")
Back to Journals » Journal of Pain Research » Volume 15
Median Effective Concentration of Ropivacaine for Femoral Nerve Block Maintaining Motor Function During Knee Arthroscopy in Two Age Groups
Authors Tai YL , Peng L, Wang Y, Zhao ZJ, Li YN, Yin CP, Hou ZY, Shao DC, Zhang YH, Wang QJ
Received 10 January 2022
Accepted for publication 21 May 2022
Published 7 June 2022 Volume 2022:15 Pages 1647—1657
DOI https://doi.org/10.2147/JPR.S357750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Yan-Lei Tai,1 Li Peng,1 Ying Wang,2 Zi-Jun Zhao,3 Ya-Nan Li,1 Chun-Ping Yin,1 Zhi-Yong Hou,4 De-Cheng Shao,5 Ya-Hui Zhang,1 Qiu-Jun Wang1
1Department of Anesthesiology, Third Hospital Affiliated to Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Anesthesiology, Tangshan Gongren Hospital, Tangshan, Hebei, People’s Republic of China; 3Department of Anesthesiology, Hebei Chest Hospital, Shijiazhuang, Hebei, People’s Republic of China; 4Center of Emergency and Trauma, Third Hospital Affiliated to Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 5Department of Sport Medicine, Third Hospital Affiliated to Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Qiu-Jun Wang, Department of Anesthesiology, Third Hospital Affiliated to Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China, Tel +8618533112929, Email [email protected]
Background: Femoral nerve block combined with general anesthesia is commonly used for patients undergoing knee arthroscopy in ambulatory care centers. An ideal analgesic agent would selectively (differentially) block sensory fibers, with little or no effect on motor nerves. Ropivacaine is considered to cause less motor block than others. This study investigated the median effective concentration (EC50) of ropivacaine for differential femoral nerve block in adults either younger or older than 60 years.
Methods: Patients with American Society of Anesthesiologists physical status I–III and scheduled for knee arthroscopy were categorized as 18- to 60-years-old (Group 1), or older than 60 years (Group 2). Surgeries were performed under general anesthesia combined with femoral nerve block via 22 mL ropivacaine. The EC50 of ropivacaine for differential femoral nerve block was determined using the up-and-down method and probit regression. The primary outcome was the EC50 (95% confidence interval [CI]) of the 2 groups. Data on the sensory block, analgesic effect, complications, and hemodynamics during surgery were also recorded.
Results: The EC50 of 22 mL ropivacaine for differential femoral nerve block of Group 1 (0.124%, 95% CI 0.097– 0.143%) was significantly higher than that of Group 2 (0.088%, 95% CI 0.076– 0.103%). The sensory block and hemodynamic data of the 2 groups were comparable. None of the patients experienced neurological complications.
Conclusion: The EC50 of ropivacaine administered for differential femoral nerve block during knee arthroscopy was lower in patients older than 60 years, relative to younger adults.
Keywords: femoral nerve block, ropivacaine, motor block, age groups, EC50
Background
Knee arthroscopy is commonly performed in ambulatory care centers. The procedure is accompanied by varying degrees of postoperative pain, including static and dynamic pain. Patients are asked to perform knee flexion exercises within 24 hours after surgery. Effective pain relief and early mobilization are essential for fast-track rehabilitation, according to the principles of Enhanced Recovery After Surgery (ERAS);1 specifically regional analgesia, opioid-sparing anesthesia, and early mobilization. These protocols allow a shorter hospital stay and fewer complications such as postoperative ileus, pneumonia, and venous thrombosis.
General anesthesia combined with femoral nerve block is widely used during knee arthroscopy. The combination facilitates patient recovery through effective perioperative analgesia and reducing the use of long-acting opioids.2 The concentrations of ropivacaine used in clinical practice range from 0.2% to 0.5%. However, these concentrations often cause complete sensory and motor block, and consequently weakness of the quadriceps and delayed mobilization. Data collected during follow-up visits indicate that quadricep weakness may last as long as 20 hours. This interferes with fast-track rehabilitation and can increase the risk of undesirable events such as falling.3 Furthermore, in ambulatory care centers the number of older patients undergoing knee arthroscopy is increasing. Especially for this population, long-term immobilization in bed may be associated with a higher incidence of postoperative complications.
Attempts have been made to mitigate quadricep weakness after peripheral nerve block for knee arthroplasty.4–6 Various delivery methods for local anesthetics,4 supplemented with dexmedetomidine as adjuvant5 and adductor canal blocks (ACBs),6 have been explored, and ACBs are associated with less quadricep weakness. According to Yee et al,6 the prevalence of quadricep weakness after the administration of ACBs was 9%, and increased with dose. However, the optimal level and amount of local anesthetic for ACBs has not been definitively decided.
Femoral nerve block is widely used in clinical practice because of its fixed location, effective analgesia, and minimal tourniquet hypertension. Ropivacaine is associated with a lower incidence or grade of motor block compared with bupivacaine at lower concentrations in epidural anesthesia.7,8 The degree of sensory and motor block induced by ropivacaine is believed to be dose- and age-dependent.9 In epidural labor analgesia, the minimum local analgesic concentration of ropivacaine is defined as the median effective local analgesic concentration (EC50), which represents the relative analgesic potency of epidural ropivacaine. This concentration is reportedly 0.089%.10 However, the corresponding concentration of ropivacaine in peripheral nerve block has not been determined.
The present study explored the minimum analgesic concentration of ropivacaine (EC50) that induces an effective sensory block without influencing motor function, (i.e., a differential nerve block).11 Furthermore, analgesia without motor dysfunction is of great significance for older patients, and the effect of age on the EC50 has not been studied previously. This study determined the EC50 of ropivacaine for differential femoral nerve block in knee arthroscopy in adults aged either less or older than 60 years, and we also hypothesized that the EC50 values may differ between younger adult and elderly patients.
Methods
Design and Patients
This study is an up-and-down sequential allocation trial, approved by the Ethics Committee of the Third Hospital of Hebei Medical University (2019-022-1). This trial was registered prior to patient enrollment in the Chinese Clinical Trial Registry (ChiCTR1900027211, Principal investigator: Qiujun Wang, Date of registration: 05/11/2019). All enrolled patients provided written informed consent. All procedures of this study were performed in accordance with the Declaration of Helsinki (October 2013) and clinical practice guidelines.
The patients eligible for this study were adults (aged ≥18 years) with an American Society of Anesthesiologists (ASA) physical status I–III and scheduled for knee arthroscopy at the Ambulatory Care Center of Third Hospital of Hebei Medical University. The types of knee arthroscopies included partial meniscectomy, meniscus formation and suture, removal of knee joint loose bodies, and knee arthroscopic debridement. All subtypes of arthroscopy surgery were similar in stimulation intensity and duration. Patients with any of the following were excluded from this study: infection at the puncture site; sepsis; bleeding diathesis; allergy to amide-type local anesthetics; diabetes mellitus; peripheral neuropathies; abnormal muscle weakness; or inability to communicate during the perioperative period.
The enrolled patients were apportioned to 2 groups based on age, with Group 1 comprising those aged 18 to 60 years, and Group 2 those older than 60 years.
Determination of the EC50 of Ropivacaine for Differential Nerve Block
The up-down sequential method12 was used to determine the EC50 of ropivacaine for differential femoral nerve block, as follows. A positive response (or, differential block) was defined as an effective sensory block while maintaining motor function at the timepoints of assessment (30 minutes after ropivacaine injection, and at emergence from general anesthesia). A negative response was defined as effective sensory block with motor block.
The start level of ropivacaine concentration administered to both groups was 0.5%, as determined from the study by Casati et al.13 This is also the concentration commonly used in clinical practice. The concentrations were administered in this trial in a geometric sequence, as follows. The ratio of the 2 adjacent concentrations was 1.1. The concentration administered to each participant was determined based on the nerve blocking response of the previous patient. If a patient had a positive response, the next patient received a higher concentration, while a lower concentration was administered to the next patient after a negative response. If the nerve block was unsuccessful (i.e., an ineffective sensory block), the patient received a supplementary saphenous nerve block with 0.375% ropivacaine 15 mL for rescue analgesia, and was excluded from the study. Accordingly, the next patient would receive the same concentration.
One investigator was responsible for recording and selecting the concentration of ropivacaine given to each patient. The nerve block administrator and the researcher responsible for the assessments were blinded to the information.
The sample size was determined based on previous studies14–16 using the up-and-down method. In each group, the study ended when the number of crossovers from negative to positive responses reached 7.
Anesthesia
Each patient was brought to the preparation room before anesthesia. Standard vital signs were continuously monitored: electrocardiogram, pulse oxygen saturation, respiratory rate, and non-invasive blood pressure. Oxygen was administered via a face mask. Intravenous access was established and sufentanil 0.1 μg/kg was injected for moderate analgesia. Immediately before femoral nerve blocking, the baseline sensation and motor function of the operative extremity were assessed. Patients were excluded from this study if the baseline assessment was abnormal.
All femoral nerve blocks were performed by an experienced anesthesiologist blinded to the concentration for each participant. Nerve blocking was guided by a liner ultrasound probe (L38T7C, TuoRen TRU80, China). The patients were placed supine, and the ultrasound probe was placed on the inguinal crease under aseptic conditions. The operator moved the probe until the femoral artery and nerve were identified. The needle (22 gauge, 50 mm) was advanced using an in-plane approach (from lateral to medial). When the tip of the needle was close to the nerve, 22 mL ropivacaine (LBVK, AstraZeneca AB, Sweden) was injected slowly (Figure 1).
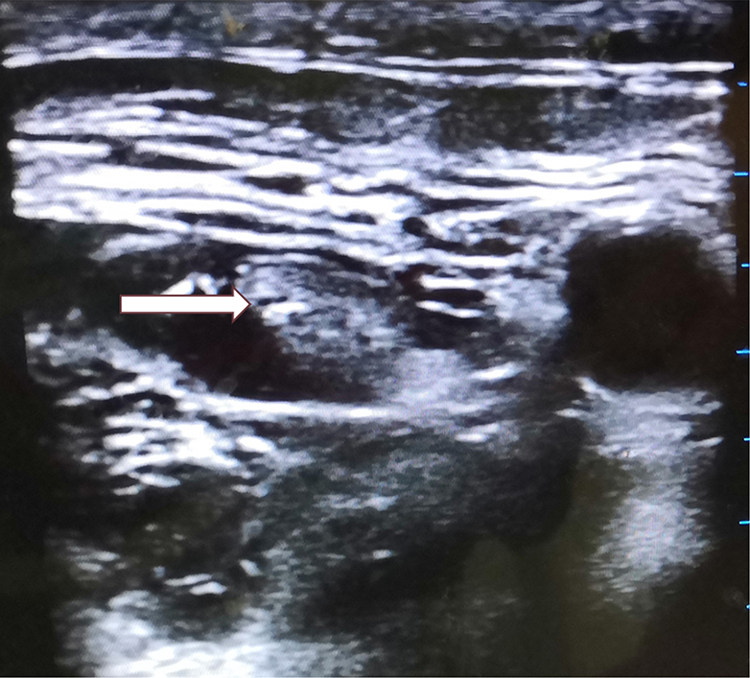 |
Figure 1 Femoral nerve blocking guided by ultrasound. Arrow indicates the femoral nerve, which is surrounded by injected ropivacaine. |
The volume 22 mL of ropivacaine was chosen based on Casati et al.13 These researchers reported a reduction in the amount of ropivacaine necessary for femoral nerve block with ultrasound guidance; in the ultrasound group, 22 mL of 0.5% ropivacaine was required to achieve the desired effect in 95% of the population (ED95).
The time of completion of ropivacaine injection was recorded for assessment. The observation period and assessment timepoints were 30 minutes after ropivacaine injection and immediately upon the patient waking from general anesthesia.
At 30 minutes after femoral nerve blocking, patients were transferred to the operating room. During the perioperative period the following monitoring data were collected for each patient: electrocardiogram, pulse oxygen saturation, respiratory rate, end-tidal carbon dioxide (ETCO2), bispectral index (BIS), and non-invasive blood pressure. General anesthesia was induced with 2 mg/kg propofol, 0.2 μg/kg sufentanil, 0.1 mg/kg midazolam, and 0.15 mg/kg cisatracurium. Airway management was established by applying a laryngeal mask airway. Propofol (3–8 mg/kg/h) and remifentanil (0.1–0.2 μg/kg/min) infusion were administered to maintain anesthesia, and the doses were titrated to the BIS values. During the operation, breathing parameters were adjusted to maintain ETCO2 between 35 to 45 mmHg, and the appropriate anesthesia depth was maintained (BIS values were maintained at 40–60). After surgery, the laryngeal mask was removed when the patient could open his eyes on command and maintain adequate spontaneous breathing. Afterward, 100% oxygen was administered via a face mask for 5 minutes. Patients were transferred to the post-anesthesia care unit after consciousness and adequate breathing were established. Atropine was administered for bradycardia. When systolic blood pressure was below 90 mmHg or less than 20% of the baseline, ephedrine was administered intravenously.
Postoperative Pain Management
Celecoxib 200 mg (oral, 2×/d) was prescribed while patients were in the day surgery unit. The non-steroidal anti-inflammatory drug ketorolac tromethamine, 30 mg, was prescribed intravenously for rescue analgesia when the visual analogue scale (VAS) score was higher than 4. If the rescue analgesia was not effective within 30 minutes, tramadol 0.1 g was administered by intravenous injection.
Measurements
The researcher responsible for assessing the nerve block effect was blinded to the ropivacaine concentration of each patient. Sensory and motor block were assessed every 2 minutes during the first 10 minutes after ropivacaine injection and subsequently every 5 minutes for the next 20 minutes.
Sensations changes were assessed by response to pinprick using a sharp piece of wood on the skin of the patella, anterior aspect of the thigh, and medial side of the calf, and graded as nil, 1, and 2 based on no sensation, sensation of touch only, and sensation of sharpness, respectively. Temperature sensation was also assessed with an alcohol wipe and was graded nil, 1, or 2 corresponding to no sensation, touch only, and cold sensation. Motor block was rated according to muscle strength of the quadriceps, reflected by the patients’ ability to extend the knees using a 6-point numerical rating scale,17 as follows: nil, no visible muscle contraction; 1, visible contraction without extension of the knee joint; 2, extension of the knee joint but not against gravity; 3, extension of the knee against gravity; 4, extension against gravity and moderate resistance; 5, normal, assessor unable to overcome the muscle power.
The patient was considered to have an effective sensory block only if the grades for the pinprick and temperature sensations were nil or 1. Motor function was considered unaffected only if the quadriceps muscle strength was grade 5 within 30 minutes after nerve blocking, and grade 4 or 5 upon emergence from general anesthesia. A positive response (differential block) was defined as effective sensory block while maintaining motor function. A negative response was defined as effective sensory blocking with motor blocking (quadriceps muscle strength <5 within 30 minutes or <4 upon emergence from general anesthesia).
The onset time and the scores of sensory block and motor block during the first 30 minutes after ropivacaine injection, and upon emergence from general anesthesia, were recorded. Postoperative pain was evaluated using the VAS score (a 10 cm horizontal line with the words “no pain” on the left and the “worst possible pain” on the right). The VAS scores were recorded immediately after surgery, and at 2, 6, and 24 hours after operation at rest and during movement (knee flexion).
The durations of sensory and motor blocks were recorded. The duration of sensory block was defined as the time interval between the onset of sensory blockade and when the temperature sensation score for the femoral nerve distribution area returned to grade 2 (feeling a cold sensation from an alcohol wipe). The duration of motor block was defined as the time interval between the onset of motor blockade and when the quadriceps muscle strength score returned to grade 5. Intraoperative events like bradycardia and hypotension were recorded. Complications related to the nerve block and adverse events such as falling were recorded.
The primary endpoint was the EC50 of 22 mL ropivacaine for differential femoral nerve block in each of the 2 age groups. The secondary endpoints were the sensory block, analgesic effects of the nerve block, complications, and adverse events.
Statistical Analysis
Patient demographic data are shown as the mean (standard deviation) or median (inter-quartile range), as appropriate, and compared using the independent sample t-test or Mann–Whitney U-test. Counts, incidence rates, or proportions were analyzed with the chi-squared test or Fisher’s exact test. The EC50 and 95% confidence intervals (CIs) were estimated by probit regression analysis. Comparison of the EC50 of the 2 age groups was performed with the Z test. All statistical analyses were performed using SPSS-21 software. P < 0.05 was considered statistically significant.

Symbols description:  , mean; S, standard deviation; n, number of patients in each group.
, mean; S, standard deviation; n, number of patients in each group.
The sample size was determined based on previous studies14–16 (7 crossovers from negative to positive responses). Additional analyses were performed with PASS 2021 software to confirm the statistical power of the sample size. We hypothesized that the EC50 of ropivacaine for differential nerve block in the adult (Group 1) and elderly (Group 2) patients would be 0.12% and 0.09%, respectively. The standard deviation was 0.017%. Thus, to achieve a power of 90% and a type I error of 0.05 with a possible dropout rate of 20%, 10 patients per group were required. According to Paul et al,16 2-to-3 patients are required for one crossover, so that the actual sample size in the present study would be 14-to-21 patients per group. The actual power would be higher than 90%.
Results
Participants and Complications
A total of 95 patients were initially enrolled in this study. Of these, one patient was excluded due to unsuccessful sensory blocking, and one patient refused to participate. Additionally, 13 patients (6 in Group 1, and 7 in Group 2) were excluded because of loss to follow-up. Thus, 80 patients completed this study (Figure 2). Among them, 39 and 41 were in Group 1 (adult) and Group 2 (elderly), respectively; there were 13 (33.3%) and 17 (41.5%) patients before the first negative-positive crossover. Therefore, data for 26 (66.67%) and 24 (58.5%) patients were included in the EC50 decisive sequential arrays of Group 1 and 2.
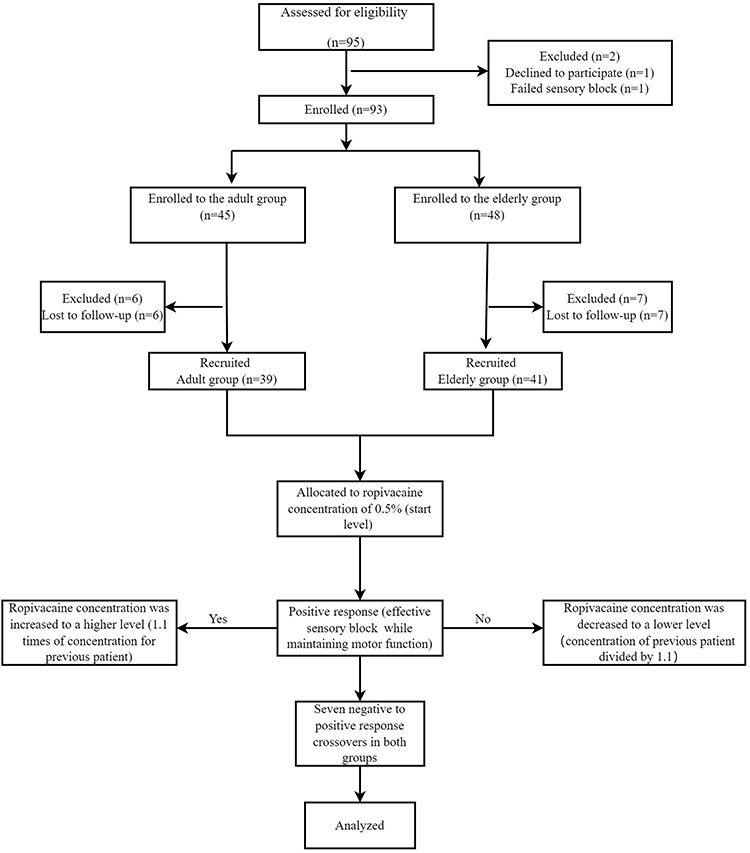 |
Figure 2 Flow diagram for the up-and-down method. |
The time to onset of motor block was more than 30 minutes for one patient in Group 1. None of the 95 patients had complications such as local anesthetic toxicity, hematoma at the puncture site, or neurological injury and none suffered adverse events such as falling.
Group Characteristics and Demographic Data
The mean ages of Group 1 and Group 2 were 37.90 and 65.46 years, respectively (Table 1). The 2 groups were statistically comparable with respect to gender ratio, body mass index, operation subtype rates, and duration of surgery. There were significantly more patients classified as ASA physical status II in Group 2 compared with Group 1 (P < 0.001).
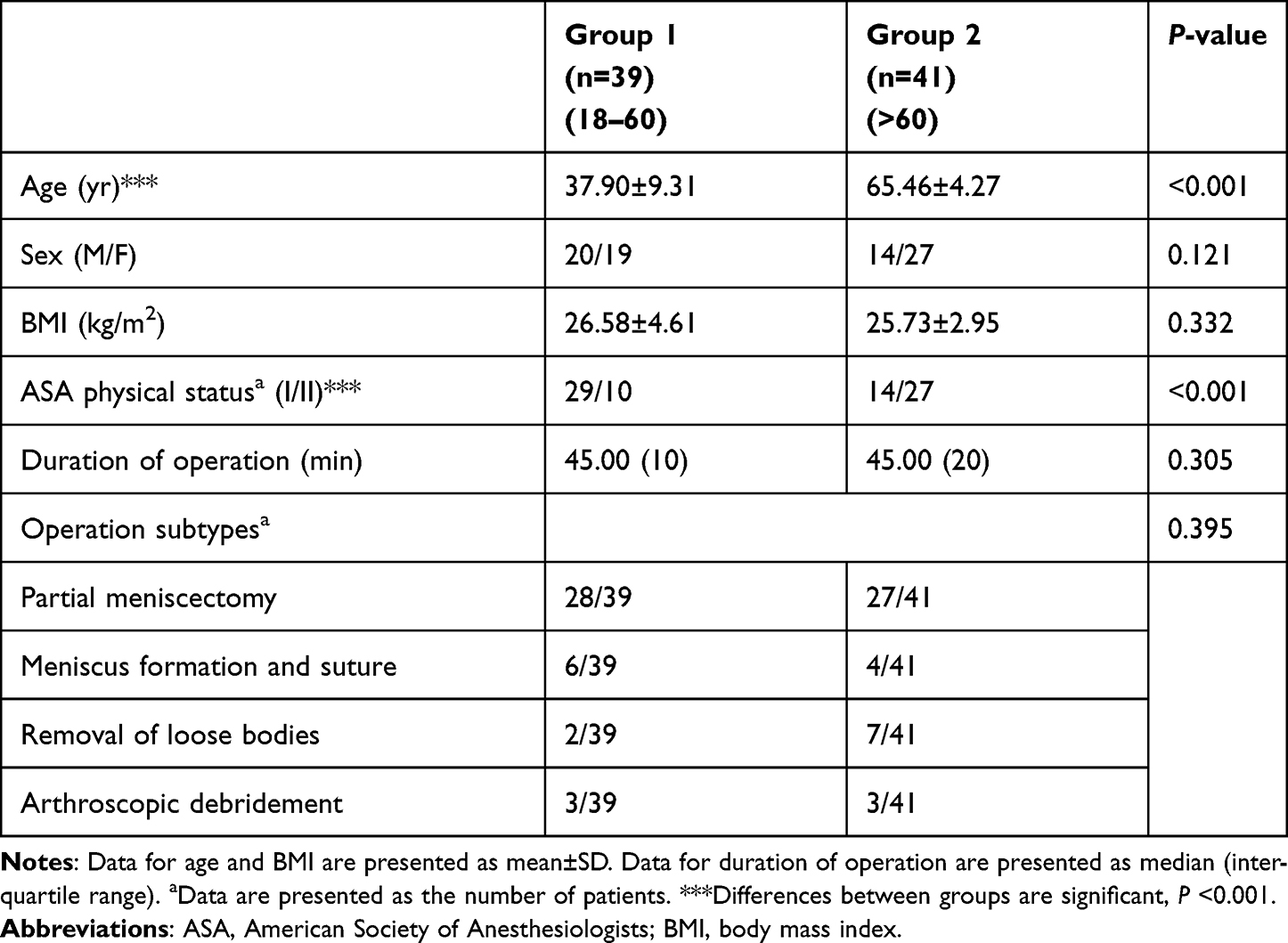 |
Table 1 Group Characteristics and Demographic Data |
EC50 of Ropivacaine in the 2 Age Groups
The primary endpoint of this study was the EC50 of ropivacaine for differential femoral nerve block in each of the 2 age groups. The sequential block responses from the first negative to positive crossover of the 2 groups are shown in Figure 3. It contained 7 crossover responses. Using probit regression analysis, the EC50 of 22 mL ropivacaine for differential femoral block in Group 1 and Group 2 was, respectively, 0.124% (95% CI, 0.097–0.143%) and 0.088% (95% CI, 0.076–0.103%). The comparison of the EC50 in the 2 age groups was performed with the Z test (P < 0.05).
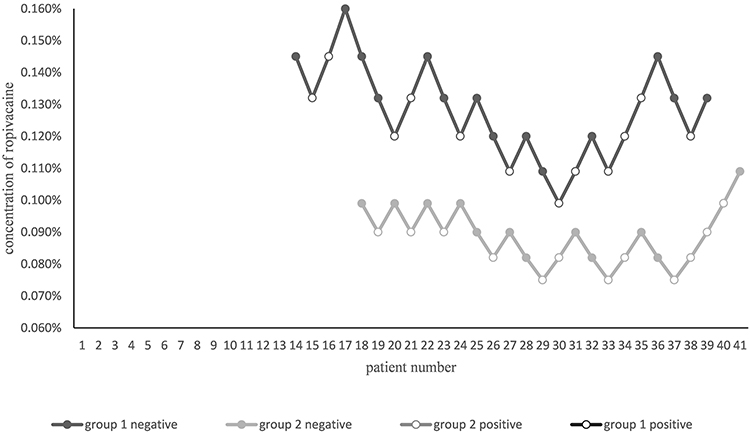 |
Figure 3 Femoral nerve block responses to predetermined ropivacaine concentrations using the Dixon’s up-and-down method in consecutive Group 1 (in black) and Group 2 (in grey) patients. Only patients from the first negative to positive response crossover in the 2 respective age groups were included. These sequential arrays included seven crossovers from negative to positive responses in 2 groups (Group 1, aged 18–60 years; Group 2, >60 years). Solid circle, negative response concentration; open circle, positive response concentration. |
Sensory Block Data
Table 2 presents the sensory block and analgesic data for the 2 age groups. None of the patients in the 2 groups complained of pain during rest or movement (knee flexion) immediately or 2 hours after surgery. Two patients in Group 2 complained of dynamic pain 6 hours after surgery (VAS score: 5). Two patients in Group 2 complained of popliteal pain 24 hours postoperatively. VAS scores at rest and during movement 24 hours after surgery are presented in Table 2. The 2 groups were comparable regarding the following: time to onset of sensory blockade; VAS score; percentage of patients with moderate or severe pain at postoperative 24 hours who required rescue analgesia (ketorolac tromethamine 30 mg alone or with tramadol 0.1 g); and duration of sensory block.
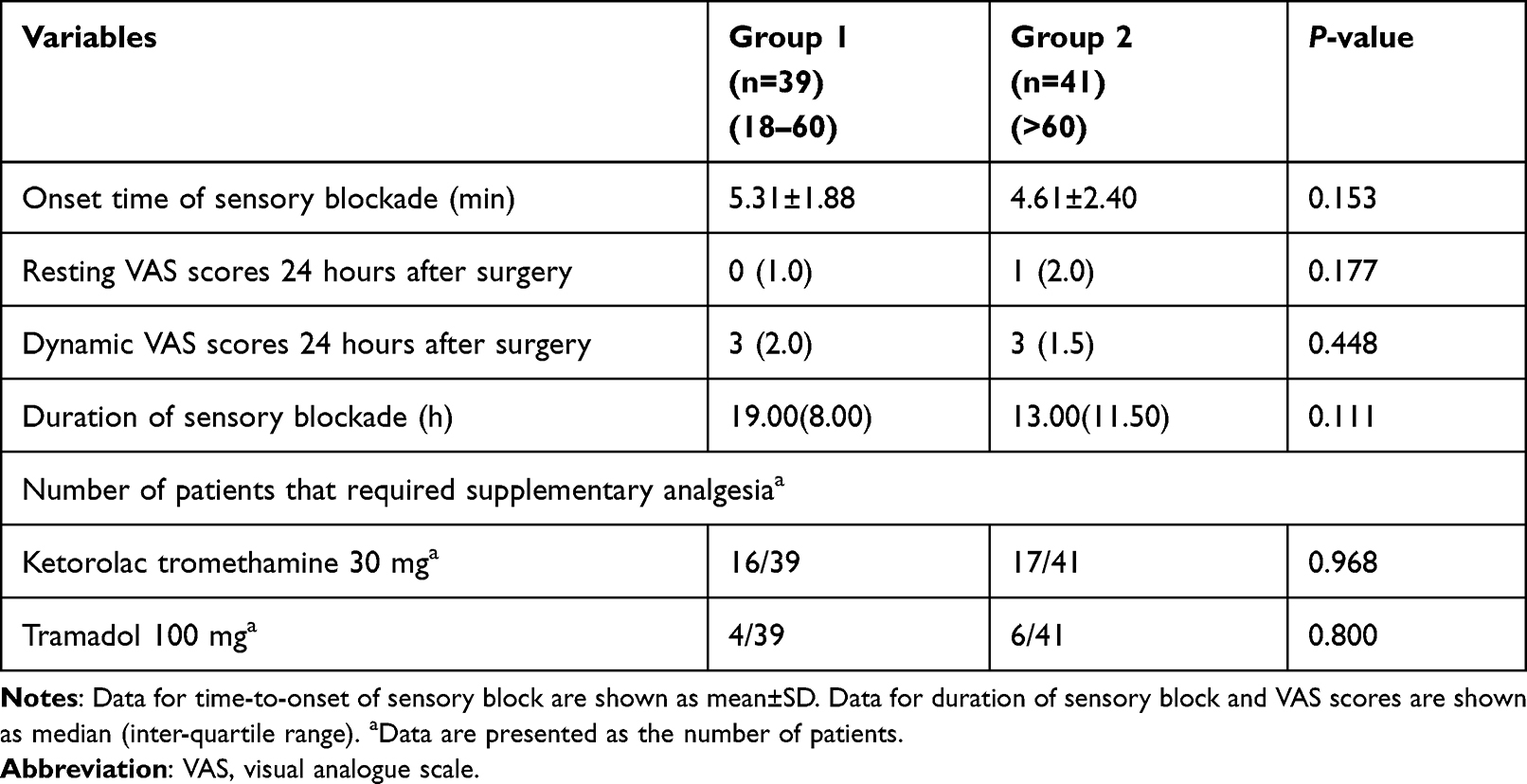 |
Table 2 Sensory Blockade Data |
Postoperative Analgesic Data for Differential Nerve Block
In the overall population, 24 participants experienced differential femoral nerve block; 12 in each group. None of these patients complained of pain immediately, or 2 or 6 hours after surgery. The VAS scores at rest and during knee flexion 24 hours after surgery and the number of patients who required rescue analgesia are presented in Table 3. Two patients in Group 1 and 6 in Group 2 required rescue analgesia (ketorolac tromethamine 30 mg). One patient in Group 1, and 3 in Group 2, required further tramadol 0.1 g. The 2 groups were comparable regarding the analgesic data.
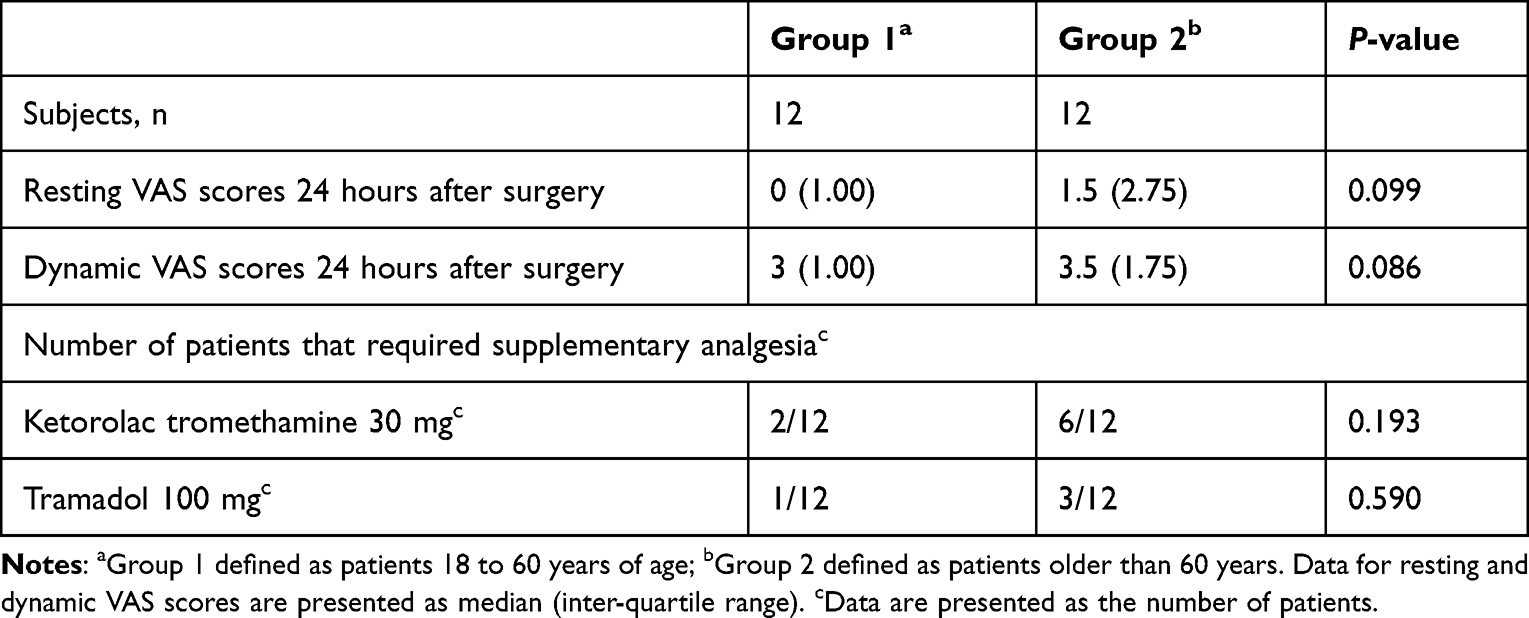 |
Table 3 Postoperative Analgesic Data in Differential Nerve Block |
Hemodynamic Data
Hemodynamic data were collected for the 2 groups perioperatively. In Group 1, one patient developed hypotension during surgery, and none experienced bradycardia. In Group 2, 4 patients experienced hypotension and 4 patients developed bradycardia. The incidence rates of bradycardia and hypotension during surgery did not differ significantly between the 2 age groups.
Discussion
The results of this study indicate that differential femoral nerve block in knee arthroscopy is feasible, both for adults between the ages of 18 and 60 years (Group 1), and those older than 60 years (Group 2). A relatively low concentration of ropivacaine resulted in effective sensory block while maintaining motor function. The EC50 of ropivacaine for differential femoral nerve block in Group 1 and Group 2 was 0.124% (95% CI, 0.097–0.143%) and 0.088% (95% CI, 0.076–0.103%), respectively. None of the patients suffered neurological complications or adverse events. Thus, the selective blocking characteristics of local anesthetics is worth exploring. In addition, one of the two main research directions to improve the action of local anesthetics is the development of compounds or methods that elicit nociception-selective blockade.18
The EC50 of ropivacaine observed in the present study was relatively lower than reported previously. For example, Paauwe et al19 compared 3 concentrations of ropivacaine (0.025, 0.05, and 0.1%) for postoperative analgesia after total knee arthroplasty and found that concentrations lower than 0.1% provided no advantage. Brodner et al20 concluded that 0.1% ropivacaine provided ineffective analgesia, while 0.2% and 0.3% were equally effective.
The different conclusions regarding femoral nerve blocking may be explained by differences in surgeries: Knee arthroplasty was performed in the 2 studies above, whereas knee arthroscopy was performed in the current study. It may be that pain intensity is higher after arthroplasty. Furthermore, in the previous 2 studies, ropivacaine was injected through a femoral catheter, whereas presently ropivacaine was administered with a single injection. The different infusion rates and volumes may affect the degree of analgesia. Finally, the previous study populations were not stratified by age, and this may contribute to the different conclusions.
Peripheral nerve blocks are beneficial for elderly patients, as analgesia is better and opioid consumption is reduced. However, protocols for specific local anesthetics in the aged need to be determined.21 Previous studies have suggested that there are indeed age differences for local anesthetics among several analgesic techniques. Chen et al22 found that the ED50 of intrathecally administered bupivacaine for motor block decreased steeply with advancing age, and Li et al23 reported that the motor block EC50 of ropivacaine for epidural anesthesia also decreased significantly.
Several explanations have been proposed to account for the effect of age. Decreased expression of myelin proteins and age-related decline in nerve regeneration may lead to a deterioration of myelin sheaths.24 Age-dependent decrease in axon diameter and the disruption of myelin sheaths25 may be why peripheral nerves in older individuals are more sensitive to local anesthetics. In another study, the duration of sciatic nerve block was longer in the older patients (55–80 y) compared with the younger (18–35 y).26 In the present study, the EC50 of ropivacaine for differential femoral nerve block in the elderly group was 0.088%, which was approximately 30% lower than that of Group 1, although the onset time of sensory block and VAS scores of the 2 groups did not differ significantly. A new randomized controlled trial is needed to compare differences in sensory block parameters.
The analgesic effect has always been a topic of concern. Kii et al27 investigated the maximum effective concentration of ropivacaine for differential block in hand or forearm soft-tissue surgery. They concluded that a high concentration of ropivacaine could cause sufficient analgesia with a loss of motor function, whereas a low concentration could result in insufficient sensory block despite the maintenance of motor function. This is consistent with our concern about the postoperative analgesia of differential femoral nerve block, especially with low concentrations. The analgesic data of 24 patients who experienced differential nerve block were compared. The shortest sensory block duration was 7 hours, experienced by one patient in each group. For this population, the median VAS scores at rest 24 hours postoperatively were 0 to 1.5, while the median dynamic VAS scores were 3 to 3.5.
The pain after arthroscopy is more intense during movement, especially knee flexion. Two patients in Group 1, and 6 patients in Group 2, required rescue analgesia due to moderate-to-severe pain. The relatively lower concentration used in Group 2 may explain the difference. Nonetheless, the data did not differ significantly between the 2 groups. Two patients in Group 2 complained of popliteal pain, which may be resolved by sciatic nerve block, but not by increasing the concentration used for the femoral nerve block. This may be due to different operative sites in the joint cavity, which is innervated by the sciatic nerve. Further studies are needed to determine the optimal multimodal analgesia protocol that maximizes analgesia (especially analgesia during knee flexion) while minimizing motor block.
This study has several limitations. The 2 groups comprised patients aged 18- to 60-years, and those older than 60 years. However, the response of patients at 20 years of age may differ from those aged 50 years. The ages within each group were not evenly distributed. In future studies, patients should be analyzed in groups aged more-or-less by decade, to reduce selection bias. Presumably, such groupings would help illuminate the underlying principles governing how age influences the necessary concentration. A second consideration is that for high efficiency in the present study only femoral nerve block was administered, but both femoral and sciatic nerve blocks are necessary for comprehensive analgesia during knee arthroscopy. Finally, the start level of ropivacaine concentration was relatively distant from the actual threshold. Although this did not influence the EC50 determination, more patients were required before the first negative-to positive-crossover responses.
Conclusion
This study found that the EC50 of ropivacaine for differential femoral nerve block was significantly lower in patients older than 60 years, compared with adults aged 18 to 60 years. These data may be useful for avoiding excessive local anesthetics in different age groups. Animal studies are needed to explore the underlying mechanisms of differences due to age.
Trial Registration
This study was part of the research registered in the Chinese Clinical Trial Registry (ChiCTR1900027211, research name: Correlational research between local anesthetics and nerve block; date of registration: 05/11/2019).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This sequential allocation study was approved by the Ethics Committee of the Third Hospital of Hebei Medical University (2019-022-1). Written informed consent was obtained from all patients before participation in this study. All procedures of this study were conducted in accordance with the Declaration of Helsinki (October 2013) and clinical practice guidelines.
Consent for Publication
All probands gave written consent for anonymized publication of data as required by the Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, in one or more of the following: conception, study design, execution, acquisition of data, analysis, interpretation, drafting, revising, and critical review of the article. All the authors approved the final version for publication in the current journal and are accountable for all aspects of the work.
Funding
This work is supported by the National Natural Science Foundation of China (81771134), Hebei Province Technology Innovation Guide Project Science and Technology Winter Olympics Special Project (19977790D), and the Professional Capacity Building and Specialist Training Program Funded by Hebei Provincial Government. The funding bodies had no role in the design of the study, the collection, analysis, or interpretation of the data, or writing the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
2. Ardon AE, Prasad A, McClain RL, Melton MS, Nielsen KC, Greengrass R. Regional anesthesia for ambulatory anesthesiologists. Anesthesiol Clin. 2019;37(2):265–287. doi:10.1016/j.anclin.2019.01.005
3. Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and Hip arthroplasty. Anesth Analg. 2010;111(6):1552–1554. doi:10.1213/ANE.0b013e3181fb9507
4. Charous MT, Madison SJ, Suresh PJ, et al. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. 2011;115(4):774–781. doi:10.1097/ALN.0b013e3182124dc6
5. Yang X, Kang W, Xiong W, et al. The effect of dexmedetomidine as adjuvant to ropivacaine 0.1% for femoral nerve block on strength of quadriceps muscle in patients undergoing total knee arthroplasty: a double-blinded randomized controlled trial. J Pain Res. 2019;12:3355–3363. doi:10.2147/JPR.S217283
6. Yee EJ, Gapinski ZA, Ziemba-Davis M, Nielson M, Meneghini RM. Quadriceps weakness after single-shot adductor canal block: a multivariate analysis of 1083 primary total knee arthroplasties. J Bone Joint Surg Am. 2021;103(1):30–36. doi:10.2106/JBJS.19.01425
7. Oda A, Ohashi H, Komori S, Iida H, Dohi S. Characteristics of ropivacaine block of Na+ channels in rat dorsal root ganglion neurons. Anesth Analg. 2000;91(5):1213–1220. doi:10.1097/00000539-200011000-00031
8. Wang RD, Dangler LA, Greengrass RA. Update on ropivacaine. Expert Opin Pharmacother. 2001;2(12):2051–2063. doi:10.1517/14656566.2.12.2051
9. Simpson D, Curran MP, Oldfield V, Keating GM. Ropivacaine: a review of its use in regional anaesthesia and acute pain management. Drugs. 2005;65(18):2675–2717. doi:10.2165/00003495-200565180-00013
10. Polley LS, Columb MO, Naughton NN, Wagner DS, van de Ven CJ, Goralski KH. Relative analgesic potencies of levobupivacaine and ropivacaine for epidural analgesia in labor. Anesthesiology. 2003;99(6):1354–1358. doi:10.1097/00000542-200312000-00017
11. Gerner P, Luo SH, Zhuang ZY, et al. Differential block of N-propyl derivatives of amitriptyline and doxepin for sciatic nerve block in rats. Reg Anesth Pain Med. 2005;30(4):344–350. doi:10.1016/j.rapm.2005.04.008
12. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991;15(1):47–50. doi:10.1016/S0149-7634(05)80090-9
13. Casati A, Baciarello M, Di Cianni S, et al. Effects of ultrasound guidance on the minimum effective anaesthetic volume required to block the femoral nerve. Br J Anaesth. 2007;98(6):823–827. doi:10.1093/bja/aem100
14. Yang C, Kang F, Meng W, et al. Minimum alveolar concentration-awake of sevoflurane is decreased in patients with Parkinson’s disease: an up-and-down sequential allocation trial. Clin Interv Aging. 2021;16:129–137. doi:10.2147/CIA.S291656
15. Wu Y, Jin S, Zhang L, et al. Minimum alveolar concentration-awake of sevoflurane is decreased in patients with end-stage renal disease. Anesth Analg. 2019;128(1):77–82. doi:10.1213/ANE.0000000000003676
16. Paul M, Fisher DM. Are estimates of MAC reliable? Anesthesiology. 2001;95(6):1362–1370. doi:10.1097/00000542-200112000-00014
17. Kleyweg RP, van der Meché FG, Schmitz PI. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barré syndrome. Muscle Nerve. 1991;14(11):1103–1109. doi:10.1002/mus.880141111
18. Lirk P, Hollmann MW, Strichartz G. The science of local anesthesia: basic research, clinical application, and future directions. Anesth Analg. 2018;126(4):1381–1392. doi:10.1213/ANE.0000000000002665
19. Paauwe JJ, Thomassen BJ, Weterings J, van Rossum E, Ausems ME. Femoral nerve block using ropivacaine 0.025%, 0.05% and 0.1%: effects on the rehabilitation programme following total knee arthroplasty: a pilot study. Anaesthesia. 2008;63(9):948–953. doi:10.1111/j.1365-2044.2008.05538.x
20. Brodner G, Buerkle H, Van Aken H, et al. Postoperative analgesia after knee surgery: a comparison of three different concentrations of ropivacaine for continuous femoral nerve blockade. Anesth Analg. 2007;105(1):256–262. doi:10.1213/01.ane.0000265552.43299.2b
21. Corcoran E, Kinirons B. Regional anaesthesia in the elderly patient a current perspective. Curr Opin Anaesthesiol. 2021;34(1):48–53. doi:10.1097/ACO.0000000000000940
22. Chen M, Chen C, Ke Q. The effect of age on the median effective dose (ED50) of intrathecally administered plain bupivacaine for motor block. Anesth Analg. 2014;118(4):863–868. doi:10.1213/ANE.0000000000000147
23. Li Y, Zhu S, Bao F, Xu J, Yan X, Jin X. The effects of age on the median effective concentration of ropivacaine for motor blockade after epidural anesthesia with ropivacaine. Anesth Analg. 2006;102(6):1847–1850. doi:10.1213/01.ane.0000215999.60513.da
24. Verdú E, Ceballos D, Vilches JJ, Navarro X. Influence of aging on peripheral nerve function and regeneration. J Peripher Nerv Syst. 2000;5(4):191–208. doi:10.1111/j.1529-8027.2000.00026.x
25. Chase MH, Engelhardt JK, Adinolfi AM, Chirwa SS. Age-dependent changes in cat masseter nerve: an electrophysiological and morphological study. Brain Res. 1992;586(2):279–288. doi:10.1016/0006-8993(92)91637-T
26. Hanks RK, Pietrobon R, Nielsen KC, et al. The effect of age on sciatic nerve block duration. Anesth Analg. 2006;102(2):588–592. doi:10.1213/01.ane.0000189552.85175.db
27. Kii N, Yamauchi M, Takahashi K, Yamakage M, Wada T. Differential axillary nerve block for hand or forearm soft-tissue surgery. J Anesth. 2014;28(4):549–553. doi:10.1007/s00540-013-1773-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.