")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mediating Role of Teamwork in the Influence of Team Role on Team Performance
Authors Han C, Zhang L, Liu J, Zhang P
Received 1 November 2022
Accepted for publication 4 January 2023
Published 17 April 2023 Volume 2023:16 Pages 1057—1066
DOI https://doi.org/10.2147/JMDH.S394670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chunjie Han,1,* Lingli Zhang,2,* Jihong Liu,2 Ping Zhang3
1Department of Rehabilitation Medicine, Beijing Luhe Hospital, Capital Medical University, Beijing, 101149, People’s Republic of China; 2Department of Neurology, Beijing Luhe Hospital, Capital Medical University, Beijing, 101149, People’s Republic of China; 3Department of Nursing, Beijing Rehabilitation Hospital, Capital Medical University, Beijing, 100144, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jihong Liu, Department of Neurology, Beijing Luhe Hospital, Capital Medical University, No. 82 of Xin Hua South Road, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel +86 10-69543901-1041, Fax +86 10 69531069, Email [email protected] Ping Zhang, Department of Nursing, Beijing Rehabilitation Hospital, Capital Medical University, No. 15 of Xixiazhuang South Road, Shijingshan District, Beijing, 100144, People’s Republic of China, Tel +86 10 5689 1513, Fax +86 10 5698 1555, Email [email protected]
Objective: As an important hospital task, the quality and efficiency of nursing practice directly affect the medical quality and sustainable development of the hospital. Increasing attention is now paid by managers to nursing teamwork. From the level of the nursing team, this study explored the relationship between team roles, using teamwork as the intermediate variable, and team performance to provide a theoretical foundation for the human resource management of nursing managers.
Methods: Taking 29 general inpatient areas of a tertiary general hospital in Beijing as research objects, a questionnaire survey was used to collect basic information on nursing staff, teamwork, team roles and team performance. The collected data were analysed. A pathway analysis based on a multiple regression analysis was used to interpret the effect of each team role on teamperformance.
Results: ①The mean and maximum value of emotional type (Teamworker and Finisher) were the largest in the role combination of nursing team. In the team role combination, the average value of emotional type was 12.58 ± 1.48, with significant difference (P< 0.001). ② The average level of emotion, thinking and decision of team role combination is positively correlated with work performance; The average level and maximum value of emotion have a positive correlation with team cooperation; The average level of willingness was negatively correlated with team cooperation, job performance and satisfaction (P< 0.05). ③ Teamwork plays a certain intermediary role in the mean value of emotion to improve level of team satisfaction and performance.
Conclusion: This study identified the important roles of different types of nursing staff in work performance and used a pathway analysis to create a path showing each role. Increasing the emotional-type nursing staff in a team can not only improve the mean level of team emotion but also effectively improve both teamwork and work performance.
Keywords: nursing staff, teamwork, team role, team performance, intermediary role
Introduction
The teamworking mode, with flexibility and good coordination, is the preferred management mode of the majority of managers. Robbins,1 a famous American organisational behaviourist, stated that a team is a formal group of individuals who cooperate in order to achieve a common goal. Every member of this group plays a specific role and performs particular responsibilities. According to Dr Belbin,2,3 “team role” refers to the tendency of the behaviours, contributions and interpersonal interactions of individual members within a group. From a psychological point of view, team roles refer to the way that team members behave when they interact with other members in order to promote the development of the whole team.4 People tend to have different team roles due to personality and other factors. Different team members comprise different team structures, which lead to different performances.5,6 As nursing work is one of the important functions of a hospital, the quality and efficiency of that work directly affect the medical quality and sustainable development of the hospital.7 Applying the team concept to hospital management has a positive significance in improving the management level and competitiveness of the hospital.8
Research shows that strengthening the construction of a nursing team requires the reasonable allocation of nursing staff in various roles; this is conducive to the complementary functions of nursing staff, improving the cooperation of nurses, jointly achieving team goals, ensuring patient safety and improving both quality and performance.9 A recent study found the importance of professional development activities that go beyond knowledge- or skill-based training. Activities that cater to nurses’ personal professional development needs are also associated with more positively perceived teamwork and performance. Their findings provide insights into the mediating mechanisms: Participation in personal professional development activities encouraged reflective thinking, which was associated with better-perceived teamwork and performance.10
Many researchers have adopted the “input–process–output” theoretical framework to evaluate team performance. McGrath’s11 descriptive performance evaluation model indicates that the team’s input variable affects the output variable, which is mediated by the process variable. Strengthening team building to change input variables and process variables is an important way to improve team performance.12 Related studies also prove that a team’s structural and process factors are two important aspects affecting team performance, and changing either factor has a positive effect on improving performance.13
Team role theory is a theoretical discussion based on team structural factors.13 In recent years, team role theory has become a research focus in terms of team structural factors, but there is very little research on the correlation between nursing team roles and team performance. The team role theory used in this current study is shown in Figure 1. Therefore, based on Belbin’s team role theory and McGrath’s11 descriptive performance evaluation model, this study explored the relationship between nursing team roles and team performance, with teamwork as an intermediate variable, and laid a theoretical foundation for human resource management by nursing managers.
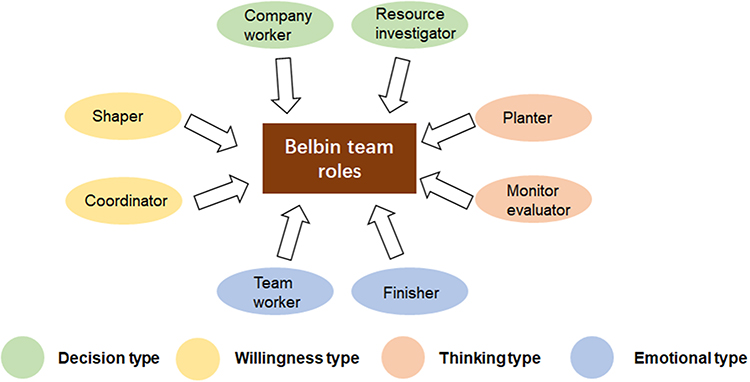 |
Figure 1 Schematic diagram showed the team roles theory used in the current study. |
Study Objects
Study Teams
According to the principle of convenience sampling, this study took 29 general inpatient areas of a tertiary general hospital in Beijing as research objects. These teams had been established for more than 2 years and were in a stable period according to the development stage of the teams.
Study Members
The inclusion of the team members mainly followed the principle of cluster sampling, and all nurses who contributed to performance performance during team data collection were selected. The inclusion criteria were ① registered nurses, ② working department remained unchanged during data collection, ③ independent practice and ④ provided informed consent to participate in this study. The exclusion criteria were ① rotation nurses, ② refresher nurses, ③ nurses transferred in a department during the data collection period and ④ nurses who were taken off for ≥2 months during the data collection period.
Study Tools
Questionnaire
This part was designed according to the relevant documents and included the basic information of the survey participants, including their department, gender, age, nursing duration, professional title, academic background, post level and position.
In this study, Belbin’s team role self-perception inventory5 was used, which was divided into two parts: the instruction language and the main body. The main body comprised seven parts, and it was scored out of 70 points. Each part had eight questions, totalling 10 points, which were assigned to eight questions. The principle of distribution was that the problem that best reflects a person’s behaviour scored the highest, and so on. The most extreme case could score 10 points in response to one of the questions. For the reliability analysis of the Chinese version, the Cronbach’s α coefficient of this questionnaire in some studies5 was emotional type = 0.710, willingness type = 0.674, thinking type = 0.742 and decision type = 0.751, with a total table Cronbach’s α coefficient of 0.672.
In the scale, the testing problems of each role were scattered. Each role comprised seven questions, and the role score was obtained by totalling the scores of the seven questions. Role typing involved adding the scores of two roles to obtain the average. The score values of the roles were counted, as shown in Table 1.14
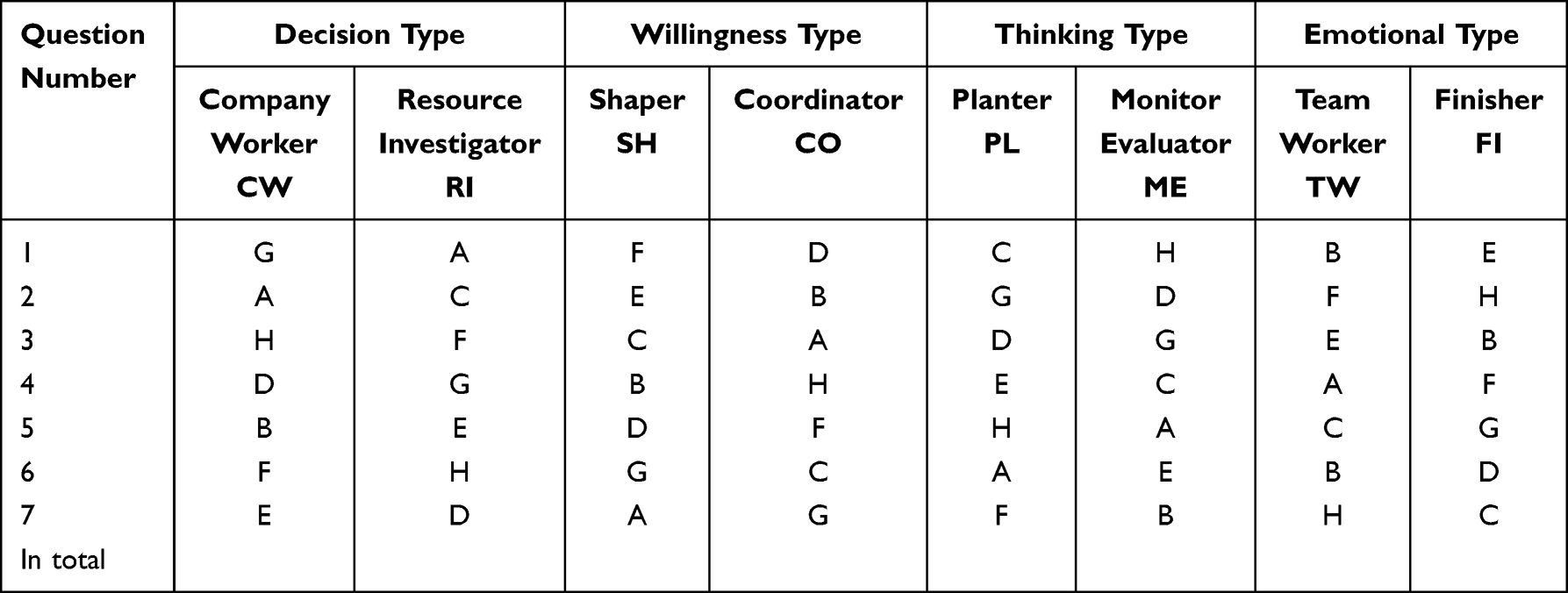 |
Table 1 Statistical Order of the Team Role Test Options |
In terms of the quantitative measures of the team role combination, this study used the average level and the maximum, which were expressed as the average and the maximum scores of each type of all the tested members of the team.
This study used the Chinese version of the special nurse job satisfaction scale, which was translated from the English version of the McCloskey/Mueller Satisfaction Scale [MMSS] by He et al.15 The MMSS scale was used to measure the level of clinical nurse job satisfaction and influencing factors. It contained a total of 8 dimensions with 31 items and was divided into welfare treatment (3 items), scheduling system (6 items), family and work balance (3 items), colleague relationship (2 items), social and professional communication opportunities (4 items), professional development opportunities (5 items), work praise and recognition (4 items) and work quality control and decision making (4 items). Each item was graded as “very satisfied” (5 points), “satisfied” (4 points), “general” (3 points), “unsatisfactory” (2 points) and “very unsatisfactory” (1 point). A higher score indicated higher job satisfaction, and an average score of 3.03 was the lowest score for the job satisfaction evaluation. The internal consistency coefficient of the English version of this scale was 0.97, and the Pearson reliability correlation coefficient of the Chinese version was 0.758.15–18 Team satisfaction was calculated as the average satisfaction of all the nurses in a team.
The nursing teamwork status questionnaire developed by Kaliseh et al19 and translated by Song et al18 was used for evaluation. The questionnaire is the only one designed for the study of teamwork among nursing staff. Research has proved that the questionnaire can effectively measure the degree of nurse team cooperation by a nurse in a team or department. The questionnaire involved 5 dimensions with 32 items, including 7 items for “trust”, 6 items for “support”, 7 items for “team mental model”, 4 items for “leadership”, and 8 items for “team orientation”. A five-level score of “almost none” (5 points), “25% of the time” (4 points), “50% time” (3 points), “75% time” (2 points) and “always” (1 point) was used. The internal consistency reliability Cronbach’s α of the English version of this questionnaire was 0.94 overall, with 0.74~0.85 for each dimension. A pre-survey showed that in the Chinese version of the questionnaire, Cronbach’s α coefficient was 0.908, with 0.717–0.839 for each dimension.18 Teamwork status was calculated as the average of all the nurses in a team.
Teamwork Performance Evaluation Tool
The evaluation index for team performance was an evaluation system based mainly on the quantity and quality of nursing work devised by the nursing department by consulting the literature and referring to previous research.20–22 It mainly included the proportion of Primary Care, the per capita nursing workload ratio, the accompanying occupancy rate, patient satisfaction and nursing quality, and it adopted a 100-point scoring system for assessment.
Data Collection and Quality Control
Team Role, Nurse Job Satisfaction and Teamwork Status Data
Data on team roles, nurse job satisfaction and teamwork were collected via the questionnaire. An investigator was aided by a regular member of the research team. The survey site was located in the conference room of each department, and the specific process was as follows: ① The investigator explained the purpose and significance of the investigation to the head nurse of the nursing department and each department to ensure cooperation. ② The investigator and the head nurse explained to the nursing staff the purpose of the questionnaire, promised confidentiality of the questionnaire’s information and explained the methods and requirements for its completion. ③ There was no time limit for completing the questionnaire. ④ Questionnaire completion: On the premise of uniform guidance, self-evaluation was conducted after fully understanding the meaning of the entry, which was required to be completed independently on the spot and was returned on the spot after completion. ⑤ The respondents were thanked. ⑥ The questionnaire was evaluated on the same day.
Team Performance Data
Every month, the full-time staff of the nursing departments used the observation method to collect the data according to the quality control standard, collect the workload via their computer system and calculate the work performance score of each team according to the performance evaluation index. To reduce bias in the results, this study calculated work performance from the 12-month mean throughout the year.
Statistical Analysis
The analysis was performed using SPSS 17.0software. Measurement data conforming to a normal distribution were described by  , and a rank–sum test was used for comparisons between groups. Count data were described using examples and percentages and were compared between groups using the χ2 test. The correlation between the scores for emotion, willingness, thinking and decision, and the team status, team performance and nurse job satisfaction was determined using a Pearson correlation analysis and a multiple regression analysis. The path analysis and path drawing were based on the multiple results of multiple regression analyses and used common knowledge and rational logic to determine the correlation order. A value of P < 0.05 was statistically significant.
, and a rank–sum test was used for comparisons between groups. Count data were described using examples and percentages and were compared between groups using the χ2 test. The correlation between the scores for emotion, willingness, thinking and decision, and the team status, team performance and nurse job satisfaction was determined using a Pearson correlation analysis and a multiple regression analysis. The path analysis and path drawing were based on the multiple results of multiple regression analyses and used common knowledge and rational logic to determine the correlation order. A value of P < 0.05 was statistically significant.
Study Results
Participants’ Basic Information
A total of 376 questionnaires were distributed, and 376 were recovered in this study. Two questionnaires with missing answers and 3 questionnaires with trend answers were excluded. Finally, there were 371 valid questionnaires, with an effective recovery rate of 98.7%. The 371 respondents were from 29 teams; all were female, aged 22–55 years, with a median of 27 years. Among them, 256 were aged 22–30 years, 86 were aged 31–40 years, 20 were aged 41–50 years, and 9 were aged >50 years. The nursing duration ranged from 1 to 34 years, with a median of 6 years. In terms of academic background level, 21 (5.7%) attended a middle special school, 205 (55.3%) attended college, and 145 (39.1%) had a bachelor’s degree or above. In terms of title, 104 nurses (28.0%) had a professional title, 201 (54.2%) were nurse practitioners, 62 (16.7%) were charge nurses, and 4 (1.1%) were deputy chief nurses or above. The total enrolment was 110 (29.6%) enrolled employees and 261 (70.4%) non-enrolled employees. According to the standards of nursing age and working ability, the respondents were divided into grades N1–N3 and head nurses, including 157 (42.3%) N1 nurses, 122 (32.9%) N2 nurses, 63 (17.0%) N3 nurses and 29 (7.8%) head nurses. The detailed information is shown in Table 2.
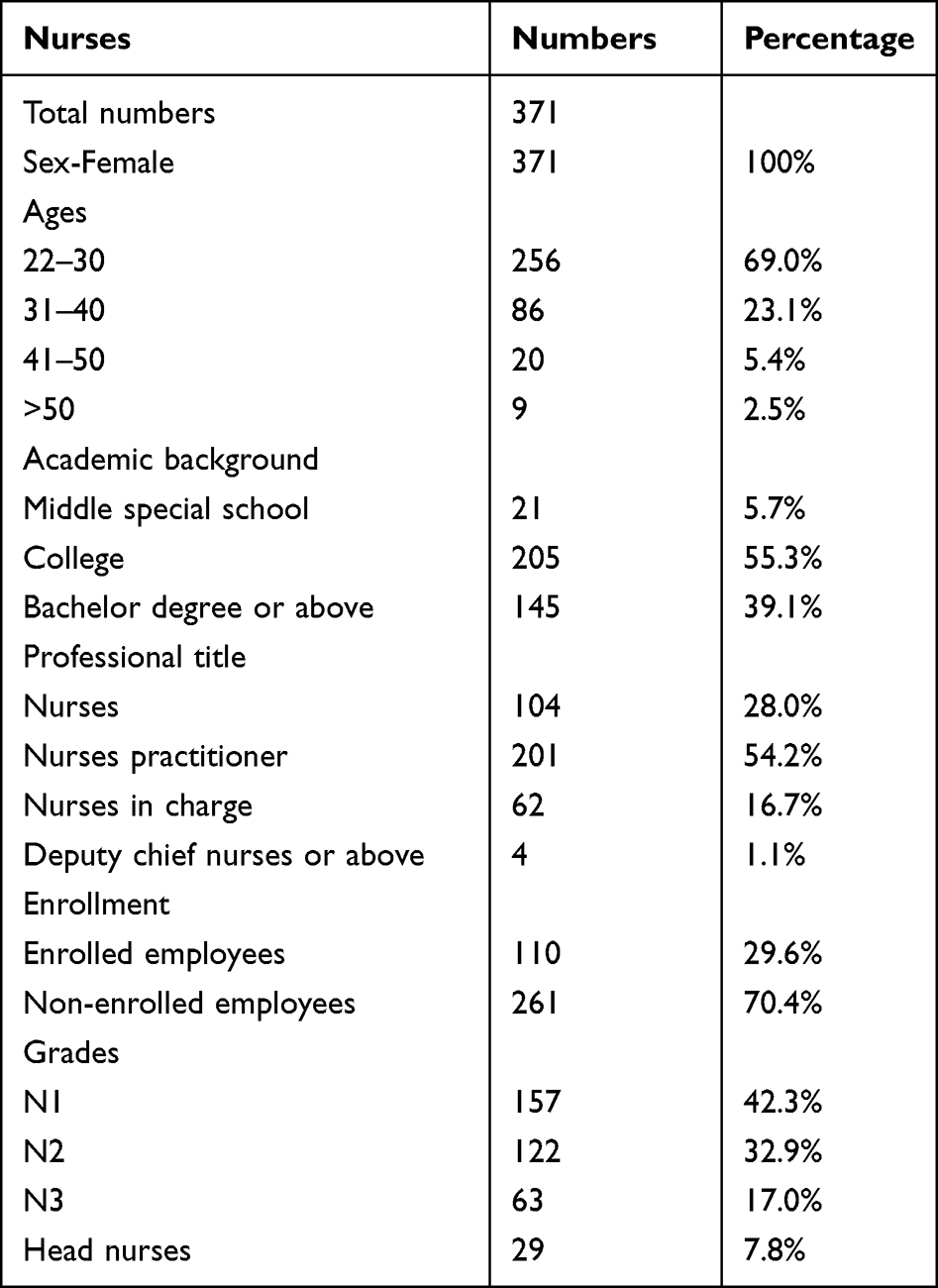 |
Table 2 Basic Information of the Study Subjects |
Distribution of Team Role Combination
The average and maximum values of the team members’ role combination were normally distributed (P > 0.05, Table 3) and were described by ¯χ ± S. The nursing team role self-evaluation score varied, with the highest average scores being for the emotional type (12.58 ± 1.48), followed by decision type (8.73 ± 0.96), willingness type (7.52 ± 2.39) and thinking type (6.16 ± 1.04). The variance of the mean value and the maximum value was not homogeneous (homogeneity test for mean value: P < 0.001, maximum value: P = 0.005); therefore, the rank–sum test was used to analyse the differences in the four types of scores. The results showed that the differences in the mean and maximum values of the emotional, willingness, thinking and decision subtypes were all statistically significant (P < 0.001, Table 4).
 |
Table 3 Normal Distribution Test of Nursing Team Role Combination (n=371) |
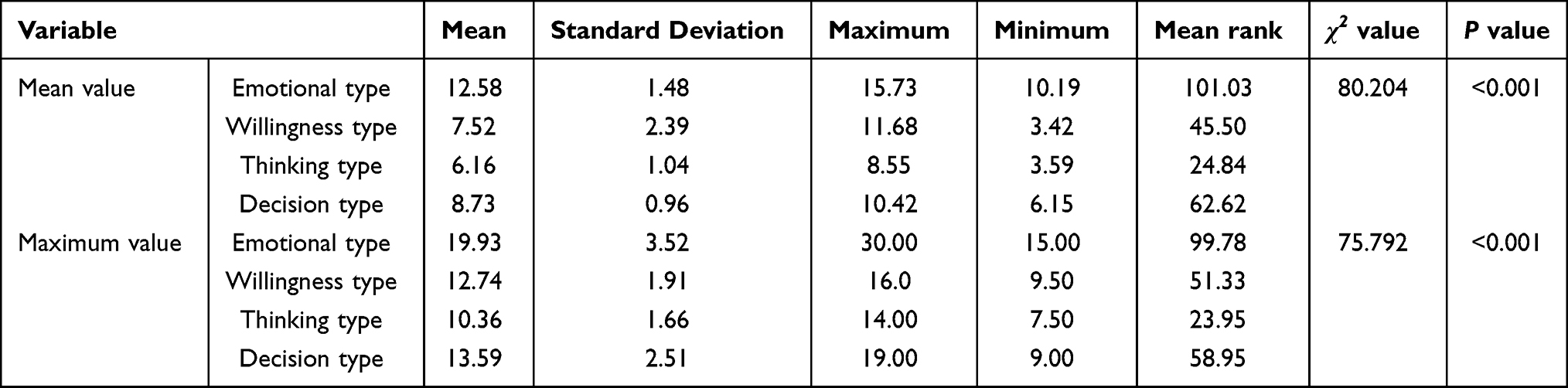 |
Table 4 Descriptive Statistics and Comparison of Nursing Team Role Combination (n=371) |
Teamwork, Performance and Satisfaction
Teamwork, work performance and nurse job satisfaction were normally tested for a normal distribution (P > 0.05) and were described by ¯χ ± S. The 29 nursing teams had an average score of (3.97 ± 0.23) for teamwork, (88.82 ± 3.59) for work performance and (3.37 ± 0.30) for nurse satisfaction. The standard deviation for teamwork and work performance was small, while the job satisfaction of the nurses in the various teams was not quite uniform. The minimum value was 2.93 points, which did not reach the minimum standard of the job evaluation satisfaction score of 3.03 points, and the maximum value was 4.09 points (see Table 5). Out of 29 teams, 3 scored below 3.03 points for team satisfaction. According to the evaluation scale, the nurses in some departments (10.34%) had low overall job satisfaction.
 |
Table 5 Descriptive Statistics of Teamwork, Job Performance and Satisfaction (n=371) |
Pathway Analysis of Team Role Combination of Average Level, Teamwork and Work Performance
Three steps13,22 are needed according to the mediation role: The first step is the regression of the dependent variable to the independent variable to observe whether the regression coefficient is significant. If it is significant, proceed to the next step. The second step is the regression of the intermediary variable to the independent variable to observe whether the regression coefficient is significant. If it is significant, the final step is taken. In the final step, the dependent variable is regressed on both the independent variable and the intermediary variable.
In the regression analysis of the average level of team roles combined for teamwork and work performance, the regression coefficient was significant (P < 0.05); that is, the third step could be performed through the first two steps of mediation. When the emotional average level of team role and teamwork combined entered the regression model simultaneously, the Beta value of the independent variable decreased from 0.553 to 0.448 (Table 6). Through a significance test, teamwork played an intermediary role in the average level of team emotion, improving team performance.
 |
Table 6 Teamwork as a Mediation Variable of Emotional Average Level Influencing Teamwork Performance |
We explored the indirect role of teamwork between the two variables, with work performance as the dependent variable and the average level of team role combination as the independent variable. From the correlation analysis and regression model, the path analysis of the average level of team role combination and teamwork, team performance and satisfaction is shown in Figure 2.
Figure 2 reveals that in the path analysis of the team role combination of average level and teamwork on work performance, the average level for decision had a direct effect on work performance (β = 0.394, P <0.05), the average level for thinking had a direct effect on work performance (β = 0.422, P <0.01), and the average level for emotion had an indirect effect on work performance and team satisfaction (β = 0.493, P < 0.01) through teamwork.
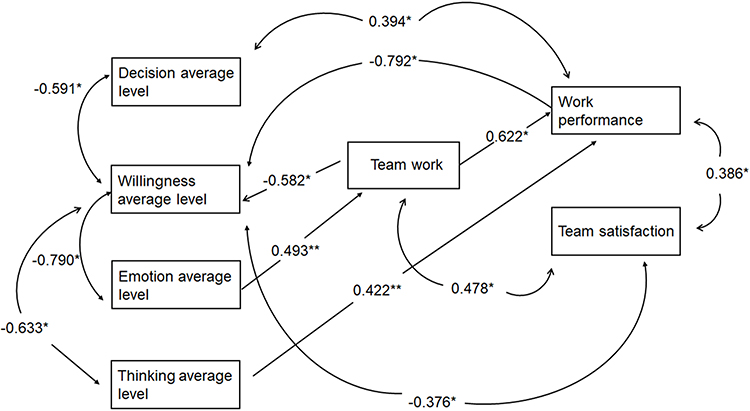 |
Figure 2 Path analysis of the mean level of nursing team role combination and team performance. Variables were linked by arrows that indicated the directions of the causal relationships, straight arrows pointed in one direction indicated that a variable cannot be both a cause and an effect of another variable; curved, double-headed arrows indicate correlation between exogenous variables. The number indicated the Beta coefficient, and *P <0.05, **P <0.01 were considered as significant. |
Discussion
In the nursing team role self-evaluation score for type, the 29 teams scored the highest for emotional roles, indicating that the staff were more inclined to be emotional members within the team. Emotional members are centred on completing team tasks. They pay more attention to team tasks, the relationships between team members and the team atmosphere. They trust that the members can support each other, maintain team cohesion and play a positive role in team satisfaction, communication and cooperation, and, when there are problems, actively coordinate.23 Emotional members include two main types: Team Worker (TW) and Finisher(FI); among them, the Finisher(FI) members work diligently and orderly, perform well and pay attention to details, which is in line with the characteristics of complicated nursing work and the need for carefulness and patience and is conducive to the achievement of teamwork and the improvement of performance. The typical characteristics of the TW are that they are good at helping others and taking measures to alleviate conflicts to reduce friction between team members, and they play a major role in enhancing team cohesion. It can be seen that with the more emotional members of the team, the higher the tendency, the higher the cohesion and the higher the level of team cooperation.
Similar to our findings, a recent study also reported that nurse–nurse collaboration is linked to benefits for nurses in terms of improved job satisfaction, better nurse retention, improved quality of patient care and enhanced healthcare efficiency and productivity. This suggests that improving nurse–nurse collaboration may have consequential beneficial effects, not only for nurses but also for patients, organisations and the overall healthcare system.24
In a responsible nursing system with a clear division of labour, nurses have both a division of labour and cooperation. Because the requirements of 24-hour continuous inpatient nursing practice cannot be completed independently by one nurse and require the cooperation of the whole nursing team, nurses must rely on each other for support. In the form of teamwork, joint efforts can achieve both the nursing care of patients and the success of the organisation.25 According to the definition of the team,26–30 all the nurses in each ward can form a team, and the nursing team formed in the ward’s nursing unit can fully meet the basic characteristics of the team.31 Cooperation plays an important role in improving the quality of nursing, so nurses should perform efficient shift handovers and develop complementary skills. For example, when a nurse is off work, they must explain a patient’s problems and precautions to the next nurse to ensure the safety of the patient. The two nurses must cooperate well. Any problems will lead to mistakes in the handover, even resulting in medical accidents. Good cooperation between nurses is also an important guarantee of patient safety and high-quality care. There are many collaborative situations in nursing work, such as turning over patients and changing bed sheets. Meanwhile, well-skilled nurses can help junior nurses to improve the success rate of venepuncture, and senior nurses can guide junior nurses. It can be seen that cooperative relationship plays an important role in improving nursing quality.
Through a correlation analysis and a regression model, this study showed that the mean decisional level has a direct effect on work performance, the mean thinking level has a direct effect on work performance, and the mean emotional level has an indirect effect on both work performance and team satisfaction through teamwork. Teamwork in a nursing team plays a certain intermediary role at the mean emotional level, thereby improving teamwork performance (P < 0.05). The higher the emotional tendency, the better the promotion of collaboration between nurses and the improvement in teamwork level. A recent study found that nurses’ job satisfaction is associated with the level of nursing care provided and teamwork.32 The nursing team comprises individual nursing staff, but the nursing team is not the mechanical addition of the individual attributes of the nurses, who will connect and influence each other within the team. The characteristics and nature of nursing tasks require nursing team members to communicate smoothly, rely on each other and cooperate closely under a unified workflow and standards to ensure the efficient completion of team tasks. Practice has confirmed that good teamwork will produce a 1 + 1 > 2 effect. Studies have also shown that the improvement of nursing staff collaboration can reduce the occurrence of patient falls and ensure patient safety.33 Good collaboration among nurses can enhance technical complementarity and handover efficiency to improve the quality of care.
In summary, this study identified the important roles of different types of nursing staff on work performance and created a pathway to show each role, using a pathway analysis. In nursing practice, the mean emotional level of the team improves the team’s work performance mainly by improving teamwork. Additionally, a team with more emotional members, that is, a team with a high proportion of team workers and finishers tends to achieve better job performance. Hence, the team’s emotional members should be considered more during daily teamwork, and the team should organise activities to increase their emotional level and enhance teamwork.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Beijing Luhe Hospital, Capital Medical University, and informed consent was obtained from all participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stephen P. Robbins Essentials of Organizational Behavior (Zheng Xiaoming, Translator). Beijing: Machinery Industry Press; 2000:161–169.
2. Belbin RM. Management Teams: Why They Succeed or Fail (Zheng Haitao, Translator). Beijing: China National Machinery Industry Press; 2001:44–78.
3. Belbin RM. Management Teams: Why They Succeed or Fail? Oxford: Butterworth-Heinemann; 1994:84–89.
4. Kusi-Appiah E, Dahlke S, Stahlke S, Hunter KF. Acute care nursing team members’ perceptions of roles: their own and each other’s. J Nurs Manag. 2019;27(8):1784–1790. doi:10.1111/jonm.12877
5. Aberdeen SM, Byrne G. Concept mapping to improve team work, team learning and care of the person with dementia and behavioural and psychological symptoms. Dementia. 2018;17(3):279–296. doi:10.1177/1471301216641785
6. Zhang XA, He H, Gu F. The impact of paternalistic leadership behavior on team performance: the intermediary role of team conflict management mode. Manage World. 2009;3:121–133.
7. Koy V, Yunibhand J, Turale S. Comparison of 12 and 24-hours shift impacts on ICU nursing care, efficiency, safety, and work-life quality. Int Nurs Rev. 2022;69(1):38–46. doi:10.1111/inr.12715
8. Zheng XW, Huang QM. Team management in a hospital. Hosp Administration J Chin People Liberation Army. 2007;14(12):899–900.
9. Huang XL. Nursing human resource management and team building. J Tradit Chin Med Manag. 2004;6:40–41.
10. Welp A, Johnson A, Nguyen H, Perry L. The importance of reflecting on practice: how personal professional development activities affect perceived teamwork and performance. J Clin Nurs. 2018;27(21–22):3988–3999. PMID: 29775493. doi:10.1111/jocn.14519
11. McGrath JE. Social Psychology: A Brief Introduction. New York: Holt, Rinehart and Winston; 1964:78.
12. Ling WQ, Zhang ZC. Organizational commitment of enterprise employees. Chin Manag Sci. 1997;3:34–35.
13. Chen G. Team role theory and its application. Hum Resour Dev. 2005;11:86–87.
14. Shao J. Knowledge Sharing Strategy Research for Building a Role Balanced Team [Master’s dissertation]. Nanjing: Nanjing University of Aeronautics and Astronautics; 2007.
15. He SZ. Survey and Analysis of Nurses ‘Job Satisfaction in Secondary or Above General Hospitals in Taiyuan City [Master’s thesis]. Shanxi: Shanxi Medical University; 2006.
16. Waltz LA, Muñoz L, Weber Johnson H, Rodriguez T. Exploring job satisfaction and workplace engagement in millennial nurses. J Nurs Manag. 2020;28(3):673–681. doi:10.1111/jonm.12981
17. He SZ, Zhang BL, Bai LX, Qu CY, Zhang YX. An introduction to the MMSS scale. Nurs Res. 2008;22(12):1063.
18. Song CY, Wang GL, Wu HY. Investigation on cooperation status of nursing teamwork in third-grade hospitals in Wuhan city. Nurs Res. 2014;28(2):406.
19. Kaliseh BJ, Lee H, Salas E. The development and testing of the nursing teamwork survey. Nurs Res. 2010;59(1):42–50. doi:10.1097/NNR.0b013e3181c3bd42
20. Yang X, Shao WL, Han BR, et al. Establishment and application of nursing team performance evaluation system based on post management. Chin Nurs Manag. 2012;12(05):14–17.
21. Dai DM, Fan ST, Li Y, Zhao YL, Yang QP. Effect of nursing quality comprehensive evaluation correction method for performance evaluation of nursing team. Nurs Res. 2013;27(13):1241–1242.
22. Sun YB, Wang JL, Song CM, et al. Establishment and research on performance evaluation index system for clinical nursing unit in class 3 grade 1 general hospitals. China Mod Doctor. 2016;54(16):139–143.
23. Espinoza P, Peduzzi M, Agreli HF, Sutherland MA. Interprofessional team member’s satisfaction: a mixed methods study of a Chilean hospital. Hum Resour Health. 2018;16(1):30. doi:10.1186/s12960-018-0290-z
24. Al-Hamdan ZM, Alyahia M, Al-Maaitah R, et al. The relationship between emotional intelligence and nurse-nurse collaboration. J Nurs Scholarsh. 2021;53(5):615–622. doi:10.1111/jnu.12687
25. Luo QH. Cultivate the nursing team spirit. Mod Hosp. 2006;6(12):115.
26. McHugh SK, Lawton R, O’Hara JK, Sheard L. Does team reflexivity impact teamwork and communication in interprofessional hospital-based healthcare teams? A systematic review and narrative synthesis. BMJ Qual Saf. 2020;29(8):672–683. doi:10.1136/bmjqs-2019-009921
27. Silverio SA, Cope LC, Bracken L, Bellis J, Peak M, Kaehne A. The implementation of a Technician Enhanced Administration of Medications [TEAM] model: an evaluative study of impact on working practices in a children’s hospital. Res Social Adm Pharm. 2020;16(12):1768–1774. doi:10.1016/j.sapharm.2020.01.016
28. Belbin RM. Management Teams: Why they Succeed or Fail. Elsevier Ltd; 2004:12–21.
29. Wang ZJ, Yan ZQ, Jin M. Team-building evaluation and research. J Shanghai Univ. 2000;5:441–447.
30. He YZ. Work management team. China Hum Resour Dev. 2001;6:50–51.
31. Sui HY. Application of Entropy and Dissipation Structure Theory in Team Performance Evaluation- -Take the Hospital Nursing Team as an Example [Master’s thesis]. Zhejiang: Zhejiang Sci-Tech University; 2011.
32. Kalisch BJ, Lee H, Rochman M. Nursing staff teamwork and job satisfaction. J Nurs Manag. 2010;18(8):938–947. doi:10.1111/j.1365-2834.2010.01153.x
33. Kalisch BJ, Curley M, Stefanov S. An intervention to enhance nursing staff teamwork and engagement. J Nurs Adm. 2007;37(2):77–84. doi:10.1097/00005110-200702000-00010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.