")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Medical Mask Wearing During Treatment for Patients Undergoing Radiotherapy in COVID-19 Pandemic – An Experience of Protocol Setup and Dosimetric Evaluation for Particle/Proton Beam Therapy
Authors Wang YM , Hsieh YW, Huang BS, Sung KC, Juan KJ, Lee SP , Lee SH, Huang EY
Received 12 October 2020
Accepted for publication 19 February 2021
Published 2 March 2021 Volume 2021:14 Pages 869—873
DOI https://doi.org/10.2147/RMHP.S286404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Yu-Ming Wang,1– 4,* Yang-Wei Hsieh,1,2,* Bing-Shen Huang,1,2,5 Kuo-Chiang Sung,1,2 Kuo-Jung Juan,1,2 Steve P Lee,6 Shen-Hao Lee,1,2,5 Eng-Yen Huang1,2
1Department of Radiation Oncology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 2Proton and Radiation Therapy Center, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 3School of Traditional Chinese, Chang Gung University, Taoyuan, Taiwan; 4Institute of Physiology, National Yang-Ming University, Taipei, Taiwan; 5Department of Radiation Oncology, Linkou Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Taoyuan, Taiwan; 6Department of Radiation Oncology, David Geffen School of Medicine, University of California, Los Angeles, CA, USA
*These authors contributed equally to this work
Correspondence: Shen-Hao Lee Email [email protected]
Eng-Yen Huang
Department of Radiation Oncology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
Email [email protected]
Background: The coronavirus disease 2019 (COVID-19) pandemic has caused extreme challenges for the healthcare system. Medical masks have been proven to effectively block disease transmission. Radiotherapeutic departments are at unique risk for disease exposure with the repeated daily treatment schedule. A protocol of mask wearing during daily treatment was established, and the effect of wearing medical masks on dosimetry during proton beam therapy (PBT) was validated.
Methods: A department protocol of medical mask wearing was initiated after the COVID-19 pandemic. Medical masks that were made under standardized specification and regulation were obtained for analyses. The physical and dosimetric characteristics of these medical masks were measured by different proton energies using commercialized measurement tools.
Results: Patients and staff were able to adopt the protocol on a weekly basis, and no adverse events were reported. The average physical thickness of a single piece of medical mask was 0.5 mm with a water equivalent thickness (WET) of 0.1 mm.
Conclusion: Our study revealed that mask wearing for patients undergoing daily radiotherapy is feasible and can provide basic protection for patients and staff. The impact of mask wearing on dosimetry was only 0.1 mm in WET, which has no impact on clinical PBT treatment. A medical mask-wearing policy can be applied safely without dosimetric concerns and should be considered as a standard practice for PBT centers during the COVID-19 pandemic.
Keywords: COVID-19, mask-wearing, radiotherapy, dosimetry, proton beam therapy
Introduction
The coronavirus disease 2019 (COVID-19) outbreak started in late 2019 and soon became a worldwide pandemic, as announced by the World Health Organization in March 2020.1 To date, more than 37 million people have been confirmed to have had the disease, which caused more than 1 million deaths worldwide.2 This pandemic led to considerable challenges for healthcare units and professionals.3 Different policies have been established in different countries and institutions to prevent possible transmission of the disease and to reduce the damage caused by the disease. Here, in our country, the practice of wearing a medical mask for every person entering hospitals has been recommended since late Jan 20204 to prevent the transmission from communities to hospitals, which could subsequently lead to nosocomial infection of patients and healthcare workers.
Medical masks are thin textiles manufactured following standard specifications and regulations, such as CNS14774 in Taiwan, ASTM F2100 in the United States, and EN14683 in the European Union. This waterproof device made of three layers of nonwoven fabrics was designed for medical use to prevent contamination and infection from fluid, droplets, and aerosols carrying pathogens. With the relatively low cost of medical masks and the high filter rate of pathogens compared to the cost of the treatments required for COVID-19 infection, medical mask wearing represents a very cost-effective practice during this pandemic.5
However, it was not a standard practice for patients to wear medical masks during their course of radiotherapy (RT) prior to the COVID-19 pandemic. Radiation oncology departments need to establish protocols in response to the pandemic and to incorporate the protocol into daily practice. In addition to establishing institutional protocols, considerations about the impact of dosimetry were also raised for patients during proton beam therapy (PBT) when treatment beams passing through a medical mask were unavoidable. To the best of our knowledge, no previous studies have been conducted to evaluate the dosimetric impact.
The study objective in this report was to investigate the feasibility of medical mask wearing during PBT treatment, particularly during the COVID-19 pandemic. A series of dosimetric evaluations with different proton beam energies were conducted to investigate the dosimetric changes and possible impact on medical mask wearing during the daily PBT treatment in the clinic. In addition, we also reported our department protocol and our experience with a medical mask-wearing policy for patients undergoing RT since the start of the pandemic.
Materials and Methods
Medical Mask-Wearing Protocol in Our Department
Before the start of an RT course, all patients were informed of the mask-wearing policy during the initial consultation. For patients whose RT fields were outside the mask area on the face, there were only minimal changes in routine practice. Patients underwent immobilization device preparation, computed tomography (CT) simulation, and treatment as routine except they wore a medical mask during the entire procedure and at every visit.
For patients requiring RT to the head and neck (HN) region, such as for HN cancer or brain tumors, or clinical scenarios that require HN region immobilization devices, additional instructions and explanations were provided at the initial consultation by the treating physician. With the standard specifications and regulations of medical masks in Taiwan,6 the differential pressure of the mask is less than 5 mm-H2O/cm2, and the risk of breathing difficulties were negligible for patients with voluntary breathing.
During the preparation of the HN immobilization devices, the metal stick of the medical mask designed for nose clipping was removed by the therapist to avoid possible activation following local PBT. HN immobilization devices, typically a thermoplastic cast, were made to cover the HN region with the mask on the patients’ face. The outside contour of the mask was marked on the cast. Then, the mask became part of the patients’ immobilization device and went along with the cast during patients’ CT simulation and following daily treatment. During daily treatment, patients were carefully immobilized with their own customized devices and the mask. Then, onboard images were obtained to adjust all setup errors before PBT delivery.
Medical Mask Measurement and Dosimetry for PBT
The physical thickness of the medical mask was repeatedly measured using a commercialized electronic Vernier caliper (Figure 1), and an average of the physical thickness was then documented. Since the physical thickness of a single piece of medical mask is too thin to be visualized on a CT simulation and for dosimetric evaluation, ten pieces of medical masks were tightly packed together for subsequent dosimetry analysis.
 |
Figure 1 Measurement of the physical thickness of a single piece of medical mask using a commercialized caliper. |
The PBT facility in our institution was designed and manufactured by a commercialized company (Sumitomo Heavy Industries, SHI, Japan). Proton energies that coincide with those generated for clinical use range from 70 to 230 MeV. Five different proton energies, including 70 MeV, 110 MeV, 150 MeV, 190 MeV, and 220 MeV, were chosen to evaluate the corresponding water equivalent thickness (WET) change by delivering the beam directly through the 10-piece mask pack. A commercialized detector with multilayer ionization chambers (Giraffe, IBA Dosimetry, Schwarzenbruck, Germany) was used to record the percent dose range of 90% (R90) and 80% (R80) shifts (Figure 2); thus, the WET of the medical masks was generated.
 |
Figure 2 Measurement of the water equivalent thickness of medical masks in 10-piece packs. |
Results
Daily Practice of Mask Wearing
At the time of this manuscript writing, no adverse events were reported in our department. With good communication and cooperation between personnel inside our department, routine practice changes following our mask-wearing protocol were achieved within less than one week for patients with treatment outside the mask-wearing area. For patients who needed RT or immobilization devices over the HN region, another week was adopted until our dosimetric reports and internal discussions were completed.
Medical Mask Measurement and Dosimetry for PBT
Three different regions on a single mask were measured, and 10 pieces of masks were used to repeat the same measurements. The physical thickness of a single piece of medical mask was 0.505±0.021 mm (mean±SD).
The results of the range shift by the 10-piece medical mask pack are shown in Table 1. In brief, the WET with a 10-piece pack of medical masks remained almost unchanged between different energies. The average WET of a single piece of medical mask was 0.095±0.010 mm.
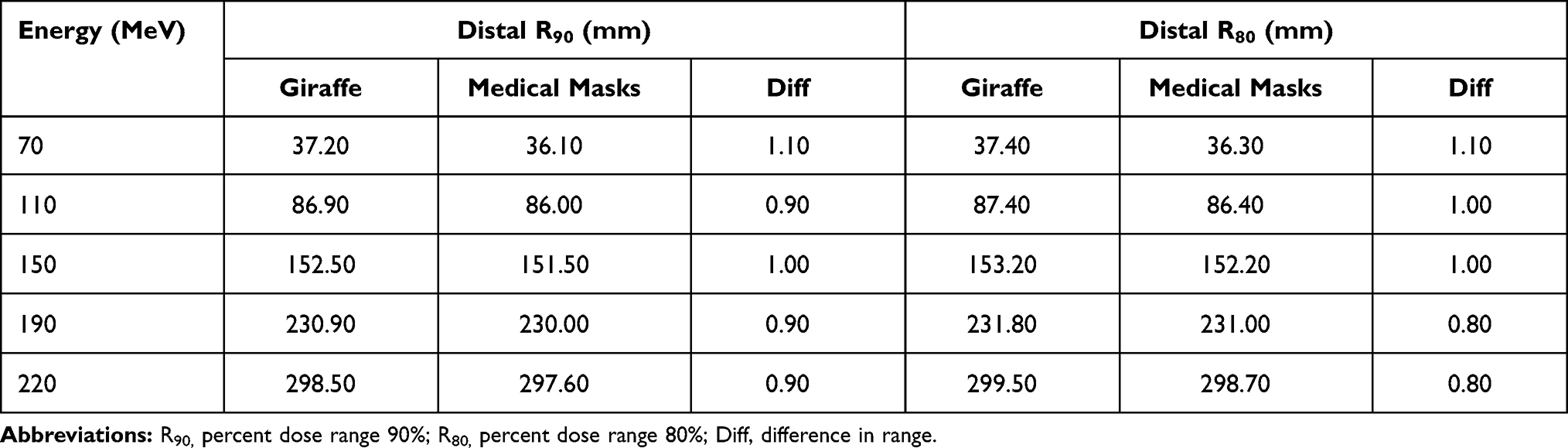 |
Table 1 Measurement of Water Equivalent Thickness (WET) for Medical Masks (in 10-Piece Pack) |
Discussion
The results of this study on our protocol demonstrated that medical mask wearing for patients undergoing radiotherapy is feasible, even for patients with HN cancer, brain tumors, and immobilization devices that need to cover the area of the mask. In addition, with respect to the possible dosimetric influence on PBT for patients wearing medical masks, our results showed a constant WET change of 0.1 mm per medical mask among different proton beam energies. Given that it is difficult to visualize and contour the mask on a simulation CT scan with only 0.5 mm physical thickness, this WET of 0.1 mm serves as an evidence-based reference for clinics with particle therapy/PBT facilities.
Recent research has reported that the viral load of COVID-19 patients can be high during their asymptomatic phase, and these patients can start to transmit the virus as asymptomatic carriers.7,8 These facts put healthcare workers exposed to the coronavirus at unpredictable risk. In addition, staff in the Department of Radiotherapy/Radiation Oncology may have an even higher risk for exposure because of our unique situation:9 a daily treatment schedule that requires repeated exposures to patients and the environment, a treatment time of at least 15–20 minutes per fraction and close contact with the therapist with the patients lead to meaningful exposure risks. Actions and protocols to protect our staff and patients are reasonable and should be taken.
The benefit of mask wearing for medical staff is undoubted.10 However, controversies of its benefit do exist for wearing masks in the community; thus, mask wearing during radiotherapy has never been a protocol in our institution until the start of the COVID-19 pandemic. Given that the major transmission route of coronavirus is the droplets and aerosols from COVID-19 patients, blocking droplets and aerosols that are released from patients’ upper aerodigestive route, the nose and the mouth, may represent an effective method to minimize the risk of contamination.11,12 Medical masks manufactured under standardized regulations and thin enough for use with radiotherapeutic immobilization devices serve as cost-effective tools for clinical radiation oncology scenarios. After thorough discussions inside our department, medical mask-wearing protocols were first initiated for patients without HN region immobilizers and then further applied to patients using HN region immobilization devices.
Worries about the safety, tolerance, and compliance of cancer patients wearing a mask during RT can be concerns. However, a difference in pressure across a certified medical mask of less than 5 mm H2O/cm2 in Taiwan is estimated to have a value of only 1% of the inspiratory pressure in adults;13 therefore, we proposed that it is safe for our patients. Careful protocol information, explanation, and communication at the initial consultation, during simulation procedures, and during daily treatment by the staff are mandatory. With an average daily treatment volume of more than 200 patients in a medical center such as ours, the patients tolerated our protocol well, and no adverse events were reported.
For PBT, the dosimetry levels of beams directly passing through the mask are important for treatment plans and delivery with our protocol. This study on WET of medical masks was conducted and served as evidence before we started to use the protocol for HN region treatment. Currently, in our practice, we try to avoid beams directly passing through the mask region. However, for patients whose beams pass through the mask, the 0.1 mm WET change is taken into consideration and can typically be neglected during PBT plan optimization and evaluation.
Currently, there is a lack of an optimal treatment strategy for COVID-19, and different research regarding this issue has been started.14 It has been proposed that low-dose RT to the lung might be helpful and is now being conducted in clinical trials.15,16 The results are pending; however, RT has been in the front-line of the battle. The actual quantitative benefit that may be gained by medical mask wearing is currently unknown, but this protocol offers feasible and cost-effective protection for medical staff, the treatment environment, and patients during daily RT practice in this difficult time.
There are several limitations of this study. First, the dosimetric change in PBT because of mask wearing was 0.1 mm WET, which can be neglected during practice; however, clinical outcomes during this pandemic should be further evaluated. Second, the feasibility of mask wearing for patients with respiratory distress was not studied. Third, the psychologic and emotional impact, such as for patients with claustrophobia, needs to be further investigated.
Conclusion
Medical mask wearing for all patients undergoing RT is feasible for clinical practice. Based on our study, the concern about mask wearing influencing dosimetry, even with the beam passing directly through the mask, was 0.1 mm in WET and can be neglected during daily practice for PBT and particle therapy treatment. Our protocol may serve as a basic protection method in addition to personal protective equipment for daily practice during the COVID-19 pandemic.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Coronavirus disease 2019 (COVID-19) situation report – 51; 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10pdficon.
2. World Health Organization. Coronavirus disease (COVID-19) pandemic; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
3. Haleem A, Javaid M, Vaishya R. Effects of COVID-19 pandemic in daily life. Curr Med Res Pract. 2020;10(2):78–79. doi:10.1016/j.cmrp.2020.03.011
4. Taiwan Centers for Disease Control. Government recommendation: mask-wearing for all person entering hospitals; 2020. Available from: https://www.cdc.gov.tw/Bulletin/Detail/PmzbJfskvJF2crtxBJ0fqg?typeid=9.
5. Rab S, Javaid M, Haleem A, Vaishya R. Face masks are new normal after COVID-19 pandemic. Diabetes Metab Syndr. 2020;14(6):1617–1619. doi:10.1016/j.dsx.2020.08.021
6. Taiwan Food and Drug Administration. COVID-19 mask Q&A; 2020. Available from: https://www.fda.gov.tw/tc/includes/GetFile.ashx?id=f636973161683844034.
7. Lai CC, Liu YH, Wang CY, et al. Asymptomatic carrier state, acute respiratory disease, and pneumonia due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): facts and myths. J Microbiol Immunol Infect. 2020;53(3):404–412. doi:10.1016/j.jmii.2020.02.012
8. Wolfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581(7809):465–469. doi:10.1038/s41586-020-2196-x
9. Mukherjee RK, Back MF, Lu JJ, Shakespeare TP, Wynne CJ. Hiding in the bunker: challenges for a radiation oncology department operating in the severe acute respiratory syndrome outbreak. Australas Radiol. 2003;47(2):143–145. doi:10.1046/j.0004-8461.2003.01165.x
10. Ma QX, Shan H, Zhang HL, Li GM, Yang RM, Chen JM. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020;92(9):1567–1571. doi:10.1002/jmv.25805
11. Anfinrud P, Stadnytskyi V, Bax CE, Bax A. Visualizing speech-generated oral fluid droplets with laser light scattering. N Engl J Med. 2020;382(21):2061–2063. doi:10.1056/NEJMc2007800
12. Meselson M. Droplets and aerosols in the transmission of SARS-CoV-2. N Engl J Med. 2020;382(21):2063. doi:10.1056/NEJMc2009324
13. Black LF, Hyatt RE. Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Respir Dis. 1969;99(5):696–702. doi:10.1164/arrd.1969.99.5.696
14. Haleem A, Javaid M, Vaishya R, Deshmukh SG. Areas of academic research with the impact of COVID-19. Am J Emerg Med. 2020;38(7):1524–1526. doi:10.1016/j.ajem.2020.04.022
15. Kirkby C, Mackenzie M. Is low dose radiation therapy a potential treatment for COVID-19 pneumonia? Radiother Oncol. 2020.
16. ClinicalTrials.gov. Radiation eliminates storming cytokines and unchecked edema as a 1-day treatment for COVID-19; 2020. Available from: https://ClinicalTrials.gov/show/NCT04366791.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.