")
Back to Journals » Open Access Journal of Contraception » Volume 12
Men’s Knowledge of Vasectomy and Its Associated Factors in Debre Tabor Town, Northwest Ethiopia: A Community-Based Cross-Sectional Study
Authors Degu Ayele A , Yenealem Beyene F , Getnet Kassa B , Nibret Mihretie G
Received 10 December 2020
Accepted for publication 14 January 2021
Published 11 February 2021 Volume 2021:12 Pages 27—34
DOI https://doi.org/10.2147/OAJC.S296798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Alemu Degu Ayele,1 Fentahun Yenealem Beyene,2 Bekalu Getnet Kassa,1 Gedefaye Nibret Mihretie1
1Department of Midwifery, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Midwifery, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Alemu Degu Ayele Tel +251920770887
Email [email protected]
Purpose: Even though vasectomy is one of the safest, simplest, and most effective family planning methods available for men, it is one of the least used contraceptive methods in the developing world, including Ethiopia. The goal of this study was to assess the level of knowledge towards vasectomy and its associated factors among married men in Debre Tabor Town.
Methods: A community-based cross-sectional study was conducted from December 5– 25, 2019. A total of 413 married men participated and selected by simple random sampling. Data was entered using EpiData version 4.2 and analyzed by SPSS version 23. A bivariable and multivariable logistic regression model was carried out. Finally, variables having a P-value of < 0.05 at 95% CI were considered as statistically significant.
Results: In this study, 38.5% of men had an adequate level of knowledge about vasectomy. Multivariable logistic regression showed that an educational status of secondary education and college and above (AOR=4.70, 95% CI=1.26– 17.55; and AOR=8.36, 95% CI=2.41– 28.97, respectively), having four or more alive children (AOR=0.51, 95% CI=0.29– 0.89), and positive attitude (AOR=2.47, 95% CI=1.58– 3.86) were significantly associated with knowledge of vasectomy.
Conclusion: Knowledge of married men towards vasectomy was relatively low. Educational status, number of children, and attitude were statistically significant with the men’s knowledge about vasectomy. Emphasis should therefore be put on improving the educational status of men and positively changing the male upbringing culture right from their childhood which will also improve their attitude towards vasectomy in the future.
Keywords: vasectomy, knowledge, Ethiopia
Introduction
Vasectomy is a man’s permanent contraceptive method for those have already have the desired number of children they want, which is accepted and appropriate only in certain developed countries of the world. Even though it is very safe and easy to perform, only 45 million couples worldwide are relying on it.1,2 The number of world population is showing increments from day-to-day and it is expected to reach around 9.9 billion by 2050, and the population of Africa will be more than double.2 In Africa, Ethiopia is the second most populous country next to Nigeria, with an estimated population of 101.7 million in mid-2016.3 The country is also affected by high maternal morbidity and mortality due to unintended and unwanted pregnancies.4,5 The goal of family planning across the world has gained attention because of its significance in decision- making on population growth and developmental issues.6 Globally, the use of contraceptive has significantly decreased the maternal mortality rate by 44%.7
Despite the 1994 International Conference on Population and Development (ICPD) in Cairo, which highlighted that men’s involvement in sexual and reproductive health issues is very crucial for better outcome and set specific guidelines for increasing men’s participation in family planning, the involvement of men in family planning is still very low in Africa.8–10
In developing countries, greater than 200 million women need to prevent pregnancy, but they are not using any modern contraceptive methods.11 Utilizing the most effective long-acting and permanent contraceptive methods can prevent these huge numbers of unintended pregnancies and induced abortions could essentially be reduced.12 Furthermore, evading barriers that hiders long-acting contraceptive use and enhancing the demand for more effective contraceptives could avert 54 million unintended pregnancies, more than 79,000 maternal deaths, and one million infant deaths each year.11
In recent years, international health organizations have indicated that the role of men in the use and promotion of contraceptive methods is imperative in providing couples with male-oriented contraceptive options, such as vasectomy. Although thisprocedure is simple and easy with a high success rate (>99%) and minor complications, it is underused around the world, predominantly in developing countries like Ethiopia.13–15 Studies in African countries have shown that knowledge of vasectomy is low.16–18
Ethiopia has a target program to raise the prevalence of contraceptive use to 55% by 2020.19 To achieve this target the government, in partnership with other stack holders, is focusing on diversifying the FP method mix by increasing demand and access to long-acting and permanent methods.20 As a result of this initiative, the contraceptive prevalence rate (CPR) reached 41% in 2019 from 35% in 2016, but the method mix is still dominated by female-dependent short acting methods such as injectables (27%), followed by implants (9%).21
Different reviewed literature reports have shown that the level of knowledge about vasectomy was associated with different variables, like educational status, occupation, cultural beliefs, societal norms, number of live children, and attitude.22–27
According to 2016 Ethiopian demographic and health survey (EDHS) data, only 23.5% of married men had heard about vasectomy.28 However, this survey simply measured whether the men and women had heard about vasectomy or not. A more recent studies done in Gondar Town and Dangila Town, Northwestern Ethiopia showed that only 13.3% and 44.8% of married men had an adequate level of knowledge of vasectomy,26,27 respectively. And a study by Ayele et al.29 showed that only 19.6% of men had any future intention to use vasectomy as a contraceptive method This inadequate level of knowledge about vasectomy may hinder the current and future utilization of the service. Therefore, this study aimed to assess married men's level of knowledge and its associated factors in Debre Tabor Town, Northwest Ethiopia. The result of this study may be a benchmark for governments, policy-makers, and respective stakeholders in Ethiopia and other developing countries to design an effective strategy that scales up male participation in family planning.
Methods
Study Design and Setting
This was a community-based cross-sectional study done in Debre Tabor Town from December 5–25, 2019. Debre Tabor Town is located 665 kilometers Northwest of Addis Ababa (the capital city of Ethiopia) and 103 kilometers Southwest of Bahir Dar and it is the capital city of south Gondar zone, Northwest Ethiopia. The town has six small administrative units called kebeles, with a total population of 92,530 based on a 2018 report of the town administration. It has one general hospital, four health centers, and five private clinics which provide community health services including family planning.30
All married men living in the town were the study population. All married men living in the town within the study period were included. Married men who were critically ill (bed ridden), and who lived for less than 6 months during the data collection period in the town were excluded from the study.
Sample Size and Sampling Procedure
The sample size was determined by using EPI-INFO version 7.0 statistical software. With the assumption of the prevalence of good level of knowledge about vasectomy at 44.8%,27 and 95% confidence interval with 5% margin of error, the sample size becomes 380. We added a 5% non-response rate to yield a final sample size of 418. The town has a total of six kebeles and all these were involved in this study. A total of 14,088 households and 14,614 married men were living in the town.30 A household was the sampling unit in each kebele and samples were allocated proportionally to each kebele based on their total household number. Household numbers with married men in each kebele were obtained from the kebeles registration book. Then we reached the calculated 418 study households through a simple random sampling technique by using a table of random numbers starting from kebele one from a random start point. The first household was chosen in each kebele by using a lottery method. One married man per household was involved. In case two or more eligible men were found in one household, only one was selected by lottery method and if no eligible men were found in the selected household, the next eligible household situated in a clockwise direction was visited and involved until we achieved the calculated sample size.
Operational Definitions
Knowledge
Men's level of knowledge about vasectomy was assessed by using nine knowledge-related questions. A value of one or zero was given for each correct and incorrect response, respectively, and labeled as good knowledge for those participants who correctly respond to at least five knowledge-related questions and poor knowledge for those who responded correctly to less than five knowledge-related questions.27
Attitude
In this study, the attitude of study participants towards vasectomy was also assessed by using nine attitude-related questions, and labeled as positive attitude for those respondents who scored greater than or equal to the mean score and negative attitude for those respondents who scored less than the mean score.23
Data Collection Procedures and Data Quality Control
The data were collected through face-to-face interview techniques using a structured and pre-tested questionnaire. The questionnaire was first prepared in English, then translated to the local language, Amharic, for simplicity, and back to English for consistency, by two different language expert individuals who speak both English and Amharic fluently. The tool had four items (socio-demographic characteristics, obstetrics and reproductive related characteristics, medical and health facility characteristics, and knowledge-related characteristics). Pre-testing of the questionnaire was done on 5% of participants (20 married men) in Gassay Town near to the study setting. Based on the pre-test, modifications and corrections like wording, logical sequence and skip patterns were made immediately. The data were collected by four diploma health professionals who had previous experience of data collection and who were supervised by two BSc health professionals. Data collectors and supervisors were trained for 1 day on the aim of the study, method of data collection, contents of the questionnaire, how to keep confidentiality, responders’ right, and informed consent before they start the data collection. The completeness and consistency of data was cross-cheeked, cleaned, and compiled on a daily basis by supervisors and the principal investigator. The overall activity was supervised by the principal investigator of the study.
Data Processing and Analysis
The collected data were coded and entered by using the Epi-Data version 4.2 and then exported to SPSS version 23 for analysis. Descriptive statistics including tables and percentages were used to describe the data. Bivariable and multivariable logistic regression analyses were carried out. Variables that showed association in binary logistic regression analysis and which have P-value of less than 0.20 were entered into a multivariable logistic regression analysis model for farther analysis. Lastly, a significant association was declared depending on a P-value of <0.05 and adjusted odds ratio (AOR) with 95% CI.
Ethical Consideration
Ethical clearance was secured from the institutional review board of Bahir Dar University. Also, a support letter was granted from Debre Tabor Zonal Health Office and administrative office of the town. Informed consent was secured from each study participant. Any personal identifiers were excluded to keep privacy and to assure confidentiality. This paper follows the principles enunciated in the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
In this study, a total of 413 married men were involved with a response rate of 98.8%. The mean age of the participants was 38.06 (SD=±6.873) years. The majority of the participants (400, 96.9%) were Amhara by ethnicity and orthodox Christians followers (365, 88.4%) (Table 1).
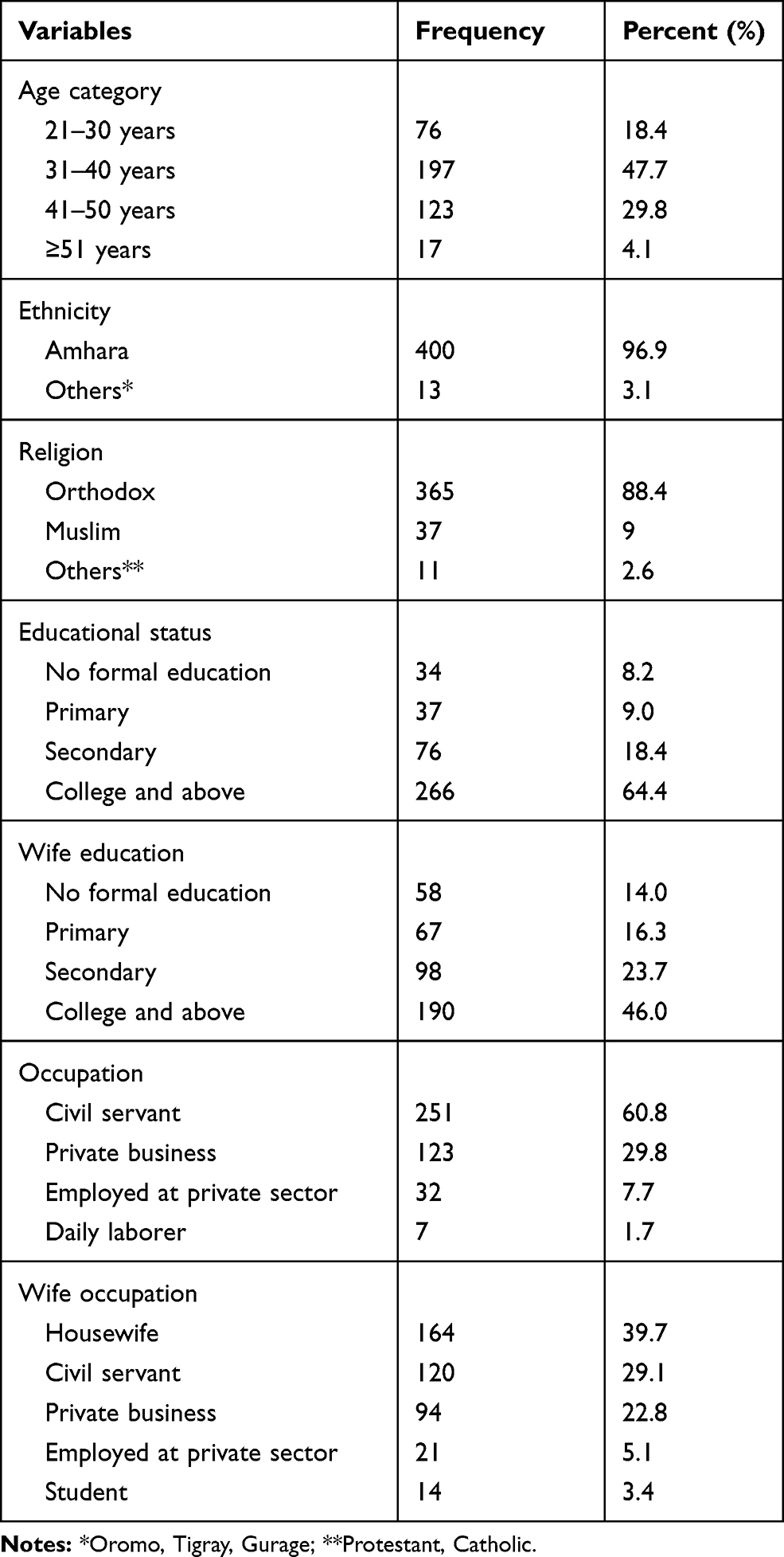 |
Table 1 Socio -Demographic Characteristics of Men in Debre Tabor Town, Northwest Ethiopia, December 2019 (N=413) |
Reproductive Characteristics of Participants
Out of the total participants, 258 (62.5%) had three or more alive children. The majority of the study participants (370, 89.6%) had discussed FP with their partner. One hundred and twenty-four (30%) participants had completed their family size (Table 2).
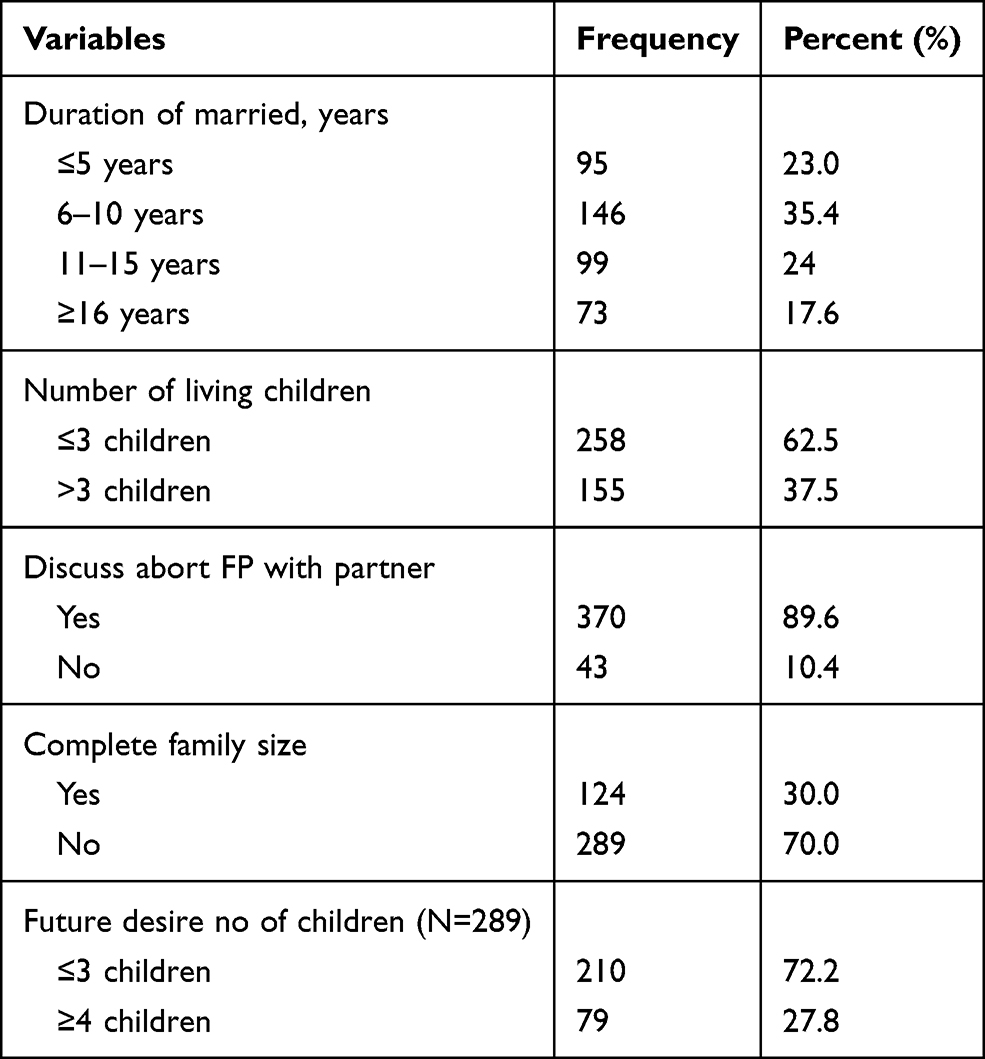 |
Table 2 Reproductive Characteristics of Men in Debre Tabor Town, Northwest Ethiopia, December, 2019 (N=413) |
Knowledge of Study Participants About Vasectomy
More than half the participants (250, 60.5%) reported that they had ever heard about vasectomy. Of those who had ever heard, healthcare providers (107, 43%), colleagues (89, 35.6%), mass media (71, 28.4%), and volunteers (34, 13.6%) were the main source of information. In this study only 147 (58.8%) participants defined vasectomy correctly as “it is a men permanent contraceptive method after completing their desire number of children”. Overall, 159 (38.5%) married men with a 95% CI of 33.8–43.7 had good knowledge about vasectomy (Table 3).
 |
Table 3 Knowledge of Men About Vasectomy in Debre Tabor Town, Northwest Ethiopia, December 2019 (N=413) |
Attitude of Participants Towards Vasectomy
Two thirds of the study participants (259, 62.7%) had a negative attitude, while 154 (37.3%) had a positive attitude toward vasectomy.
Factors Affecting Level of Knowledge About Vasectomy Among Study Participants
In binary logistic regression, men’s age, educational status, wife educational status, wife occupation, number of live children, and attitude of participants towards vasectomy have shown a statistically significant association with the knowledge of vasectomy. In multivariable binary logistic regression analysis, only educational status, number of live children, and attitude were remained statistically significant with participants’ level of knowledge about vasectomy.
Based on our finding respondents who had completed secondary education were nearly 5-times more likely to have a good level of knowledge about vasectomy (AOR=4.70, 95% CI=1.26–17.55) as compared to those who did not attended formal education. Similarly, study participants who had attended college and above were 8.36-times higher the odds of having good knowledge about vasectomy (AOR=8.36, 95% CI=2.41–28.97) as compared to those who did not attend formal education.
Moreover, participants who had four or more alive children were inversely correlated with level of knowledge of vasectomy (AOR=0.51, 95% CI=0.29–0.89) as compared to men who had less than or equal to three alive children. Married men who had a positive attitude toward vasectomy were 2-times more likely to had good knowledge about vasectomy (AOR=2.47, 95% CI=1.58–3.86) as compared to their counterparts (Table 4).
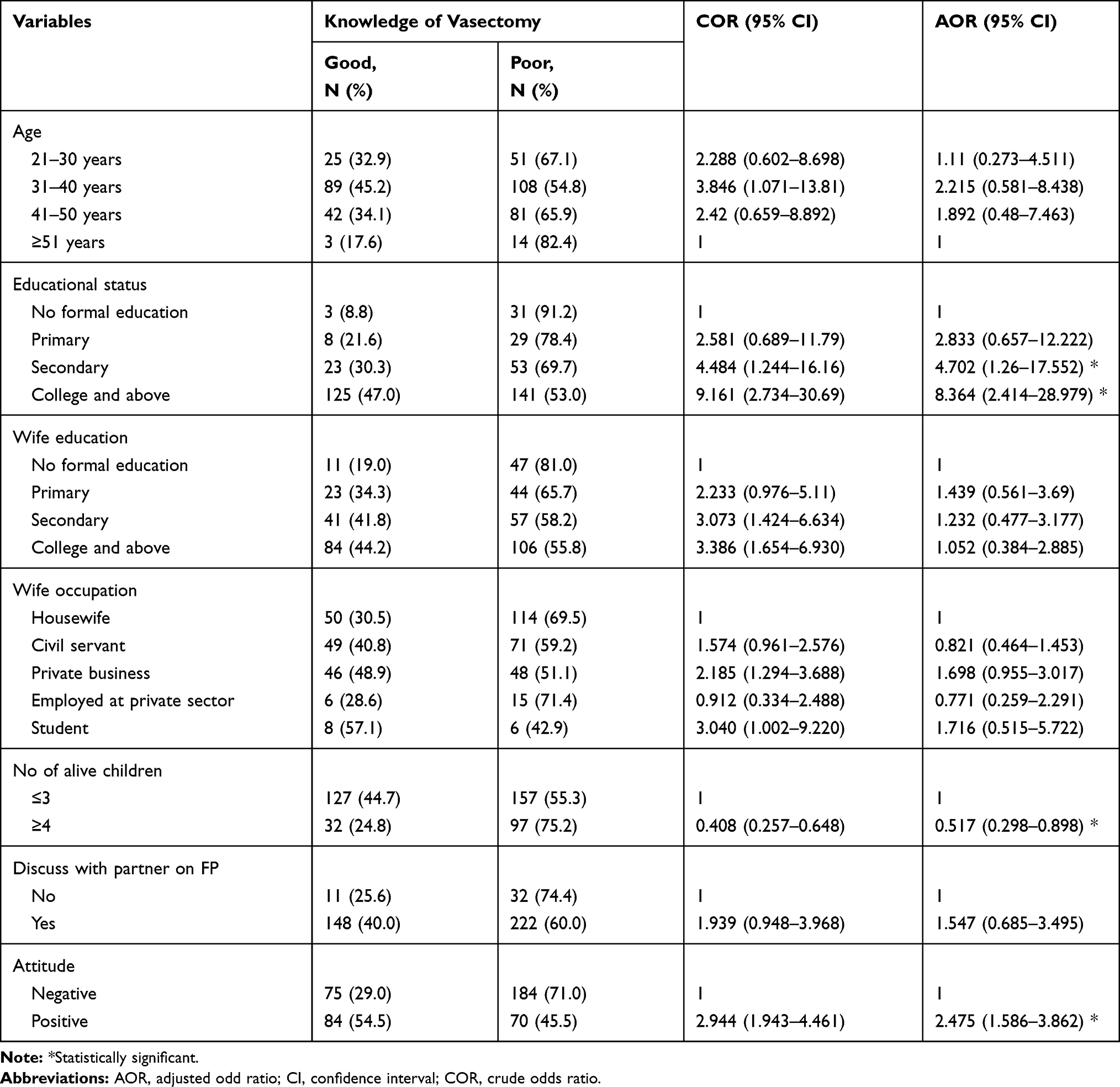 |
Table 4 Bivariable and Multivariable Logistic Regression on Predictors of Level of Knowledge of Men About Vasectomy in Debre Tabor Town, Northwest Ethiopia, December 2019 (N=413) |
Discussion
Within the sphere of family planning, vasectomy is very often ignored, despite being one of the safest, simplest, and most highly effective and least expensive contraceptive methods.8 In this study, about 60.5% of married men had ever heard about vasectomy. This is higher than a study done in Turkey, which reprted 45.1% of participants had heard about vasectomy prior to the survey.13 This might be due to differences in educational status of the participants, since 64.4% of the respondents had attended College and above, but in the comparable studies only 21.4% had attended college and above. This may also be due to time difference and study setting variation. This finding is also higher than the 2016 EDHS report, which indicated that only 23.5% of married men had ever heard about vasectomy.28 This may be because of time change, since EDHS 2016 was done 5 years ago. Also, the current study was done in a more urban setting, whereas the EDHS incorporates both rural and urban areas. Also, great commitment of the government and other stakeholders to scale up the acceptance of long-acting and permanent FP methods may be the other possible reason.
Of those who had ever heard about vasectomy, only 58.8% defined it correctly (they reported vasectomy as “a men permanent contraceptive method after completing their desired number of children”). Other responses in the survey clearly showed the presence of misconceptions about vasectomy among married men. Biases and misconceptions are the main reasons for low health service use. This is the reason why vasectomy use is low in Ethiopia. For example, about 25.6% and 15.6% of married men reported that vasectomy is similar to castration and makes the men impotent, respectively.
This study showed that 38.5% of participants had an adequate level of knowledge about vasectomy. This finding was in line with studies done in Nigeria, which revealed that 37.5% and 38% of the participants had good knowledge levels about vasectomy, respectively.18,23 Once more our study finding was comparable with a study conducted in east Wollega Zone of Oromia region, Ethiopia, which revealed that 35.3% of men knew about vasectomy.25 However, this finding was lower than studies conducted in India, which showed that 70.2% and 44.6% of married men were knowledgeable about vasectomy respectively.31,32 The possible explanation might be increased male involvement in family planning service due to socio-demographic variation and healthcare system differences.
Our finding was also lower than a cross-sectional study conducted in Pakistan, which indicated that 85.6% of the participant had adequate knowledge about vasectomy.33 This may be due to socio-demographic variation between the countries, like the educational status of participants, since 74.3% of men in Pakistan were secondary and above in their educational level. On the other hand, the finding of this study was higher than another study conducted in Pakistan (11%).34 The variation may be explained due to differences in perception towards vasectomy since 89% of married men in Pakistan perceived that vasectomy decreases male’s sexual desire but, in our study, only 41.2% of participants had this misconception about vasectomy. This finding is also higher than a study conducted in Nigeria (27.5%).16 The discrepancy may be explained due to differences in sociodemographic characteristics such as educational status, since 64.4% of participant in this study attained college and above but in the comparable study only 30.5% of participants attained above secondary school. Government concern and NGO emphasis is also another reason.
The result of this study revealed that as the educational status of the participant increases the knowledge level of vasectomy also increased linearly. This finding is supported by studies conducted in Rwanda,24 Gondar,26 and Dangila Town.27 The reason for this might be that educated men are more likely to be exposed to different media. They are also more likely to comprehend the information they obtained.
According to our study the number of children has an inverse relation with level of knowledge. Men who had four or more children are inversely associated with good knowledge about vasectomy. Likewise, research conducted in Gondar Northwest Ethiopia also concluded that the number of children was inversely correlated with knowledge of vasectomy.26 The possible explanation for this finding might be as the numbers of children increase the men think over about the economic issues for his family, considered costly and likely it results in family quarrels and tensions. This may also have a negative impact on accessing information and continued education.
The result of this study also showed that there was a positive relationship between attitude towards vasectomy and its level of knowledge of married men. It revealed that participants who had a good level of knowledge positively affected the attitude towards vasectomy. Likewise, a study conducted in Nigeria showed that there is a significant association between participants attitude towards vasectomy and their level of knowledge about it.23 Since attitude is a key factor that influences the decision-making about vasectomy uptake, men with a positive attitude towards vasectomy are better able to know about it and share responsibilities in FP practice with their partner. And also, further reason may be when the individual had a positive attitude; they can break myths and misconception that were negatively affecting the knowledge about vasectomy, like vasectomy being similar to castration.
Conclusion
In conclusion, the level of knowledge of married men was low in Debre Tabor Town Northwest Ethiopia. The educational status, number of alive children, and attitude towards vasectomy were significantly associated with the level of knowledge about vasectomy.
Recommendations
As per the findings, emphasis should be given on improving the educational status of men to improve their knowledge, and positively changing the men's upbringing culture right from their childhood which will also improve their attitude towards vasectomy. This in turn would motivate more men to actively participate in family planning and readily accept vasectomy as a safe and effective method of family planning. Avoiding misconception regarding vasectomy through regular health education may also be a very important strategy to scale up vasectomy knowledge and its utilization in the future. We also recommend further researcher to come up with additional and detailed findings, especially on qualitative aspects.
Data Sharing Statement
The datasets used in this study are available from the corresponding author on request.
Acknowledgments
The authors would like to acknowledge Bahir Dar University for ethical clearance and technical support as well as the Debre Tabor Town administration, study participants, data collectors, and supervisors.
Funding
No funding sources.
Disclosure
The authors declare that they have no conflict of interests for this work or regarding the publication of this paper.
References
1. Adeyimika T, Oyedunni S, Ademola J, et al. Antecedent factors relating to the adoption of vasectomy among married men in peri-urban communities of Ibadan, Nigeria. Int J Nurs Midwif. 2016;8(6):47–54. doi:10.5897/IJNM2015.0203
2. Ajuwon A, Desmenuu A. Men’s awareness of, barriers to, and intention to adopt vasectomy among married men in Ibadan, Nigeria. 2014. Available from: https:/wwwresearchgatenet/peblication/313512381.
3. Population Reference Rureau. 2016 world population data sheet. 2016. Available from: http://wwwprborg/Publications/Datasheets/2016/2016-world-population-data-sheetaspxv.
4. Population Reference Bureau. 2016 world population data sheet with a special focus on human needs and sustainable resource. 2016. Available from: www.world.pop.data.org.
5. WHO, UNICEF, UNFPA, World Bank Group and the United Nations population division trends in maternal mortality: 1990 to 2015. Geneva: World Health Organization. 2015.
6. Chaudhary BK, Wantamutte AS, Sah JK, et al. Knowledge, attitude and practices regarding family planning methods among married men in urban field practice area of Ramnagar urban health center. Belagavi-A Cross-Sectional Study. 2015;8:212–219.
7. Ahmed S, Li Q, Liu L, et al. Maternal deaths averted by contraceptive use: resultsfrom a global analysis of 172 countries. lancet. 2012;380:111–125. doi:10.1016/S0140-6736(12)60478-4
8. United Nation Population Information Network. Report of the international conference on Population and development. Cairo; 1994. Available from: www.un.org/popin/icpd/conference/offeng/poahtml.
9. Mulatu K, Men’s MW. Involvement in long acting and permanent contraceptive use in Mizan-Aman District Southwestern Ethiopia: a community based cross-sectional study. Health Sci J. 2016;10(2).
10. Butto D, Mburu S. Factors associated with male involvement in family planning in West Pokot county. Kenya Univers J Public Health. 2015;3(4):160–168. doi:10.13189/ujph.2015.030404
11. Bongaarts J: Family planning programs for the 21st century: rationale and design. New York, NY 10017 USA: Population Council; 2012. Available from: http://www.popcouncil.org.
12. Bradley S, Croft T, Rutstein S: The impact of contraceptive failure on unintended births and induced abortions: estimates and strategies for reduction. DHS analytical studies No. 22. Calverton, Maryland, USA: ICF Macro; 2011.
13. Kısa S, Savaş E, Zeyneloğlu S, et al. Opinions and attitudes about vasectomy of married couples living in Turkey.American. Am J Men’s Health. 2017;11(3):531–541. doi:10.1177/1557988315620275
14. Shongwe P, Ntuli B, Madiba S. Assessing the acceptability of vasectomy as a family planning option: a qualitative study with men in the Kingdom of Eswatini. Int J Environ Res Public Health. 2019;16:5158. doi:10.3390/ijerph16245158
15. Shattuck D, Perry B, Packer C, et al. A review of 10 years of vasectomy programming and research in low resource settings. Glob Health Sci Pract. 2016;4(4):647–660.
16. Tijani K, Ojewola RW, Yahya GL, et al. Attitudes and acceptance of nigerians towards vasectomy- a comparison of married men and women in lagos. East Afr Med J. 2013;90(3):89–94.
17. Akpamu U, Nwoke E, Osifo U, et al. Knowledge and acceptance of ‘vasectomy as a method of contraception’ amongst Literate Married Men in Ekpoma, Nigeria. Afr J Biomed Res. 2010;13:153–156.
18. Onasoga O, Edoni E, Ekanem J. Knowledge and attitude of men towards vasectomy as a family planning method in Edo State, Nigeria. J Res Dev Nurs Midwifery. 2013;2(1):13–21.
19. Federal Ministry of Health [Ethiopia]. Health sector transformation plan, 2015–2020. October, 2015.
20. Marie Stopes International Ethiopia Addis Ababa. Knowledge, attitudes and practices (KAP) survey, permanent methods of family planning in four regions of Ethiopia. USAID; 2017.
21. Central Statistical Agency [Ethiopia]. Mini Ethiopia demographic and health survey. 2019.
22. Ajeet S, Shilpa H, Jaydeep N. Denial mode for vasectomy among married men in central India: causes and suggested strategies. Psychol Psychother. 2013;3(4).
23. Owopetu C, Chukwuma S, Nwozichi C. Knowledge and attitude of men about vasectomy as a method of family planning among married men working in Babcock University, Ogun state, Nigeria. Int J Nurs Midwif. 2015;7(3):30–35. doi:10.5897/IJNM2014.0157
24. Ntakirutimana C, Umuziga P, Nikuze B, et al. Vasectomy is family planning: factors affecting uptake among men in eastern province of Rwanda. Rwanda J Med Health Sci. 2019;2(2):126–137. doi:10.4314/rjmhs.v2i2.8
25. Awie B. Men’s knowledge and attitude towards vasectomy in east Wollega zone of Oromia region, Ethiopia. 2014.
26. Yenus H, Assefa G, Atenafu A. Knowledge and attitude of married men towards vasectomy in Gondar Town, Northwest Ethiopia. BAOJ Hiv. 2016;2:010.
27. Jemberie A, Abeje G, Asrat A. Educational status as determinant of men’s knowledge about vasectomy in Dangila town administration, Amhara region,Northwest Ethiopia.Reproductive. health. 2017;14(1):54.
28. Central Statistical Agency [Ethiopia]. Ethiopia demographic and health survey. 2016.
29. Ayele AD, Beyene FY, Wudineh KG, et al. Intention to use vasectomy and its associated factors among married men in Debre Tabor Town, North West Ethiopia,2019. PLoS One. 2020;15(9):e0238293. doi:10.1371/journal.pone.0238293
30. Town Administration of Debre Tabor [Debre Tabor]. Population size and number of households of Debre Tabor town. 2018.
31. Nair G, Wadke R, Relwani N, et al. Knowledge and attitude of married men towards vasectomy in an urban slum of Navi Mumbai. Int J Community Med Public Health. 2017;4(12):4563–4568. doi:10.18203/2394-6040.ijcmph20175331
32. Choudhary H. A study to assess the knowledge, attitude and practice regarding vasectomy among males, working in nandini milk dairy at Kolar. Int J Nurs Sci Pract. 2013;10:1–4.
33. Zareen H, Shahzad S, Salahhudin M. Sociodemographic and reproductive factors affecting knowledge of married men accepting vasectomy. J Ayub Med Coll Abbottabad. 2016;28(2):323–326.
34. Naz S, Saqib M. An assessment of the knowledge and attitude towards family planning among educated married men of urban Islamabad, Pakistan. Pak J Med Res. 2017;56(3):73–77.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.