) AND (unresectable OR stage IV) AND chemotherapy; with the search filter: clinical trial, abstract, title-abstract.
Study selection
Titles and abstracts were screened for all studies, and full text was obtained for those meeting the inclusion criteria. Inclusion criteria were: comparative study, majority of patients with stage IV CRC, chemotherapy/radiochemotherapy plus primary tumor resection as one intervention and chemotherapy/radiochemotherapy alone as the other. Chemotherapy included both targeted therapy agents and second-generation agents. Single-arm studies and studies in which nonresection patients did not receive chemotherapy/radiochemotherapy were excluded. Case series, letters, comments, editorials, case reports, proceedings, personal communications, and reviews were also excluded, as well as non-English and non-Chinese studies. Finally, 26 studies were determined eligible for meta-analysis.14–39
Primary outcome measures for the studies included were patient outcomes, including OS and free survival (PFS). Two author–reviewers determined the eligibility of all retrieved studies independently, and discrepancies were resolved through consultation with a third reviewer.
Data extraction
Two independent reviewers extracted all data from eligible studies. Extracted data included first author’s name, year of publication, study design, interventions, participants and participants’ demographics (age, sex), clinical data (tumor stage, metastasis), targeted therapy agents, surgical data (with/without primary resection), and survival (OS and PFS).
Quality assessment
The methodological aspects of nonrandomized studies were assessed using the Newcastle–Ottawa Scale (NOS).40 This scale comprises eight items categorized into three dimensions: selection, comparability, and exposure. A star system is used for a semiquantitative assessment of study quality, awarding the highest-quality studies a maximum of one star for each item with the exception of the item related to comparability, which allows assignment of two stars. NOS scores range between zero and nine stars.
Statistical analysis
The primary outcome for this meta-analysis was the hazard ratio (HR) for OS, and the secondary outcome was HR for PFS. Crude or adjusted HRs with 95% confidence interval (CI) were extracted for survival outcomes for each individual study. If available data were presented from the Kaplan–Meier curve, the survival rates at specified times were extracted to reconstruct the HR estimate and its variance, assuming that the rate of patients censored was constant during study follow-up, as described previously.41 An HR <1 indicated that primary tumor-resection patients were favored. A χ2-based test of homogeneity was performed, and the inconsistency index (I2) and Q-statistics were determined. If the I2-statistic were >50%, a random-effect model was used. Otherwise, fixed-effect models were employed. Pooled effects were calculated, and a two-sided P-value <0.05 was established as statistical significance. Subgroup analysis was also performed to evaluate differences between patients receiving and not receiving targeted therapy agents (bevacizumab/cetuximab). Sensitivity analysis was carried out using the leave-one-out approach. Publication bias was assessed by constructing funnel plots, with the absence of publication bias indicated by data points forming a symmetric funnel-shaped distribution and one-tailed significance level of P>0.05 (Egger’s test). If publication bias was found, adjusted-effect sizes were calculated using Duval and Tweedie’s “trim and fill” procedure.42 However, a funnel plot is only used if the meta-analysis includes more than ten studies.43 All analyses were performed using Comprehensive Meta-Analysis statistical software, version 2.0 (Biostat, Englewood, NJ, USA).
Results
Literature search
Figure 1 summarizes the literature search procedure. A total of 167 studies were identified with the database search and screened for relevance. After 119 were excluded based on the aforementioned criteria, 48 were assessed for eligibility and 26 were finally determined eligible for inclusion in meta-analysis, including 24 retrospective studies, one prospective study, and one randomized controlled trial14–39 (Figure 1).
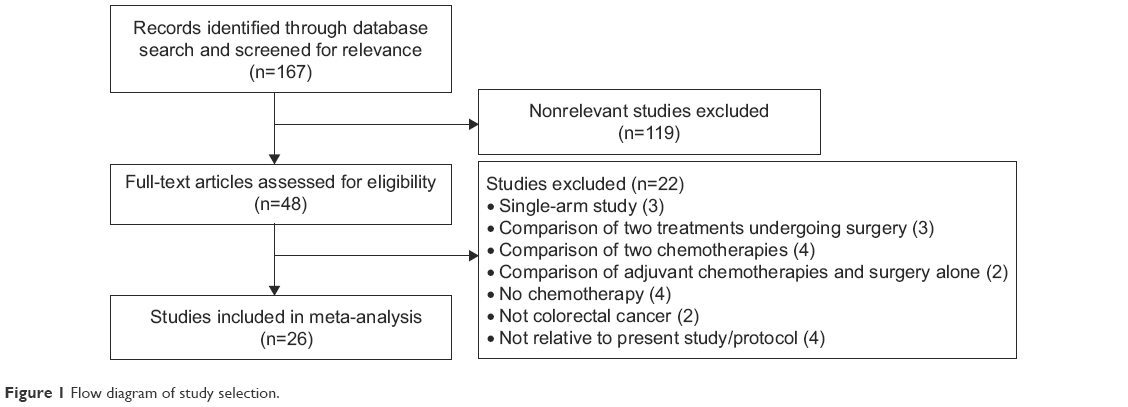 | Figure 1 Flow diagram of study selection. |
Characteristics of included studies
Table 1 summarizes characteristics of the 26 studies included. All included studies were nonrandomized clinical studies, except for Ferrand et al.37 The 26 studies included a total of 43,903 patients with CRC, among whom 29,639 were treated with chemotherapy/radiotherapy plus primary tumor resection (primary tumor resection group) and 14,264 were first managed medically with chemotherapy/chemoradiotherapy alone (without primary tumor resection group). Patients’ ages were fairly similar between studies, ranging from 49 to 73 years. Sex distribution varied between studies, and the proportion of male patients ranged from 33% to 78% (Table 1).
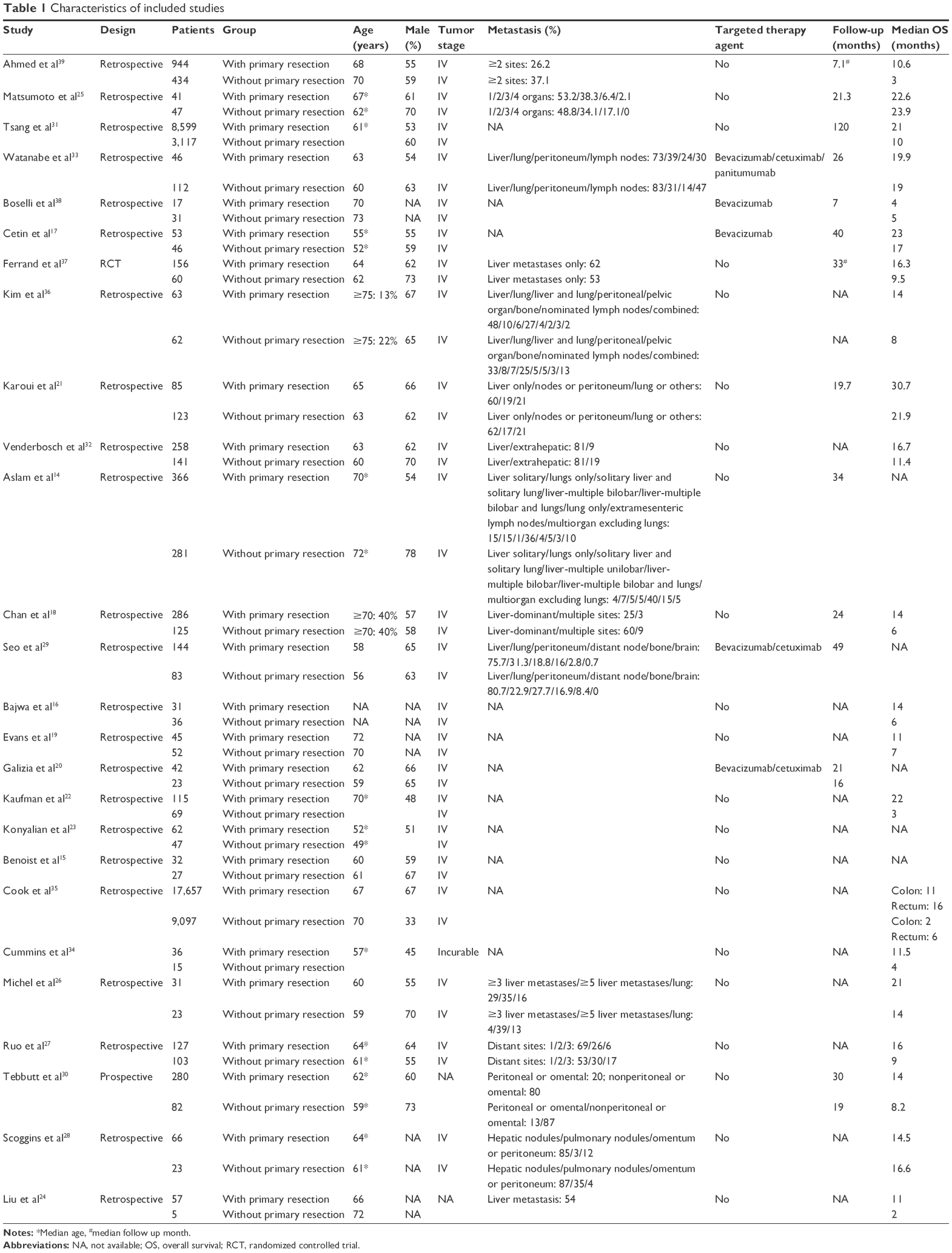 | Table 1 Characteristics of included studies |
Meta-analysis: overall survival and PFS
Median OS ranged from 4 months to 30.7 months in patients receiving primary tumor resection and 2–23.9 months in patients without primary tumor resection. Four studies, including Kim et al,36 Cook et al,35 Ruo et al,27 and Liu et al,24 did not provide enough information to estimate HRs for OS; hence, HRs of the 22 evaluable studies were calculated by the method reported in the “Statistical analysis” section. Heterogeneity was observed among the 22 studies; therefore, a random-effect model was used (Q=167.868, I2=87.49%). Overall analysis revealed that patients treated with primary tumor resection in addition to chemotherapy/radiotherapy were associated with longer OS (HR 0.59, 95% CI 0.51–0.68; P<0.001) (Figure 2A).
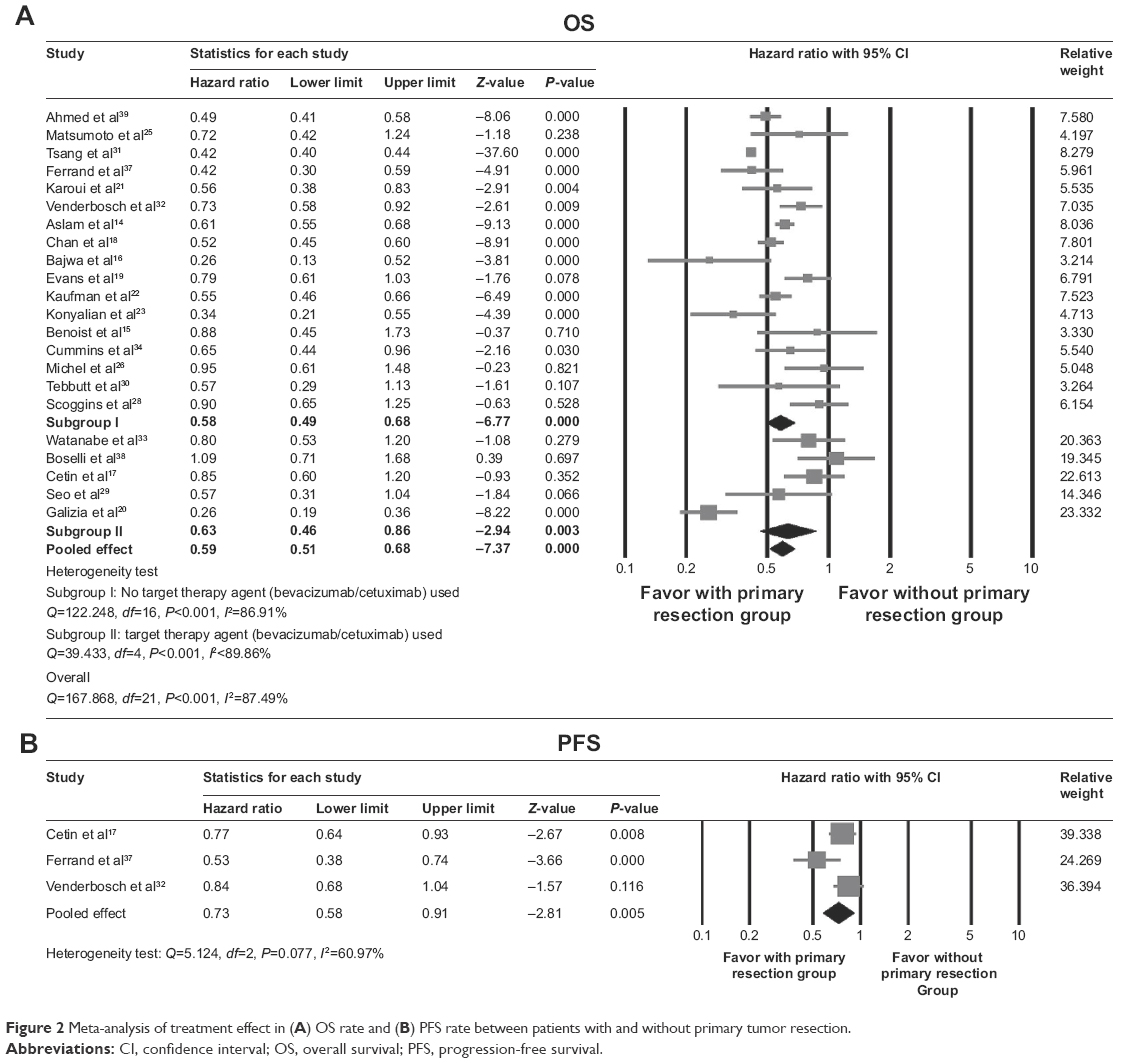 | Figure 2 Meta-analysis of treatment effect in (A) OS rate and (B) PFS rate between patients with and without primary tumor resection. |
A random-effect model was used for analysis of the subgroup of studies (n=17) that recruited patients receiving second-generation agents without targeted therapy agents (bevacizumab/cetuximab) (Q=122.248, I2=86.91%). Results showed significant differences in OS between patients with and without primary tumor resection (HR 0.58, 95% CI 0.49–0.68; P<0.001). In addition, a random-effect model was also used for analysis of the subgroup of studies (n=5) that also recruited patients receiving targeted therapy agents (bevacizumab/cetuximab) (Q=39.433, I2=89.86%). Results indicated that among patients receiving primary tumor resection, longer OS was also found among those receiving bevacizumab/cetuximab targeted therapy agents (HR 0.63, 95% CI 0.46–0.86; P=0.003).
Only three studies17,32,37 provided enough information to estimate HRs for PFS. Heterogeneity was observed among the three studies, and thus a random-effect model was used (Q=5.124, I2=60.97%). Overall analysis revealed that patients who received primary tumor resection were associated with longer PFS (HR 0.73, 95% CI 0.58–0.91; P=0.005) (Figure 2B).
Sensitivity analysis
Sensitivity analyses were performed using the leave-one-out approach, in which meta-analysis of OS and PFS was performed with each study removed in turn (Table 2). The direction and magnitude of combined estimates of OS did not vary markedly after removing the studies, indicating good reliability of the meta-analysis and that data were not overly influenced by any study. However, for PFS, sensitivity analysis indicated that pooled estimates might have been affected by one study.17 After that study had been removed, no significant differences were found in PFS between patients with primary tumor resection and those without primary tumor resection (Table 2).
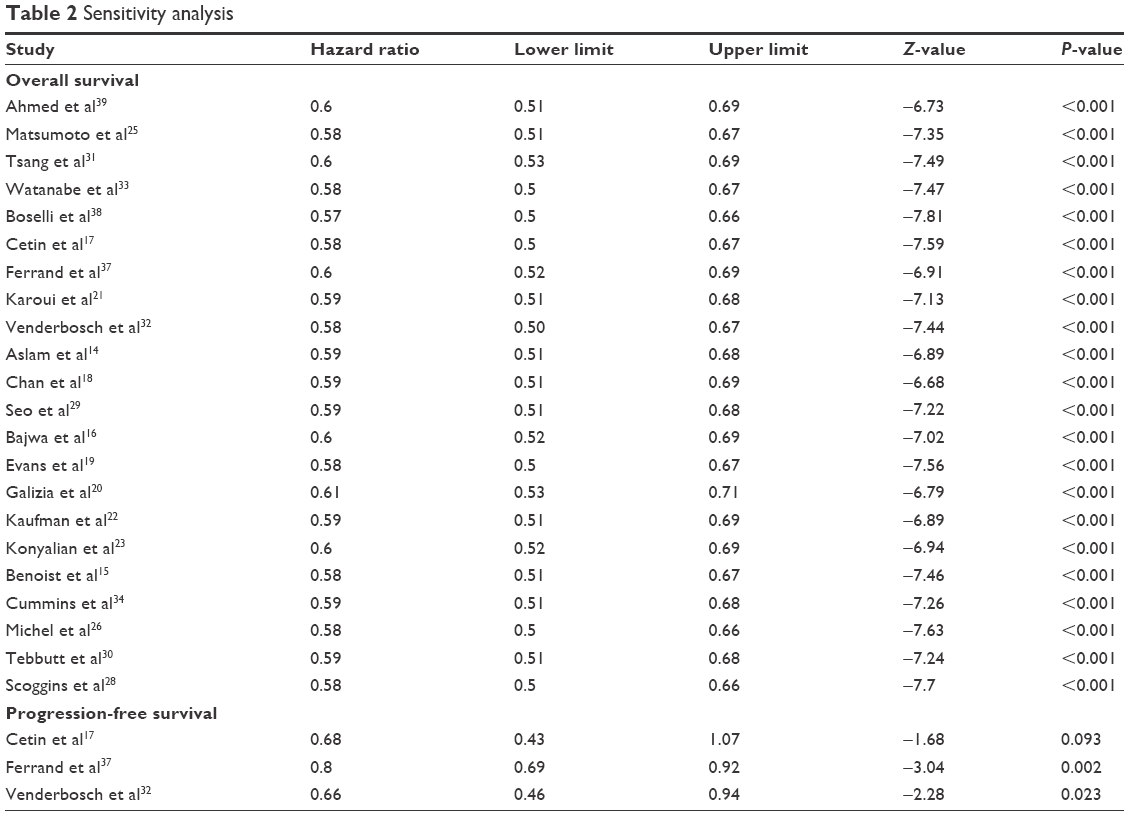 | Table 2 Sensitivity analysis |
Publication bias
Results via Egger’s test indicated possible publication bias for findings regarding OS (t=3.024, one-tailed, P=0.003), as summarized in Figure 3. After simulation by the trim-and-fill method to look for missing studies based on the random-effect model, the imputed point estimate was changed to 0.48 (95% CI 0.42–0.55). However, for PFS, the power of the test for publication bias was too low to distinguish chance from real asymmetry, due to the small number of studies (Figure 3).
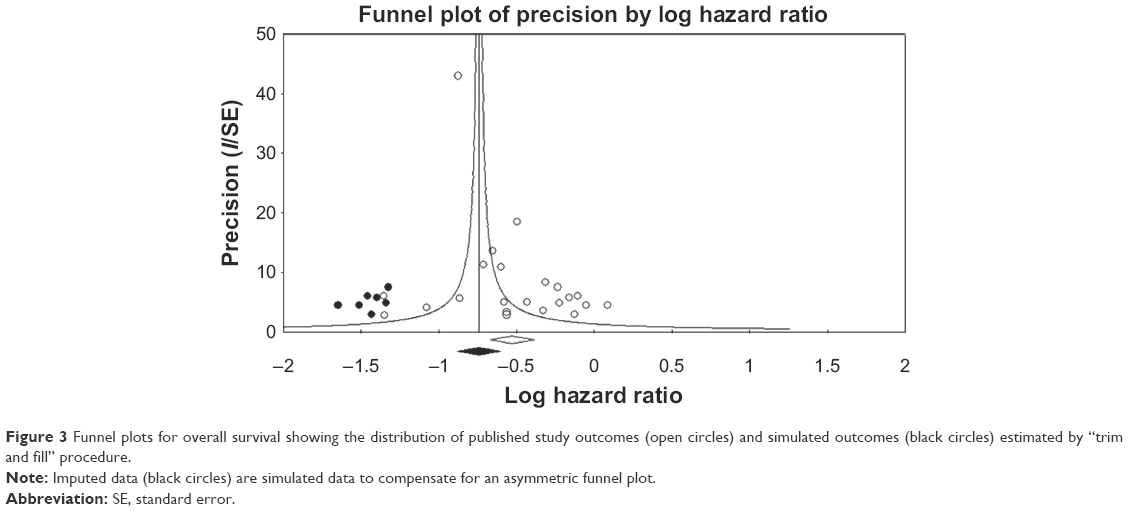 | Figure 3 Funnel plots for overall survival showing the distribution of published study outcomes (open circles) and simulated outcomes (black circles) estimated by “trim and fill” procedure. |
Quality assessment
Table 3 summarizes study quality. In general, the studies included had moderate to high quality. However, the one included RCT37 could not be properly evaluated for quality using the NOS (Table 3).
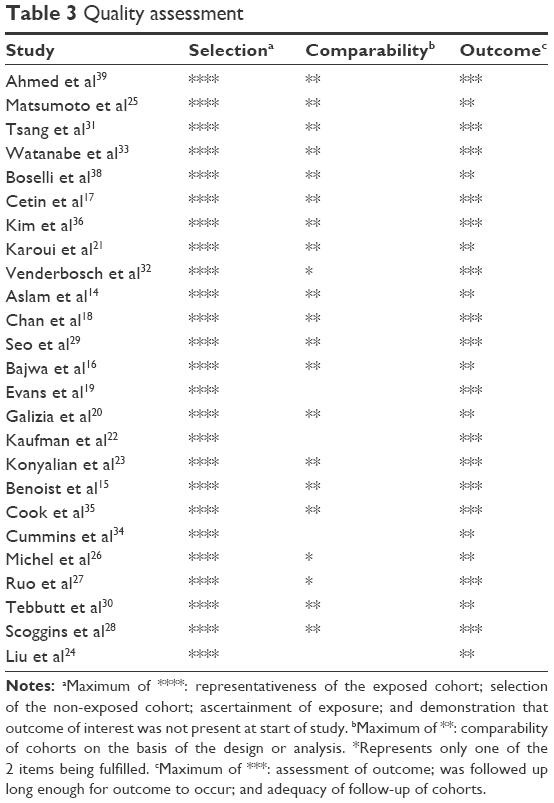 | Table 3 Quality assessment |
Discussion
This meta-analysis was conducted to update the evidence regarding benefits of noncurative primary tumor resection for treating stage IV CRC in patients being treated with chemotherapy/radiochemotherapy. Outcome data of patients receiving chemotherapy with and without primary tumor resection were compared with data of patients receiving chemotherapy alone. Overall analysis of 26 studies, including ~44,000 CRC patients, revealed that patients treated with primary tumor resection and chemotherapy were associated with longer OS than patients treated with chemotherapy alone. That is, ~30,000 patients who received primary tumor resection combined with chemotherapy with targeted therapy or second-generation therapy had longer OS and PFS than ~15,000 patients receiving targeted therapy or second-generation chemotherapy agents without resection. Sensitivity analysis, however, showed that OS data were more reliable than data for PFS, results of which were found only in three of the 26 included studies. Results also showed that among patients receiving primary tumor resection, longer OS was found among those receiving bevacizumab/cetuximab targeted therapy agents.
Results of previous systematic reviews and meta-analyses conducted between 2011 and 2014 were somewhat mixed, being both consistent and inconsistent with results of the present study.10–12,44,45 In 2011, Verhoef et al10 found that results of 24 included studies were unclear regarding survival outcomes among asymptomatic CRC patients, but median OS seemed to be improved in resected patients in the majority of studies. This understated result was more defined in the meta-analysis conducted by Ahmed et al,11 who performed prespecified subgroup analyses assessing the survival of patients with minimally symptomatic primary tumors and patients receiving second- and third-generation anticancer therapy. Those authors found that the retrospective data favored primary tumor resection in patients with advanced CRC, but they noted the low quality of the evidence at that time, suggesting that better-quality cohort studies and well-designed randomized trials were necessary to assess all outcomes adequately, especially survival outcomes.
Cirocchi et al12 highlighted the clinical issue of chemotherapy with and without primary tumor resection as one of determining how best to palliate patients with advanced, unresectable CRC. These authors included only seven nonrandomized trials with 1,086 patients, finding that primary tumor resection in asymptomatic patients with unresectable advanced CRC who were being managed with systemic chemotherapy agents did not improve OS. This may have been due to the small sample; the study was sufficiently vigorous otherwise. While chemotherapy with novel targeted agents was shown to prolong survival, a previous meta-analysis13 also reported improved survival and lower incidence of emergency surgery in patients treated with primary tumor resection. Clearly, managing the tumor itself is a critical aspect of palliation, and there is still no consensus on the benefits of resection in this population. Another meta-analysis by Anwar et al44 asked the important question all investigators have asked: “Is there a survival benefit?” After analyzing 21 studies in which the majority demonstrated survival benefits of palliative primary tumor resection, they found that the combination of selection bias, incomplete follow-up, and lack of standardized reporting of complications limited the interpretation of data. However, multivariate analysis in that study did show that tumor burden and performance status were major independent prognostic variables among the patient population and suggested that primary tumor resection should be based on these factors, rather than presence or absence of symptoms. Finally, the investigators could only conclude that there “may be” a survival benefit for primary tumor resection in stage IV CRC.
A meta-analysis by Clancy et al,45 which was conducted to determine the effects on survival of primary tumor resection in patients with stage IV unresectable, metastatic CRC, found, as we did, that primary tumor resection confers a survival advantage in advanced CRC with unresectable metastases, but significant selection bias was found in the included studies. Some of the same studies were included in the meta-analysis as in our study and those authors also suggested that only randomized controlled trials will validate these findings.
In addition, another recent meta-analysis conducted in 2015 focused on the survival benefits of chemotherapy alone, showing that oxaliplatin and capecitabine or infusional/bolus 5-fluorouracil-based chemotherapy plus bevacizumab (XELOC + B and FOLFOX + B) are active,46 approved first-line combination therapies for advanced CRC with improved OS (23.7 months) and PFS (10.3 months) when bevacizumab is part of the combination. However, the included retrospective studies were not homogeneous for site, extent of disease, performance status, comorbidities, or KRAS status (mutant or wild type). Although the present study did not focus on systemic chemotherapy, results did show that longer OS was found among resected patients receiving bevacizumab/cetuximab targeted therapy agents.
In general, among recent meta-analyses seeking answers to the question of resection benefits in advanced CRC, many patients who were in the primary tumor-resection population of studies included were those with a more favorable performance status and better overall prognosis in terms of fewer metastatic sites. Another issue may be that data on systemic chemotherapy are inconsistent between the included studies, or as Verhoef et al10 noted: “few if any data on the use of systemic therapy are presented.” Limitations in patient selection and systemic therapy data may indeed skew results and may be important factors influencing results for OS and PFS. While the present study was intended to update the evidence on the benefits of primary tumor resection in advanced CRC, it agrees with other investigators that prospective studies with adequate data on the chemotherapy agents used are needed to determine the value of resection.
Limitations
This meta-analysis has certain limitations, especially that most included studies were retrospective. In addition, complication/safety data were not reported by all included studies and thus were not assessed, which does not give a full picture of the benefits of primary tumor resection plus chemotherapy/radiotherapy for treating advanced CRC patients. The chemotherapy protocols between included studies were heterogeneous among patients in the nonresection group: some were treated with stent/bypass alone, and the studies did not report the subgroup data of chemotherapy. Possible publication bias may be inevitable during the time of decision making. Primary tumor resection may have a high proportion of patients who are unfit for chemotherapy or chemoradiotherapy, especially for data from retrospective studies. However, this might not be necessarily true for some included studies that treated patients with initial resection of primary tumor before chemotherapy and used chemotherapy as an adjuvant therapy.
Conclusion
Results of this systematic review and meta-analysis clearly show that patients with advanced CRC who receive primary tumor resection plus chemotherapy/radiotherapy have longer OS than those not receiving primary tumor resection. However, although results of this study support primary tumor resection in combination with chemotherapy/radiochemotherapy for treating stage IV CRC, possible publication bias was noted for findings regarding OS. Therefore, randomized trials are warranted to confirm findings of the present study.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Naishadham D, Jernal A. Cancer statistics, 2012. CA: Cancer J Clin. 2012;62:1–20. | ||
American Cancer Society. Colorectal Cancer Facts & Figures: 2014–2016. Atlanta: American Cancer Society; 2016. | ||
National Center for Health Statistics, Division of Health Interview Statistics. National Health Interview Survey public use data file 2010. 2011. Available from: http://www.cdc.gov/nchs/nhis/nhis_questionnaires.htm. Accessed March 25, 2016. | ||
American Cancer Society. Key statistics for colorectal cancer. 2015. Available from: http://www.cancer.org/cancer/colonandrectumcancer/detailedguide/colorectal-cancer-key-statistics. Accessed January 19, 2016. | ||
Grothey A, Sargent D, Goldberg RM, Schmoll HJ. Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J Clin Oncol. 2004;22:1209–1214. | ||
Sanoff HK, Sargent DJ, Campbell ME, et al. Five-year data and prognostic factor analysis of oxaliplatin and irinotecan combinations for advanced colorectal cancer. J Clin Oncol. 2008;26:5721–5727. | ||
Van Cutsem E, Köhne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. | ||
Costi R, Leonardi F, Zanoni D, Violi V, Roncoroni L. Palliative care and end-stage colorectal cancer management: the surgeon meets the oncologist. World J Gastroenterol. 2014;20:7602–7621. | ||
Kim YW, Kim IY. The role of surgery for asymptomatic primary tumors in unresectable stage IV colorectal cancer. Ann Coloproctol. 2013;29:44–54. | ||
Verhoef C, de Wilt JH, Burger JW, Verheul HM, Koopman M. Surgery of the primary in stage IV colorectal cancer with unresectable metastases. Eur J Cancer. 2011;47:S61–S66. | ||
Ahmed S, Shahid RK, Leis A, et al. Should noncurative resection of the primary tumour be performed in patients with stage IV colorectal cancer? A systematic review and meta-analysis. Curr Oncol. 2013;20:e420–e441. | ||
Cirocchi R, Trastulli S, Abraha I, et al. Non-resection versus resection for asymptomatic primary tumor in patients with unresectable stage IV colorectal cancer. Cochrane Database Syst Rev. 2012:CD008997. | ||
Stillwell AP, Buettner PG, Ho YH. Meta-analysis of survival of patients with stage IV colorectal cancer managed with surgical resection versus chemotherapy alone. World J Surg. 2010;34:797–807. | ||
Aslam MI, Kelkar A, Sharpe D, Jameson JS. Ten years experience of managing the primary tumours in patients with stage IV colorectal cancers. Int J Surg. 2010;8:305–313. | ||
Benoist S, Pautrat K, Mitry E, Rougier P, Penna C, Nordlinger B. Treatment strategy for patients with colorectal cancer and synchronous irresectable liver metastases. Br J Surg. 2005;92:1155–1160. | ||
Bajwa A, Blunt N, Vyas S, et al. Primary tumour resection and survival in the palliative management of metastatic colorectal cancer. Eur J Surg Oncol. 2009;35:164–167. | ||
Cetin B, Kaplan MA, Berk V, et al. Bevacizumab-containing chemotherapy is safe in patients with unresectable metastatic colorectal cancer and a synchronous asymptomatic primary tumor. Jpn J Clin Oncol. 2013;43:28–32. | ||
Chan TW, Brown C, Ho CC, Gill S. Primary tumor resection in patients presenting with metastatic colorectal cancer: analysis of a provincial population-based cohort. Am J Clin Oncol. 2010;33:52–55. | ||
Evans MD, Escofet X, Karandikar SS, Stamatakis JD. Outcomes of resection and non-resection strategies in management of patients with advanced colorectal cancer. World J Surg Oncol. 2009;7:28. | ||
Galizia G, Lieto E, Orditura M, et al. First-line chemotherapy vs bowel tumor resection plus chemotherapy for patients with unresectable synchronous colorectal hepatic metastases. Arch Surg. 2008;143:352–358. | ||
Karoui M, Roudot-Thoraval F, Mesli F, et al. Primary colectomy in patients with stage IV colon cancer and unresectable distant metastases improves overall survival: results of a multicentric study. Dis Colon Rectum. 2011;54:930–938. | ||
Kaufman MS, Radhakrishnan N, Roy R, et al. Influence of palliative surgical resection on overall survival in patients with advanced colorectal cancer: a retrospective single institutional study. Colorectal Dis. 2008;10:498–502. | ||
Konyalian VR, Rosing DK, Haukoos JS, et al. The role of primary tumour resection in patients with stage IV colorectal cancer. Colorectal Dis. 2007;9:430–437. | ||
Liu SK, Church JM, Lavery IC, Fazio VW. Operation in patients with incurable colon cancer: is it worthwhile? Dis Colon Rectum. 1997;40:11–14. | ||
Matsumoto T, Hasegawa S, Matsumoto S, et al. Overcoming the challenges of primary tumor management in patients with metastatic colorectal cancer unresectable for cure and an asymptomatic primary tumor. Dis Colon Rectum. 2014;57:679–686. | ||
Michel P, Roque I, Di Fiore F, et al. Colorectal cancer with non-resectable synchronous metastases: should the primary tumor be resected? Gastroenterol Clin Biol. 2004;28:434–437. | ||
Ruo L, Gougoutas C, Paty PB, Guillem JG, Cohen AM, Wong WD. Elective bowel resection for incurable stage IV colorectal cancer: prognostic variables for asymptomatic patients. J Am Coll Surg. 2003;196:722–728. | ||
Scoggins CR, Meszoely IM, Blanke CD, Beauchamp RD, Leach SD. Non operative management of primary colorectal cancer in patients with stage IV disease. Ann Surg Oncol. 1999;6:651–657. | ||
Seo GJ, Park JW, Yoo SB, et al. Intestinal complications after palliative treatment for asymptomatic patients with unresectable stage IV colorectal cancer. J Surg Oncol. 2010;102:94–99. | ||
Tebbutt NC, Norman AR, Cunningham D, et al. Intestinal complications after chemotherapy for patients with unresected primary colorectal cancer and synchronous metastases. Gut. 2003;52:568–573. | ||
Tsang WY, Ziogas A, Lin BS, et al. Role of primary tumor resection among chemotherapy-treated patients with synchronous stage IV colorectal cancer: a survival analysis. J Gastrointest Surg. 2014;18:592–598. | ||
Venderbosch S, de Wilt JH, Teerenstra S, et al. Prognostic value of resection of primary tumor in patients with stage IV colorectal cancer: retrospective analysis of two randomized studies and a review of the literature. Ann Surg Oncol. 2011;18:3252–3260. | ||
Watanabe A, Yamazaki K, Kinugasa Y, et al. Influence of primary tumor resection on survival in asymptomatic patients with incurable stage IV colorectal cancer. Int J Clin Oncol. 2014;19:1037–1042. | ||
Cummins ER, Vicky KD, Poole GV. Incurable colorectal carcinoma: the role of surgical palliation. Am Surg. 2004;70:433–437. | ||
Cook AD, Single R, McCahill LE. Surgical resection of primary tumors in patients who present with stage IV colorectal cancer: an analysis of Surveillance, Epidemiology and End Results data 1988–2000. Ann Surg Oncol. 2005;12:637–645. | ||
Kim SK, Lee CH, Lee MR, Kim JH. Multivariate analysis of the survival rate for treatment modalities in incurable stage IV colorectal cancer. J Korean Soc Coloproctol. 2012;28:35–41. | ||
Ferrand F, Malka D, Bourredjem A, et al. Impact of primary tumor resection on survival of patients with colorectal cancer and synchronous metastases treated by chemotherapy: results from the multicentre, randomized trial Fédération Francophone de Cancérologie Digestive 9601. Eur J Cancer. 2013;49:90–97. | ||
Boselli C, Renzi C, Gemini A, et al. Surgery in asymptomatic patients with colorectal cancer and unresectable liver metastases: the authors’ experience. Oncol Targets Ther. 2013;6:267–272. | ||
Ahmed S, Leis A, Fields A, et al. Survival impact of surgical resection of primary tumor in patients with stage IV colorectal cancer: results from a large population-based cohort study. Cancer. 2014;120:683–691. | ||
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–605. | ||
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17:2815–2834. | ||
Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56:455–463. | ||
Sterne JA, Sutton AJ, Ioannidis JP, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002. | ||
Anwar S, Peter MB, Dent J, Scott NA. Palliative excisional surgery for primary colorectal cancer in patients with incurable metastatic disease Is there a survival benefit? A systematic review. Colorectal Dis. 2012;12:920–930. | ||
Clancy C, Burke JP, Barry M, Kalady MF, Calvin-Coffey J. A meta-analysis to determine the effect of primary tumor resection for stage IV colorectal cancer with unresectable metastases on patient survival. Ann Surg Oncol. 2014;21:3900–3908. | ||
Petrelli F, Coinu A, Gilardi M, Cabiddu M, Zaniboni A, Barni S. Efficacy of oxaliplatin-based chemotherapy + bevacizumab as first-line treatment for advanced colorectal cancer: a systematic review and pooled analysis of published trials. Am J Clin Oncol. 2015;38:227–233. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.