")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Medication Profile and Treatment Cost Estimation Among Outpatients with Schizophrenia, Bipolar Disorder, Depression, and Anxiety Disorders in Indonesia
Authors Puspitasari IM , Sinuraya RK , Rahayu C, Witriani W , Zannah U, Hafifah A, Ningtyas AR, Vildayanti H
Received 27 November 2019
Accepted for publication 10 March 2020
Published 26 March 2020 Volume 2020:16 Pages 815—828
DOI https://doi.org/10.2147/NDT.S240058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Irma M Puspitasari,1,2,* Rano K Sinuraya,1,2,* Cherry Rahayu,3 Witriani Witriani,4 Uzlifatul Zannah,1 Auliani Hafifah,1 Ajeng R Ningtyas,1 Hilda Vildayanti1
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Center of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 3Hasan Sadikin General Hospital, Bandung, Indonesia; 4Faculty of Psychology, Universitas Padjadjaran, Jatinangor, Indonesia
*These authors contributed equally to this work
Correspondence: Irma M Puspitasari
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jalan Bandung Sumedang KM 21, Sumedang, West Java, Jatinangor 45363, Indonesia
Tel +62 22 84288888 (Ext 3510)
Email [email protected]
Purpose: The present retrospective study aimed to determine the medication profile and estimate the treatment costs from medical records of new outpatients with schizophrenia, bipolar disorder, depression, and anxiety disorders from a healthcare perspective at a national referral hospital in Indonesia from 2016 to 2018.
Methods: Medical records (including medical and administrative data) of 357 new outpatients with schizophrenia, bipolar disorder, depression, or anxiety disorders were collected from the hospital information system. The records of new outpatients with schizophrenia, bipolar disorder, depression, or anxiety disorders aged > 18 years and had only received drugs for treatment were included. The medication profile was descriptively assessed, and estimated costs were calculated based on direct costs from a healthcare perspective.
Results: Overall, 173 medical records were further analyzed. The main drugs administered to the new outpatients were atypical and typical antipsychotics for schizophrenia, atypical antipsychotics and mood stabilizers for bipolar disorder, antidepressants and atypical antipsychotics for depression, and antidepressants and benzodiazepines for anxiety disorders. The average annual treatment costs per patient were IDR 3,307,931 (USD 236) for schizophrenia, IDR 17,978,865 (USD 1,284) for bipolar disorder, IDR 1,601,850 (USD 114) for depression, and IDR 1,190,563 (USD 85) for anxiety disorders.
Conclusion: The most commonly prescribed drugs for schizophrenia were haloperidol and risperidone; for bipolar disorders, sodium divalproex and risperidone; for depression, fluoxetine and sertraline; and for anxiety disorders, sertraline and lorazepam. Considering the high prevalence and estimated treatment costs for mental disorders, special attention is required to prevent an increase in their prevalence in Indonesia.
Keywords: schizophrenia, bipolar disorder, depression, anxiety disorders, medication profile, cost estimation
Introduction
According to the World Health Organization, one in four individuals globally will be affected by mental or neurological disorders at some point in their lives.1 In 2018, the psychiatric disorders with the highest prevalence worldwide were depression (300 million individuals), bipolar disorder (60 million individuals), and schizophrenia and other psychoses (23 million individuals).2 As of August 2018, Indonesia’s population aged >15 years included approximately 194 million individuals,3 and in 2017 there were 67 million households.4 The prevalence of schizophrenia in individuals aged >15 years according to basic health research (RISKESDAS) from the Ministry of Health, Indonesia, in 2018 was 7°/oo (7 of 1000 households have a member with schizophrenia, corresponding to approximately 470,000 individuals), and the prevalence of mental–emotional disorders including bipolar disorder, depression, and anxiety disorders was 9.8% (approximately 19 million).5 Among this 9.8% of mental–emotional disorders, the prevalence of depression was 6.1% (approximately 11.8 million individuals).5
Schizophrenia is a complex psychiatric disorder characterized by changes in inappropriate behavior, chaotic thought patterns, delusion, hallucination, and psychosocial dysfunction.6 Antipsychotics are the main choice for schizophrenia therapy, and they are divided into typical and atypical antipsychotics.6 According to the American Psychiatric Association, typical and atypical antipsychotics other than clozapine are recommended for the treatment of acute phase schizophrenia.7 The choice of antipsychotics is influenced by several factors, such as side effects and cost.7,8 Cognitive behavioral therapy (CBT) was one of the first non-pharmacological interventions included in the treatment guidelines for schizophrenia.9 CBT is an intervention that helps modify undesirable thought patterns, feelings, and behavior. Moreover, CBT is useful in reducing disorganized behavior, which affects daily life in individuals with schizophrenia.9
Bipolar disorder is a mood disorder characterized by episodes of mania or hypomania that appear alternately or concurrent with depressive episodes.10 Treatment for bipolar disorder typically focuses on acute stabilization, with the aim of improving the symptoms of mania or depression in a patient, thereby enabling a stable mood (euthymia) to be achieved.11 The maintenance phase aims to prevent relapse, reduce subthreshold symptoms, improve social functioning, and reduce suicide risk and mood instability-related risk.11,12 The main therapies for episodes of mania in bipolar disorder are mood stabilizers, antipsychotic agents, or a combination of both agents, whereas the therapies for depressive episodes are mood stabilizers and certain antipsychotics.13 Antidepressants can be used with mood stabilizers to reduce the risk of mood change to mania or can be used after a patient fails to respond to mood stabilizer therapy.13 Non-pharmacological therapies, such as short-term psychotherapies, offer fairly consistent benefits to patients with bipolar disorder as an adjunctive therapy.14 CBT, family-focused therapy, and psychoeducation offer the most robust efficacy in terms of relapse prevention.14
Depression is a mental illness characterized by decreased mood, loss of interest, guilty feelings, decreased appetite, disturbed sleep, and low concentration.15 Depressive disorders are typically treated with antidepressants, psychotherapy, or a combination of both.16 There are four groups of antidepressants as follows: selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), monoamine oxidase inhibitors (MAOIs), and tricyclic antidepressants (TCAs) and other heterocyclic agents.17,18 A systematic review published in 2017 revealed that in contrast to pharmacological treatment, most non-pharmacological interventions for treating patients with major depressive disorder are not evidence-based.19 On the other hand, exercise therapy, bibliotherapy, CBT, short-term psychodynamic supportive psychotherapy, and interpersonal psychotherapy (IPT) are considered valid non-pharmacological treatments for adult patients with mild or moderate depression in Korea.20
Anxiety disorders involve excessive fear and are irrational.21 They are considered the most common psychiatric disorders, particularly in developed countries, and are characterized by physical symptoms, such as fatigue.22 Therapy for anxiety disorder aims to prevent recurrence and improve the quality of life of patients.23 The suggested first-line therapy includes a single SSRI or SNRI.24 These drugs are effective for reducing anxiety symptoms according to randomized controlled trials.25 TCAs are another drug choice; however, these drugs are rarely used owing to increased side effects and mortality risk associated with overdose.26,27 CBT has been proven to be effective as a non-pharmacological therapy for anxiety disorders.28
The burden of disease (BOD), also known as the cost of illness (COI), encompasses various aspects of the disease impact on the health outcomes in a country, specific regions, communities, and even individuals.29 COI studies traditionally stratify costs into three categories: direct, indirect, and intangible costs.29 Direct costs most often refer to the “visible costs” associated with diagnosis and treatment in the healthcare system, such as those related to medication, physician visits, psychotherapy sessions, and hospitalization. Indirect costs refer to the “invisible costs” associated with income losses due to mortality, disability, and care seeking, including productivity losses due to work absence or early retirement.30 COI studies can be performed from various perspectives, such as determining costs to society, the healthcare system, third-party payers, business sectors, the government, and the participants and their families.29 From a healthcare perspective, only medical costs are included in such studies.29
Mental health disorders are some of the main causes of the overall disease burden worldwide.31 Approximately one-third of the BOD of mental health is associated with productivity losses, including those related to unemployment, disability, and low work performance.32 According to the World Economic Forum in 2011, the economic burden of psychiatric disorders in 2010 was estimated at USD 2.5 trillion, and it is expected to increase to USD 6 trillion by 2030.30,33 In 2004–2005, the direct cost associated with schizophrenia in the UK reached GBP 2 billion and the indirect cost was GBP 4.7 billion, with a total cost of GBP 6.7 billion.34 In a study conducted in the United States in 2009, it was estimated that the total cost of type I and II bipolar disorders was USD 151.1 billion, with a direct cost of approximately USD 30.7 billion and an indirect cost of approximately USD 120.3 billion.35 In 2015, Cloutier et al estimated a total cost associated with bipolar disorder of USD 202.1 billion, with an average cost per patient of USD 81,559.36 In 2017, the American Psychological Association reported that the cost of treating depression was approximately USD 71 billion in the United States.37 Moreover, in Japan, the cost of treating anxiety disorders reached USD 20.5 billion in 2008.38 We believe that these costs are high in Indonesia. The present study aimed to retrospectively determine the medication profile and estimate the treatment costs in from the medical records of new outpatients with schizophrenia, bipolar disorder, depression, and anxiety disorders from a healthcare perspective at one of the national referral hospitals in Indonesia from 2016 to 2018.
Methods
Study Design
This was an observational study with a cross-sectional design. Data were retrospectively collected from medical records, prescriptions, and administration records of outpatients at the mental clinic of one of the national referral hospitals in Indonesia from 2016 to 2018. New outpatients, in example, patients who were treated or registered in the hospital for the first time, with a diagnosis of schizophrenia (F20), bipolar disorder (F31), depression (F32 and F33), or anxiety disorders (F40–F43) according to the ICD-10 criteria, age more than 18 years, and had only received drugs for treatment were included. Patients with incomplete outpatient data, those who received only psychotherapy treatment, and those diagnosed with >1 mental disorders and had concomitant diseases that affect mental disorders, such as metabolic syndrome, endocrine disease, chronic disease, nervous system disorders, and cancer, were excluded.
Ethics
This study was approved by the ethics committee of Faculty of Medicine, Universitas Padjadjaran, Indonesia. Additionally, personal information was kept confidential by providing a numeric code for each medical record.
Medication Profile
The medication profile was analyzed according to patient characteristics and the types of drugs received by the patients during outpatient treatment. Each patient who received a drug type was recorded and then descriptively analyzed. One patient could receive more than one type of drug. Moreover, medication profiles were provided based on patient category (national insurance and uninsured).
Treatment Cost Estimation
Treatment cost estimation involved direct cost from a healthcare perspective. Direct costs consisted of drug cost, administrative cost, and doctor consultation fees. Each new outpatient data cost was recorded and calculated for 1 year. The sum of the annual direct cost for 1 year, was then divided by the total number of patients to obtain the average estimated annual cost for each patient. We estimated the annual direct costs deeming that the patients were adherent to the treatment. Cost data were obtained from the hospital information system.
Statistical Analysis
The medication profile was analyzed descriptively. The annual cost difference was analyzed by either the Kruskal–Wallis test or the Mann–Whitney test. The difference was considered significant at a p-value <0.05. All statistical analyses were performed using SPSS software version 22 for Windows (IBM Corp., Armonk, NY, USA).
Results
Data Collection
Figure 1 shows the process of data collection. Among 357 new outpatients from 2016 to 2018, we excluded 184. Thus, 173 outpatients met the inclusion and exclusion criteria and were eligible for further analysis.
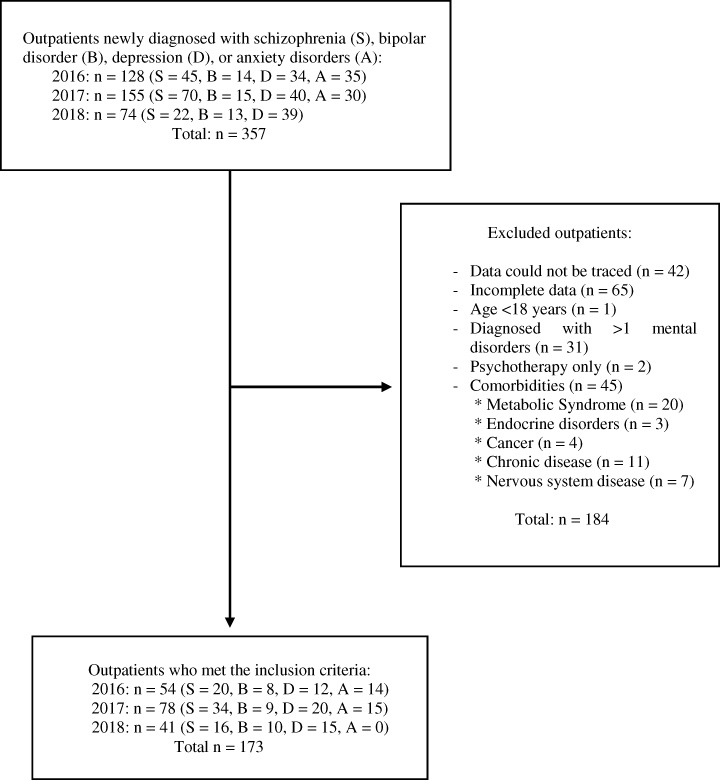 |
Figure 1 Data collection process. |
Subject Characteristics
Table 1 presents the characteristics of the new outpatients who visited the mental health department in 2016, 2017, and 2018, and who met the inclusion and exclusion criteria. Among the new outpatients, 59% (n=102) were male, 56.1% (n=97) were aged 26–45 years, and 56.6% (n=98) used insurance. The total number of visits was 422, and the average number of visits a year per patient was 2–3. Among the 173 outpatients selected, 40.5% (n=70) had schizophrenia, 15.6% (n=27) had bipolar disorder, 27.2% (n=47) had depression, and 16.7% (n=29) had anxiety disorders. Most patients with schizophrenia (48 of 70) and bipolar disorder (21 of 27) were insured, whereas most patients with depression (27 of 47) and anxiety disorders (20 of 29) were uninsured.
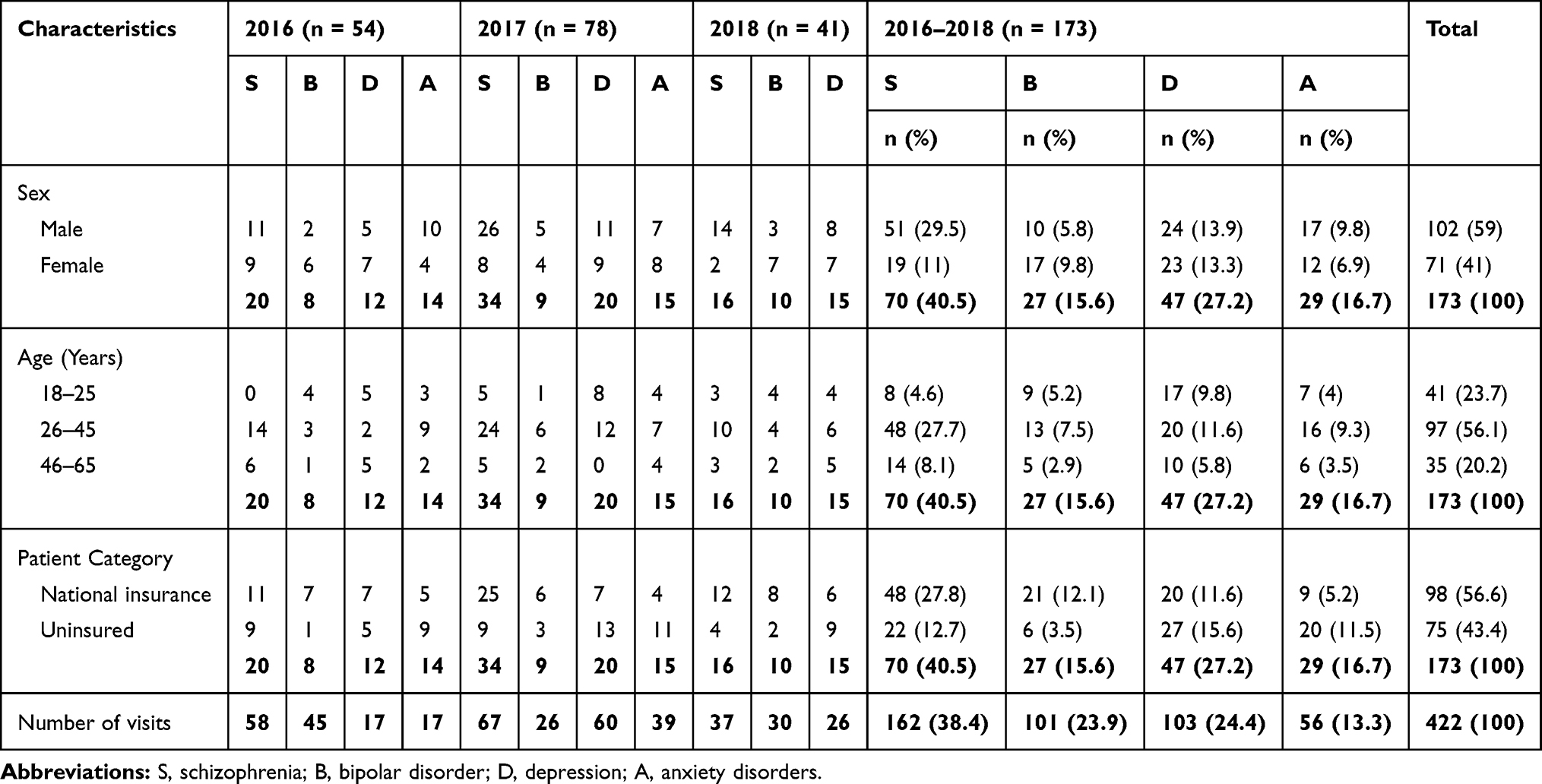 |
Table 1 Patient Characteristics |
Schizophrenia Medication Profile
The medication profile of outpatients with schizophrenia is presented in Table 2. The first-line drugs administered to outpatients with schizophrenia who visited the mental health department were usually antipsychotic drugs (both typical and atypical types). Other drugs, such as anticholinergics, benzodiazepines, and antidepressants, were administered as adjunct drugs. The use of typical antipsychotics decreased from 35.8% of patients in 2016 to 14.3% in 2018, whereas the use of atypical antipsychotics increased from 22.6% in 2016 to 57.1% in 2018. Haloperidol was the most commonly used typical antipsychotic (16.0%), and risperidone was the most commonly used atypical antipsychotic (22.7%). The use of trihexyphenidyl decreased from 39.6% in 2016 to 7.1% in 2018, whereas the use of lorazepam increased from 1.9% in 2016 to 17.9% in 2018. Overall, 83.3% (40 of 48) of insured outpatients received atypical antipsychotic drugs.
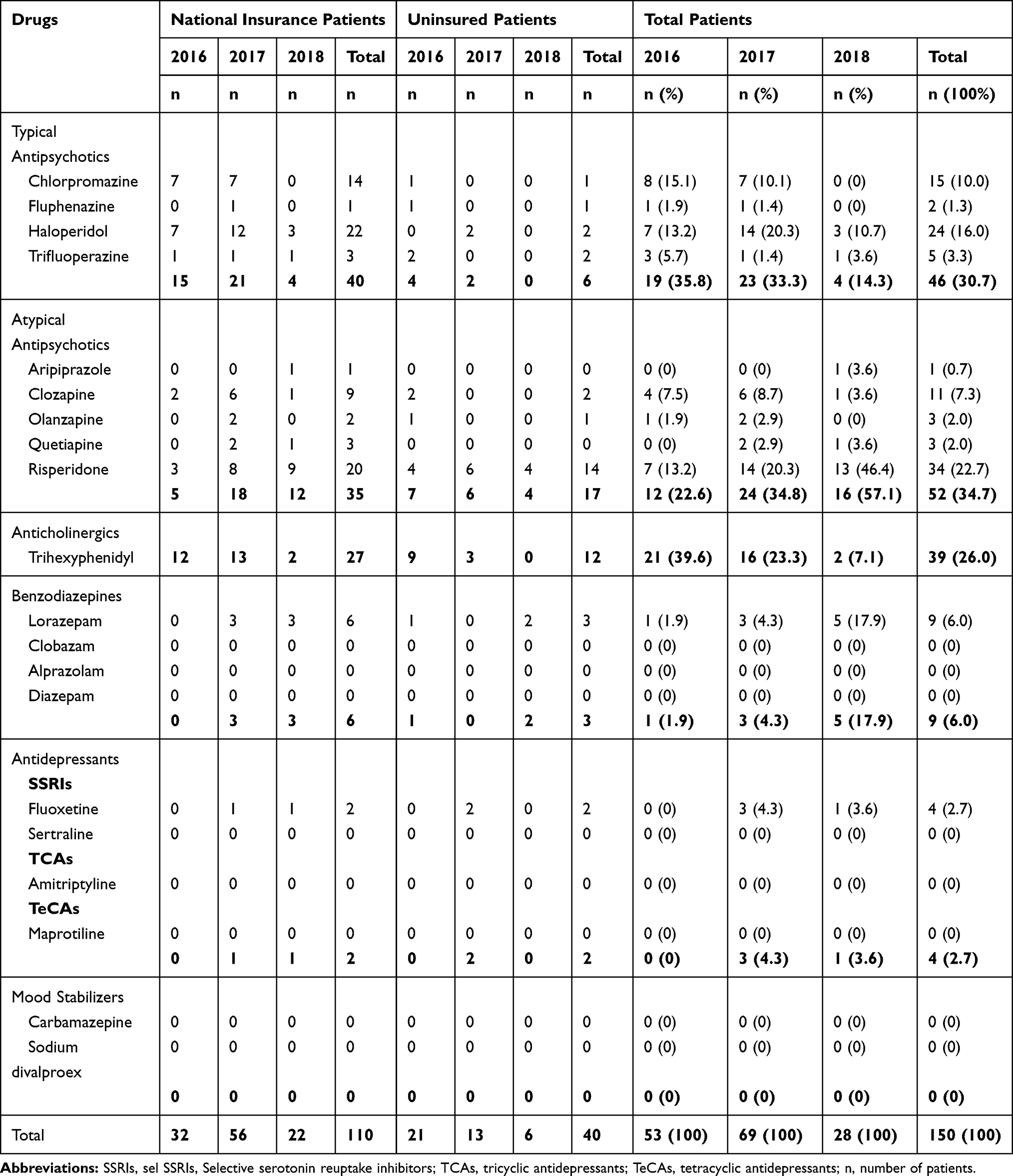 |
Table 2 Medication Profile of Schizophrenia Patients |
Bipolar Disorder Medication Profile
The medication profile of outpatients with bipolar disorder is presented in Table 3. Several classes of drugs were administered to the patients, including mood stabilizers, antipsychotics, antidepressants, benzodiazepines, and anticholinergics. Mood stabilizers were first-line drugs in patients with bipolar disorder, and they were used in 29.4% of patients. Sodium divalproex was the most commonly used mood stabilizer (27.9%). Atypical antipsychotics were used in 39.7% of patients. Risperidone was the most commonly used atypical antipsychotic (11.8%). All insured patients received at least one type of atypical antipsychotic drug, and 81% (17 of 21) received sodium divalproex for treatment.
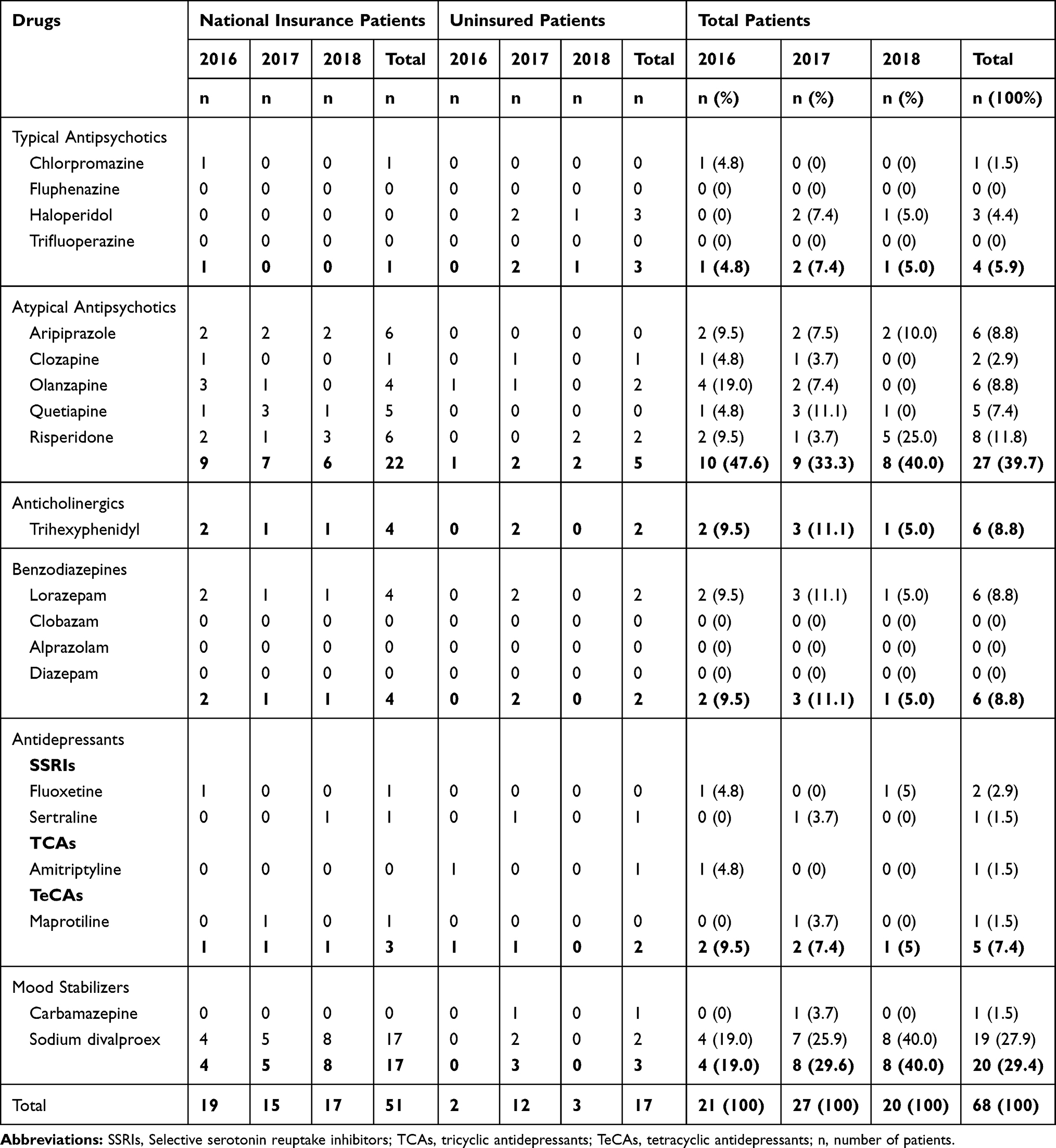 |
Table 3 Medication Profile of Bipolar Disorders Patients |
Depression Medication Profile
The medication profile of outpatients with depression is presented in Table 4. Antidepressants were commonly used for treatment (51.2%). Benzodiazepines, atypical antipsychotics, anticholinergics, and mood stabilizers were also used. The atypical antipsychotic risperidone was the most common drug (18%). The drugs used in both insured and uninsured patients did not show considerable difference.
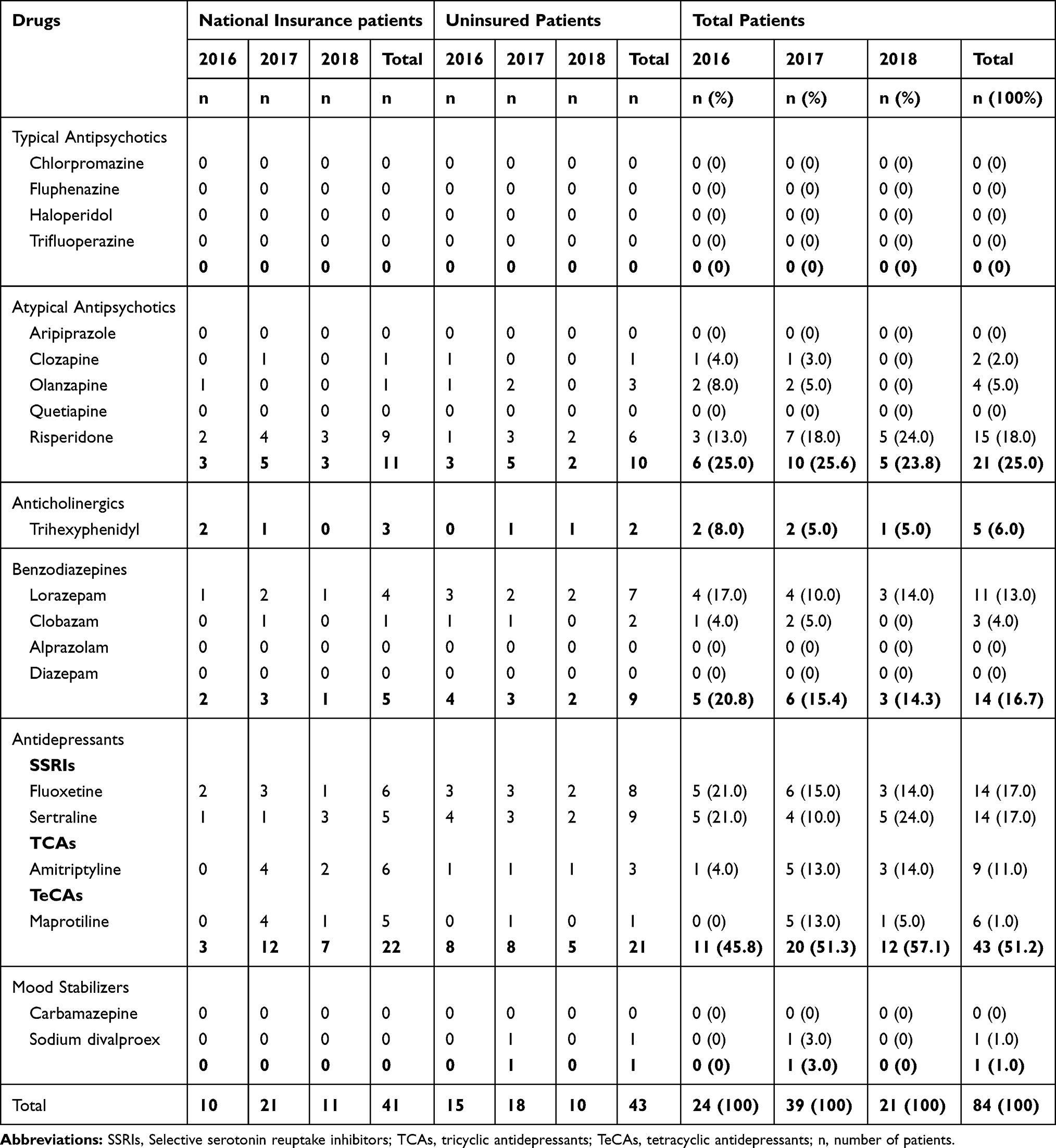 |
Table 4 Medication Profile of Depression Patients |
Anxiety Disorder Medication Profile
The medication profile of outpatients with anxiety disorders is presented in Table 5. Several classes of drugs were administered to the patients, including antidepressants, benzodiazepines, and antipsychotics. Antidepressants and benzodiazepines were dominantly used (both 47.6%). Sertraline was the most commonly used antidepressant (28.6%), and lorazepam was the most commonly used benzodiazepine (22.2%). Most of the insured patients received more than one benzodiazepine and antidepressant.
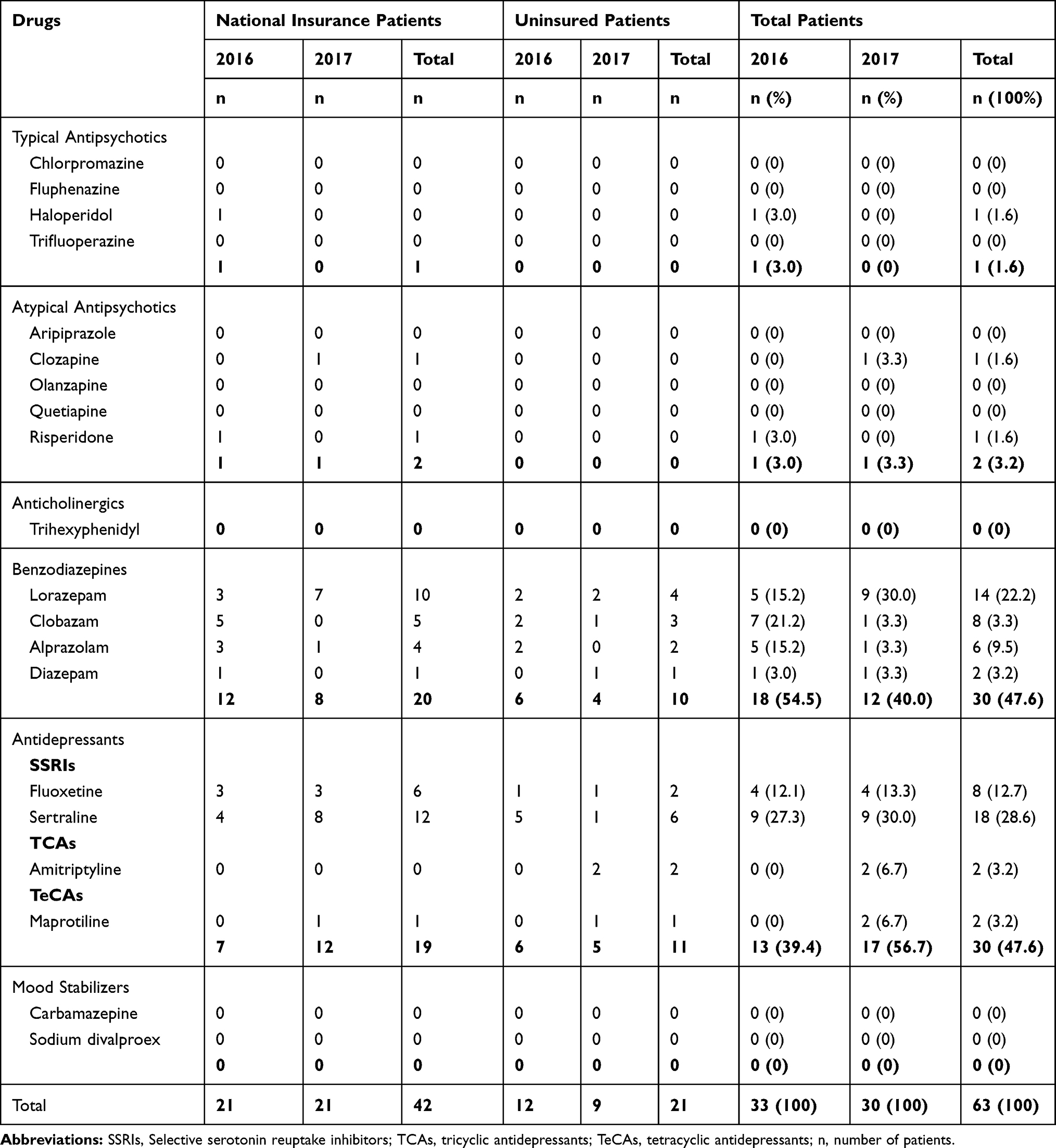 |
Table 5 Medication Profile of Anxiety Disorders Patients |
Treatment Cost Estimation
Table 6 presents the average estimated annual treatment costs from a healthcare perspective for outpatients with schizophrenia, bipolar disorder, depression, and anxiety disorders if the patients were adherent to regular medical treatment for 1 year. Among all the mental disorders, bipolar disorder had the highest average annual treatment cost of IDR 17,978,865 (USD 1,284) per patient. The average annual treatment costs for schizophrenia, depression, and anxiety disorders were IDR 3,307,931 (USD 236), IDR 1,601,850 (USD 114), and IDR 1,190,563 (USD 85) per patient, respectively. There was a significant difference (p =0.012) in the depression treatment cost owing to changes in the guideline in 2017. Based on patient category, the costs were not significantly different (p >0.05) between insured and uninsured patients with schizophrenia, depression, and anxiety disorders. However, the costs were significantly different (p =0.012) between insured and uninsured patients with bipolar disorder.
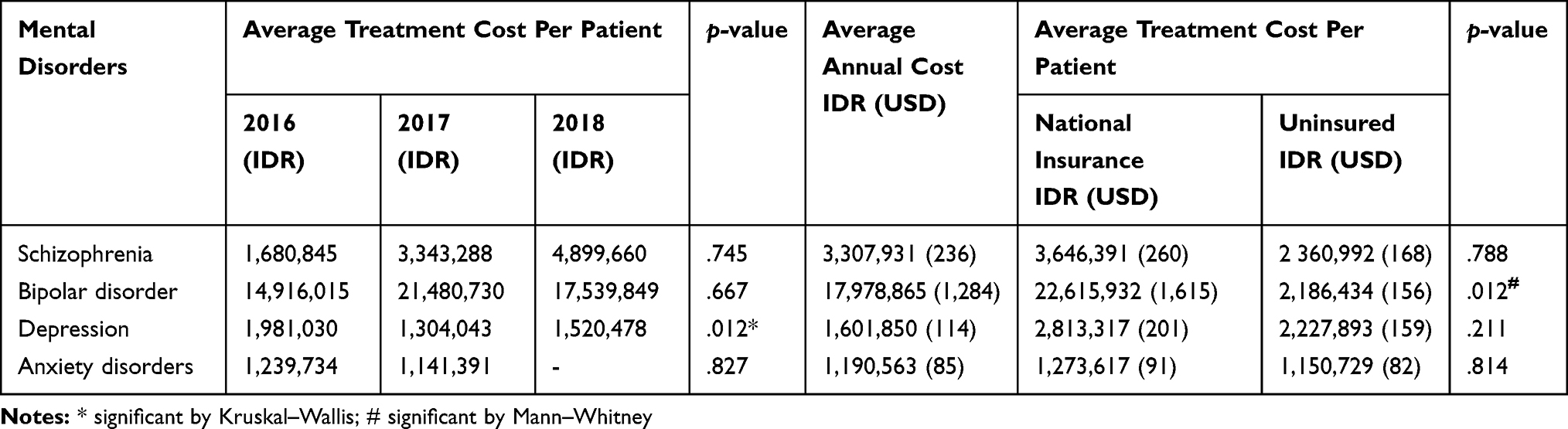 |
Table 6 Average Treatment Cost Estimation |
Discussion
The present study provides an overview of the medication profile and estimated annual treatment costs of outpatients with schizophrenia, bipolar disorder, depression, and anxiety disorders, as well as the total estimated annual treatment cost for these disorders at one of the national referral hospitals in Indonesia from 2016 to 2018. The main drugs were atypical and typical antipsychotics for schizophrenia, atypical antipsychotics and mood stabilizers for bipolar disorder, antidepressants and atypical antipsychotics for depression, and antidepressants and benzodiazepines for anxiety disorders. The average annual treatment costs for schizophrenia, depression, and anxiety disorders were IDR 3,307,931 (USD 236), IDR 1,601,850 (USD 114), and IDR 1,190,563 (USD 85) per patient, respectively.
In patients with schizophrenia, our study found that haloperidol was the most commonly used typical antipsychotic and risperidone was the most commonly used atypical antipsychotic. These results are consistent with the findings in the 2017 study by Oktapaku in Nigeria, which reported that haloperidol was the most widely used antipsychotic among outpatients, and the 2018 study by Khan, which reported that the atypical antipsychotic risperidone was most widely used by patients with schizophrenia.39,40 The American Psychiatric Association states that the use of different types of antipsychotics depends on the clinical outcome desired. In addition, factors, such as patient response, hospital policy, drug availability, and cost influence the choice of antipsychotics.7 In this study, the other drugs administered were anticholinergics (trihexyphenidyl), benzodiazepines (lorazepam), and antidepressants (fluoxetine). The anticholinergic trihexyphenidyl was mostly used in 2016 to reduce extrapyramidal side effects (dystonia, akathisia, pseudoparkinsonism, and tardive dyskinesia), and its use decreased with the decrease in typical antipsychotic use in 2017 and 2018. Benzodiazepines, such as lorazepam, when used together with antipsychotics can reduce the risk of extrapyramidal side effects.7 The use of antidepressants in patients with schizophrenia is uncommon, and some studies suggest that the use of antidepressants in patients with schizophrenia is ineffective because not all patients recover from the depression symptoms experienced.41
In this study, for the treatment of bipolar disorder, most patients received more than one type of drug other than mood stabilizers. They were also administered antipsychotics, antidepressants, benzodiazepines, and anticholinergics. This approach is common and has the purpose of preventing recurrence that cannot be avoided because the efficacy profiles of drugs differ and the needs for handling both episodes of bipolar disorder also differ.42 Sodium divalproex is a type of mood stabilizer that was the most widely used drug among patients with bipolar disorder (27.9%) in this study. This finding is consistent with the finding in the 2012 study by Chawla et al, which reported that the most widely used drug among patients with bipolar disorder in India was sodium valproate (54.7%).43 In addition, a 2009 study involving bipolar disorder outpatients in South Africa mentioned that most patients (83.8%) were prescribed at least one standard mood stabilizer and that sodium valproate was the most prescribed mood stabilizer (37.1%).44 The National Institute for Health and Care Excellence (NICE) has recommended the use of valproate as first-line therapy in acute manic episodes. It can be combined with antidepressants for the treatment of acute depressive episodes and for prophylaxis.45 In addition to mood stabilizers, antipsychotics, such as haloperidol, aripiprazole, and risperidone; benzodiazepines, such as lorazepam; and antidepressants, such as quetiapine, can be combined for treatment.46 In this study, the most widely used atypical antipsychotic was risperidone. Antipsychotics are often used in the acute phase of bipolar disorder and are mostly used in patients who have psychotic symptoms.47 Benzodiazepines, such as lorazepam, can also be used as an alternative therapy or as an adjunct therapy with antipsychotics in patients with acute manic episodes or those who cannot use mood stabilizers.18
In this study, fluoxetine and sertraline were frequently administered in patients with depression (both 17%). A previous study at a hospital in Sragen, Indonesia, reported that 93.33% of patients were administered fluoxetine,48 and another study at a hospital in Surakarta, Indonesia, reported that 64.4% of patients were administered this drug.49 In addition to antidepressants, atypical antipsychotics and benzodiazepines were administered in patients with depression in the present study. Antipsychotics were frequently used for depression treatment because 80% of patients experienced psychotic symptoms in 2017. Antidepressants are widely used in combination with benzodiazepines to increase patient compliance and reduce the severity of depression.50
The main drugs among patients with anxiety disorders in this study were antidepressants and benzodiazepines. Antidepressants with an SSRI mechanism were administered in 41.3% of patients with anxiety disorders, and the SSRI sertraline was administered in 28.6% of patients. An antidepressant with an SSRI mechanism is the first-line therapy recommended for most anxiety disorders, and it is typically started at a low dose to avoid side effects.51 To provide additional efficacy for reducing symptoms, antidepressants are usually combined with benzodiazepines.52 In the present study, the benzodiazepine lorazepam was administered in 28.6% of patients. However, benzodiazepines are not recommended for long-term treatment owing to side effects and potential addiction.53 Benzodiazepines are usually administered for severe anxiety disorders and are administered at night to overcome insomnia.54,55
In our study, the estimated annual treatment cost for outpatients with schizophrenia from a healthcare perspective was USD 236 per patient. This cost is similar to the direct cost for outpatients with schizophrenia reported in Tianjin, China, in 2015 (USD 231 per patient annually)56 and in Nigeria in 2012 (USD 349.6 per patient annually).57 In 2013, the direct costs were USD 7247 in Japan, USD 154 in the UK, USD 10,635 in Germany, USD 774 in the Netherlands, and USD 4742–29,279 in the USA.58
The annual treatment cost was the highest for bipolar disorder [IDR 17,978,865 (USD 1,284) per patient] among the mental disorders in this study. This finding is consistent with that obtained in the 2017 study by Sarkar, which reported that the treatment cost was the highest for bipolar disorder among mental disorders in South India.59 In 2015, in the USA, the direct cost per individual for bipolar disorder type I was approximately 13 times higher than the cost in our study of USD 17,127 [21% of the total cost in the USA (USD 81,559)].60 Furthermore, we found that the direct costs of insured and uninsured individuals with bipolar disorder significantly differed. This difference might have occurred because 80% of patients with national insurance (17 of 21) received sodium divalproex for treatment, whereas only 33% (2 of 6) of uninsured patients received sodium divalproex. Sodium divalproex was assumed to be the drug that contributed the most to the high costs of medication treatment.
The annual estimated direct costs for depression and anxiety disorders in our study were IDR 1,601,850 (USD 114) and IDR 1,190,563 (USD 85) per patient, respectively. The direct costs for depression were relatively lower than those per individual in Japan in 2008 (USD 689), in the UK in 2000 (USD 264), and in the USA in 1990–2000 (USD 1195–1400).61 Moreover, the direct costs for anxiety disorders were lower than those in the USA, which were estimated to be USD 1657.52 per patient in 2009–2010.62
Considering the absence of official data on the prevalence of bipolar and anxiety disorders, this prevalence can be estimated by subtracting the prevalence of depression from the prevalence of all mental–emotional disorders, which yields a value of 3.7%. To estimate treatment costs, the prevalence of bipolar disorder and anxiety disorders individually were determined as 1.85% (half of 3.7%), which corresponds to approximately 3.5 million individuals. Considering these prevalence estimations, if we estimated the annual direct costs based on our results, assuming that all patients adhered to medical treatment in 1 year, the estimated annual direct costs for schizophrenia, bipolar disorder, depression, and anxiety disorders were as follows: IDR 1.5 trillion (USD 110 million), IDR 62.9 trillion (USD 4.5 billion), IDR 18.9 trillion (USD 1.3 billion), and IDR 4.2 trillion (USD 297 million), respectively. Additionally, the total estimated annual direct costs for these four disorders are IDR 87.5 trillion (USD 6.2 billion). However, this cost determined might be overestimated as it is extremely high and almost six times higher than the cost for all catastrophic diseases, which was IDR 14.6 trillion according to BPJS financial data in 2016.63
Although huge costs have been estimated based on the prevalence, the costs for mental health in Indonesia will be lower than the estimations because not all individuals with mental disorders in Indonesia seek help for their condition or are adherent to medication. In our study, the mean value obtained by dividing the total number of visits by the total number of patients was 2.4, indicating that each patient visits the hospital only 2–3 times a year. This finding was in accordance with the RISKESDAS data that reported that only 9% of patients with depression in Indonesia received treatment.5 A systematic review published in 2017 revealed that patients with mental disorders discontinue or show non-adherence to their medication because of poor insight, negative attitude toward medication, distressing medication side effects, poor therapeutic alliance, and stigma.64 Those factors might also affect the treatment adherence of patients with mental disorders in Indonesia.
Furthermore, our study showed that there are some differences in the number of cases detected in different years. Most of the increase occurred in 2017 for all disorders. It may be assumed that the increase in the number of cases detected occurred because of the increase in the prevalence of mental disorders. This finding was consistent with the basic health research report from the Ministry of Health, Indonesia, in 2018, which stated that the prevalence of mental–emotional disorders increased from 3.8%–6% in 2013 to 9.8% in 2018.5 Second, in 2017, there were changes in national guidelines. Consequently, due to the new policy, medications were unavailable in primary and secondary healthcare in some cases, resulting in several patients being referred to the national referral hospital to continue their medication. In 2018, there were some improvements in the national guidelines to ensure that the patients could yet again receive their medications in primary or secondary hospitals.
The present study has limitations because data were collected from only one national referral hospital, included only new outpatient data, and some of the data were presented descriptively. Further analyses, such as analysis of the relationships between the medication profile and treatment cost considering community income per capita and cost from a societal perspective, are necessary, and they could explain nationally representative results with regard to the medication profile and estimation of BOD for mental disorders. This study provides information on the medication profile for mental disorders, and it could be the first step to estimate the annual cost for mental disorder treatment in Indonesia.
Conclusion
The most commonly administered drugs for schizophrenia treatment were haloperidol and risperidone, those for bipolar disorders were sodium divalproex and risperidone, those for depression were fluoxetine and sertraline, and those for anxiety disorders were sertraline and lorazepam. The average estimated annual treatment costs per patient from a healthcare perspective were IDR 3,307,931 (USD 236) for schizophrenia, IDR 17,978,865 (USD 1,284) for bipolar disorder, IDR 1,601,850 (USD 114) for depression, and IDR 1,190,563 (USD 85) for anxiety disorders. Considering the increasing prevalence each year and high costs, it is important for the government and all Indonesian citizens to work toward reducing the prevalence of mental disorders in Indonesia.
Funding
This work was supported by the Ministry of Research and Technology and Higher Education, Indonesia (grant number 1123k/UN6.O/LT/2019).
Disclosure
The authors declare there is no conflicts of interest in this work.
References
1. WHO. Mental disorders affect one in four people; 2001. Available from: https://www.who.int/whr/2001/media_centre/press_release/en/.
2. World Health Organization. Mental disorders; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders.
3. Statistics Indonesia. Population 15 years of age and over by age group and type of activity during the previous week, 2008–2018; 2019. Available from: https://www.bps.go.id/statictable/2016/04/04/1904/penduduk-berumur-15-tahun-ke-atas-menurut-golongan-umur-dan-jenis-kegiatan-selama-seminggu-yang-lalu-2008—2018.html.
4. SI BPS. Statistical Yearbook of Indonesia.
5. Ministry of Health Republic of Indonesia. National report basic health research 2018; 2018. Available from: http://labmandat.litbang.depkes.go.id/images/download/laporan/RKD/2018/Laporan_Nasional_RKD2018_FINAL.pdf.
6. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiologic Approach.
7. Work Group on Schizophrenia. Practice Guideline for the Treatment of Patients with Schizophrenia.
8. Miyamoto S, Miyake N, Jarskog LF, Fleischhacker WW, Lieberman JA. Pharmacological treatment of schizophrenia: a critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol Psychiatry. 2012;17(12):1206–1227. doi:10.1038/mp.2012.47
9. Ganguly P, Soliman A, Moustafa AA. Holistic management of schizophrenia symptoms using pharmacological and non-pharmacological treatment. Front Public Heal. 2018;6(166):1–9. doi:10.3389/fpubh.2018.00166
10. Vieta E. Managing Bipolar Disorder in Clinical Practice: Third Edition; 2013. doi:10.1007/978-1-908517-94-4.
11. Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet. 2013;381(9878):1672–1682. doi:10.1016/S0140-6736(13)60857-0
12. Grande I, De Arce R, Jiménez-Arriero MÁ, et al. Patterns of pharmacological maintenance treatment in a community mental health services bipolar disorder cohort study (SIN-DEPRES). Int J Neuropsychopharmacol. 2013;16(3):513–523. doi:10.1017/S1461145712000405
13. Chisholm-Burns MA, Schwinghammer TL, Well BG, Malone PA, Kolesar JM, DiPiro JT. Pharmacotherapy Principles & Practice.
14. Mirabel-Sarron C, Giachetti R. Non pharmacological treatment for bipolar disorder. Encephale. 2012;38(4). doi:10.1016/S0013-7006(12)70094-5
15. Kumar KPS, Srivastava S, Paswan S, Dutta AS. Depression - symptoms, causes, medications and therapies. Pharm Innovation. 2012;1(3):37.
16. Spijker J, Van Straten A, Bockting CLH, Meeuwissen JAC, Van Balkom AJLM. Psychotherapy, antidepressants, and their combination for chronic major depressive disorder: a systematic review. Can J Psychiatry. 2013;58(7):386–392. doi:10.1177/070674371305800703
17. Wang S-M, Han C, Bahk W-M, et al. Addressing the side effects of contemporary antidepressant drugs: a comprehensive review. Chonnam Med J. 2018;54(2):101. doi:10.4068/cmj.2018.54.2.101
18. Wells BG, DiPiro JT, Schwinghammer TL, Dipiro CV. Pharmacotherapy Handbook.
19. Gartlehner G, Wagner G, Matyas N, et al. Pharmacological and non-pharmacological treatments for major depressive disorder: review of systematic reviews. BMJ Open. 2017;7(6):e014912. doi:10.1136/bmjopen-2016-014912
20. Park S-C, Oh HS, Oh D-H, et al. Evidence-based, non-pharmacological treatment guideline for depression in Korea. J Korean Med Sci. 2014;29(1):12–22. doi:10.3346/jkms.2014.29.1.12
21. Victoria Institute of Strategic Economic Studies. The economic cost of serious mental illness and comorbidities in Australia and New Zealand. R Aust New Zeal Coll Psychiatr. 2016:1–48. Available from: https://www.ranzcp.org/Files/Publications/RANZCP-Serious-Mental-Illness.aspx. Accessed March 12, 2020.
22. Gariepy G, Nitka D, Schmitz N. The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. Int J Obes. 2010;34(3):407–419. doi:10.1038/ijo.2009.252
23. Reinhold JA, Mandos LA, Rickels K, Lohoff FW. Pharmacological treatment of generalized anxiety disorder. Expert Opin Pharmacother. 2011;12(16):2457–2467. doi:10.1517/14656566.2011.618496
24. Lampe L. Drug treatment for anxiety. Aust Prescr. 2013;36(6):186–189. doi:10.18773/austprescr.2013.076
25. Strawn JR, Geracioti L, Rajdev N, Clemenza K, Levine A. Pharmacotherapy for generalized anxiety disorder in adults and pediatric patients: an evidence-based treatment review. Expert Opin Pharmacother. 2018;19(10):1057–1070. doi:10.1080/14656566.2018.1491966
26. Bystritsky A, Khalsa SS, Cameron ME, Schiffman J. Current diagnosis and treatment of anxiety disorder. Pharm Ther. 2013;38(1):30–57.
27. Combs H, Markman J. Anxiety disorders in primary care. Med Clin North Am. 2014;98(5):1007–1023. doi:10.1016/j.mcna.2014.06.003
28. Cottraux J. Nonpharmacological treatments for anxiety disorders. Dialogues Clin Neurosci. 2002;4(3):305–319.
29. Jo C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. 2014;20(4):327–337. doi:10.3350/cmh.2014.20.4.327
30. Trautmann S, Rehm J, Wittchen H. The economic costs of mental disorders. EMBO Rep. 2016;17(9):1245–1249. doi:10.15252/embr.201642951
31. Vos T, Barber RM, Bell B, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. doi:10.1016/S0140-6736(15)60692-4
32. Goetzel RZ, Roemer EC, Holingue C, et al. Mental health in the workplace: a call to action proceedings from the mental health in the workplace-public health summit. J Occup Environ Med. 2018;60(4):322–330. doi:10.1097/JOM.0000000000001271
33. Bloom D, Cafero E, Jané-Llopis E, et al. The global economic burden of non-communicable diseases. Geneva: world Economic Forum; 2011. Available from: http://www3.weforum.org/docs/WEF_Harvard_HE_GlobalEconomicBurdenNonCommunicableDiseases_2011.pdf.
34. Mangalore R, Knapp M. Cost of Schizophrenia. J Ment Health Policy Econ. 2007;10(1):23–41.
35. Dilsaver SC. An estimate of the minimum economic burden of bipolar i and II disorders in the United States: 2009. J Affect Disord. 2011;129(1–3):79–83. doi:10.1016/j.jad.2010.08.030
36. Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the United States in 2015. J Affect Disord. 2018;226:45–51. doi:10.1016/j.jad.2017.09.011
37. Dieleman JL, Baral R, Birger M, et al. US spending on personal health care and public health, 1996–2013. JAMA. 2016;316(24):2627–2646. doi:10.1001/jama.2016.16885
38. Sado M, Takechi S, Inagaki A. et al. Cost of anxiety disorders in Japan in 2008: a prevalence-based approach. BMC Psychiatry. 2013:13. doi:10.1186/1471-244X-13-338.
39. Okpataku CI, Tawani D, Article O. Psychotropic prescriptions for the treatment of schizophrenia in an outpatient clinic. Trends Psychiatry Psychother. 2017;39(3):165–172. doi:10.1590/2237-6089-2016-0088
40. Khan A, Iqbal Z, Sultan SM, Nazar Z, Tariq M. Antipsychotic prescription patterns and treatment costs of schizophrenia in northwestern Pakistan: a one-year observational study. Trop J Pharm Res. 2018;17:339–344.
41. Irene M. A systematic review of instruments to measure depressive symptoms in patients with schizophrenia publisher’ s pdf, also known as version of record publication date. J Affect Disord. 2012;140(1):38–47. doi:10.1016/j.jad.2011.10.014
42. National Collaborating Centre for Mental H. Bipolar Disorder: The NICE Guideline on the Assessment and Management of Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care. Leicester: The British Psychological Society & The Royal College of Psychiatrists; 2014.
43. Chawla S, Agarwal M, Sharma S, Jiloha RC. Drug utilization study of psychotropic drugs among psychiatric outpatients in a tertiary care hospital. Indian J Pharm Sci. 2017;79(6):1008–1013. doi:10.4172/pharmaceutical-sciences.1000319
44. Holzapfel EM, Szabo CP. Pharmacotherapy prescribing patterns in the treatment of bipolar disorder in a South African outpatient population. Glob Psychiatry. 2018;1(2):39–51. doi:10.2478/gp-2018-0006
45. National Institute for Health and Care Excelence. Bipolar disorder: assessment and management; 2014. Available from: https://www.nice.org.uk/guidance/cg185/chapter/1-Recommendations.
46. Taylor D, Paton C, Kapur S. Prescribing Guidelines in Psychiatry.
47. Turner TL. The use of antipsychotics in maintenance treatment of bipolar disorder. Ment Heal Clin. 2013;2(12):412–415. doi:10.9740/mhc.n155513
48. Rossatria E. Evaluation of Antidepressants Drug Prescribing for Depressed Patients at Pharmacy Installation Outpatient in Regional Hospital Dr. Soehadi Prijonegoro Sragen; 2016.
49. Yuniastuti. Evaluation of Antidepressant Drug for Therapy Patient In Depression Mental Hospital Surakarta 2011–2012; 2013.
50. Ogawa Y, Takeshima N, Hayasaka Y, et al. Antidepressants plus benzodiazepines for adults with major depression. Cochrane Database Syst Rev. 2019;2019(6). doi:10.1002/14651858.CD001026.pub2
51. Bandelow B, Zohar J, Hollander E, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of anxiety, obsessive-compulsive and post-traumatic stress disorders - First revision. World J Biol Psychiatry. 2008;9(4):248–312. doi:10.1080/15622970802465807
52. Farach FJ, Pruitt LD, Jun JJ, Jerud AB, Zoellner LA, Roy-Byrne PP. Pharmacological treatment of anxiety disorders: current treatments and future directions. J Anxiety Disord. 2012;26(8):833–843. doi:10.1016/j.janxdis.2012.07.009
53. Tanguay Bernard MM, Luc M, Carrier JD, et al. Patterns of benzodiazepines use in primary care adults with anxiety disorders. Heliyon. 2018;4(7). doi:10.1016/j.heliyon.2018.e00688
54. Crocco EA, Jaramillo S, Cruz-Ortiz C, Camfield K. Pharmacological management of anxiety disorders in the elderly. Curr Treat Options Psychiatry. 2017;4(1):33–46. doi:10.1007/s40501-017-0102-4
55. Ellen S, Selzer R, Norman T, Blashki G. Depression and anxiety: pharmacological treatment in general practice. Aust Fam Physician. 2007;36(4):222–228.
56. Ye W. Health care resource use and direct medical costs for patients with schizophrenia in Tianjin, People’ s Republic of China. Neuropsychiatr Dis Treat. 2015;11:983–990.
57. Oloniniyi IO, Akinsulore A, ALoba OO, Mapayi BM, Oginni OA, Makanjuola R. Economic cost of schizophrenia in a Nigerian Teaching Hospital. J Neurosci Rural Pract. 2019;10(1):39–47. doi:10.4103/jnrp.jnrp_210_18
58. Chong HY, Teoh SL, Wu DB-C, Kotirum S, Chiou C-F, Chaiyakunapruk N. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:357–373. doi:10.2147/NDT.S96649
59. Sarkar S, Mathan K, Sakey S, Shaik S, Subramanian K, Kattimani S. Cost-of-treatment of clinically stable severe mental lilnesses in India. Indian J Soc Psychiatry. 2017;33(3):262. doi:10.4103/0971-9962.214600
60. Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the United States in 2015. J Affect Disord. 2018;15(226):45–51. doi:10.1016/j.jad.2017.09.011
61. Okumura Y, Higuchi T. Cost of depression among adults in Japan. Prim Care Companion CNS Disord. 2011;13(3):
62. Shirneshan E, Bailey J, Relyea G, Franklin BE, Solomon DK, Brown LM. Incremental direct medical expenditures associated with anxiety disorders for the U.S. adult population: evidence from the medical expenditure panel survey. J Anxiety Disord. 2013;27(7):720–727. doi:10.1016/j.janxdis.2013.09.009
63. Ministry of Health Republic Indonesia. Heart disease is the highest cause of death, Ministry of Health reminds the CERDIK; 2017. Available from: https://www.depkes.go.id/article/view/17073100005/penyakit-jantung-penyebab-kematian-tertinggi-kemenkes-ingatkan-cerdik.html.
64. Velligan DI, Sajatovic M, Hatch A, Kramata P, Docherty JP. Why do psychiatric patients stop antipsychotic medication? A systematic review of reasons for nonadherence to medication in patients with serious mental illness. Patient Prefer Adherence. 2017;11:449–468. doi:10.2147/PPA.S124658
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.