")
Back to Journals » Risk Management and Healthcare Policy » Volume 9
Medicine reclassification processes and regulations for proper use of over-the-counter self-care medicines in Japan
Authors Nomura K , Kitagawa Y, Yuda Y, Takano-Ohmuro H
Received 12 October 2015
Accepted for publication 11 February 2016
Published 25 July 2016 Volume 2016:9 Pages 173—183
DOI https://doi.org/10.2147/RMHP.S98099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Frank Papatheofanis
Kaori Nomura,1 Yuki Kitagawa,2 Yasukatsu Yuda,2 Hiromi Takano-Ohmuro2
1Division of Molecular Epidemiology, Jikei University School of Medicine, 2Faculty of Pharmacy, Musashino University, Shinmachi, Tokyo, Japan
Objectives: Japan has actively reclassified substances ranging from prescription drugs to over-the-counter (OTC) drugs in recent years. The sale of most OTC drugs was deregulated several times and pharmacists’ supervision was deemed no longer mandatory. Japan established a new OTC evaluation system in 2015 to hear opinions from various stakeholders regarding medicine types to be reclassified. This study aimed to examine the new framework to identify candidate substances for reclassification. Moreover, we examined how to manage the safe, self-care use of OTC drugs in Japan.
Methods: The necessary regulatory information on OTC approvals as of January 2015 was collected using an Internet search and relevant databases. To highlight the characteristics of OTC drugs in Japan, the UK was selected as a comparison country because it too was actively promoting the reclassification of medicines from prescription to nonprescription status, and because of economic similarity.
Results: Japan and the UK have a risk-based classification for nonprescription medicines. Japan has made OTC drugs available with mandatory pharmacists’ supervision, face-to-face with pharmacists, or online instruction, which is similar to the “pharmacy medicine” practiced in the UK. Japan recently reformed the reclassification process to involve physicians and the public in the process; some interactions were back to “prescription-only medicine” in the UK.
Conclusion: It is expected that the opinion of marketers, medical professionals, and the public will improve the discussion that will greatly contribute to the safe use of drugs. Monitoring the new system will be noteworthy to ensure that OTC drug users are managing their self-care properly and visiting a doctor only when necessary. The supply methods are similar in Japan and the UK; however, the expected growth in the Japanese OTC market by the Cabinet and the industry is still uncertain.
Keywords: OTC, healthcare policy, switch drugs, drug safety, health expenditure, pharmacists’ role, self-medication
Introduction
An aging society faces increasing health care and medical costs caused by multiple medicines and device use for comorbidities and geriatric diseases, such as cancer.1 It is estimated that aging has a relatively small influence on these expenditure increases. However, the prevention of illness and promotion of self-care healthy living, particularly among the elderly, has been recognized as an important strategy to reduce costs (eg, cost-of-illness studies on age-related diseases).1 In such situations, the Japanese government implemented a policy in 2013 with the goal being to extend healthy life expectancy2 by addressing preventive activities and self-care. Similar to other health-related policies, a country’s strategies and tools for planning and implementing self-care inevitably reflect its sociocultural perspective and community involvement.3 The definition of self-care has been documented by the World Health Organization (WHO), its regional office, and others (Table 1).3–8 Health care systems vary between countries and periods; therefore, health-related terms and concepts have different regional-dependent definitions.
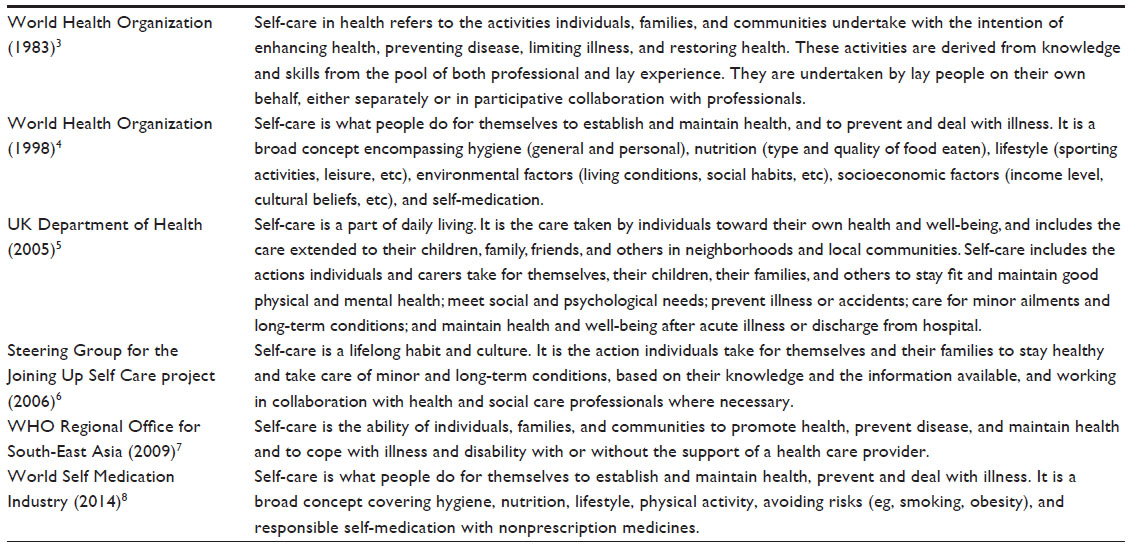 | Table 1 Definitions of self-care acknowledged in literature |
The increase of health care expenditures is a significant concern for Japan as well as other developed countries (eg, the US, Germany, and France); therefore, taking measures to prevent this increase is unavoidable: cutting prices, promoting generic use, and coverage reduction.9 In terms of pharmaceutical expenditures, Japan accounted for more than 750 billion US dollars of purchasing power parity per capita in 2013, the second largest consumption in the world9; hence, reducing drug cost was a highlighted domestic topic. The Japanese Cabinet believed that reclassifying drug use from prescription to over-the-counter (OTC) was a solution to cut costs because prescribers who have to pay prescription fees would choose inexpensive generic drugs instead of original drugs and patients could not buy reclassified drugs as inexpensively as generics.10 The use of generic or OTC drugs would ease the governmental financial burden, and the responsibility of OTC drugs users would increase simultaneously.
Furthermore, the industry strongly stresses the positive aspect of OTC drugs that are expected to provide immediate access to treatment. Moreover, self-care of self-recognizable and some chronic or recurrent conditions following initial medical diagnosis eliminate unnecessary visits to doctors. Therefore, the Japanese Cabinet policy encourages the industry and regulatory authority to take actions that accelerate OTC use and reclassification.11 An additional business issue is that the OTC industry would enjoy its economical consequence, whereas the prescription medicines and medical services industry would not.
Regarding self-care activities in Japan, comprehensive periodic health examinations have been part of the national effort to promote self-care. Employers are obliged to provide workers with health checkups as part of a program initiated in 1951 to prevent and detect tuberculosis.12 In addition, numerous local authorities have provided citizens with a health checkup program. After the 1998 WHO report,4 Japan anticipated an expansion of OTC drugs in self-medication, which was observed in other countries, such as the UK and the US.13 In addition to periodic health checkups and the health promotion program, the Japanese Cabinet recently suggested that the promotion of health and extending the healthy life expectancy could be achieved by using various resources, including “self-medication”,2 which is defined as “the treatment of minor ailments and assuming responsibility for one’s own self-health.”13 This focus differs slightly from the WHO’s definition of self-medication that refers to “the use of drugs to treat self-diagnosed disorders or symptoms or the intermittent or continued use of a prescribed drug for a chronic or recurrent disease or symptoms.”14
To accelerate self-care with OTC drugs, Japan began registering salespersons in 2009 to sell most OTC drugs, namely, medicines in the General Sale Risk Class (GSC) 2 and 3; without a pharmacist’s instructions, these drugs are “OTC”.15–17 A registered sales person is required to take some examinations to determine whether they understand the regulations and possess a basic knowledge of the products they sell; however, these examinations differ from those required for national licensing for health professionals, such as physicians and pharmacists. The GSC1 OTC medicines remain with the instructions of a pharmacist due to potential risk for users.16 In parallel, in 2008, a framework of the Pharmaceutical Society of Japan was implemented to accelerate reclassification that was used to propose drug candidates for reclassification from prescription to nonprescription to the Ministry of Health, Labour and Welfare (MHLW).18 This framework was reformed in 201519 as the MHLW was requested by the Cabinet to rebuild a process for reclassification to get wider opinions and make more switched drugs available.2 On the other hand, the majority of physicians in Japan expressed concern over the reclassification expansion because of the threat to users’ safety. Nonetheless, some physicians understood the positive economic effect that the widespread use of OTC drugs by individuals in their attempts to maintain their health would bring about.20 Public opinions have been scarce and need to be introduced to the debate.
Underpinned by the WHO definition of self-care,3,4 this study aimed to describe the new reclassification framework in Japan that was implemented in 2015 to understand the perspectives of physicians, negotiate these with Japanese public health needs, and examine Japanese nonprescription drugs provided under pharmacist supervision. The UK regulatory processes and OTC licenses were reviewed to accentuate Japan’s characteristics since both the UK and Japan have been active in drug reclassification in the past 10 years.21
Methods
This study reviewed Japan’s OTC regulatory framework and compared it with the UK’s framework by reviewing the implementation of self-care policies in both countries. Both Japan and the UK have actively approved the switch of some prescription medicines to an OTC classification this decade.21 The UK and Japan have innovative pharmaceutical companies that are regulated by an agency that oversees pharmaceuticals and medical devices. Furthermore, regulatory information is accessible in both countries, and the UK is an economic leader with a high gross domestic product similar to Japan. However, differences exist in the regulatory framework, health care system, and logistics for medicinal products between the countries. Germany and France were also considered because of the similarity of their health care system (social insurance), pharmaceutical circumstances (having innovative companies), and size of their pharmaceutical market (a share of gross domestic product)9; however, it was difficult to acquire sufficient regulatory information.
The MHLW’s web pages, including frameworks concerning OTC drugs,17,22,23 OTC drug sales, and reclassification regulations, were reviewed. Documents and websites referred to by these web pages were also included in our review.
Nonprescription drugs are mainly divided into two groups in both Japan and the UK: with supervision of a pharmacist or without. The Japanese reclassified medicinal products were identified using the Kyoto Encyclopedia of Genes and Genomes for OTC drugs: the latest risk-based category in Japan as of December 2014,24 the reclassification history as of February 2015,25 and the website information maintained by the MHLW in order to obtain the correct information.23 For the UK, the reclassification history provided by the Proprietary Association of Great Britain in January 201526 was used.
This study did not use human participants; therefore, ethical approval was not acquired.
Results
Regulations for OTC Sale
The UK Medicines Act of 1968 and the Council Directive 2001/83/EC (European Commission) regulate the sale and supply of medicines.27,28 These regulations refer to prescribed medicines as prescription-only medicines (POMs), while medicines provided by a pharmacy without a prescription but under the supervision of pharmacists are under the “P” classification. In addition, medicines sold in general retail outlets without a pharmacist’s supervision and listed for general sale are classified as General Sale List (GSL). The UK has a risk-based system in that medicines associated with the least amount of risk are classified as GSL, followed by P medicines, and finally POMs, which tend to be associated with the most risk.29 Internet sales are available for P and GSL when the Medicines and Healthcare products Regulatory Agency (MHRA) provides the pharmacy and the outlet the “European Union Internet logo”30 that was recently launched for display on medicines. This guidance was officially published for pharmacists, pharmacy technicians, and registered pharmacies in England, Scotland, and Wales in April 2015 by the General Pharmaceutical Council to instruct how to provide services at a distance, including over the Internet.31
Japanese regulations for OTC retail appear more complicated than those of the UK, and have a risk-based classification among nonprescription medicines (Table 2). They are regulated by The Pharmaceutical Affairs Act.32 Typically, the GSCs need to be assigned by the committee for drug safety at the MHLW at the time of approval, and the following new category was recently adopted for reclassified drugs. The nonprescription medicine category consisting of medicines available only on site through “face-to-face instructions by pharmacists” (Japan’s P) has been implemented since June 2014.33 Although this category is not identical to the UK’s P, it is similar. Following the relaxation of sales regulation in 2014, Internet websites can legally list all GSCs for sale. This triggered the initiation of Japan’s P for users’ safety. Reclassified drugs stay in Japan’s P for 3 years, and then they can be assigned as GSC1 for the 1-year period while the MHLW committee experts decide how to set the GSC for the switched OTC from a safety viewpoint. While P and GSL of a certain active moiety are separately licensed in the UK, Japan’s P is a type of “OTC” medicines intensively monitored by pharmacists and deemed to be a trial period for GSC. Online customers who want to buy GSC1 medicines must answer questions about their use of the product, and must receive pharmacists’ instructions through emails or on site, mimicking what retail customers must do. Similar to the POMs, the GSC1 medicines also require the provision of mandatory instructions by pharmacists; however, some sale locations were noncompliant. This issue was discovered based on a report from a research company to the MHLW, which stated that some pharmacies and retail stores sold Japan’s P and GSC1 medicines with insufficient instructions.34
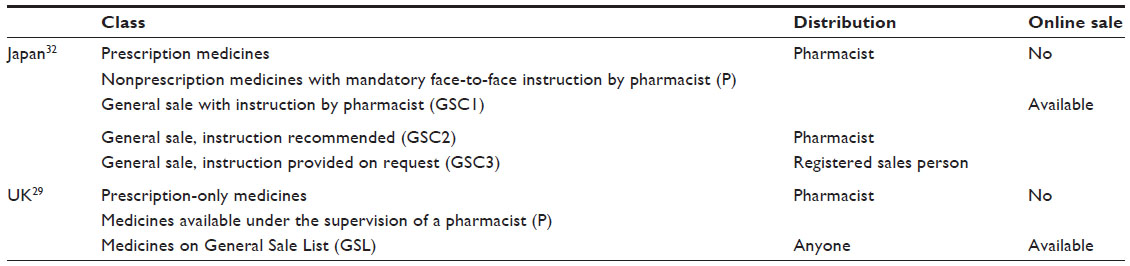 | Table 2 Type of nonprescription medicines in UK and Japan |
Reclassification processes in Japan
The UK and Japan support the safe use of nonprescription medicines if the adverse reactions of the medicines are deemed acceptable at the time of reclassifying, are minor/moderate, and occur within a reasonable period in the market as prescription medicine.13,27 When switching from prescription to OTC medicine, information on the safety and efficacy of the active substance from clinical trials must be reviewed. The European Commission makes decisions about products through their Centralized Procedure29 while the European Medicines Agency reviews product reclassification applications. In addition, the MHRA reviews dossiers and approves P and GSL medicines in the UK, which amended its regulations in 2002 to adopt the approach implemented by other European Union countries. The MHRA initiated a risk management plan (Figure 1A) and accelerated the reclassification of medicines in 2012.27
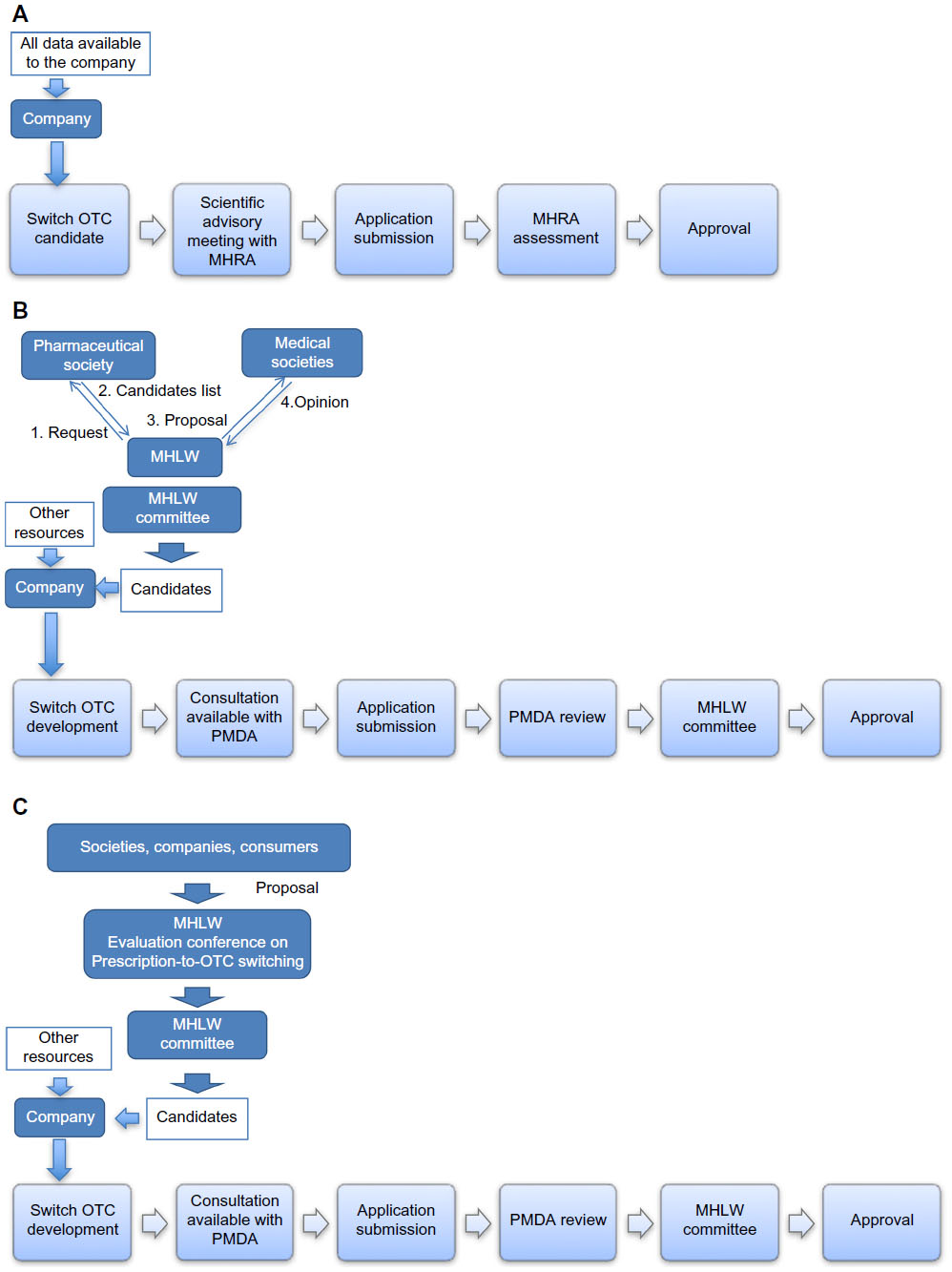 | Figure 1 Approval processes in the UK and Japan. |
In Japan, the Pharmaceuticals and Medical Devices Agency reviews the GSC and Japan’s P medicine applications of companies prior to approval by the minister of the MHLW. In 2005, the MHLW proposed a classification system for the general sale of medicines and in 2008, initiated a strategy to list candidate substances for reclassification by pharmaceutical experts to encourage new OTC approvals (Figure 1B). Although this strategy worked only thrice in 2008, 2009, and 2010,35 it has been used in Japan to approve five candidates: cetirizine (2012), ebastine (2014), icosapent ethyl (2013), loxoprofen sodium hydrate (2011), and pemirolast potassium (2012). On the other hand, 16 unlisted substances were also reclassified and launched between 2008 and 2014. Therefore, the system required improvement, and the MHLW has since set up a new framework involving a public hearing with companies, consumers, and academic experts (Figure 1C).36 In other words, the inclusion of diverse opinions other than those of the pharmaceutical academia was critical for Japan to change the process of identifying candidate prescription medicines for reclassification as OTCs. In principle, Japan’s P medicines are routinely reclassified as GSC1 3 years after their initial launch, and then they are reviewed by the MHLW for assignment to the risk class the following year.22 This means that Japan’s P products change periodically, depending on their launch date.
Examples of recent reclassifications
The POM to P switch history in the UK listed 106 active ingredients with route of administration, while 89 were listed in Japan, and 28 substances overlapped in the reclassification from prescription medicines to OTCs. Among the 28 substances, the results of only one of Japan’s P (cetirizine hydrochloride) and 12 GSC1 medicines (acyclovir, cimetidine, clotrimazole, famotidine, isoconazole nitrate, miconazole nitrate, minoxidil, nicotine [gum], nicotine [patch], nizatidine, ranitidine hydrochloride, and tranexamic acid) indicated that the Japanese regulations required fewer medicines to be supervised by Japanese pharmacists. Furthermore, as of January 2015, among 12 of Japan’s P substances (acitazanolast hydrate, alminoprofen, antistax [vine leaf extracts], cetirizine hydrochloride, chaste berry extract, ebastine, fexofenadine hydrochloride, icosapent ethyl, tranilast [eye drops], trimebutine maleate, neticonazole hydrochloride, and pemirolast potassium), only cetirizine hydrochloride was switched in the UK. Among the 20 GSC1 substances that were switched and launched before 2012, eight were not approved in the UK as of January 2015 (Table 3).
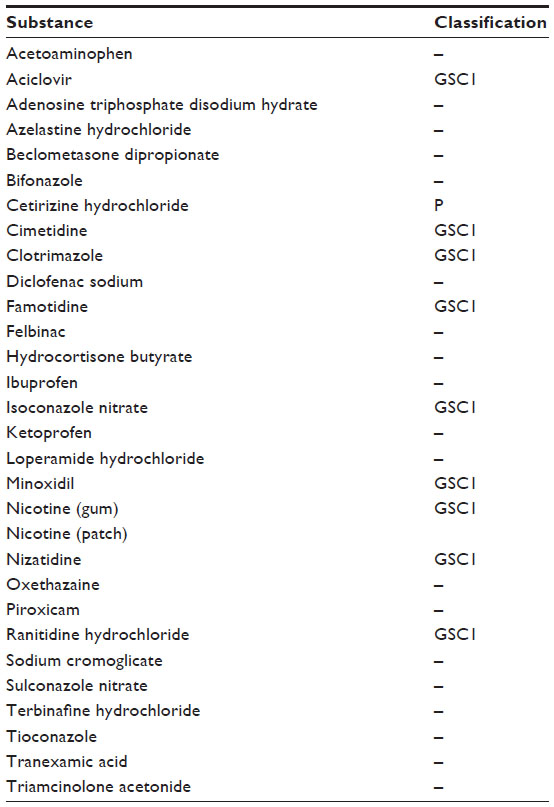 | Table 3 The list of substances reclassified from nonprescription medicines to pharmacy or general sale medicines commonly in the UK and Japan, from 1983 to January 2015 |
The types of medicines available in the UK are broader than in Japan, not limited to the treatments for just acute self-limiting ailments, including simvastatin, tamsulosin, and orlistat. In terms of significant changes in the last 10–15 years, the UK now has two antibiotics (topical chloramphenicol for acute bacterial conjunctivitis and oral azithromycin for asymptomatic chlamydia), various proton pump inhibitors (omeprazole, rabeprazole, pantoprazole, and esomeprazole), a cholesterol-lowering medicine (simvastatin), orlistat for weight loss, tranexamic acid for menorrhagia, tamsulosin for benign prostatic hypertrophy, and a triptan (sumatriptan) for migraine. Most recently, in 2015, ulipristal acetate was reclassified as an emergency contraception as an additional option to levonorgestrel. Japan has some corticosteroids (betamethasone, dexamethasone, fluocinolone acetonide, hydrocortisone, and prednisolone) as OTC products for intranasal use for rhinitis and topical use with limited indications (eg, anti-itch and atopic dermatitis), while the UK has intranasal corticosteroids for rhinitis, topical corticosteroids for dermatitis/insect bites, and hydrocortisone pellets for mouth ulcers.
No medicines have been reclassified to POM in Japan yet; however, one company quit selling a reclassified Japan’s P (ethyl icosapentate37) because they could not complete the surveillance requested by the MHLW. The approval of ethyl icosapentate, the antihyperlipidemic OTC in 2013, caused tremendous controversy from the Japan Medical Association38 because medicines for lifestyle-related diseases require doctors’ supervision. Even though safety concerns are carefully discussed at the time of approval, a safety issue postapproval is to be reviewed when necessary. In Japan, there is no legal restriction for package size; however, it is reviewed in the approval process.
The UK reclassified omeprazole and simvastatin (10 mg each), in 2003 and 2005, respectively, changing their reclassification indications from acute, short-term, and self-recognized conditions to chronic or recurrent disease management. The results of studies on these OTC statins were controversial in medical articles39 and the US rejected the OTC application of Lovastatin (20 mg) in January 2005 because of safety concerns. The MHLW committee has not approved or listed any statin as a candidate substance.
The UK has had two recent reclassifications return to POM (domperidone40 and oral diclofenac41) due to cardiac risks. Moreover, they have increased the pack size restrictions now for misused medicines (eg, codeine, dihydrocodeine, pseudoephedrine, and ephedrine). One of the most controversial switches was tamsulosin, due to a risk of delaying/masking prostate cancer. If the patient receives tamsulosin as a P medicine, The Commission of Human Medicines in UK advises the patient to respond to a questionnaire, a doctor’s diagnosis of benign prostatic hypertrophy, and a subsequent annual review.42 This scheme is similar to the protocol for ethyl icosapentate in Japan. Another example of a safety concern in the UK concerns chloramphenicol. The MHRA said there was no evidence that making chloramphenicol available OTC would lead to more antibiotic resistance; however, the British Medical Association expressed concerns about giving the P medicine by pharmacists and increasing problems of antibiotic resistance in community.43
Discussion
Our comparison of the UK and Japanese systems confirmed that medicinally active ingredients in OTC drugs have different categories in different societies. There are OTC drugs approved only in Japan, and vice versa. The notable difference is that the UK introduced OTC drugs not just for acute self-limiting ailments, but also long-term management. It is expedient to consider the case of ethyl icosapentate in Japan where the old framework was not successful in inviting stakeholders, and did not efficiently approve a new reclassification of OTC drugs. One explanation for this situation is an insufficient valid statement on self-medication and reclassification by the regulatory authority, other than its interim report on the general sale of medicines for self-medication by the MHLW’s expert panel in 2002 (not finalized).13 Many medical professionals, encouraging people’s self-care, untruthfully looked at such self-medication policy and reclassification candidates. Successful launch of a P medicine would require the consensus among stakeholders on what kinds of medicines are suitable for reclassification. Regarding ethyl icosapentate, following the Japan Medical Association’s request, the MHLW revised the user’s checklist and made it available only following a previous doctor’s visit. This approach is analogous to the UK’s approach to prescribed OTC drugs.
It would be valuable to highlight points-to-consider for the reformation process. First, a few prescription drug candidates for OTC drugs were placed on the market, while more than ten noncandidates were approved by the MHLW from 2008 to 2014. The new working group for switching prescriptions to OTC drugs should focus on the needs of the populace and feasibility of the process. Second, the medical societies and physicians group had not been involved in the direct discussions on the candidates proposed by the pharmacists group. As seen in the controversy with ethyl icosapentate, medical professionals have opinions. The inclusion of clinical insights in the proposed new framework would help determine the medicines that should be available for self-care from medical professionals’ perspectives. Third, the opinions of individuals who use OTC drugs should be included and effectively implemented. Finally, it is necessary to publicize the discussions on the reclassification of candidate drugs. Discussions were closed previously; however, openness and transparency would encourage experts to build a better consensus in the future. The new framework is expected to work better.
In self-care, people are held responsible for their own cost and health care management. How to empower people to properly choose and use OTC drugs is a concern for self-care, which is also guided by the regulatory authority in general. To promote self-care with OTC drugs, medicines with proven efficacy, safety, and quality should be used as instructed and reclassified substances are no exception. When reclassifying from prescription medicines to a nonprescription status, we must consider safety, delays in seeking treatment for serious conditions, and the emergence of drug resistance.1 Strategies for avoiding adverse drug reactions and pharmacovigilance are essential for nonprescription medicines, and they might require information unique to self-use. One option is Japan’s P or GSC1 medicine distribution by pharmacists to control the proper use of nonprescription medicines that are not considered sufficiently safe for selection based on self-judgment. Another approach to promote safe use of medicines could be the backwards process to withdraw an OTC drug and keep it within prescription medicines; however, this was not mentioned clearly in Japan. The lack of evidence surrounding some products’ effectiveness (eg, serrapeptase44 in Japan) led to withdrawal from the market, safety concerns leading to reclassification back to POM (eg, domperidone45 and oral diclofenac46 in the UK), and other issues, such as misuse/abuse. This potential has resulted in changes to practice (eg, codeine use in children, cough and cold products in children). There may be more concerns in the postauthorization phase from scientific, regulatory, and social viewpoints (eg, substances less suitable for nonprescription and setting medicines categories to fit daily activities). To monitor OTC drugs as such, the UK Risk Management Plan has been implemented for the P medicines since 2012,27 which suggests that a risk–benefit analysis by the regulatory authority and the stakeholders responsible for marketing might be an option for instituting safety measures. This might be another option for the future. A national logo for display on the Internet would be useful and make it easy to find whether the website is operated by the pharmacy and acknowledged by the regulatory authority. To date, Japan has not implemented such a system; however, it is advisable to watch how the UK approach works. Both Japan and the UK have applied limited indications, smaller package sizes, and subsequent visits to a doctor for some OTC drugs.
We noticed that the concept of self-care/self-medication differed. Health policymakers are required to maintain and improve health care systems while considering determinants of health, such as health care use, lifestyles, and support from community health care professionals as well as OTC drug use. They should facilitate consensus building among community members, including encouraging collaboration between pharmacies/drug stores and general practitioners/medical facilities, which is inevitable if the policy of OTC use is to succeed. Self-medication and the safe use of OTC medicines should be regulated and guided in this self-care and regional context. In a report regarding its citizens, the Cabinet of Japan stated, “individuals tend to have little incentive to continuously prevent disease and manage their health, such as diet control, exercise, etc. when they are healthy.”2 However, the interim report by the MHLW stated the increase of those who care about their health.13 In contrast, the WHO has suggested that the effective promotion of good health practices and determinants of health are influenced by characteristics and behaviors as well as the social, economic, and physical environment of individuals.47,48 The World Self-Medication Industry recently encouraged the use of OTC drugs in self-care49; however, decision-makers in health policy need to consider that the role of nonprescription medicines varies among countries due to public health factors and the value placed on social, medical, and scientific evidence. Like the UK, the restrictive product marketing authorizations or selling licenses should be considered to make some OTC products only an option for a minority of patients and a time-consuming consultation, to promote safe use of responsible OTC drugs.
The influence of reclassification on consumer behavior in the UK was evident when the government empowered individuals to control their own health care, and sales of OTC drugs for self-medication still declined slightly from 2008 to 2010.50 Instead, the use of prescribed OTC drugs increased because they were cheaper. In addition, this increase was thought to be associated with the economic crisis, and the economic status of the UK strongly correlated with the living conditions of the populace (eg, unemployment) as well as their interest in paying for OTC medications.50 People would not pay for OTC drugs when they could get prescription medicines cheaper. Therefore, it is difficult to say that increased reclassification contributed to improving individual and regional health and reducing health care cost, although the UK approved numerous P and GSL drugs.
The situation is similar in Japan where although the reclassification of some prescription medicines as OTC drugs was approved, the OTC market volume of the country shrank from 800 billion yen in 2000 to 650 billion yen in 2011.51 Furthermore, a slight decline in the market continued in 2012 and 2013.52 Then, the industry set a goal for 2014 to create a new OTC market that would potentially produce over 1,000 billion yen as a result of reducing health care cost by the use of OTC medications. However, no blueprint for collaboration among community stakeholders has been presented. Whereas, we assume that the reduction in OTC consumption by Japanese consumers would continue, even if more switched drugs were approved.
OTC medicines can be used to treat self-recognized ill health. Moreover, healthy individuals should institute different measures and activities, such as diet and exercise, to remain in good health. Additionally, the majority of health care consumers in Japan are the elderly who typically require medical treatment by a physician rather than self-medication. Although it is recognized that information on the primary care activities in Japan is scarce,53 the Japanese system as well as the system in France and the UK requires patients to pay lower costs from their pockets. Therefore, the elderly people and lower-income families would not use OTC drugs but continue medical visits. Another aspect is that Japan, France, and Germany have a combination of health insurance and health care expenditure tax. They have a relatively low private share of pharmaceutical spending (25%~30%) compared to the US and Canada (over 60%) where the payment system is typically private and uses a social insurance program for health care costs.9 Activities in France and Germany seem to be informative for the Japanese system.
Limitations
This study focused on comparing the regulatory frameworks of Japan and the UK only. It is not necessary to make the same OTC drugs available throughout all countries; however, it is useful to include information from various countries. Moreover, the difference in health care systems between both countries was not fully assessed. Furthermore, the situation in developing countries where prescription medicines are scarce needs to be discussed and investigated from different viewpoints.
Conclusion
Japan has operated OTC medicines with mandatory pharmacists’ supervision and GSC1 and Japan’s P since 2009 and 2014, respectively. Japan initiated the reformation of the reclassification system in 2015 to promote nonprescription approval and will have the first meeting in the first quarter of 2016. This will include the opinions of physicians and the public directly in the process. It is expected that the opinion of marketers, medical professionals, and the public will meaningfully contribute to the discussion regarding the safe use of drugs. Monitoring the new system will be noteworthy to see if OTC drug users manage self-care properly and visit the doctor only when necessary. The supply methods are similar in Japan and the UK; however, the growth in the Japanese OTC market through reclassification expected by the Cabinet and the industry is still uncertain.
Acknowledgments
We would like to thank Mr Takahiro Inoue at the MHLW for advice on the Japanese regulatory framework, and Editage (www.editage.jp) for English language editing. The part of this research regarding reclassified substances in the UK and Japan is a reformed version of Yuki Kitagawa’s report that was initially conducted during an undergraduate program and reported in Japanese to the Faculty of Pharmacy, Musashino University. Moreover, her research was originally planned and conducted using OTC lists generated by the MHRA for the UK, which are not available now.54 There was no financial support from any grant.
Disclosure
The authors report no conflicts of interest in this work.
References
National Institute on Aging, World Health Organization. Global Health and Aging; 2011. Available from: https://d2cauhfh6h4x0p.cloudfront.net/s3fs-public/global_health_and_aging.pdf. Accessed December 20, 2015. | |
Prime Minister of Japan and His Cabinet. Japan Revitalization Strategy; June 14, 2013. Available from: https://www.kantei.go.jp/jp/singi/keizaisaisei/pdf/en_saikou_jpn_hon.pdf. Accessed December 20, 2015. | |
World Health Organization. Health Education in Self-Care: Possibilities and Limitations (Report of a Scientific Consultation). Geneva, Switzerland; November 21–25, 1983. | |
World Health Organization. The Role of the Pharmacists in Self-Care and Self-Medication: Report of the 4th WHO Consultative Group on the Role of the Pharmacist. WHO/DAP/98.13. The Hague, The Netherlands; August 26–28, 1998. Available from: http://apps.who.int/iris/bitstream/10665/65860/1/WHO_DAP_98.13.pdf. Accessed July 5, 2015. | |
UK Department of Health. Self-Care – A Real Choice; 2005. Available from: http://webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4101702.pdf. Accessed 20 June 2016. | |
Steering Group for the Joining Up Self Care Project. Joining Up Self-Care in the NHS; 2006. Available from: http://www.selfcareforum.org/wp-content/uploads/2011/07/JUSCFullReport.pdf. Accessed December 20, 2015. | |
World Health Organization Regional Office for South-East Asia. Self-Care in the Context of Primary Health Care: Report of the Regional Consultation Bangkok, Thailand, January 7–9, 2009; India; 2009. Available from: http://apps.searo.who.int/PDS_DOCS/B4301.pdf. Accessed December 20, 2015. | |
World Self Medication Industry (WSMI). The Story of Self-Care and Self-Medication: 40 Years of Progress, 1970–2010. Available from: http://www.wsmi.org/wp-content/data/pdf/storyofselfcare_brochure.pdf. Accessed December 20, 2015. | |
Organisation for Economic Co-Operation and Development. Health at a Glance 2015. Paris, France: OECD Publishing; 2015. | |
Cabinet Office, Government of Japan. Basic Policies for the Economic and Fiscal Management and Reform 2014; June 24, 2014. Available from: http://www5.cao.go.jp/keizai-shimon/kaigi/cabinet/2014/2014_basicpolicies_02.pdf. Accessed December 20, 2015. | |
Cabinet Office, Government of Japan. Regulatory Reform Implementation Plan [in Japanese]; June 30, 2015. Available from: http://www8.cao.go.jp/kisei-kaikaku/kaigi/publication/150630/item1.pdf. Accessed December 20, 2015. | |
Ministry of Health, Labour and Welfare. [Annual Report on Health and Welfare]; 2014. Available from: http://www.mhlw.go.jp/wp/hakusyo/kousei/14/. Accessed July 5, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. [The Interim Report by the Meeting on Rationalizing OTC Approval]; 2002. Available from: http://www.mhlw.go.jp/shingi/2002/11/s1108-4.html. Accessed July 5, 2015. Japanese. | |
World Health Organization. Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication; 2000. Available from: http://apps.who.int/medicinedocs/en/d/Js2218e/. Accessed July 5, 2015. | |
Ministry of Health, Labour and Welfare. [Designation of Over-the-Counter Drugs Classes: Notification of Pharmaceutical and Medical Safety Bureau No. 0330037]; March 30, 2007. Available from: http://www.mhlw.go.jp/bunya/iyakuhin/ippanyou/pdf/a.pdf. Accessed December 20, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. Section 10 Promotion of Measures for Safety and Security of People. In White Papers and Reports Annual Health, Labour and Welfare Report 2009–2010; 2011. Available from: http://www.mhlw.go.jp/english/wp/wp-hw4/dl/honbun/2_2_10.pdf. Accessed December 20, 2015. | |
Ministry of Health, Labour and Welfare. [OTC Medicines Sales System]. Available from: http://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/iyakuhin/ippanyou/index.html. Accessed July 5, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. [OTC Committee Proceedings]; March 22, 2007. Available from: http://www.mhlw.go.jp/shingi/2007/03/txt/s0322-6.txt. Accessed December 20, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. [OTC Committee Proceedings]; May 29, 2015. Available from: http://www.mhlw.go.jp/stf/shingi2/0000097160.html. Accessed December 20, 2015. Japanese. | |
Maeda Y, Yoshida S. Survey on drugs and diagnostic test kits available without prescription. Japan Medical Association Research Institute working paper No. 318; June 8, 2014. Available from: http://www.jmari.med.or.jp/download/WP318.pdf. Accessed December 20, 2015. | |
Gauld NJ, Kelly FS, Kurosawa N, Bryant LJ, Emmerton LM, Buetow SA. Widening consumer access to medicines through switching medicines to non-prescription: A six country comparison. PLoS One. 2014;9(9): e107726. Available from: http://www.plosone.org/article/fetchObject.action?uri=info:doi/10.1371/journal.pone.0107726&representation=PDF. Accessed July 5, 2015. | |
Ministry of Health, Labour and Welfare. Over-the-Counter Medicines Website. Available from: http://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000092787.html. Accessed December 20, 2015. | |
Ministry of Health, Labour and Welfare. Ministry of Health, Labour and Welfare Database of Laws, Ministerial Ordinances and Notifications. Available from: http://wwwhourei.mhlw.go.jp/hourei/. Accessed December 20, 2015. | |
KEGG Drug. Risk Category of Japanese OTC Drugs; December 2014. Available from: http://www.kegg.jp/kegg-bin/get_htext?br08312.keg. Accessed July 5, 2015. | |
KEGG Drug. Rx-to-OTC Switch List in Japan; February 2015. Available from: http://www.kegg.jp/kegg/drug/br08314.html. Accessed July 5, 2015. | |
Proprietary Association of Great Britain. Promoting Responsible Consumer Health POM-P Switches. Available from: http://www.pagb.co.uk/regulatory/pdfs/pomtoplist.pdf. Accessed July 5, 2015. | |
Medicines and Healthcare Products Regulatory Agency. How to Change the Legal Classification of a Medicine in the UK; 2012. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/277307/Legal_classification_changes.pdf. Accessed July 5, 2015. | |
European Commission. A Guideline on Changing the Classification for the Supply of a Medicinal Product for Human Use. Brussels, Belgium; 2006. Available from: http://www.it-asso.com/gxp/eudralex_v27/contents/vol-2/c/switchguide_160106.pdf. Accessed July 5, 2015. | |
Medicines and Healthcare Products Regulatory Agency. Medicines: Reclassify Your Product; December 18, 2014. Available from: https://www.gov.uk/guidance/medicines-reclassify-your-product. Accessed December 20, 2015. | |
Medicines and Healthcare Products Regulatory Agency. Register for the EU Common Logo; June 16, 2015. Available from: https://www.gov.uk/guidance/register-for-the-eu-common-logo. Accessed December 20, 2015. | |
General Pharmaceutical Council. Guidance for Registered Pharmacies Providing Pharmacy Services at a Distance, Including on the Internet. London; 2015. Available from: http://www.pharmacyregulation.org/sites/default/files/guidance_for_registered_pharmacies_on_distance_and_internet_services_.pdf. Accessed December 20, 2015. | |
Ministry of Internal Affairs and Communications. [The Pharmaceutical Affairs Law, Act No. 145 of 1960. 10 August 1960]. Available from http://law.e-gov.go.jp/htmldata/S35/S35HO145.html. Accessed 5 May 2016. Japanese. | |
Ministry of Health, Labour and Welfare. OTC Internet Sale; July 2014. Available from: http://www.mhlw.go.jp/file/06-Seisakujouhou-11120000-Iyakushokuhinkyoku/sinseido.pdf. Accessed December 20, 2015. | |
Softbrain Field Co, Ltd. [Pharmaceutical Sales System Actual Conditions Survey FY2014]; May 1, 2015. Available from: http://www.mhlw.go.jp/file/06-Seisakujouhou-11120000-Iyakushokuhinkyoku/houkoku26_2.pdf. Accessed September 5, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. [The Candidate Substance Considered to be Also Available as OTC Drugs Out of the Active Ingredient of Prescription]; April 11, 2011. Available from: http://www.mhlw.go.jp/stf/houdou/2r98520000018qzd.html. Accessed July 5, 2015. Japanese. | |
Ministry of Health, Labour and Welfare. [The Assessment System for Substances Possibly Switched from Prescription Medicines]; June 25, 2015. Available from: http://www.mhlw.go.jp/file/05-Shingikai-11121000-Iyakushokuhinkyoku-Soumuka/0000089801.pdf. Accessed July 5, 2015. Japanese. | |
Nomura K. [Epaarute, OTC of Epadel, Discontinued]. NIKKEI Drug Information; September 26, 2014. Available from: http://medical.nikkeibp.co.jp/leaf/mem/pub/di/trend/201409/538576.html. Accessed December 20, 2015. Japanese. | |
Japan Medical Association. [Epadeal Switched to OTC. Regular Press Conference on 9 January 2013]. Available from: http://www.med.or.jp/nichinews/n250120e.html. Accessed July 5, 2015. Japanese. | |
Abrams J. Over-the-counter statins: A new controversy. Nat Clin Pract Cardiovasc Med. 2005;2(4):174–175. | |
Medicines and Healthcare Products Regulatory Agency. Domperidone: No Longer Available Without Prescription; September 25, 2014. Available from: https://www.gov.uk/drug-safety-update/domperidone-no-longer-available-without-prescription. Accessed December 20, 2015. | |
Medicines and Healthcare Products Regulatory Agency. Diclofenac Tablets Now only Available as a Prescription Medicine; January 14, 2015. Available from: https://www.gov.uk/government/news/diclofenac-tablets-now-only-available-as-a-prescription-medicine. Accessed December 20, 2015. | |
Medicines and Healthcare Products Regulatory Agency. FLOMAX RELIEF MR (PL 00015/0280) UKPAR. Available from: http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con068200.pdf. Accessed December 20, 2015. | |
BBC News. Pharmacy Antibiotic Sale Go-Ahead; June 8, 2008. Available from: http://news.bbc.co.uk/2/hi/health/4072314.stm. Accessed December 20, 2015. | |
Takeda Pharmaceutical Company Limited. Recall of Anti-Inflammatory Enzyme Product “Dazen”; February 21, 2011. Available from: http://www.takeda.co.jp/news/2011/20110221_4752.html. Accessed December 20, 2015. | |
Medicines and Healthcare Products Regulatory Agency. Pseudoephedrine and Ephedrine: Nasal Decongestants; September 1, 2009. https://www.gov.uk/drug-safety-update/pseudoephedrine-and-ephedrine-nasal-decongestants. Accessed December 20, 2015. | |
Medicines and Healthcare Products Regulatory Agency. Codeine for Cough and Cold: Restricted Use in Children; April 29, 2015. https://www.gov.uk/drug-safety-update/codeine-for-cough-and-cold-restricted-use-in-children. Accessed December 20, 2015. | |
World Health Organization. Global Programme on Health Promotion Effectiveness. Available from: http://www.who.int/healthpromotion/areas/gphpe/en/. Accessed July 5, 2015. | |
World Health Organization. The Determinants of Health. Available from: http://www.who.int/hia/evidence/doh/en/. Accessed July 5, 2015. | |
World Self-Medication Industry. The Shanghai Declaration – on International Self-Care Day; July 24, 2012. Available from: http://www.wsmi.org/wp-content/data/pdf/INTLSELFCARE_DAYS/TheShanghaiDeclaration.pdf. Accessed July 5, 2015. | |
Intercontinental Marketing Services Health. Prescribed OTC Sector Buoyant in UK. OTC Bulletin; 2011. Available from: https://www.imshealth.com/ims/Global/Content/Corporate/Press%20Room/OTCbulletin.pdf. Accessed July 5, 2015. | |
Ministry of Health, Labour and Welfare. [Vision of the Pharmaceutical Industry]; 2013. Available from: http://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/iryou/shinkou/dl/vision_2013b.pdf. Accessed July 5, 2015. Japanese. | |
Yano Research Institute Ltd. [The Survey Results 2014 on the OTC Market]; October 17, 2014. Available from: https://www.yano.co.jp/press/pdf/1312.pdf. Accessed July 5, 2015. Japanese. | |
Organisation for Economic Co-Operation and Development. Reviews of Health Care Quality. Japan; November 5, 2014. Available from: http://www.oecd.org/els/health-systems/ReviewofHealthCareQualityJAPAN_ExecutiveSummary.pdf. Accessed July 5, 2015. | |
Medicines and Healthcare Products Regulatory Agency. List of Substances. Available from: http://webarchive.nationalarchives.gov.uk/20141205150130/http://www.mhra.gov.uk/Howweregulate/Medicines/Licensingofmedicines/Legalstatusandreclassification/Listsofsubstances/index.htm. Accessed July 5, 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.