")
Back to Journals » International Journal of Women's Health » Volume 6
Medical factors influencing decision making regarding radiation therapy for breast cancer
Authors Dilaveri C, Sandhu N, Neal L, Neben-Wittich M, Hieken T, Mac Bride M, Wahner-Roedler D , Ghosh K
Received 23 July 2014
Accepted for publication 26 September 2014
Published 20 November 2014 Volume 2014:6 Pages 945—954
DOI https://doi.org/10.2147/IJWH.S71591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Christina A Dilaveri,1 Nicole P Sandhu,1 Lonzetta Neal,1 Michelle A Neben-Wittich,1,2 Tina J Hieken,3 Maire Brid Mac Bride,1 Dietlind L Wahner-Roedler,1 Karthik Ghosh1
1Division of General Internal Medicine, 2Department of Radiation Oncology, 3Division of Subspecialty General Surgery, Mayo Clinic, Rochester, MN, USA
Abstract: Radiation therapy is an important and effective adjuvant therapy for breast cancer. Numerous health conditions may affect medical decisions regarding tolerance of breast radiation therapy. These factors must be considered during the decision-making process after breast-conserving surgery or mastectomy for breast cancer. Here, we review currently available evidence focusing on medical conditions that may affect the patient–provider decision-making process regarding the use of radiation therapy.
Keywords: cardiac devices, connective tissue disease, prior radiation
Introduction
Radiation therapy (RT) is an important and effective adjuvant treatment for breast cancer.1,2 Whole-breast radiation is a standard recommendation after breast-conserving surgery, whereas chest wall radiation is performed for select patients after mastectomy. Whole-breast radiation is associated with improved survival and reduced risk of locoregional recurrence after lumpectomy.1 Postmastectomy radiation reduces locoregional recurrence risk and improves survival2 in patients with metastatic disease in axillary lymph nodes or with primary breast malignancies less than 5 cm.3,4
Surgical decision making is a significant challenge for women with newly diagnosed breast cancer. Underlying medical issues may introduce additional complexity. Indwelling cardiac devices, a history of RT, or underlying medical or genetic disorders may all affect patient tolerance of RT, and these factors must be considered in surgical decision making. In this review of the literature, we describe potential medical factors that affect the use of adjuvant RT in the setting of a breast cancer diagnosis and provide the best current medical evidence that can be used to assist providers and their patients in the surgical decision-making process (Table 1).
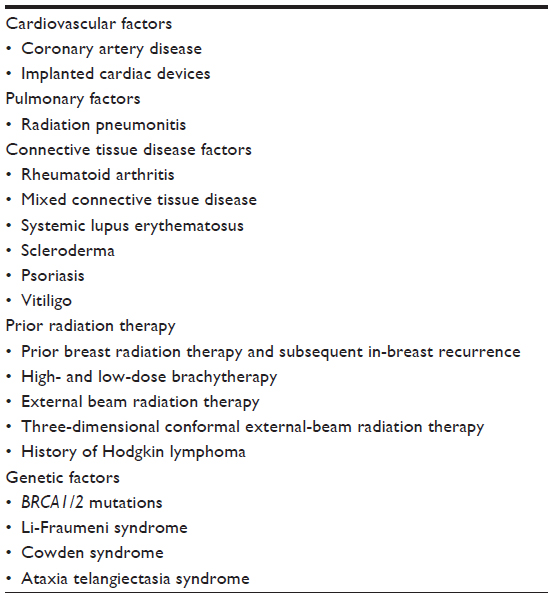 | Table 1 Medical factors influencing decision making regarding radiation therapy for breast cancer |
Methods
For this review, we conducted a PubMed search, English language only, with no date limitations, followed by abstract review of select relevant articles. The following search terms or combination of terms was used: radiation, breast cancer, complications, prior radiation, Hodgkin lymphoma, implanted cardiac devices, coronary artery disease, radiation pneumonitis, connective tissue disease (CTD), rheumatoid arthritis (RA), scleroderma, systemic lupus erythematosus, psoriasis, vitiligo, genetic mutation, BRCA1/2, Li-Fraumeni syndrome, and Cowden syndrome. The influence of RT on these factors and disease processes and its impact on decision making is summarized in this paper.
Cardiovascular factors
Tangential fields used with standard whole-breast RT for left-sided breast cancer may affect the heart and result in delayed complications from RT. Modern RT techniques have successfully reduced but not yet totally eliminated potential cardiac effects.5–7 As part of the surgical decision-making process, patients and providers must be made aware of potential adverse effects of adjuvant breast RT so that they may ameliorate cardiac complications and guide future management of cardiac risk factors.
Coronary artery disease
The potential for cardiac damage from RT was identified in a 1994 report that showed breast cancer survivors treated with RT for 10 or more years earlier had excess overall mortality from adverse cardiac effects.8 Studies have shown that patients treated with RT before 1995 had increased rates of cardiovascular disease. Patients receiving left-sided treatment had the most significant cardiac effects,9,10 with a latency of 10 to 20 years. Patients treated from 1973 through 1979 had a 15-year cardiac mortality rate of 13%. Patients treated from 1985 through 1989 had a 15-year cardiac mortality rate of 5.5%. Further improvements in delineating and avoiding cardiac radiation should continue to improve survival. Anticipating the risk of current techniques is difficult, given the apparent latency period of at least 10 years before clinical outcomes become evident. However, a modern study that defined cardiac risk based on dose and treatment volume of the heart shows the excess cardiac events appear to be closer to 0.5% to 3% greater than for age-matched controls if the dose to the heart is minimized with computed tomographic planning and modern techniques.7
Additional factors can influence the risk of cardiovascular complications after RT for breast cancer. The combination of RT and chemotherapy has a higher risk of cardiovascular complications than RT alone.5 A similar increase in cardiovascular complications is seen in smokers undergoing RT compared with nonsmokers.10 However, other studies have not shown adverse cardiovascular effects from RT. Wang et al11 reported that among patients receiving RT who subsequently underwent coronary angiography (median, 4.2 years later), patients with left-sided breast cancer did not have increased risk of coronary artery disease compared with patients with right-sided disease. The authors of that study acknowledged that they could not exclude late development of coronary stenosis. In another study, Park et al12 reported no significant difference in cardiac events in an average of 8 years after RT for left-sided vs right-sided ductal carcinoma in situ, but the authors noted that longer follow-up is needed to evaluate late events. These reports did not evaluate the incidence of cardiac events in patients not receiving RT. In a report assessing the location of disease after RT, coronary stenosis was observed most often in the left anterior descending and diagonal artery, indicating a direct association between the RT field and stenosis location.13 The above data support use of RT after breast-conserving surgery but also suggest that it is prudent for providers to educate patients about ongoing measures to reduce long-term cardiac risk factors.
No studies have evaluated the risk of worsening existing coronary artery disease in women undergoing RT for breast cancer. However, the magnitude of increased risk of coronary disease appears to be independent of preexisting risk factors.7 Currently, no guidelines suggest withholding RT from women with underlying coronary artery disease who desire breast-conserving therapy.
Implanted cardiac devices
Implantable cardiac pacemakers (ICPs) or implantable cardioverter-defibrillators (ICDs) introduce additional complexity because they are sensitive to radiation. Guidelines for management of patients with ICPs requiring RT were published in 199414 but have not been updated and do not address ICDs or modern RT modalities. The majority of data regarding the impact of RT on ICPs and ICDs is from case reports and small case series. The lack of a large body of evidence is compounded by the seemingly conflicting findings of some authors who identified harmful effects15,16 and others who did not,17,18 particularly when the device was outside the treatment field or when pretreatment device relocation was undertaken. Nevertheless, adverse effects have been reported, even when the device is located outside the treatment field.16 A retrospective study of 33 patients with an ICD who received RT15 was prompted by a patient with prostate cancer who was found to have a malfunctioning ICD. Subjects were treated from 2005 through 2007 at Memorial Sloan-Kettering Cancer Center and either had the device relocated or the treatment dose limited. Only one patient had an adverse device effect. A retrospective review of Mayo Clinic patients undergoing RT from 2002 through 2007 with the device outside the therapeutic field also found no evidence of reset or malfunction during or after RT.19 The authors concluded that malfunction or device reset due to scatter radiation is likely a rare, unpredictable occurrence.
Patients with breast cancer receiving RT generally are accepted to have some risk of adverse device effects, and appropriate precautions therefore should be taken before starting RT. Implanted cardiac devices are not considered a contraindication to breast RT; we recommend that the device be relocated outside of the treatment field whenever possible, and dose limits should not be exceeded. Close collaboration with a cardiologist can determine device dependency and need for safe device relocation. A minimum distance from the treatment field has not been established, although one group suggests at least 4 cm.20 Many device manufacturers publish recommended device radiation dose limits. Patients should be closely monitored by device function evaluation before, during, and after RT.
Pulmonary factors
Radiation pneumonitis is a known potential adverse effect of pulmonary RT.21,22 Symptomatic radiation pneumonitis occurs in less than 1% of all patients undergoing breast RT and generally occurs 4 to 12 weeks after therapy is complete.5,23 Most patients have a self-limited course that does not require treatment, and corticosteroid treatment is rarely required in patients with persistent symptoms. Although lung changes are typically localized to the irradiated area, exceptionally rare instances of extensive radiation pneumonitis have been reported.24,25 Risk does seem to be associated with the type of treatment. In patients receiving tangential radiation, the risk of grade 2 pneumonitis (symptomatic, medical intervention indicated, limiting instrumental activities of daily living) was 0.2% vs 1.3% in patients receiving comprehensive nodal radiation, which included the internal mammary chain.26 Long-term pulmonary function is generally unaffected.5
In general, no pulmonary conditions absolutely contraindicate use of RT for breast cancer. In view of the potential for pulmonary complications, lung comorbidities should be noted in the evaluation of patients with breast cancer.
Connective tissue disease factors
Controversy is ongoing regarding risk of RT-related toxicity in patients with CTD. The degree of toxicity may vary significantly, depending on lymphovascular involvement of the specific CTD process, the presence of collagen deposition in subcutaneous fat, and intimal involvement of the vascular system. Most of the available information is from studies that included a wide range of patients receiving RT for various malignancies.
Rheumatoid arthritis
Morris and Powell27 reviewed the records of 209 patients with CTD treated with RT from 1960 through 1995. Average follow-up was longer than 6 years (range, 2 months to 32 years). Of these, 131 patients (60%) had RA. Those without RA had diagnoses such as systemic lupus erythematosus (SLE), polymyositis or dermatomyositis, scleroderma or “calcinosis, Raynaud, esophagus, sclerodactyly, telangiectasia” (CREST) syndrome, ankylosing spondylitis, juvenile RA, discoid lupus, and mixed CTD (MCTD). Approximately 10% of patients in both groups had a diagnosis of breast cancer. Patients received 10 to 87.6 Gy of RT (mean, 45 Gy). The authors concluded that acute effects of mucositis, dysphagia, and skin changes were similar in both groups. Patients with RA had late effects, such as cardiac toxicity, small-bowel obstruction, and tissue fibrosis or necrosis, commensurate with a normal population undergoing RT, whereas patients with non-RA connective tissue disorders had a high risk of significant late toxicity (6% vs 21% at 5 years [P=0.002]). Late toxicity in these patients included toxicity to the bowel and pelvic organs, tissue fibrosis or necrosis, and central nervous system toxicity. The toxicity was confined to the radiation field and depended on the area treated. Patients who used nonsteroidal anti-inflammatory drugs during RT had a lower risk of late RT-related complications (6% vs 11% [P=0.04]). Patients using corticosteroids, high-dose salicylates, or methotrexate had a lower risk of late RT complications than those not receiving medical therapy during RT, but these were not statistically significant differences.28 RT dose, tobacco use, and nonmalignant comorbidities had no significant impact on acute or chronic toxicities related to RT.
Ross et al28 undertook a similar matched-pair case-control study and noted only a nonsignificant increase in acute and chronic effects of RT in patients with CTD. However, the number of patients with breast cancer was not clearly identified in this study. Thus, underlying RA does not appear to be a contraindication to RT for breast cancer.
Mixed connective tissue disease
Mayr et al29 described a patient with MCTD who had severe skin toxicity associated with RT for occult breast cancer with axillary presentation. This patient had early, severe, prolonged, and moist desquamation (injury to the basal layer of the epidermis). Additionally, late RT changes of fibrosis developed; they were thought to be caused by vascular injury within the dermis and typical of similar changes noted in the setting of systemic sclerosis and SLE. Although the data are insufficient to determine the impact of RT in patients with MCTD and breast cancer, we advise that such patients with MCTD be educated about the lack of evidence regarding the safety of RT when considering breast-conserving therapy.
Systemic lupus erythematosus
A large series by Pinn et al30 described 21 patients with SLE treated with varying types of RT for malignancy between 1985 and 2003. Two patients had breast cancer, and one was noted to have grade 2 desquamation. The authors concluded that SLE did not preclude the use of RT.
Scleroderma
Gold et al31 studied 20 patients with systemic scleroderma treated with RT from 1980 through 2003 to identify treatment-related toxicities. Average follow-up was 4.7 years (range, 4–22.6 years), and of the three patients with breast cancer, one had chest wall radiation and two received orbit and spine radiation. Limited acute toxicity developed in three patients, but pronounced acute skin reactions (greater than grade 3) was not noted. Furthermore, grade 1 or 2 late toxicity of tissue fibrosis, necrosis or ulceration, xerostomia, and hyperpigmentation were noted in 12 patients. Grade 3 or higher toxicity occurred in four patients and included ileus and wound infection; one patient with esophageal cancer had severe mediastinal fibrosis. In another study investigating 36 patients with CTD who received radiation after lumpectomy for breast cancer, the four patients with scleroderma had a significantly increased incidence of RT-related complications of marked fibrosis in the treatment field, leading to the need for mastectomy in two of the three patients with severe late complications.32 Thus, for patients with scleroderma, consultation with a radiation oncologist and rheumatologist, to discuss risks and benefits of RT, should be undertaken before surgical decision making.
Psoriasis
Charalambous and Bloomfield33 reported a case of exacerbation of psoriasis after palliative breast RT for metastatic adenocarcinoma. They discussed the Koebner phenomenon (KP), which is the skin changes (vitiligo or psoriasis in this case) that develop in areas of previously unaffected skin, due to skin trauma (eg, from radiation, physical trauma, surgical incisions, psoralen-ultravioletA, or sunburn). KP is also known as an isomorphic response because the skin changes noted in damaged areas are reflective of those elsewhere on the body. Psoriasis is most commonly associated with the isomorphic response and has a reported incidence of 38% to 76%, occurring 7 to 14 days after the injury.34 Other skin conditions, including vitiligo, lichen planus, and active eczema, are associated with KP but to a lesser degree. With the advent of skin-sparing external-beam RT, the incidence of KP has decreased compared with several decades ago. For patients with psoriasis who prefer a lumpectomy, we recommend consultation with a radiation oncologist before surgical decision making.
Vitiligo
In 2007, Munshi et al35 described a 42-year-old woman with untreated vitiligo who had RT-induced depigmentation. After a modified radical mastectomy and adjuvant chemotherapy, she received 45 Gy to the chest and axilla over 4 weeks. At her 6-month follow-up evaluation, she reported depigmentation in the irradiated fields. This example of KP was believed to be caused by radiation-induced apoptosis of susceptible melanocytes. Several cases have been reported, and the possibility of depigmentation should be discussed between the patient and the radiation oncologist.
Prior radiation therapy
When evaluating a patient with newly diagnosed, early-stage breast cancer who is considering breast conservation, a careful history regarding previous chest RT must be obtained as part of surgical decision making.
Prior breast radiation therapy and subsequent in-breast recurrence
Approximately 10% of patients treated with lumpectomy and RT will have in-breast recurrence during long-term follow-up those with favorable tumor biology have a less than 5% risk of recurrence, but those with unfavorable biology have closer to a 10% risk.36,37 Mastectomy is the standard of care for cancer in a previously irradiated breast because another course of RT is contraindicated (unacceptable soft-tissue toxicity). However, many women prefer repeating breast-conserving measures for in-breast recurrence. A limited number of publications have reported patient outcomes after a second lumpectomy followed by RT, usually in patients refusing mastectomy. The radiation techniques used include low-dose-rate brachytherapy (in which the radiation source is positioned in the breast using radioactive seeds),38,39 high-dose-rate brachytherapy (in which catheters are loaded with an isotope, such as iridium 192, and inserted into the breast),39,40 or external-beam RT.41 Brachytherapy and partial breast radiation techniques may be feasible in some patients, but their use depends on multiple patient and tumor factors.
Low-dose-rate brachytherapy
Chadha et al38 described 15 patients with localized breast lesions who underwent a second lumpectomy and received low-dose brachytherapy. The first six patients received a dose of 30 Gy. With no unacceptable acute toxicity observed, the brachytherapy dose was increased to 45 Gy. The authors reported low complication rates after a median follow-up of 36 months, a high rate of local control, and freedom from mastectomy. The cosmetic results were described as good to excellent for all patients. Trombetta et al39 examined the feasibility of using the MammoSite® brachytherapy applicator in the retreatment of three patients with breast cancer that was previously irradiated. With a mean follow-up of 32 months, no patient had a local recurrence develop, and cosmesis was reported as excellent. Dosimetric calculations demonstrated that the device facilitated appropriate local irradiation, while sparing the previously irradiated skin of the involved breast.
Experience with low-dose-rate brachytherapy has also been reported in a French study.42 Sixty-nine patients (14.6% of all patients presenting with a local recurrence) underwent a second lumpectomy and partial breast irradiation. Toxicity and dose were clearly associated, with grade 2 and 3 complication rates of 0%, 28%, and 32% with brachytherapy doses of 30 Gy, 45 to 46 Gy, and 50 Gy, respectively. Although 27.5% had no long-term adverse effects (grade 0), 50.7% experienced grade 1 (toxicity not requiring symptomatic medical treatment), 11.6% had grade 2 (toxicity requiring symptomatic medical treatment), and 10.2% had grade 3 (toxicity requiring surgical intervention) effects. The complications observed were as follows (some patients had several complications): fibrosis in 16 cases (23.2%), breast retraction in six cases (8.7%), telangiectasia in five cases (7.3%), necrosis requiring surgery in two cases (2.9%), association between the above complications in 15 cases (21.7%), and other complications in six cases (8.7%). The authors concluded that repeat conservative treatments for local relapse is feasible and gave results comparable with standard mastectomy.
High-dose-rate brachytherapy
Few data are available regarding the use of high-dose-rate brachytherapy for retreatment. Preliminary experience in three patients previously treated with external beam RT and retreated using the MammoSite brachytherapy device between 2004 and 2007 was published by Trombetta et al.39 Two patients were treated for an ipsilateral breast tumor recurrence after breast-conserving treatment, whereas the third patient had an in-field breast cancer develop that likely was associated with mantle irradiation 27 years before. During a mean follow-up of 32 months, no patient had a local recurrence. Cosmesis was reported as excellent in all patients. Dosimetric calculations demonstrated that the device facilitated appropriate local irradiation, while sparing the previously irradiated skin of the involved breast, as defined by the protocol standard.
Guix et al40 described 36 patients with in-breast recurrence measuring less than 3 cm in diameter after breast-conserving therapy for breast cancer treated with wide local excision and RT between 1990 and 2001. Special attention was paid to local, regional, or distant recurrences, survival, cosmesis, and adverse effects. During follow-up, ranging from 1–13 years, eight patients presented with metastases (two regional and six distant) as their first site of failure. Cosmetic results were satisfactory in 90.4% of the patients evaluated. No patient had grade 3 or 4 adverse effects. Of the eleven patients for whom follow-up for at least 10 years was obtained, only one had undergone mastectomy, and overall survival was 96.7%, with 64.4% having disease-free survival.
External-beam radiation therapy
Deutsch41 described 39 women with an in-breast recurrence after lumpectomy and breast RT (invasive carcinoma, n=31; ductal carcinoma in situ, n=8) who were treated with excision of the in-breast recurrence and RT. The estimated overall 5-year survival rate was 77.9%. Twelve patients had excellent or very good cosmetic results. Fifteen patients had a good cosmetic result, and nine patients had a fair or poor cosmetic outcome, with marked deformity or a marked difference in size between the two breasts (or both). Regardless of the cosmetic result, the surviving women were pleased to have avoided mastectomy.
Three-dimensional conformal external-beam radiation therapy
The use of partial breast radiation after breast-conserving surgery is increasingly reported. As partial breast RT limits radiation to only the portion of the breast at risk for subsequent malignancy, use of partial breast RT in patients previously treated with whole-breast RT potentially limits radiation-induced toxicity. Several external-beam partial breast RT techniques have been described.43–45 The advantage of utilizing three-dimensional conformal external-beam RT is that it is less invasive than brachytherapy, and most radiation facilities in the United States already have the tools required for this method of RT delivery.
In summary, mastectomy is still the accepted standard of care for patients who have received prior RT to the chest or breast for various reasons. Patient requests for breast-conserving therapy in these situations need careful evaluation of various factors (eg, tumor size, time from previous RT, previous radiation dose and fields, willingness to proceed with other adjuvant therapies, such as chemotherapy and hormonal therapy), and shared decision making by the patient and radiation oncologist. Medical comorbidities and life expectancy also must be considered. Further investigation is needed to determine whether RT is a safe and acceptable alternative to mastectomy for managing early stage breast cancer for patients with a history of RT. Currently, in most situations, repeat irradiation should not be routinely offered and may be considered only for institutional review board-approved protocols, with stringent eligibility criteria and clearly defined radiation techniques and follow-up for patient outcomes.
History of Hodgkin lymphoma
Mastectomy is the most widely accepted surgical treatment for breast cancer in patients who were previously treated with mantle RT. This is primarily based on concerns regarding possible severe sequelae arising in the breast from a high total cumulative dose of RT, both from standard RT for breast cancer and from treatment delivered to portions of the breast for Hodgkin lymphoma. Nevertheless, with significant improvement in radiation techniques and the advent of partial breast irradiation, the question of breast-conserving treatment in this group is being reevaluated.46–49
Additionally, other factors need to be considered. Chemotherapy for Hodgkin lymphoma also leads to cardiac toxicity that is additive with RT to the heart from Hodgkin treatment and from breast treatment. The prior radiation field can help determine which areas would be receiving RT again. Chadha et al46 described five patients with a history of Hodgkin lymphoma who underwent lumpectomy and sentinel lymphadenectomy (with or without axillary dissection) followed by low-dose interstitial brachytherapy. At follow-up (range, 5–67 months), all five patients had an intact breast without evidence of relapse. No patients had infection, and no skin toxicities greater than grade 2 were observed. All patients were reported to have excellent cosmetic results.
Deutsch et al48 described 12 women treated with RT (with or without chemotherapy) for Hodgkin lymphoma (n=11) and non-Hodgkin lymphoma (n=1) with development of breast cancer 10 to 29 years later. Patients underwent lumpectomy and whole-breast RT with a boost to the operative area. Six also received adjuvant chemotherapy. Breast RT was reported to be well tolerated and not associated with any unusual acute or chronic sequelae. All women had good to excellent cosmetic results. Ten women were alive and well 1 to 174 months (median, 46 months) after completion of RT. Two women died of distant metastasis without local recurrence. The authors concluded that breast conservation with RT is not contraindicated by previous RT for lymphoma.
These reports of small case series are encouraging, and although treatment of lymphoma is also evolving, the standard of care for women with breast cancer after prior mantle RT is still mastectomy. For patients with a history of RT who are keen to pursue breast conservation, it is vital that they meet with the radiation oncologist before surgery to receive further education regarding options and to facilitate optimal decision making.
Genetic factors
Ionizing radiation can cause genetic damage, including mutations, chromosomal aberrations, DNA strand breaks, and chromosomal instability in normal cells.50 For women with hereditary germline mutations involving genes associated with DNA repair (eg, BRCA1 and BRCA2 [BRCA1/2] mutations, Li-Fraumeni syndrome, and Cowden syndrome), the potentially increased risk of subsequent malignancy due to RT must be considered in surgical decision making.
BRCA mutations
BRCA1/2 genes are involved in DNA repair,51 and as ionizing radiation damages DNA,52 there is concern about exposing BRCA carriers to therapeutic doses of ionizing radiation. Outcomes after therapeutic RT in women with BRCA mutation are conflicting. A case-control study examined BRCA1/2 mutation carriers treated with breast-conserving surgery followed by whole-breast RT and compared them with women with sporadic breast cancer similarly treated.53 Outcomes were similar for BRCA1/2 vs sporadic cancer groups with regard to 5-year rates of ipsilateral recurrence (98% vs 96%, respectively [P=0.80]) and survival (86% vs 91%, respectively [P=0.70]). However, the time to a contralateral breast cancer was very different, with 20% of the BRCA group having contralateral breast cancer by 5 years compared with only 2% in the sporadic group (P<0.001). This study demonstrated that breast RT did not increase the rate of an ipsilateral breast cancer in these high-risk women.53 Similar results were noted by Kirova et al in 2010.54 After more than 13 years of follow-up, the rate of ipsilateral breast cancer recurrence was no different among women with BRCA mutations who had breast-conserving treatment vs those with sporadic breast cancer who had similar treatment (36% vs 33%, respectively [P=0.42]). Metcalfe et al55 also reported a reduced rate of breast cancer recurrence after RT in BRCA1/2 carriers. In a retrospective review of 396 women with BRCA1/2 mutations previously treated with lumpectomy, they reported that women treated with RT after lumpectomy had a reduced risk of local recurrence (mean follow-up, 10.5 years; range, 0.9–27.1 years) compared with those who had lumpectomy alone (relative risk [RR], 0.28; 95% confidence interval [CI], 0.12–0.63; P=0.002).
Other studies show conflicting results. Both Haffty et al56 and Garcia-Etienne et al57 found higher local recurrence after RT in BRCA1/2 carriers compared with the sporadic breast cancer controls. In the study by Haffty et al,56 the women had 12 years of follow-up before the difference was observed (49% vs 21%, respectively [P=0.007]), whereas the study by Garcia-Etienne et al57 observed a divergence in recurrence rates after 5 years (15% vs 4%, respectively [P=0.03]). Together, these studies support the hypothesis that RT to the chest increases risk of future breast cancer in women with BRCA mutations. Although we consider the patient’s preference in these situations, we generally advise women with breast cancer who carry the BRCA1/2 mutation to undergo a therapeutic mastectomy (and contralateral prophylactic mastectomy).
Li-Fraumeni syndrome
Li-Fraumeni syndrome is an autosomal dominant disorder associated with an increased risk of malignancies, most commonly breast cancer, sarcoma, brain tumors, and adrenocortical cancers.58 It is associated with heterozygous germline mutations in the p53 tumor suppressor gene, which controls apoptosis and DNA repair.59 In laboratory experiments, ionizing radiation on human lymphoblast cells causes defective cell arrest and interferes with normal apoptosis.60
In a 2001 case report of a woman who underwent mastectomy and RT of the axilla and supraclavicular lymph nodes and later RT to the ovaries, the authors noted that within 8 years after RT, small-cell lung cancer and colon adenocarcinoma were detected in the original radiation fields. Subsequent tests showed that she had Li-Fraumeni syndrome.61 Another 2007 case report described a 27-year-old woman with bilateral breast cancer treated with mastectomy of the left breast, lumpectomy of the right breast, and postoperative RT to the right breast, axilla, and supraclavicular regions. Forty months later, a second cancer in the right breast and a malignant fibrous histiocytoma of the right clavicle developed. She was ultimately found to have a de novo p53 mutation.62
In 2010, Heymann et al63 reviewed the records of 47 families with Li-Fraumeni syndrome and found eight patients whose first cancer affected the breast. Six of the eight women had received postoperative RT, three after lumpectomy and three after mastectomy. After 6 years of follow-up, only one patient had contralateral breast cancer, and it was one of the two women who had not received RT. Of the women who had received RT, three ipsilateral and four contralateral breast cancers were identified. A chest wall angiosarcoma and a breast histiocytofibrosarcoma were also reported, both of which were radiation induced. The authors recommended mastectomy and prophylactic contralateral mastectomy for women with Li-Fraumeni syndrome who have breast cancer and suggested that RT should be avoided.
Cowden syndrome
Cowden syndrome is a rare germline mutation associated with benign hamartomas and increased risk of breast, thyroid, endometrial, and renal cancers. This mutation results in loss of function of the phosphate and tensin homologue gene (PTEN), a tumor suppressor gene involved in cell proliferation and apoptosis.64 No guidelines exist on the role of RT in the treatment for breast cancer in this group of women.
Ataxia telangiectasia syndrome
Ataxia telangiectasia syndrome is an autosomal recessive germline mutation of the ATM gene involved in cell division and DNA repair. The mutation increases risk of breast cancer, lymphoma, leukemia, and neurologic and skin conditions. Late radiation effects include necrosis of the breast tissue. An ATM mutation is thought to be a relative contraindication for RT.65
Bernstein et al66 showed that breast cancer survivors heterozygous for the ATM gene with a history of RT were more likely to have contralateral breast cancer than women who did not carry the single ATM allele. For women receiving 0.01 to 0.99 Gy, the RR was 2.8 (95% CI, 1.2–6.5); for those receiving at least 1.0 Gy, the RR was 3.3 (95% CI, 1.4–8.0).
Other syndromes
Mutations in CHEK2, PALB2, and CDH1, and Peutz-Jeghers syndrome are all known to increase breast cancer risk because of DNA repair abnormalities. However, little information has been published regarding the risk of RT in these settings.
In conclusion, multiple germline mutations increase risk of breast cancer and ionizing radiation-induced malignancies, but for some mutations, the data are insufficient to draw definitive conclusions regarding RT safety. Caution should be exercised when treating patients with BRCA1/2 mutations or Li-Fraumeni syndrome when the evidence suggests increased risk with RT.
Conclusion
RT is an important and effective adjuvant therapy for breast cancer. Whole-breast RT has demonstrated improved survival and decreased risk of locoregional recurrence and is considered part of definitive treatment of breast cancer after lumpectomy. Postmastectomy RT also reduces breast cancer recurrence risk and improves survival in select patients. Overall, adjuvant RT is well tolerated by patients; very little acute toxicity is reported, and for most patients, late toxicity is minimal as well. In this review, we summarized the medical factors that must be considered during surgical decision making to balance benefits and risks of therapeutic options. Providers must be aware that although RT rarely is absolutely contraindicated, it also has the potential for long-term adverse effects. Women must be counseled appropriately by a multidisciplinary team, including a radiation oncologist, regarding their choices during the breast cancer treatment decision-making process.
Disclosure
The authors report no conflicts of interest in this work.
References
Darby S, McGale P, Correa C, et al; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378(9804):1707–1716. | |
Yadav BS, Sharma SC, Singh R, Singh G, Kumar V. Postmastectomy radiation and survival in patients with breast cancer. J Cancer Res Ther. 2007;3(4):218–224. | |
Recht A, Edge SB. Evidence-based indications for postmastectomy irradiation. Surg Clin North Am. 2003;83(4):995–1013. | |
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC Cancer Staging Handbook: From the AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010. | |
Carver JR, Shapiro CL, Ng A, et al; ASCO Cancer Survivorship Expert Panel. American Society of Clinical Oncology clinical evidence review on the ongoing care of adult cancer survivors: cardiac and pulmonary late effects. J Clin Oncol. 2007;25(25):3991–4008. | |
Giordano SH, Kuo YF, Freeman JL, Buchholz TA, Hortobagyi GN, Goodwin JS. Risk of cardiac death after adjuvant radiotherapy for breast cancer. J Natl Cancer Inst. 2005;97(6):419–424. | |
Darby SC, Ewertz M, Hall P. Ischemic heart disease after breast cancer radiotherapy. N Engl J Med. 2013;368(26):2527. | |
Cuzick J, Stewart H, Rutqvist L, et al. Cause-specific mortality in long-term survivors of breast cancer who participated in trials of radiotherapy. J Clin Oncol. 1994;12(3):447–453. | |
Correa CR, Litt HI, Hwang WT, Ferrari VA, Solin LJ, Harris EE. Coronary artery findings after left-sided compared with right-sided radiation treatment for early-stage breast cancer. J Clin Oncol. 2007;25(21):3031–3037. | |
Hooning MJ, Botma A, Aleman BM, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. 2007;99(5):365–375. | |
Wang W, Wainstein R, Freixa X, Dzavik V, Fyles A. Quantitative coronary angiography findings of patients who received previous breast radiotherapy. Radiother Oncol. 2011;100(2):184–188. | |
Park CK, Li X, Starr J, Harris EE. Cardiac morbidity and mortality in women with ductal carcinoma in situ of the breast treated with breast conservation therapy. Breast J. 2011;17(5):470–476. | |
Nilsson G, Holmberg L, Garmo H, et al. Distribution of coronary artery stenosis after radiation for breast cancer. J Clin Oncol. 2012;30(4):380–386. | |
Marbach JR, Sontag MR, Van Dyk J, Wolbarst AB. Management of radiation oncology patients with implanted cardiac pacemakers: report of AAPM Task Group No 34. American Association of Physicists in Medicine. Med Phys. 1994;21(1):85–90. | |
Gelblum DY, Amols H. Implanted cardiac defibrillator care in radiation oncology patient population. Int J Radiat Oncol Biol Phys. 2009;73(5):1525–1531. | |
Soejima T, Yoden E, NIshimura Y, et al. Radiation therapy in patients with implanted cardiac pacemakers and implantable cardioverter defibrillators: a prospective survey in Japan. J Radiat Res. 2011;52(4):516–521. | |
Munshi A, Wadasadawala T, Sharma PK, et al. Radiation therapy planning of a breast cancer patient with in situ pacemaker – challenges and lessons. Acta Oncol. 2008;47(2):255–260. | |
Wadasadawala T, Pandey A, Agarwal JP, et al. Radiation therapy with implanted cardiac pacemaker devices: a clinical and dosimetric analysis of patients and proposed precautions. Clin Oncol (R Coll Radiol). 2011;23(2):79–85. | |
Kapa S, Fong L, Blackwell CR, Herman MG, Schomberg PJ, Hayes DL. Effects of scatter radiation on ICD and CRT function. Pacing Clin Electrophysiol. 2008;31(6):727–732. | |
Nibhanupudy JR, de Jesus MA, Fujita M, Goldson AL. Radiation dose monitoring in a breast cancer patient with a pacemaker: a case report. J Natl Med Assoc. 2001;93(7–8):278–281. | |
Minor GI, Yashar CM, Spanos WJ Jr, et al. The relationship of radiation pneumonitis to treated lung volume in breast conservation therapy. Breast J. 2006;12(1):48–52. | |
Lingos TI, Recht A, Vicini F, Abner A, Silver B, Harris JR. Radiation pneumonitis in breast cancer patients treated with conservative surgery and radiation therapy. Int J Radiat Oncol Biol Phys. 1991;21(2):355–360. | |
Jung JI, Kim HH, Park SH, et al. Thoracic manifestations of breast cancer and its therapy. Radiographics. 2004;24(5):1269–1285. | |
Stone DJ, Schwartz MJ, Green RA. Fatal pulmonary insufficiency due to radiation effect upon the lung. Am J Med. 1956;21(2):211–226. | |
Bennett DE, Million RR, Ackerman LV. Bilateral radiation pneumonitis, a complication of the radiotherapy of bronchogenic carcinoma. (Report and analysis of seven cases with autopsy). Cancer. 1969;23(5):1001–1018. | |
Whelan TJ, Olivotto I, Ackerman I, et al. NCIC-CTG MA.20: an intergroup trial of regional nodal irradiation in early breast cancer [abstract]. J Clin Oncol. 2011;29(Suppl 15):LBA1003. | |
Morris MM, Powell SN. Irradiation in the setting of collagen vascular disease: acute and late complications. J Clin Oncol. 1997;15(7):2728–2735. | |
Ross JG, Hussey DH, Mayr NA, Davis CS. Acute and late reactions to radiation therapy in patients with collagen vascular diseases. Cancer. 1993;71(11):3744–3752. | |
Mayr NA, Riggs CE, Saag KG, Wen BC, Pennington EC, Hussey DH. Mixed connective tissue disease and radiation toxicity. A case report. Cancer. 1997;79(3):612–618. | |
Pinn ME, Gold DG, Petersen IA, Osborn TG, Brown PD, Miller RC. Systemic lupus erythematosus, radiotherapy, and the risk of acute and chronic toxicity: the Mayo Clinic Experience. Int J Radiat Oncol Biol Phys. 2008;71(2):498–506. | |
Gold DG, Miller RC, Petersen IA, Osborn TG. Radiotherapy for malignancy in patients with scleroderma: The Mayo Clinic experience. Int J Radiat Oncol Biol Phys. 2007;67(2):559–567. | |
Chen AM, Obedian E, Haffty BG. Breast-conserving therapy in the setting of collagen vascular disease. Cancer J. 2001;7(6):480–491. | |
Charalambous H, Bloomfield D. Psoriasis and radiotherapy: exacerbation of psoriasis following radiotherapy for carcinoma of the breast (the Koebner phenomenon). Clin Oncol (R Coll Radiol). 2000;12(3):192–193. | |
Farber EM, Nall ML. The natural history of psoriasis in 5,600 patients. Dermatologica. 1974;148(1):1–18. | |
Munshi A, Jain S, Budrukkar A, Jalali R, Sarin R. Radiotherapy-induced depigmentation in a patient with breast cancer. Indian J Cancer. 2007;44(4):157–158. | |
Chadha M, Trombetta M, Boolbol S, Osborne MP. Managing a small recurrence in the previously irradiated breast. Is there a second chance for breast conservation? Oncology (Williston Park). 2009;23(11):933–940. | |
Solin LJ, Gray R, Goldstein LJ, et al. Prognostic value of biologic subtype and the 21-gene recurrence score relative to local recurrence after breast conservation treatment with radiation for early stage breast carcinoma: results from the Eastern Cooperative Oncology Group E2197 study. Breast Cancer Res Treat. 2012;134(2):683–692. | |
Chadha M, Feldman S, Boolbol S, Wang L, Harrison LB. The feasibility of a second lumpectomy and breast brachytherapy for localized cancer in a breast previously treated with lumpectomy and radiation therapy for breast cancer. Brachytherapy. 2008;7(1):22–28. | |
Trombetta M, Julian T, Miften M, McWilliams W, Kim Y, Parda D. The use of the MammoSite balloon applicator in re-irradiation of the breast. Brachytherapy. 2008;7(4):316–319. | |
Guix B, Lejárcegui JA, Tello JI, et al. Exeresis and brachytherapy as salvage treatment for local recurrence after conservative treatment for breast cancer: results of a ten-year pilot study. Int J Radiat Oncol Biol Phys. 2010;78(3):804–810. | |
Deutsch M. Repeat high-dose external beam irradiation for in-breast tumor recurrence after previous lumpectomy and whole breast irradiation. Int J Radiat Oncol Biol Phys. 2002;53(3):687–691. | |
Hannoun-Levi JM, Houvenaeghel G, Ellis S, et al. Partial breast irradiation as second conservative treatment for local breast cancer recurrence. Int J Radiat Oncol Biol Phys. 2004;60(5):1385–1392. | |
Baglan KL, Sharpe MB, Jaffray D, et al. Accelerated partial breast irradiation using 3D conformal radiation therapy (3D-CRT). Int J Radiat Oncol Biol Phys. 2003;55(2):302–311. | |
Formenti SC, Truong MT, Goldberg JD, et al. Prone accelerated partial breast irradiation after breast-conserving surgery: preliminary clinical results and dose-volume histogram analysis. Int J Radiat Oncol Biol Phys. 2004;60(2):493–504. | |
Kozak KR, Katz A, Adams J, et al. Dosimetric comparison of proton and photon three-dimensional, conformal, external beam accelerated partial breast irradiation techniques. Int J Radiat Oncol Biol Phys. 2006;65(5):1572–1578. | |
Chadha M, Yoon H, Feldman S, Shah N, Moore E, Harrison LB. Partial breast brachytherapy as the primary treatment for breast cancer diagnosed after mantle radiation therapy for Hodgkin’s disease. Am J Clin Oncol. 2009;32(2):132–136. | |
Intra M, Gentilini O, Veronesi P, et al. A new option for early breast cancer patients previously irradiated for Hodgkin’s disease: intraoperative radiotherapy with electrons (ELIOT). Breast Cancer Res. 2005;7(5):R828–R832. | |
Deutsch M, Gerszten K, Bloomer WD, Avisar E. Lumpectomy and breast irradiation for breast cancer arising after previous radiotherapy for Hodgkin’s disease or lymphoma. Am J Clin Oncol. 2001;24(1):33–34. | |
Aref I, Cross P. Conservative surgery and radiation therapy for early stage breast cancer after previous mantle radiation for Hodgkin’s disease. Br J Radiol. 2000;73(872):905–906. | |
National Toxicology Program. Report on Carcinogens. 12th ed. 2011. Washington, DC: US Department of Health and Human Services; 2011. Available from: http://www.ntp.niehs.nih.gov/ntp/roc/twelfth/roc12.pdf. Accessed September 28, 2014. | |
Scully R, Livingston DM. In search of the tumour-suppressor functions of BRCA1 and BRCA2. Nature. 2000;408(6811):429–432. | |
Goss PE, Sierra S. Current perspectives on radiation-induced breast cancer. J Clin Oncol. 1998;16(1):338–347. | |
Pierce LJ, Strawderman M, Narod SA, et al. Effect of radiotherapy after breast-conserving treatment in women with breast cancer and germline BRCA1/2 mutations. J Clin Oncol. 2000;18(19):3360–3369. | |
Kirova YM, Savignoni A, Sigal-Zafrani B, et al. Is the breast-conserving treatment with radiotherapy appropriate in BRCA1/2 mutation carriers? Long-term results and review of the literature. Breast Cancer Res Treat. 2010;120(1):119–126. | |
Metcalfe K, Lubinski J, Lynch HT, et al; Hereditary Breast Cancer Clinical Study Group. Family history of cancer and cancer risks in women with BRCA1 or BRCA2 mutations. J Natl Cancer Inst. 2010;102(24):1874–1878. | |
Haffty BG, Harrold E, Khan AJ, et al. Outcome of conservatively managed early-onset breast cancer by BRCA1/2 status. Lancet. 2002;359(9316):1471–1477. | |
Garcia-Etienne CA, Barile M, Gentilini OD, et al. Breast-conserving surgery in BRCA1/2 mutation carriers: are we approaching an answer? Ann Surg Oncol. 2009;16(12):3380–3387. | |
Kast K, Krause M, Schuler M, et al. Late onset Li-Fraumeni Syndrome with bilateral breast cancer and other malignancies: case report and review of the literature. BMC Cancer. 2012;12:217. | |
Goi K, Takagi M, Iwata S, et al. DNA damage-associated dysregulation of the cell cycle and apoptosis control in cells with germ-line p53 mutation. Cancer Res. 1997;57(10):1895–1902. | |
Delia D, Goi K, Mizutani S, et al. Dissociation between cell cycle arrest and apoptosis can occur in Li-Fraumeni cells heterozygous for p53 gene mutations. Oncogene. 1997;14(18):2137–2147. | |
Limacher JM, Frebourg T, Natarajan-Ame S, Bergerat JP. Two metachronous tumors in the radiotherapy fields of a patient with Li-Fraumeni syndrome. Int J Cancer. 2001;96(4):238–242. | |
Salmon A, Amikam D, Sodha N, et al. Rapid development of post-radiotherapy sarcoma and breast cancer in a patient with a novel germline ‘de-novo’ TP53 mutation. Clin Oncol (R Coll Radiol). 2007;19(7):490–493. | |
Heymann S, Delaloge S, Rahal A, et al. Radio-induced malignancies after breast cancer postoperative radiotherapy in patients with Li-Fraumeni syndrome. Radiat Oncol. 2010;5:104. | |
Bennett KL, Mester J, Eng C. Germline epigenetic regulation of KILLIN in Cowden and Cowden-like syndrome. JAMA. 2010;304(24):2724–2731. | |
Iannuzzi CM, Atencio DP, Green S, Stock RG, Rosenstein BS. ATM mutations in female breast cancer patients predict for an increase in radiation-induced late effects. Int J Radiat Oncol Biol Phys. 2002;52(3):606–613. | |
Bernstein JL, Haile RW, Stovall M, et al; WECARE Study Collaborative Group. Radiation exposure, the ATM Gene, and contralateral breast cancer in the women’s environmental cancer and radiation epidemiology study. J Natl Cancer Inst. 2010;102(7):475–483. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.