")
Back to Journals » International Journal of Women's Health » Volume 12
Maternal Delays for Institutional Delivery and Associated Factors Among Postnatal Mothers at Public Health Facilities of Gamo Zone, Southern Ethiopia
Authors Wanaka S, Hussen S , Alagaw A, Tolosie K, Boti N
Received 30 November 2019
Accepted for publication 20 February 2020
Published 4 March 2020 Volume 2020:12 Pages 127—138
DOI https://doi.org/10.2147/IJWH.S240608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Seifu Wanaka,1 Sultan Hussen,2 Amsalu Alagaw,2 Kabtamu Tolosie,3 Negussie Boti2
1Gamo Zone Health Department, Arba Minch, Ethiopia; 2Arba Minch University, College of Medicine & Health Sciences, Department of Public Health, Arba Minch, Ethiopia; 3Arba Minch University, College of Natural Sciences, Department of Statistics, Arba Minch, Ethiopia
Correspondence: Negussie Boti
Department of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Email [email protected]
Background: Maternal health delays like delay in deciding to seek care, reaching a health facility, and receiving appropriate care were identified as the main contributing factors for maternal mortality and morbidity in many developing countries including Ethiopia. However, little is known about the magnitude and factors predisposing for maternal health delays in Ethiopia especially in a rural part of the country. Therefore, the aim of this study is to assess the magnitude of maternal delays for institutional delivery and associated factors among mothers attending post-natal service at public health facilities of the Gamo zone, Southern Ethiopia.
Methods: A cross-sectional study was conducted in rural districts of Gamo zone. Eleven public health centers in the two districts were selected randomly. The Systematic random sampling method was used to select study participants from each public health centers. A total of 394 postnatal mothers were selected every secondly and interviewed in a separate room. Face to face interview methods were used to collect the data. Binary and multivariable logistic regression analyses were conducted to identify the associated factors for the three delays.
Results: The magnitude of first, second and third maternal delays were 46.80%, 44.00%, and 31.70%, respectively. Unemployed women [AOR: 2.20, 95% CI (1.15, 4.16)], birth preparedness [AOR: 2.70, 95% CI (1.29, 5.71)], husband’s decisions making [AOR: 6.00, 95% CI (2.87, 12.42)] were found to be significantly associated with first delay. Distance to health facility [AOR: 7.00, 95% CI (3.58, 13.71)], and means of transportation [AOR: 3.30, 95% CI (1.13, 9.54)] were found to be significantly associated with the second delay. Availability of obstetric drugs [AOR: 8.40, 95% CI (3.76, 18.76)], and availability of skilled health provider [AOR: 10.40, 95% CI (4.24, 25.69)] were found to be significantly associated with the third delay for institutional delivery.
Conclusion: The magnitude of first, second and third maternal delays were high which indicates that most mothers were not receiving institutional delivery services at the recommended time. Maternal socio-economic, obstetric factors and health-care system factors affected the three delays in this study. Therefore, improving women empowerment and resource availability at health facilities is vital.
Keywords: maternal delays, institutional delivery service utilization, Ethiopia
Background
Globally, an estimated 303,000 women died each year from complications of pregnancy and childbirth.1 Almost 99% of these maternal deaths occur in developing countries, while sub-Saharan Africa (SSA) accounting for nearly two-thirds of maternal deaths.1,2 Ethiopia is one of the SSA countries that markedly contribute a high toll of avoidable maternal deaths worldwide, 412 per 100,000 live births.3 However, by 2030 global target to reduce maternal mortality ratio to less than 70 per 100,000 live births, working towards a vision of ending all preventable maternal mortality.4
Three maternal delays are identified as the main contributing factors for maternal mortality and morbidity in many developing countries. Ethiopia, the causes of maternal morbidity and morbidity are similar to many developing.5,6 Maternal delays contributing not only for maternal and neonatal mortality but also maternal morbidities like vaginal/uterine prolapse or puerperal psychosis can cause unwanted physical, mental, social, and economic consequences for respective families.7
There are variations in the magnitude of the three maternal delays for utilizing institutional delivery from deciding to seek emergency care to start in receiving of first healthcare. In developing countries, a study showed that the magnitude of the women, who experienced the first, second and third maternal delays were 71%, 40%, and 79%, respectively.8 A study was done in the Northern part of Ethiopia also showed that the magnitude of mothers who experienced the first, second and third maternal delays in utilization of institutional delivery services were 37.8%, 31.7%, and 30.7%, respectively.9
Many efforts have been made to tack the problem of the unacceptably high maternal delays in Ethiopia through several initiatives to increase access to and enhance communities’ demand for greater service use. By aligning with health extension program activities like user-fee exemption for institutional delivery service, maternity waiting home service, by availing ambulance service to reach a health facility for childbirth and community mobilization endeavors since July 2005 have been conducted in Ethiopia.2–4
Despite these efforts to increase institution-based delivery service in the country, only 26% of births were attended by skilled birth attendants (SBA). Skilled birth attendants play an important role in reducing maternal and neonatal mortality because they provide timely obstetric and newborn care for life-threatening complications.10
According to available evidence, illiteracy, poor knowledge on danger signs at labor and childbirth, inadequate birth preparedness and its complication readiness, decision-making powers of women, distance, lack of transport, lack of skilled health provider, lack of obstetric drugs were factors that contribute to three maternal delays.11,12,13
Even if the number of studies conducted in the country were identified factors associated with maternal delays for institutional delivery service utilization in urban settings, there is still information gap as well as minimal evidence on maternal delays for institutional delivery service utilization and associated factors among postnatal mothers in rural part of Ethiopia. Therefore, this study aimed to determine the magnitude of the maternal delays for institutional delivery service utilization in rural parts of the Gamo zone, Southern Ethiopia.
Objectives
General Objective
To determine the magnitude of maternal delays for institutional delivery service utilization and associated factors among postnatal mothers who gave birth at public health facilities in selected rural Woredas in Gamo zone, Southern Ethiopia in 2019.
Specific Objectives
To determine the magnitude of maternal delays for institutional delivery service utilization among postnatal mothers who gave birth at public health facilities in selected rural Woredas in Gamo zone, Southern Ethiopia in 2019.
To identify the factors associated with maternal delays for institutional delivery service utilization among postnatal mothers who gave birth at public health facilities in selected rural Woredas in Gamo zone, Southern Ethiopia in 2019.
Methods
Study Design and Setting
This facility-based cross-sectional study was conducted from March 1, 2019-April 30, 2019 in the Gamo zone which located 450kms from Addis Ababa, the capital city of Ethiopia and 275 km from Hawassa. Gamo zone is one of the zones of Southern Ethiopia. The Zone has a total of nine rural districts. There are four primary hospitals and one general hospital, 53 health centers, and 299 health posts.
Population
All postnatal mothers who give birth at public health facilities of the Gamo zone were source population whereas all post-natal mothers who give birth at public health facilities of the Gamo zone during the data collection period were study population.
Eligibility Criteria
All postnatal women who visited the public health facilities (PHF) for delivery service were included in the study area whereas all women who are severely ill during data collection period and women who utilized maternal waiting home were excluded.
Sample Size and Sampling Procedure
The minimal sample size required for this study was calculated using the Epi Info version 7.02 statistical software package with the assumption of 95% confidence level (Zα/2= 1.96), 80% power (Zβ= 0.84). The magnitude of first, second, and third maternal delays in utilizing institutional delivery service were 37.8%,14 29.7%,15 and 34.7%16 respectively. Considering a 10% nonresponse rate, the maximum sample size requires for this study was found to be 394 postnatal mothers (for first delay), 352 postnatal mothers (second delay), and 383 postnatal mothers (third delay). Since the sample size calculated for the first delay was greater than the second and third delays, 394 postnatal mothers were involved in the study.
To get the study participants, first, two districts (Dita and Chencha Zuriya districts) were selected randomly from the nine rural districts. All public health centers in the two selected districts were included and the sample size was proportionally allocated to all public health centers based on their monthly delivery load. Then, by using a simple random sampling method study participants were selected and interviewed in each health center.
Study Variables
Dependent Variables
First maternal delay: Was the time interval between recognition of the labor and make decision to seek institutional delivery service. Time taken ≥1 hr to make decision to seek care was considered as delay and less than an hour considered no delay.
Second maternal delay: was time interval from starting to reach health facilities after decision has made. Time taken ≥1 hr to reach facility considered as delay and less than an hour considered no delay.
Third maternal delay: was the time interval between reaching the facility and the delivery care service received. Time taken ≥1 hr to receive delivery service considered as delay and less than an hour considered no delay.
Independent Variables
Socio-economic factors: Maternal age, educational status of mother, husband’s education status, occupation of mother, occupation of husband, household monthly income, women decision-making power.
Obstetric health related factors: ANC follow-up, ANC frequency, number of children, previous pregnancy related problem, birth preparedness, type of delivery, and mother’s knowledge on danger signs of labor and childbirth.
Health-care system related factors: Multiple referrals, Absence of care provider, Lengthy admission process, and absence of obstetric drugs
Accessibility of facility-related factors: distance to health care facility, transportation inaccessibility, road unavailability and means of transportation used.
Data Collection Procedure
The data were collected by using face-to-face interviewer-administered and pre-tested structured questionnaires. The questionnaire was partly adapted from the survey tools developed by JHPIEGO maternal and neonatal health program.13 Also, it was adapted from published relevant literature.6,9,17,18,19 Initially it was prepared in English. The English version of the questionnaire was translated to the local language (Gammotho) and back-translated to English by language experts to check for its original meaning. The questionnaire was pre-tested on 20 respondents (5% of sample size) in Chencha primary hospital which was one of unselected health facilities to ensure clarity, wordings, logical sequence and skip patterns of the questions. Based on the pretest, the time needed to complete an interview and the total number of days needed for data collection was estimated. An appropriate training for data collectors and supervisors that include a briefing on the data collection process of the study, discussing the contents of the questionnaire were carried out. The overall activity of data collection was supervised and coordinated by the supervisors. The collected data were reviewed and checked for completeness and relevance before data entry by the investigator. The variables were defined or coded, then the data editing was carried out during the entry of data.
Data Processing and Analysis
Data were entered into Epi Data version 4.4 software and then exported to SPSS version 21.0 statistical package for social science (SPSS) for analysis. Descriptive statistics using frequencies, percentages, mean and standard deviations were used to describe findings. Bivariate analysis using logistic regression was done and all explanatory variables which have an association with the outcome variable at the p-value of less than 0.25 were selected as candidates for multi–variable analysis. Multi-collinearity between the candidate variables was checked. The level of statistical significance was declared at a p-value of less than 0.05 and AOR with 95% CI was used to measure the degree of association between independent variables and an outcome variable. Model fitness was checked using Hosmer and Lemeshow goodness of fitness test.
Ethics Consideration
Before the study conducted ethical clearance obtained from Arba Minch University, College of Medicine and Health Sciences institutional review board (IRB) with reference number of CMHS/12033814/111. Written informed consent was obtained from study participant for those aged 18 and above. For those participants, less than 18 years of age written informed consent was obtained from a parent or guardian using standard disclosure procedures. The confidentiality and privacy of participants were actively protected. All participants were assigned a unique identification number. Every effort was made to emphasize the voluntariness of this study and decisions to stop or discontinue in the study was respected and did not affect the regular attendance of care in any way.
Results
Socio-Economic Characteristics of the Study Participant
A total number of 394 respondents were included in the study, with a 99.24% response rate. Of which 316 (80.8%) of the respondents were aged between 21 and 34 years old and the mean age of mothers was 29 years (SD ±4.6). Most of the respondents, 266 (68%) were unemployed and 248 (63.4%) of respondents’ husbands were also unemployed. Regarding educational status, almost half of women and their husbands cannot read and write, 226 (57.8%) and 201 (51.4%) respectively (Table 1).
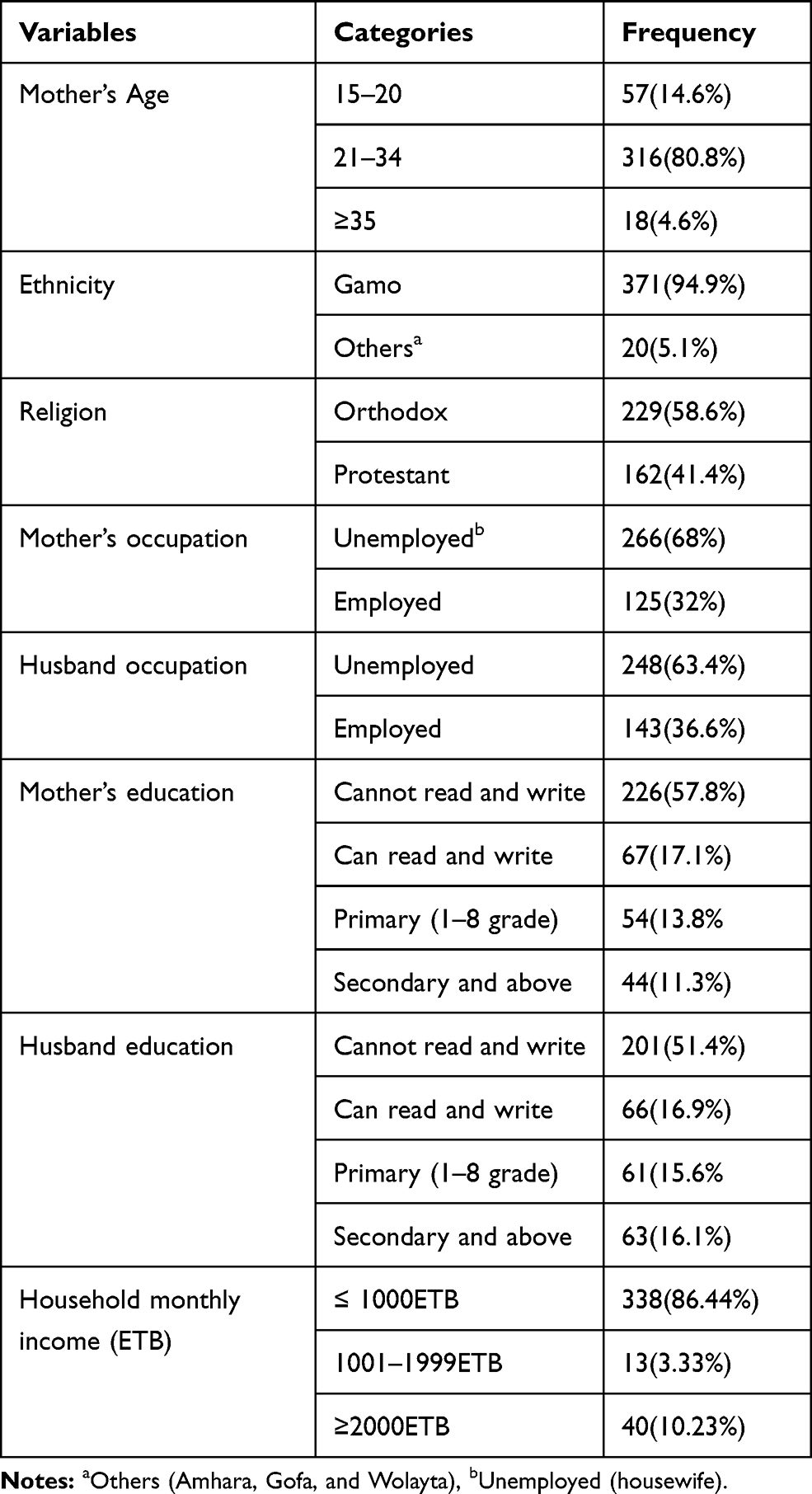 |
Table 1 The Socio-Economic Characteristics of Study Participants in Selected Rural Districts in Gamo Zone, Southern Ethiopia, 2019 (N=391) |
Obstetric Related Characteristics of the Study Participant
About 60 (15.3%) of the respondents faced obstetric problems during previous pregnancy. Out of respondents 239 (61.1%) were well prepared for birth and its complication and 209 (53.5%) of them had good knowledge on danger signs of labor/childbirth. Regarding women’s decisions, 108 (27.6%) decide jointly, 133 (37.4%) decide by their husbands, and the rest 137 (35%) decide by women (Table 2).
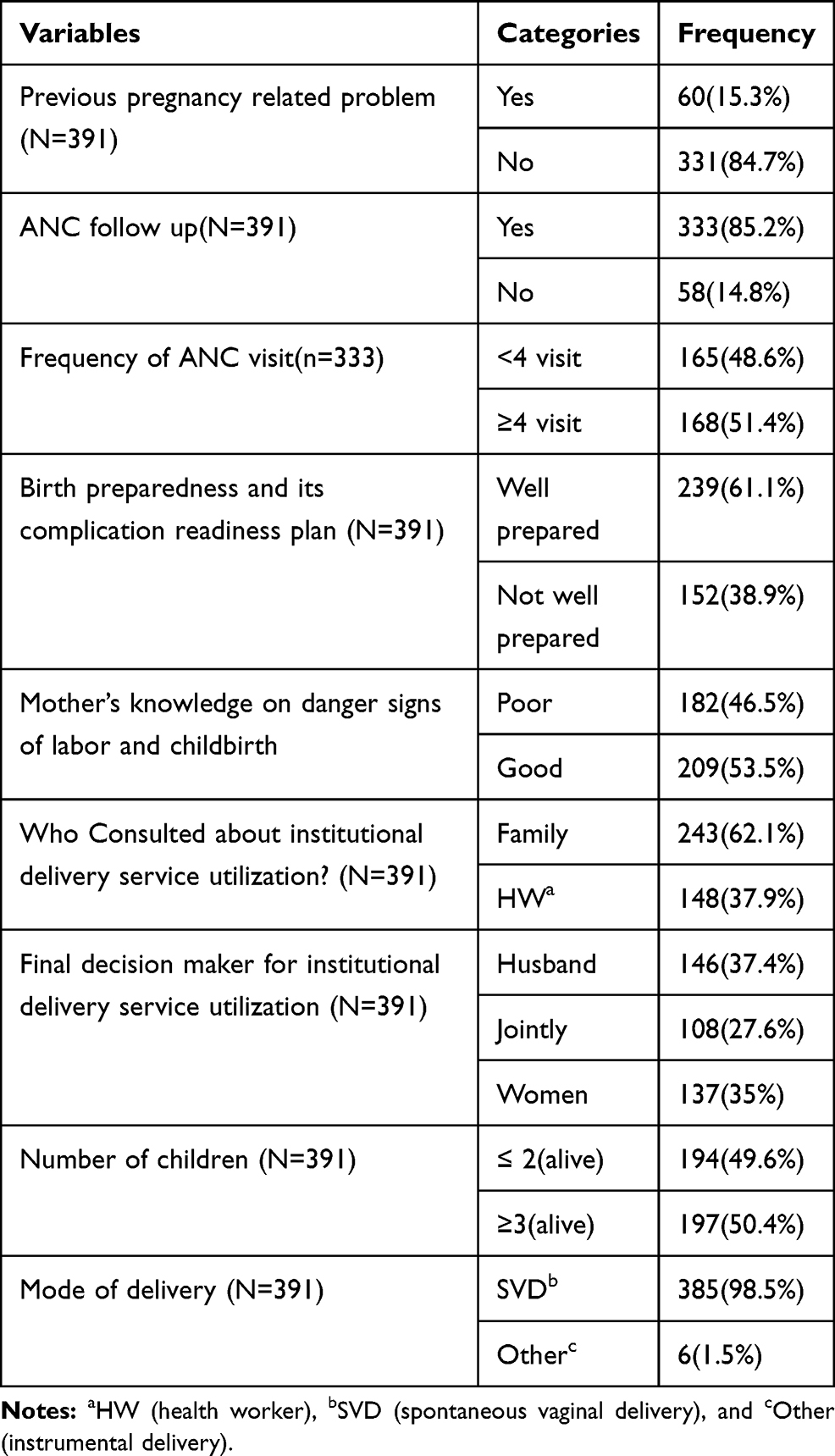 |
Table 2 The Obstetric Related Characteristics of Study Participants in Selected Rural Districts in Gamo Zone, Southern Ethiopia, 2019 |
Health Facility-Related Characteristics the Study Participant
Among respondents, 148 (37.9%) of mothers live in a physical distance greater than or equal to 5 km to reaching nearby health facilities. Concerning means of transportation 199 (50.9%) respondents were carried by wooden stretcher, 133 (34%) were traveled on foot and, the rest 59 (15.1%) were traveled by Ambulance to reach the nearest health facility. With regards to the health-care system, 107 (27.4%) respondents did not get skilled health providers after arrival at the nearby health center. Nearly one-third, 126 (32.2%) of respondents had not got drugs from nearby health centers (Table 3).
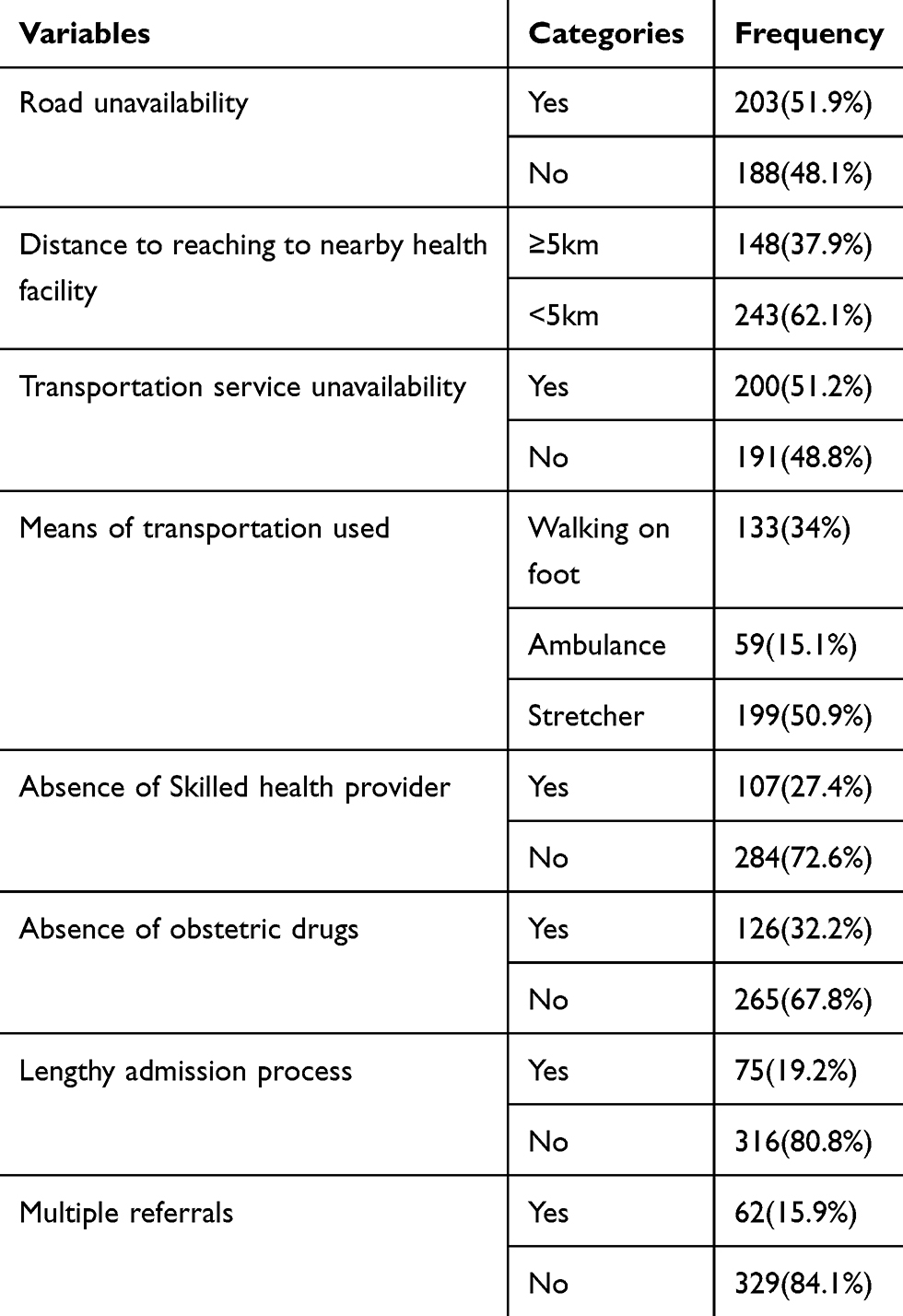 |
Table 3 Health Facility-Related Characteristics of Study Participants in Selected Rural Districts in Gamo Zone, Southern Ethiopia, 2019 (N=391) |
Magnitude of Maternal Delays
In this study, the first delay, delay in decision making to seek institutional delivery service was 183 (46.8%) with [95% CI (41.9, 51.7)] and the mean delay time was 5 hrs with SD±2.6. Among respondents, the reasons for mothers to experience first delay was previous normal pregnancy outcome in 177 (45.3%) of the respondents, labor starting at night in 98 (25.1%) of the respondents, no money for transportation service in 13 (3.3%) of study subjects, no one to care for children remained at home in 82 (21%) of study participants. Besides, the study showed that the magnitude of the second maternal delay in utilization for institutional delivery service was 172 (44%) with [95% CI (39.4, 48.9)] and the mean delay time was 2.1 hrs with SD±0.93. Also, the study showed that the magnitude of third maternal delay in utilization for institutional delivery service was 124 (31.7%) with [95% CI (27.1, 36.1)] and the mean delay time was 1.56 hrs with SD±0.98 (Figure 1).
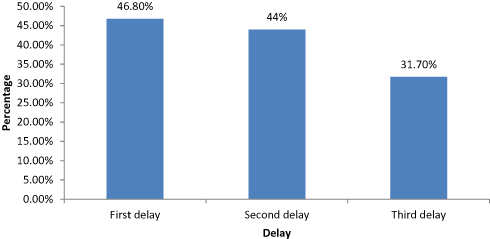 |
Figure 1 Magnitude of maternal delays among post-natal mothers in selected rural Woredas in Gamo Zone, Southern Ethiopia, 2019. |
Factors Associated with Maternal Delays Among Post-Natal Mothers
The binary logistic regression analysis showed that age of mother, mother’s occupation, husband’s occupation, mother’s education, husband’s education, previous pregnancy-related problem, ANC follow up, birth preparedness and complication readiness, mother’s knowledge on danger signs of labor and child health, number of children, consultation for institutional delivery service, decision-maker for institutional delivery service, and household monthly income were found to be candidate variables for multivariable logistic regression analysis with the first maternal delay at p-value less than or equal to 0.25. From the total 13 variables that were entered into multivariable logistic regression analysis by stepwise backward logistic regression technique, five variables were significantly associated with the first maternal delay in utilization of institutional delivery service. Mother’s education, previous pregnancy health-related problems, birth preparedness, knowledge of danger signs of labor & childbirth, and decision-maker for institutional delivery were found to be significantly associated with first delay (Table 4).
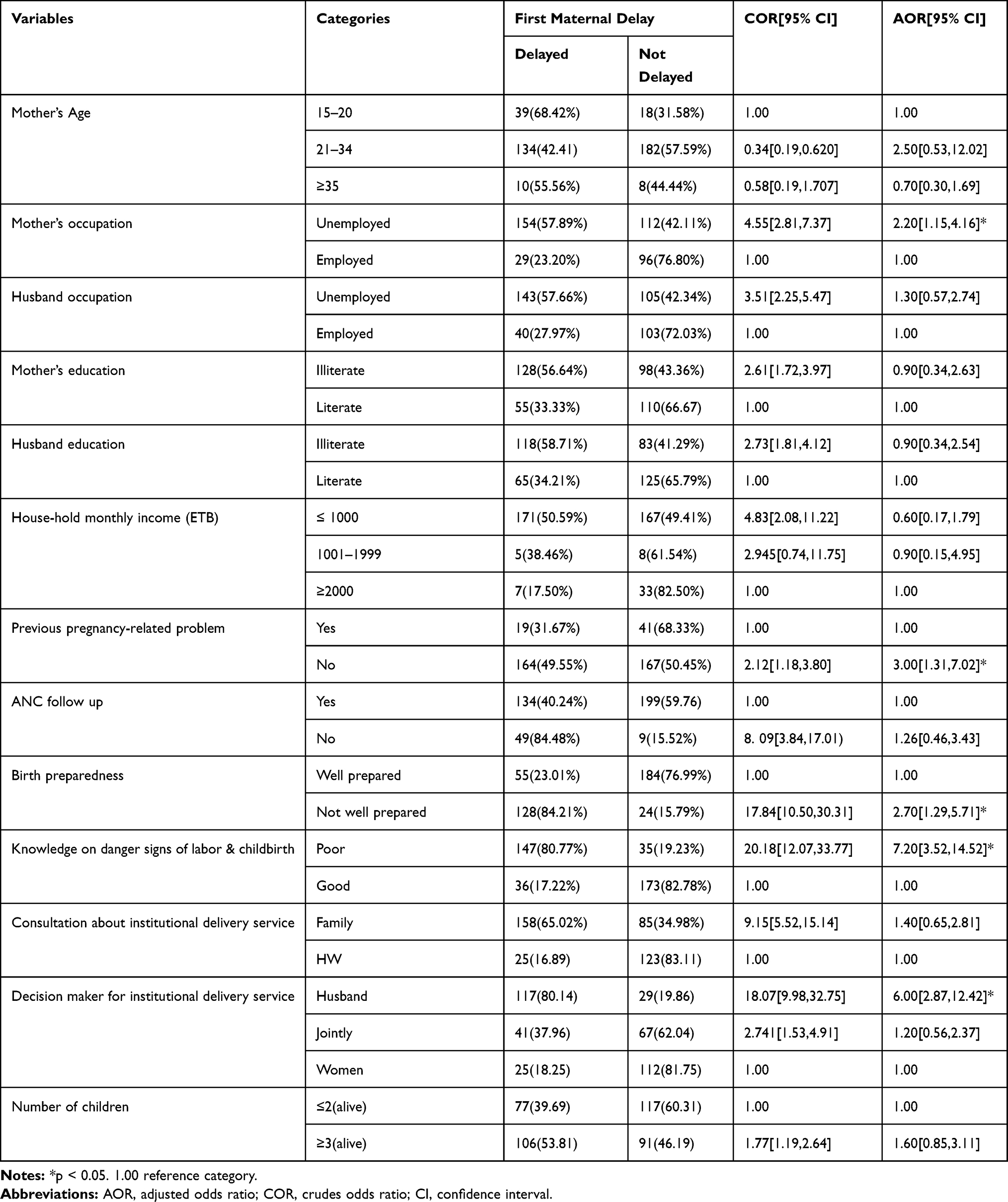 |
Table 4 Factors Associated with First Maternal Delay in Utilization of Institutional Delivery Service Among Post-Natal Mothers in Selected Rural Districts of Gamo Zone, Southern Ethiopia, June 2019 |
Factors Associated with First Maternal Delay Among Postnatal Mothers
Factors Associated with Second Maternal Delay Among Postnatal Mothers
From the total nine variables were entered into multivariable logistic regression analysis, five variables were significantly associated with a second maternal delay in the utilization of institutional delivery service. Husband education, transport unavailability, distance to health facility, and means of transportation were found to be significantly associated with the second delay (Table 5).
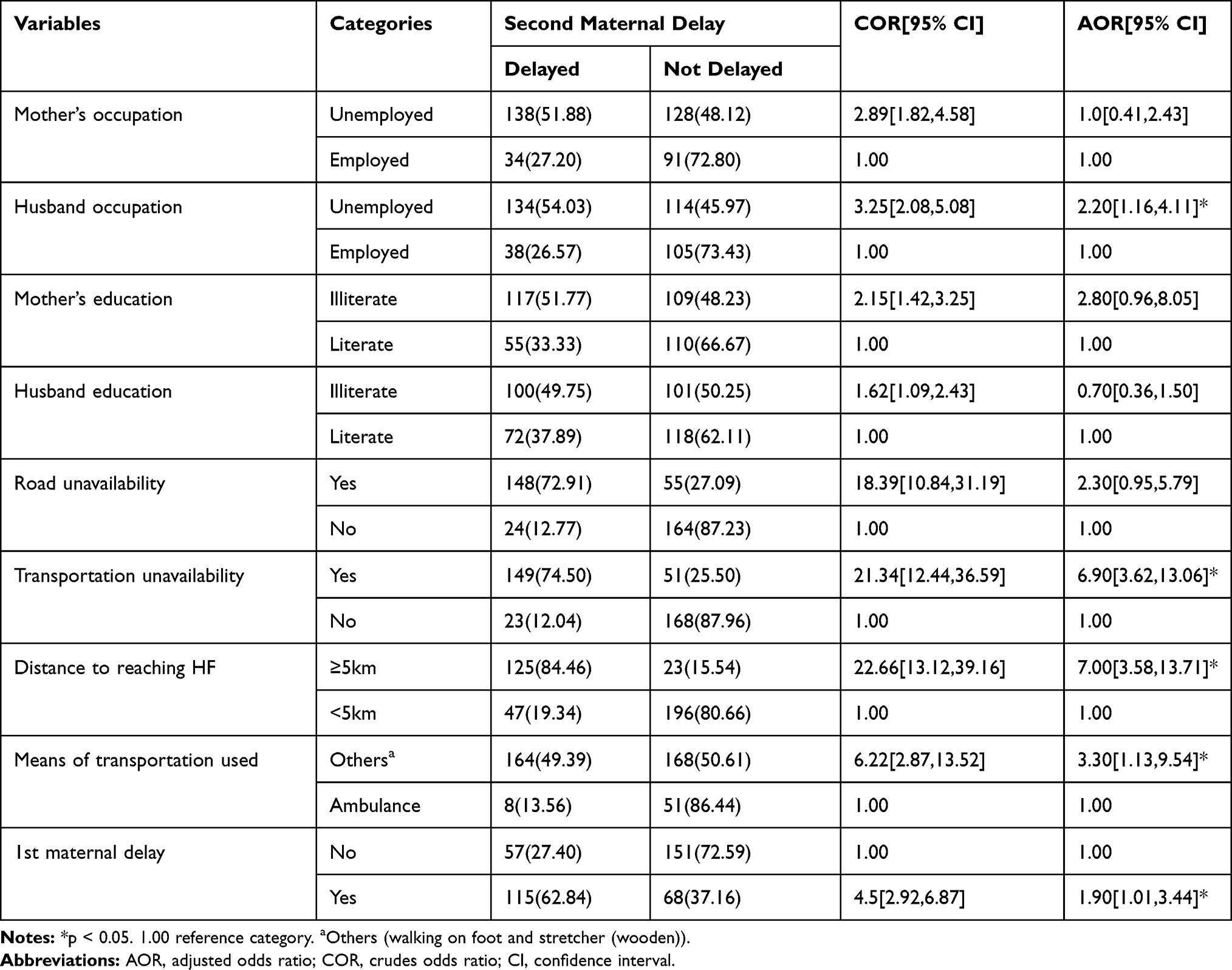 |
Table 5 Factors Associated with Second Maternal Delay in Utilization of Institutional Delivery Service Among Post-Natal Mothers in Selected Rural Districts of Gamo Zone, Southern Ethiopia, June 2019 |
Factors Associated with Third Maternal Delay Among Postnatal Mothers
From the total six variables were entered into multivariable logistic regression analysis, four variables were significantly associated with the third maternal delay in the utilization of institutional delivery service. Absence of skilled health provider, absence of essential obstetric drugs, first maternal delay and second maternal delay were found to be significantly associated with the third delay (Table 6).
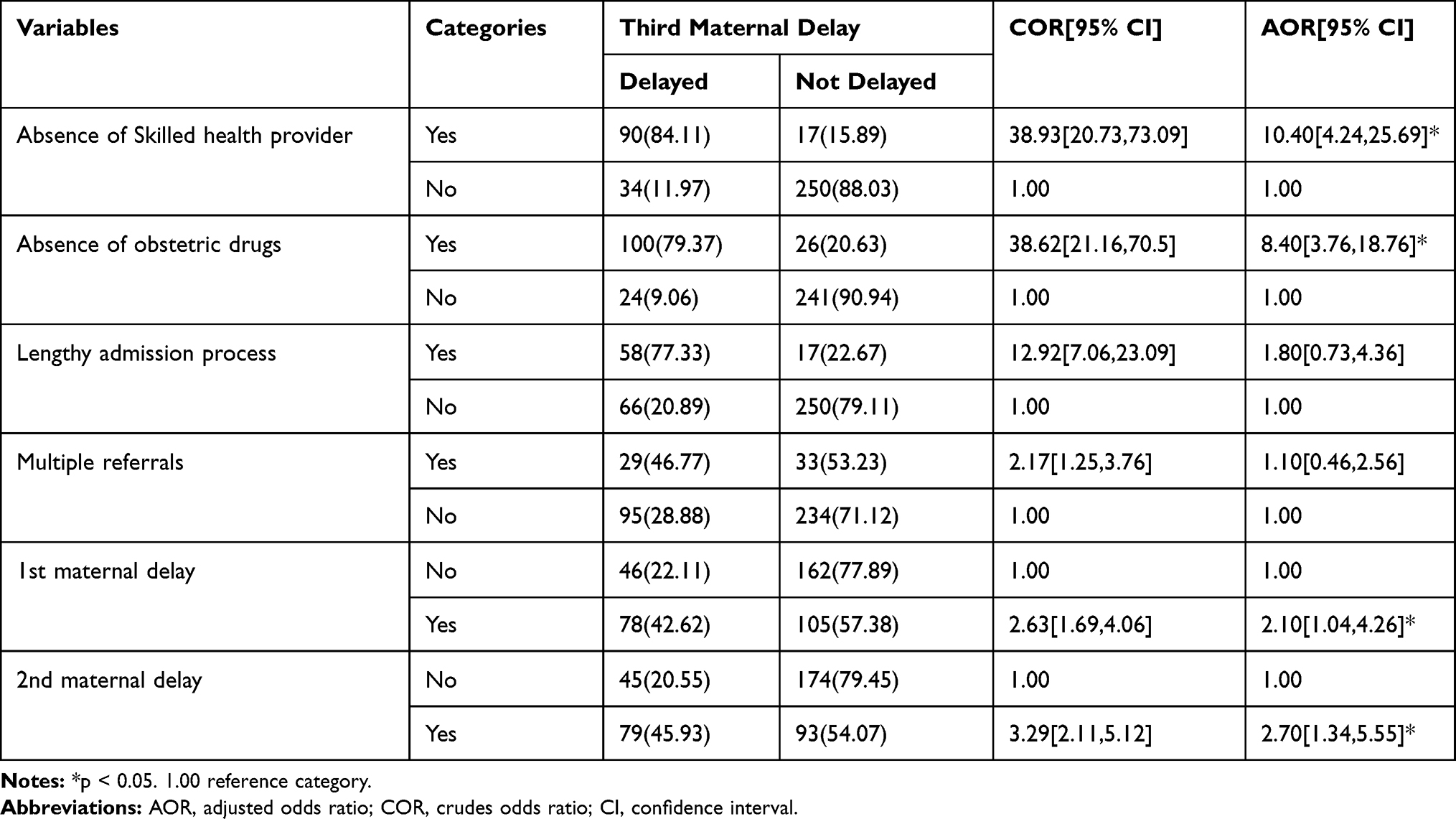 |
Table 6 Factors Associated with the Third Delay in the Utilization of Institutional Delivery Service Among Post-Natal Mothers in Selected Rural Districts of the Gamo Zone, Southern Ethiopia. June 2019 |
Discussion
The finding of this study found that the magnitude of first, second and third maternal delays were 46.80%, 44.00%, and 31.70%, respectively. Unemployed women, birth preparedness, husband’s decisions making were found to be significantly associated with first delay. Distance to health facility and means of transportation were found to be significantly associated with the second delay. Availability of obstetric drugs and availability of skilled health provider were found to be significantly associated with the third delay for institutional delivery.
The magnitude of the first maternal delay in the utilization of institutional delivery service was 46.8%. The finding of this study was consistent with the study done in Yem special district, Southern Ethiopia, 44.2%.18 But it is higher than the findings from studies in Bahir Dar town, Northern Ethiopia, 37.8% and Hadiya zone, Southern Ethiopia,40.1%.9,17 The possible reason for this discrepancy might be since the current study only involved in rural women while the previous studies conducted in urban women. It is known that urban women have relatively better education, economy and access to information. This implies that most mothers did not decide to seek institutional delivery service on time at the household level.15
However, the finding of this study is lower than the study findings in Pakistan, 71%,15 in Bangladesh, 69.3%,16 in Nigeria, 57%.19 This is might be due to the difference in time of the studies conducted, population difference, scope of the study, methodological difference, lack of health extension program, and the way of people’s life.
The result of this study showed that the first maternal delay in the utilization of institutional delivery service was significantly influenced by the occupation of the mother. Unemployed mothers were more likely to have first maternal delay in utilization of institutional delivery service than employed mothers. This study is in line with the study done in Bahir Dar, Amhara region and Hadiya zone, Southern Ethiopia.9,17 The possible explanation could be women not involved in income-generating activities, which in turn can be the cause of women’s dependency on their husbands’ income, consequently, influence timely decide to receive institutional delivery service.
Women’s decision-making power was also one of the factors associated with the first maternal delay in the utilization of institutional delivery service. Women whose husband made decisions were more likely to experience a first maternal delay in the utilization of institutional delivery service as compared to those who decided on their own. This finding is similar to those of studies conducted in Bahir Dar, Amhara region and Yem special district, Southern Ethiopia.9,18 This might be due to husbands or male partner’s dominance in decision making and hence, increase the risk of delay.
Similarly, birth preparedness and its complication readiness were some of the other factors associated with the first maternal delay in the utilization of institutional delivery service. Women with no birth preparedness for institutional delivery service were more likely to have first maternal delay in the utilization of institutional delivery service as compared to those were well prepared for birth and its complications. This finding was supported by a study conducted in Bangladesh and Yem special district, Southern Ethiopia.14,18 This could be due to those well-prepared women aware of the importance of timely decision to receive delivery service and know where or when to go to seek care.
The study indicated that women who faced no obstetric problems during the previous pregnancy were more likely to have the first delay in the utilization of institutional delivery service compared to those who faced obstetric problems. This finding is coherent with the study done in Bahir Dar Ethiopia.9 This might be because of mothers develop confidence and experiences that the index pregnancy would also be without problems. This implies that health workers should create awareness of obstetric complications during pregnancy, labor and childbirth, and post-partum because all pregnant mothers were risky unless served by a skilled health provider.
The study also revealed that women who have poor knowledge of the danger signs of labor and childbirth were more likely to experience the first delay in the utilization of institutional delivery service as compared to those who had good knowledge. This finding in line with the study done in Tanzania.20 This might be women have poor awareness of obstetric danger signs during labor and childbirth. This implies that health professionals should strive to create awareness activities for pregnant mothers on danger signs during labor and childbirth during ANC follow uptime.
This study finding showed that the magnitude of second maternal delay in utilization of institutional delivery service was 44%. This finding was similar to the finding of the study done in Yem special woreda, Southern Ethiopia, 43.2%.18 But it is higher than the findings from studies in Urban Bangladesh 38%,14 in Bahir Dar town, Amhara region 31.7%9 and in Hadiya zone, the Southern region was 29.7%.17 The difference might be due to the inaccessibility of health facility, place of study setting, unavailability of road and inadequate Ambulance service, and economic status of women. This implies that many mothers were spent their time walking on foot as well as were carried by wooden stretchers to reach nearby health centers.12 However, the findings of this study are lower than the study findings in Pakistan, 74%,15 in Afghanistan, 65%,21 in Egypt, 55.3%.22 This might be the time gap of the study, road, and telecommunication infrastructure improvements, and expansion and closeness of health facilities to the community.
The study found that mothers who use other means of transportation were more likely to face second maternal delay in utilizing institutional delivery service than mothers those used ambulances. This result is coherent with the study done in Hadiya zone, Southern Ethiopia.17 This might be inadequate ambulance services as well as transportation difficulties and a lack of money for accessing institutional delivery services.23 This all might delay the mother to utilize delivery services. This implies that the majority of postnatal mothers were not used in Ambulance services.
The study also revealed that second maternal delay in utilizing institutional delivery service was higher among mothers living more than 5 kms from nearby health centers when compared to those living within 5 kms rang. This result is coherent with the study done in Hadiya zone, Southern Ethiopia.17 This might be the longer the physical distance to reaching caregiving health centers may require more relatives to accompany with mother and prolongs reaching time to health facility. This implies that women have difficulty to obtain transportation services, which may require more relatives to accompany as well as walking on foot for a long time, which in turn can be the cause of women’s face obstetric complications, consequently influence timely reach to nearby health facility to receive institutional delivery service.21
Further, the study showed that mothers with unemployed husbands were more likely to face a second delay in utilizing institutional delivery service when compared to those mothers with employed husbands. This may be explained with the husband was not involved in income-generating activities, which in turn can be directly the cause of women to have not accessing to transportation service even if transportation service is available as well as needs more relatives to accompany at times of referrals in case of emergencies. This implies that further efforts are required husband’s occupational status affects the second delay.
This study investigation showed that the magnitude of third delay in utilization of institutional delivery service was found 31.7% which was consistent with the study findings in Bahir Dar Ethiopia 30.7%,9 in Yem special district, 34.7%,18 and in Hadiya zone, Southern region was 32.6% 17 but this is higher than study finding in Jordan, which was 17.1%.24 This might be a health service delivery system difference, difference in the study setting, medical supply difference, and professional staff in skilled delivery.25 This implies that mothers waited for a long time to utilize institutional delivery service after they arrived at the health center.18,25
The absence of skilled health providers was the factor associated with the third maternal delay in the utilization of institutional delivery service. The study revealed that mothers who did not get skilled health providers were more likely to experience a third maternal delay in the utilization of institutional delivery service when compared to mothers who had got a skilled health-care provider. This result is in line with the study done in Hadiya zone Ethiopia.17 This can be explained in different ways as the health workers were overwhelmingly deficient due to the absence of continuing education programs, adequate formal learning, as well as poor access to update educational resources, lack of staff motivation issues, and lack of accountability.25,26 This all might delay the mother to utilize delivery services.
The absence of obstetric drugs was another factor that associated with a third maternal delay in the utilization of institutional delivery service. This study showed that mothers who did not get drugs were at higher risk of delaying in the utilization of institutional delivery service than mothers who had to get drugs. This finding was supported by the systematic review study in developing countries.25
Limitations
Readers should be cautious when interpreting the findings of this study, since the data were obtained from women who attended institutional delivery that might not representative to all women who give birth in Ethiopia. Since interviewer-administered questionnaire was used to collect data that may be prone to social desirability bias. Furthermore, this study uses of a cross-sectional design which failed to distinction case and effect relationship. Further research should be conducted to identify factors associated with maternal delays to strengthen and broaden our results in different countries.
Conclusion
This study showed that the magnitude of first, second and third maternal delays in the utilization of institutional delivery services in our study area was high which indicates that most of the mothers were not utilize institutional delivery services in the recommended time range. Mother’s knowledge of danger signs of labor, mother’s occupation, birth preparedness and complication readiness, husband’s decision making for utilization of institutional delivery service and history of pregnancy-related problem, and husband’s decision making for utilization of institutional delivery service were factors that associated with first maternal delay. Besides, distance to reaching health-care facility means of transportation used, husband occupation, and transportation service difficulties were factors associated with maternal second delay. Furthermore, the absence of skilled health providers and the absence of obstetric drugs were factors associated with the third maternal delay in the utilization of institutional delivery service. Therefore, emphasis should be given for awareness creation on key danger signs during labor and childbirth, women empowerment in decision making, strengthening ambulance services and availing obstetric drugs at health center levels to save mother and neonate.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; BPCR, Birth Preparedness and Complication Readiness; CI, Confidence Interval; CMHS, College of Medicine and Health Sciences; COR, crudes odds ratio; HW, Health Worker; IRB, Institutional Review Board; SBA, Skilled birth attendants; SPSS, Statistical Package for Social Science; SSA, Sub-Saharan Africa; SVD, Spontaneous Vaginal Delivery.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request with an email address of [email protected]
Acknowledgment
We would like to acknowledge all study participants for their voluntary participation in this study. We would like to extend our gratitude to Arba Minch University for all the support and opportunity provided for us to conduct this study.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of version to be published and agree to be accountable for all aspects of the worker.
Funding
Arba Minch University supports this research financially. The university has no role in the design of the study, collection, analysis, and interpretation of the data and in writing the manuscript.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091–1110. doi:10.1016/0277-9536(94)90226-7
2. Darega B, Dida N. Challenges of maternal health services utilization and provision from health posts in Bale Zone, Oromiya Regional State, Southeast Ethiopia: Qualitative Study. Primary Health Care. 2015;5(189):2167–1079.
3. EFMoH. The Health Sector Development Program IV (HSDP IV). Addis Ababa, Ethiopia; 2010 November.
4. Shigute T, Tejineh S, Tadesse L. Institutional delivery service utilization and associated factors among women of child-bearing age at Boset Woreda, Oromia Regional State, Central Ethiopia. J Women's Health Care. 2017;6(394):2167–2420. doi:10.4172/2167-0420.1000394
5. Mathers C; WHO U. Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). Organization; 2016.
6. Andarge E, Nigussie A, Wondafrash M. Factors associated with birth preparedness and complication readiness in Southern Ethiopia: a community based cross-sectional study. BMC Pregnancy Childbirth. 2017;17(1):412. doi:10.1186/s12884-017-1582-3
7. Gultie T, Wasihun B, Kondale M, Balcha B. Home delivery and associated factors among reproductive age women in Shashemene Town, Ethiopia. J Women's Health Care. 2016;5(300):2167–2420. doi:10.4172/2167-0420.1000300
8. El Gelany S, Mansour MG, Hassan MM. The three delays of maternal mortality in a public-sector tertiary teaching hospital: is there a paradigm shift. Gynecol Obstet Res Open J. 2015;2(2):52–56. doi:10.17140/GOROJ-2-112
9. Awoke W, Seleshi K. Maternal delays in utilizing institutional delivery services, Bahir Dar, Ethiopia. Health. 2013;5(06):1026. doi:10.4236/health.2013.56137
10. Choguya NZ. Traditional and skilled birth attendants in Zimbabwe: a situational analysis and some policy considerations. J Anthropol. 2015;2015.
11. Tegegne TK, Chojenta C, Loxton D, Smith R, Kibret KT, McKinnon B. The impact of geographic access on institutional delivery care use in low and middle-income countries: systematic review and meta-analysis. PLoS One. 2018;13(8):e0203130. doi:10.1371/journal.pone.0203130
12. Win T, Vapattanawong P, Vong-ek P. Three delays related to maternal mortality in Myanmar: a case study from maternal death review, 2013. J Health Res. 2015;29(3):179–187.
13. JHPIEGO. Monitoring Birth Preparedness and Complication Readiness. Tools and Indicators for Maternal and Newborn Health. Baltimore, Maryland 21231-3492. USA; 2004. Avialable from: http://reprolineplus.org/system/files/resources/bpcr_monitoringtools.pdf.
14. Nahar S, Banu M, Nasreen HE. Women-focused development intervention reduces delays in accessing emergency obstetric care in urban slums in Bangladesh: a cross-sectional study. BMC Pregnancy Childbirth. 2011;11(1):11. doi:10.1186/1471-2393-11-11
15. Shah N, Hossain N, Shoaib R, Hussain A, Gillani R, Khan NH. Socio-demographic characteristics and the three delays of maternal mortality. J Coll Physicians Surg Pak. 2009;19(2):95–98.
16. Killewo J, Anwar I, Bashir I, Yunus M, Chakraborty J. Perceived delay in healthcare-seeking for episodes of serious illness and its implications for safe motherhood interventions in rural Bangladesh. J Health Popul Nutr. 2006;24(4):403.
17. Lire A, Beyamo A, Tadele D, Facha W. Delays for utilizing institutional delivery and associated factors among mothers attending public health facility in Hadiya Zone, Southern Ethiopia. Science. 2017;5(6):149–157.
18. Yarinbab TE, Balcha SG. Delays in utilization of institutional delivery service and its determinants in Yem Special Woreda, Southwest Ethiopia: health institution based Cross Sectional Study. J Gynecol Women's Health. 2018;10(4):555793.
19. Okusanya BO, Okogbo FO, Momoh MM, Okogbenin SA, Abebe JO. Maternal mortality and delay: socio-demographic characteristics of maternal deaths with delay in Irrua, Nigeria. Niger J Med. 2007;16(1):38–41. doi:10.4314/njm.v16i1.37279
20. Mrisho M, Schellenberg JA, Mushi AK, et al. Factors affecting home delivery in rural Tanzania. Trop Med Int Health. 2007;12(7):862–872. doi:10.1111/tmi.2007.12.issue-7
21. Hirose A, Borchert M, Cox J, Alkozai AS, Filippi V. Determinants of delays in travelling to an emergency obstetric care facility in Herat, Afghanistan: an analysis of cross-sectional survey data and spatial modelling. BMC Pregnancy Childbirth. 2015;15(1):14. doi:10.1186/s12884-015-0435-1
22. Abdel-Raheem SS, Al-Attar GS, Mahran DG, Qayed MH, Alib ZA, Othman EE. Delays associated with maternal near-miss cases admitted in Women’s Health Hospital, Assiut University. J Curr Med Res Pract. 2017;2(1):1. doi:10.4103/2357-0121.210300
23. Kawuwa MB, Mairiga AG, Usman HA. Community perspective of maternal mortality: experience from Konduga local government area, Borno state, Nigeria. Ann Afr Med. 2007;6(3):109. doi:10.4103/1596-3519.55724
24. Okour AM, Khader Y, Amarin Z, Jaddou H, Gharaibeh M. Maternal mortality in Jordan: role of substandard care and delays. East Mediterr Health J. 2012;18(5):426–431, 2012. doi:10.26719/2012.18.5.426
25. Knight HE, Self A, Kennedy SH, Young RC. Why are women dying when they reach hospital on time? A systematic review of the ‘third delay’. PLoS One. 2013;8(5):e63846. doi:10.1371/journal.pone.0063846
26. Pitchforth E, Lilford RJ, Kebede Y, Asres G, Stanford C, Frost J. Assessing and understanding quality of care in a labour ward: a pilot study combining clinical and social science perspectives in Gondar, Ethiopia. Soc Sci Med. 2010;71(10):1739–1748. doi:10.1016/j.socscimed.2010.08.001
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.