")
Back to Journals » Journal of Pain Research » Volume 13
Mediators of Pain and Physical Function in Female and Male Patients with Chronic Pain
Authors Danielsson L , Kvarstein G , Bergvik S
Received 5 October 2019
Accepted for publication 19 February 2020
Published 19 May 2020 Volume 2020:13 Pages 1059—1071
DOI https://doi.org/10.2147/JPR.S233501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael A Ueberall
Lena Danielsson,1,2 Gunnvald Kvarstein,1,2 Svein Bergvik3
1Pain Clinic, Division Surgical Medicine and Intensive Care, University Hospital of North Norway, Tromsø, Norway; 2Department of Clinical Medicine, UiT - the Arctic University of Norway, Tromsø, Norway; 3Department of Psychology, UiT the Arctic University of Norway, Tromsø, Norway
Correspondence: Lena Danielsson
Pain Clinic, Division Surgical Medicine and Intensive Care, University Hospital of North Norway, Tromsø NO-9038, Norway
Tel +4799023564
Email [email protected]
Purpose: Chronic pain is often multifactorial and accompanied by psychological distress, catastrophizing thoughts, reduced physical function, and socio-economic worries. In this explorative study, we investigated potential mediators in the relationships of psychological and demographic variables with chronic pain and physical function in women and men.
Patients and Methods: The study included 301 patients admitted to a multidisciplinary pain clinic. Prior to their first consultation, patients completed a questionnaire including items on demographics (age, education, occupational and financial situation), catastrophizing thoughts, psychological distress, pain intensity, and physical function. Hierarchical multiple regression analyses examined demographic and psychological factors associated with pain intensity and physical function. Mediation and reversed mediation models were tested and developed based on calculated relations in the regression analyses between demographic, psychological, pain intensity and physical function variables.
Results: Fifty-eight percent were females and mean age 43.8 and 46.0 years for women and men, respectively. In the regression analyses, psychological factors accounted better for pain intensity than demographic variables, while physical function was best accounted for by demographic variables. Among women, catastrophizing thoughts mediated significantly the relationships between education and pain intensity, and between education and physical function. Psychological distress mediated significantly the relationships between financial situation and pain intensity, and between financial situation and physical function in women. In men, the only significant mediation model was psychological distress mediating the relationship between financial situation and pain intensity. Some of the reversed models revealed indirect effects, indicating bidirectionality.
Conclusion: The results indicate that there might be gender-specific mediators in how demographic variables are associated with pain intensity and physical function. This suggests an awareness among clinicians of potential gender-specific factors mediating pain problems, and the need for a gender-specific, multidisciplinary approach in the treatment of chronic pain.
Keywords: depression, physical disability, comorbidity, catastrophizing, mediation, multidisciplinary treatment
Introduction
Clinical and experimental studies have documented that women are more prone to pain compared with men.1–5 The sex hormones play a role and the effect seems to be regulated by immunological mediators.6,7 However, chronic pain is a complex condition and several psychosocial characteristics have been identified as risk factors,8–11 and these may also explain the gender-related differences.12–14
Comorbidity of pain and depressive symptoms is associated with poorer prognosis and more disability than either condition alone,15,16 and this is found to be more pronounced among women compared with men.17 In a review, including 105 epidemiological studies of recurrent pain, women experienced more recurrent pain, longer pain duration, more severe pain intensity, and they were more vulnerable to psychosocial factors than men.18 In an epidemiological Canadian survey based on data from a national database with more than 131 000 adults, depressive symptoms and chronic pain were twice as prevalent in women as in men, and comorbidity of depression and pain was significantly associated with psychological distress and disability among women.17 In another large population-based study from 13 European countries, women with chronic pain were also more prone to report depressive symptoms than men with chronic pain. Treatment of depressive symptoms interestingly seemed to protect from persistent pain among women but not among men.19 When Keefe et al in pre-treatment data from two randomized, clinical treatment studies (N: 168) found relatively higher pain levels and worse physical function among women than men suffering from osteoarthritis, catastrophizing thoughts mediated the relation between gender and pain outcomes.20
Clinical outcome of patients being treated for chronic pain varies. A large Finnish follow-up study of patients (N=1043) subjected to multidisciplinary treatment addresses the need for more research on factors which are associated with improved health-related quality of life in order to understand why some patients don´t benefit from multidisciplinary treatment.21 When treating patient with severe chronic pain Hysing et al argue for increased awareness of the huge burden of symptoms additional to pain, and particularly psychiatric comorbidity and low physical functioning.22 Since chronic pain and health problems are closely associated with socioeconomic status,23–26 factors like education and economy and potential associations with psychological factors need to be included in the study of chronic pain.
Considering the biological gender differences and the complex and multifactorial nature of chronic pain, we hypothesized that psychological distress and negative cognitions mediate the relations between demographic factors and pain intensity and physical function. In this explorative study, we, therefore, performed separate analyses for men and women and also tested for potential bidirectional27 mediation by psychological distress and catastrophizing thoughts on demographic factors and pain intensity as well as physical function. If different mediators could be identified in women and men, this would imply the need for further research on this topic which might have important clinical implications for future treatment of chronic pain.
Materials and Methods
Participants
Patients admitted to the Multidisciplinary Pain Clinic at the University Hospital of North Norway (UNN) in the period of 2010–2012, were included in the study. All referrals were evaluated by a multidisciplinary team before being accepted for admittance. The same criteria to be accepted were used for all referrals. The clinic admitted patients with a non-malignant complex chronic pain condition. The project included all patients admitted to the clinic.
Design
In this cross-sectional designed study, data were collected by a set of self-reported questionnaire routinely completed by all patients admitted to the clinic as part of the clinical assessment. The questionnaire was attached to the invitation letter for hospital admittance sent to the patients by mail, in a paper-and-pencil format, and completed by the patients prior to their first consultation.28
Methods
Ethics
The study was part of a quality assurance project approved by the Data Protection Official at UNN (Project no 0084/Ref2008/4213-1), and exempted from patient consent according to the Norwegian Health Personnel Act.
Measures
The set of questionnaires, including validated and internationally acknowledged instruments, was compiled and recommended by the Norwegian Association of Pain for use in Norwegian Pain Clinics. The variables applied in this study include:
Demographics: Gender, age, total years of education (dichotomized into ≤12 or >12 years), working/in education status (“work status”) (dichotomized to yes= full or part-time work or study, no= no work or study). Perceived financial situation: How do you perceive your financial situation? Three answer options (poor, medium and good) which was dichotomized into poor or medium/good.
Pain assessment: Most severe, least severe, and average pain intensities during the last week were assessed by 11-point numeric rating scales (NRS) ranging from 0 to 10 where 0 = no pain and 10 = worst possible pain. The pain scales originate from the Brief Pain Inventory (BPI) and have shown satisfactory properties.29,30 In this study, pain intensity was presented as an average of the scores from the three pain assessment scales.
Catastrophizing thoughts: Two items from the catastrophizing subscale of the Coping Strategies Questionnaire (CSQ) were included to assess tendencies for catastrophizing thoughts: 1. “When I feel pain it is terrible, and I feel it is never going to get any better”. 2. “When I feel pain, I feel I can’t stand it anymore.” Response format was a 7-point scale (0–6 where 0 = never and 6 = always). These items have proved useful for clinical purposes in the initial screening and treatment monitoring.31 The two-item version of CSQ provides adequately valid estimates of catastrophizing, due to the strong associations with the original scales and their sensitivity to changes with treatment.32
Physical function: The 10 questions originate from the health domain on physical function in the Norwegian version of the RAND 36-Item Short Form Health Survey.33 Physical function captures both the presence and extent of physical limitations, applying a three-level response format, ranging from 1 to 3 (1= yes, limited a lot, 2= yes, limited a little, 3= no, not limited at all). The scores are converted into 0–100 scales (0 = worst possible physical function, 100 = best possible physical function).
Psychological distress: The Hopkins Symptom Checklist-25 (HSCL-25) is a widely used, self-administrated instrument. It is based on the main symptom dimensions of depression and anxiety and is a valid and reliable measure of psychological distress.34 The questionnaire contains 25 items with 4-point scales response format ranging from 1 = not at all to 4 = extremely. The average item score is calculated by dividing the total score by the number of items answered.35,36 A cut-off point of 1.75 for women and 1.67 for men have been suggested as a valid predictor of psychological distress.34,36,37 Items missing were imputed according to the Expectation Maximization (EM) algorithm provided by the SPSS.38 Only patients completing a minimum of 20 of the 25 items, were included.
Statistical Methods
All data were analysed using SPSS for Windows version 24. For bivariate analyses, Pearson’s product-moment correlations were examined for continuous independent and dependent variables (age, psychological distress, catastrophizing, pain and physical function). Phi correlations were applied to examine dichotomous variables (work status, perceived financial situation and education) while point-biserial correlations examined the strength of the association between dichotomous (work status, financial situation and education) and continuous variables (age, psychological distress, catastrophizing, pain and physical function). The bivariate analyses were separated by gender.
First, hierarchical regression analyses examined the associations among variables of relevance based on previous clinical research. Then, mediation models, based on the regression results, were developed and tested.
The hierarchical multiple regressions analyzed the main effects of the independent variables age, education, work status, perceived financial position, psychological distress and catastrophizing thoughts on the two dependent variables pain intensity and physical function for men and women, respectively. To identify and differentiate the effects of demographics and psychological factors, they were entered into the regression in respective blocks. Demographic factors (age, education, work status and perceived financial situation) were entered into block 1, followed by psychological factors (psychological distress and catastrophizing thoughts) into block 2.
To explore potential mediating effects of psychological distress and catastrophizing thoughts, mediation models were developed based on the observed significant relations in the regression analyses. Models for women and men were created and tested separately. Alternative, reversed models were tested due to potential reversed directionality of the mediations. In these reversed models, the dependent variable was defined as the mediating variable and the mediating variable as dependent variable. The mediation analyses separated the direct and indirect effects, which could be essential for establishing new relevant hypotheses on causality. Due to alike analysis schemes, we chose a mediation approach similar to what was described by Newman et al,27 applying Hayes’ SPSS macro, PROCESS with 5000 bootstrap resampling. Bootstrapping is a nonparametric resampling procedure that does not assume multivariate normality.39,40 We estimated 95% bias-corrected and accelerated (BCa) bootstrapped confidence intervals and point estimates. When the corresponding bootstrapped confidence intervals did not contain zero, the indirect effect was considered statistically significant.40 The analyses were performed in accordance with recommendations from statisticians at the institution.
Results
Demographics
The sample included the complete patient population admitted to the pain clinic during a two-year time-period; a total of 301 patients. Two thirds were referred from general practitioners and one third from physicians at hospitals. The same criteria to be accepted were used for all referrals. The patients had experienced pain for a notable period of time (91% > 1 year, 37% >10 years). The criteria41 for widespread pain was fulfilled by 45% (135) patients, of them 65% (88) were women. Mean age was 45 years (SD 13.4) and 58% (176) were females. Higher education (>12 years) was reported by 24% (72), 72% (209) were out of work, and 66% (194) perceived their financial situation as average or good. We found moderately high levels of pain intensity (mean=6.0, SD=1.76), and relatively high levels of psychological distress (2.0, SD=0.59) and catastrophizing thoughts (mean=3.8, SD=1.4), while physical function was relatively low with a mean of less than 50% of full score (mean=49, SD=25). Sample characteristics are presented separately for each gender in Table 1.
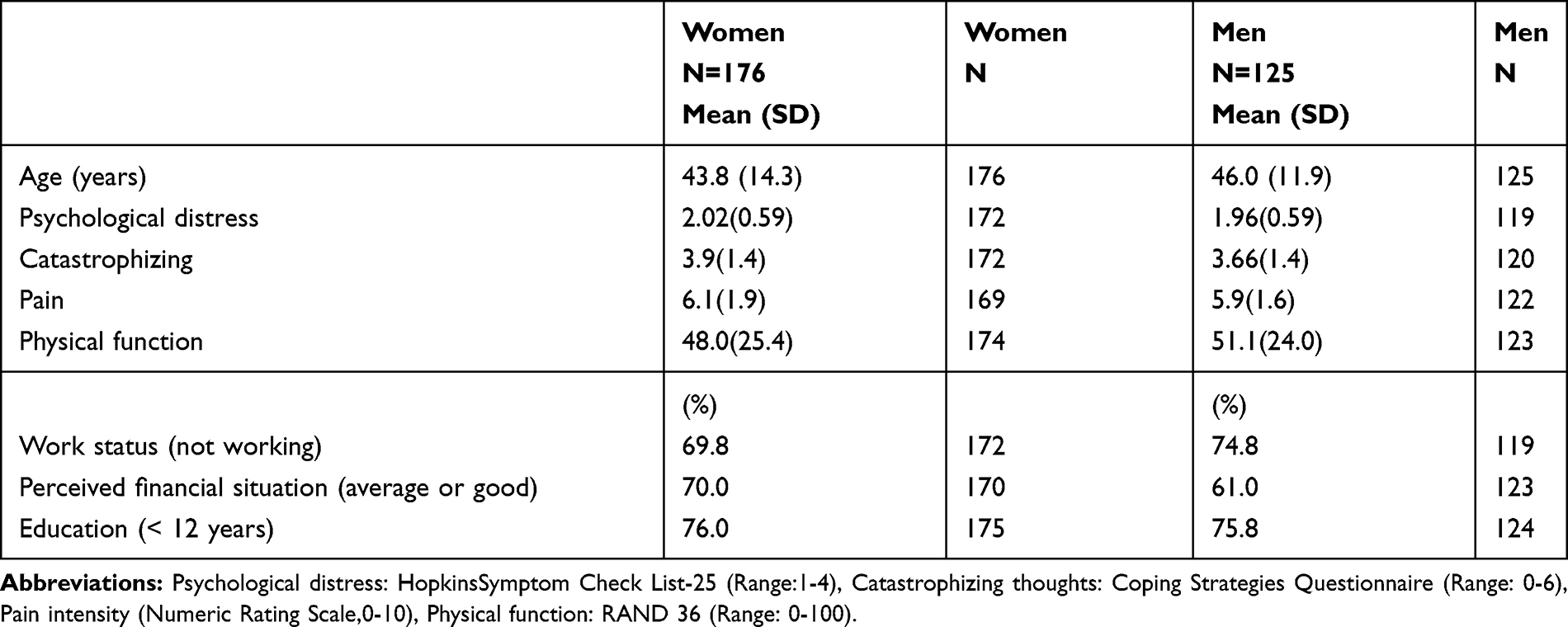 |
Table 1 Sample Characteristics |
In bivariate correlations among women, we found strong (r>0.50) associations between psychological distress and pain intensity, and catastrophizing thoughts and pain intensity, medium (r=0.30 to 0.49) associations between age and physical function, work status and physical function, psychological distress and pain intensity, and between pain intensity and physical function. In men, we found medium (r=0.30 to 0.49) associations between psychological distress and pain intensity, catastrophizing thoughts and pain intensity, pain intensity and physical function, financial situation and psychological distress, and between psychological distress and catastrophizing thoughts. Some additional associations were statistically significant, but weak. The gender-specific bivariate correlations are presented in Tables 2 and 3.
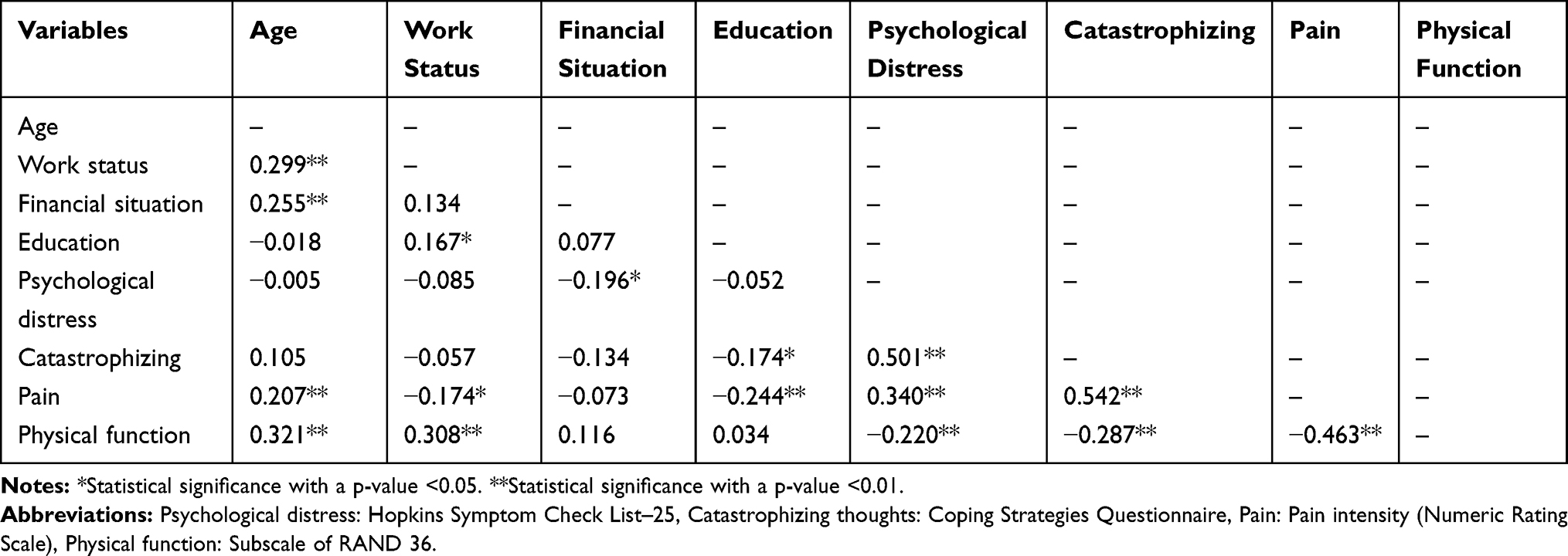 |
Table 2 Bivariate Correlations Among Study Variables (Women) |
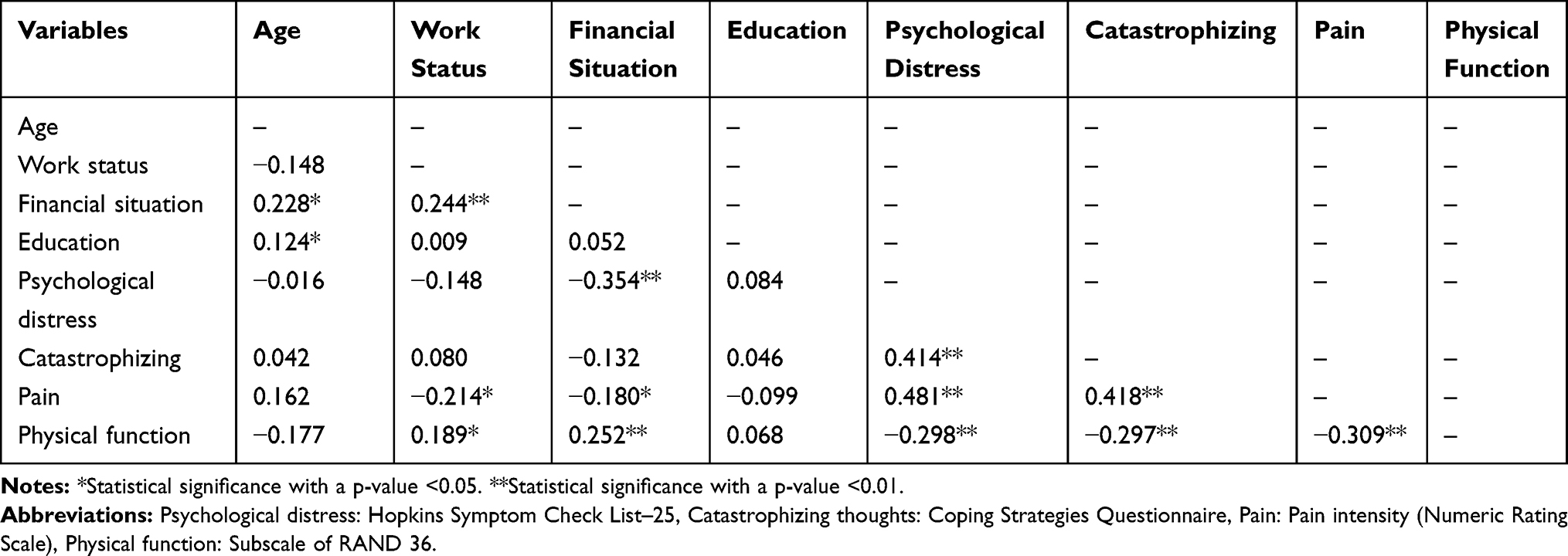 |
Table 3 Bivariate Correlations Among Study Variables (Men) |
Hierarchical Multiple Regressions
Regression Analyses of Pain Intensity and Physical Function Among Women
The first regression model examined the dependent variable pain intensity among women. When age, work status, perceived financial situation, and education were entered in block 1, only age and education remained statistically significant predictors. Adding psychological distress and catastrophizing thoughts in block 2 resulted in a model with education and catastrophizing thoughts as significant predictors. In this model (F(6,157)= 14.32, p<0.001) demographic variables explained 11.6% and psychological variables 23.8% of the variance of pain intensity among women (Table 4).
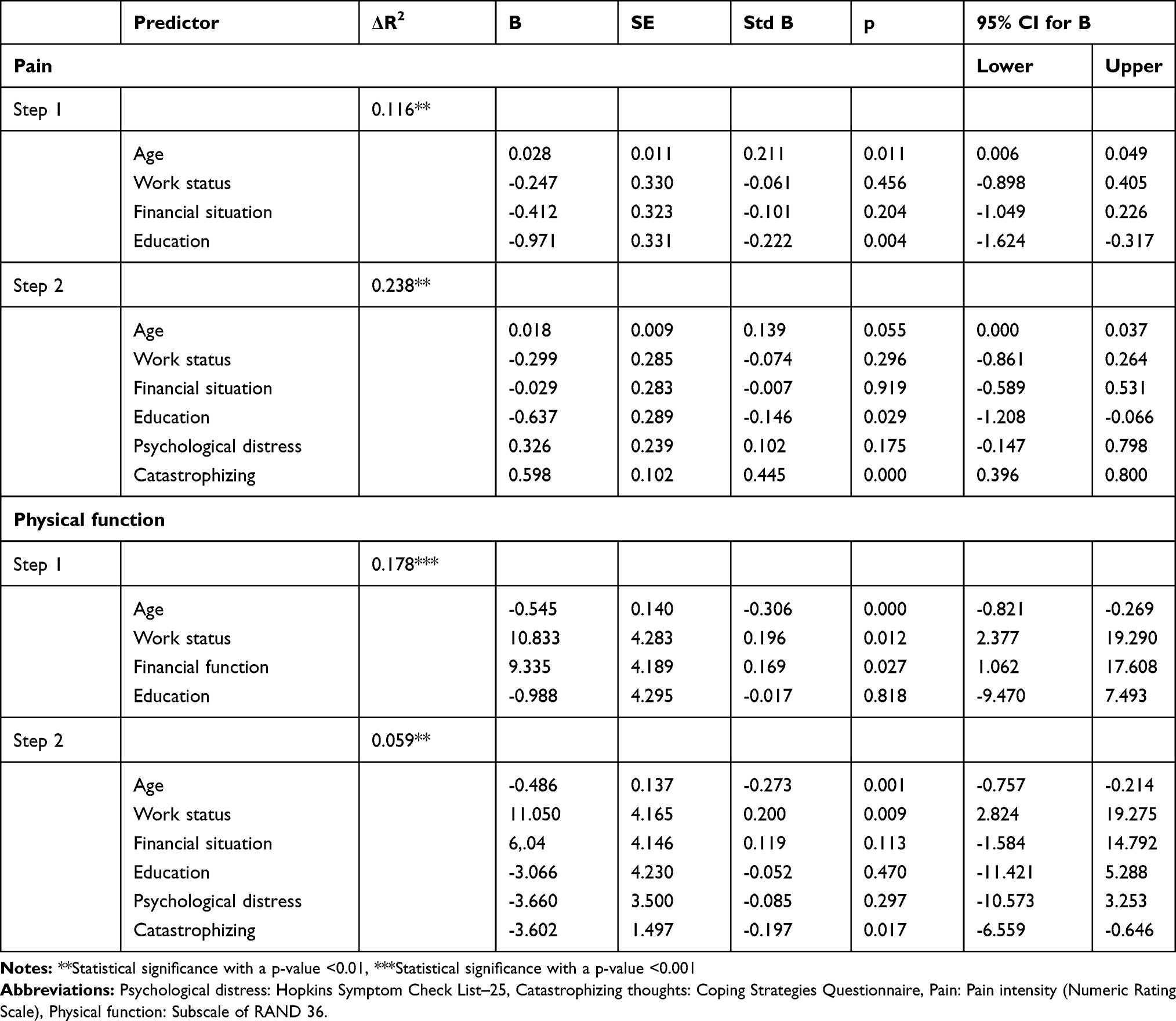 |
Table 4 Summary of Multiple Regression Analyses of Pain and Physical Function in Women |
In the second regression model, the dependent variable physical function among women was examined. Age, work status, perceived financial situation, and education were entered in block 1. Here, age, work status, and perceived financial situation remained significant predictors. Adding psychological distress and catastrophizing thoughts in block 2 resulted in a model with age, work status, and catastrophizing thoughts as significant predictors. In this model (F(6,160)=8.26, p<0.001) demographic variables explained 17.8% and psychological variables 5.9% of the variance of physical function among women (Table 4).
Regression Analyses of Pain Intensity and Physical Function Among Men
The first regression model examined the dependent variable pain intensity among men. When age, work status, perceived financial situation, and education were entered in block 1, age remained a significant predictor. Adding psychological distress and catastrophizing thoughts in block 2 resulted in a model with education, psychological distress, and catastrophizing thoughts as significant predictors. In the model (F(6,107)= 10.23, p<0.001) demographic variables explained 10.6% and psychological variables 25.8% of the variance of pain intensity among men (Table 5).
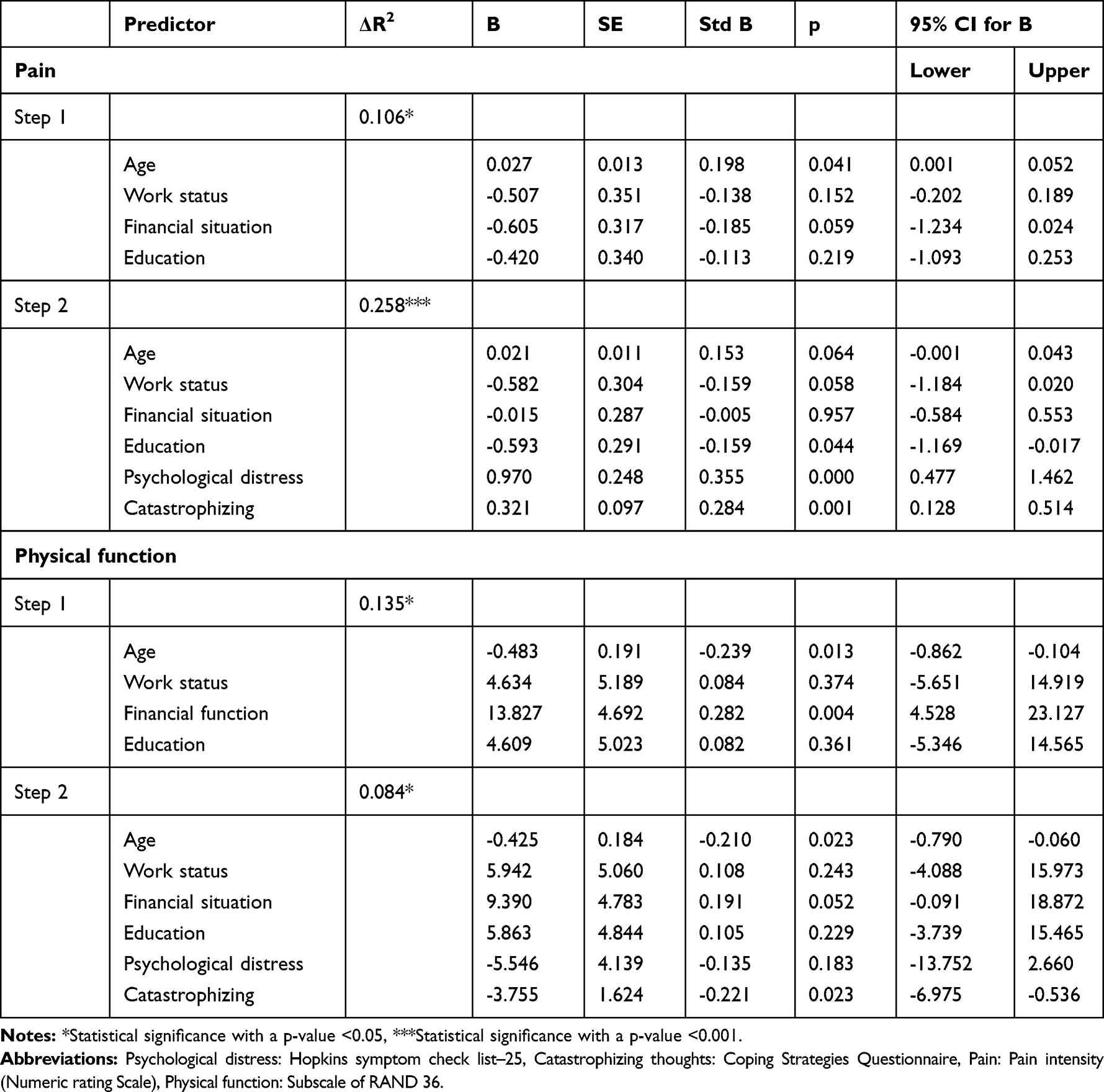 |
Table 5 Summary of Multiple Regression Analyses of Pain and Physical Function in Men |
The second model examined the dependent variable physical function among men. When age, work status, perceived financial situation, and education were entered in block 1, age and perceived financial situation remained significant predictors. Adding psychological distress and catastrophizing thoughts in block 2 resulted in a model with age and catastrophizing thoughts as significant predictors. In the model (F(6,107)=4.99, p<0.001) demographic variables explained 13.5% and psychological variables 8.4% of the variance of physical function among men (Table 5).
Regression Analyses of Catastrophizing Thoughts and Psychological Distress in Women and Men
The first regression model examined associations between the dependent variable catastrophizing thoughts and demographic factors in woman and men, respectively. Age, work status, perceived financial situation and education were included as independent variables. Perceived financial situation and education remained significant predictors among women (F(4,162)=2.82, p=0.027), and the demographic variables explained 6.5% of the variance of catastrophizing thoughts among women. None of the demographic variables were significantly associated with catastrophizing thoughts among men (Tables 6 and 7).
 |
Table 6 Summary of Multiple Regression Analyses of Catastrophizing and Psychological Distress Variables in Women |
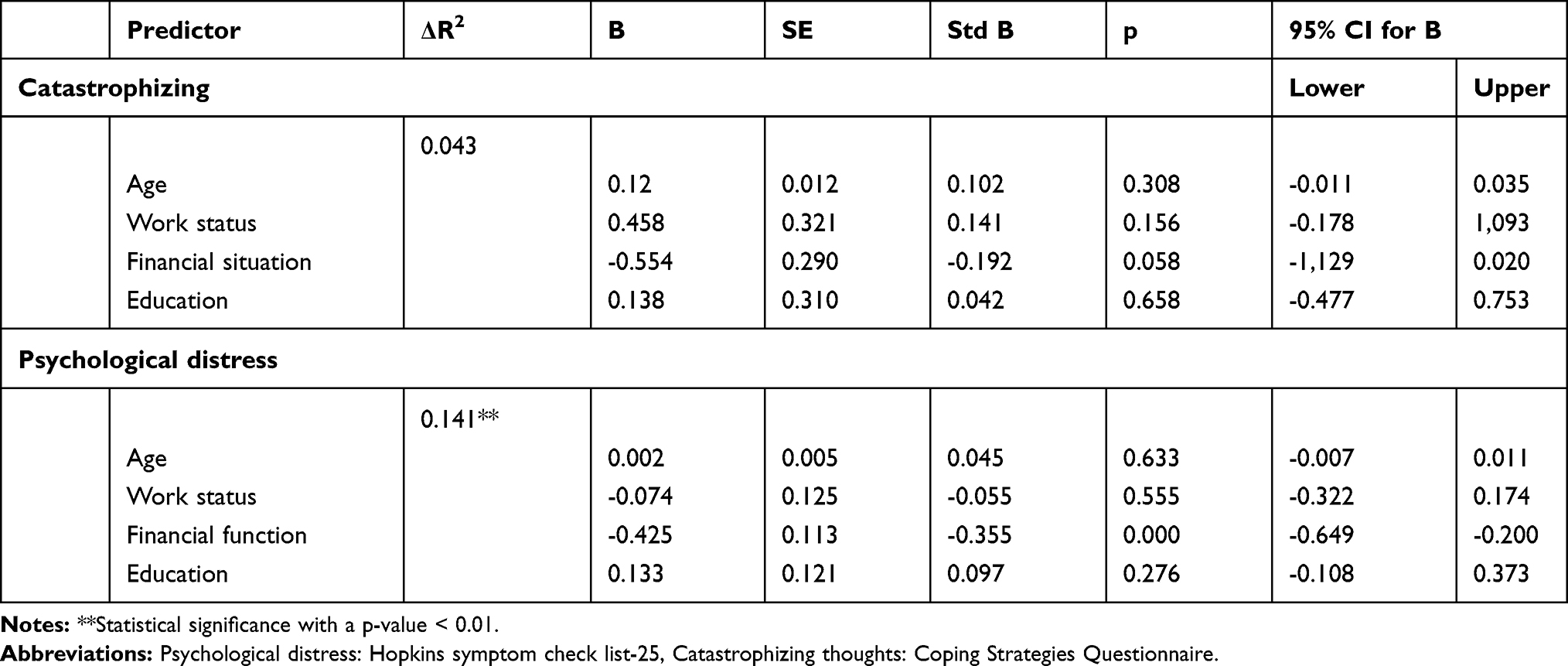 |
Table 7 Summary of Multiple Regression Analyses of Catastrophizing and Psychological Distress Variables in Men |
Thesecond regression model examined associations between the dependent variable psychological distress and demographic factors for women and men, respectively. When age, work status, perceived financial situation, and education were entered, only perceived financial situation remained a significant predictor, both in the model for women and in the one for men. In the model, demographic variables explained 14.1% of the variance of psychological distress among men (F(4,110)=4,53, p=0.002), for women the model was non-significant (F(4,162)=1,84, p=0.123) (Tables 6 and 7).
Mediation (Figure 1)
Based on relations established in the regressions, we examined a series of 11 mediation models among women and 6 models among men (Tables 6 and 7). The criterion for selecting these variables was a statistically significant association between the independent and dependent variable. Furthermore, following the arguments provided by Preacher and Hayes,40 a significant association between independent (X) and dependent variables (Y) is not necessary for considering a mediation analysis. Thus, among the female models, we also included perceived financial situation due to the statistically significant relationship with the mediator variables (M) catastrophizing and psychological distress. Among the male models, we included perceived financial situation due to the statistically significant relationship with the mediator variable psychological distress.
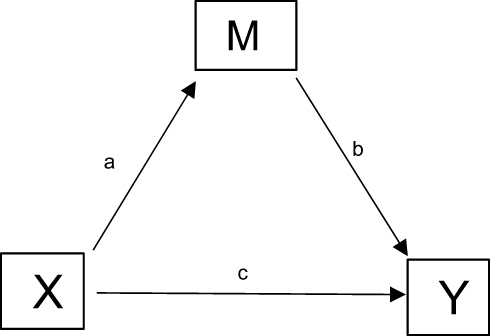 |
Figure 1 Indirect effect of X on Y through M=ab. Direct effect of X on Y=c. |
Due to potential bidirectionality, alternative reversed models were tested. In these models, pain intensity and physical function were mediators (M) and the psychological variables (psychological distress and catastrophizing thoughts) dependent variables (Y).
Mediation Results in Women
The models 1–6 (Table 8) among women examined catastrophizing thoughts (M) as a potential mediator. Two of the six tested models with catastrophizing thoughts (M) as mediator were statistically significant. The indirect effects showed that catastrophizing thoughts (M) fully mediated the relationship between education (X) and physical function (Y) (model number 6), and partially between education (X) and pain intensity (Y) (model number 2). The models 7–11 examined psychological distress (M) as a potential mediator (Table 6). Two of the five tested models with psychological distress (M) as mediator were statistically significant. The indirect effects showed that psychological distress (M) fully mediated the relationship between perceived financial situation (X) and physical function (Y) (model number 7), and also fully between perceived financial situation (X) and pain intensity (Y) (model number 8). The other models were not statistically significant (Table 8).
 |
Table 8 Summary of Mediation Models with Catastrophizing and Psychological Distress as Mediators in Women, Based on 5000 Bootstrap Samples |
When reversing the significant models (numbers 2, 6, 7 and 8), pain intensity (M) and physical function (M) were defined as mediators and catastrophizing thoughts (Y) and psychological distress (Y) as dependent variables (Table 9). One of the 2 tested models with pain intensity (M) as mediator was statistically significant (model number 2). The indirect effects confirmed that pain intensity (M) fully mediated the relation between education (X) and catastrophizing thoughts (Y). None of the two tested models with physical function (M) as mediator were statistically significant (Table 9).
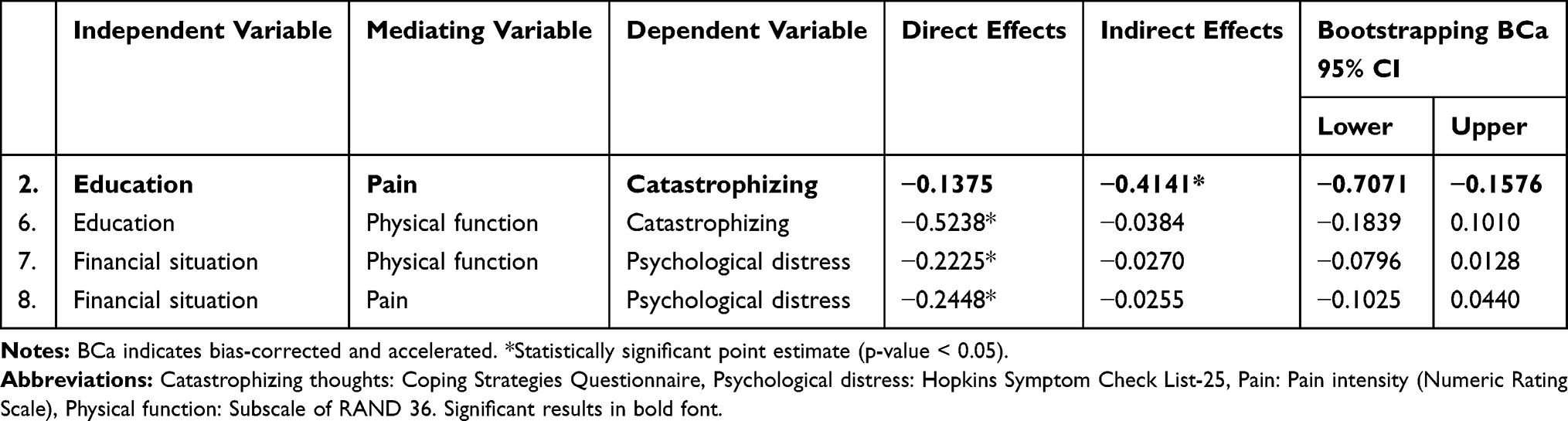 |
Table 9 Summary of Reversed Mediation Models (The Significant Models from Table 8) with Pain and Physical Function as Mediators in Women, Based on 5000 Bootstrap Samples |
Mediation Results in Men
Model number 1 for men examined catastrophizing thoughts (M) as a potential mediator. However, this model was not statistically significant. The models 2–6 examined psychological distress (M) as a potential mediator (Table 10), and one of these five tested models was statistically significant. The indirect effect showed that psychological distress (M) fully mediated the relationship between perceived financial situation (X) and pain intensity (Y) (model number 2). None of the other models were statistically significant (Table 10).
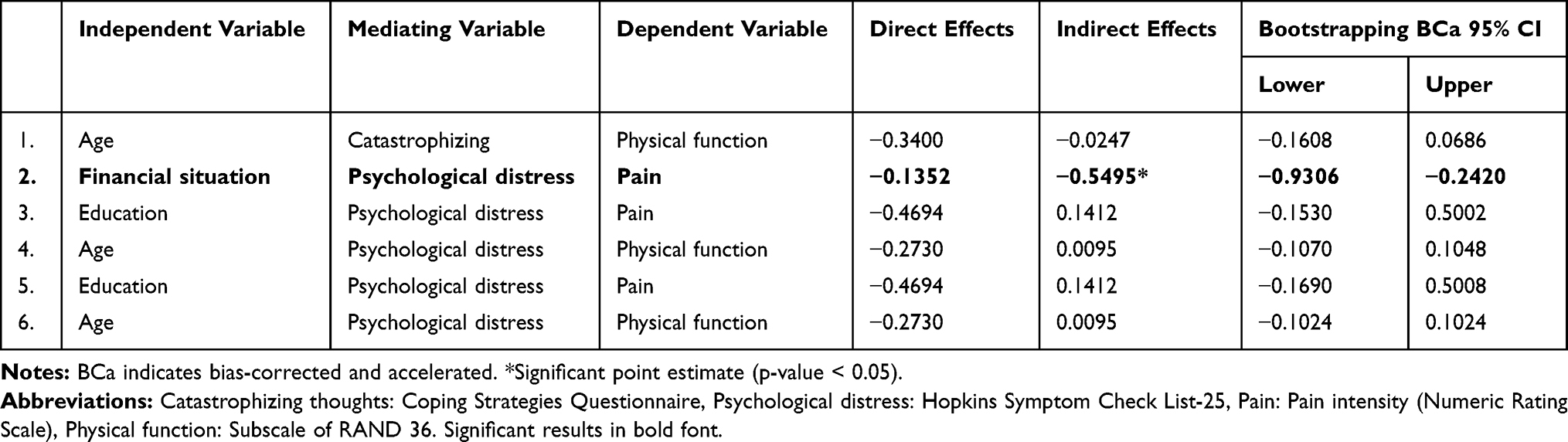 |
Table 10 Summary of Mediation Models with Catastrophizing and Psychological Distress as Mediators in Men, Based on 5000 Bootstrap Samples |
When reversing the significant model (number 2), pain intensity (M) was defined as mediator and psychological distress (Y) as dependent variables (Table 11), and the model was statistically significant (Table 11). The indirect effect confirmed that pain intensity (M) partially mediated the relation between perceived financial situation (X) and psychological distress (Y).
 |
Table 11 Result of Reversed Mediation Model (The Significant Model from Table 10) with Pain as Mediator in Men, Based on 5000 Bootstrap Samples |
Discussion
The comorbidity of psychological distress and chronic pain, and how these health problems are associated with socio-economic status are well documented.23–26 This study confirms these associations and brings further the knowledge of these issues by identifying psychological mediators of these associations. Our results show that catastrophizing thoughts may contribute to increased pain perception in women, not only as a direct relationship as shown by others,42–44 but also as a mediator explaining how other factors are related to pain and physical function. In this way, the results confirm the association between high pain intensity and lower educational level among women, but more importantly, demonstrate that this association is partly mediated by catastrophizing thoughts (Table 8). A similar relation was established for the association between low physical function and lower educational level among women. This relationship was completely mediated by catastrophizing thoughts (Table 8). Indeed, tendencies to catastrophizing thoughts in patients with chronic pain are well known,42,44-48 and has been suggested to aggravate pain and hamper physical function.47 Our findings indicate that the link between physical function and educational level among women with chronic pain was associated with catastrophizing thoughts. In general, negative health effects of negative cognitions like catastrophizing thoughts have been reported both for pain and other health problems48,49 and in association with low socioeconomic status (SES).23,24 Our results thus support and extend this line of research, indicating that catastrophizing thoughts may contribute to health problems among pain patients with low SES, in this study identified by educational level. However, in this cross-sectional study, we cannot conclude about the direction of any causality. The catastrophizing thoughts may lead to a reduced activity level, but could also be due to physical disability.
No mediating effects of catastrophizing thoughts were found among men, although men reported catastrophizing thoughts at a comparable level to women (Table 1). Thus, since women and men with chronic pain have comparable tendencies to catastrophizing thoughts, we may speculate whether these cognitions contribute to perceived health problems among lower educated women but not men, suggesting that women are more vulnerable to these mechanisms than men. Perceived poor financial situation is another SES factor that our results confirmed to be associated with the patients´ health problems. Both women and men with a perceived poor financial situation reported relatively higher pain intensity. However, for both genders, the mediation analyses revealed that these relations were fully explained by psychological distress. It should be noted that our study reports perceived financial situation, and not the patient’s income level. We were not seeking an objective measure of SES, but the subjective appraisal of the financial situation. This taps into the stress component of the concept of economic hardship, as discussed by Rios and Zautra.50 Our findings further suggest that the link between stress related to their personal economy and pain intensity is mediated by a psychological distress. Although other studies have correspondingly found a relation between both poor financial situation and low educational level and pain-related outcomes.,25,26 a causality remains to be confirmed with a prospective study design.
The biopsychosocial model of pain is complex. It involves the interaction of multiple factors, and bidirectional relations between biological, psychological and social factors.51 The reversed models in this study confirm this assumption. One of the reversed models (Model 2, Table 9) showed a relatively stronger, mediating effect of pain intensity on catastrophizing thoughts among women with low education than the hypothesized model (Table 8), where catastrophizing thoughts were mediator. This may suggest that pain intensity triggers catastrophizing thoughts in lower educated women (Table 9). In men, however, the indirect effect of perceived financial situation on psychological distress in the reversed model (Table 11) was only partly mediated by pain intensity, while psychological distress as mediator in the hypothesized model showed a relatively stronger effect (Table 10). This could indicate that psychological distress in a setting of perceived poor financial situation may aggravate the pain intensity in men.
In our study sample and in line with previous studies27,52 the psychological factors catastrophizing thoughts and psychological distress accounted better for pain problems for both genders than demographic factors. For both genders, there were moderate to strong bivariate relations between pain intensity and physical function, and between psychological distress and catastrophizing. These findings have been well established in a range of studies45,53,54 and may reflect that chronic pain causes suffering for both genders.
An important contribution of this study is the detection of mediating factors in the well-established associations between demographic and psychological factors, pain and physical function. Separate analyses for men and women indicated some gender-specific mediators in these relations, but further studies are needed to establish whether there are any significant gender differences.
Limitations and strengths
We investigated psychological and demographic variables based on already known associations with pain and physical functions, but limited by a cross-sectional design we could not conclude on potential causal relations between the investigated variables. Other variables, not included in our analyses, might also contribute to the relationships presented in this paper. The study sample further represents a highly selected sample of patients referred and admitted to a pain clinic, and may not be representative for the population of chronic pain patients in general. Furthermore, a majority of the patients referred to our pain clinic are women, and we cannot rule out gender or other biases in the referral practice by GPs and referring hospitals.
The questionnaire was primarily compiled for clinical use and some categorical questions concerning work, education and perceived financial situation were not validated. However, the HSCL-25, RAND-36, NRS, 2-items from CSQ are validated and frequently used in clinical research.
A strength of the study is the inclusion of a complete population admitted to a multidisciplinary pain clinic within a given time frame representing the most complex cases, which increases the generalizability for patients referred to multidisciplinary pain clinics.
The methodological approach, testing potential mediations, further provides new insights to the complex relation between factors associated with pain and physical function in patients with chronic pain. With this insight, we can establish new hypotheses on causality for future research on more individualized and gender-specific treatment programs.
Conclusion
This study identified mediating psychological variables associated with pain intensity and physical function. This may have important clinical implications, directing clinicians’ awareness to the complex relationships of demographics and psychological factors mediating chronic pain and physical function, and suggesting a more gender-specific, multidisciplinary approach in the treatment of chronic pain. The findings also imply the need for further research on this topic.
Acknowledgments
The project was funded by the Northern Norway Regional Health Authority.
The publication charges for this article have been funded by a grant from the publication fund of UiT The Arctic University of Norway.
Disclosure
Lena Danielsson reports grants from Northern Norway Regional Health Authority during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Mogil JS. Sex differences in pain and pain inhibition: multiple explanations of a controversial phenomenon. Nat Rev Neurosci. 2012;13(12):859–866. doi:10.1038/nrn3360
2. Fillingim RB. Sex, gender, and pain: women and men really are different. Curr Rev Pain. 2000;4(1):24–30. doi:10.1007/s11916-000-0006-6
3. Picavet HSJ, Hazes JMW. Prevalence of self reported musculoskeletal diseases is high. Ann Rheum Dis. 2003;62(7):644–650. doi:10.1136/ard.62.7.644
4. Ostrom C, Bair E, Maixner W, et al. Demographic predictors of pain sensitivity: results from the OPPERA study. J Pain. 2017;18(3):295–307. doi:10.1016/j.jpain.2016.10.018
5. Racine M, Tousignant-Laflamme Y, Kloda LA, Dion D, Dupuis G, Choinière M. A systematic literature review of 10 years of research on sex/gender and experimental pain perception – part 1: are there really differences between women and men? Pain. 2012;153(3):602–618. doi:10.1016/j.pain.2011.11.025
6. Rosen S, Ham B, Mogil JS. Sex differences in neuroimmunity and pain. J Neurosci Res. 2017;95(1–2):500–508. doi:10.1002/jnr.23831
7. Sorge RE, Totsch SK. Sex differences in pain. J Neurosci Res. 2017;95(6):1271–1281. doi:10.1002/jnr.v95.6
8. Suso-Ribera C, Garcia-Palacios A, Botella C, Ribera-Canudas MV. Pain catastrophizing and its relationship with health outcomes: does pain intensity matter? Pain Res Manage. 2017;2017:9762864. doi:10.1155/2017/9762864
9. Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–1156. doi:10.1097/00007632-200005010-00017
10. Nicholl BI, Macfarlane GJ, Davies KA, Morriss R, Dickens C, McBeth J. Premorbid psychosocial factors are associated with poor health-related quality of life in subjects with new onset of chronic widespread pain – results from the EPIFUND study. Pain. 2009;141(1–2):119–126. doi:10.1016/j.pain.2008.10.022
11. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433–2445. doi:10.1001/archinte.163.20.2433
12. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013;111(1):52–58. doi:10.1093/bja/aet127
13. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
14. Keogh E, Eccleston C. Sex differences in adolescent chronic pain and pain-related coping. Pain. 2006;123(3):275–284. doi:10.1016/j.pain.2006.03.004
15. Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression, chronic pain, and disability in primary care. Psychosom Med. 2006;68(2):262–268. doi:10.1097/01.psy.0000204851.15499.fc
16. Mossey JM, Gallagher RM. The longitudinal occurrence and impact of comorbid chronic pain and chronic depression over two years in continuing care retirement community residents. Pain Med. 2004;5(4):335–348. doi:10.1111/j.1526-4637.2004.04041.x
17. Munce SEP, Stewart DE. Gender differences in depression and chronic pain conditions in a national epidemiologic survey. Psychosomatics. 2007;48(5):394–399. doi:10.1176/appi.psy.48.5.394
18. Unruh AM. Gender variations in clinical pain experience. Pain. 1996;65(2):123–167. doi:10.1016/0304-3959(95)00214-6
19. Calvó-Perxas L, Vilalta-Franch J, Turró-Garriga O, López-Pousa S, Garre-Olmo J. Gender differences in depression and pain: a two year follow-up study of the survey of health, ageing and retirement in Europe. J Affect Disord. 2016;193:157–164. doi:10.1016/j.jad.2015.12.034
20. Keefe FJ, Lefebvre JC, Egert JR, Affleck G, Sullivan MJ, Caldwell DS. The relationship of gender to pain, pain behavior, and disability in osteoarthritis patients: the role of catastrophizing. Pain. 2000;87(3):325–334. doi:10.1016/S0304-3959(00)00296-7
21. Vartiainen P, Heiskanen T, Sintonen H, Roine RP, Kalso E. Health-related quality of life change in patients treated at a multidisciplinary pain clinic. Eur J Pain. 2019;23(7):1318–1328. doi:10.1002/ejp.1398
22. Hysing E-B, Smith L, Thulin M, Karlsten R, Butler S, Gordh T. Identifying characteristics of the most severely impaired chronic pain patients treated at a specialized inpatient pain clinic. Scand J Pain. 2017;17(1):178. doi:10.1016/j.sjpain.2017.09.008
23. Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med. 2013;90:24–31. doi:10.1016/j.socscimed.2013.04.026
24. Gallo LC, Matthews KA. Understanding the association between socioeconomic status and physical health: do negative emotions play a role? Psychol Bull. 2003;129(1):10–51. doi:10.1037/0033-2909.129.1.10
25. Poleshuck EL, Green CR. Socioeconomic disadvantage and pain. Pain. 2008;136(3):235–238. doi:10.1016/j.pain.2008.04.003
26. Latza U, Kohlmann T, Deck R, Raspe H. Can health care utilization explain the association between socioeconomic status and back pain? Spine. 2004;29(14):1561–1566. doi:10.1097/01.BRS.0000131435.56714.15
27. Newman AK, Van Dyke BP, Torres CA, et al. The relationship of sociodemographic and psychological variables with chronic pain variables in a low-income population. Pain. 2017;158(9):1687–1696. doi:10.1097/j.pain.0000000000000964
28. Fredheim OBP, Landmark T. Et nytt skjema for kartlegging av smerter. Tidskrift Norsk Legeforening. 2008;18(128):2082–2084.
29. Klepstad P, Loge JH, Borchgrevink PC, Mendoza TR, Cleeland CS, Kaasa S. The Norwegian brief pain inventory questionnaire: translation and validation in cancer pain patients. J Pain Symptom Manage. 2002;24(5):517–525. doi:10.1016/S0885-3924(02)00526-2
30. Keller S, Bann CM, Dodd SL, Schein J, Mendoza TR, Cleeland CS. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin J Pain. 2004;20(5):309–318. doi:10.1097/00002508-200409000-00005
31. Tan G, Nguyen Q, Cardin SA, Jensen MP. Validating the use of two-item measures of pain beliefs and coping strategies for a veteran population. J Pain. 2006;7(4):252–260. doi:10.1016/j.jpain.2005.11.007
32. Jensen MP, Keefe FJ, Lefebvre JC, Romano JM, Turner JA. One- and two-item measures of pain beliefs and coping strategies. Pain. 2003;104(3):453–469. doi:10.1016/S0304-3959(03)00076-9
33. Ware JE, Sherbourne CD, The MOS. 36-Item short-form health survey (SF-36): i. conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
34. Strand BH, Dalgard OS, Tambs K, Rognerud M. Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nord J Psychiatry. 2003;57(2):113–118. doi:10.1080/08039480310000932
35. Hesbacher PT, Rickels K, Morris RJ, Newman H, Rosenfeld H. Psychiatric illness in family practice. J Clin Psychiatry. 1980;41(1):6–10.
36. Nettelbladt P, Hansson L, Stefansson CG, Borgquist L, Nordstrom G. Test characteristics of the Hopkins Symptom Check List-25 (HSCL-25) in Sweden, using the Present State Examination (PSE-9) as a caseness criterion. Soc Psychiatry Psychiatr Epidemiol. 1993;28(3):130–133. doi:10.1007/BF00801743
37. Sandanger I, Moum T, Ingebrigtsen G, Dalgard OS, Sørensen T, Bruusgaard D. Concordance between symptom screening and diagnostic procedure: the hopkins symptom checklist-25 and the composite international diagnostic interview I. Soc Psychiatry Psychiatr Epidemiol. 1998;33(7):345–354. doi:10.1007/s001270050064
38. Dong Y, Peng C-YJ. Principled missing data methods for researchers. SpringerPlus. 2013;2(1):222. doi:10.1186/2193-1801-2-222
39. Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr. 2009;76(4):408–420. doi:10.1080/03637750903310360
40. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
41. Wolfe F, Smythe HA, Yunus MB, et al. The american college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheumatism. 1990;33(2):160–172. doi:10.1002/(ISSN)1529-0131
42. Leung L. Pain catastrophizing: an updated review. Indian J Psychol Med. 2012;34(3):204–217. doi:10.4103/0253-7176.106012
43. Sullivan MJL, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. doi:10.1097/00002508-200103000-00008
44. Burns LC, Ritvo SE, Ferguson MK, Clarke H, Seltzer Z, Katz J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: a systematic review. J Pain Res. 2015;8:21–32. doi:10.2147/JPR.S64730
45. Edwards RR, Cahalan C, Mensing G, Smith M, Haythornthwaite JA. Pain, catastrophizing, and depression in the rheumatic diseases. Nat Rev Rheumatol. 2011;7(4):216–224. doi:10.1038/nrrheum.2011.2
46. Edwards RR, Haythornthwaite JA, Sullivan MJ, Fillingim RB. Catastrophizing as a mediator of sex differences in pain: differential effects for daily pain versus laboratory-induced pain. Pain. 2004;111(3):335–341. doi:10.1016/j.pain.2004.07.012
47. Sullivan MJL, Stanish W, Waite H, Sullivan M, Tripp DA. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain. 1998;77(3):253–260. doi:10.1016/S0304-3959(98)00097-9
48. Wertli MM, Eugster R, Held U, Steurer J, Kofmehl R, Weiser S. Catastrophizing—a prognostic factor for outcome in patients with low back pain: a systematic review. Spine J. 2014;14(11):2639–2657. doi:10.1016/j.spinee.2014.03.003
49. Verkuil B, Brosschot JF, Gebhardt WA, Thayer JF. When worries make you sick: a review of perseverative cognition, the default stress response and somatic health. J Exp Psychopathol. 2010;1(1):
50. Rios R, Zautra AJ. Socioeconomic disparities in pain: the role of economic hardship and daily financial worry. Health Psychol. 2011;30(1):58–66. doi:10.1037/a0022025
51. Fillingim RB. Heritability of catastrophizing: the biopsychosocial model in action. Pain. 2015;156(3):357–358. doi:10.1097/01.j.pain.0000460338.16353.8e
52. Day MA, Thorn BE. The relationship of demographic and psychosocial variables to pain-related outcomes in a rural chronic pain population. PAIN®. 2010;151(2):467–474. doi:10.1016/j.pain.2010.08.015
53. Hassett AL, Cone JD, Patella SJ, Sigal LH. The role of catastrophizing in the pain and depression of women with fibromyalgia syndrome. Arthritis Rheumatism. 2000;43(11):2493–2500. doi:10.1002/(ISSN)1529-0131
54. Scott EL, Kroenke K, Wu J, Yu Z. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain. 2016;17(2):215–222. doi:10.1016/j.jpain.2015.10.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.