")
Back to Journals » Patient Related Outcome Measures » Volume 9
Measuring and monitoring health-related quality of life responsiveness in systemic lupus erythematosus patients: current perspectives
Authors Mikdashi J
Received 15 November 2017
Accepted for publication 23 August 2018
Published 4 October 2018 Volume 2018:9 Pages 339—343
DOI https://doi.org/10.2147/PROM.S109479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Liana Bruce
Jamal Mikdashi
Division of Rheumatology and Clinical Immunology, University of Maryland School of Medicine, Baltimore, MD 21201, USA
Objective: Little is known about health-related quality of life (HRQoL) responsiveness in systemic lupus erythematosus (SLE) patients, compared to other chronic diseases. This review summarizes the available data in HRQoL responsiveness and sensitivity to change in SLE, and recommends directions for research and clinical application.
Methods: A review of the literature was conducted reporting on HRQoL responsiveness in adult SLE patients between 1984 and 2018. HRQoL studies were assessed for responsiveness, sensitivity of change, minimal important differences, minimal clinical important differences, or change in improvement or deterioration.
Results: Responsiveness or sensitivity to change in health-related status was observed in Medical Outcome Survey Short Form-36, SLE Symptom Checklist, EuroQoL, and Medical Outcomes Study Short Form 6D. SLE-specific quality of life questionnaire demonstrated greater responsiveness than the individual domains of SF-36. Lupus quality of life showed large responsiveness when there was improvement. LupusPRO and its derivative Lupus Impact Tracker were found to be responsive to change in disease activity, reflecting both improvement and worsening. Lupus Impact Tracker and physical health and pain domains of Lupus quality of life were responsive to SLE composite responder index.
Conclusion: This review highlights the need for further studies that capture responsiveness and change in HRQoL that are clinically meaningful and sustained. Most importantly, the choice of one measure over another is influenced by the purpose of the HRQoL measure, the particular HRQoL domain, and the SLE disease state that are relevant to the research question.
Keywords: quality of life, systemic lupus, measurements, monitoring
Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystemic autoimmune disease associated with significant humanitarian burden and lower health-related quality of life (HRQoL).1–5 To date there have been a number of reviews conducted to assess measures of HRQoL in SLE, mostly focusing on the developmental process and the psychometric properties.6–8 Measuring responsiveness of generic and SLE-specific HRQoL questionnaires and the ability to capture a change in SLE-related health status remain underreported.
The aim of this review is to appraise studies that estimate the responsiveness to change in HRQoL status according to adult SLE patients’ concerns and determine the magnitude of change in the domain scores of these tools.
Methods
Search strategy: review of the literature
A review of English language publications limited to adult (age ≥18 years) SLE patients was performed from 1984 till January 2018. Search terms used were “quality of life and lupus”, “responsiveness”, “sensitivity of change”, minimally important difference (MID), or minimal clinical important difference (MCID). Inclusion criteria were manuscripts that reported HRQoL responsiveness or change of improvement or worsening. Exclusion criteria were abstracts, reviews, manuscripts that reported HRQoL in children or adolescents, or articles contained insufficient information on responsiveness or magnitude of change.
Results
The impact of change of generic and SLE-specific HRQoL measures used in SLE is described and depicted in Table 1.
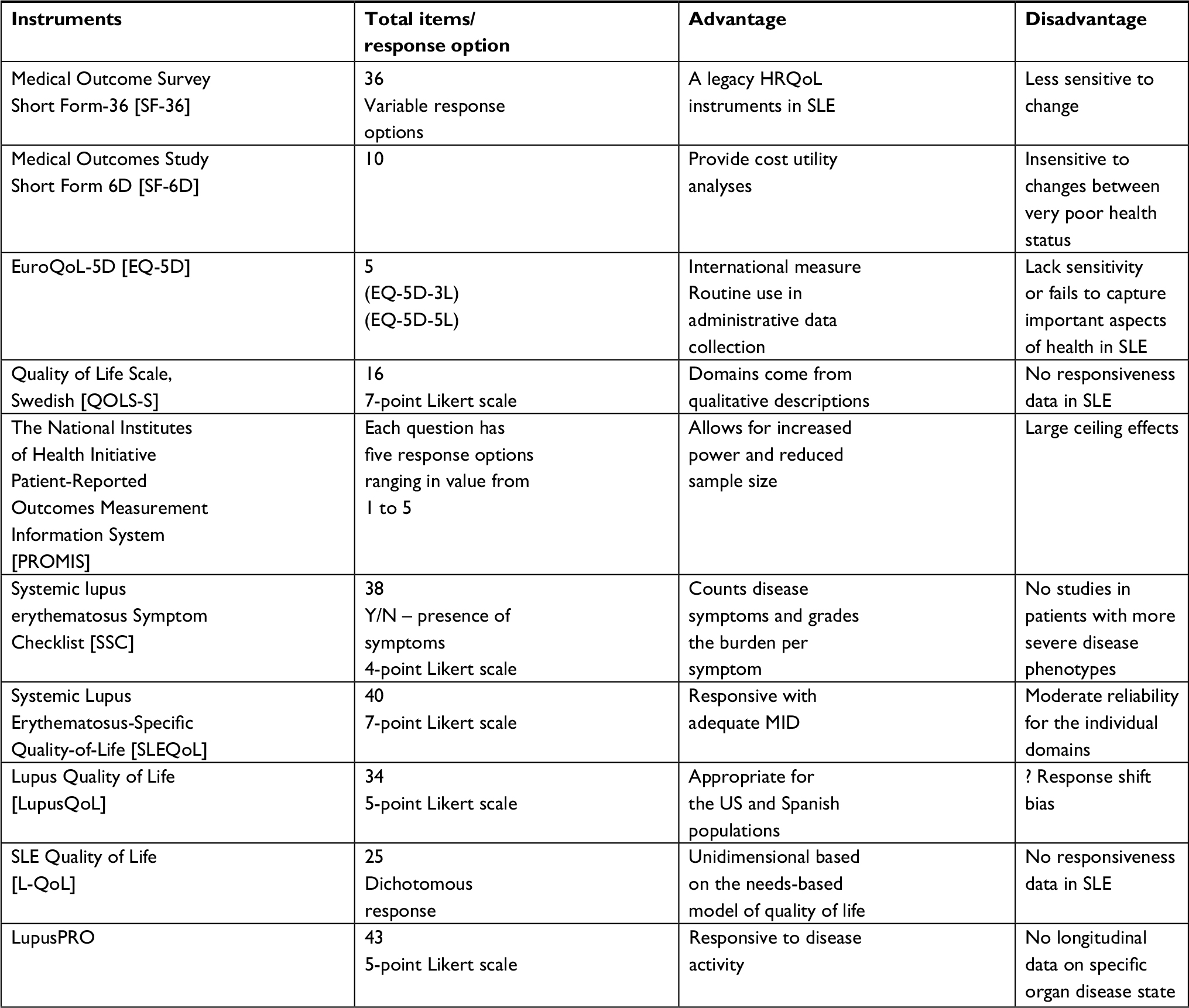 | Table 1 HRQoL measures used in SLE Abbreviations: HRQoL, health related quality of life; MID, minimally important difference; SLE, systemic lupus erythematosus. |
Generic HRQoL measures used in SLE
Medical Outcome Survey Short Form-36 (MOS SF-36)
The SF-36 has been widely used successfully to assess HRQoL in SLE patients in many regions of the world. Therapeutic interventions in clinical trials had shown improvement in HRQoL using SF-36 allied with reduction in SLE disease activity including, prasterone,9 mycophenolate mofetil,10 abetimus sodium,11 epratuzumab,12 and belimumab.13
Mild to moderate responsiveness of SF-36 is reported in SLE patients. Mean changes from baseline in the eight SF-36 domain scores, physical component summary (PCS) and mental component summary (MCS) scores, were generally in agreement with improved, unchanged, and worsened patient global assessment scores. Patients with improved or unchanged British Isles Lupus Activity Group score (BILAG) General and Musculoskeletal status compared to baseline experienced a statistically significant improvement in most SF-36 PCS scores with effect sizes (ES) in the range of 0.3–0.7. Scores remained stable for patients with worsened BILAG ratings compared to baseline with ES generally <0.3.14
Using a patient-reported overall health status anchor, MID for SF-36 was reported at 2.1 (better) and –2.2 (worse) for the PCS and 2.4 (better) and –1.2 (worse) for the MCS.15
The sensitivity to change of SF-36 was also compared to other SLE-specific HRQoL measures reflecting improvement and worsening overtime in patients with low and active disease state.16–19 Using the anchor-based approach, the mean MID ranged from –2.0 for general health to –11.1 for role physical, and for improvement, the mean MID ranged from 2.8 for general health to 10.9 for bodily pain and vitality. Summary scores ranged from +2.5 to –0.8, and +5.0 to –2.5 for domain scores for improvement and deterioration, respectively.18
Medical Outcomes Study Short Form 6D (SF-6D)
Evidence for the ability of SF-6D to detect change is mixed. SF-6D was found to be sensitive to self-reported improvement in health with small to medium ES, but insensitive to decline in health with a small to absent effects.20
EuroQoL-5D (EQ-5D)
Similar to SF-6D, and SF-36, the sensitivity of the EQ-5D to improvement or decline in SLE disease activity index (SLEDAI) scores longitudinally was poor, with small to absent ES.20 The EQ-5D measured significant improvement in HRQoL for patients self-reporting somewhat or much better health (mean EQ-5D change from 0.70 to 0.77) with small to medium ES. EQ-5D was insensitive to self-reported decline in health, showing small to absent effects. EQ-5D showed a trend towards improvement, with increased EQ-5D Visual Analog Scale (VAS) score during two visits, but not with decline.
Quality of Life Scale, Swedish version (QOLS-S)
No data on responsiveness is reported.
The National Institutes of Health Initiative Patient-Reported Outcomes Measurement Information System (PROMIS)
Limited responsiveness related to large ceiling effects is recognized, though patterns of worsening PROMIS-29 scores with increasing disease severity or declining health status were observed.21 The 14 PROMIS Computer Adaptive Tests domains scores showed a weak and statically insignificant correlation with SELENA-SLEDAI and SLE damage index.22
Disease-specific measures of HRQoL in SLE
Lupus Quality of Life (LupusQoL)
Responsiveness was assessed based on patient-reported global rating of change and physician-reported disease activity change scores in a longitudinal SLE study.18 For disease activity, some LupusQoL domains showed responsiveness when there was improvement but none for deterioration. For deterioration, the mean LupusQoL change scores ranged from –2.5 for the body image domain to –7.7 for the intimate relationships domain. For improvement, the mean LupusQoL change scores ranged from 5.6 in the physical health domain to 10.4 in the burden to others domain. Using the anchor-based approach, the mean MID for LupusQoL ranged from –2.4 for body image to –8.7 for intimate relationship for deterioration, and 3.5 for body image to 7.3 for burden to others for improvement.
LupusQoL and SF-36 were measured using anchors for responsiveness defined by patients’ global assessment of disease impact according to changes in VAS.16 Absence of symmetry in the responsiveness between worsening and improving patients was observed. Responsiveness varied among symptoms. The MID for global improvement ranged from 1.1 to 9.2 and from 1.9 to 11.3 for LupusQoL and SF-36 domain scores, respectively (excluding LupusQoL aggregated domains and SF-36 MCS/PCS). In worsening patients, the MID ranged from –0.5 to –6.4 in LupusQoL domains and from –4.4 to –15.6 in SF-36 domains.
LupusQoL and SF-36 were found to be responsive to SLE flares and improvement according to clinical anchors using SLEDAI-2K.17 Both SF-36 and LupusQoL were responsive in patients with low disease activity state. No clear distinction was made in terms of standardized response mean (SRM) between the SF-36 and LupusQoL, but LupusQoL values were slightly better.
Both SF-36 and LupusQoL were found to be sensitive to change in SLE patients with active disease state and using different definitions of MCID, reflecting both improvement and worsening.19 LupusQoL-specific domains (planning, burden to others, body image, and intimate relationship) were largely responsive to change.
Two domains of LupusQoL were found to be responsive to SLE Responder index (SRI). SRM and (ES) for physical health and pain domains were 0.42 (0.23) and 0.65 (0.44), respectively.23
Systemic Lupus Erythematosus-Specific Quality-of-Life Questionnaire (SLEQOL)
SLEQOL demonstrated greater responsiveness than the individual domains of SF-36 in SLE.24 MID was derived using a distributional approach in which SLEQOL scores were anchored to the patient global ratings of changes in their HRQoL. By taking the mean of the absolute difference of SLEQOL scores in the group of patients who rated their global HRQoL change as +2 to +3 (“moderately worse” or “a little worse”) and –2 to –3 (“moderately better” or “a little better”), the MID was calculated at 24.76. The Thai version of SLEQOL had moderate response to change in HRQoL with a SRM estimated at 0.50.25
SLE Quality of Life Questionnaire (L-QoL)
No data on responsiveness is reported.
Systemic Lupus Erythematosus Symptom Checklist (SSC)
Responsiveness was investigated in patients with proliferative lupus nephritis at the beginning of treatment with cyclophosphamide and 1 year after.26 Significant changes were observed in several symptoms related to the disease and total distress level. The Euro-Lupus group tended to show a higher HRQoL than the National Institute of Health group on 4 of 7 scales of the SF-36.
Systemic Lupus Erythematosus PRO (LupusPRO)
Most of LupusPRO domains were found to be responsive to changes against self-reported change in health status, physician global assessment, BILAG, SLEDAI, and Lupus Foundation-defined flare (SFI).23 Body Image in Lupus Screen was found to be responsive to change in body image. Lupus Impact Tracker (LIT) was found to be responsive to changes in SELENA-SLEDAI, SFI, and SRI.27 LIT mean scores decreased by more than 3 with improvement in physician global assessment (SRM –0.26), while it increased by more than 5 with worsening in SELENA-SLEDAI (SRM 0.42). Mean change in LIT of >±3 was noted with change in SFI status. Mean LIT score decreased by >4 and increased by >2 with patient-reported improvement and worsening in SLE health status respectively. LIT SRM (ES) among SRI responders and nonresponders were –0.69 (–0.36) and –0.20 (–0.12), respectively.
Conclusion
The SF-36, SF-6D, EQ-5D, LupusQoL, SLEQOL, and LupusPRO are the most used measures in SLE research. The larger ceiling effects observed in generic measures make them less sensitive to change in disease or treatment effect than SLE-specific questionnaires. Findings from this review support the use of both generic, such as PROMIS domains or SF-36, and specific SLE-related measures, such as LupusPRO, LupusQoL, SLEQOL, or LIT. Future research with well-defined samples of SLE subjects including, similar disease activity state (mild, severe, remission), specific organ involvement, therapeutic measures, and comorbid conditions, with appropriate statistical analyses and longitudinal design is needed.
Disclosure
The author reports no conflicts of interest in this work.
References
Urowitz M, Gladman DD, Ibañez D, et al. Changes in quality of life in the first 5 years of disease in a multicenter cohort of patients with systemic lupus erythematosus. Arthritis Care Res. 2014;66(9):1374–1379. | ||
Jolly M. How does quality of life of patients with systemic lupus erythematosus compare with that of other common chronic illnesses? J Rheumatol. 2005;32(9):1706–1708. | ||
Plantinga L, Lim SS, Bowling CB, Drenkard C. Association of age with health-related quality of life in a cohort of patients with systemic lupus erythematosus: the Georgians Organized Against Lupus study. Lupus Sci Med. 2016;3(1):e000161. | ||
Fortin PR, Abrahamowicz M, Neville C, et al. Impact of disease activity and cumulative damage on the health of lupus patients. Lupus. 1998;7(2):101–107. | ||
Thumboo J, Fong KY, Chan SP, et al. A prospective study of factors affecting quality of life in systemic lupus erythematosus. J Rheumatol. 2000;27(6):1414–1420. | ||
Mcelhone K, Abbott J, Teh LS. A review of health related quality of life in systemic lupus erythematosus. Lupus. 2006;15(10):633–643. | ||
Mahieu M, Yount S, Ramsey-Goldman R. Patient-Reported Outcomes in Systemic Lupus Erythematosus. Rheum Dis Clin North Am. 2016;42(2):253–263. | ||
Holloway L, Humphrey L, Heron L, et al. Patient-reported outcome measures for systemic lupus erythematosus clinical trials: a review of content validity, face validity and psychometric performance. Health Qual Life Outcomes. 2014;12:116. | ||
Nordmark G, Bengtsson C, Larsson A, et al. Effects of dehydroepiandrosterone supplement on health-related quality of life in glucocorticoid treated female patients with systemic lupus erythematosus. Autoimmunity. 2005;38(7):531–540. | ||
Tse KC, Tang CS, Lio WI, Lam MF, Chan TM. Quality of life comparison between corticosteroid- and-mycofenolate mofetil and corticosteroid- and-oral cyclophosphamide in the treatment of severe lupus nephritis. Lupus. 2006;15(6):371–379. | ||
Strand V, Crawford B. Improvement in health-related quality of life in patients with SLE following sustained reductions in anti-dsDNA antibodies. Expert Rev Pharmacoecon Outcomes Res. 2005;5(3):317–326. | ||
Strand V, Petri M, Kalunian K, et al. Epratuzumab for patients with moderate to severe flaring SLE: health-related quality of life outcomes and corticosteroid use in the randomized controlled ALLEVIATE trials and extension study SL0006. Rheumatology. 2014;53(3):502–511. | ||
Strand V, Levy RA, Cervera R, et al. Improvements in health-related quality of life with belimumab, a B-lymphocyte stimulator-specific inhibitor, in patients with autoantibody-positive systemic lupus erythematosus from the randomised controlled BLISS trials. Ann Rheum Dis. 2014;73:838–44. | ||
Stoll T, Gordon C, Seifert B, et al. Consistency and validity of patient administered assessment of quality of life by the MOS SF-36; its association with disease activity and damage in patients with systemic lupus erythematosus. J Rheumatol. 1997;24(8):1608–1614. | ||
Colangelo KJ, Pope JE, Peschken C. The minimally important difference for patient reported outcomes in systemic lupus erythematosus including the HAQ-DI, pain, fatigue, and SF-36. J Rheumatol. 2009;36(10):2231–2237. | ||
Devilliers H, Amoura Z, Besancenot JF, et al. Responsiveness of the 36-item Short Form Health Survey and the Lupus Quality of Life questionnaire in SLE. Rheumatology. 2015;54(5):940–949. | ||
Touma Z, Gladman DD, Ibañez D, Urowitz MB. Is there an advantage over SF-36 with a quality of life measure that is specific to systemic lupus erythematosus? J Rheumatol. 2011;38(9):1898–1905. | ||
Mcelhone K, Abbott J, Sutton C, et al. Sensitivity to Change and Minimal Important Differences of the LupusQoL in Patients With Systemic Lupus Erythematosus. Arthritis Care Res. 2016;68(10):1505–1513. | ||
Nantes SG, Strand V, Su J, Touma Z. Comparison of the Sensitivity to Change of the 36-Item Short Form Health Survey and the Lupus Quality of Life Measure Using Various Definitions of Minimum Clinically Important Differences in Patients With Active Systemic Lupus Erythematosus. Arthritis Care Res. 2018;70(1):125–133. | ||
Aggarwal R, Wilke CT, Pickard AS, et al. Psychometric properties of the EuroQol-5D and Short Form-6D in patients with systemic lupus erythematosus. J Rheumatol. 2009;36(6):1209–1216. | ||
Katz P, Pedro S, Michaud K. Performance of the PROMIS 29-Item Profile in Rheumatoid Arthritis, Osteoarthritis, Fibromyalgia, and Systemic Lupus Erythematosus. Arthritis care & research. 2017;69:1312–1321. | ||
Kasturi S, Szymonifka J, Burket JC, et al. Validity and Reliability of Patient Reported Outcomes Measurement Information System Computerized Adaptive Tests in Systemic Lupus Erythematosus. J Rheumatol. 2017;44(7):1024–1031. | ||
Devilliers H, Bonithon-Kopp C, Jolly M. The lupus impact tracker is responsive to changes in clinical activity measured by the systemic lupus erythematosus responder index. Lupus. 2017;26(4):396–402. | ||
Leong KP, Kong KO, Thong BY, et al. Development and preliminary validation of a systemic lupus erythematosus-specific quality-of-life instrument (SLEQOL) Rheumatology (Oxford). 2005;44:1267–1276. | ||
Kasitanon N, Wangkaew S, Puntana S, Sukitawut W, Leong KP, Louthrenoo WTan Tock Seng Hospital Lupus Study Group. The reliability, validity and responsiveness of the Thai version of Systemic Lupus Erythematosus Quality of Life (SLEQOL-TH) instrument. Lupus. 2013;22(3):289–296. | ||
Daleboudt GM, Berger SP, Broadbent E, Kaptein AA. Health-related quality of life in patients with systemic lupus erythematosus and proliferative lupus nephritis. Psychol Health Med. 2011;16(4):393–404. | ||
Giangreco D, Devilliers H, Annapureddy N, Block JA, Jolly M. Lupus Impact Tracker is responsive to physician and patient assessed changes in systemic lupus erythematosus. Lupus. 2015;24(14):1486–1491. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.