")
Back to Journals » Advances in Medical Education and Practice » Volume 10
Medical student mentoring programs: current insights
Authors Nimmons D, Giny S , Rosenthal J
Received 10 August 2018
Accepted for publication 9 January 2019
Published 4 March 2019 Volume 2019:10 Pages 113—123
DOI https://doi.org/10.2147/AMEP.S154974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Danielle Nimmons,1 Shaista Giny,2 Joe Rosenthal1
1Department of Primary Care and Population Health, UCL Medical School, Royal Free Campus, London, UK; 2Department of Ophthalmology, Royal Surrey County Hospital, Guildford, UK
Abstract: Medical school mentoring programs incorporate a wide range of objectives. Clinical mentoring programs help to develop students’ clinical skills and can increase interest in under-subscribed specialties. Those that focus on teaching professionalism are integrated into medical school curriculums in order to overcome the “hidden curriculum”. Positive mentoring plays a part in reversing the decline of academic medicine, by sparking interest through early research experiences. It also has an important role in encouraging recruitment of under-represented minority groups into the medical profession through widening access programs. The aim of our review of the literature, is to analyze current trends in medical student mentoring programs, taking into account their objectives, execution, and evaluation. We outline the challenges encountered, potential benefits, and key future implications for mentees, mentors, and institutions.
Keywords: medical education, mentee, mentor, design, delivery, evaluation
Introduction
The word “mentor” originates from Greek mid-eighteenth century, and in Homer’s epic, the Odyssey. It was the name of the friend Odysseus assigned as a trusted adviser to his son Telemachus in his absence. In the present day, the word can be used as a verb – “to advise or train”, or a noun defined as: “An experienced and trusted adviser” 1
In medical education, a mentor may have many roles, for example, supervisor, teacher, or a coach.2 However, unlike teaching, mentoring involves developing a relationship that focuses on achieving specific goals.3 A mentor is employed to counsel and teach a less experienced student or colleague, for example, in near-peer mentoring. The aim is to guide juniors to achieve a wide array of objectives, such as attainment of a practical skill, personal and professional development, research opportunity, and academic development.3 Mentors also provide emotional support and counseling, as well as professional help.4
A prominent review described five key elements to mentoring:5
- Should help the mentee to achieve short- and long-term goals.
- Should include role modeling, and help with career development.
- Both mentee and mentor should benefit from the relationship.
- Relationships should involve direct interaction between mentor and mentee.
- Mentors should be more experienced when compared with the mentee.
With increasing awareness of the potential value of mentoring, programs are now being established at medical schools worldwide. Through this literature review, we will summarize current insights in undergraduate medical mentoring programs, and highlight the key take-home messages, in order to guide institutions, mentors, and mentees in the future design and delivery of effective mentoring programs.
Methods
A database search was performed, including PubMed, Scopus, and Cochrane in order to identify articles related to mentoring in undergraduate medical education. The keywords used alone and in combination were mentoring, mentoring programme, medical student, mentor, mentee, mentorship, undergraduate, peer mentoring, students as mentors, medical education and, medical school. The searches included articles published between 1990 and 2018 due to the broad scope of the topic, considering primary literature, reviews, commentaries, and case studies. In total, the searches fielded 528 articles. Two of the authors independently sorted the articles for those relevant to mentoring in medical schools. Duplicates were excluded (n=6), as well as a further 423 articles after reading titles and abstracts. Finally, the remaining 99 articles were assessed for eligibility and 17 were excluded because: patients carried out mentoring activities; or articles did not focus specifically on mentoring or undergraduate medical education. Of these, 82 articles were deemed appropriate and were included in this review. Searches were complete on the 12 February 2018 and the process demonstrating how articles were selected is shown in Figure 1.
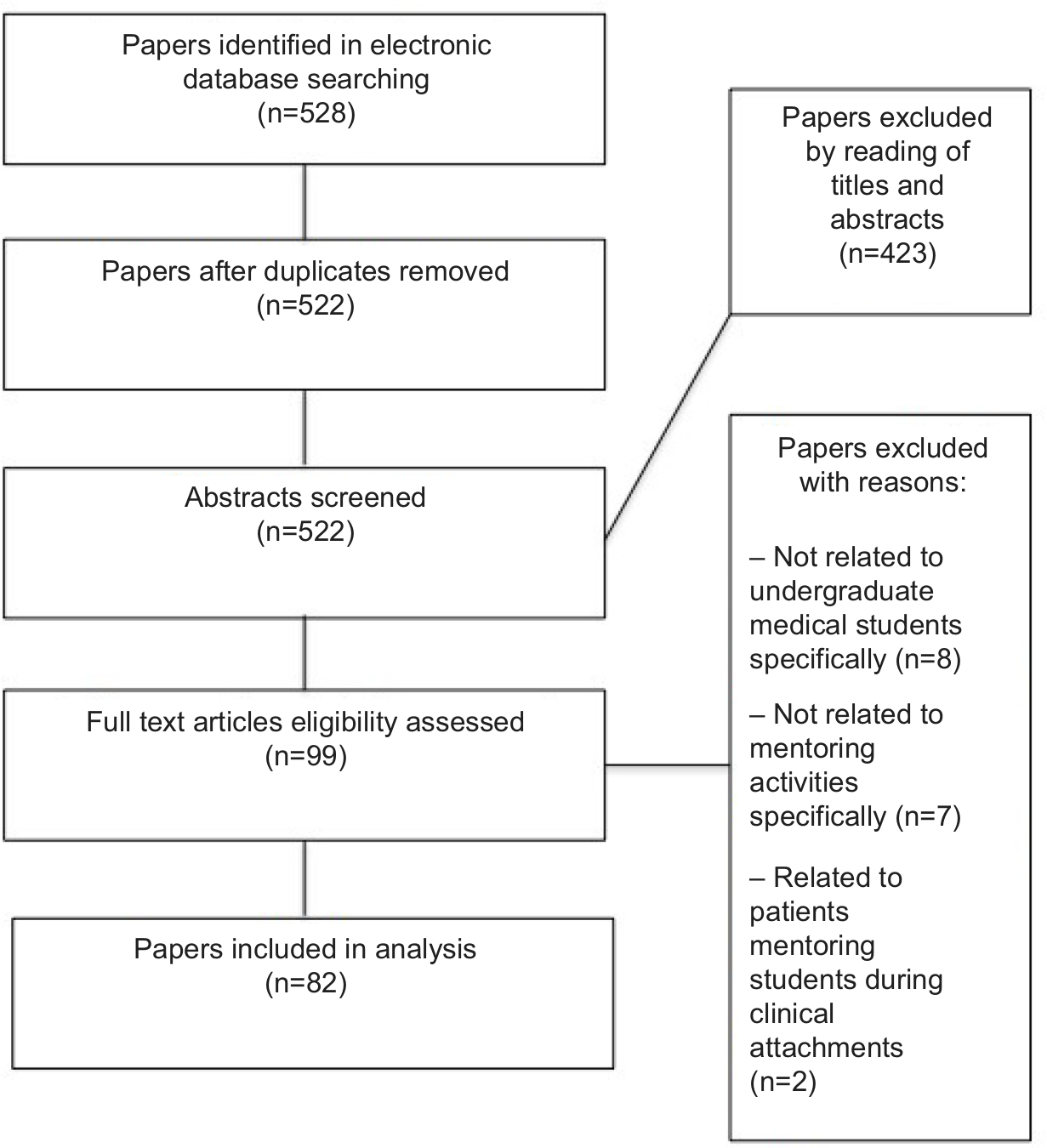 | Figure 1 Search algorithm for articles included. |
Mentor program objectives
Medical school mentoring programs are established worldwide, with varying aims and objectives. These were summarized by Frei et al3 as follows: to increase interest in clinical specialties, to develop professionalism and personal growth, to promote interest in academic medicine, and to provide career counseling. In addition, mentoring is a key component of widening access programs that are often medical student led, and aim to increase applications to medicine from under-represented groups.
Clinical mentoring
Formally recognized supervisors are assigned to trainees at all stages of clinical training. This differs from mentors; who are more likely to be hand selected by mentees and with whom the relationship is more informal. Traditionally, supervisors ensure that trainees have sufficient evidence to progress through training, while the role of a mentor is to offer advice and guidance. However, the two are not mutually exclusive as a supervisor can act as a mentor, and vice versa.6
A number of clinical mentoring initiatives have been specifically designed to prepare final-year medical students for working as a junior doctor.7–9 Recently qualified doctors act as mentors by facilitating clinical skills sessions, bedside teaching, and simulation. This can result in an increase in confidence and self-perceived preparedness for starting work as doctors and a reduction in the performance gap.8,9
Also, positive mentoring can have a significant influence on speciality choice.10 Under-subscribed specialities use mentoring initiatives in the early years of medical school to increase exposure and generate interest. Early mentoring can offer students an insight into what it is like to work in that speciality and challenges preconceptions they may have.11–13 By increasing interaction between specialists and students, these initiatives facilitate learning through constructive feedback and career counseling.14 This can encourage students to apply to particular specialties and provides them adequate time and guidance to begin preparing for the application process.15 A study showed that students who undertook surgery-related research and developed mentor relationships in years 1 and 2 were significantly more likely to maintain an interest in surgical specialities later in their training.16 However, we note the lack of studies identifying a causal relationship between early speciality mentoring and a direct increase in trainee applications. We acknowledge that such a study may not be possible due to a combination of factors affecting career choice, including ethnic, economic, and social influences.10
Professionalism and personal development
As well as its influence on specialty recruitment, mentoring plays a role in student and trainee personal development and professionalism. Professionalism was not always an explicit part of the medical curriculum, and largely fell within the remit of the “hidden curriculum”. This has been defined as: “the context in which the formal curriculum is delivered, and comprises the norms, attitudes, and policies learners implicitly embrace”.17 In other words, the hidden curriculum comprises the unintended lessons that are learned but not taught, and can support or contradict the formal, overt curriculum. Professionalism, in this way, was learned through socialization of the profession and upwards networking, as well as lessons learned in observing clinical teachers.
Nevertheless, over the last two decades, there have been increasing concerns regarding negative role modeling. This occurs when students witness unprofessional behavior in the clinical setting. A failure to address these issues formally can compound detrimental effects of such behavior and result in ethical erosion,18 rather than enabling positive professional enculturation.19
More recently, with increasing recognition that deliberate teaching alongside role-modeling is necessary to cultivate professionalism,20 teaching and assessment of professionalism has now been integrated into formal medical school curricula in the UK and USA. Mentoring plays a key role in the teaching and assessment of professionalism in these curricula – an example is the “Professionalism and the Practice of Medicine (PPM)” course at the Keck School of Medicine of the University of Southern California, implemented in 2001. Faculty mentors were introduced to assist and counsel students, as well as serving as role models. Assessment was undertaken through the presentation of a portfolio and self, peer, and mentor evaluation.21
Ramani et al discussed the role of mentoring in the cultivation of medical student professional development.22 They emphasize the importance of mentoring relationships and the need to balance support and challenge, noting: “If mentors are overly supportive without challenging mentees, the mentees do not grow professionally; on the other hand, challenging without supporting causes mentees to regress in their professional development”. Nevertheless, they acknowledge the limitation that faculty members do not always receive the training they may require to serve as effective mentors alongside their other core responsibilities.
Academic medicine and research
Around the world, academic medicine is in decline. In order to tackle this, a number of institutions, for example in the UK and Canada, have established academic training programs with an emphasis on university faculty mentoring trainees in research.23
The opportunity for research involvement varies across medical schools, with some universities offering integrated PhD programs, and others introductory research components as part of their curriculum.24 Furthermore, student engagement with research varies, and although some institutions have a high proportion of students involved in research,25 it is more likely to be at research-elite universities, and students with research experience prior to commencing medical training.26 Those at research-elite universities have a more satisfactory research training experience,27 while their counterparts at other institutions may be more limited in the type of research they are able to conduct.28
The aim of academic mentoring programs is to cultivate a positive attitude toward academia and enable mentees to tailor and apply research in ways that can benefit their future careers.23,27,29 Trainees value programs taking a holistic approach, with clear pathways and flexibility, allowing them to move in and out of research at different stages of their careers.30 Such programs expose trainees not only to research, but also other aspects of academic learning and personal and professional development, including teaching and the process of peer review.31
Widening access
Over the last two decades, there has been increasing awareness of the lack of social diversity of students in the medical profession. Globally, women, ethnic minorities, and students from disadvantaged socioeconomic backgrounds are under-represented in the medical profession. Although gender disparity is reducing, with women now representing approximately half of medical students in the USA, they remain a minority within certain specialties, for example, general surgery.32 There is a suggestion that same sex mentoring for female medics may be of benefit, with female students highly rating exposure to female mentors and organizations supporting women in surgery. However, as noted by O’Connor, in orthopedic surgery, only 14% of faculty and residents are women, as compared with other specialties, therefore, same gender mentorship opportunities are limited.33 Furthermore, internal motivators can have a significant influence on career direction for female students, for example, the perception that specializing in orthopedic surgery may be detrimental to work/life balance.34
Socioeconomic disparity is a major issue worldwide, including in the UK despite the introduction of several widening access foundation degree programs to medicine.35,36 A number of outreach medical student-led mentorship programs have been established worldwide, with the aim of increasing applicants from diverse, non-traditional backgrounds. Examples of two such programs are in Detroit, MI, USA37 and in the UK.38 Both involve linking medical students with school students from under-represented minorities in order to foster an interest in a career in medicine and assist in providing work experience opportunities and experiential learning through summer schools and career counseling. Varying levels of success are reported with such programs for a number of reasons, in the case of the UK program, the majority of mentees were lost to follow-up. Nonetheless, feedback received from mentees annual evaluations was positive.
Medical students from under-represented minorities identify a lack of access to adequate mentoring when facing key career decisions, as a major issue and challenge. Freeman et al and Nicholson and Cleland explored how medical students from lower socioeconomic backgrounds perceived their own social capital, noting that these students struggled due to reduced awareness of the need for upwards networking in order to negotiate access to resources required to create capital.39,40 The authors recommended a system of peer mentorship for under-represented students with traditional, senior medical students, finding that this was able to facilitate the bridging of capital for both applicants and students from lower socioeconomic backgrounds.
Students as mentors (near-peer mentoring)
Generally, there are two scenarios where medical students act as mentors, when senior medical students mentor junior students and when medical students mentor school or college pupils applying to higher education.
A number of near-peer mentoring programs have been established, often in order to teach an aspect of the curriculum, such as a clinical or procedural skill. At one medical school, fifth- and sixth-year students train fourth-year students how to perform and interpret abdominal ultrasound scans. The skill is taught over three sessions, with both mentors and mentees reporting high satisfaction scores on completion of the program.41 Senior medical students acting as mentors for junior students can also allow mentees to uncover the “hidden curriculum”, negotiate access to resources, and navigate aspects not formally covered in the medical school curriculum.42 Nevertheless, not all medical students are suitable as mentors; those who are self-selecting or selected tend to be better than those randomly allocated.43–45 Moreover, students involved in mentoring require training, for example, in areas, such as giving constructive feedback and setting goals and expectations.37,43
Medical students involved in mentoring school pupils are able to provide an insight into life as a medical student, as well as support with the rigorous application process.46 Moreover, those involved in widening access programs can also serve as role models and engage students who may previously have not considered a career in the medical profession.37,47,48
Senior medical student mentors can bridge a gap between physicians and junior students. As student mentors and mentees are closer in terms of training, there is a more collaborative working environment and mentors are more able to relate to their mentees, and vice versa. This can enable mentees to gain a deeper understanding of challenging concepts that may otherwise be difficult to grasp.41,43,49 Junior students may also be more comfortable raising areas of uncertainty with senior students, and a subsequent increase in knowledge, skills, and confidence can enhance their future interactions with clinicians.44
Design and delivery of medical mentoring programs
The design and delivery of medical mentoring programs differ between medical schools, and programs are adapted to meet specific institutional or departmental requirements. Variables include mentee, mentor, and program characteristics.
Mentee characteristics
While some mentoring programs are designed for medical students in all years, others offer mentoring at a specific stage of training, such as preclinical or clinical years. Others focus on one particular year group, in order to provide students with skills that they will need in the near future. This is seen in UK mentoring programs for final-year students, which aim to prepare students for life as a newly qualified doctor and cover topics, including “how to clerk a patient” and “how to manage a ward round”.7,9
Programs involving all years are often primarily there to provide professional and pastoral support to students as they progress through medical school.50,51 Others offer clinical support to students during certain specialty rotations.52,53 There are also a number of programs that cater to groups of students possessing certain characteristics, for example, to mentor those struggling academically,54 and support those from under-represented minority groups.55 Widening access programs recruit mentees that meet specific criteria, usually taking into account socioeconomic background and attendance at schools in disadvantaged areas.38,45,47
Methods to recruit mentees to programs are diverse and include the following: emails; flyers in the canteen; lecture shout-outs; social media advertising, and events, such as “mentor speed dating”.8,9,12,55,56 Following recruitment, prospective mentees may be offered training,57 and are usually given information on ground rules and expectations via email, lectures, or as a paper handout.7,9,12,56,58–61
Mentor characteristics
Mentors come from a range of backgrounds depending on the aim of the program, and can be residents, academic staff, faculty physicians, recently qualified doctors, speciality doctors, and senior medical students.7,29,31,62,63 Many mentors put themselves forward for the role,64 others are recommended or have demonstrated an interest in teaching or mentoring.65,66
Early career specialists with <10 years of experience can have a great impact on mentees, due to the fact that they are often more able to relate to students’ current personal and professional needs than more senior mentors, and likely to have more up-to-date information on the specialty application and interview process.61,67,68 Likewise, doctors nearing retirement can also be highly valued as mentors due to their wealth of experience and reduced clinical workload, often allowing them to contribute more time to mentoring activities than their more junior counterparts.69
Finally, there is variation as to whether mentors receive reimbursement for their role. In some programs, mentors are paid,7,52,56,57,59,63,65 and less commonly, they are approved to use mentoring activities for academic promotion.57,65 Once appointed, most mentors receive some form of training, which can be provided face-to-face or online.8,12,51,52,56,70
Program characteristics
Medical school mentoring programs tend to be based on and modified from successful initiatives at other institutions, and further developed from mentee/mentor feedback.50,51,65 Less often, a needs analysis is performed, or a program piloted prior to delivery;8,56,67 which help to ensure that the program is designed adequately and effectively.
Programs may be funded by a range of sources, including the host university and/or third parties.50,51,55,56,58,61,64,66 Those that are funded are more likely to have dedicated admin support to help co-ordinate activities12,50,55 and subsidize food and travel costs.51,55
Programs differ in the way mentors are assigned mentees. They can be randomly assigned,57,62,63 or mentees can choose their own mentors, for example, via a mentor database.9,50,56,58,71,72 There are also online matching validated processes, such as electronic data processing (EDP)-supported matching procedures. Mentees and mentors complete online matching profiles consisting of questions that focus on professional orientation, work life priorities, and interests. An automated algorithm then provides matches depending on weighted correlated scores.25 One study found no significant difference in satisfaction between personal and EDP-supported matching procedures and concluded that they could offer similar matching quality.59 However, they suggested that offering a combination of matching methods is optimal, allowing students to pick the method that suits them best.
Mentors may have one or multiple mentees, and occasionally more than one person may mentor a group of mentees.8,51,52,58,60,63,73 Interestingly, some initiatives use student peer mentoring to support physician mentoring.25,59 Once the relationship has been initiated, mentees and mentors usually meet face-to-face, but increasingly other forms of communication are used, including via email and telephone.9,51,58 Frequency of meetings depends on the aims of the particular program .7,51,58,63,73 Many meetings take place in the clinical or university environment62 but other schemes require meeting outside of work in a neutral environment.12,62 Mentoring activities tend to occur over a substantial period of time to help cultivate successful mentor relationships,7,31 with one study showing that mentees were more likely to share personal problems and socialize with their mentors 6 months after initiation of the program.65
Finally, topics covered at meetings vary significantly, both within one scheme, and when compared with other mentoring programs. Examples include the following: simulation,73 clinical supervision/shadowing,7,9 feedback and discussion on specific mentee selected topics,61,73 ethics,63 career planning,56 and personal development plans;56,62 to highlight but a few. These meetings can be informal or in the form of seminars and tutorials.55 In this way, a range of mentees’ needs can be met by means of a more holistic approach to medical learning.
Evaluating medical mentoring programs
Most mentoring programs are evaluated to some extent but the quality of this evaluation is variable. Many assess short-term impact that are conducted within a short period of time at the end of a program, for example, after a week.29,62,67 Programs that evaluate on a more frequent basis use results to continuously make improvements to the design and delivery of the mentoring initiative.25
Very few initiatives look at long-term effectiveness. One example is the Stanford Medical Youth Science Program, a widening participation program for high school pupils from under-represented minority groups. Its aim is to support these students in developing the skills required for college admission. The program followed 96% of candidates for up to 18 years, with 81% of pupils having earned a 4-year college degree, of which 52% had graduated from medical or graduate school. The authors concluded that 10 years was a sufficient follow-up duration.47
A combination of qualitative and quantitative evaluation is usually undertaken, with the use of surveys being the most common method employed to appraise a program. These include the Likert scale, Yes/No surveys, and open-ended questions.7,61,67 Other methods include focus groups,12,73 and semi-structured,63 and telephone interviews.66 Quantitative analysis usually consists of descriptive analysis. Less commonly, statistical tests, such as the unpaired t-test, chi-squared, and Wilcoxon tests are used,25,60 allowing groups of students to be compared and differences measured.
The sample population for evaluation surveys tends to be mentees or both mentors and mentees.7,9,25,62,67,72 Few look only at the mentors’ perspective.64 Questions are based on expert advice,29 frameworks,74 and literature.7,57,60,63,67 Few are based on previously validated surveys25,29,65 or are piloted before use,8,29,51,66,74 which fails to prove the questionnaire is suitable to be used in this context. Control groups are rarely used to evaluate programs designed for only a subset of the student population,66 thus it is difficult to compare groups and test the true effect of the mentoring provided.
One tool to measure effectiveness is the Kirkpatrick model.75 This evaluation framework has four sequential levels, where information at each level affects the next (Figure 2). If a mentoring program is intended to bring about institutional change, such as an increase in numbers of students being accepted into a speciality, then Level 4 evaluation is needed. However, few mentoring programs do this and next to none look at cost effectiveness. This may be because it is more difficult to evaluate programs as levels increase, despite the value of information increasing at each level.76 Mentoring programs that have evaluated at Level 4 tend to cover objectives related to research and have tangible outcomes, such as number of publications, presentations, awards, and higher degrees.31,50,55,71 Others look at exam success and number of students who later enter a speciality-training program.50,71,73
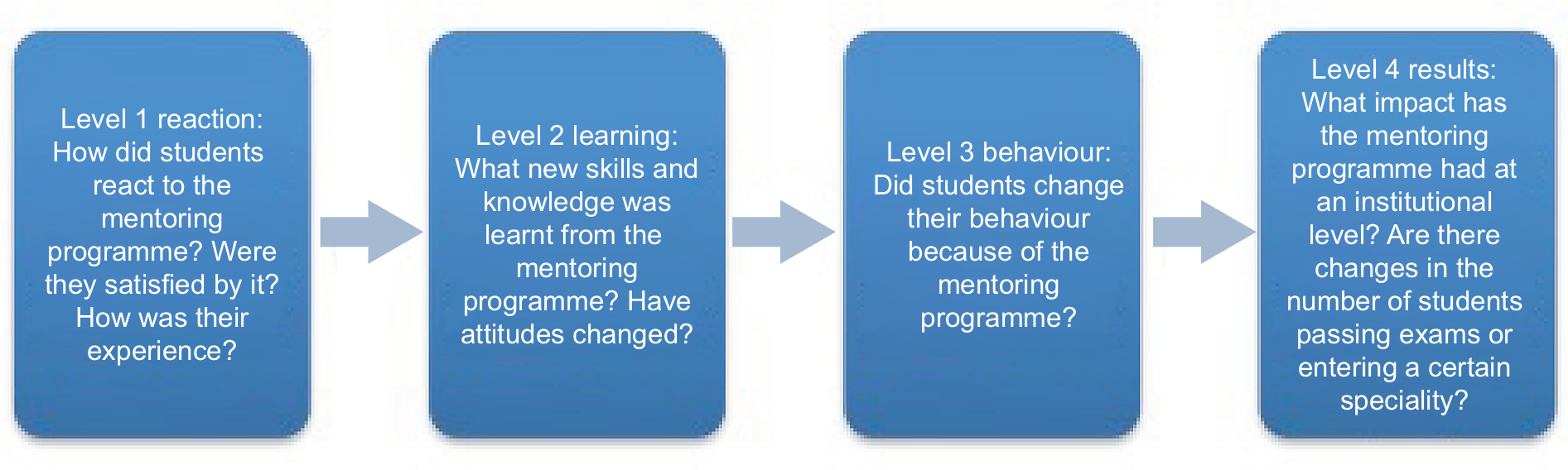 | Figure 2 The Kirkpatrick model. Notes: Adapted from Bewley WL, O’Neil HF. Evaluation of medical simulations. Mil Med. 2013;178(10 Suppl):64–75, by permission of Oxford University Press.76 |
Most programs evaluate at Level 1 and mainly explore mentee satisfaction.29,51,52,55,58,59,61–63,67,70,73 This is unsurprising as it is relatively the easiest form of evaluation to perform. Furthermore, institutions value high satisfaction scores as this can lead to an increase in the number of students applying and enrolling on to courses, thereby increasing revenue.
Some programs evaluate the impact of their initiative by measuring changes in mentees’ knowledge, skills, and attitude (Level 2).8,25,29,52,66 Fewer schemes explore if a change in behavior has occurred as a result of participation in the program (Level 3), for example, if mentees subsequently changed their choice of residency.12,52
On the whole, mentoring programs do well in demonstrating short-term mentee and mentor satisfaction, but few evaluate beyond this to consider the impact at an institutional level. To do so would require clear, measurable outcomes, including cost effectiveness, alongside the use of validated and reliable tools of assessment. Although, this may require time and funding, it would enable an insight into the true long-term benefits of a mentoring initiative.
Benefits of mentoring
Mentoring programs have been shown to be of value to mentees, mentors, and institutions, including medical schools and benefits can be seen in Table 1. Mentoring has been identified as crucial to the retention and recruitment of trainees in medical and surgical specialties, as well as promoting research and academia. One example is a recent study of a research-mentoring program for junior doctors and medical students within a Melbourne cardiothoracic surgery department. The study covered a 10-year period, and reported success in engaging students early in training, with 81% of mentees publishing at least one research article, attainment of scholarships, doctoral degrees, and recruitment to cardiothoracic specialty training. The authors concluded that academic mentoring benefitted not only the individuals’ careers, but also ensured that the unit was able to maintain a high research output.31
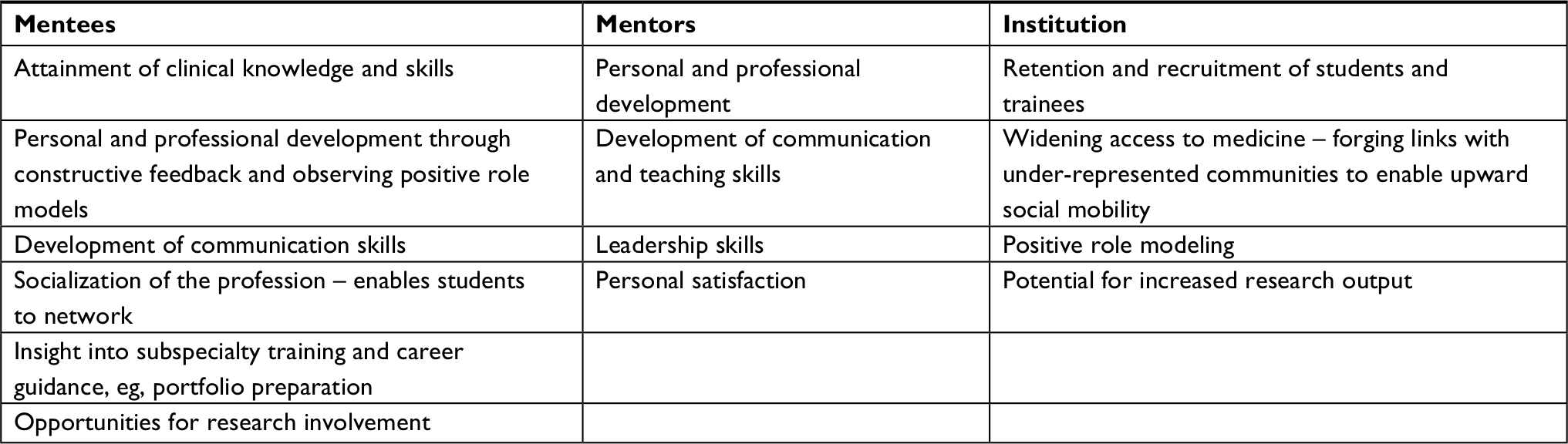 | Table 1 Summary: potential benefits of mentoring |
Similarly, a 2015 study at the Boston School of Medicine evaluated a medical student mentorship program for students keen to pursue a career in neurology. The program provided guidance as well as teaching and research opportunities, and peer teaching/mentoring in the run up to exams. Results included an increase in the number of students entering neurology, as well as an increase in research publications, poster presentations, and a book chapter since the implementation of the program 5 years prior.77
A final example is of a recent trainee-led mentorship program in general surgical recruitment in Ireland. A total of 89% of mentees reported a positive impact on their decision to pursue a surgical career. Other benefits included a self-perceived improvement in technical ability, alongside guidance and information about a career, and training in surgery.78 This study also highlights the benefits of near-peer mentoring, developing a trainee-led program in order to bridge a perceived “generation gap” between consultants and students. Studies in anesthesiology,79 family medicine/primary care,12,80 and plastic surgery81 also report similar academic and recruitment benefits.
Near-peer mentoring is now increasingly prevalent at medical schools and has been shown to have a range of benefits, including improving student’s exam scores,43 acquisition of procedural skills,41,82 and in improving the communication skills and personal and professional development of both mentors and mentees.74,83 Medical students also usually volunteer as mentors, with the incentive that the experience can be included as evidence of teaching in their personal and professional development portfolios. This can also reduce potential departmental reimbursement costs.38,41,43 As previously discussed, widening participation programs also employ the use of near-peer mentoring, with medical students acting as role models and counseling school students from socioeconomically disadvantaged backgrounds. This can, in turn, benefit the institutions’ social accountability agendas, by forging networks with schools from these communities and guiding students toward a career in the medical profession.45,84
Challenges to mentoring
The benefits of mentorship programs are well recognized, however, effective delivery of such programs can face a number of challenges. Challenges can arise from the fact that mentors are often clinician-educators who may not have received adequate training when taking on the role of a mentor. The need to provide mentors with clear expectations of their roles, and equip them with means to develop key listening and feedback skills, as well as knowledge of professional boundaries was highlighted by Ramani et al in “Twelve tips for effective mentors” and remains relevant.22A study of the challenges reported by mentors at the Faculdade de Medicina da Universidade de São Paulo highlighted difficulties surrounding expectations about the mentoring role and activities.85 Similar concerns were also raised by mentors at the University of Washington School of Medicine.86
Moreover, mentee engagement with mentoring can also pose a problem with a number of studies reporting low student participation.83,85 Similarly, a 2018 study of a mentorship program at King Abdulaziz University Faculty of Medicine, Saudi Arabia, reported that group meetings and one-on-one meetings were attended by only 60% and 49% of all students, respectively.87 The authors concluded that sustained mentor and administration staff motivation is prerequisite for a successful mentoring program.
A study of final-year medical student–junior doctor mentorship program at Great Western Hospital, Swindon found that despite 96% of students recommending the scheme, not all students felt that they needed a mentor, and 20% of students chose not to have any contact with their mentor.7 Nevertheless, students have also faced challenges in finding a mentor, particularly in academia – in one study, 44% of students were able to find a suitable research mentor with ease.31 It is, therefore, imperative to identify students who want or need a mentor and assist in matching them with suitable mentors.
Mentors have also reported difficulties in undertaking mentoring sessions alongside their other core commitments, for example, clinical and academic responsibilities, due to time constraints.7,85 In these cases, protected time for mentors may be necessary to cultivate positive mentee–mentor relationships.22
Implication and future of mentoring
Mentoring programs are increasingly recognized in medical schools as crucial components of the curriculum, and can aid in developing students’ professionalism, personal growth, knowledge, and skills. They have also been shown to be of benefit in the retention and recruitment of trainees to under-subscribed specialities, including academic medicine. Medical student mentors are able to develop their teaching and communication skills, as well as contribute to widening access programs that can help to increase diversity in the medical profession.
Design and delivery of these programs can vary significantly, making direct comparisons difficult. Nonetheless, most mentors receive training on appointment, however, may not be reimbursed financially or with protected time for mentoring activities. Furthermore, some students do not feel they need a mentor and this can affect the success of a mentoring relationship and engagement. It is, therefore, important for mentees and mentors to be matched in a way that encourages their relationship to succeed, whether this is by mentees choosing their mentor or using a validated matching tool.
The quality of evaluation that occurs varies. Few programs follow the students over an extended period of time to assess the long-term impact of a mentoring initiative. The majority of programs use surveys to assess students’ experiences and satisfaction, with only a few evaluating tangible outcomes, such as examination results. It is, therefore, hard to establish best practice. Despite this, mentoring has the potential to bring multiple benefits to mentees, mentors, and institutions.
Take-home messages
Finally, in order to develop a sustainable and effective mentoring program, we highlight the following key messages:
- Before a mentoring program is established, a needs analysis or/and pilot should be undertaken to ensure that the design and intended goals are appropriate and achievable.
- Programs should have clear measurable objectives and outcomes, both short and long term.
- Mentees and mentors should be matched in a way that encourages their relationship to succeed. This may be through a validated matching process or mentees choosing their own mentor.
- Mentors should receive training in the requirements of the role and in delivering effective feedback. Incentives should be offered, for example, recognition of mentoring for promotion. Likewise, mentees should be made aware of what is expected of them.
- Protected time should be allocated for mentoring activities to encourage engagement and motivation.
- Evaluation should include the mentee, mentor, and institution, and follow the mentee through an extended period of time to assess long-term impact of the initiative.
- Evaluation should utilize validated methods of assessment.
Disclosure
The authors report no conflicts of interest in this work.
References
Oxford Dictionary. Mentor definition. Oxford: Oxford University Press; 2018. Available from: https://www.oxforddictionaries.com/. Accessed August 10, 2018. | ||
Keshavan MS, Tandon R. On mentoring and being mentored. Asian J Psychiatr. 2015;16:84–86. | ||
Frei E, Stamm M, Buddeberg-Fischer B. Mentoring programs for medical students--a review of the PubMed literature 2000–2008. BMC Med Educ. 2010;10(1):32. | ||
Siddiqui S. Of mentors, apprenticeship, and role models: a lesson to relearn? Med Educ Online. 2014;19(1):25428. | ||
Jacobi M. Mentoring and undergraduate academic success: a literature review. Rev Educ Res. 1991;61(4):505–532. | ||
Rashid P, Narra M, Woo H. Mentoring in surgical training. ANZ J Surg. 2015;85(4):225–229. | ||
Hawkins A, Jones K, Stanton A. A mentorship programme for final-year students. Clin Teach. 2014;11(5):345–349. | ||
Dalgaty F, Guthrie G, Walker H, Stirling K. The value of mentorship in medical education. Clin Teach. 2017;14(2):124–128. | ||
Tran K, Tran GT, Fuller R. West Yorkshire mentor scheme: teaching and development. Clin Teach. 2014;11(1):48–52. | ||
Kollias C, Banza L, Mkandawire N. Factors involved in selection of a career in surgery and orthopedics for medical students in Malawi. Malawi Med J. 2010;22(1):20–23. | ||
Farrell TW, Shield RR, Wetle T, Nanda A, Campbell S. Preparing to care for an aging population: medical student reflections on their clinical mentors within a new geriatrics curriculum. Gerontol Geriatr Educ. 2013;34(4):393–408. | ||
Indyk D, Deen D, Fornari A, Santos MT, Lu WH, Rucker L. The influence of longitudinal mentoring on medical student selection of primary care residencies. BMC Med Educ. 2011;11(1):27. | ||
Zink T, Halaas GW, Finstad D, Brooks KD. The rural physician associate program: the value of immersion learning for third-year medical students. J Rural Heal. 2008;24(4):353–359. | ||
Hoffmann JC, Flug JA. A call to action for medical student mentoring by young radiologists. Curr Probl Diagn Radiol. 2016;45(2):153–154. | ||
Kashkoush A, Feroze R, Myal S, et al. Fostering student interest in neurologic surgery: the University of Pittsburgh experience. World Neurosurg. 2017;108:101–106. | ||
Berger AP, Giacalone JC, Barlow P, Kapadia MR, Keith JN. Choosing surgery as a career: early results of a longitudinal study of medical students. Surgery. 2017;161(6):1683–1689. | ||
Assosication of American Medical Colleges. The hidden curriculum in academic medicine. 2015. Available from: https://www.youtube.com/watch?v=L5V8u9zqFaI. Accessed August 10, 2018. | ||
Feudtner C, Christakis DA, Christakis NA. Do clinical clerks suffer ethical erosion? Students’ perceptions of their ethical environment and personal development. Acad Med. 1994;69(8):670–679. | ||
Satterwhite WM 3rd, Satterwhite RC, Enarson CE. Medical students’ perceptions of unethical conduct at one medical school. Acad Med. 1998;73(5):529–531. | ||
Kirch DG, Gusic ME, Ast C. Undergraduate medical education and the foundation of physician professionalism. JAMA. 2015;313(18):1797–1798. | ||
Elliott DD, May W, Schaff PB, et al. Shaping professionalism in pre-clinical medical students: professionalism and the practice of medicine. Med Teach. 2009;31(7):e295–e302. | ||
Ramani S, Gruppen L, Kachur EK. Twelve tips for developing effective mentors. Med Teach. 2006;28(5):404–408. | ||
Eley DS, Jensen C, Thomas R, Benham H. What will it take? Pathways, time and funding: Australian medical students’ perspective on clinician-scientist training. BMC Med Educ. 2017;17(1):242. | ||
Meijs L, Zusterzeel R, Wellens HJ, Gorgels AP. The Maastricht-Duke bridge: an era of mentoring in clinical research – a model for mentoring in clinical research – a tribute to Dr. Galen Wagner. J Electrocardiol. 2017;50(1):16–20. | ||
Dimitriadis K, von der Borch P, Störmann S, et al. Characteristics of mentoring relationships formed by medical students and faculty. Med Educ Online. 2012;17(1):17242. | ||
Chang Y, Ramnanan CJ. A review of literature on medical students and scholarly research: experiences, attitudes, and outcomes. Acad Med. 2015;90(8):1162–1173. | ||
Funston G, Piper RJ, Connell C, Foden P, Young AM, O’Neill P. Medical student perceptions of research and research-orientated careers: an international questionnaire study. Med Teach. 2016;38(10):1041–1048. | ||
White MT, Satterfield CA, Blackard JT. Essential competencies in global health research for medical trainees: a narrative review. Med Teach. 2017;39(9):945–953. | ||
Devi V, Ramnarayan K, Abraham RR, Pallath V, Kamath A, Kodidela S. Short-term outcomes of a program developed to inculcate research essentials in undergraduate medical students. J Postgrad Med. 2015;61(3):163–168. | ||
O’Sullivan PS, Niehaus B, Lockspeiser TM, Irby DM. Becoming an academic doctor: perceptions of scholarly careers. Med Educ. 2009;43(4):335–341. | ||
Fricke TA, Lee MGY, Brink J, D’Udekem Y, Brizard CP, Konstantinov IE. Early mentoring of medical students and junior doctors on a path to academic cardiothoracic surgery. Ann Thorac Surg. 2018;105(1):317–320. | ||
Faucett EA, McCrary HC, Milinic T, Hassanzadeh T, Roward SG, Neumayer LA. The role of same-sex mentorship and organizational support in encouraging women to pursue surgery. Am J Surg. 2017;214(4):640–644. | ||
O’Connor MI. Medical school experiences shape women students’ interest in orthopaedic surgery. Clin Orthop Relat Res. 2016;474(9):1967–1972. | ||
Rohde RS, Wolf JM, Adams JE. Where are the women in orthopaedic surgery? Clin Orthop Relat Res. 2016;474(9):1950–1956. | ||
Southampton University. Southampton university BM6. 2018. Available from: https://www.southampton.ac.uk/meded/curriculum_design_and_delivery/bm6.page. Accessed July 17, 2018. | ||
Kings College. Kings College extended medical degree programme. 2018. Available from: https://www.kcl.ac.uk/study/undergraduate/courses/extended-medical-degree-programme-mbbs.aspx. Accessed July 12, 2018. | ||
Derck J, Zahn K, Finks JF, Mand S, Sandhu G. Doctors of tomorrow: an innovative curriculum connecting underrepresented minority high school students to medical school. Educ Health (Abingdon). 2016;29(3):259–265. | ||
Smith S, Alexander A, Dubb S, Murphy K, Laycock J. Opening doors and minds: a path for widening access. Clin Teach. 2013;10(2):124–128. | ||
Freeman BK, Landry A, Trevino R, Grande D, Shea JA. Understanding the leaky pipeline: perceived barriers to pursuing a career in medicine or dentistry among underrepresented-in-medicine undergraduate students. Acad Med. 2016;91(7):987–993. | ||
Nicholson S, Cleland JA. “It’s making contacts”: notions of social capital and implications for widening access to medical education. Adv Health Sci Educ. 2017;22(2):477–490. | ||
Garcia-Casasola G, Sánchez FJ, Luordo D, et al. Basic abdominal point-of-care ultrasound training in the undergraduate: students as mentors. J Ultrasound Med. 2016;35(11):2483–2489. | ||
Barker TA, Ngwenya N, Morley D, Jones E, Thomas CP, Coleman JJ. Hidden benefits of a peer-mentored ‘Hospital Orientation Day’: first-year medical students’ perspectives. Med Teach. 2012;34(4):e229–e235. | ||
Taylor JS, Faghri S, Aggarwal N, Zeller K, Dollase R, Reis SP. Developing a peer-mentor program for medical students. Teach Learn Med. 2013;25(1):97–102. | ||
Choudhury N, Khanwalkar A, Kraninger J, Vohra A, Jones K, Reddy S. Peer mentorship in student-run free clinics: the impact on preclinical education. Fam Med. 2014;46(3):204–208. | ||
Karpa K, Vakharia K, Caruso CA, Vechery C, Sipple L, Wang A. Medical student service learning program teaches secondary students about career opportunities in health and medical fields. Adv Physiol Educ. 2015;39(4):315–319. | ||
Azmy J, Nimmons D. Reflections on a widening participation teaching role. Clin Teach. 2017;14(2):139–140. | ||
Winkleby MA. The Stanford Medical Youth Science Program: 18 years of a biomedical program for low-income high school students. Acad Med. 2007;82(2):139–145. | ||
Nimmons D. Developing mentoring skills as a student. Clin Teach. 2016;13(1):72–73. | ||
Al-Khudairi R, Jameie-Oskooei S, Lobo R. Dealing with emotions in medical school: are senior students preferable to mentors? Med Educ. 2017;51(4):452. | ||
Boninger M, Troen P, Green E, et al. Implementation of a longitudinal mentored scholarly project: an approach at two medical schools. Acad Med. 2010;85(3):429–437. | ||
Macaulay W, Mellman LA, Quest DO, Nichols GL, Haddad J, Puchner PJ. The Advisory Dean Program: a personalized approach to academic and career advising for medical students. Acad Med. 2007;82(7):718–722. | ||
McGeehan J, English R, Shenberger K, Tracy G, Smego R. A community continuity programme: volunteer faculty mentors and continuity learning. Clin Teach. 2013;10(1):15–20. | ||
Denunzio N, Parekh A, Hirsch AE. Mentoring medical students in radiation oncology. J Am Coll Radiol. 2010;7(9):722–728. | ||
McLaughlin K, Veale P, McIlwrick J, de Groot J, Wright B. A practical approach to mentoring students with repeated performance deficiencies. BMC Med Educ. 2013;13(1):56. | ||
Yager J, Waitzkin H, Parker T, Duran B. Educating, training, and mentoring minority faculty and other trainees in mental health services research. Acad Psychiatry. 2007;31(2):146–151. | ||
Pinilla S, Pander T, von der Borch P, Fischer MR, Dimitriadis K. 5 years of experience with a large-scale mentoring program for medical students. GMS Z Med Ausbild. 2015;32(1):Doc5. | ||
Fornari A, Murray TS, Menzin AW, et al. Mentoring program design and implementation in new medical schools. Med Educ Online. 2014;19(1):24570. | ||
Meinel FG, Dimitriadis K, von der Borch P, Störmann S, Niedermaier S, Fischer MR. More mentoring needed? A cross-sectional study of mentoring programs for medical students in Germany. BMC Med Educ. 2011;11(1):68. | ||
Schäfer M, Pander T, Pinilla S, Fischer MR, von der Borch P, Dimitriadis K. A prospective, randomised trial of different matching procedures for structured mentoring programmes in medical education. Med Teach. 2016;38(9):921–929. | ||
Singh S, Singh N, Dhaliwal U. Near-peer mentoring to complement faculty mentoring of first-year medical students in India. J Educ Eval Health Prof. 2014;11:12. | ||
Kman NE, Bernard AW, Khandelwal S, Nagel RW, Martin DR. A tiered mentorship program improves number of students with an identified mentor. Teach Learn Med. 2013;25(4):319–325. | ||
Sobbing J, Duong J, Dong F, Grainger D. Residents as medical student mentors during an obstetrics and gynecology clerkship. J Grad Med Educ. 2015;7(3):412–416. | ||
Kalén S, Ponzer S, Seeberger A, Kiessling A, Silén C. Longitudinal mentorship to support the development of medical students’ future professional role: a qualitative study. BMC Med Educ. 2015;15(1):97. | ||
Scheckler WE, Tuffli G, Schalch D, MacKinney A, Ehrlich E. The class mentor program at the University of Wisconsin Medical School: a unique and valuable asset for students and faculty. WMJ. 2004;103(7):46–50. | ||
Lin CD, Lin BY, Lin CC, Lee CC. Redesigning a clinical mentoring program for improved outcomes in the clinical training of clerks. Med Educ Online. 2015;20(1):28327. | ||
Coates WC, Crooks K, Slavin SJ, Guiton G, Wilkerson L. Medical school curricular reform: fourth-year colleges improve access to career mentoring and overall satisfaction. Acad Med. 2008;83(8):754–760. | ||
Bhatia A, Navjeevan S, Dhaliwal U. Mentoring for first year medical students: humanising medical education. Indian J Med Ehtics. 2013;10(2):100–103. | ||
Kostrubiak DE, Kwon M, Lee J, et al. Mentorship in radiology. Curr Probl Diagn Radiol. 2017;46(5):385–390. | ||
Weinstein L. A special programme to revitalise the senior physician while improving the clinical education and mentoring of medical students and residents. BJOG. 2017;124(7):1027. | ||
Martina CA, Mutrie A, Ward D, Lewis V. A sustainable course in research mentoring. Clin Transl Sci. 2014;7(5):413–419. | ||
Areephanthu CJ, Bole R, Stratton T, Kelly TH, Starnes CP, Sawaya BP. Impact of professional student mentored research fellowship on medical education and academic medicine career path. Clin Transl Sci. 2015;8(5):479–483. | ||
Weiner J, Small AC, Lipton LR, et al. Establishing an online mentor database for medical students. Med Educ. 2014;48(5):542–543. | ||
Kalet A, Krackov S, Rey M. Mentoring for a new era. Acad Med. 2002;77(11):1171–1172. | ||
Kalén S, Stenfors-Hayes T, Hylin U, Larm MF, Hindbeck H, Ponzer S. Mentoring medical students during clinical courses: a way to enhance professional development. Med Teach. 2010;32(8):e315–e321. | ||
Smidt A, Balandin S, Sigafoos J, Reed VA. The Kirkpatrick model: a useful tool for evaluating training outcomes. J Intellect Dev Disabil. 2009;34(3):266–274. | ||
Bewley WL, O’Neil HF. Evaluation of medical simulations. Mil Med. 2013;178(10 Suppl):64–75. | ||
Zuzuárregui JR, Hohler AD. Comprehensive opportunities for research and teaching experience (CORTEX): a mentorship program. Neurology. 2015;84(23):2372–2376. | ||
Ahmed O, Nugent M, Cahill R, Mulsow J. Attitudes to trainee-led surgical mentoring. Ir J Med Sci. 2018;187(3):821–826. | ||
Wenzel V, Gravenstein N. Anesthesiology mentoring. Curr Opin Anaesthesiol. 2016;29(6):698–702. | ||
Myhre DL, Sherlock K, Williamson T, Pedersen JS. Effect of the discipline of formal faculty advisors on medical student experience and career interest. Can Fam Physician. 2014;60(12):e607–e612. | ||
Barker JC, Rendon J, Janis JE. Medical student mentorship in plastic surgery: the mentee’s perspective. Plast Reconstr Surg. 2016;137(6):1934–1942. | ||
Jeppesen KM, Bahner DP. Teaching bedside sonography using peer mentoring. J Ultrasound Med. 2012;31(3):455–459. | ||
Stenfors-Hayes T, Kalén S, Hult H, Dahlgren LO, Hindbeck H, Ponzer S. Being a mentor for undergraduate medical students enhances personal and professional development. Med Teach. 2010;32(2):148–153. | ||
Henderson RI, Williams K, Crowshoe LL. Mini-med school for aboriginal youth: experiential science outreach to tackle systemic barriers. Med Educ Online. 2015;20(1):29561. | ||
Gonçalves MC, Bellodi PL. Mentors also need support: a study on their difficulties and resources in medical schools. Sao Paulo Med J. 2012;130(4):252–258. | ||
Dobie S, Smith S, Robins L. How assigned faculty mentors view their mentoring relationships: an interview study of mentors in medical education. Mentor Tutoring Partnersh Learn. 2010;18(4):337–359. | ||
Fallatah HI, Soo Park Y, Farsi J, Tekian A. Mentoring clinical-year medical students: factors contributing to effective mentoring. J Med Educ Curric Dev. 2018;5:2382120518757717. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.